Embed Size (px)
Citation preview

PII S0730-725X(98)00127-1
● Original Contribution
MR VIRTUAL ENDOSCOPY OF THE PANCREATICOBILIARY TRACT
EMANUELE NERI,* PIERO BORASCHI,† GIOVANNI BRACCINI,† DAVIDE CARAMELLA ,* GIUSEPPEPERRI,†AND CARLO BARTOLOZZI*
*Diagnostic and Interventional Radiology, University of Pisa, Pisa; and †2nd Department of Radiology,Pisa University Hospital, Pisa, Italy
Purpose: To evaluate the feasibility of surface-rendered magnetic resonance virtual endoscopy (MRVE) ofmagnetic resonance cholangiopancreatography (MRCP) data sets. We retrospectively reviewed MR cholangio-pancreatography data sets of 120 patients with biliary stone (n 5 40), inflammatory ampullary stenosis (n 5 12),pancreatic tumor (n 5 8), cholangiocarcinoma (n 5 7), stenosis of surgical bilio-enteric anastomosis (n 5 4),extrinsic localized common bile duct stenosis (n 5 2), ampullary carcinoma (n 5 2), pancreatic duct stone (n 51), tumor of the gallbladder (n 5 1), and normal pancreaticobiliary tree (n 5 43). MRVE views were generatedwith Navigator software. Segmentation of the acquired data sets was performed with a thresholding technique.Navigation sequences were simulated through the entire biliary tract. MRVE was obtained in 27 (63%) of the 43normal patients. Endoscopic views were generated in all 77 patients with partial or complete obstruction of thepancreaticobiliary tree. Among these, three groups of patterns were identified: 36 (47%) endoluminal masses(polyp-like masses), 17 (22%) luminal stenoses, 24 (31%) luminal occlusion. In 29 cases, hole artifacts throughthe internal wall were observed and interpreted as mistakes of segmentation. MRVE proved to show the internalanatomy of the biliary tract and endoluminal changes due to pathological condition. Further investigations areneeded to test the usefulness and the potentialities of this technique. © 1998 Elsevier Science Inc.
Keywords:Bile ducts; Image processing; Calculi; Endoscopy.
INTRODUCTION
The exploration of the biliary tract with fyberopticcholangioscopy is a relatively new and well-establishedprocedure that has found interesting applications in thediagnostic approach and therapeutic management of bil-iary stones, in the differential diagnosis between benignand malignant lesions, and in the staging of duct malig-nancy. However this technique is invasive and affectedby many complications related to the use of the cholan-gioscopes, e.g., haemorrhage into the biliary ducts (witha percentage ranging between 4.1% and 12%), lacerationof the bile duct (2%), bacteriemia, vagal reactions, nau-sea, fever and diarrhoea.1–4 Therefore, the diagnosticapproach to biliary tract pathology is reasonably coveredby other less- or non-invasive techniques, such as ultra-sound, computer tomography, magnetic resonancecholangiopancreatography (MRCP) and endoscopic ret-rograde cholangiopancreatography (ERCP). Among
these, MRCP has shown high diagnostic potentialities,and has been effectively introduced in the clinical prac-tice. One of the advantages of this technique is thepossibility to process its data sets to generate three-dimensional (3D) reconstruction of the bile ducts thatcan be obtained through the maximum intensity projec-tion (MIP) and the shaded surface display (SSD) algo-rithms. With these methods the 3D model provides ex-ternal views of the biliary tract that have not provenuseful for the diagnosis.5–10
The virtual simulation of fyberoptic endoscopy can beobtained with virtual endoscopy (VE). VE is a newsoftware tool, that render computer tomography and MRdata sets and is based on surface- or volume-renderingtechniques. The reported applications of VE include thestudy of the bronchial tree, colon, vascular structures,brain, ear, and urinary tract.11–23
The purpose of this study was to verify the feasibilityof MR virtual endoscopy (MRVE) of the biliary tract
RECEIVED 1/30/98; ACCEPTED4/5/98.Address correspondence to Emanuele Neri, M.D., Diparti-
mento Immagini - Ospedale Cisanello, Via Paradisa, 2–56100Pisa, Italy. E-mail: [email protected]
Magnetic Resonance Imaging, Vol. 17, No. 1, pp. 59–67, 1999© 1998 Elsevier Science Inc. All rights reserved.
Printed in the USA.0730-725X/99 $–see front matter
59

using MRCP data sets as source images, and thus todepict the endoluminal pattern of anatomy and patholog-ical findings showed by MRCP images.
MATERIALS AND METHODS
PatientsWe retrospectively reviewed MRCP data sets of 120
patients (age range 15–95, mean 59.96 16.3), 59 males(49%) and 61 females (51%), with biliary stone (n 5 40),inflammatory ampullary stenosis (n 5 12), pancreatictumour (n 5 8), cholangiocarcinoma (n 5 7), stenosis ofsurgical bilio-enteric anastomosis (n 5 4), extrinsic lo-calised common bile duct stenosis (n 5 2), ampullarycarcinoma (n 5 2), pancreatic duct stone (n 5 1), tumourof the gallbladder (n 5 1), and normal pancreaticobiliarytract (n 5 43). In all pathological cases the presence ofendoluminal mass, stenosis or obstruction of the biliarytract was clearly shown by MRCP images, and furtherconfirmed by ERCP in 62 cases, percutaneous transhe-patic cholangiography in 7 cases, and surgery in 8 cases.In the remaining normal patients, diagnosis was estab-lished by means of an ultrasound follow-up for at least 6months.
Among the patients investigated, 34 previously un-derwent cholecystectomy, whereas 12 had biliary-entericanastomoses (7 hepatico-jejunostomies, 5 choledoco-jejunostomies).
Image AcquisitionAll patients were imaged with a 1.5 T MR unit (Signa;
GE/Medical System, Milwaukee, WI, USA) with use ofa body coil for both excitation and signal reception.
A previous intramuscular (i.m.) administration of 20mg of scopolamine methyl-bromide (Buscopan®, Boehr-inger Ingelheim) was performed to avoid peristaltic ar-tefacts, whereas 300–500 mL of H2O were used as oralcontrast agent in an attempt to improve the visualisationof the duodenum.
A survey T1-weighted, respiratory-triggered, spin-echo axial MR examination [repetition time (TR)5 700ms; echo time (TE)5 20 ms; thickness5 5 mm;interslice gap5 1.5 mm; number of excitations (NEX)52] and a fast spin-echo T2-weighted, fat-suppressed, axialMR examination (TR5 4000 ms; TE5 100 ms; echotrain length (ETL)5 16; thickness5 5 mm; interslicegap 5 1.5 mm; 2 NEX) of the upper abdomen wereperformed first. These images served for general surveyof the upper abdomen and to localise the biliary andpancreatic trees for MRCP.
MRCP was performed with a non-breathhold, fat-suppressed, two-dimensional, heavily T2-weighted fastspin-echo sequence in coronal plane. Imaging parametersincluded the following: 7000/200 (TR ms/effective TE
ms); ETL 5 32; section thickness5 3 mm with nointerslice gap; field of view (FOV)5 24–26 cm; ma-trix 5 256 3 128 pixels; 2–4 NEX. Anterior-posteriorspatial presaturation was used for all images. The receivebandwidth was 10–16 kHz. Flow compensation and no-phase-wrap options were used. The length of time foracquisition of MRCP data sets ranged between 6 and 8min.
MR Virtual EndoscopyEndoscopic views were generated with Navigator
software (GE/Medical Systems, Milwaukee, WI, USA),that allows to display internal views by surface renderinganatomical structures with simulated lightning and shad-ing. Navigator ran on a UNIX workstation (SunSparc 20,Sun Microsystems, Mountain View, CA, USA), thatprovided 128 Mb of random access memory and 1.2 Gbdisk space available for images temporary local archive.
Source images for MRVE were obtained with thenon-breathhold, fat-suppressed, two-dimensional,heavily T2-weighted fast spin-echo sequences in thecoronal plane. Time for image acquisition ranged be-tween 5 and 9 min (mean 6,7). Images were transmittedthrough a local area network (Ethernet 802.6) from theMR scanner to the workstation.
The software allowed the segmentation of the data setwith a thresholding technique. With this method, therange of gray values, in which the desired voxels wereincluded, could be selected directly. Subsequently, on theworkstation screen that was divided into four quadrants,each displaying variably the endoscopic views, the coro-nal images, the multiplanar recontructions (MPR) andthe MIP reconstructions, the selected voxels were auto-matically painted on the desired image (we preferred thecoronal and MIP). The density range was consideredreliable when all the brightest voxels corresponding tothe bile ducts were selected and painted.
The interaction between the images displayed simul-taneously on the four quadrants was possible by usingthe “pick-a-point” function. This function allowed toselect a point on the endoscopic view with the mousecursor and display simultaneously on the screen quad-rants the corresponding point in the MIP reconstruction,or the coronal, axial and sagittal views crossing throughthis point. With the pick-a-point function, each endo-scopic finding could be interactively correlated with allthe other images.
Endoscopic perspectives were represented by meansof bi-dimensional images with 5123 512 pixels on a16-bit gray level. The perspectives simulated the conicview of fyberoptic endoscopy, and the virtual FOV couldbe ranged from 15° to 60°, allowing the representation, atdifferent angles, of a focused region of interest. In each
60 Magnetic Resonance Imaging● Volume 17, Number 1, 1999

perspective, the software allowed for the measurement ofdistances, angles and areas.
An additional tool of VE was represented by thenavigation sequence. With this tool, it was possible tosimulate a virtual navigation through the bile ducts byselecting a path and creating consecutive endoluminalviews along this path. Navigation paths were manuallytraced on the basis of source coronal images and MPR onthe sagittal and axial planes. The computer performed thesimulation storing on the local hard disk, step by step, theperspectives created at an interval of 1 mm along thepath, and showing all frames in a sequence effect usingthe cine-loop tool.
Image AnalysisTwo radiologists (D.C. and G.B.) experienced in im-
age-processing techniques, and informed about diagnosisand site of obstruction, evaluated in consensus MRVEviews and navigation sequences. They aimed to describethe internal anatomy of the bile ducts and the endolumi-nal patterns of the pathological findings. In case of dis-agreement on the interpretation and description of en-doluminal findings, a third radiologist (P.B.) wasinvolved, and decision was based on a major opinioncriteria. The time for the evaluation of each case was notlimited.
The investigators used all the software tools previ-ously mentioned; they could change the direction of theviews, the angle of the FOV, the threshold level; theycould also measure distances, angles, and areas.
RESULTS
The length of time for the generation of a singleMRVE was approximately 5 min, including: transmis-sion of images over the network (2 min, depending onthe network traffic), images loading into the randomaccess memory and creation of the volumetric data set(20–30 s for 40 images), segmentation (with the thresh-olding technique it was extremely fast, ranging between1 and 2 min), and selection of the best endoscopic viewfor the visualisation of the desired finding (30–60 s).
By contrast, the length of time requested to generatenavigation sequences was significantly higher, includingthe time for the single endoscopic view (5 min as above-mentioned), the tracing of the path inside the selectedtract of the bile duct (manually), the creation and regis-tration on the local hard disk consecutive endoluminalviews along the path (performed automatically by thesoftware), and the visualisation of the navigation se-quence with the cine-loop tool. The length of time re-quested for all these steps was 15–20 min.
Navigation sequences were simulated through thecommon bile duct (CBD), hepatic duct (HD), left (LHD)
and right (RHD) hepatic ducts and intrahepatic branches,pancreatic duct (PD) cystic duct (CD) and gallbladder.All these anatomical details appeared as tubular struc-tures with smooth internal surfaces. The confluence be-tween intrahepatic branches, LHD and RHD, PD andCBD, CD and CBD was also visualised. Because of theirlittle calibre, CD and PD were in all cases the mostdifficult structures to represent from the inside. Meantime required to obtain a single navigation sequencethrough the CBD was 10 min, and more than 10 min forthe whole bile ducts because of the tortuosity of theintrahepatic ducts.
However, internal views were obtained only in 27(63%) of the 43 patients with a normal pancreaticobiliarytree. In fact, in 13 patients, the signal intensity and thebile ducts dilation were not enough to get a sufficientnumber of voxels for the segmentation process and in-ternal rendering, while in 3 patients motion artifactsduring the acquisition generated poor quality source im-ages. On the contrary, endoscopic views were obtainedin all 77 patients with partial or complete obstruction ofthe pancreaticobiliary tree and subsequent dilation. Inonly one patient were motion artifacts present, but theydid not influence the source data-set rendering.
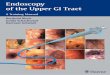
Among the 77 patients with pathology, three mainendoluminal (Fig. 1) patterns were described as follows:36 (47%) endoluminal masses (“polyp-like” masses)(Fig. 2,3), 17 (22%) luminal stenoses (Fig. 4), 24 (31%)luminal occlusion (Fig. 5). The association between thepattern observed and the corresponding pathology isshown in Table 1. The polyp-like pattern was definedaccording to the morphology of the endoluminal mass,that appeared as a well-circumscribed and elevated mass,
Fig. 1. Plot of the MRVE findings: (A) endoluminal masses(single, multiple and grouped); (B) luminal stenosis; (C) lumi-nal occlusion; (D) holes through the internal wall.
MRVE of the pancreaticobiliary tract● E. NERI ET AL. 61

with a large area of attachment to the internal wall, single(Fig. 3), multiple grouped (Fig. 2) or multiple separated.
According to our data, biliary stones were depictedmainly as polyp-like endoluminal masses (85% of cases).Thus, it is supposed that the polyp-like pattern is theirmost probable appearance inside the lumen, but in a fewcases, when the stones determined an important degreeof stenosis of the lumen, they were identified as luminalstenosis (10%) and occlusion (5%). In these cases, thepolyp-like morphology of the stone was not recognisedbecause the lumen did not provide sufficient space forthe navigation. A similar situation could be observed inthe unique case of pancreatic duct stone that causedluminal occlusion. On the contrary, despite the degree ofocclusion, MRCP was more helpful because it clearlyshowed the stone as an hypointense mass on coronalimages.
In the remaining cases, the pathological conditions ofthe bile ducts were interpreted variably as stenoses orocclusions, but a peculiar morphology of the endolumi-nal changes was never detected by the observers. Thismeans that MRVE did not show the cause of the luminalinvolvement, but only provided information about theeffects of this involvement.
In 29 cases “holes” through the internal wall wereobserved and interpreted as mistakes of segmentation,
due to the contiguity between hepatic duct or CBD andthe gallbladder (n 5 13) (Fig. 4), between CBD andduodenum (n 5 11), between CBD and pancreatic duct(n 5 5) (Fig. 3). In fact, when some structures areattached and there is not cleavage among these, thesegmentation become difficult and less accurate. In thiscase, the contiguous structures appear as part of the sameobject because are connected by some voxels.
DISCUSSION
Among the different applications of VE, the bronchialairways and the colon are anatomical structures that havebeen better investigated. In these cases, the segmentationwas facilitated by the natural contrast existing betweenairways and bronchial tree walls, respectively, or inflatedair inside the colon and colon walls. Consequently, thesestructures have been investigated to demonstrate the fea-sibility and usefulness of virtual endoscopy. The recentexperiences of Hara et al. and Dachman et al. haveshown that 3D computer tomography colography is aninteresting tool for the detection of polyps of the colon,while Ferretti et al., reported an equal sensitivity (95%)of virtual and fyberoptic bronchoscopy in the detectionof tracheobronchial stenoses.14,16,17
The use of MR data sets for virtual endoscopy was
Fig. 2. The coronal image (A), obtained with non-breathhold, fat-suppressed, two-dimensional, heavily T2-weighted fast spin-echosequence, shows the CBD, RHD and LHD. The presence of multiple and grouped stones inside the distal part of the CBD can beeasily recognized because of their hypointense pattern respect to the bile ducts signal intensity. Rendering from the inside this dataset, the MRVE view (B) can be simulated in the cephalocaudal direction looking toward the ampulla. Multiple and grouped polyp-likemasses (arrowheads) can be observed in the posterior-superior-left (PSL)–inferior-anterior-left (IAL) side of the internal wall.
62 Magnetic Resonance Imaging● Volume 17, Number 1, 1999

reported by Davis et al. in the study of the aorta and itsbranches with MR angiography.18 Due to the high signalintensity of the blood, generated with this acquisitiontechnique, the voxels representing the aorta corre-sponded to the brightest gray level. In this approach the
voxels of the vascular structures could be easily seg-mented to be used for VE. Because MRCP images havecomparable characteristics respect to the images pro-vided by MR angiography, segmentation and generationof endoscopic views is potentially feasible.
Fig. 3. The coronal view (A) shows the presence of a filling defect inside the CBD (arrowhead), corresponding to a single stone. Inthe MIP reconstruction (B) of the entire biliary tract is shown the cephalocaudal direction of the virtual endoscope called ENDO,corresponding to the endoscopic perspective looking toward the ampulla (C). In this perspective, the single stone appears attachedto the posterior wall of the CBD (length 9 mm). At the posterior-inferior-left (PIL)–anterior-superior-left (ASL) side of the CBD wall,a parietal hole (length 22.3 mm) is caused by the contiguity between the CBD and PD. The presence of an hole (D) can be observedin case of contiguity between the HD and the gallbladder (G) as well.
MRVE of the pancreaticobiliary tract● E. NERI ET AL. 63

Fig. 4. The coronal view (A) demonstrates the dilatation of CBD and PD, due to the narrowing of the ampulla (arrowhead). TheMRVE view (B), looking toward the ampulla, shows the luminal stenosis pattern of the CBD. Two sites of residual lumen are evident(arrowheads). ERCP (C) confirms the presence of ampullary stenosis.
64 Magnetic Resonance Imaging● Volume 17, Number 1, 1999

Fig. 5. In the coronal view (A) is evident the complete occlusion of the HD caused by a unique large stone, that determines a severedilation of the RHD, LHD and intrahepatic ducts, well evident both in the MIP (B) and SSD (C) reconstructions. The MRVE view(D) is simulated to look in the direction of the confluence of the LHD and RHD. If the endoscope is turned around in the oppositedirection the luminal occlusion pattern (E) is demonstrated for the absence of residual lumen.
MRVE of the pancreaticobiliary tract● E. NERI ET AL. 65

Segmentation of MRCP data sets has been madefeasible by the high contrast difference between the bileducts (brightest voxels) and the surrounding tissue (dark-est voxels). Therefore, thanks to the segmentation facil-ities MRVE has clearly shown internal views of thebiliary tract, although in some cases, represented bynormal patients with no bile ducts dilatation, the signalintensity was not enough to provide the necessary num-ber of voxels for segmentation.
In the evaluation of endoscopic views, we took intoaccount the possible presence of holes through the inter-nal walls, caused by the incorrect segmentation.23 Thesefindings were considered as artifacts and could be recog-nised with the “pick-a-point” function. For instance, inthe case shown in Fig. 4, by pointing to an hole locatedon the wall of the HD, the coronal reconstruction cross-ing through the indicated point, corresponded to thegallbladder. The use of the pick-a-point function wasextremely important to avoid the misinterpretation ofholes. This function allowed to correct the segmentationthreshold in order to reduce the occurrance of theseartefacts. However, holes are a typical pitfall of thebinary segmentation performed with surface rendering.We expect to avoid their occurrance with volume-ren-dering techiques, in which the use of transparency effects
should allow the user to promptly recognize the structurein contiguity of the biliary tract.
A possible source of further artifacts in endoluminalviews could be the presence of noise in the MRCP dataset (specifically Fig. 1 represents one peculiar case).However, in our series the noise did not create endolu-minal artifacts. The reason for that might be explained bythe properties of surface rendering technique. Surface-rendered MRVE is based on the marching cube algo-rithm that allows to generate a smooth surface of theinternal wall of the biliary tract even if the surface isirregular and coarse.24 Therefore, this algorithm allowedto reduce the surface irregularities caused by the noise.
The first evaluation performed was the anatomicalcorrespondence between MRCP images and MRVE per-spectives, even if, in our opinion, a further comparisonshould be performed between fyberoptic cholangioscopyand MRVE. With the abovementioned pick-a-point func-tion, each perspective could be compared with MRCPsource coronal images, axial, sagittal and MIP recon-structions. Therefore, according to our evaluation, theanatomy of the biliary tract was demonstrated from theinside by MRVE. Although the knowledge of the internalanatomy is of less importance in normal patients, it couldassume a significative role in the evaluation of pre- andpost-surgical patients (before and after bilio-enteric anas-tomosis), or in the assessment of anatomical variants.The knowledge of the length of the CBD and HD can behelpful in planning of the surgical anastomosis, as wellas the site of confluence of the hepatic ducts, the PD andCD into the CBD.
In conclusion, our study has opened several issues tobe investigated more in depth. Will MRVE improve thediagnostic accuracy of MRCP? And if yes, will be help-ful in all pathological conditions, or there will be arestricted group of applications? Of course, further stud-ies are needed to answer these questions.
REFERENCES
1. Nakamura, K.; Takasaki, T.; Toki, F.; Kozu, T.; Hamano,K.; Takada, T.; Hanyu, T.; Takemoto, T. The research oftransduodenal pancreaticoscopy. Rev Gastroenterol. Mex.40:216–7; 1975.
2. Yamakawa, T.; Mieno, K.; Noguchi, T.; Shikata, J. Animproved choledochofiberscope and non-surgical removalof retained biliary calculi under direct visual control. Gas-trointest. Endosc. 22:160–164; 1976.
3. Picus, D. Percutaneous biliary endoscopy. J. Vasc. Interv.Radiol. 6:303–310; 1995.
4. Rossi, P.; Bezzi, M.; Fiocca, F.; Salvatori, F.M.; Grasso,E.; Speranza, V. Percutaneous cholangioscopy. Semin. In-terv. Radiol. 13:185–193; 1996.
5. Panasen, P.; Partanen, K.; Pikkarainen, P.; Alhava, E.;Pirinen, A.; Janatuinen, E. Ultrasonography, CT, and
Table 1. MRVE patterns observed in the differentpathologies
Endoluminalmass
(n 5 36)
Luminalstenosis
(n 5 17)
Luminalocclusion(n 5 24)
Biliary stone(n 5 40) 34 (85%) 4 (10%) 2 (5%)
Inflammatoryampullary stenosis(n 5 12) (6 (50%) 6 (50%)
Cholangiocarcinoma(n 5 7) 1 (14%) 1 (14%) 5 (72%)
Pancreatic tumor(n 5 8) 1 (12%) 7 (88%)
Stenosis of surgicalbilio-entericanastomosis(n 5 4) 3 (75%) 1 (25%)
Extrinsic localizedCBD stenosis(n 5 2) 2 (100%)
Ampullarycarcinoma(n 5 2) 2 (100%)
Pancreatic duct stone(n 5 1) 1 (100%)
Tumor of thegallbladder(n 5 1) 1 (100%)
66 Magnetic Resonance Imaging● Volume 17, Number 1, 1999

ERCP in the diagnosis of choledochal stones. Acta Radiol.33:53–56; 1992.
6. Guibaud, L.; Bret, P.M.; Reinhold, C.; Atri, M.; Barkum,A.N. Bile duct obstruction and choledocholithiasis: diag-nosis with MR cholangiography. Radiology 197:109–15;1995.
7. Reinhold, C.; Bret, P.M. Current status of MR cholangio-pancreatography. AJR 166:1285–1295; 1996.
8. Boraschi, P.; Braccini, G.; Geloni, M.; Gigoni, R.; Cartei,S.; Perri, G. MR cholangiopancreatography: two dimen-sional fast spin echo imaging versus 3D MIP reconstruc-tions. Radiology 201(P):501; 1996.
9. Fleischmann, D.; Ringl, H.; Schofl, R.; Potzi, R.; Kontrus,M.; Henk, C.; Bankier, A.A.; Kettenbach, J.; Mostbeck,G.H. Three-dimensional spiral CT cholangiography in pa-tients with suspected obstructive biliary disease: compari-son with endoscopic retrograde cholangiography. Radiol-ogy 198:861–8; 1996.
10. Zeman, R.K.; Berman, P.M.; Silverman, P.M.; Cooper C.;Garra B.S.; Patt R.H.; Ascher S.M. Biliary tract: three-dimensional helical CT without cholangiographic contrastmaterial. Radiology 196:865–7; 1995.
11. Lacrosse, M.; Trigaux, J.P.; Van Beers, B.E.; Weynants, P.3D spiral CT of the tracheobronchial tree. J. Comput.Assist. Tomogr. 19:341–347; 1995.
12. Vining, D.J.; Liu, K.; Choplin, R.H.; Haponik, E.F. Virtualbronchoscopy: relationships of virtual reality endobron-chial simulations to actual bronchoscopic findings. Chest109:549–553; 1996.
13. De Nicola, M.; Salvolini, L.; Salvolini, U. Virtual endos-copy of nasal cavity and paranasal sinuses. Eur. J. Radiol.24:175–180; 1997.
14. Ferretti, G.R.; Knoplioch, J.; Bricault, I.; Brambilla, Ch.;Coulomb, M. Central airway stenoses: preliminary resultsof spiral-CT generated virtual bronchoscopy simulations in29 patients. Eur. Radiol. 7:854–859; 1997.
15. Rubin, G.D.; Beaulieu, C.F.; Argiro, V.; Ringl, H.; Norbash,A.M.; Feller, J.F.; Dake, M.D.; Jeffrey, R.B.; Napel, S. Per-
spective volume rendering of CT and MR images: applica-tions for endoscopic imaging. Radiology 199:321–330; 1996.
16. Hara, A.K.; Johnson, C.D.; Reed, J.E. Colorectal lesions:evaluation with CT colography. Radiographics 17:1157–1167; 1997.
17. Dachman, A.H.; Lieberman, J.; Osnis, R.B.; Chen, S.-Y.J.;Hoffmann, K.R.; Chen, C.-T. Small simulated polips in pigcolon: sensitivity of CT virtual colography. Radiology203:427–430; 1997.
18. Davis, C.P.; Ladd, M.E.; Romanowski, B.J.; Wilder-muth, S.; Knoplioch, J.F.; Debatin, J.F. Human aorta:preliminary results with virtual endoscopy based onthree-dimensional MR imaging data sets. Radiology199:37– 40; 1996.
19. Kimura, F.; Shen, Y.; Date, S.; Mochizuki, T. Thoracicaortic aneurysm and aortic dissection: new endoscopicmode for three-dimensional CT display of the aorta. Radi-ology 198:573–578; 1996.
20. Igel, B.J.; Durham, N.C.; McDermott, V.G.; Nelson, R.C.Abdominal aortic aneurysms from the inside out: applica-tions and limitations of virtual angioscopy. Radiology201(P):467; 1996.
21. Marro, B.; Galanaud, D.; Valery, C.A.; Zouaoui, A;Biondi, A.; Casasco, A.; Sahel, M.; Marsault, C. Intracra-nial aneurysm: inner view and neck identification with CTangiography virtual endoscopy. J. Comput. Assist. To-mogr. 21:587–589; 1997.
22. Merkle, E.M.; Fleiter, T.; Wunderlich, A. Virtual cystos-copy based on helical CT scan data: possibilities andlimitations. Eur. Radiol. 7:S229; 1997.
23. Neri, E.; Caramella, D.; Falaschi, F.; Sbragia, P.; Vignali,C.; Bartolozzi, C. Virtual endoscopy of the aorta: Segmen-tation artifacts with perspective surface rendering of spiralCT data sets. Radiology 205(P):262; 1997.
24. Lorensen, W.E.; Cline, H. Marching cubes: a high resolu-tion 3D surface construction algorithm. Comput. Graphics21:163–169; 1987.
MRVE of the pancreaticobiliary tract● E. NERI ET AL. 67













![arXiv:2101.04240v2 [cs.CV] 15 Jan 2021Wireless Capsule Endoscopy allows non-invasive visualization of the entire gastrointestinal tract including the small-bowel region by the gastroenterologist](https://img.dokumen.tips/doc/110x75/613bf1fef8f21c0c82694954/arxiv210104240v2-cscv-15-jan-2021-wireless-capsule-endoscopy-allows-non-invasive.jpg)