-
8/14/2019 Mountain and Cold Medical Considerations
1/18
ColdWeatherMedicalConsiderations
FlightERDoc2010
Contents:
IntroductionTheMountainEnvironment
Section1Hypothermia
Section2
Frostbite
Section3AcuteMountainSickness
Section4HighAltitudeCerebralEdema
Section5HighAltitudePulmonaryEdema
Section6SolarKeratitis(SnowBlindness)
Section7ConsiderationsforFirstAidSupplies
Bibliography
-
8/14/2019 Mountain and Cold Medical Considerations
2/18
IntroductionTheMountainEnvironment
At10,000feetelevation(abovesealevel),thestandardairpressureis10.1psi.
Thisis40%lessthanthe
airpressure atsea levelof14.7psi. Becauseof this,
theamountofoxygenavailable toyourbody is
much less. At sea level, a normal amount of oxygen in oxygenated
(arterial) blood is 97% of the
maximumcarrying
capacity,
at
10,000
feet
it
is
only
90%.
You
have
less
oxygen
to
work
with,
so
it
is
importanttouseitwell,throughcardiovascularconditioning.
Bytheway,apackadaycigarettesmoker
is already cruising at 10,000 feet, when they are at sea level,
based on their bloods oxygen carrying
capacitysosmokingisnothealthyforyouinthemountains,either.
Because of less air above you and the highly reflective snow
around you, the effects of sunlight are
muchhigherwhichcan leadtosunburn.
Thereflectionsfromthesnowonthegroundoften leadto
sunburnonnormallyprotectedareas(thelowerportionofthenoseandtheentranceofthenostrilsare
oftensunburnedinthesesituations).
Sunburncanoccurevenindarkskinnedpeople,andcanbecome
severeenoughto leadtoblistering (seconddegreeburns) inboth
lightanddarkskinnedpeople. Lips
can become sun and windburned, and this injury can lead to
reduced desire to eat or drink
compounding
other
problems.
Mountaintemperaturesataltitudearealso lowerespecially
inthewinter. Lowtemperaturesaffect
the body in different ways. It can both hurt you (via cold
injuries like frostbite or hypothermia) and
make life difficult for your body. Since cold air is usually dry
air, you will lose more bodily fluids
breathing than at normal elevations and humidity levels but
because of the low temperatures,you
maynotfeelthirsty,andyoucanendupdehydrated.
Waterisheavy,andcarryingenoughofittodrink
canbedifficult. Meltingsnow forwatertodrinkorcookwith
istimeconsuming,andyoumustcarry
fuelabovetreelinetouseformelting. Thiscanaddtothedehydration.
Becausethevariousmetabolic
processesinthebody(onthecellularlevel)arequitesensitivetothetemperatureandpHlevels,these
changescanaffecttheabilityofthebodytodigestfood,whichcanresultinloweredenergyavailability
justwhenyouneedextraenergythemost.
Overall,themountainenvironmentischallenging.
Adaptation
Thehumanbodyhasaremarkableabilitytoadapttovariousenvironmentalconditionswhich
iswhy
peopleliveinthehigharcticareaswherewintertemperaturescanbebelow
40oF,andinSaharanAfrica
where the temperatures can reach over 120oF, or from high
humidity locations (jungles) to very low
(deserts), or high elevations (mountains) or low. Some
adaptations happen quite rapidly, some take
longer. Someofthenormaladaptationsthathappeninclude:
Hyperventilation(deeper,fasterbreathingbecausethereislessoxygenavailableperbreathso
youneedmorebreath.
Shortnessofbreathonexertionwhichcan
includejuststandingorsittingaround,sinceyour
body is working harder at altitudejust keeping you alive. Breath
patterns during sleep can be quite
different,includingCheyneStokesrespiration(breathing)whichiscyclesofincreasinglydeepbreaths
followed by a short period of no breathing at all (called
apnea)this is very noticeable in your tent
partnersandtheperiodsofapneacanbeenoughtowakeyouupfromsleep.
Whiledistressing,thisis
normal, and aside frompreventinga good nights sleep
isnotespeciallydangerous in theabsenceof
other medical problems. This is not AMS acute mountain sickness.
CheyneStokes respirations
happenbecausedeeperbreathschangestheacidityofyourblood(makes
itmorealkalinesinceyoure
-
8/14/2019 Mountain and Cold Medical Considerations
3/18
blowing off carbon dioxide in the form of carbonic acid) and the
part of your brain that controls
breathingsayswaitasecond,letslettheacidbuildupagain.
Awakeningfrequentlyatnightthisisannoying,butnotserious,andiscausedbydisruptionsin
breathing,CheyneStokesrespirations,beingcoldoruncomfortable,orneedingtourinate.
Finally,increased
urination,
especially
at
night.
Your
kidneys
are
responsible
for
keeping
your
bloodspHbalance inaverynarrowrange,andoneway itdoesthis
isbyexcretingbicarbonate ions
which needs to be flushed from the body. This is only dangerous
if you become dehydrated, so its
important to drink lots of water. Having a pee bottle at night
makes this frequent urination less
onerous.
Nothavingtourinate,especiallyatnight,maybeasignthatyouaredehydrated,whichcanbe
dangerous.
Likelihood
Somepeoplearemorelikelytohavevariousformsofaltitudeorcoldinjuriesthanothersare.
Genetic
background,pastincidentsofcoldinjuries,chronicdiseases,andphysicalconditionareallvariablesthat
can affect individual performance. However, some people, even
those in very good cardiovascular
conditioncan
have
difficulties
in
the
cold/high
altitude
environments,
and
people
who
have
done
well
previously can have difficulties apparently without an obvious
reason. Only time will tell. One good
marker forexpectingdifficulties from cold injuries
isapreviouscold injury: Ifyouhave had frostbite
beforeyouaremuchmore likelythanothers inthesameconditionstohave
itagain. Likewise, ifyou
havehadaltituderelatedproblems,youaremorelikelytohaveitagain.
Knowyourlimitations.
Risksofchronicconditionsinthemountainenvironment
MinimalriskSomedocumentedrisk considermedical
monitoring,availabilityofoxygen
Substantialrisk
ascentnotadvised
Childrenandelderly Carotidsurgeryorirradiation COPD,severe
Physically
fit
and
unfit
Sleep
disordered
breathing
and
apnea
Coronaryarterydisease,withpoorly
controlledangina
Obesity COPD,moderate CHF,uncompensated
Chronicobstructivepulmonarydisease(COPD),
mildCysticfibrosis
CongenitalheartdiseaseASD,PDA,
Downssyndrome
Asthma Hypertension,poorlycontrolled Pulmonaryhypertension
Hypertension,controlled Coronaryarterydisease,withstableangina
Pulmonaryvascularabnormalities
Coronaryarterybypassgrafting,angioplasty,or
stenting(withoutangina)Arrhythmias,highgrade
Sicklecellanemia(withhistoryof
crises)
Anemia,stable Congestiveheartfailure(CHF),compensated Pr
egnancy,highrisk
Migraine Sicklecelltrait
Seizuredisorder,onmedication Cerebrovasculardisorders
Diabetes
mellitus
Seizure
disorder,
not
on
medicationLASIK,PRK Radialkeratotomy
Oralcontraceptives Diabeticretinopathy
Pregnancy,lowrisk
Psychiatricdisorders
Neoplasticdiseases
Inflammatoryconditions
Fromtable385,TravelMedicine1stEd.
-
8/14/2019 Mountain and Cold Medical Considerations
4/18
Prevention
Mostmedicalproblemsduetothemountainenvironmentarepreventable.
Be
aware
of
your
own
condition,
and
the
condition
of
your
partners.
The
onset
of
most
problems
is
insidiousandthevictimmaynotbeawareofthembothvisibleproblems
likefrostbiteandproblems
thatmayresultinbehavioralchanges,forinstanceduetolessoxygenintheair.
Havingthecorrectequipment(clothing,shelter,water,sunglasses,etc)iscriticaltopreventinginjuries
butyouhavetocarryallthatgear!
Takewhatyouneed,buttrynottooverdoit.
Structure
Definitionsarenormallyexplainedwhenatechnicalormedicalterm
isfirstused. Generally,however,
thedistinctionbetweenasignandasymptom is important:
(symptomsarewhatthepatientreports,
signs are what the physician can see, touch, or measure). In
other words, you complain about
symptoms,thedoctorseessigns.
Eachsectionissetupwitha
Definitionof the condition; the keys todifferentiating
conditionswithsimilar signs/symptoms
betweenseriousandnonseriousconditions
Identifyingthecondition(signsandsymptoms,and
ifnecessaryhowtotellaseriouscondition
fromalessseriousonewithsimilarsignsandsymptoms
Treatmentbothimmediateandintermediate
Prognosis,orhowthevictimcanbeexpectedtofarewiththecondition,andmostimportantly
Prevention.
Preventioniseasyforalloftheseconditions,andismuchpreferredovertreatment.
-
8/14/2019 Mountain and Cold Medical Considerations
5/18
Section1:Hypothermia
Definition
Hypothermia is the loweringof thebodiescore temperature, which
isnormallyaround37oC (98.6oF),
below the normal range (that is, to a temperature below 35oC or
95oF). While hypothermia is often
deliberatelyinduced
(for
certain
kinds
of
surgery,
for
example)
we
are
only
concerned
with
accidental
hypothermia.
Accidental hypothermia can occur slowly and insidiously because
of inadequate clothing in cold
temperatures,orsuddenlyandcatastrophically,fromfallingthroughafrozen
lakesurface. Eitherway,
loweringthebodiestemperatureisdangerous.
Thevariouschemicalprocessesthatoccurinyourbody
areverysensitivetoslightchangesinconditions,includingtemperature,andloweringtheirtemperature
canstopthemfromhappening.
IdentificationSigns,symptoms
Theclassicsignofhypothermia isa2oC(ormore)
lowerthannormalbodytemperature. So,thebest
wayto
identify
hypothermia
is
with
athermometer.
Special,
low
range
thermometers
are
available
for
hypothermiause,mostoraldigitalthermometerswillreadlowenoughaswell.
Hypothermiacanbe categorizedby theeffect that lower
temperaturescause,anddifferentiated into
fourdistinctrangesthatcanbeestimatedbytheirsigns:
Stage CoreTemp Characteristics
Mild 99.6 Normalrectaltemperature
98.6 Normaloraltemperature
96.8 Increaseinmetabolicrates,preshiveringmuscletone
95.0 Maximumshivering(togenerateheatfrommusclemovement)
93.2 Developmentofpoorjudgmentandamnesia
91.4
Developmentofataxia(staggeringgate)andapathy,fasterbreathing(tachypnea)
Moderate 89.6 Stupor
87.8
Shiveringstops
(DANGER)
86.0 Atrialfibrillationandotherheartarrhythmiasbegin
85.2 Progressive decrease in level of consciousness, pulse, and
respiration; pupils dilated; paradoxical
undressing(thevictimiscoldbutremovesclothing)
Severe 82.4
Ventricularfibrillationbegins,hypoventilation(breathingnearlystops)
80.6 Lossofreflexesandvoluntarymotion
78.8 Majorbloodacidbasedisturbances,nopainresponseorreflexes
Profound 68.0 Pulse20%ofnormal
64.4 Asystole(heartstops,flatlines)
59.2 Lowestinfantaccidentalhypothermiarecovery
58.6 Lowestadultaccidentalhypothermiarecovery
Treatmentinitial,intermediate
Foramild
to
moderately
hypothermic
person,
the
most
important
step
is
to
first
stop
their
heat
loss.
Get them into warmer surroundings, dry or warm clothes, and/or
get them out of the wind. Even a
slightwindbreakcreatedbydiggingasmalldepressioninsnowisbetterthancontinuingtoexposethe
patienttotheeffectsofwindchill,atent,oramoreformalstructureisbetter.
Formoderately(ormore)hypothermicpatients,expecttheirheartstobeirritabledonthandlethem
roughlywhileattemptingtowarmthembecausetheroughhandlingmaycauseaheartarrhythmia.
-
8/14/2019 Mountain and Cold Medical Considerations
6/18
Forpatients
foundwhoappeartohaveseveretoprofoundhypothermia,considerpostponingCPR.
A
rigid chest wall will prevent chest compressions, and blood pH
changes can themselves cause heart
arrhythmias,especiallywhencoldperipheralbloodmovestothecorebymechanicalcompressions.
Moderately or more hypothermic patients should be transported to
medical care for evaluation.
Warmingcanoccurwithgentlehotwaterbottlesinthegroinandaxilla,
ifthevictim isabletograspa
containeranddrinkfromitonhisown,warmfluids(nonalcoholic)canbetakeninsmallsipsbutmake
certainthefluidsarenttoowarm,sincereflexesandtemperaturesensationmaybemissing.
Ifavictim is foundcold,pulseless,andunresponsive, treat
themasaprofoundlyhypothermicvictim:
Handlegently,packagefortransport(seebelow),andgetthemtodefinitivemedicalcareasrapidlyas
possible. It is impossible to tell in the field if a patient is
suffering from a heart attack, or profound
hypothermia,bothcaneasilymimicconditionsofdeath.
ThereisasayingThepatientisntdead,until
theyrewarmanddead,becauseofthisgivethevictimthechance,ifpossible.
PreparingthehypothermicpatientforTransport
Prognosis
Theprognosis
isdependentonthedegreeofhypothermiathatthevictimsustained.
Itcanvary from
fullrecoverywithnosequelaetobeinginapersistentvegetativestatefromprolongedhypoxia.
Prevention
Staywarmanddry.
Avoidoverheatingandconsequentialperspiration,whichwillresultinrapidcooling
onceyourexertionsstop.
Wearingwickingundergarmentstomovemoistureawayfromyourskinwill
helpkeepyoudry,butyoumustcontrolyourperspirationandventilationtostaydry.
Vasculardilators(bloodpressuremedication)mayincreasetheriskofhypothermia.
Discussusingthem
withyour
physician
prior
to
cold
exposure.
1.
Thepatientmustbedry.Gentlyremoveorcutoffwetclothingandreplaceitwithdryclothingoradry
insulationsystem.Keepthe
patienthorizontal,
and
do
not
allow
exertion
or
massage
of
the
extremities.
2.
Stabilizeinjuries(i.e.,thespine;placefracturesinthecorrectanatomicposition).Openwoundsshouldbecoveredbeforepackaging.
3.
Initiateintravenousinfusions(IVs)iffeasible;bagscanbeplacedunderthepatient'sbuttocksorinacompressorsystem.Administera
fluidchallenge.
4. Active rewarming should be limited to heated inhalation (if
available) and truncal heat. Insulate hot water bottles in
stockings or
mittensandthenplacetheminthepatient'saxillae(armpits)andgroin.
5.
Thepatientshouldbewrapped.Beginbuildingthewrapbyplacingalargeplasticsheetontheavailablesurface(floor,ground),andon
itplaceaninsulatedsleepingpad.Alayerofblankets,asleepingbag,orbubblewrapinsulatingmaterialislaidoverthesleepingpad.The
patientisthenplacedontheinsulation.HeatingbottlesareputinplacealongwithIVs,andtheentirepackageiswrappedlayeroverlayer,
with the plastic as the final closure. The patient's face should
be partially covered, but a tunnel should be created to allow
access for
breathingandmonitoring.
-
8/14/2019 Mountain and Cold Medical Considerations
7/18
Section2:Frostbite
Definition
While hypothermia is a reduction in the bodys core temperatures,
frostbite, frosting, chilblains and
trenchfootarehypothermiarelatedinjuriestoperipheral(extremity)tissues.
IdentificationSigns,symptoms
Frostbiteinjuriesarecategorizedintodegreesofdamage,similarlytoburns.
First andseconddegreefrostbitesaresuperficial
injuriesthatpresentwithedema(swelling),burning,
erythema(redness),andinseconddegree,blistering.
Thirddegreefrostbiteisadeeperinjuryinvolvingthefullthicknessskinandthesubdermaltissue.
The
tissuesappearancewillbeonacontinuumfromtherednessoffirstdegreefrostbitetothepale,hard
tissue of fourth degree. Like burns, various areas of the
affected tissue will have different levels of
frostbite.
Fourthdegree injury includes subcutaneous tissue, muscle,
tendon, and bone. Patients present with
cyanoticandinsensatetissuethatmayhavehemorrhagicblistersandskinnecrosis.
Subsequently,this
tissueappearsmummified.
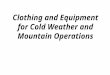
FrostbiteInfeetandtoes
Figa Figb Figc
Fig a and b Before thawing, the clinical appearance of the
frozen part is cold, white, or bloodless. The outer shell of skin
is rigid,and the depth of freezing is difficult to determine. (c)
After rapid thawing, the part is flushed red or pink, or has a
violaceous hue.Blebs appear 1 to 24 hours after the thaw and
rupture spontaneously in 4 to 10 days. The cast-like eschar forms
after the blebs
rupture, and the eschar sheds after 21 to 30 days.
PhotosfromMedicalAspectsofHarshEnvironments,vol1.
FrostbiteOuterEar
-
8/14/2019 Mountain and Cold Medical Considerations
8/18
Figure a Figure b Figure c
Warmingtechniquesandtissueloss.(a)Frostbiteofanearwithouttissuelossafterrapidrewarming.Frostbiteofearin(b)ayoung
manand(c)anelderlypatient;eachhadtissuelossafterspontaneousthawing.
PhotosfromMedicalAspectsofHarshEnvironments,vol1.FrostbiteInHandsandFingers
Figurea Figureb Figurec Figured
Figuree Figuref
Rapidrewarminginawaterbathat42C(108F). (a)Firstday.
ThepatientsustainedfreezingofhandsandfeetontheArcticSlope
whenmaroonedintheopenasaresultofavehicleaccident.
Windswere80knots,ambienttemperaturebetween20Cand26C.
Thepatientlosthisoverbootsandglovesintheaccident.Hisentireexposuretime,hestates,was15to20minutes,followedby45
minutesinthewreckedvehicleawaitingrescue.
Onrescue,hewaswarmedinwaterat42C(160F);thewarmingandcarewere
directedbyradiofromAnchorage,Alaska.
ThepatientwasthentransferredfromtheArcticOceanshoretoAnchoragebyairtravel
at24hours.
Onarrival,thehandsdemonstratedlarge,clear,pinkblebsextendingtofingertips;theseareexcellentprognosticsigns,
especiallythat
the
blebs
are
distal
and
extend
to
the
nailbeds.
NOTE:
Only
after
rapid
rewarming
in
warm
water
is
there
return
of
sensation inthe fingertips;thisremainsuntilblebsappear
inthedermisandepidermisandseparate those tissues from thedeep
structures. (b) Fourth day. Constant, twicedaily whirlpool is
prescribed with digital exercises, using surgical soaps such as
pHisoHex,*Hibiclens,orBetadine.(c)Twentyfirstday.Bythethirdweek,epidermalescharhasformed,preventingjointmotion.
(d) Fourth week. Periodically, when the tissue permits, the
eschar is incised to allow joint motion. Escharotomy usually is
performedfromthe14thtothe31stday.(e)Fifthweek.Digitalexercisesaredoneatfrequentintervalsatleastfourtimesdaily,as
withwhirlpoolandbiofeedback training.By this time, lossofvolar
fatpadand lossofnailshaveoccurred andhypesthesia is
resolving.(f)Seventhweek.Theanatomicalresultisgood,butvolarfatpadlossandintrinsicmusclelossareobvious.Thepatient
has considerable atrophy of the first dorsal interosseus, and of
the abductordigiti quinti. PhotosfromMedicalAspects
ofHarshEnvironments,vol1.
-
8/14/2019 Mountain and Cold Medical Considerations
9/18
Treatmentinitial,intermediate
Rapidlyrewarmfrostbiteoveraperiodof20minutesinwaterrangingfrom40to42C(104107oF).
Be
carefulthewaterisnottoohotnormaltaphotwateristoohot,itcancauseseriousdamagethatthe
victimmaynotbeabletosenseduetothelossofsensationfromthefrostbite.
Donotmassageorrubthefrozenpartitmightincreasetissuedamage.
Rewarmingwillbepainful;use
ananalgesicaneeded.
Ibuprofen(Motrin)ispreferredinthisapplicationsinceitsprostaglandineand
thromboxaneinhibitingroleassists
inpreventingfurthertissuedamagebypreventingvasoconstriction
andplateletaggregation.
Prognosis
Prognosis of frostbite injury depends on the degree and location
of the injury, but can be severe,
especiallyifnottreatedcorrectly,oriftheaffectedpartisallowedtorefreeze.
Ifthereisanydoubtthat
the affected part can be kept from refreezing, consider delaying
the initial thawing until there is
assurancethatthepartwillremainwarm.
Administration (by a medical professional in the appropriate
setting) of tissue plasminogen activator
(tPa) given intravenously within 24 hours of injury and within 6
hours of rewarming significantly
decreasedtheextentofamputationinseverefrostbite.
Prevention
Frostbite isusuallypreventablebyproperclothing
includingfaceshieldsormasks. Observepartners
or use a mirror to check your own nose and ears for frostbite if
necessary. In extreme conditions,
consider spare gloves, hats, scarves, etc, in case you lose
yours or they become wet. In particular,
keepingglovesandsocksdrycanbeproblematic,havingsparestochangeintocanbeimportant.
Use
of
ergot
alkaloid
drugs
(sometimes
used
for
migraine
treatment)
can
increase
the
chances
of
developingfrostbitediscussusingorstoppingthedrugswithyourphysicianpriortotravellingtocold
locations.
Nonfreezingcoldinducedinjuries
Chilblains Chilblains (pernio) presents with painful and
inflamed skin lesions caused by chronic,
intermittentexposuretodamp,nonfreezingambienttemperatures.
Frostnip
isalesssevereformoffrostbitethatresolveswithrewarmingandinvolvesnotissueloss.
Trenchfoot
Trenchfootresultsfromcoolingoftissueinawetenvironmentatabovefreezing
temperaturesoverseveralhourstodays.
Longtermhyperhidrosis(increasedperspiration)andcold
insensitivityarecommonresults.
Preventionisbykeepingfeetdrybychangingsocksasneeded.
Onceaffectedbychilblains,frostnip,orfrostbite,theinvolvedbodypartbecomesmoresusceptibleto
reinjury.
-
8/14/2019 Mountain and Cold Medical Considerations
10/18
Section3:AcuteMountainSickness
Definition
AMS is a constellation of symptoms that represents your body not
being acclimated to the current
altitude.
Asyouascend(bywalking,driving,flying,oranyothermethod)yourbodyattemptstoadjust
tothe
hypoxia
(reduced
oxygen
available
at
that
altitude).
Atanygivenaltitude,there
isasweetspotthatyourbodytriestoachievebetweenbreathing,blood
pressure,metabolism,etc.
AMSoccurswhenyourbodyisnotinthatsweetspot.
TheactualcauseofAMSisnotunderstood,itisthoughtthatslightbrainswellingcausedbyachangein
bloodpHmaybeinvolved.
IdentificationSigns,symptoms
AsdefinedbytheLakeLouiseConsensusontheDefinitionsofAltitudeSickness,AMSisagroupingof
symptoms
thatinthesettingofrecentaltitudegain,anyoneormoreofthefollowingsymptomsconstitutes
AMS:
In
the
setting
of
arecent
gain
in
altitude,
the
presence
of
headache
and
at
least
one
of
thefollowingsymptoms
Gastrointestinaldistress(anorexia(lossofappetite),nauseaorvomiting);
Fatigueorweakness;
Dizzinessorlightheadedness,ataxia(unsteadygait);
Difficultysleeping; constitutesAMS.
Clearly,thesecommonsymptomsmayresultfromanynumberofunrelatedconditions.
More
specifically,AMScanbeconsideredasevereheadache(oftenintheareaabovetheeyes)thatisnot
causedbydehydration(seebelow),andsevereindicationsoftheseothercriteria.
DifferentiatingAMSandsevereheadache.
Severeheadachescanbecommon
inthemountainenvironment,duetocold,dehydration,andstress
but this is not the same as AMS. While it is impossible to
totally differentiate between these two
causes, if a person complains of a headache first have them
drink a liter of fluid, and take a mild
analgesic (ibuprofen (Motrin),acetaminophen
(Tylenol),aspirin)andhave them restabit: Iftheir
headache resolves completely in a short time (3060 minutes) it
is probably not AMS related. AMS
symptomsdontresolvewiththesetreatments,noraretheymadeworsebythem.
Treatmentinitial,intermediate
Ifsymptoms
are
caused
by
AMS,
descending
is
the
best
treatment.
A
descent
of
only
1000
2000
feet
may be sufficient to resolve the symptoms. Because of the
unsteady gait, the victim must have
assistanceduringthedescentusuallyatleasttwopersonstohelpsteadythem.
A prescription drug, acetazolamide (Diamox) can be given orally
(250mg, bid) if available, and the
individualisnotallergictosulfatypedrugs.
AcetazolamidedoesnotpreventallsymptomsofAMS,does
notmaskthesymptomsofAMS,andisnotareplacementforslow,steadyacclimatization.
SupplementaloxygentherapyisusuallynotindicatedforAMS,descentisafarbettertreatment.
-
8/14/2019 Mountain and Cold Medical Considerations
11/18
Hyperbaricchambertherapy(Gamowbagorsimilar)isnotindicatedforAMStherapyatintermediate
altitudes.
Recently, some interest in gingko biloba as a cure or
preventative for AMS has been discussed.
Extensivedoubleblindinvestigationshaveshownthatgingkoisnobetterthanaplaceboinpreventing
AMS,soitsuseisnotrecommended.
Prognosis
TheprognosisfollowingAMSisgenerallygood.
Withrapiddescent,thepatientusuallyrecoverswithout
anysequelae. Itgenerallywontkillyou (although
theheadachecanbesoseverethatat firstyoure
worried it will kill you, then youre worried it wont), but it
can develop into HACE high altitude
cerebraledema(seebelow),whichisquiteserious.
Prevention
Slow, steady acclimatization is the key to avoiding most
altitude related conditions. The typical
individualstravelfromnearsealeveltotrailheadsatsomeconsiderableelevation,justtojumpofftoa
higherelevation
on
foot
is
asure
prescription
for
AMS
and
other
altitude
related
disorders.
Forlongerascentsagoodstrategytofollowforclimbingistoclimbhigheachday,butreturntoalower
altitudetosleepforthenight.
ThisismoreapplicabletoexpeditionclimbssuchasintheHimalayas,but
ifpossible,itworksatloweraltitudes.
-
8/14/2019 Mountain and Cold Medical Considerations
12/18
Section4:HighAltitudeCerebralEdema(HACE)
Definition
HACE can be considered a serious continuation of the
constellation of symptoms of AMS. At the
"severely ill" end of this spectrum is High Altitude Cerebral
Edema; this is when the brain swells and
ceasesto
function
properly.
Since
the
skull
is
rigid
in
adults
any
swelling
compresses
the
brain
tissue,
obstructingbloodflow,andinseriouscasescancausethebrainstemtoherniate(squeezethrough)the
openinginthebottomoftheskullthatthespinalcordpassesthrough,theforamenmagnum.
Persons with this illness are often confused, and may not
recognize that they are ill. They are, and
propertreatmentiscritical.
HACE can progress rapidly, andcan be fatal in a matter of a few
hours to one or two days. It can
rapidlybecomeamedicalemergency,requiringtreatmentorthevictimmaydie.
IdentificationSigns,symptoms
Canbe
considered
"end
stage"
or
severe
AMS.
In
the
setting
of
arecent
gain
in
altitude,
either:
Thepresenceofachangeinmentalstatusand/orataxiainapersonwithAMS
Or,thepresenceofbothmentalstatuschangesandataxiainapersonwithoutAMS
ThehallmarkofHACEisachangeinmentation,ortheabilitytothink.
Theremaybeconfusion,changes
inbehavior,orlethargy.
Thereisalsoacharacteristiclossofcoordinationcalledataxia.
Thisstaggering
walk issimilarto thewayapersonwalkswhenvery
intoxicatedonalcohol. This lossofcoordination
may be subtle, and must be specifically tested for. Have the
sick person do a straightline walk (the
"tandemgaittest").
Drawastraight
line
on
the
ground,
and
have
them
walk
along
the
line,
placing
one
foot
immediately
in
front of the other, so that the heel of the forward foot is
right in front of the toes behind. Try this
yourself. Youshouldbeabletodoitwithoutdifficulty.
Iftheystruggletostayontheline(thehighwire
balancingact),cannotstayonit,falldown,orcannotevenstandupwithoutassistance,theyfailthetest
andshouldbepresumedtohaveHACE.
Treatmentinitial,intermediate
ImmediatedescenttolowerelevationsisthepreferredtreatmentforHACE.
Thisiscriticallyimportant,
it must be done immediately, it cant wait until morning even
though HACE symptoms become
apparent or worse at night. The moment HACE is recognized, begin
evacuating the victim, with
assistance,(atleasttwopeopleassisting),toatleastthelowestelevationthevictimlastfeltwell.
Other treatments, including supplemental oxygen therapy,
hyperbaric chambers (Gamow bags or
similar),etcarelesseffectiveintreatingHACE.
Pharmaceuticaltherapywithsystemiccorticosteroidsmaybeusedaswell.
Dexamethasone(4mg,two
doses 6 hours apart) may be given orally or intramuscularly if
the patient is vomiting. These
supplementaltherapiesshouldnotbeusedincaseswheredescentandevacuationarepossible.
-
8/14/2019 Mountain and Cold Medical Considerations
13/18
Prognosis
TheprognosisfromHACE
isgenerallygood,withfullrecoveryhowevertheataxicgatemaycontinue
for several days following descent to normal elevation. Once
full recovery occurs, the victim may
attemptre
ascent
with
proper
acclimatization.
-
8/14/2019 Mountain and Cold Medical Considerations
14/18
Section5:HighAltitudePulmonaryEdema(HAPE)
Definition
Anotherformofseverealtitude illness
isHighAltitudePulmonaryEdema(HAPE),orfluid inthe lungs.
ThoughitoftenoccurswithAMS,itisnotfelttoberelatedandtheclassicsignsofAMSmaybeabsent.
HAPEmay
also
be
mistaken
for
other
diseases
(see
below).
IdentificationSigns,symptoms
Inthesettingofarecentgaininaltitude,thepresenceofthefollowing:
Symptoms:atleasttwoofthefollowing:
Dyspnea(difficultyinbreathing)atrest;
cough;
weaknessordecreasedexerciseperformance;
chesttightnessorcongestion;
Signs:atleasttwoofthefollowing:
cracklesorwheezinginatleastonelungfield;
centralcyanosis(bluetingetoskinoncentralbodychest,lips,throat,etcabluetingeon
lips,fingers,etcmaybecoldrelated);
tachypnea(rapidbreathing,fasterthan30breathsperminute);
Tachycardia(rapidheartbeat,greaterthan100beatsperminuteinarestingindividual);
Othersignsandsymptomsinclude:
Extremefatigue
Breathlessness
at
rest
Fast,shallowbreathing
Cough,possiblyproductiveoffrothyorpinksputum
Gurglingorrattlingbreaths
Chesttightness,fullness,orcongestion
Blueorgraylipsorfingernails
Drowsiness
HAPEusuallyoccursonthesecondnightafteranascent,andismorefrequentinyoung,fitclimbersor
trekkers.
Insomepersons,thehypoxiaofhighaltitudecausesconstrictionofsomeofthebloodvessels
inthelungs,shuntingallofthebloodthroughalimitednumberofvesselsthatarenotconstricted.
This
dramaticallyelevatesthebloodpressureinthesevesselsandresultsinahighpressureleakoffluidfrom
the
blood
vessels
into
the
lungs.
Exertion
and
cold
exposure
can
also
raise
the
pulmonary
blood
pressureandmaycontributetoeithertheonsetorworseningofHAPE.
HAPEcanbeconfusedwithanumberofotherrespiratoryconditions:
High Altitude Cough and Bronchitis both are characterized by a
persistent cough, with or without
sputum production. There is no shortness of breath at rest, and
no severe fatigue. Normal oxygen
saturations(forthealtitude)areseenifapulseoximeterisavailable.
-
8/14/2019 Mountain and Cold Medical Considerations
15/18
PneumoniacanbedifficulttodistinguishfromHAPE.
FeveriscommonwithHAPEanddoesnotprove
thepatienthaspneumonia.
CoughingupgreenoryellowsputummayoccurwithHAPE,andbothcan
cause lowblood levelsofoxygen. Thediagnostic test(andtreatment)
isdescentHAPEwill improve
rapidly. If thepatientdoesnot
improvewithdescent,thenconsiderantibiotics. HAPE ismuchmore
commonataltitudethanpneumonia,andmoredangerous;manyclimbershavediedofHAPEwhenthey
weretreatedforpneumonia.
AsthmamightalsobeconfusedwithHAPE.
Fortunately,asthmaticsseemtodobetterataltitudethan
atsea level. Ifyouthink itsasthma,tryasthmamedications,but
ifthepersondoesnot improvefairly
quicklyassumeitisHAPEandtreatitaccordingly.
Treatmentinitial,intermediate
Minimizeexertionandkeepwarm. LikeHACE,rapiddescent
isthebesttreatment. Othertreatments
include:
Oxygen,4to6L/minuntilimproving,then2to4L/min
Ifoxygenisnotavailable:
Nifedipine,10mgPOq4hbytitrationtoresponse,or10mgPOonce,followedby30mgextended
releaseq12to24h
Inhaledbetaagonist (albuterol,Ventolin)
Considersildenafil(Viagra)50mgevery8hrs
HyperbarictherapyviaGamowbagorsimilar
Prognosis
ItiscommonforpersonswithsevereHAPEtoalsodevelopHACE,presumablyduetotheextremelylow
levels of oxygen in their blood (equivalent to a continued rapid
ascent). HAPE resolves rapidly with
descent,andoneortwodaysofrestatalowerelevationmaybeadequateforcompleterecovery.
Once
thesymptomshavefullyresolved,cautiousreascentisacceptable.
Prevention
Whilecarefulascentwithacclimatizationispreferred,somepeoplearepredisposedtoaltitudeillnesses
evenwithgoodphysicalconditioningandcarefulacclimatization.
-
8/14/2019 Mountain and Cold Medical Considerations
16/18
Section6: UV/SolarKeratitis(SnowBlindness)
Definition
Becauseof lessatmosphereaboveyou filtering light,and thehighly
reflectivesnowfieldsaroundyou,
theeyecanreceive1015timesasmuchlight,especiallyultravioletlight,asishealthy.
Thisextralight
canresultintemporarydamagetotheouterlayeroftheeye.
IdentificationSigns,symptoms
Intensepainandafeelingofgritorsandintheeyes,feltwhenblinking.
Theeyesarepainfulandthe
victimmayhaveanearlyuncontrollableurgetorubthem.
Treatmentinitial,intermediate
Treatment consists of antibiotic ointment (if available, and
only optic formulations), mild analgesics
(NSAIDSlike
ibuprofen)
and
perhaps
eye
patching.
If
the
victims
eyes
are
patched,
they
are
unable
to
assistintheirownevacuation;ifonlyoneeyeispatched,theywillstillrequireassistancebecauseofthe
lossofdepthofvision.
Prognosis
The prognosis forsolarkeratitis is good while the condition is
painful andannoying it will normally
resolvewithinadayortwowithoutanyfollowonproblems.
Prevention
Wearing
high
quality
tinted
glasses
or
goggles
will
help
prevent
snow
blindness
and
having
a
spare
pair
incaseyouloseorbreakyourprimarypairisagoodidea.
Goodgogglesorglasseshavethefollowingcharacteristics:
99100%UVabsorption
PolycarbonateorCR39lens(lighter,morecomfortablethanglass)
510%visiblelighttransmittance
Largelensesthatfitclosetotheface
Wraparoundorsideshieldedtopreventincidentallightexposure
Theactualcolor
ismoreamatterofpersonalpreferencesomepeoplepreferneutralgray
lensesto
minimize color changes, others find that various shades of
yellow or amber help with flat light
conditions.
Ifsunglassesarenotavailable,areplacementcanbemadefromfabric,woodorplastictiedacrossthe
face(asglassesare)withasmallhorizontalslitcutinitovertheeyeposition,toprovidevision.
While
wearingahatisnecessary,abrimmedhatwillprovideminimalprotectionagainstsnowblindness
becauselightwillbereflectedupfromthesnowontheground.
-
8/14/2019 Mountain and Cold Medical Considerations
17/18
Section7:ConsiderationsforFirstAidKits
Becauseofthecoldtemperatures,avoid(asmuchaspossible)any
liquidsorgels includingointments.
Drugs that freeze may separate, and when they thaw not recombine
correctly, rendering them
dangerousoruseless. Inparticular,proteincontainingdrugs (suchas
insulin)mustnotbeallowedto
freeze, or NOT USED if frozen the proteins will precipitate from
the solution and can cause a
thrombosis.
Solidpillsortabletscanbe frozen ifneeded. Capsules (whicharemade
fromgelatin)willdeteriorate
rapidlywhenfrozenandshouldbeavoided.
Ifliquidsorgelsarenecessaryandunavoidable,packthemwithgoodinsulation.
Asmallchemicalheat
packmayhelpkeepthemfromfreezing;orkeepthemclosetoyourbody.
Hyperbaricchamber
therapy
Forhighaltitude(>15,000feet)atransportable,fabric,hyperbaricchambersuchastheGamowBagis
commercially available, for use when evacuation to lower
elevations are not possible because of
distanceorweatherconditions.
Thevictimisplacedinthebag,whichisthenzippedclosed,andafoot
operatedairpumpincreasestheatmosphericpressureinsidethebagbyapoundortwo,whichcanbe
theequivalent (athighaltitude)ofa5,000footdescent.
Withsufficientresourcesthepatientcanbe
evacuatedwhileinthechamber,usingabasketstretcherorsimilardevice.
Gamowbag(picturefromWikipedia)
Gamow and similar bags are heavy, and somewhat expensive. They
can be rented for specific
expeditionsfromvarioussourcesifdesired.
-
8/14/2019 Mountain and Cold Medical Considerations
18/18
Bibliography:
Auerbach,etal.FieldGuidetoWildernessMedicine,3rdEd.
NewYork,NYMosby,2008Auerback,etal.
WildernessMedicine,5thEd,Philadelphia,PAMosby,2006Fauci,
et
al,
ed.
HarrisonsPrincipals
of
Internal
Medicine,
17
th
Ed,
New
York,
NY.
McGraw
Hill,
2008
Forgey,William. WildernessMedicine,BeyondFirstAid,5thEd.
Guilford,CTGlobePequodPress,1999Guyton, Arthur C, Hall, John E,
Textbook of Medical Physiology, 11th Ed. Philadelphia, PA,
ElsevierSaunders. 2006.
High Altitude Medical Guide, Lake Louise Consensus on the
Definition of Altitude
Sickness,http://www.highaltitudemedicine.com/AMSLakeLouise.html,lastaccessed2Feb2010.
Keystone,etal.
TravelMedicine,1stEd,Philadelphia,PAMosby2004Kumar, et al. Robbins
and Cotran Pathological Basis of Disease, 7th Ed. Philadelphia, PA.
ElsevierSaunders,
2005.
Ma,etal. TintinallisEmergencyMedicineManual,6thEd,NewYork,NY.
McGrawHill,2003Marx,RosensEmergencyMedicine,6thEd,Philadelphia,PA,Mosby,2002MontgomeryandKotwal,RangerMedicHandbook,75thRangerRegimentTraumaManagementTeam(Tactical),USArmySpecialOperationsCommand,2007
National Association of Emergency Medical Technicians.
Prehospital Trauma Life Support
MilitaryEdition,6thEd.Philadelphia,PA.Mosby/Jems,2006
Pandolf,Burr(eds),MedicalAspectsofHarshEnvironmentsvols1and2,BordenInstitute,OfficeoftheSurgeon
General,
US
Army,
Falls
Church,
VA
2002
TheInternationalMountaineeringAndClimbingFederation/UnionInternationaleDesAssociations
Dalpinisme(UIAA),ConsensusStatementOfTheUIUAAMedicalCommissionVol:10TheEffectOfExtremesOfTemperatureOnDrugs,Berne,Switzerland,2008Yevich,etal.
SpecialOperationsForcesMedicalHandbook1stEd,Jackson,WYTetonPress,2001