Embed Size (px)
Citation preview
Inside this issue
Levels of Sedation ........................ 1
Pre-sedation Evaluation ............... 1
Sedation Process ………….............. 3
Medication for Sedation.…………...4
Potential Complications……….......6
Case Examples ………………...........6
Non-medical Preparations .………..7
QUIZ Link..……………………………...7
Introduction
When children need medical procedures or prolonged imaging, sedation is often required to help
achieve the goals of effective pain management, anxiolysis, and behavior modification. Sedation with
a natural airway and the patient spontaneously breathing but in a minimally altered level of con-
sciousness is the goal for most procedural sedation.. Safe and effective sedation for medical proce-
dures and imaging in children using a natural airway requires an understanding of (1) levels of seda-
tions (2) pre-sedation evaluations (3) candidates selection (4) equipment for sedation (5) monitoring
during sedation (6) management of common sedation complications (7) medications for sedation and
(8) steps in recovery from sedation. In this review, we provide a general overview of sedating children
while maintaining their natural airway by discussing each of the topics listed above.
Levels of Sedation
There are three levels of sedation: minimal sedation, moderate sedation, and deep sedation. Each
level has different effects on the patient’s level of consciousness, respiratory drive, and cardiovascular
stability. The deeper the level of sedation there is a higher risk for cardiopulmonary complications.
These levels of sedations are compared to each and general anesthesia in Table 1.
MOTT BUILDING BLOCK Pediatric Trauma Surgery Newsletter Volume I Issue IX ~ Fall 2016
SEDATION IN THE PEDIATRIC PATIENT
AUTHOR: Lauren Yagiela, MD, Critical Care Fellow, Division of Pediatric Critical Care, C. S Mott Children’s Hospital Univ. of Mich. Health System
Tim Cornell MD, Pediatric Fellowship Director, Division of Pediatric Critical Care, C. S. Mott Children’s Hospital Univ. of Mich. Health System
Article authors, or faculty planner Dr. Peter Ehrlich, have no financial relationships with any commercial interest producing health care goods or services r/t this article
LESSONS FOR PRACTICE:
Develop an understanding of
the levels of sedation
Learn the components of a pre-
sedation evaluation and candi-
date selection for sedation
Equipment and medications
used for sedation
Sedation monitoring and man-
agement of common complica-
tions
Sedation recovery steps
The University of Michigan Medical School is accredited by the Accreditation Council for Continuing Medical Educa-tion (ACCME) to provide continuing medical education for physicians. The University of Michigan Medical School designates this enduring material for a maximum of 1.0 AMA PRA Catego-ry 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activi-ty. The CME activity is comprised of this newsletter and an online knowledge test. To receive credit, participants must read the newsletter article and pass the exam with a score > 70%. The activity can be completed within 1 hour. This CME ac-tivity was released in December 2016 with credit available through November 2019. Continuation of credit from that date depends on a thorough review of the content currency and accuracy.
Level of
Sedation
Level of Consciousness
Effects on Respiratory
System
Effects on Cardiovascular
System
Minimal
Patient may have impairment of cognitive function or coordination but is able to respond normally to verbal commands
Patient should spontaneously breath effectively
Patient should be cardiovascularly stable
Moderate
Patient has a depression of consciousness but can respond purposefully to verbal com-mands or light touch
Patient should spontaneously breath effectively
Patient should be cardiovascularly stable
Deep
Patient has depression of con-sciousness during which they cannot be easily aroused but could respond purposefully to repeated verbal or painful stimulation
Patient may require assistance with maintaining a patent airway and adequate spontaneous ventilation
Patient should be cardiovascularly stable
General Anesthesia
Patient has loss of conscious-ness during which they are not arousable to even painful stimuli
Patient will need assistance with airway protection and ventilation
Patient may become cardiovascularly unstable
Table 1
2
“Life starts all over again when it gets crisp in the fall….” F. Scott Fitzgerald
Physical status exam. Assess the patient’s over-all physical status using ASA classification, see Table 2. Physical exam. Pediatric patient physical exam prior to any sedation procedure should minimally include the following information:
Weight
Vital signs (heart rate, blood pressure, respira-tory rate, room air oxygen saturation, tempera-ture)
General exam
Focused airway exam to determine risk of airway obstruction
Tonsillar hypertrophy
Abnormal anatomy (mandibular hypoplasia, large neck)
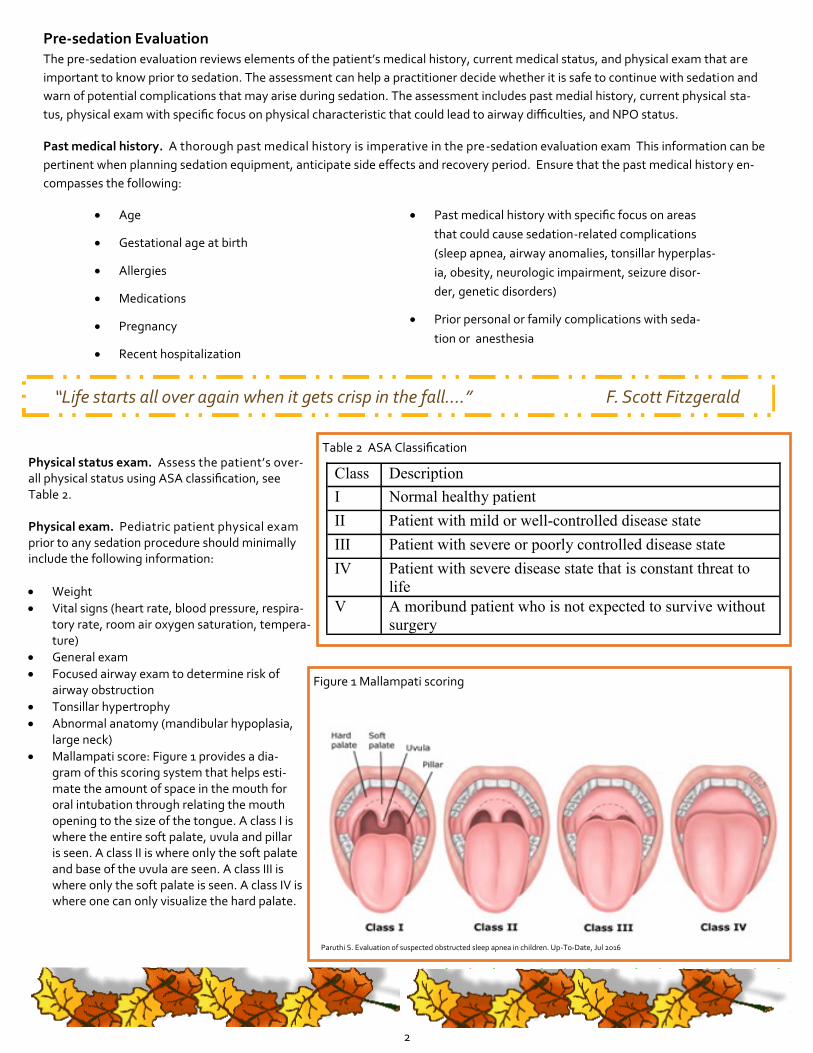
Mallampati score: Figure 1 provides a dia-gram of this scoring system that helps esti-mate the amount of space in the mouth for oral intubation through relating the mouth opening to the size of the tongue. A class I is where the entire soft palate, uvula and pillar is seen. A class II is where only the soft palate and base of the uvula are seen. A class III is where only the soft palate is seen. A class IV is where one can only visualize the hard palate.
Pre-sedation Evaluation
The pre-sedation evaluation reviews elements of the patient’s medical history, current medical status, and physical exam that are
important to know prior to sedation. The assessment can help a practitioner decide whether it is safe to continue with sedation and
warn of potential complications that may arise during sedation. The assessment includes past medial history, current physical sta-
tus, physical exam with specific focus on physical characteristic that could lead to airway difficulties, and NPO status.
Past medical history. A thorough past medical history is imperative in the pre-sedation evaluation exam This information can be
pertinent when planning sedation equipment, anticipate side effects and recovery period. Ensure that the past medical history en-
compasses the following:
Age
Gestational age at birth
Allergies
Medications
Pregnancy
Recent hospitalization
Past medical history with specific focus on areas
that could cause sedation-related complications
(sleep apnea, airway anomalies, tonsillar hyperplas-
ia, obesity, neurologic impairment, seizure disor-
der, genetic disorders)
Prior personal or family complications with seda-
tion or anesthesia
Class Description
I Normal healthy patient
II Patient with mild or well-controlled disease state
III Patient with severe or poorly controlled disease state
IV Patient with severe disease state that is constant threat to
life
V A moribund patient who is not expected to survive without
surgery
Table 2 ASA Classification
Figure 1 Mallampati scoring
Paruthi S. Evaluation of suspected obstructed sleep apnea in children. Up-To-Date, Jul 2016

3
Pre-sedation Evaluation (cont.)
NPO status. Establish the time of the last food and drink consumed by the patient. Guidelines for NPO time are noted in Table 4.
Additional
Appropriate candidates for sedation. After completion of the pre-
sedation assessment, a practitioner should review the gathered infor-
mation with two objectives in mind. First, is this patient a safe minimal to
deep sedation candidate. Second, what complications should I anticipate
with this patient.
Patients with ASA I or II and those with no airway concerns are the best
candidates for minimal to deep sedation with a natural airway. However,
patients with the following conditions may not be suitable candidates for
moderate or deep sedation: children with an ASA III, children with airway concerns (moderate-to-severe tonsillar hypertrophy, anatom-
ic airway anomalies), prematurity (<60wks gestation), patients requiring home monitors (apnea, respiratory, cardiac), acute or chronic
respiratory condition (bronchopulmonary dysplasia, poorly controlled asthma, pneumonia, bronchiolitis, or croup), uncontrolled sei-
zures, multiple psychotropic medications, active emesis, increased intracranial pressure, or prior history of difficult sedation. For these
patients, consultation with an anesthesiologist may be necessary before sedation.
Food Item Recommended NPO time
prior to sedation
Clear liquids 2 hours
Human milk 4 hours
Infant formula 6 hours
Nonhuman milk 6 hours
Light meal 6 hours
Sedation Process
Prior to starting sedation, a “time-out” should be conducted to make sure at the
appropriate personal, equipment, sedation plan, and emergency contingency
plans are in place. Elements to be discussed during a “time-out” include identify-
ing the correct patient through verification of their medical record number and
birth date, review plans for monitoring during the sedation, running through
equipment available at bedside, discuss the sedation plan, and evaluate whether
parents, patient, or practitioners at bedside have any last questions or concerns.
Sedation equipment. Preparation of equipment for monitoring the patient
and providing support to assist with complications prior to initiation of sedation is necessary. A common acronym for the equipment is
SOAPME (Table 5).
S Suction Age appropriate suction catheters and suction device
O Oxygen A way to administer oxygen
A Airway Equipment Age appropriate airway equipment including simple face
mask, bag-valve-mask with appropriately sized mask,
nasopharyngeal airway, oropharyngeal airway, laryngeal
mask airway (LMA), laryngoscope blades, endotracheal
tubes, stylets
P Pharmacy Medication for managing emergency situations includ-
ing basic code medications and medications needed for
intubation
M Monitors Pulse oximeter, end-tidal CO2 monitoring, noninvasive
blood pressure, and other monitors (EKG, stethoscope)
E Special equipment
or drugs
Specific needs for a particular case
Table 5
4
Sedation Process (cont.)
Monitoring. Patients should have continuous pulse oximetry, a non -invasive blood pressure cycling every 5-10 minutes, end-tidal car-
bon dioxide continuous monitoring, and often continuous cardiac monitoring. This provides information on oxygenation, ventilation, and
hemodynamic stability during sedation. Monitoring the end-tidal carbon dioxide waveform can be especially helpful during sedation as a
reduction or loss of the waveform could indicate ineffective ventilation either through upper airway obstruction or apnea. End-tidal moni-
toring detectes early changes in ventilation and can alert the practitioner of potential problems quicker than pulse oximetry.
Documentation. Documentation should include information pertaining to the medication administered (name of medication, route
of administration, site administered, time administered, and dosage) and the effect of the medication effect on the patient. Additionally,
vital signs (heart rate, blood pressure, expired carbon dioxide values, and oxygen saturations) at regular intervals should additionally be
recorded.
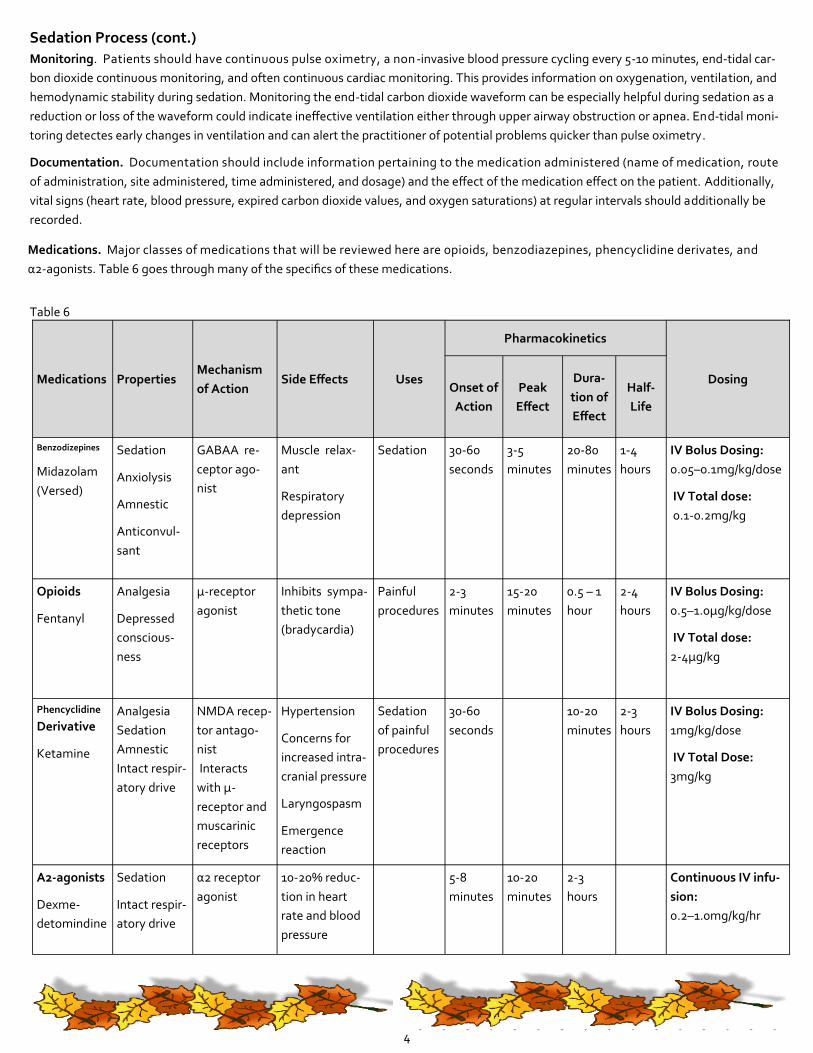
Medications. Major classes of medications that will be reviewed here are opioids, benzodiazepines, phencyclidine derivates, and
α2-agonists. Table 6 goes through many of the specifics of these medications.
Medications Properties Mechanism
of Action Side Effects Uses
Pharmacokinetics
Dosing Onset of
Action
Peak
Effect
Dura-
tion of
Effect
Half-
Life
Benzodizepines
Midazolam
(Versed)
Sedation
Anxiolysis
Amnestic
Anticonvul-
sant
GABAA re-
ceptor ago-
nist
Muscle relax-
ant
Respiratory
depression
Sedation
30-60
seconds
3-5
minutes
20-80
minutes
1-4
hours
IV Bolus Dosing:
0.05–0.1mg/kg/dose
IV Total dose:
0.1-0.2mg/kg
Opioids
Fentanyl
Analgesia
Depressed
conscious-
ness
µ-receptor
agonist
Inhibits sympa-
thetic tone
(bradycardia)
Painful
procedures
2-3
minutes
15-20
minutes
0.5 – 1
hour
2-4
hours
IV Bolus Dosing:
0.5–1.0µg/kg/dose
IV Total dose:
2-4µg/kg
Phencyclidine
Derivative
Ketamine
Analgesia
Sedation
Amnestic
Intact respir-
atory drive
NMDA recep-
tor antago-
nist
Interacts
with µ-
receptor and
muscarinic
receptors
Hypertension
Concerns for
increased intra-
cranial pressure
Laryngospasm
Emergence
reaction
Sedation
of painful
procedures
30-60
seconds
10-20
minutes
2-3
hours
IV Bolus Dosing:
1mg/kg/dose
IV Total Dose:
3mg/kg
Α2-agonists
Dexme-
detomindine
Sedation
Intact respir-
atory drive
α2 receptor
agonist
10-20% reduc-
tion in heart
rate and blood
pressure
5-8
minutes
10-20
minutes
2-3
hours
Continuous IV infu-
sion:
0.2–1.0mg/kg/hr
Table 6
5
“Autumn, the year’s last, loveliest smile” William Cullen Bryant
Sedation Process (cont.) Recovery. After receiving sedation, a patient should be continued to be monitored until their presedation level of consciousness has returned. During this monitoring, a patient should have vital signs recorded at regular intervals and if they are not alert, continuous pulse oximetry and heart rate monitoring. At completion of this monitoring, a child or an infant should be able to remain awake in a quiet environment for at least 20 minutes.
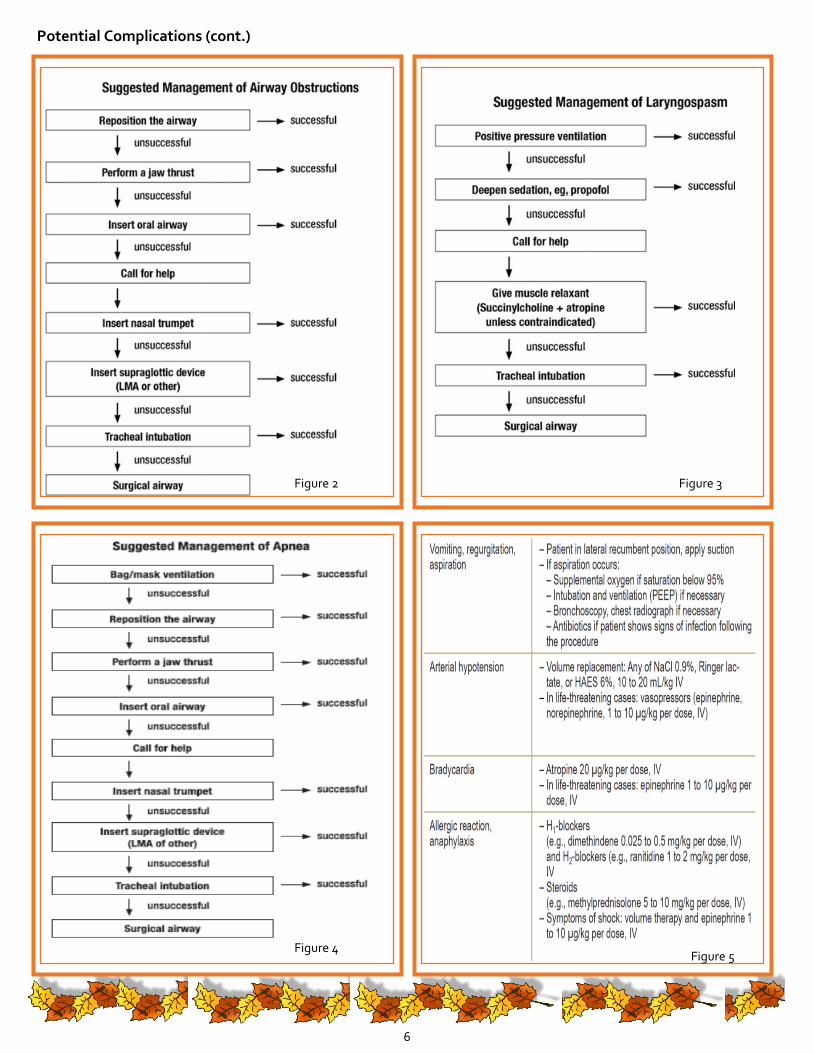
Potential Complications
Three of the most common side effects include airway obstruction, laryngospasm, and apnea. The recent AAP guidelines (Coté et al 2016)
for monitoring and managing sedation have suggested algorithms for managing these complications (Figures 2-4). Airway obstruction
occurs during sedation due to the fact that many of the sedating medications reduce airway tone, specifically opioids and benzodiaze-
pines. If a patient has a predisposition to having an airway obstruction (obesity, large tonsils, known sleep apnea) this is more likely to oc-
cur. Laryngospasm occurs when irritation of the vocal cords occurs causing them to spasm shut and obstruct the airway. This is a known
side effect of ketamine. Apnea can occur when medications such as opioids or benzodiazepines are over-dosed leading to respiratory drive
suppression. Additional complications that can occur are vomiting, arterial hypotension, bradycardia and allergic reaction. Approaches to
treatments for these conditions can be found in figure 5.
Sedation Case Examples
Case #1 An 11-year-old boy comes in with fever, hypotension, and tachycardia. He receives 60cc/kg normal saline bolus but continues
to have a BP of 70/40 with a heart rate of 140bpm. He is conversent with an appropriate mental status and saturating 100% on
room air. He has a clear chest xray. The decision is made that he need a femoral central line placed to administer vasopressor
medications. What would be the most appropriate level of sedation and method of sedation?
Case #2 A three-year-old patient has a concern for acute appendicitis. Her appendix was not able to be seen with an US and she needs
a CT scan. She is however is refusing to be separated from her mother and to lie flat. What would be the most appropriate level
of sedation and method of sedation?
Case #3 A 5-year-old boy is newly diagnosed with a brain tumor and needs to have an MRI of head and spine that will last 2 hours. For
this, he needs to lay still. He is conversing and appropriate on exam. He has a normal pulmonary and cardiovascular exam. What
would be the most appropriate level of sedation and method of sedation?
Answers
Case #1 Here we would recommend moderate sedation with ketamine.The benefit of this medication is that it causes both sedation
and pain management for a painful procedure needing sedation. Additionally, this medication will not suppress his drive to breath and
will likely cause an increase in his blood pressure rather than further hypotension.
Case #2 Here we would recommend minimal to moderate sedation. Since she will just need mild sedation and anxiolysis not analge-
sia, a dose of versed may be appropriate.
Case #3 Here we would recommend moderate sedation. Since he needs sedation not analgesia for along period time along with a
normal cardiopulmonary exam, dexmeditomidine infusion would be an appropriate option. Additionally, since this is in infusion, it can
be run for the length of case and also has the benefit of not causing any respiratory depression.
6
Potential Complications (cont.)
Figure 2 Figure 3
Figure 4
Figure 5
7
CONTACT US
EDITOR: AMY RANDALL, MSN, RN Pediatric Trauma Program Manager
EMAIL: [email protected]
C. S. Mott Children’s Hospital 1500 E. Medical Center Drive Ann Arbor, MI 48109-5231
NURSES: Remember 1 CME = 1 CEU credit for nursing! This activity WILL count toward your 25 hours/2yrs of required CEU for licensure
TAKE THE QUIZ!
KNOWLEDGE TEST AND AMA/PRA
CATEGORY 1 CREDIT
After reading the article, continue the educational activity by
taking the online CME quiz at:
https://cme.med.umich.edu/assessment/questions.asp?gid=177 After you initially take the test, the test will be immediately electronically scored.
If fewer than 70% of the questions are answered correctly, the questions that were not answered correctly will be
noted in red. Review the CME content related to those topics and retake the test.
If 70% or more of the questions are answered correctly, the correct and incorrect answers for all questions will be
shown along with explanations of the basis for the correct answer. The link to register and receive credit is shown
at the end of the items and explanations. Complete the electronic credit request and activity evaluation. An
electronic certificate of participation will be provided immediately. Print the certificate of participation for your
personal records.
Article references: Coté CJ, Wilson S. Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures: Update 2016. Pediatrics 2016; 138:e1.
Hansen T. Sedative medications outside the operating room and the pharmacology of sedatives. Current Opinion in Anesthesiology 2015; 28:446.
Fuhrman BP and Zimmerman JJ, Carcillo JA, Clark RS, Relvas M, Rotta AT, Thompson AE, Tobias JD.Pediatric Critical Care. Philadelphia, PA: Mosby-Elsevier, 2011.rman Neuhauser, Wagner, Heckman, Weigand, and Zimmer. Analagesia and Sedation for Painful Interventions in Children and Adolescents. Dtsch Arztebl Int 2010; 107(14):241-7.
Paruthi S. Evaluation of suspected obstructed sleep apnea in children. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on August 21, 2016.)
Samsoon GL, Young JR. Difficult tracheal intubation: a retrospective study. Anaesthesia 1987; 42:487
Ketamine. Lexicomp.In: Lexicomp Online® , Pediatric & Neonatal Lexi-Drugs® , Hudson, OH (Accessed August 21, 2016)
Midazolam. Lexicomp In: Lexicomp Online® , Pediatric & Neonatal Lexi-Drugs® , Hudson, OH (Accessed August 21, 2016)
Fentanyl. Lexicomp. In: Lexicomp Online® , Pediatric & Neonatal Lexi-Drugs® , Hudson, OH (Accessed August 21, 2016)
Dexmedatomidine. LexicompIn: Lexicomp Online® , Pediatric & Neonatal Lexi-Drugs® , Hudson, OH (Accessed August 21, 2016)
Non-medical Preparations for Procedures: Child Life Bethany Folsom, MS, CCLS, CPST
Many of the experiences a child encounters in a medical setting are new and unfamiliar. Child Life Specialists are part of the medical team and bring an expertise in child development, especially as affected by medical experiences. They offer a wide array of tools and techniques to calm fears, soothe anxiety, allow for emotional expression, and encourage compliance. Child Life Specialists provide developmentally appropriate education individualized to each child and family to help them prepare for a hospital experience Example Interventions include:
preparation materials that allow patients to explore the experience before the actual procedure: books, pictures, and medical equipment
collaboration with the patient and family to identify current coping techniques or learn new techniques practice/rehearsal of procedure utilizing coping strategy and tools distraction/coping before, during, and after the procedure
Distraction. Giving children something to focus on to distract them from the perceived threats of their experience can be an espe-cially effective way to minimize anxiety. Whether it be video games, toys, bubbles, or something as simple as conversation, an individual-ized distraction plan can help create a positive experience for both patients and family members.
Medical Play. Play is the work of a child and through play a child learns about the world around them. Play allows children to learn new information and explore new concepts in a non-threatening and natural way, and should be included in the medical environment. Medical play is used as a teaching tool to familiarize children about a new experience, pro- cedure, or medical equipment. Through a medical play session, Child Life Specialists can:
identify patient misconceptions promote mastery and instill a sense of control allow expression of feelings.
Research shows that the interventions done by services such as Child Life can:
increase patient satisfaction scores give both the patient and the family a sense of control help patients cope effective with both the current and future medical encounters facilitates the concept and practice of Patient and Family Centered Care
For more information, visit
www.childlife.org





























