Embed Size (px)
Citation preview

Motor Speech Assessment Packet Assembled by: Piper Doering (2013)
Includes:
After a full review of the patient’s chart:
1. History Components
Patient Interview: to collect information first-hand from the patient about the
nature and course of impairment. This information pertains to the specific body
functions and structures that are impaired. Patient-perceptions on functional
limitations and perceived disabilities are also included. This information pertains
to the activities the patient is involved in and the participation limitations
experienced as a result of the patient’s impairments. In addition, personal factors
are emphasized to determine the emotional impact of the current impairment.
Partner Interview: to collect information on partner perceptions related to the
patient’s impairment and how the impairment impacts daily life. This information
pertains to the specific body functions and structures that are impaired in addition
to their functional impact on activities and participation. Information on family
resources is also included. Knowing and incorporating the strengths and social
circles of the family will promote successful intervention.
2. Physical Examination
Oral Mechanism Examination: to assess each component of the speech system
separately and to define and classify notable changes by cranial nerves (V, VII,
IX, X, XII). The face, lips, jaw, tongue, and palate are all assessed for the
following: strength, speech, range of motion, tone, and coordination. Pertinent
questions related to patient history are included throughout to supplement the
physical examination findings. A test for apraxia of speech is included, but should
only be used if groping is present during the evaluation.
3. Motor Speech Evaluation
Oral Mechanism Examination: an overview of RPRAP components are also
included within the oral mechanism examination to screen for changes in
respiration, phonation, resonance, articulation, and prosody. This includes the
“acoustic motor speech evaluation” and “combined systems” sections. This is a
perceptual examination of the patient’s speech at the sound, syllable, and
connected speech levels.
ASHA NOMS: this rating scale is to be used in conjunction with the connected
speech sample from the oral mechanism examination. This rating helps to classify
how easily the patient can be understood by others and provides more concrete
data on an individual’s speech for reporting purposes.
The Frenchay Intelligibility Test: this portion of the Frenchay Dysarthria
Assessment is included to assess intelligibility at the word and sentence level.
Intelligibility examines the clarity of the patient’s acoustic signal to an unfamiliar
listener within a clinical context.
PACE Rating Scale: to assess comprehensibility in consideration to
environmental and activity/participation components. This assessment allows for
observation of the conversational roles of the patient (patient as sender &
receiver); in addition to the roles of the patient’s partner (clinician/partner as
sender & receiver). This rating provides information on how effectively the
patient can share new information. The patient can use any communicative
modalities to convey information. This assessment provides useful information to
be applied to intervention in relation to co-constructed conversations and
communication success within functional social contexts.

Interview Questions for Patient Duffy, 2005; Yorkston 1999
Patient Name:
Date of Birth:
Referring Physician:
Date of Evaluation:
Onset and Course
1. What difficulty do you have with your speech?
2. What comments have others made about your speech?
3. When did your speech problems begin? Suddenly or gradually? Have other problems
developed in addition to your speech difficulties?
4. How has your speech changed compared to 6 months ago or a year ago?
5. Has your speech ever returned to normal? If so, when and for how long?

6. Are you taking any medications that affect your speech positively or negatively? What else
influences your speech (time of day, rest, who you’re talking to, etc.)
Associated Deficits
1. Have you had any difficulties with chewing or swallowing? Describe.
2. Is it difficult to move food in your mouth or move food back to get the swallow started?
3. Is it more difficult to swallow solids versus liquids? Do you have any coughing or choking
sensations at meals?
4. Any difficulty managing your own secretions or drooling?
5. Have you had any change in your emotional expression? Do you cry or laugh more easily or
less easily than in the past?

Patient’s Perception of Deficit
Describe your current speech difficulty. If your speech was 100% before this all began, what
would you rate your speech now?
Consequences of the Disorder
1. Do people have trouble understanding you? If so when and what happens during these
instances?
2. Have you altered your work or social activities because of your speech? In what way? Does
your speech keep you from doing things you would like to do?
3. How do you feel when you have difficulty being understood?
4. How do others react when you have difficulty being understood?
5. How has your speech difficulties affected your interactions with your family?

Management
1. What have you done to compensate for your difficulty?
2. Do you think you need help with your speech now?
Awareness of Diagnosis and Prognosis
1. What have you been told is the cause of this problem?
2. What does the diagnosis mean is going to happen?
Interview Questions for Partners Based on Lubinski, 1991 in Yorkston, 1999
Demands
1. What significant events were occurring in your family prior to the onset of your family
member’s communication difficulties?
2. How have these events changed since the onset of the physical and communication
problems?
3. Is your family member independent in caring for himself or do they depend on someone for
all or some of their cares?
4. How as the communication difficulties affected your family member’s social life?
5. How has the communication difficulties affected your family member’s caregiver(s)?
6. How as the primary caregiver and your family member’s daily life changed since the start of
the communication difficulties?
7. What are the financial implications of the communication difficulties?

8. How did the family change immediately at the onset of the problem? How has it changed
since?
Resources
1. How would you describe your family’s strengths?
2. How willing is your family member to seek help from friends, counselors, religious
institutions, social services, others.
3. Who are the primary communication partners of your family member and will they be able
to participate in the therapy program?
Definition of the Problem
1. What do you perceive as the major problem facing your family at the present time?
2. What do you think can be done about this problem?
3. If there are other issues going on in your family and family member’s life, how do they
compare to the current communication difficulties your family member is experiencing?

Oral Mechanism Examination Adapted from Freed, 2012 and Enderby, 1983
Patient’s Name:
Date of Examination:
Patient’s Age:
Neurological Diagnosis:
Relevant Personal Information:
Medical History:
Instructions: Answer each item yes or no and indicate the degree of impairment as follows:
0 = no impairment
1 = mild impairment
2 = moderate impairment
3 = severe impairment
Also be sure to answer all other questions in the space indicated
If any groping is present, an additional test for nonverbal oral apraxia must be completed.

Facial musculature at rest: CN VII Yes No Degree
Is the mouth symmetrical?
Can patient resist examiner’s attempt to force lips open?
Are eyes open?
Are eyes partially closed?
Is the face rigid or masked?
Is there wrinkling of forehead when asked to look up?
Is nose symmetrical (look at nasolabial fold)?
Facial musculature during movement: CN VII Yes No Degree
Is the smile symmetrical?
Is groping present?
Can patient pucker lips?
Is groping present?
Can patient puff out cheeks and maintain lip seal when
pressure is applied?
Mandibular musculature at rest: CN V Yes No Degree
Does mandible hang lower than normal?
Is there even bulk of mandibular musculature on each side of
the face?
Mandibular musculature during movement: CN V Yes No Degree
When mouth is open as widely as possible, is there deviation
to one side?
Is groping present?
Can patient move mandible voluntarily to the right or left?
Can the patient resist the examiner’s attempt to lower the jaw
when the teeth are clenched?
Can the patient keep mouth wide open as the examiner
attempts to force it closed?
Any pain with movement?
General Observations of the Oral Cavity
Observe teeth: cavities, missing teeth, overall hygiene
Does the patient have dentures?
Observe oral cavity: moisture, color, bite marks on cheeks

Tongue musculature at rest: CN XII Yes No Degree
Is tongue normal in size (normal bulk, no atrophy)?
Is tongue moist?
Does the tongue lie midline?
Is the tongue symmetrical in shape?
With tongue resting atop edges of lower incisor teeth, is
fasciculation observable?
Tongue musculature during movement: CN XII Yes No Degree
Can patient protrude tongue completely?
Is groping present?
With tongue protruded, can patient resist examiner’s attempt to
force tongue to the other side?
With tip of tongue, can patient touch the upper lip and alveolar
ridge?
With tongue in cheek, can patient resist examiner’s effort to
force tongue inward?
Can the patient move the tongue from side to side?
Velum and Pharynx at rest and during movement: CN X Yes No Degree
Is the velum symmetrical at rest?
Does the velum rise symmetrically each time the patient
sustains /a/?
Does the velum rise symmetrically each time the patient says
/a, a, a/?
Is the uvula symmetrical?
Is there a gag reflex when the back wall of the pharynx is
touched?
Is the patient able to produce a sharp cough?
Can the patient produce a sharp glottal stop?
Is inhalatory stridor present?
Questions for Patient 1. Do you cough or choke when eating or drinking? - reflex
2. Do you have difficulty clearing your throat? - reflex
3. Do you have difficulty swallowing? - reflex
4. Do you ever notice dribbling or drooling from your mouth? - reflex
5. Do you notice running out of breath when you speak? - respiration
6. Does food or drink ever come down your nose? - soft palate

Testing for Nonverbal oral Apraxia This is to be used only if groping is present during the oral mechanism examination
Directions to patient: “Now I want you to do some things. Listen closely and do everything as
completely and as well as you can. Are you ready?”
Response Test Item Graded Response Scale
1. Stick out your tongue 1. Accurate and immediate
response with no hesitation
2. Accurate after trial-and-error
searching movement on
command
3. Crude, defective in amplitude,
accurate, or speed on
command
4. Partial response (an important
part missing) on command
5. Same as (1) after
demonstration
6. Same as (2) after
demonstration
7. Same as (3) after
demonstration
8. Same as (4) after
demonstration
9. Perseverative response
10. Irrelevant response
11. No oral performance
2. Show me how you blow out a match
3. Show me your teeth
4. Round your lips
5. Touch your nose with the tip of your tongue
6. Bite your lower lip
7. Show me how you whistle
8. Lick your lips all around
9. Clear your throat
10. Move your tongue in and out
11. Click your teeth together once
12. Show me how you smile
13. Click your tongue
14. Chatter your teeth as if you were cold
15. Touch your chin with the tip of your tongue
16. Show me how you cough
17. Puff out your cheeks
18. Wiggle your tongue from side to side
19. Pucker your lips
20. Alternately pucker and smile
Testing for Apraxia of Speech (Oral Verbal Apraxia) This is to be used only if groping is present during the oral mechanism examination
Directions to patient: “Say these words for me.” If patient is unable to repeat to verbal stimuli,
present words as printed on cards. As patient reads or repeats the following, tape record and
transcribe errors.
1. slowpoke _______________________________________________________________
2. conference ______________________________________________________________
3. Tahiti __________________________________________________________________
4. dressmaker ______________________________________________________________

5. Annapolis _______________________________________________________________
6. kindergarten _____________________________________________________________
7. condominium ____________________________________________________________
8. industrial revolution _______________________________________________________
9. Winnie-the-Pooh and Tigger too _____________________________________________
________________________________________________________________________
10. stiff-stiffer-stiffening ______________________________________________________
________________________________________________________________________
11. base-baseball-baseball cap __________________________________________________
________________________________________________________________________
12. fan-fancy-fantastic ________________________________________________________
________________________________________________________________________
13. glow-glowing-glistening-glamorously _________________________________________
________________________________________________________________________
14. rid-riddle-ridicule-ridiculous ________________________________________________
________________________________________________________________________
“Now these.”
1. The beautiful girl was dancing. ______________________________________________
________________________________________________________________________
2. Open this birthday present first. ______________________________________________
________________________________________________________________________
3. The stranger walked into the store. ___________________________________________
________________________________________________________________________
4. The birdwatcher saw a Norwegian Blue parrot. _________________________________
________________________________________________________________________
Test for Apraxia of Speech continued
“Count from 1 to 20.” Indicate pauses for breath by a slash (/) after the appropriate number.
1. 2. 3. 4. 5.
6. 7. 8. 9. 10.
11. 12. 13. 14. 15.
16. 17. 18. 19. 20.
“Now count backward from 20 to 1.”
20. 19. 18. 17. 16.
15. 14. 13. 12. 11.
10. 9. 8. 7. 6.
5. 4. 3. 2. 1.
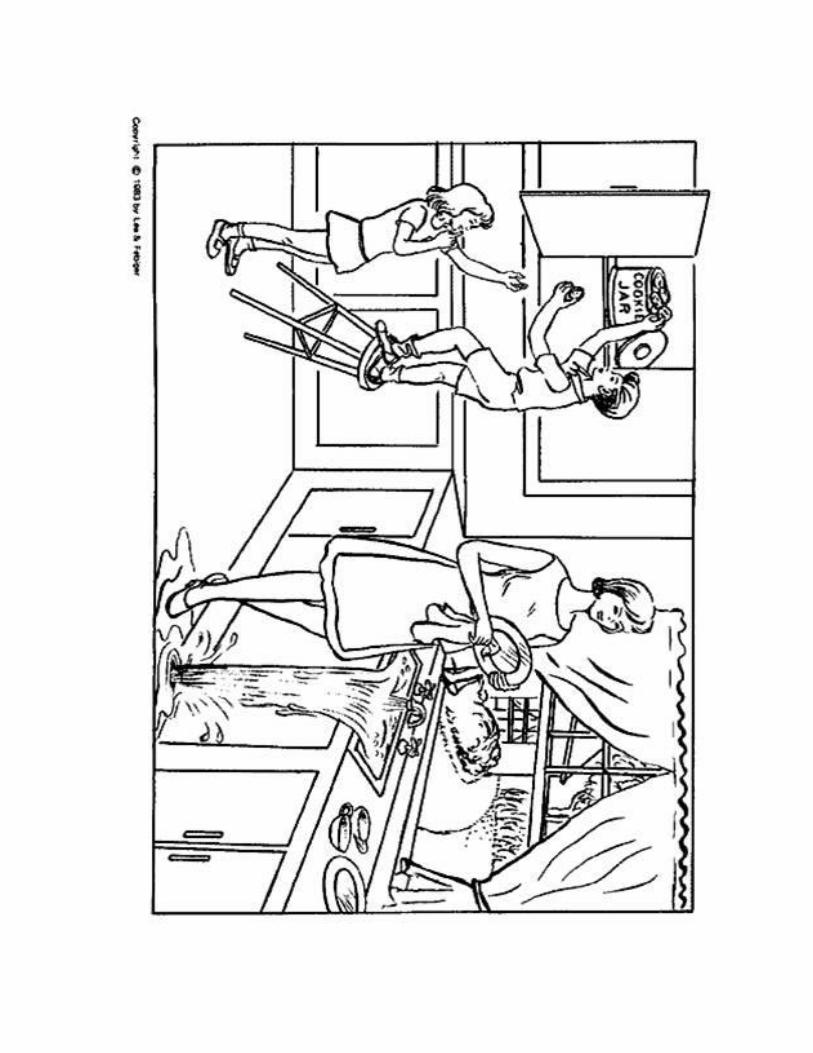
“Tell me what is happening in this picture.” Use the Boston’s “Cookie Theft” picture to evoke at
least 1 minute of ongoing speech. If necessary, point out neglected features of the picture by
asking, “What’s happening here?”

Testing for Apraxia of Speech continued
Write down four sentences that the patient says. If the patient provides an insufficient
speech sample here, use any four sentences produced at any point in the evaluation.
1. ________________________________________________________________________
________________________________________________________________________
2. ________________________________________________________________________
________________________________________________________________________
3. ________________________________________________________________________
________________________________________________________________________
4. ________________________________________________________________________
________________________________________________________________________
“Say these sentences after me.” Use the sentences just written above. Write down (and if
necessary phonetically transcribe) the patient’s imitations.
1. ________________________________________________________________________
________________________________________________________________________
2. ________________________________________________________________________
________________________________________________________________________
3. ________________________________________________________________________
________________________________________________________________________
4. ________________________________________________________________________
________________________________________________________________________
Connected Speech Sample
Have the patient read “My Grandfather” or another standard reading passage and rate the
following questions:
Yes No Degree
Are vowels and consonants produced clearly?
Is the patient’s rate of speech too slow?
Is the patient’s rate of speech too fast?
Does the patient show inappropriate silent intervals between
words?
Does the patient show hypernasality?
Is nasal emission present?

Does the patient vary loudness normally?
If not, is there evidence of monoloudness?
Is there evidence of tremor in the patient’s voice?
Does the patient show abnormal pitch variations?
Does the patient’s voice have a harsh vocal quality?
Does the patient’s voice have a strained-strangled voice
quality?
Does the patient’s voice have a breathy vocal quality?
Does the patient speak in abnormally short phrases?
Are there moments of involuntary inhalation or exhalation?
Is inhalatory stridor present?
Does the patient use normal stress on the appropriate syllables
or words?
If not, is there a reduction in normal stress?
Or is there excess and equal stress?

Grandfather Passage
You wished to know all about my grandfather. Well, he is nearly ninety-
three years old. He dresses himself in an ancient black frock coat,
usually minus several buttons; yet he still thinks as swiftly as ever. A
long, flowing beard clings to his chin, giving those who observe him a
pronounced feeling of the utmost respect. When he speaks his voice is
just a bit cracked and quivers a trifle. Twice each day he plays skillfully
and with zest upon our small organ. Except in the winter when the ooze
or snow or ice prevents, he slowly takes a short walk in the open air each
day. We have often urged him to walk more and smoke less, but he
always answers, “Banana Oil!” Grandfather likes to be modern in his
language.
Rainbow Passage
When the sunlight strikes raindrops in the air, they act like a prism and
form a rainbow. The rainbow is a division of white light into many
beautiful colors. These take the shape of a long, rough arch, with its path
high above, its two ends apparently beyond the horizon. There is,
according to legend, a boiling pot of gold at one end. People look, but no
one ever finds it. When a man looks for something beyond reach, his
friends say he is looking for the pot of gold at the end of the rainbow.

Acoustic Motor Speech Examination
Directions to patient: “Take a deep breath and say /a/ as long, steadily, and clearly as you can.”
a. Duration: the average is 15 seconds for adults and 10 seconds for school-age children
Trial 1:
Trial 2:
Trial 3:
Average:
b. Latency: Is there a latency period between signal to say /a/ and initiation of phonation?
c. Quality
Steady and even
Smooth and clear
Hypernasality
Breathiness
Harshness
Diplophonia
d. Pitch
Too high
Too low
Normal
Tremor
Pitch breaks
e. Loudness
Excessive loudness
Inadequate loudness
Normal loudness
f. Describe Abnormalities: __________________________________________________
________________________________________________________________________
________________________________________________________________________

Combined Systems (Phonatory, Respiratory, Resonatory, and Articulatory)
Alternate Motion Rate (AMR)
Directions to patient: “Take in a deep breath and say (e.g., puh, puh, puh) as long, as fast, and as
evenly as you can.”
Yes No Degree
Is AMR slow?
Is AMR excessively fast?
Is AMR dysrhythmic?
Is AMR uneven in loudness?
Is AMR uneven in pitch?
Is there a tremor?
Is there equal spacing between syllables?
Is there blurring between syllables?
Is there hypernasality?
Is there nasal emission?
Is there restriction in amplitude of motion of lips and jaw?
Are there imprecise or distorted consonants?
Indicate rate per 5-second intervals on this table. The average rate for “puh” and “tuh” is
about 30 to 35 repetitions for 5 seconds; “kuh” is somewhat slower.
puh tuh kuh puh, tuh, kuh
Trial 1
Trial 2
Trial 3
Average
Sequential Motion Rate
Directions to patient: “Now I want you to make those three sounds, ‘puh,’ ‘tuh,’ and ‘kuh’
together as long, as fast, and as evenly as you can.
Yes No Degree
Is the patient able to move smoothly from syllable to
syllable?
Are sounds blocked, transposed, or omitted?

Stress Testing of the Motor Speech Mechanism
Directions: Instruct the patient to count rapidly (approximately two numbers per second) at least
up through 100. Demonstrate 1 – 10.
Yes No Degree
Is there audible deterioration of phonation or articulation?
Respiration Task
Directions: Ask the patient to count to 20 as quickly as possible on one breath. Assure that you
are unconcerned about articulation. Just note the number of breaths necessary to complete the
task. Normally, this task can be performed in one breath. People with velopharyngeal
incompetence may be mistaken for patients with poor respiratory control. You may ask the
patient to hold his or her nose to discriminate between the two.
Check the most applicable option
No abnormality
Very occasional breaks in fluency due to poor respiratory control. The patient may
state that he or she is conscious of having to stop to take deep breaths on occasions. An
extra breath may be required to complete the task.
Patient has to speak quickly because of poor respiratory control. The voice may fade.
Patient may require up to four breaths to complete the task.
Patient speaks on inhalation or exhalation, or breath is so shallow that only a few
words are managed. Poor coordination and marked variability. Patient may require
seven breaths to complete the task.
Speech is grossly distorted by lack of control over respiration. May only manage one
word on each breath.
Conversation
Directions: Engage the patient in conversation (e.g., “Tell me about your morning” or “Tell me
about your speech problems”), taking note of relevant speech characteristics. After observing for
each component of RPRAP, rate the patient’s speech using ASHA NOMS.
Respiration
Phonation
Resonance
Articulation
Prosody

ASHA NOMS for Motor Speech Note: Individuals who exhibit deficits in speech production may exhibit underlying deficits in
respiration, phonation, articulation, prosody, and resonance. In some instances it may be
beneficial to utilize additional FCMs focusing on voice if disordered phonation is a large
component.
Level 1: The individual attempts to speak, but speech cannot be understood by familiar or
unfamiliar listeners at any time.
Level 2: The individual attempts to speak. The communication partner must assume
responsibility for interpreting the message, and with consistent and maximal cues, the
patient can produce short consonant-vowel combinations or automatic words that are
rarely intelligible in context.
Level 3: The communication partner must assume primary responsibility for interpreting the
communication exchange, however, the individual is able to produce short consonant-
vowel combinations or automatic words intelligibly. With consistent and moderate
cueing, the individual can produce simple words and phrases intelligibly, although
accuracy may vary.
Level 4: In simple structured conversation with familiar communication partners, the individual
can produce simple words and phrases intelligibly. The individual usually requires
moderate cueing in order to produce simple sentences intelligibly, although accuracy
may vary.
Level 5: The individual is able to speak intelligibly using simple sentences in daily routine
activities with both familiar and unfamiliar communication partners. The individual
occasionally requires minimal cueing to produce more complex sentences/messages in
routine activities, although accuracy may vary and the individual may occasionally use
compensatory strategies.
Level 6: The individual is successfully able to communicate intelligibly in most activities, but
some limitations in intelligibility are still apparent in vocational, avocational, and
social activities. The individual rarely requires minimal cueing to produce complex
sentences/messages intelligibly. The individual usually uses compensatory strategies
when encountering difficulty.
Level 7: The individual's ability to successfully and independently participate in vocational,
avocational, or social activities is not limited by speech production. Independent
functioning may occasionally include the use of compensatory techniques.

Intelligibility
Adapted from the Frenchay Dysarthria Assessment (Enderby, 1983)
Words/Repetition
The following words should be written on individual cards. It is suggested that bold ¼” high
print on 6”x4” cards be used.
Farm Jagged Here Pay Sergeant
Warm Glow Error Briar Brought
Swarm Go Air Prior Thought
Storm Grow Single Area Brawn
Spark Goat Jungle Floor Thorn
Park Bubble Cycle Galore Spain
Dark Stubble Sprinkle Explore Loyal
Dragger Trouble Sway Though Lair
Gadget Double Slay Know Vat
Jacket Car Play Urgent Fat
Task: Shuffle cards and place face down. Select 12 cards at random, taking care not to look at the
cards. Expose the face of each card to the patient. The patient should read the card and the
therapist should write down what the word is understood to be. The first two of the 12 cards are
practice cards and the other 10 are test cards. When the patient has attempted all the cards, take
and check the cards against the words written down. Add the number of words correctly
interpreted and score using the following grades.
Check the most applicable option
Ten words correctly interpreted by the therapist, with speech easily intelligible.
Ten words correctly interpreted by the speech therapist, but therapist had to use
particular care in listening and interpreting what was heard.
Seven to nine words interpreted correctly.
Five words interpreted correctly.
Two or less words interpreted correctly.

Sentences/Description
Clearly write the following sentences on cards. “The man is ____________.”
clocking repeating teaching pitching bending
plotting receding tagging numbing bringing
leaping catering ticking thumbing biting
creeping tinkering lagging pinning dancing
cashing damning airing finding fencing
patching sending blocking receiving tugging
coming proving blotting naming tucking
summing fighting sleeping drinking picking
spinning spitting reaping stinking gagging
sinning prancing catching standing hearing
Task: Use the sentence cards in the same manner as you did for the word-level intelligibility
task. Add the number of sentences correctly interpreted and score using the following grades.
Check the most applicable option
Ten sentences correctly interpreted by the therapist, with speech easily intelligible.
Ten sentences correctly interpreted by the speech therapist, but therapist had to use
particular care in listening and interpreting what was heard.
Seven to nine sentences interpreted correctly.
Five sentences interpreted correctly.
Two or less sentences interpreted correctly.

Rating Scale for PACE Interaction (Davis, 1980)
Score 5 Message conveyed on first attempt. There are two definitions of best performance: (1) message
is conveyed by client with combined active participation of the client’s sending behavior and the
clinician’s ability to make an appropriate interpretation from information given by the client,
acknowledging the usual contribution of the receiver in any conversation or (2) a specified
required completeness of the client’s sending behavior in terms of number of concepts conveyed,
minimizing the clinician’s filling in of missing parts and placing a greater burden on the client
for the communication.
Score 4 Message conveyed as above (either 1 or 2) after general feedback from the clinician indicating
the first attempt had not been completely understood. This includes the clinician’s repeating the
client’s attempt in a questioning fashion.
Score 3 Message conveyed as above (either 1 or 2) after specific feedback. This feedback reflects the
clinician’s assuming an active role as receiver in determining the client’s message, either by
proposing hypotheses about the messages (topic, semantic relations) or by suggesting an
additional channel be used (“Show me” “Tell me anything about it”). Clinicians sometimes risk
pursuing this level of feedback too long, especially having ignored that the message was
conveyed. Because of the varied types and amounts of feedback possible, this category might be
differentiated into a greater number of scale points in order to make the scale more sensitive to
efficiency.
Score 2 Message partially conveyed by the client, only after general (point 4) and specific (point 3)
feedback have been attempted.
Score 1 Message not conveyed appropriately despite efforts by the patient and clinician reflected in
points 4 and 3.
Score 0 Client does not attempt to convey the message.
Score “U” Unscorable response, usually because one or more of the principles of PACE were violated in the
interaction.

PACE Instructions
Basic Overview
The patient and partner take turns exchanging new information, as in a natural conversational
context. Conversations should be personally-relevant to the patient. The receiver provides natural
feedback aimed at problem-solving the sender’s message (i.e., co-constructing the conversation).
In other words, the receiver must make educated guesses on the sender’s message that simulates
a natural conversation. The turn ends when the sender’s message is conveyed, not when a pre-
determined linguistic form is produced (Davis, 2005). In essence, emphasis is placed on the
transaction of information.
Four Principles of PACE
(1) Equal participation: the clinician and patient participate equally as senders and receivers of
messages.
This is done by taking turns sending messages.
When the clinician sends a message, the patient can verbalize in a different role, that of
receiver.
(2) New information: There is an exchange of new information between the clinician and the
patient.
This is done by the sender’s keeping his message (picture, printed word) from view of
the receiver. Usually, a stack of message stimuli is face-down on the table, and the
participants take turns drawing from the stack.
It is difficult to maintain genuinely; so, the clinician must minimize familiarity with the
message stimuli. When the clinician is the receiver, s/he should give general feedback
first in order to avoid responses based on familiarity with the stimuli.
(3) Free choice of channels: The patient has a free choice as to which communicative channels
(modalities) s/he may use to convey new information.
The patient, when sending, may use any single channel or channels in combination.
The clinician does not direct the patient to use any particular channel. The clinician,
when sending, can model the communicative value of channels which the patient may
not be choosing to use.
This is a process of self-discovery by the patient as to his or her communicative options.
(4) Natural feedback: Feedback is provided by the clinician, when receiving, in response to the
patient’s success in conveying a message.
The clinician responds first to communicative adequacy.
Once the patient realizes the message is conveyed, the clinician may pursue linguistic
adequacy for the same message. The clinician may encourage revisions or repairs or
may provide standard cues. The latter can be done only because the clinician has
understood the patient’s message. Time to pursue linguistic adequacy is taken usually
only when the patient wants to improve a verbal attempt.

In giving feedback for determining the patient’s message, the clinician proceeds in a
sequence from general to specific feedback, corresponding to scale points on a rating
scale.
Wilcox, M.J., and Davis, G.A., PACE: Promoting Aphasics’ Communicative Effectiveness.
Activity Ideas
Descriptive picture task
Place a stack of picture cards face down on the table. The patient and partner take turns picking
up a picture card and describing it to the other person. Example picture cards are attached to this
document; however please use pictures that are more applicable to the individual client.
Conversational cards
The patient and partner will take turns drawing conversational cards from a stack. The patient
and partner take turns discussing the topic on the card, exchanging new information to the other
person. Example conversational cards are attached to this document.
Story sharing
Patient and partner will take turns sharing stories about their childhoods. This task is
unstructured, increasing the complexity of the task.



Find out what television program
your partner watched last evening.
Extend the conversation by adding
two more comments of your own.
Find out about what your partner is
doing for this upcoming holiday.
Extend the conversation by adding
two more comments of your own.
Find out what vacations or road
trips your partner gone on or is
planning. Extend the conversation
by adding two more comments of
your own.
Find out where your partner grocery
shops. Extend the conversation by
talking about where you usually
grocery shop and why.
Find out what important
information your partner heard or
watched in the news this week.
Extend the conversation add two
more comments of your own.
Find out about a restaurant at which
your partner has eaten. Extend the
conversation by asking about the
food and environment. Also, share
information about a restaurant you
like.
Find out if your partner has attended
or will be attending a wedding this
year. Extend the conversation by
sharing information about a
wedding you have attended.
Find out about a home project your
partner is working on this summer,
either in the house, garage, or yard.
Extend the conversation by sharing
information about a project on
which you are working.

Find out about a grandchild, niece,
nephew, or other young person with
whom your partner is close. Extend
the conversation by sharing a story
about a young person with whom
you are close.
Find out your partner’s plans for the
weekend. Extend the conversation
by sharing your plans for the
weekend.
Find out if your partner attends any
social, church, or other type of
group during the week. Extend the
conversation by sharing information
about a group you have attended.
Find out about a special recipe your
partner has used in the past. Extend
the conversation by describing a
recipe with which you have had
good luck.