Embed Size (px)
Citation preview

Morphometric Analysis of Pediatric andNonhyperplastic Prostate Glands: Evidence That
BPH Is Not a Unique Stromal Process
Ellen Shapiro,1* Victor Hartanto,1 Elizabeth J. Perlman,2 Rui Tang,1 Bo Wang,1and Herbert Lepor1
1Department of Urology, New York University School of Medicine, New York, New York2Department of Pathology, Johns Hopkins Hospital, Baltimore, Maryland
BACKGROUND. Although quantitative morphometry of benign prostatic hyperplasia (BPH)has been described, there is a paucity of information on the morphometry of the nonhyper-plastic prostate. This study determines the histologic composition of prostates obtained frommales, ages 2 days to 40 years, in order to provide insights into the morphometry of the‘‘normal’’ gland.METHODS. The histologic composition of 45 prostates was obtained from autopsies of maleswith age groups stratified to reflect the neonatal, childhood, peripubertal, adolescent, andyoung adult periods. Double immunoenzymatic staining and computer image analysis wereused to determine the mean area densities of the smooth muscle (SM), connective tissue (CT),glandular epithelium (E), and lumen (L).RESULTS. A progressive decrease in SM area density throughout childhood, prepuberty, andpuberty was seen. The density of SM significantly increased following puberty and through-out adolescence and early adulthood. There was a concomitant increase in CT from theneonatal period throughout childhood, prepuberty, and puberty, and a decrease after pubertyand throughout adolescence and early adulthood. Since the changes in SM and CT wereinversely related, the percent contribution of the stromal compartment to the total glandremained constant.CONCLUSIONS. The stromal to epithelial ratio remains constant from birth to age 40 innonhyperplastic glands and is similar to the ratios in asymptomatic and symptomatic BPHtissues. Prostate 33:177–182, 1997. © 1997 Wiley-Liss, Inc.
KEY WORDS: histology; smooth muscle; quantitative morphometry; prostate
INTRODUCTION
Benign prostatic hyperplasia (BPH) represents be-nign growth of the prostate that spontaneously devel-ops in the aging male population [1]. Histologic evi-dence of BPH is rarely observed in males prior to thefifth decade of life. The development of BPH is anunavoidable phenomenon for the majority of agingmales, since 90% of octogenarians have evidence ofmicroscopic BPH. BPH may result in macroscopic en-largement of the prostate and bladder outlet obstruc-tion. The pathogenesis of BPH is poorly understood.Aging and functioning testes are required for the de-velopment of BPH [2]. McNeal [3] has proposed thatBPH represents a ‘‘reawakening’’ of the embryonic
and inductive potential of prostatic stroma. Growthfactors may also be responsible for initiating cellularproliferation [4].
Berry et al. [2] determined the relationship betweenage and prostate volume, based upon an extensivereview of previously reported autopsy observations.
Victor Hartanto, M.D., is currently at the Department of Surgery,UMDNJ-Robert Woods Johnson Medical School, New Bruns-wick, NJ.*Correspondence to: Ellen Shapiro, M.D., Department of Urology,New York University Medical Center, 540 First Ave., Suite 10U,New York, NY 10016.Received 30 July 1996; Accepted 26 November 1996
The Prostate 33:177–182 (1997)
© 1997 Wiley-Liss, Inc.

Prostatic growth occurs throughout life. Approxi-mately 30% of total prostate growth occurs betweenthe fifth and ninth decades of life. Therefore, the ma-jority of total prostatic growth is not due to BPH.
Although the quantitative morphometry of humanBPH has been well-described [5–8], there is a paucityof descriptive information on the morphometry of thenonhyperplastic prostate. The present study was de-signed to determine the histologic composition ofprostates obtained from males between ages 2 days to40 years in order to provide insights into the mor-phometry of the ‘‘normal’’ gland. The majority ofspecimens were representative of the pediatric agerange. We evaluated 5 prostates from men ranging inage from 23–40 years in order to characterize the cel-lular composition of the adult nonhyperplastic pros-tate. The age groups were stratified to reflect the neo-natal, childhood, peripubertal, adolescent, youngadult, and nonhyperplastic adult periods of develop-ment. Determining the histologic components of theprostate using double immunoenzymatic staining andcomputer-assisted color image analysis has providedimportant insights into the commonality of age-dependent composition of prostatic growth through-out life.
MATERIALS AND METHODS
Patient Selection
Prostate specimens were obtained from randomlyselected autopsy specimens of 45 males between ages2 days to 40 years. Age ranges for subjects weredivided into group I, 0–12 months (mean, 14 weeks);group II, 1–8 years (mean, 4 years); group III, 9–14 years (mean, 11.9 years); group IV, 15–20 years(mean, 17 years); and group V, 21–40 years (mean,28 years). The available clinical data were reviewedon each subject. None of the subjects had a historyof an intersex condition or an endocrine disorder thatwould affect the normal development of the prostate.None of the subjects were receiving medicationswhich would affect the prostate. The typical causesof death in most of these patients included congeni-tal cardiac anomalies, sudden infant death syndrome,acute pulmonary etiologies, and trauma. None ofthe patients had cancer or other chronic diseases.The prostate specimens were stained with hema-toxylin and eosin and reviewed by a pathologist.The gross and qualitative microscopic diagnosis was‘‘no pathologic condition’’ or normal for all speci-mens.
Tissue Processing and Staining
Prostatic tissues embedded in paraffin wax weresectioned (4 mM) using the Leitz 1512 Rotary Micro-tome (Wetzlar, Germany). The precise regional orien-tation of the prostatic tissues was unknown, since thespecimens were obtained from archival sources. Ow-ing to the small size of many of the prostates, thetissue block was felt to be representative of the wholegland. The tissues were deparaffinized with xyleneand rehydrated with graded series of ethanol. The de-paraffinized tissue sections were stained using theuniversal Dako Double-Stain Kit System 40 (Dako,Carpinteria, CA). The kit is designed to simulta-neously detect two different tissue antigens usingdouble-immunoenzymatic staining with peroxidase-antiperoxidase (PAP) and alkaline phosphatase-antialkaline phosphatase (APAAP) techniques. Mouseanti-actin (Dako, Carpinteria, CA) and rabbit anti-human prostatic acid phosphatase (PSAP) (Dako,Carpinteria, CA) were bound to smooth muscle andprostatic epithelium, respectively. The optimal dilu-tions for anti-actin and anti-human PSAP were 1:25and 1:200, respectively. The staining procedure in-cluded incubations with hydrogen peroxide andblocking serum to quench endogenous peroxidase ac-tivity and reduce nonspecific staining. Tissue sectionswere incubated with the following reagents: rabbitanti-human PSAP, mouse anti-actin, and the providedrabbit APAAP immune complex and mouse PAP im-mune complex. The mouse anti-actin and mouse PAPimmune complexes were linked with a secondary rab-bit antibody. Alkaline phosphatase activity was devel-oped with the chromogen Fast Red (DAKO Corpora-tion, Carpinteria, CA). The rabbit anti-human PSAPand the rabbit APAAP immune complex were linkedwith a secondary mouse antibody. The peroxidase an-tibody was developed with diamino benzidine (DAB)and peroxide. The smooth muscle stained red, and theepithelium stained dark brown.
Computer-Assisted Quantitative ColorImage Analysis
The stained tissue sections were viewed under aWild-Leitz Microscope using a 6.3 Planafluotar objec-tive and a Variolum adapter under 250× magnifica-tion. A high-resolution JVC color video camera head(TK-870U) captured the image of the histologic sec-tion, which was displayed on a Sony RGB 12-inchcolor monitor (Dell Computer Corp., Austin, TX). Theimage was simultaneously digitized using the ATVista inside the Dell System 220 personal computer.The automated analysis was performed by the Bio-quant Image Analysis System (BQ MEG IV-Vista,
178 Shapiro et al.

R & M Biometrics, Nashville, TN). The BQ MEG IV-Vista is a color image analysis system which discrimi-nates color differences of stained tissue sections. Thethresholds were set to identify the tissue componentsof the prostate. The area densities corresponding toeach of these tissue components were calculated foreach full screen of the Sony RGB color monitor. Atleast 30 different fields were examined from each tis-sue section. The mean percentages of smooth muscle(SM), connective tissue (CT), glandular epithelium (E),and lumen (L) were determined from the tissue sec-tions obtained from the 45 males.
Statistical Analysis
The Bonferroni multiple range comparison test,performed after analysis for variance, was used tocompare differences between percent smooth muscle,connective tissue, and stromal:epithelial ratio for thefive different age groups.
RESULTS
The mean area densities of prostate smooth muscle,connective tissue, glandular epithelium, and glandu-lar lumen were determined and are shown in Table I.Groups I–V correspond to neonatal, childhood, peri-pubertal, adolescent, and young adult. The mean areadensities of prostate smooth muscle, connective tissue,glandular epithelium, and glandular lumen were de-termined from stained tissue sections using computer-assisted color image analysis. The between-group dif-ferences that are statistically significant are shown inTable I. The density of prostatic smooth muscle wasage-group-dependent. Prostate smooth muscle com-prised 49% of area density of the gland during theneonatal period. A progressive and statistically sig-nificant decline in smooth muscle was observedthroughout childhood, prepuberty, and puberty. Thedensity of smooth muscle significantly increased fol-lowing puberty and throughout adolescence and earlyadulthood. The density of connective tissue was alsoage-group-dependent and inversely related to thedensity of smooth muscle. Prostate connective tissue
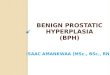
comprised 31% of the neonatal gland. A progressiveincrease in connective tissue was observed throughoutchildhood, prepuberty, and puberty. The density ofconnective tissue significantly decreased followingpuberty and throughout adolescence and early adult-hood. The age-dependent changes in smooth muscleand connective tissue were inversely related, therebymaintaining a constant stromal compartment densitythroughout these periods of development (Fig. 1). Nosignificant changes were seen in the percent area den-sities of the epithelium within any of the age groups.A progressive increase in the size of the glandularlumen was demonstrated following the onset of pu-berty.
DISCUSSION
There exists a paucity of literature on the prostate ofthe neonate, growing child, peripubertal male, andadolescent male. In 1951, Andrews [9] reported on thehistology of the prepubertal prostate. He observedthat from birth to the end of the first month, no sig-nificant changes occurred in the gland; however, be-tween the first and fourth month of life, a gradualregression in the epithelium occurred. The only othernotable change was related to the size of the prostate.Between the fourth month and puberty, the total in-crease in prostate size was attributed to an increase instroma. These observations were based entirely onqualitative examination of stained prostatic tissue sec-tions.
The present study represents the first comprehen-sive evaluation of the histologic changes in the humannonhyperplastic prostate gland occurring from birththrough early adulthood. Using the technique ofdouble immunoenzymatic staining and computer-assisted color image analysis, we quantified the histo-logic components of the prostates of males rangingfrom 2 days to 40 years of age. The advantage of thistechnique is that the mean area densities of the smoothmuscle, connective tissue, glandular epithelium, andglandular lumen are quantified. One of the potentialpitfalls of the study design is that the prostatic tissue
TABLE 1. Percent Area Density of the Histologic Components of the Prostate
Group (age) No. of patients % SM % CT % E % L Stroma epithelium
I (0–12 months) 9 48.9 ± 1.2 30.7 ± 2.0 15.9 ± 1.2 4.6 ± 0.4 5.5 ± 0.9II (>1–8 years) 14 41.1 ± 0.6 38.4 ± 0.9 14.7 ± 0.1 5.8 ± 0.4 5.8 ± 0.5
III (9–14 years) 7 32.7 ± 2.9 44.4 ± 5.2 16.7 ± 1.9 6.0 ± 1.5 5.4 ± 1.2IV (15–20 years) 10 42.0 ± 2.7 29.3 ± 3.1 19.3 ± 1.6 9.6 ± 1.3 4.1 ± 0.5V (>20 years) 5 52.4 ± 2.9 26.4 ± 2.3 14.6 ± 2.0 6.6 ± 1.9 6.3 ± 1.7
*P < 0.05.
Pediatric Nonhyperplastic Prostate Morphometry 179

available for analysis represented random sampling ofthe whole prostate specimen. Therefore, regional dif-ferences were not evaluated.
The density of prostatic smooth muscle was great-est in the neonatal group. The density of smoothmuscle comprising the gland progressively decreasedbetween the neonatal and childhood groups and thechildhood and peripubertal groups. The density ofsmooth muscle in the peripubertal group was 67% ofthat of the neonatal group. A significant increase indensity of smooth muscle was observed between theperipubertal and adolescent groups. Since reciprocalage-group-dependent changes were observed for thearea densities of prostatic connective tissue, the per-cent area density of the stromal compartment was notage-dependent. A small but significant increase in lu-men area density was demonstrated between groups Iand IV. The present morphometric study demon-strates definite age-group-dependent changes in thecellular composition of the stromal compartment ofthe prostate. These specific differences would not havebeen observed if only the stromal and epithelial com-partments had been analyzed.
Zirkin and Strandberg [10] reported on the age-dependent histologic composition of the canine pros-tate. The mean ages of pre-BPH canine groups I and IIwere 0.7 and 1.3 years, respectively. Mean prostateweight was 2-fold greater in group II. The area densityof stroma and epithelium in these groups was not sig-nificantly different despite the overall increase in pros-tate size. In these studies, the density of connectivetissue and smooth muscle volume were not indepen-
dently quantified. Although the canine and humanprostate undergo significant non-BPH growth duringmaturation, the overall proportion of stroma to epi-thelium in both species remains constant.
The present study demonstrated age-relatedchanges in the area density of prostatic smooth musclethat temporally parallel the postnatal testosteronesurge and the rise in testosterone at the onset of pu-berty. The cellular composition of the stromal com-partment may be dependent upon the hormonal mi-lieu. Cunha [11] has demonstrated that only thestromal component of the embryonic prostate is tes-tosterone-dependent. The nonembryonic epitheliumhas been shown to be androgen-dependent in animalmodels and in the aging human male. It is interestingthat epithelial volume remains relatively constant inall age groups despite significant changes in serumtestosterone levels during these periods of develop-ment [12]. The small but significant increase in lumi-nal volume may represent increased secretory activityin the postpubertal male prostate.
We previously reported [7] that the development ofclinical BPH is dependent upon the histologic compo-sition of the prostate. This was based on the findingthat the ratio of stroma to epithelium was greatest inthose individuals with clinical BPH (4.6) compared tothose patients with asymptomatic BPH (2.7) [7]. Thedensities of smooth muscle and connective tissue werenot determined, since the morphometric methods de-pended on grey-scale densities using hematoxylin andeosin-stained slides. The stromal compartment was in-directly determined since only the lumen, glandular,
Fig. 1. Bar graphs illustrating smooth muscle(SM), connective tissue (CT), and their combinedcomponents or stromal compartments of theprostate glands in groups I–V.
180 Shapiro et al.

and glandular plus stromal densities could be quanti-fied. Using these values, the various histologic com-ponents were calculated in the different BPH speci-mens.
More recent studies have utilized computer-assisted color image analysis to determine the histo-logic components of symptomatic and asymptomaticBPH specimens [8,13]. One of these studies examinedthe stromal elements in specimens from patients withsymptomatic BPH and suggested that the severity ofbladder outlet obstruction is dependent upon the den-sity of smooth muscle [8]. The stromal compartmentcomprised 78% of the total prostate volume, and thestromal-to-epithelial ratio was 6.5:1. Smooth muscleaccounted for 39% of the area density of these pros-tates.
In another study of BPH specimens derived fromcystoprostatectomy specimens using double immuno-enzymatic staining and color image analysis, the stro-mal compartment comprised 80% of the total prostate,and the stromal-to-epithelial ratio was 6:1. Smoothmuscle accounted for 52% of the area density of theprostate.
These studies show that the stromal compartmentin symptomatic and asymptomatic BPH is similar. Theepithelial volume is similar in symptomatic andasymptomatic BPH specimens except for unusuallylarge-sized prostates, where the glandular volume isrelatively high.
Historically, we have reported on numerous occa-sions that the mean stromal-to-epithelial ratio in thehyperplastic prostate is approximately 5:1, which isconsistent with the morphometric studies of Bartsch etal. [14] on BPH prostates. Bartsch et al. [14] also re-ported that in 6 men between ages 20–29 years whounderwent perineal prostatic biopsy, the stromal com-partment comprised only 45% of the gland and thestromal-to-epithelial ratio was 2:1. Based on this singlestudy with a very small sample size, it has been as-sumed that the cellular compositions of BPH and non-BPH were significantly different, and that establishedBPH is a ‘‘stromal disease.’’ There have been no otherreports in the literature to substantiate or refute thesefindings in non-BPH tissues.
The present study and our previous prostatic mor-phometric studies provide compelling evidence thatthe stromal-to-epithelial ratio of non-BPH and BPHare similar. Zirkin and Strandberg [10] observed thatthe differences between the area density of stroma toepithelium in non-BPH and BPH in the canine aresubtle. In man, non-BPH prostate is primarily periph-eral zone. We recently observed that the stromal-to-epithelial ratios of the peripheral zone and transitionalzone are relatively similar [15]. Since the cellular com-
position of BPH is similar to that of the neonatal pros-tate, it is conceivable that BPH represents an inductionof embryonic-like development [3]. Since the prostategland is primarily stromal, differences other than rela-tive proportion of stroma and epithelium and the his-tologic composition of the prostate may be responsiblefor the symptoms of clinical BPH.
CONCLUSIONS
Although the stromal to epithelial ratio of the pros-tate remains constant in males between ages 0–20years, the proportion of smooth muscle and connec-tive tissue is variable. The factors that cause changes inthe composition of the stromal compartment are un-known. The changes that occur in the smooth muscleand connective tissue appear to be reciprocal. Thestromal compartment maintains its overall contribu-tion to the total gland volume despite significantchanges in prostatic weight and hormonal milieuthroughout life. Both BPH and non-BPH prostate tis-sues are comprised of approximately 80% stroma.Since the stromal-to-epithelial ratios are similar in pe-diatric, adult non-BPH, and adult BPH tissues, factorsother than histologic composition must contribute tothe pathophysiology of clinical symptoms associatedwith BPH.
REFERENCES
1. Walsh PC: Benign prostatic hyperplasia. In Walsh PC, Retik AB,Stamey TA, Vaughan ED (eds): ‘‘Campbell’s Urology,’’ 6th ed.Philadelphia: W.B. Saunders, 1992:1007–1022.
2. Berry SJ, Coffey DS, Walsh PC, Ewing LL: The development ofhuman benign prostatic hyperplasia with age. J Urol 1984;132:474–479.
3. McNeal J: Pathology of benign prostatic hyperplasia: Insightsinto etiology. Urol Clin North Am 1990;17:477.
4. Steiner MS: Review of peptide growth factors in benign pros-tatic hyperplasia and urologic malignancy. J Urol 1995;153:1085–1093.
5. Shapiro E, Hartanto V, Lepor H: Quantifying the smooth musclecontent of the prostate using double immunoenzymatic stainingand color assisted image analysis. J Urol 1992;147:1167–1170.
6. Shapiro E, Hartanto V, Lepor H: Anti-desmin vs. anti-actin forquantifying the area density of prostate smooth muscle. Prostate1992;20:259–267.
7. Shapiro E, Becich MJ, Hartanto V, Lepor H: The relative pro-portion of stromal and epithelial hyperplasia is related to thedevelopment of symptomatic benign prostate hyperplasia. JUrol 1992;147:1293–1297.
8. Shapiro E, Hartanto V, Lepor H: The response to alpha blockadein benign prostatic hyperplasia is related to the percent areadensity of prostate smooth muscle. Prostate 1992;21:297–307.
9. Andrews GS: The histology of the human fetal and prepubertalprostates. J Anat 1951;85:44–54.
Pediatric Nonhyperplastic Prostate Morphometry 181

10. Zirkin BR, Strandberg JD: Quantitative changes in the morphol-ogy of the aging canine prostate. Anat Rec 1984;208:207–214.
11. Cunha GR: The role of androgens in the epithelio-mesenchymalinteractions involved in prostatic morphogenesis in embryonicmice. Anat Rec 1973;175:87–96.
12. Griffin JE, Nilson JD: The testis. In Bondy PK, Rosenberg LE(eds): ‘‘Metabolic Control and Disease,’’ Philadelphia: W.B.Saunders, 1980:1535–1579.
13. Lepor H, Shapiro E, Wang Bo, Liang YC: Comparison of thecellular composition of benign prostatic hyperplasia in Chineseand Caucasian-American men. Urology 1992;47:38–42.
14. Bartsch G, Muller HR, Oberholzer M, Rohr HP: Light micro-scopic stereological analysis of the normal human prostate andof benign prostatic hyperplasia. J Urol 1979;122:487–491.
15. Lepor H, Wang Bo, Shapiro E: Relationship between prostaticepithelial volume and serum prostate specific antigen levels.Urology 1994;44:199–205.
182 Shapiro et al.