Embed Size (px)
Citation preview

Bryan Bednarz, Ph.D.
Monte Carlo Methods in Proton Therapy
Research Fellow, Massachusetts General Hospital and Harvard Medical School

Overview
• Basic Monte Carlo Theory
• Proton Transport
• Modeling the Proton Beam Treatment Head
• Patient Dose Calculations
• Why Monte Carlo?
What is Monte Carlo?The Monte Carlo technique is a computational tool that samples from known probability distributions to determine the average behavior of a system. It is used in radiotherapy to improve our understanding of the production, transport and the ultimate fate of therapeutic radiation. The goal of this lecture is to introduce the basic theoretical framework behind the Monte Carlo technique and to provide demonstrations on the use of this powerful technique to solve proton therapy problems.
Monte Carlo Casino, Las Vegas NV

Sampling
The idea of using random sampling to solve problems in mathematics was first proposed by Georges‐Louis Leclerc, Comte de Buffon and was first utilized by Pierre‐Simon Laplace. Laplace solved for the value of πby randomly dropping needles onto a wood floor. We will “modernize”this problem by determining the value of π by playing darts.

Sampling
Hit
Miss
P1: Estimating π using darts.

Sampling
0 ≤ x ≤ L0 ≤ y ≤ LS:
x
y
0 L
L
0
Sampling Space
Probability Density Function
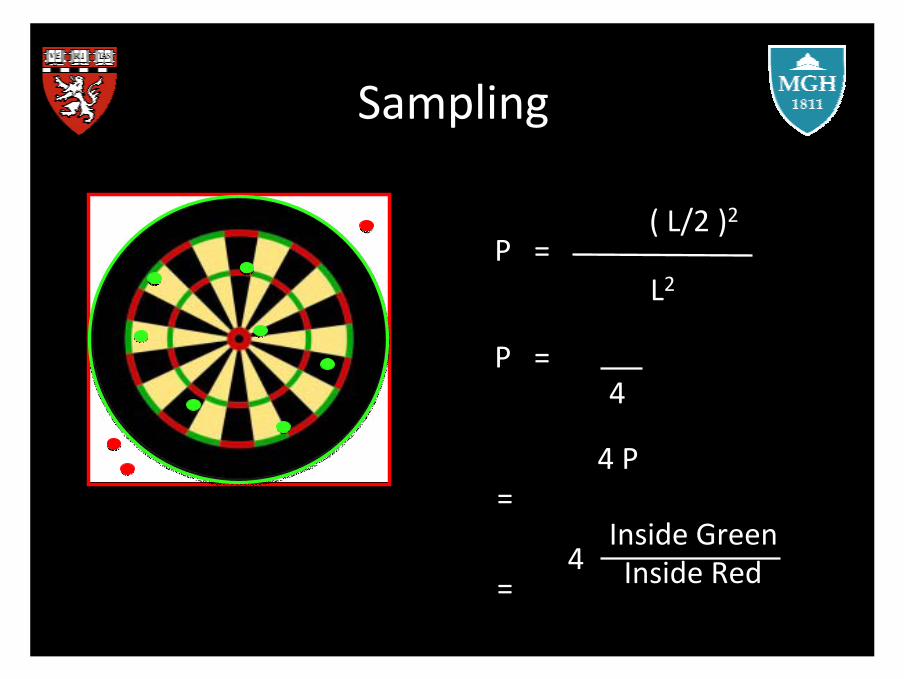
P = Inside GreenInside Red
P = π ( L/2 )2
L2
Sampling
P = π ( L/2 )2
L2
P = π
4
π=
4 P
π=
Inside GreenInside Red4

SamplingAt the very least we need to throw 30 darts to be able to estimate the value of π, as required by the Law of Large Numbers. However, the uncertainty in our estimate is proportional to the square root of the total number of darts we throw. Therefore, the more darts we throw the more accurate our estimate becomes. Fortunately, (for our arms sake) we have computers that can sample millions of throws per minute.

Proton TransportProtons may undergo one million interactions per cm in a medium giving rise to extremely complex transport kinematics. Luckily, computers today are capable of handling such complexity. In most Monte Carlo codes, proton transport is modeled by discretizing the path of a proton into a series of small steps. Below is a simple representation of how protons are transported in Monte Carlo.

Proton Transport
1. Stopping
2. Coulomb Scattering
3. Nuclear Interactions
The transport of protons is governed by three main processes:

StoppingProtons lose their energy by collisions with atomic electrons (ignoring elastic EM collisions with atomic nuclei and nuclear interactions with atomic nuclei). In Monte Carlo, the energy loss is determined for each step using tabulated restricted stopping power values (viz Bethe Bloch equation). Therefore, energy loss is deposited locally along the proton path unless the energy transfer to an electron is greater than a threshold value.
0.1 cm
water bone

ScatteringAs protons slow down they also scatter, mainly by interactions with atomic nuclei rather than electrons. Since the deflection angle of single scattering events is very small, multiple scattering theories provide us with probability density functions that represent the net result of several single scattering events. Therefore, we can sample these distributions to determine the scattering angle at the end of each step.
water bone
θ

Nuclear InteractionsAt proton therapy energies some 20% of protons undergo a nuclearinteraction before stopping. These interactions can be elastic or inelastic. The result of nuclear interactions is a loss of proton fluence, generation of neutrons and other particles, and short‐lived radioactive isotopes. A good Monte Carlo code will account for the important derivatives of nuclear interactions. The probability of these interactions occurring is determined by measured cross section data or nuclear models.

Modeling the Proton Beam Treatment Head
The next slides will cover the modeling of the treatment head in Monte Carlo using the MGH (IBA system) as an example.

Modeling the Proton Beam Treatment Head
Passive Scattered Proton Therapy Beam Scanning
Be aware of the “garbage in = garbage out” principle when modeling the treatment head. There are almost 500 components in the treatment head that need to be considered. Even slight disparities between the model and the actual treatment head may result in undesirable dose distributions.

Beam Characteristics at Entrance
1. Beam size (Measured)2. Beam angular spread (Manufacturer) 3. Beam energy (Treatment Control System)4. Beam energy spread (Manufacturer, Measured)

Double Scattering System
First Scatterer
Second Scatterer
FS
SS
Lead
Lexan
FS are made using cylindrical disks and SS are made using polycones (or multiple cones).

Modulator Wheel
MW
The modulator wheel is defined by a series of cylindrical steps.

Beam Current ModulationDue to the strong dependence of scattering on proton energy the physical dimensions and materials of a track can only be optimized for a limited amount of ranges. However, it is possible to modulate the beam intensity in synchronization with the modulator wheel rotation to further optimize the beam weights allowing for improved uniformity in the dose distributions. This is called beam current modulation.
w1
w2
w3w4w5
Ni = NT
wi
sum(wi)
The number of protons to simulate onthe ith step is given by:
where NT is the total number of protons simulated and wi is the beam current weight defined by the beam current modulation function.
Geant4 allows for geometry changes during middle of run using C++ architecture.

Other Components
JAWS
IC
SNOUT
The snout serves to reduce the air gap between the treatment head and patient and to attach patient specific devices.
Ion chamber is used for monitor unit calculations
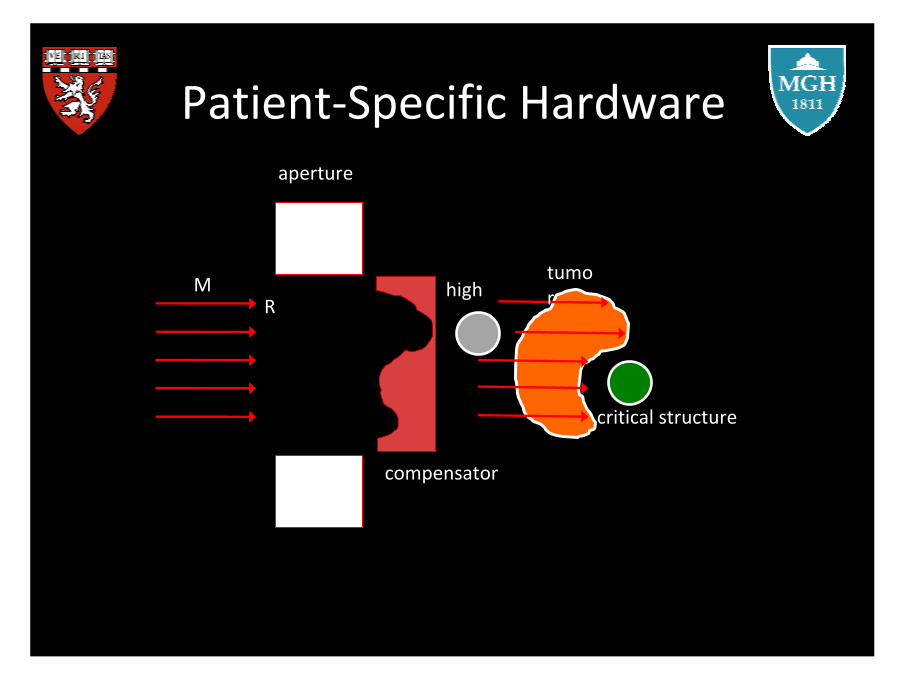
Patient‐Specific Hardware
high ρ
critical structure
RM
aperture
compensator
tumor

Patient‐Specific Hardware
To produce patient‐specific hardware in Monte Carlo we read in files from the machine milling database.
Aperture Compensator

4D Monte Carlo
Courtesy of Jungwook Shin

Patient Dose Calculations
HU ρ
M?
For each voxel on the CT grid, the CT number has to be converted to density (ρ) and material composition (M). Typically, the number of densities is equivalent to the the number of CT numbers in the scan. Tissue material compositions are defined for a group of CT numbers (5‐30). There are different schemes to do this, but at MGH we use the W. Schneider method.

Patient Dose Calculations

Relative Stopping Power
Most treatment planning systems convert CT number to relative stopping powers. Thus, when performing comparative studies with treatment plans it is important that the relative stopping power in the planning system matches what is calculated with Monte Carlo by using this correction factor.

Absolute Dose Calculations
For proton dose calculations, there are two ways of simulating absolute dose.
1. Simulate ionization chamber output charge when tracking particles through the treatment nozzle. Exact model of the treatment head including ionization chambers is required. Typically requires a large number of histories.
1. Relate the number of protons at nozzle entrance to the dose in an SOBP in water. Typically, the dose is averaged over a part of the SOBP. This method is equivalent to a direct output measurement.

Uncertainties
It is important to always consider the uncertainties associated with Monte Carlo dose calculations.
1. Physics cross sections (models versus measurements?)2. Tracking options (beware of defaults)3. Modeling uncertainties (Im, ρ, position)
Commissioning results for one of our treatment nozzles.

The MGH FrameworkPatient
DatabasePatient
Database
Treatment Planning
(FOCUS/Xio)
Treatment Planning
(FOCUS/Xio)
Treatment Control System
Treatment Head Geometry and
Beam Setup
Treatment Head Geometry and
Beam Setup
Patient Geometry
Patient Geometry
Patient Setup
Patient Setup
Phase Space Calculation
Phase Space Calculation
Patient Dose Calculation
Patient Dose Calculation
HU Conversion
HU Conversion
Beam Current Modulation
Beam Current Modulation
Passive ScatteringProton Therapy
Pencil beam distribution and
parameters
Pencil beam distribution and
parameters
Beam Scanning
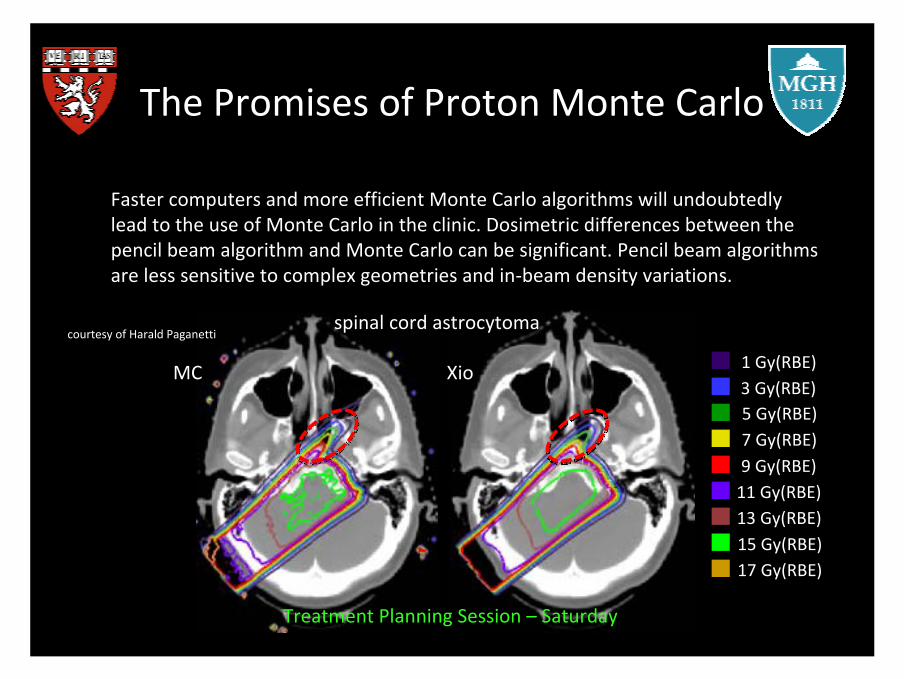
The Promises of Proton Monte Carlo
Faster computers and more efficient Monte Carlo algorithms will undoubtedly lead to the use of Monte Carlo in the clinic. Dosimetric differences between the pencil beam algorithm and Monte Carlo can be significant. Pencil beam algorithms are less sensitive to complex geometries and in‐beam density variations.
1 Gy(RBE)3 Gy(RBE)5 Gy(RBE)7 Gy(RBE)9 Gy(RBE)
11 Gy(RBE)13 Gy(RBE)15 Gy(RBE)17 Gy(RBE)
spinal cord astrocytomacourtesy of Harald Paganetti
Treatment Planning Session – Saturday
MC Xio

The Promises of Proton Monte Carlo
Traditionally dose in radiation therapy is reported as water‐equivalent dose (dose‐to‐water) since treatment planning systems calculate dose by modeling physics relative to water. Furthermore QA is done in water. However, it has been found that based on the mean dose to a structure, dose to water can be higher by almost 10% compared to dose to tissue in bony anatomy. Soft tissue differences are on the order of 2%.
courtesy of Harald Paganetti

The Promises of Proton Monte Carlo
Nuclear interactions in the patient cause the formation of positron emitters that can be imaged with post‐irradiation positron emission tomography. It is the aim of current research to determine whether the PET signal from a patient can be used to verify the beam range. Monte Carlo can be used to generate a theoretical PET image based on the prescribed radiation field.
dose distribution PET distribution
courtesy of Samuel Espana Palomares

The Promises of Proton Monte Carlo
courtesy of Uwe Oelfke
In the relevant energy range of protons, one can assume a monotone increase of RBE with increasing LET. Thus it may be feasible to characterize physics related RBE effects using LET. Distributions of LET can be simulated in the patient using Monte Carlo.
LETDose

The Promises of Proton Monte Carlo
courtesy of Basit Athar, George Xu and Wes Bolch
Neutrons produced in the treatment head and patient can deposit unwanted dose to healthy tissue outside of the treatment volume. Monte Carlo can help quantify this unwanted neutron dose in order to estimate the probability of inducing late effects, most notably second primary cancers.
UF PhantomsVIP man
p+n0
Summary
Proton Monte Carlo has played and will continue to play a vital role in both the clinical and research setting. I believe that we have reached a crossroad in regard to the implementation of Monte Carlo in treatment planning. It seems that the current culture will facilitate a gradual implementation of this powerful tool into the planning architecture. There are some of us, however, who strongly believe that Monte Carlo is indeed ready for primetime, and should be considered a key upgrade in the next commercially available treatment planning systems. This is particularly relevant as our field moves toward adaptive radiation therapy.

Acknowledgements
• Harald Paganetti
• Thomas Bortfeld
• Dr. Elichi Takada and PTCOG Japan

References
1. Paganetti, H. and T. Bortfeld, Proton Therapy. In: New Technologies in Radiation Oncology; Eds. Schlegel, W.; Bortfeld, T.; Grosu, A.L.; Springer, ISBN 3‐540‐00321‐5, 2005.3. Paganetti, H., et al., Accurate Monte Carlo for nozzle design, commissioning, and quality assurance in proton therapy. Medical Physics, 2004. 31: p. 2107‐2118.4. Hsi, W.C., et al., Energy spectrum control for modulated proton beams. Med Phys, 2009. 36(6): p. 2297‐308.5. Paganetti, H., et al., Clinical implementation of full Monte Carlo dose calculation in proton beam therapy. Phys Med Biol, 2008. 53(17): p. 4825‐53.6. Stankovskiy, A., et al., Monte Carlo modelling of the treatment line of the Proton Therapy Center in Orsay. Phys Med Biol, 2009. 54(8): p. 2377‐94.7. Titt, U., et al., Assessment of the accuracy of an MCNPX‐based Monte Carlo simulation model for predicting three‐dimensional absorbed dose distributions. Phys Med Biol, 2008. 53(16): p. 4455‐70.8. Peterson, S.W., et al., Experimental validation of a Monte Carlo proton therapy nozzle model incorporating magnetically steered protons. Phys Med Biol, 2009. 54(10): p. 3217‐29.9. Bednarz, B. and H. Paganetti, Sensitivities of spread‐out Bragg peak characteristics on material properties and beam parameters in proton beam therapy treatment heads. 2010. unpublished.10. Paganetti, H., Four‐dimensional Monte Carlo simulation of time dependent geometries. Physics in Medicine and Biology, 2004. 49: p. N75‐N81.11. Lu, H.M. and H. Kooy, Optimization of current modulation function for proton spread‐out Bragg peak fields. Medical Physics, 2006. 33: p. 1281‐1287.12. Agostinelli, S., et al., GEANT4 ‐ a simulation toolkit. Nuclear Instruments and Methods in Physics Research, 2003. A 506: p. 250‐303.13. Zacharatou Jarlskog, C., et al., Assessment of organ specific neutron doses in proton therapy using whole‐body age‐dependent voxel phantoms. Physics in Medicine and Biology, 2008. 53: p. 693‐714.14. Titt, U., et al., Monte Carlo investigation of collimator scatter of proton‐therapy beams produced using the passive scattering method. Phys Med Biol, 2008. 53(2): p. 487‐504.15. Peterson, S., et al., Variations in proton scanned beam dose delivery due to uncertainties in magnetic beam steering. Med Phys, 2009. 36(8): p. 3693‐702.
courtesy of Harald Paganetti

16. Paganetti, H., H. Jiang, and A. Trofimov, 4D Monte Carlo simulation of proton beam scanning: Modeling of variations in time and space to study the interplay between scanning pattern and time‐dependent patient geometry. Physics in Medicine and Biology, 2005. 50:17. Kimstrand, P., et al., A beam source model for scanned proton beams. Phys Med Biol, 2007. 52(11): p. 3151‐68.18. Paganetti, H., Nuclear Interactions in Proton Therapy: Dose and Relative Biological Effect Distributions Originating From Primary and Secondary Particles. Physics in Medicine and Biology, 2002. 47: p. 747‐764.19. Paganetti, H. and B. Gottschalk, Test of Geant3 and Geant4 nuclear models for 160 MeV protons stopping in CH2. Medical Physics, 2003. 30: p. 1926‐1931.20. Zacharatou Jarlskog, C. and H. Paganetti, Physics settings for using the Geant4 toolkit in proton therapy. IEEE Transactions in Nuclear Science, 2008. 55: p. 1018‐1025.21. Andreo, P., On the clinical spatial resolution achievable with protons and heavier charged particle radiotherapy beams. Phys Med Biol, 2009. 54(11): p. N205‐15.22. Jiang, H. and H. Paganetti, Adaptation of GEANT4 to Monte Carlo dose calculations based on CT data. Medical Physics, 2004. 31: p. 2811‐2818.23. Yepes, P., et al., Monte Carlo fast dose calculator for proton radiotherapy: application to a voxelized geometry representing a patient with prostate cancer. Phys Med Biol, 2009. 54(1): p. N21‐8.24. Matsufuji, N., et al., Relationship between CT number and electron density, scatter angle and nuclear reaction for hadron‐therapy treatment planning. Physics in Medicine and Biology, 1998. 43: p. 3261‐3275.25. Mustafa, A.A.M. and D.F. Jackson, The relation between x‐ray CT numbers and charged particle stopping powers and its significance for radiotherapy treatment planning. Physics in Medicine and Biology, 1983. 28: p. 169‐176.26. Schaffner, B. and E. Pedroni, The precision of proton range calculations in proton radiotherapy treatment planning: experimental verification of the relation between CT‐HU and proton stopping power. Physics in Medicine and Biology, 1998. 43: p. 1579‐1592.27. Jiang, H., J. Seco, and H. Paganetti, Effects of Hounsfield number conversions on patient CT based Monte Carlo proton dose calculation. Medical Physics, 2007. 34: p. 1439‐1449.28. Palmans, H. and F. Verhaegen, Assigning nonelastic nuclear interaction cross sections to Hounsfield units for Monte Carlo treatment planning of proton beams. Physics in Medicine and Biology, 2005. 50: p. 991‐1000.29. Schneider, W., T. Bortfeld, and W. Schlegel, Correlation between CT numbers and tissue parameters needed for Monte Carlo simulations of clinical dose distributions. Physics in Medicine and Biology, 2000. 45: p. 459‐478.30. du Plessis, F.C.P., et al., The indirect use of CT numbers to establish material properties needed for Monte Carlo calculation of dose distributions in patients. Medical Physics, 1998. 25: p. 1195‐1201.31. Schneider, U., E. Pedroni, and A. Lomax, The calibration of CT Hounsfield units for radiotherapy treatment planing. Physics in Medicine and Biology, 1996. 41: p. 111‐124.32. Unkelbach, J., T.C. Chan, and T. Bortfeld, Accounting for range uncertainties in the optimization of intensity modulated proton therapy. Phys Med Biol, 2007. 52(10): p. 2755‐73.33. Rogers, D.W.O., et al., BEAMnrc User Manual. NRCC Report PIRS‐0509, 2002.34. Parodi, K., et al., Clinical CT‐based calculations of dose and positron emitter distributions in proton therapy using the FLUKA Monte Carlo code. Phys Med Biol, 2007. 52(12): p. 3369‐87.

35. Kooy, H., et al., Monitor unit calculations for range‐modulated spread‐out Bragg peak fields. Physics in Medicine and Biology, 2003. 48: p. 2797‐2808.36. Kooy, H.M., et al., The prediction of output factors for spread‐out proton Bragg peak fields in clinical practice. Physics in Medicine and Biology, 2005. 50: p. 5847‐5856.37. Paganetti, H., Monte Carlo calculations for absolute dosimetry to determine output factors for proton therapy treatments. Physics in Medicine and Biology, 2006. 51: p. 2801‐2812.38. Liu, H.H. and P. Keall, Dm rather than Dw should be used in Monte Carlo treatment planning. Medical Physics, 2002. 29: p. 922‐924.39. Paganetti, H., Dose to water versus dose to medium in proton beam therapy. Physics in Medicine and Biology, 2009. 54: p. 4399‐4421.40. Carlsson, C.A. and G.A. Carlsson, Proton Dosimetry with 185 MeV Protons. Dose Buildup from Secondary Protons and Recoil Electrons. Health Physics, 1977. 33: p. 481‐484.41. Laitano, R.F., M. Rosetti, and M. Frisoni, Effects of nuclear interactions on energy and stopping power in proton beam dosimetry. Nuclear Instruments and Methods A, 1996. 376: p. 466‐476.42. Medin, J. and P. Andreo, Monte Carlo calculated stopping‐power ratios, water/air, for clinical proton dosimetry (50‐250 MeV). Physics in Medicine and Biology, 1997. 42: p. 89‐105.43. Paganetti, H., unpublished data. 2010.44. Newhauser, W., et al., Monte Carlo simulations for configuring and testing an analytical proton dose‐calculation algorithm. Phys Med Biol, 2007. 52(15): p. 4569‐84.45. Pflugfelder, D., et al., Quantifying lateral tissue heterogeneities in hadron therapy. Med Phys, 2007. 34(4): p. 1506‐13.46. Urie, M., et al., Degradation of the Bragg peak due to inhomogeneities. Physics in Medicine and Biology, 1986. 31: p. 1‐15.47. Newhauser, W., et al., Monte Carlo simulations of the dosimetric impact of radiopaque fiducial markers for proton radiotherapy of the prostate. Phys Med Biol, 2007. 52(11): p. 2937‐52.48. Moravek, Z., et al., Uncertainty reduction in intensity modulated proton therapy by inverse Monte Carlo treatment planning. Phys Med Biol, 2009. 54(15): p. 4803‐19.49. Kimura, A., et al., DICOM data handling for Geant4‐based medical physics application. IEEE Nuclear Science Symposium Conference Record, 2004. 4: p. 2124‐2127.50. Kimura, A., et al., DICOM interface and visualization tool for Geant4‐based dose calculation. IEEE Nuclear Science Symposium Conference Record, 2005. 2: p. 981‐984.51. Parodi, K., et al., PET/CT imaging for treatment verification after proton therapy: a study with plastic phantoms and metallic implants. Med Phys, 2007. 34(2): p. 419‐35.52. Parodi, K., et al., Patient study of in vivo verification of beam delivery and range, using positron emission tomography and computed tomography imaging after proton therapy. Int J Radiat Oncol Biol Phys, 2007. 68(3): p. 920‐34.53. Paganetti, H., et al., Relative biological effectiveness (RBE) values for proton beam therapy. International Journal of Radiation Oncology, Biology, Physics, 2002. 53: p. 407‐421.54. Wilkens, J.J. and U. Oelfke, A phenomenological model for the relative biological effectiveness in therapeutic proton beams. Physics in Medicine and Biology, 2004. 49: p. 2811‐2825.55. Paganetti, H. and M. Goitein, Radiobiological significance of beam line dependent proton energy distributions in a spread‐out Bragg peak. Medical Physics, 2000. 27: p. 1119‐1126.56. Paganetti, H. and T. Schmitz, The influence of the beam modulation method on dose and RBE in proton radiation therapy. Physics in Medicine and Biology, 1996. 41: p. 1649‐1663.57. Kempe, J., I. Gudowska, and A. Brahme, Depth absorbed dose and LET distributions of therapeutic 1H, 4He, 7Li, and 12C beams. Med Phys, 2007. 34(1): p. 183‐92.58. Athar, B.S. and H. Paganetti, Neutron equivalent doses and associated lifetime cancer incidence risks for head & neck and spinal proton therapy. Phys Med Biol, 2009. 54(16): p. 4907‐26.59. Fontenot, J., et al., Equivalent dose and effective dose from stray radiation during passively scattered proton radiotherapy for prostate cancer. Phys Med Biol, 2008. 53(6): p. 1677‐88.60. Jiang, H., et al., Simulation of Organ Specific Patient Effective Dose Due to Secondary Neutrons in Proton Radiation Treatment. Physics in Medicine and Biology, 2005. 50: p. 4337‐4353.61. ICRP, Relative Biological Effectiveness (RBE), QualityFactor (Q), and Radiation Weighting Factor (wR). International Commission on Radiological Protection (Pergamon Press), 2003. 92.62. Paganetti, H., The use of computational patient models to assess the risk of developing radiation‐induced cancers from radiation therapy of the primary cancer. Procceediings of the IEEE, 2009. 97: p. 1977‐1987.





























