Embed Size (px)
Citation preview

Intrapartum Fetal Heart Rate Monitoring
A Standardized Approach toInterpretation and Management
Lesson 4: Management

At the end of this program, participants will be able to:
Describe a standardized intrapartum FHR monitoring management decision model consisting of 4 central concepts that systematically address potential sources of preventable error
Lecture Objectives

Management (n.) The act of handling or controlling something successfully
Success = safe delivery
Birth free from injury caused by interrupted oxygenation

A “standardized management” protocol is NOT a cookbook that determines the timing and method
of delivery
Standardization does not take the “art” out the practice of medicine

The objective of a “standardized management” protocol is to minimize potential sources of
preventable error

Despite our best efforts, not all outcomes will be good…
What happens when the outcome is bad?

Root cause analysis starts with a “sentinel event” and focuses on ascertaining and analyzing potential sources of preventable error in order to establish standard procedures to minimize the chance that they will recur in the future. Root cause analysis does not focus on assigning blame
A medical liability legal action, on the other hand, focuses on assigning blame

Assigning “blame”
Deviation from standard of care↓
Proximate cause↓
Damages

What is your best defense?
1. My actions deviated from the standard of care, but they did not cause the injury
2. My actions did not deviate from the standard of care

We are expected to take reasonable actions to avoid preventable errors in intrapartum management…
What are some potential sources of preventable error??

To delivery
Determine the need for immediate operative intervention
Address common obstacles to rapid delivery
Apply appropriate corrective measures
Communicate accurately and effectively
Interpret FHR tracing accurately
Define FHR tracing accurately (terminology)
Confirm FHR and uterine activity
Potential sources of preventable error from admission
Realistically assess the decision to delivery time
Consider other factors that might be responsible for the FHR changes

By employing a standardized, systematic approach that addresses as many potential sources of preventable error as possible, we can accomplish three major goals:
1. Minimize preventable variations in the decision-making process
2. Minimize the likelihood that critical elements of the decision-making process will be overlooked
3. Demonstrate reasonableness and prudenceTwo elements that define “standard of care”

Intrapartum FHR Monitoring
Terminology Interpretation Management

What do I call it?Baseline rate…130 bpmVariability…moderateAccelerations…presentDecelerations…absentChanges or trends over time…none
1. Terminology
2. Interpretation
3. Management
One end of the FHR spectrum – “Category I”

What does it mean?

What do I do about it? This intrapartum FHR tracing requires no specific action
1. True
2. False

Intrapartum Surveillance
In a “low-risk” patient:
Review the tracing at least every 30 minutes in the active phase of the 1st stage of labor and every 15
minutes in the 2nd stage
In a “high-risk” patient:
Review the tracing at least every 15 minutes in the active phase of the 1st stage of labor and every 5
minutes in the 2nd stage

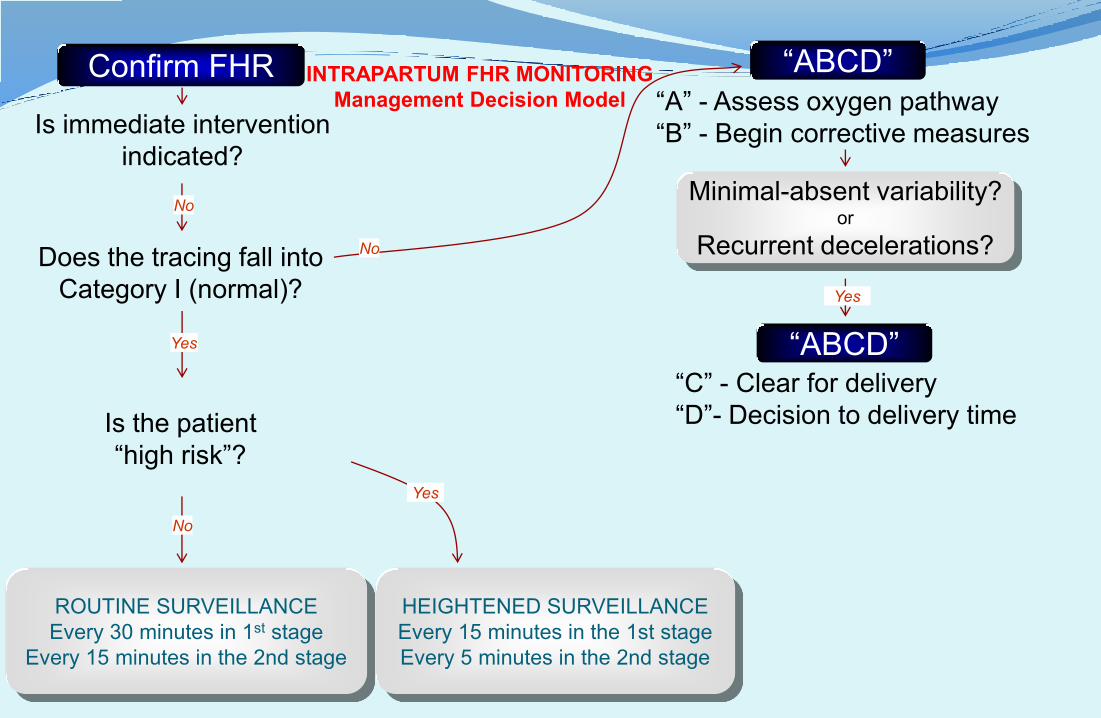
Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model

Category II
1. Terminology
2. Interpretation
3. Management
What do I call it?Baseline rate…150 bpmVariability…moderateAccelerations…absentDecelerations…presentChanges or trends…yes

What does it mean?

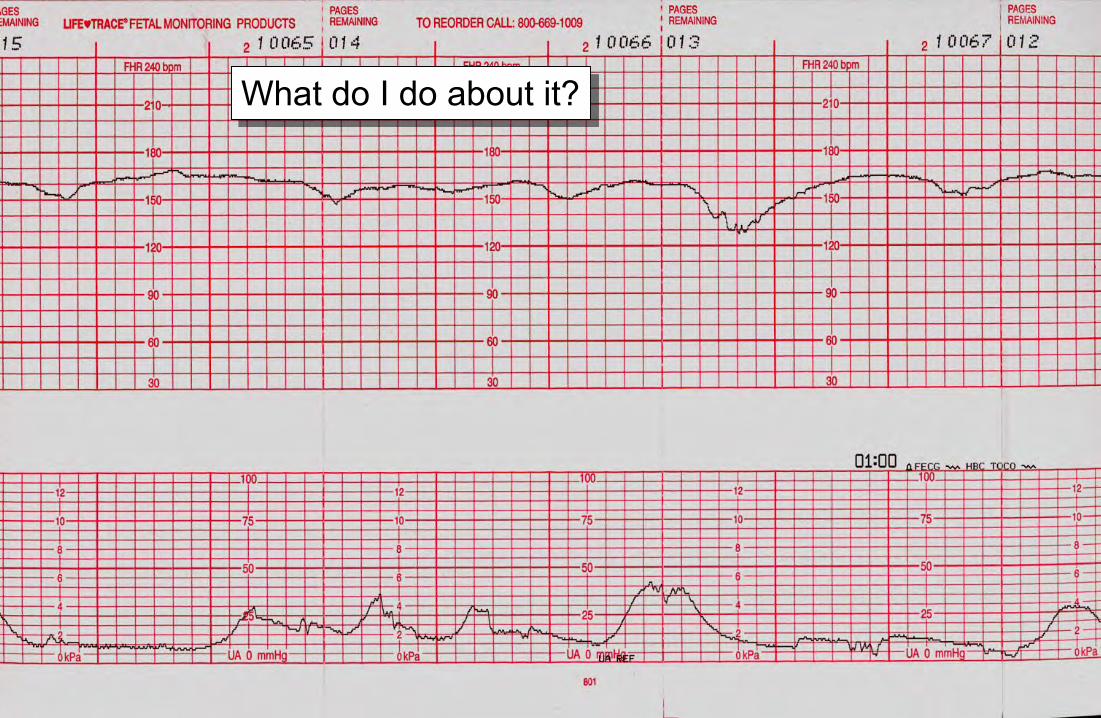
What do I do about it?

If there is evidence of interrupted transfer of oxygen from the environment to the fetus, the most logical approach is to
1. Ignore it
2. Assess the oxygen pathway
3. Begin corrective measures if needed
4. Perform immediate cesarean
5. None of the above
6. 2 & 3

Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model
“ABCD”
No
Standardized Intrapartum FHR Management
Four Central Concepts
“ABCD”A – Assess the oxygen pathwayB – Begin corrective measures

Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model
“ABCD”
No
“A” - Assess oxygen pathway“B” - Begin corrective measures

“A”Assess Oxygen
Pathway
“B”Begin Corrective
Measures if Indicated
“C”Clear Obstacles to
Rapid Delivery
“D”Determine Decision
to Delivery Time
Lungs Airway and breathingPulse oximetry or ABG
Supplemental oxygenTreat pulmonary disordersAlter breathing technique
FacilityOR availabilityInstrumentsEquipment
Realistic estimate of facility response time
Heart Heart rate and rhythmCardiac output
IV fluid bolusTreat arrhythmia Staff
NotifyObstetricianSurgical assistantAnesthesiologistNeonatologistPediatricianNursing staff
Consider staff:AvailabilityTrainingExperience
Vasculature Blood pressureVolume status
Maternal position changesCorrect hypotension Mother
Informed consentAnesthesia optionsLaboratory testsBlood productsIntravenous accessUrinary catheterAbdominal prepTransfer to OR
Surgical considerations(prior abdominal or uterine surgery uterine fibroids)
Medical considerations(obesity, hypertension, diabetes,
SLE)Obstetric considerations
(parity, pelvimetry, placental location)
UterusContraction strengthContraction frequencyBaseline uterine toneExclude uterine rupture
Stop/reduce oxytocin Remove prostaglandin Uterine relaxants if neededConsider IUPCAlter pushing technique Fetus
ConfirmFetal heart rateGestational ageFetal weightPresentationPosition
Consider FSE
Consider factors such as:Baseline FHR changesLoss of variabilityLoss of accelerationsRecurrent decelerationsGrowth restrictionMacrosomiaPresentation, positionPrematurity, infection Meconium
Placenta Placental separationBleeding vasa previa Rapid delivery if indicated
Cord Vaginal examExclude cord prolapse
Consider amnioinfusionConsider elevating fetal head Labor Consider tocolytic
Consider IUPC
Consider factors such as:Arrest disorderProtracted laborRemote from deliveryPoor expulsive efforts

“A”Assess Oxygen
Pathway
“B”Begin Corrective
Measures if Indicated
“C”Clear Obstacles to
Rapid Delivery
“D”Determine Decision
to Delivery Time
Lungs Airway and breathingPulse oximetry or ABG Supplemental oxygen Facility
OR availabilityInstrumentsEquipment
Realistic estimate of facility response time
Heart Heart rate and rhythmCardiac output IV fluid bolus Staff
NotifyObstetricianSurgical assistantAnesthesiologistNeonatologistPediatricianNursing staff
Consider staff:AvailabilityTrainingExperience
Vasculature Blood pressureVolume status
Maternal position changesCorrect hypotension Mother
Informed consentAnesthesia optionsLaboratory testsBlood productsIntravenous accessUrinary catheterAbdominal prepTransfer to OR
Surgical considerations(prior abdominal or uterine surgery uterine fibroids)
Medical considerations(obesity, hypertension, diabetes,
SLE)Obstetric considerations
(parity, pelvimetry, placental location)
UterusContraction strengthContraction frequencyBaseline uterine toneExclude uterine rupture
Stop or reduce stimulant Consider uterine relaxant
Fetus
ConfirmFetal heart rateGestational ageFetal weightPresentationPosition
Consider FSE
Consider factors such as:Baseline FHR changesLoss of variabilityLoss of accelerationsRecurrent decelerationsGrowth restrictionMacrosomiaPresentation, positionPrematurity, infection Meconium
Placenta Placental separationBleeding vasa previa
Cord Vaginal examExclude cord prolapse Consider amnioinfusion Labor Consider tocolytic
Consider IUPC
Consider factors such as:Arrest disorderProtracted laborRemote from deliveryPoor expulsive efforts

Do “conservative measures” really improve fetal oxygenation?Measures Evidence
Supplemental oxygen Direct – Pulse oximetry
Maternal position changes Direct – Pulse oximetry
IV fluid bolus Direct – Pulse oximetry
Correcting hypotension Indirect – FHR
Amnioinfusion Indirect – FHR
Reducing uterine activity Indirect – FHR, pulse oximetry
Altered pushing technique Indirect – FHR, pulse oximetry
Altered breathing technique Indirect - FHR
KR Simpson J Midwifery Womens Health. 2007 May-Jun;52(3):229-37

Category III
1. Terminology
2. Interpretation
3. Management
What do I call it?Baseline rate…165Variability…absentAccelerations…absentDeceleration…present, recurrentChanges or trends…yes

What does it mean?
What do I do about it?

If you have done “A” and “B”, but the tracing has not improved, the next step is…
1. Panic
2. Crash Cesarean
3. Nothing
4. Discharge home
5. “C”

Standardized Intrapartum FHR Management
Four Central Concepts
“ABCD”A – Assess the oxygen pathwayB – Begin corrective measuresC – Clear for deliveryD – Decision to delivery time

Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model
“ABCD”
No
“A” - Assess oxygen pathway“B” - Begin corrective measures
Minimal-absent variability?or
Recurrent decelerations?
Yes
“ABCD”“C” - Clear for delivery

Clear for delivery
If conservative measures do not correct recurrent decelerations and improve variability, it is prudent to plan ahead for the possible need for rapid delivery
There are many common sources of unnecessary delay
Addressing them in a systematic fashion reduces the likelihood that important factors will be overlooked
It also demonstrates reasonableness and prudence…two elements that define the standard of care

Clear obstacles to rapid delivery
These simple precautions are not often emphasized in a systematic way, but failing to
address them can be a major source of criticism in the event of an untoward outcome

FacilityStaffMotherFetusLabor
Consider individual characteristics of

“A”Assess Oxygen
Pathway
“B”Begin Corrective
Measures if Indicated
“C”Clear Obstacles to
Rapid Delivery
“D”Determine Decision
to Delivery Time
Lungs Airway and breathingPulse oximetry or ABG
Supplemental oxygenTreat pulmonary disordersAlter breathing technique
FacilityOR availabilityInstrumentsEquipment
Realistic estimate of facility response time
Heart Heart rate and rhythmCardiac output
IV fluid bolusTreat arrhythmia Staff
NotifyObstetricianSurgical assistantAnesthesiologistNeonatologistPediatricianNursing staff
Consider staff:AvailabilityTrainingExperience
Vasculature Blood pressureVolume status
Maternal position changesCorrect hypotension Mother
Informed consentAnesthesia optionsLaboratory testsBlood productsIntravenous accessUrinary catheterAbdominal prepTransfer to OR
Surgical considerations(prior abdominal or uterine surgery uterine fibroids)
Medical considerations(obesity, hypertension, diabetes,
SLE)Obstetric considerations
(parity, pelvimetry, placental location)
UterusContraction strengthContraction frequencyBaseline uterine toneExclude uterine rupture
Stop/reduce oxytocin Remove prostaglandin Uterine relaxants if neededConsider IUPCAlter pushing technique Fetus
ConfirmFetal heart rateGestational ageFetal weightPresentationPosition
Consider FSE
Consider factors such as:Baseline FHR changesLoss of variabilityLoss of accelerationsRecurrent decelerationsGrowth restrictionMacrosomiaPresentation, positionPrematurity, infection Meconium
Placenta Placental separationBleeding vasa previa Rapid delivery if indicated
Cord Vaginal examExclude cord prolapse
Consider amnioinfusionConsider elevating fetal head Labor Consider tocolytic
Consider IUPC
Consider factors such as:Arrest disorderProtracted laborRemote from deliveryPoor expulsive efforts
Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model
“ABCD”
No
“A” - Assess oxygen pathway“B” - Begin corrective measures
Minimal-absent variability?or
Recurrent decelerations?
Yes
“ABCD”“C” - Clear for delivery“D”- Decision to delivery time

“A”Assess Oxygen
Pathway
“B”Begin Corrective
Measures if Indicated
“C”Clear Obstacles
to Rapid Delivery
“D”Determine Decision
to Delivery Time
Lungs Airway and breathingPulse oximetry or ABG Supplemental oxygen Facility
OR availabilityInstrumentsEquipment
Realistic estimate of facility response time
Heart Heart rate and rhythmCardiac output IV fluid bolus Staff
NotifyObstetricianSurgical assistantAnesthesiologistNeonatologistPediatricianNursing staff
Consider staff:AvailabilityTrainingExperience
Vasculature Blood pressureVolume status
Maternal position changesCorrect hypotension Mother
Informed consentAnesthesia optionsLaboratory testsBlood productsIntravenous accessUrinary catheterAbdominal prepTransfer to OR
Surgical considerations(prior abdominal or uterine surgery uterine fibroids)
Medical considerations(obesity, hypertension, diabetes, SLE)
Obstetric considerations(parity, pelvimetry, placental location)
UterusContraction strengthContraction frequencyBaseline uterine toneExclude uterine rupture
Stop/reduce stimulantsConsider uterine relaxants
Fetus
ConfirmFetal heart rateGestational ageFetal weightPresentationPosition
Consider FSE
Consider factors such as:Baseline FHR changesLoss of variabilityLoss of accelerationsRecurrent decelerationsGrowth restrictionMacrosomiaPresentation, positionPrematurity, infection Meconium
Placenta Placental separationBleeding vasa previa
Cord Vaginal examExclude cord prolapse Consider amnioinfusion Labor Consider tocolytic
Consider IUPC
Consider factors such as:Arrest disorderProtracted laborRemote from deliveryPoor expulsive efforts

If I have a checklist of standard operating procedures posted on L&D, I could be held accountable for failing to address all of the standard operating procedures in the event of a bad outcome
1. True
2. False

The fact of the matter…We are required by the standard of care to follow the standard operating procedures that would be expected from a reasonable and prudent practitioner in the same or similar circumstances
Checklist or no checklist
Why not use a checklist as a reminder?

Assess oxygen pathway
Begin corrective measures
Clear for delivery
Determine decision to delivery time
√
√
√
√
Now what?

Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model
“ABCD”
No
“A” - Assess oxygen pathway“B” - Begin corrective measures
Minimal-absent variability?or
Recurrent decelerations?
Yes
“ABCD”“C” - Clear for delivery“D”- Decision to delivery time
Is vaginal delivery likely before metabolic acidemia?

Is vaginal delivery likely to occur before the onset of metabolic acidemia?

This is ALWAYS a prediction of unknown future events
It ALWAYS involves multiple interacting factors
It ALWAYS relies on clinical judgment
There will NEVER be a “cookbook” answer

USE INDIVIDUAL CLINICAL JUDGMENT TO ESTIMATE:
Time to vaginal delivery
Consider cervical dilatation, effacement, station, adequacy of uterine activity, past rate of progress and expected rate of progress in the future

With recurrent decelerations and minimal-absent variability, fetal metabolic acidemia can evolve over
approximately 60 minutes (assuming a previously normal FHR tracing and no acute events)
In the setting of acute events, absent variability, absent accelerations and decelerations that are
deeper, longer and more frequent, metabolic acidemia might occur more rapidly

The information supporting these statements is limited:
Fleischer A, Schulman H, Jagani N, Mitchell J, Randolph G: The development of fetal acidosis in the presence of an abnormal fetal heart rate tracing. I. The average for gestational age fetus, Am J Obstet Gynecol 144(1):55-60, 1982.
Ingemarsson I, Herbst A, Thorgren-Jerneck K: Long-term outcome after umbilical artery acidemia at term birth: Influence of gender and fetal heart rate abnormalities, Br J Obstet Gynaecol 104(10):1123-1127, 1997.
Low JA, Galbraith RS, Muir DW, Killen HL, Pater EA, Karchmar EJ: Factors associated with motor and cognitive deficits in children after intrapartum fetal hypoxia, Am J Obstet Gynecol 148:533-539, 1982.
Parer JT, King T, Flanders S, Fox M, Kilpatrick SJ: Fetal acidemia and electronic fetal heart rate patterns. Is there evidence of an association? J Matern Fetal Neonatal Med 19(2):289-294, 2006.

Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model
“ABCD”
No
“A” - Assess oxygen pathway“B” - Begin corrective measures
Minimal-absent variability?or
Recurrent decelerations?
Yes
“ABCD”“C” - Clear for delivery“D”- Decision to delivery time
Is vaginal delivery likely before metabolic acidemia?
OFFER OPERATIVE DELIVERYDocument decision process
Counsel patient
Yes
No

Category I
“Low risk”1st stage q 30 min2nd stage q 15 min
“High risk”1st stage q 15 min2nd stage q 5 min
Category IIAND
Metabolic acidemia CAN be excluded(Moderate variability or accelerations)
Assess Oxygen PathwayLungsHeartVasculatureUterusPlacentaCord
Begin Corrective MeasuresSupplemental oxygenPosition changeFluid bolusCorrect hypotensionStop/reduce uterine stimulantConsider uterine relaxantConsider amnioinfusion
Clear obstacles to deliveryFacilityStaffMotherFetusLabor
Decision-delivery estimateFacilityStaffMotherFetusLabor
Category II - IIIAND
Metabolic acidemia CANNOT be excluded(Minimal-absent variability and no accelerations)
ADMISSION
OUTCOME
SurveillanceConservative
Measures“A & B”
Prepare forDelivery“C & D”
DeliveryDecision
?
If, in your clinical judgment, immediate delivery is necessary, proceed without delay
If, in your clinical judgment, a brief period of expectant management is reasonable, formulate a plan that minimizes potential risks…

According to the best information in the literature…if a normal FHR tracing changes to a tracing with minimal-absent variability and recurrent decelerations, metabolic acidemia can evolve over approximately 60 minutes
How reliable is this information?
What would you consider a reasonable “margin of safety”?
Reducing the time by 50%? That’s the approach we take with risks of radiation exposure during pregnancy…

A suggested reasonable approach…
If a previously normal FHR tracing loses the ability to exclude metabolic acidemia and, in your clinical judgment, a brief period of expectant management is reasonable…
Allow no more than 30 minutes to either accomplish delivery or correct the FHR tracing (approximately 60 minute leeway gleaned from scanty literature minus a reasonable 50% margin of safety)
Remember…that’s 30 minutes until delivery or correction of the FHR tracing…not 30 minutes until the decision to proceed with delivery

Take into account your estimated “decision-to-delivery” time and subtract it from your 30-minute window
The remainder is the amount of time you have to achieve vaginal delivery or correct the FHR tracing before making a decision to proceed with operative delivery

Is this scientific?
As scientific as possible given the dearth of information in the literature
Is it reasonable and prudent?
It is as evidence-based as the current literature allows, it incorporates a 50% margin of safety and it accounts for the estimated “real-life” decision-to-delivery time

But is it “standard of care”?
By definition, if your actions are deemed to be reasonable and prudent, they meet the standard of care
Few things demonstrate reasonableness and prudence more convincingly than a thoughtful, preconceived, standardized, evidence-based, well-prepared, systematically executed plan of action

Category I
“Low risk”1st stage q 30 min2nd stage q 15 min
“High risk”1st stage q 15 min2nd stage q 5 min
Category IIAND
Metabolic acidemia CAN be excluded(Moderate variability or accelerations)
Assess Oxygen PathwayLungsHeartVasculatureUterusPlacentaCord
Begin Corrective MeasuresSupplemental oxygenPosition changeFluid bolusCorrect hypotensionStop/reduce uterine stimulantConsider uterine relaxantConsider amnioinfusion
Clear obstacles to deliveryFacilityStaffMotherFetusLabor
Decision-deliveryFacilityStaffMotherFetusLabor
Category II - IIIAND
Metabolic acidemia CANNOT be excluded(Minimal-absent variability and no accelerations)
ADMISSION
OUTCOME
SurveillanceConservative
Measures“A & B”
Prepare forDelivery“C & D”
DeliveryDecision
Evolution of metabolic acidemia ~ 60 minSubtract 50% safety margin ~ 30 min
Subtract “decision-delivery estimate” ~ X minAllow the remaining time for vaginal delivery or
correction of the FHR tracing
If vaginal delivery does not occur in this time frame and the FHR abnormalities have not been corrected,
it is reasonable to offer operative delivery
Is immediate delivery indicated?
No

Confirm FHR
Is immediate intervention indicated?
Does the tracing fall into Category I (normal)?
Is the patient“high risk”?
ROUTINE SURVEILLANCEEvery 30 minutes in 1st stage
Every 15 minutes in the 2nd stage
Yes
No
Yes
No
HEIGHTENED SURVEILLANCEEvery 15 minutes in the 1st stageEvery 5 minutes in the 2nd stage
INTRAPARTUM FHR MONITORINGManagement Decision Model “ABCD”
No
“A” - Assess oxygen pathway“B” - Begin corrective measures
Minimal-absent variability?or
Recurrent decelerations?
Yes
“ABCD”“C” - Clear for delivery“D”- Decision to delivery time
Is vaginal delivery likely before metabolic acidemia?
OFFER OPERATIVE DELIVERYDocument decision process
Counsel patient
Yes
No
Urgently needed standardization of intrapartum FHR management should
not be further delayed because this one question is difficult to anser
Is vaginal delivery likely before metabolic acidemia?





























