Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ilab20
Download by: [77.168.13.167] Date: 28 September 2015, At: 11:04
Critical Reviews in Clinical Laboratory Sciences
ISSN: 1040-8363 (Print) 1549-781X (Online) Journal homepage: http://www.tandfonline.com/loi/ilab20
Molecular malaria diagnostics: A systematic reviewand meta-analysis
Johanna M. Roth, Daniël A. Korevaar, Mariska M. G. Leeflang & Pètra F. Mens
To cite this article: Johanna M. Roth, Daniël A. Korevaar, Mariska M. G. Leeflang & Pètra F.Mens (2015): Molecular malaria diagnostics: A systematic review and meta-analysis, CriticalReviews in Clinical Laboratory Sciences, DOI: 10.3109/10408363.2015.1084991
To link to this article: http://dx.doi.org/10.3109/10408363.2015.1084991
View supplementary material
Published online: 17 Sep 2015.
Submit your article to this journal
Article views: 63
View related articles
View Crossmark data

http://informahealthcare.com/labISSN: 1040-8363 (print), 1549-781X (electronic)
Crit Rev Clin Lab Sci, Early Online: 1–19! 2015 Taylor & Francis. DOI: 10.3109/10408363.2015.1084991
REVIEW ARTICLE
Molecular malaria diagnostics: A systematic review and meta-analysis*
Johanna M. Roth1, Daniel A. Korevaar2, Mariska M. G. Leeflang2, and Petra F. Mens1,3
1Royal Tropical Institute (KIT), KIT Biomedical Research, Amsterdam, The Netherlands, 2Department of Clinical Epidemiology, Biostatistics and
Bioinformatics, Academic Medical Center, Amsterdam, The Netherlands, and 3Department of Infectious Diseases, Division of Internal Medicine,
Center of Tropical Medicine and Infectious Diseases, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands
Abstract
Accurate diagnosis of malaria is essential for identification and subsequent treatment of thedisease. Currently, microscopy and rapid diagnostic tests are the most commonly useddiagnostics, next to treatment based on clinical signs only. These tests are easy to deploy, buthave a relatively high detection limit. With declining prevalence in many areas, there is anincreasing need for more sensitive diagnostics. Molecular tools may be a suitable alternative,although costs and technical requirements currently hamper their implementation in resourcelimited settings. A range of (near) point-of-care diagnostics is therefore under development,including simplifications in sample preparation, amplification and/or read-out of the test.Accuracy data, in combination with technical characteristics, are essential in determining whichmolecular test, if any, would be the most promising to be deployed. This review presents acomprehensive overview of the currently available molecular malaria diagnostics, ranging fromwell-known tests to platforms in early stages of evaluation, and systematically evaluates theirpublished accuracy. No important difference in accuracy was found between the mostcommonly used PCR-based assays (conventional, nested and real-time PCR), with most of themhaving high sensitivity and specificity, implying that there are no reasons other than practicalones to choose one technique over the other. Loop-mediated isothermal amplification andother (novel) diagnostics appear to be highly accurate as well, with some offering potential tobe used in resource-limited settings.
Abbreviations: AJOL: African Journals Online; AQP: aquaglyceroporin; CENTRAL: CochraneCentral Register of Controlled Trials; CI: 95% confidence interval; CS: circumsporozoite; dhfr:dihydrofolate reductase; DNA: deoxyribonucleic acid; ECPR: enoyl-acyl carrier protein reduc-tase; FRET: fluorescence resonance energy transfer; HRP-II: histidine rich protein II; LAMP:loop-mediated isothermal amplification; LDR-FMA: ligase detection reaction-fluorescentmicrosphere assay; LoD: limit of detection; MGB: minor groove binding; msp: merozoitesurface protein; NA: nucleic acid; NASBA: nucleic acid sequence based amplification; PET-PCR:photo-induced electron transfer-polymerase chain reaction; pfmdr: Plasmodium falciparummultidrug resistance protein; PoC: point-of-care; Po25: p25 ookinate surface protein; PCR:polymerase chain reaction; PCR-ELISA: PCR-enzyme-linked immunosorbent assay; PCR-NALFIA: PCR-nucleic acid lateral flow immunoassay; QUADAS: Quality Assessment ofDiagnostic Accuracy Studies; RBC: red blood cell; RDT: rapid diagnostic test; RNA: ribonucleicacid; ROC: receiver operator characteristic; rRNA: ribosomal ribonucleic acid; STARD: Standardsfor the Reporting of Diagnostic Accuracy Studies; WHO: World Health Organization
Keywords
Diagnostic test accuracy, loop-mediatedisothermal amplification, microscopy,molecular diagnostic, Plasmodium,point-of-care, polymerase chain reaction,rapid diagnostic test
History
Received 12 February 2015Revised 29 May 2015Accepted 4 July 2015Published online 16 September 2015
Introduction
Accurate and fast diagnosis of malaria is essential for the
initiation of proper treatment. Diagnostic tests for malaria in
endemic areas are now recommended as routine by the World
Health Organization (WHO), in all patients suspected of
malaria1. However, correct diagnosis is challenging, espe-
cially among individuals with low parasitaemia in resource-
poor settings. Microscopy is still often considered to be the
gold standard, but it can be time consuming and has a
relatively high limit of detection (LoD), which strongly
*Referees: Dr. Georges Snounou, Universite Pierre et Marie Curie,CIMI-Paris, France; Dr. Paul LaBarre, PATH, Seattle, USA; Dr.Elizabeth Pienaar, South African Cochrane Center, Tygerberg, SouthAfrica
Address for correspondence: Johanna Roth, Royal Tropical Institute/Koninklijk Instituut voor de Tropen (KIT), KIT Biomedical Research,Meibergdreef 39, 1105 AZ Amsterdam, The Netherlands. Tel: +310205665442. E-mail: [email protected]
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

depends on the quality of the slide and the training level of the
microscopist. The LoD of Giemsa-stained thick blood film is
estimated to be 4–20 parasites/ml (p/ml) when performed by
expert microscopists using good quality equipment, but under
field conditions 50–100 p/ml are more realistic2. Antigen-
detection-based rapid diagnostic tests (RDTs) are fast and
easy to perform, but often have an even higher LoD
(4100 p/ml), especially if the infecting agent is non-falcip-
arum3,4. Furthermore, histidine-rich protein II (HRP-II) based
RDTs are unsuitable for patient follow-up after treatment,
because antigens may circulate up to 28 days after the
infection has been cleared, leading to false positive test results
in the first month after treatment3,4.
The sensitivity of molecular diagnostics, such as polymer-
ase chain reaction (PCR) or nucleic acid sequence based
amplification (NASBA), is generally believed to be higher
than that of microscopy or RDTs5. Currently, the most
commonly used molecular diagnostic for malaria is PCR, with
a LoD between 0.004 and 30 p/ml6. Although not yet common
as routine diagnostic, PCR is increasingly being used for
confirmatory diagnosis of returning travelers or migrants
suspected of malaria in Western laboratories and in some
(reference) laboratories in endemic areas. However, imple-
mentation in resource-poor endemic settings remains a
challenge, as molecular diagnostics normally require well-
equipped laboratories, expensive supplies and trained
technicians.
In an attempt to make molecular tools more suitable as
(near) point-of-care (PoC) tests for the diagnosis of malaria in
resource-poor settings, a range of easy to perform assays are
under development that circumvent some of the drawbacks of
conventional molecular methods. For example, isothermal
amplification technologies such as loop-mediated isothermal
amplification (LAMP) and NASBA do not require expensive
PCR-machines7,8. PCR-nucleic acid lateral flow immuno-
assay (PCR-NALFIA) uses simple and cheap lateral flow
read-out systems9. These characteristics make them poten-
tially powerful tools, not only for case-management, but also
for follow-up of patients after treatment and to detect
asymptomatic carriers during screening programs.
The range of molecular tests developed so far shows high
variability in performance characteristics and may differ in
type and volume of input material (DNA, RNA or whole
blood), target gene, (number of) species detected, primer/
probe composition and concentration, amplification technique
(PCR or isothermal), read-out (gel-electrophoresis, fluores-
cence detection, lateral flow) and whether it is qualitative or
quantitative10. Differences in accuracy between assays can
therefore be expected. It is important to get a clear overview
of the available diagnostics, their accuracy and characteris-
tics, to enable decisions being made on whether a test is
suitable for a particular purpose (clinical practice, asymp-
tomatic screening and/or treatment follow-up) and setting
(varying from well-equipped reference laboratories to rural
health facilities).
Determining and comparing accuracy of the different
molecular assays is challenging, because a true gold standard
does not exist so far. When evaluating PCR with microscopy
as a reference standard, some false positive test results may
actually be sub-microscopic low-density infections11, leading
to underestimations of specificity. It can be anticipated,
however, that high-quality expert microscopy will detect more
low-density infections and will therefore be a better reference
standard than routine field microscopy. In addition to
microscopy, commonly used PCR-based assays such as
nested and real-time PCR are sometimes used as reference
standards to determine the accuracy of a (novel) molecular
tool, as these assays are thought to have superior sensitivity
and specificity. Within study comparisons with both micros-
copy and PCR as reference standards are valuable in estimating
the number of low-density infections missed by microscopy.
Occasionally tests are evaluated against a composite reference
standard of molecular and/or non-molecular techniques in an
attempt to obtain optimal sensitivity and specificity.
Several descriptive reviews on the molecular diagnosis of
malaria have been published. A thorough overview of both
traditional PCR-based diagnostics and newer techniques is
given by Vasoo and Pritt10. Different PCR-based methods for
the diagnosis of imported malaria are discussed by Berry
et al.6 while Cordray et al. review the available molecular PoC
tests for endemic settings12. However, the accuracy of
currently available molecular diagnostics has never been
systematically reviewed, while accuracy data are essential in
determining which molecular test, if any, would be the most
promising to be deployed. The aim of the present review is to
provide an update on the molecular malaria diagnostics that
have been developed and to systematically evaluate their
published accuracy.
Methods
Eligible studies
Eligible were primary studies that assessed the accuracy of a
molecular diagnostic test for the detection of malaria in
clinically suspected patients recruited in malaria endemic
settings, using either microscopy or a PCR-based assay as a
reference test. Studies using a composite reference standard
including at least microscopy or PCR were also eligible.
There were no restrictions regarding year of publication.
Molecular tests in any format detecting any Plasmodium
species by DNA and/or RNA amplification were included.
Studies performing the molecular test under evaluation in a
non-endemic setting were only included if patients had been
recruited in an endemic setting. Studies that included
pregnant women only were excluded, as during pregnancy
malaria parasites can sequester in the placenta, complicating
the detection in peripheral blood of pregnant women13. A
recent systematic review describes the accuracy of molecular
tools for the detection of malaria in pregnancy14. Case–
control studies were also excluded, because they tend to
overestimate the accuracy of the test under evaluation15.
Reference test: microscopy
Microscopy is the most accurate non-molecular test available
and can detect low parasite densities when performed by a
trained microscopist. The procedure for routine microscopy is
described by the WHO and includes reading at least 100 high
power fields by a qualified microscopist16. If an included
paper made a distinction between research/expert microscopy
2 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

and routine/conventional microscopy, the first was taken as
the reference standard to ensure the use of the most optimal
microscopy quality available. In this review, the reported
quality of microscopy was assessed and considered good
when at least two independent microscopists read 100 high
power fields or more. These criteria are highly similar to
those in a systematic review describing the accuracy of
malaria RDTs compared to microscopy17. If these criteria
were not met, or when insufficient data were reported, the
quality of microscopy was considered unknown.
Reference test: PCR
PCR-based assays are increasingly being used as a reference
standard for the detection of malaria, because of their superior
sensitivity in detecting low density and mixed infections18.
Studies evaluating a molecular diagnostic against a PCR-
based assay were therefore included. Comparisons between
different PCRs, like nested and real-time PCR, were also
eligible. Comparisons using a non-PCR-based molecular
diagnostic as a reference standard were excluded, as these
tests are often still in the evaluation phase and currently rarely
used for reference purposes.
Search strategy
Relevant studies were identified by searching Medline
(PubMed), EMBASE, Web of Science, the Cochrane
Central Register of Controlled Trials (CENTRAL), African
Index Medicus and African Journals Online (AJOL). Search
terms are provided in Additional file 1. Searches were
performed in January 2014 and last updated in March 2014.
Study selection
Study references and abstracts were exported to Reference
Manager (version 12, Thomson Reuters, New York, NY).
Duplicates were removed. A primary selection, based on title
and abstract, was performed independently by two authors
(J.R. and D.K.). Studies considered relevant by at least one of
the two authors were selected and their full texts were
retrieved. If the full text could not be retrieved online, authors
were approached whenever contact details were available.
Full papers were independently assessed for inclusion by the
same two authors. Disagreements were resolved by discussion
or by consulting a third author (P.M.). Authors were contacted
if studies were eligible, but additional data were required to
derive 2� 2 tables. If 2� 2 tables could not be obtained,
studies were excluded.
Data extraction
One author (J.R.) extracted data from included studies in
Review Manager (version 5.2, the Cochrane Collaboration,
London, UK) and Excel (version 14.0, Microsoft, Redmond,
WA), which was cross-checked by a second author (D.K.).
Information on study design, study participants, reference
standard, index test and data to derive 2� 2 tables was
collected.
Two authors (J.R., D.K.) independently assessed methodo-
logical quality using the QUADAS-2 tool19, which
assesses risk of bias and applicability concerns in four
domains (patient selection, index test, reference standard, and
flow & timing). Studies were considered to have a high risk of
partial verification bias if410% of the patients did not receive
a reference standard. A high risk of differential verification
bias was defined as410% of the patients receiving a different
reference standard. Risk of bias was also considered to be
high when410% of the eligible patients were not included in
the analysis. Disagreements were resolved by discussion or
consultation of a third author (P.M.).
Statistical analyses
In Review Manager, 2� 2 tables, their estimates of sensitivity
and specificity and corresponding 95% confidence intervals
(CIs) were plotted in forest plots and receiver operator
characteristic (ROC) space. The xtmelogit command in Stata
(version 12.1, Stata, College Station, TX) was used to perform
meta-analyses, with a minimum requirement of four 2� 2
tables per index test-reference standard combination. Studies
were excluded from the meta-analysis if they had a high risk
of bias in one or more QUADAS-2 Risk of Bias domains.
Random effect models were used by default, as diagnostic
accuracy studies are expected to show a considerable amount
of heterogeneity, taking into account between study as well as
chance variation. To compare accuracy between tests and to
further investigate sources of heterogeneity, covariates were
added to the xtmelogit command. A likelihood-ratio test was
used to compare the accuracies of each index test included in
the meta-analysis. The quality of microscopy and geographic
area (continent) were investigated as sources of heterogeneity.
For other factors that were anticipated to affect accuracy, like
the species detected, the protocol used and the test setting,
insufficient data were reported to explore whether they were
sources of heterogeneity.
Results
Search results and included studies
The search identified 13 144 articles. After removing dupli-
cates, 7168 titles and abstracts were screened, of which 609
studies were selected to potentially fulfil the eligibility
criteria. Of these, 533 were excluded based on the full text,
for the following reasons (Figure 1): asymptomatic screening
(n¼ 179), case–control design (n¼ 92), no formal evaluation
against eligible reference standard (n¼ 86), study on pregnant
women or congenital malaria (n¼ 52), duplicates (n¼ 26),
laboratory study on in vitro cultured samples (n¼ 23), not
enough data to derive 2� 2 tables (n¼ 19), non-endemic
cases (n¼ 18), full text could not be derived (n¼ 16), language
barrier (Chinese, Russian, Greek, Japanese) (n¼ 13), review,
editorial, letter, case report or erratum (n¼ 9).
Additional file 2 lists the characteristics of the 76 studies
that were finally included in the review9,20–94. All studies
were published between 1992 and 2014 and covered at least
72 different endemic locations in 32 countries. Studies were
conducted in Asia (n¼ 44), Sub-Saharan Africa (n¼ 21), both
Asia and Africa (n¼ 2) and South-America (n¼ 9).
The molecular tests in most studies were performed in the
country where study participants were recruited (n¼ 56). In
12 studies, samples were sent to non-endemic countries to
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 3
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

perform the molecular assays. In four studies, the molecular
test was performed both in the study country and a non-
endemic setting. In two studies, the molecular test was
performed in another endemic country and in two studies the
test location was unknown.
There were 13 evaluations on Plasmodium falciparum
only, 4 on Plasmodium vivax only and 12 were genus-specific.
The remainder of the assays was multiplex systems, of which
16 detected P. falciparum, P. vivax, Plasmodium ovale and
Plasmodium malariae. None of the studies specifically
investigated the presence of Plasmodium knowlesi infections.
There were not enough studies to perform subgroup analyses
of the different species to determine whether a difference in
test accuracy exists between the different species, most
notably P. falciparum and P. vivax. The most referenced PCR
was that of Snounou et al.95
Methodological quality of included studies
The quality assessment results are presented in Figure 2. An
adequate assessment of study quality was often impossible
due to incomplete reporting.
In the domain of patient selection, most studies (n¼ 55)
did not state whether they enrolled a consecutive or random
sample of patients. None of the studies had a case–control
design, as this was an exclusion criterion. In four studies, both
suspected and confirmed cases were included24,26,28,71. There
were concerns about applicability in two studies that included
suspected cases instead of individual patients51,73, implying
that in the case of multiple visits during the study period,41
test result per patient could be included in the analysis. Only
nineteen29,34,41,45,49,52–56,68,74,75,77–79,81,82,87 studies reported
that the readers of the index test were blinded and twenty-
four9,28,29,31,41,45,46,49,50,52,54–56,64,68,70,74,77,80–82,87,88,92 stu-
dies reported that the readers of the reference test were
blinded. For the remaining studies, it was unclear whether
the index test or reference standard was performed
blinded to other test results. Only 16 studies reported
that microscopy was performed by at least two independ-
ent microscopists reading 100 fields or
more20,22,30,33,34,41,43,44,55,57,80,82,83,85,86,92. The quality of
microscopy was unknown for the other studies because the
number of examined fields was not reported, there was only
one microscopist or the number of microscopists was unclear,
Figure 1. Flow chart of selection procedure.Of the 76 studies in the review, 54 could beincluded in the meta-analysis.
4 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

or the independency of microscopists was unknown. The
majority of studies (n¼ 45) reported the use of expert,
research, routine, conventional or field microscopy. There was
little consensus between studies on the nomenclature and
characteristics of different types of microscopy, implying that
no quality-based distinction between studies can be made
based on the reported type of microscopy alone. A cycle
threshold discriminating between positive and negative test
results is applicable only to the real-time PCR assays, which
was clearly pre-specified in 5 of 17 studies evaluating a real-
time PCR21,33,47,74,87.
In the domain of flow and timing, one study showed high
risk of differential verification bias58, and three studies
excluded 410% of patients from the analysis, without
providing reasons31,44,69. Partial verification bias was always
avoided.
Findings
Of the 76 studies in the review, 54 were included in the meta-
analysis. Summary estimates of sensitivity and specificity of
these 54 studies are presented in Figures 3–7. Fourteen
studies reported accuracy data of a test for which an
insufficient number of 2� 2 tables was available to perform
meta-analysis. These data are presented in Figures 8–10.
Another eight studies were excluded from the meta-analysis
because only part of the 2� 2 tables could be completed
(n¼ 1)46, or because they had a high risk of bias
(n¼ 7)58,24,28,71,31,44,69. The effect on the summary estimates
of sensitivity and specificity was systematically examined and
in most cases they remained essentially unchanged. In case
summary estimates changed after exclusion of these studies,
the differences are discussed in the sections below.
PCR versus reference standard microscopy
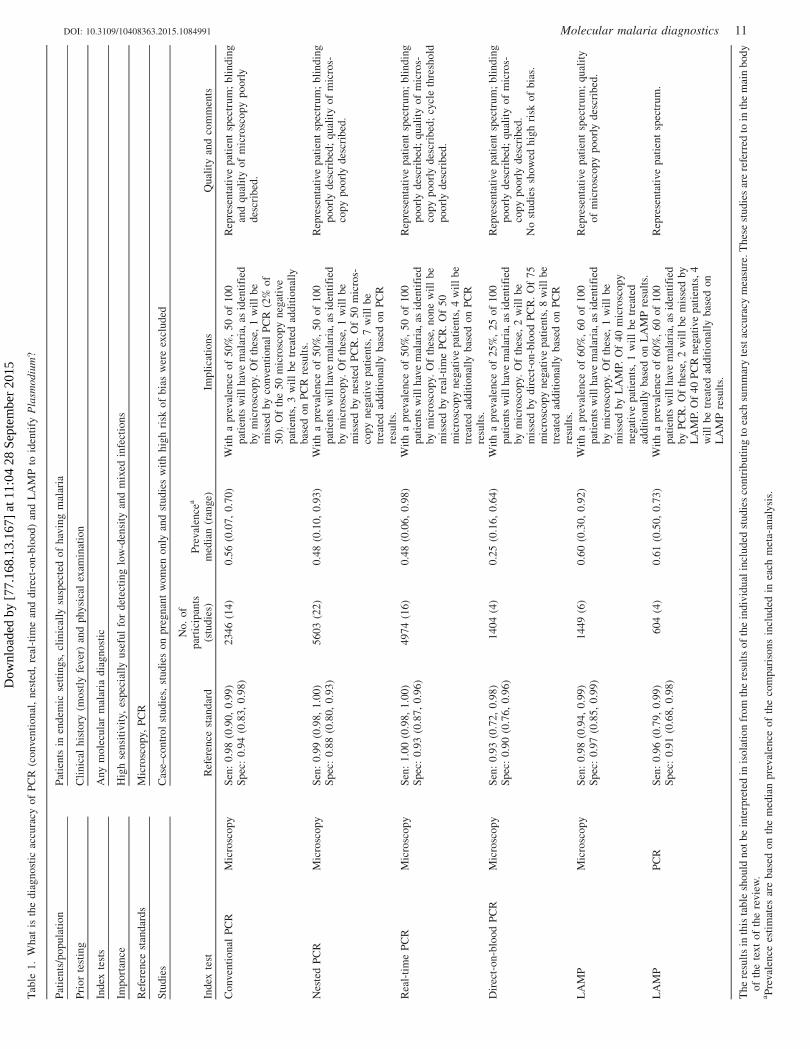
Summary estimates of sensitivity and specificity of PCR
after meta-analysis and their interpretation are presented
in Table 1.
Conventional PCR
Conventional PCR was defined as a PCR containing one or
more primer sets for the detection of Plasmodium, based on a
single reaction and a gel-electrophoresis based read-out. The
assays had either a single- or a multiplex format and most
often used the 18S rRNA gene, but some selected merozoite
surface protein-1 (msp-1)58 or msp-253 as a target. For five
studies, the target gene was not stated31,57,73,76,85.
Figure 2. Methodological quality assessmentof the 76 studies included in the review. Dataare presented for risk of bias and concernsregarding applicability domains. Stacked barsrepresent for each risk of bias quality item thepercentage of studies scored by the authors ashigh, unclear or low quality. Concernsregarding applicability are also presented instacked bars, showing low, unclear or highconcerns.
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 5
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

Nineteen studies evaluated conventional PCR against
microscopy, but five were excluded from the meta-analysis
because patients were not enrolled in a consecutive or random
way (n¼ 1)28, there was a high risk of differential verification
bias (n¼ 1)58, not all patients were included in the analysis
(n¼ 2)31,44, or not enough data to complete 2� 2 tables was
available (n¼ 1)46.
The summary estimates for sensitivity and specificity of
the 14 studies included in the meta-analysis were 98% (95%
CI: 90–99) and 94% (95% CI: 83–98), respectively (Figure 3
and Table 1). When the five studies excluded based on the
quality assessment were included in the analysis, summary
estimates for sensitivity and specificity were 96% (95% CI:
88–99) and 97% (95% CI: 90–99), respectively. Of the 14
studies included in the meta-analysis, one evaluated the
accuracy of microscopy and used PCR as the reference
standard, but presented data in such a way that sensitivity and
specificity of PCR could be derived90. There was no
difference in accuracy between studies performed in
Asia22,25,30,36,38,58,73,90 and Africa42,53,62,76,80. Insufficient
data were available to perform subgroup analyses on the
quality of microscopy.
Figure 3. Forest plots of sensitivity and specificity of conventional PCR with microscopy as a reference standard. Squares represent values forsensitivity and specificity, bars show the 95% CI. *Test comparison not included in the meta-analysis, due to high risk of bias or incomplete 2� 2tables. **Two different assays were evaluated in one study.
Figure 4. Forest plots of sensitivity and specificity of real-time PCR with microscopy as a reference standard. Squares represent values for sensitivityand specificity, bars show the 95% CI. *Test comparison not included in the meta-analysis, because of incomplete 2� 2 tables. ** Two different assayswere evaluated in one study; the first P. falciparum specific, the second P. vivax specific.
6 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015
Real-time PCR
Real-time PCR was defined as a single- or multiplex PCR
whereby detection takes place either through a non-specific
fluorescent dye intercalating with double-stranded DNA, or
through sequence-specific fluorescent labeled DNA probes
hybridizing with their complementary sequence. Of the 17
studies using real-time PCR, eight used SYBR Green or
EvaGreen dye21,30,34,40,60,74,75,87 and nine used TaqMan,
minor groove binding (MGB) or fluorescence resonance
energy transfer (FRET) probes32,33,37,43,46,47,81,86,88 for detec-
tion. The 18S rRNA gene was the most frequently used target,
only one study used cytochrome-b34 and one study used four
different target genes for the four species the assay detected;
aquaglyceroporin (AQP), enoyl-acyl carrier protein reductase
(ECPR), p25 ookinate surface protein (Po25) and circum-
sporozoite (CS)87. No difference in accuracy was observed
when comparing dye- or probe-based assays or target genes.
One study evaluating real-time PCR against microscopy
was excluded from the meta-analysis because not enough data
was available to derive 2� 2 tables46. The summary estimates
for sensitivity and specificity of the remaining 16 studies
included in the meta-analysis were 100% (95% CI: 98–100)
and 93% (95% CI: 87–96), respectively (Figure 4 and
Table 1). Of those 16 studies, 9 did not evaluate the accuracy
of the real-time PCR in the original paper, but rather used it as
a reference standard. However, sufficient data were presented
to derive diagnostic accuracy of the real-time PCR21,32–
34,40,47,60,74,75. There was no difference in accuracy between
studies performed in Asia21,30,32–34,37,40,43,47,81,87 and
Africa60,74,75,88, nor between studies with good and unknown
quality of microscopy.
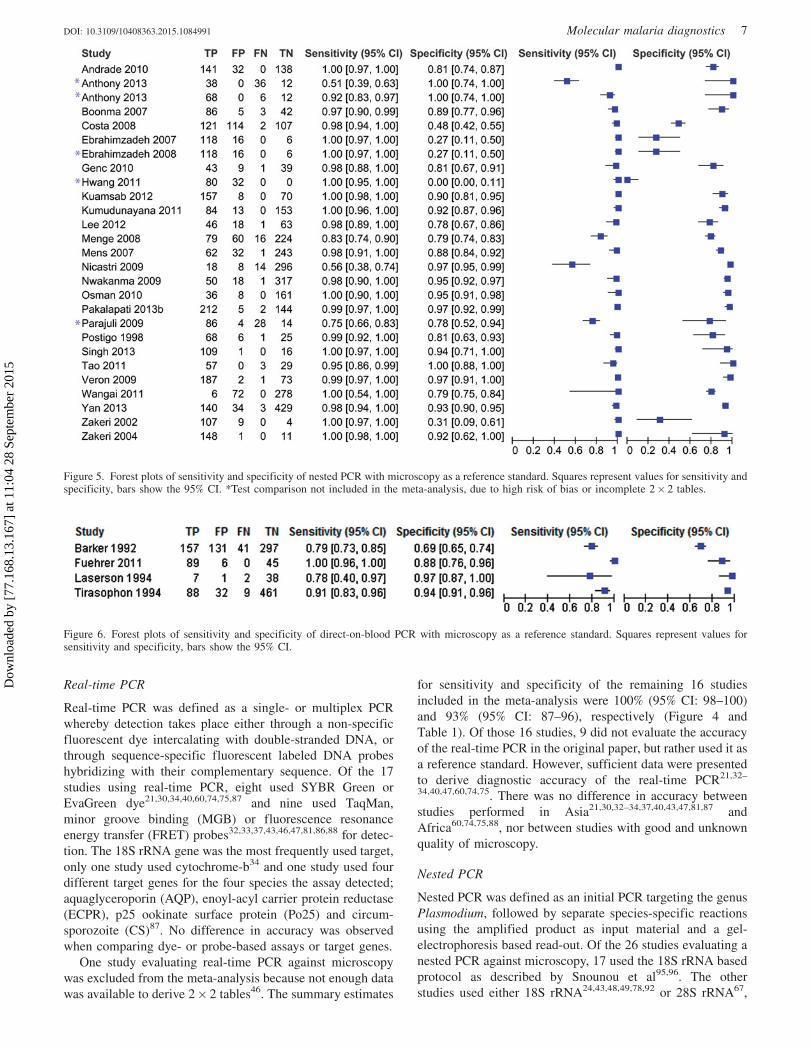
Nested PCR
Nested PCR was defined as an initial PCR targeting the genus
Plasmodium, followed by separate species-specific reactions
using the amplified product as input material and a gel-
electrophoresis based read-out. Of the 26 studies evaluating a
nested PCR against microscopy, 17 used the 18S rRNA based
protocol as described by Snounou et al95,96. The other
studies used either 18S rRNA24,43,48,49,78,92 or 28S rRNA67,
Figure 5. Forest plots of sensitivity and specificity of nested PCR with microscopy as a reference standard. Squares represent values for sensitivity andspecificity, bars show the 95% CI. *Test comparison not included in the meta-analysis, due to high risk of bias or incomplete 2� 2 tables.
Figure 6. Forest plots of sensitivity and specificity of direct-on-blood PCR with microscopy as a reference standard. Squares represent values forsensitivity and specificity, bars show the 95% CI.
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 7
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

dihydrofolate reductase (dhfr)24 or Plasmodium falciparum
multidrug resistance protein-1 (pfmdr-1)89 as target genes. No
difference in accuracy was observed between assays using
different target genes.
Four studies evaluating nested PCR to microscopy were
excluded because patients were not enrolled in a consecutive
or random way (n¼ 1)24, not all patients were included in the
analysis (n¼ 1)69, not enough data to complete 2� 2 tables
was available (n¼ 1)46 or the same data was presented in
another study within the meta-analysis (n¼ 1)20.
The summary estimates for sensitivity and specificity of
the 22 studies included in the meta-analysis were 99% (95%
CI: 98–100) and 88% (95% CI: 80–93), respectively (Figure 5
and Table 1). When the four studies excluded based on the
quality assessment were included in the analysis, summary
estimates for sensitivity and specificity remained the same. Of
the 22 studies included in the meta-analysis, 6 did not
evaluate the accuracy of the nested PCR in the original paper,
but rather used it as a reference standard and presented data to
derive sensitivity and specificity23,48,49,59,64,92. There was no
difference in accuracy between studies performed in
Asia30,39,43,48,49,67,78,83,92–94, Africa52–54,59,61,64,89 and South-
America23,35,72,86. Insufficient data were available to perform
subgroup analyses on the quality of microscopy.
Direct-on-blood PCR
Four studies evaluated a direct-on-blood PCR assay with
microscopy as a reference standard27,41,51,84. These assays
circumvent the need for DNA extraction and are based on
either conventional or nested PCR, as defined above.
The summary estimates for sensitivity and specificity were
93% (95% CI: 72–98) and 90% (95% CI: 76–96), respectively
(Figure 6 and Table 1). One study compared direct-on-blood
PCR to nested PCR, next to microscopy41. In this study,
sensitivity when using microscopy as a reference standard
Figure 7. Forest plots of sensitivity and specificity of LAMP with microscopy and PCR as reference standards. Squares represent values for sensitivityand specificity, bars show the 95% CI. *Test comparison not included in the meta-analysis, due to high risk of bias. **Multiple evaluations per studywith the same assay but different extraction method or read-out, whereby studies with **were excluded from the meta-analysis. The includedevaluations are based on a heat-treatment extraction method and a visual read-out.
Figure 8. Forest plots of sensitivity and specificity of PCR with a composite reference standard. Squares represent values for sensitivity and specificity,bars show the 95% CI. *Studies evaluating PCRs based on different target genes against a molecular composite reference standard of those PCRs.Target genes were P. falciparum chloroquine resistance transporter (pfcrt), 18S rRNA, merozoite surface protein-2 (msp-2), merozoite surface protein-1(msp-1), stevor, merozoite surface protein-2 (msp-2) and 18S rRNA, respectively. **Studies evaluating a PCR against a composite reference standard ofPCR, microscopy and an RDT. Target genes were stevor and 18S rRNA, respectively.
8 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

was 100% (95% CI: 96–100) and specificity 88% (95% CI:
76–96). When nested PCR was used as a reference standard,
sensitivity remained the same and specificity increased to
94% (95% CI: 83–99).
Comparisons
The summary ROC curve in Figure 11 presents the summary
estimates of conventional, real-time, nested and direct-on-
blood PCR compared to microscopy. The 95% CIs overlap
considerably, which may imply that the true accuracy of the
four PCR-based methods is very much alike. However,
conventional PCR showed considerable variation in its
sensitivity across studies, ranging from 51 to 100%
(Figure 3). Nested and real-time PCR on the other hand
showed consistently high sensitivity, with ranges of 56%
(as a single outlier) to 100% and 95 to 100%, respectively
(Figures 4 and 5).
The summary sensitivity of real-time PCR is slightly
higher than that of conventional PCR (p¼ 0.02).
Nevertheless, the summary estimates for sensitivity are very
similar, with 100%, 98% and 99% for real-time, conventional
and nested PCR, respectively. The specificity of nested PCR
(88%) appeared to be slightly lower than that of the other two
techniques (94% and 93% for conventional and real-time
PCR, respectively). Based on the available data, however, it is
not possible to conclude whether this was indeed due to a
larger number of false positives, or to sub-microscopic
infections detected by nested PCR. The sensitivity of direct-
on-blood PCR appeared to be slightly lower than that of the
other three techniques, but specificity was found to be similar.
There was only one study directly comparing nested PCR and
Figure 9. Forest plots of sensitivity and specificity of other molecular diagnostics with microscopy as a reference standard. Squares represent values forsensitivity and specificity, bars show the 95% CI.
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 9
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

real-time PCR to microscopy and to each other86. The two
PCRs were in complete agreement and both had a sensitivity
of 99% (95% CI: 97–100) and a specificity of 97% (95% CI:
91–100), compared to microscopy.
Four studies compared PCR to a composite reference
standard, combining the results of different assays into one
‘‘true’’ outcome63,65,66,68. Summary estimates of sensitivity
and specificity are presented in Figure 8. Composites consist
of either molecular data of different PCRs65,66 or a combin-
ation of microscopy, RDT and/or PCR results63,68. Because of
their different reference standards, these studies could neither
be included in the meta-analysis, nor can their accuracy be
compared to each other as all four used a different composite.
Finally, no clear difference in accuracy regarding the year
of publication was observed for any of the PCR-based assays.
This suggests that older techniques do not necessarily perform
worse than newer ones and that accuracy is not inevitably
lower in older compared to more recent studies.
LAMP versus reference standards microscopy and PCR
LAMP is a rather novel semi-isothermal amplification
technique that requires two temperatures for amplification.
It has been first described by Notomi et al.7 Four primers,
recognizing six different target sequences are used and
amplification usually takes less than an hour. The read-out
is based on fluorescence, turbidity or sometimes gel electro-
phoresis45,70,79. Only a UV light source is required for a visual
fluorescence based read-out, which together with the fact that
no PCR machine is required, is one of the key characteristics
for LAMP to be considered field applicable45,83. However,
there is still need for DNA extraction.
Seven studies evaluated LAMP against a reference stand-
ard of microscopy and five against PCR, of which three
compared LAMP to both methods52,71,83. One study was
excluded from the meta-analysis, because patients were not
enrolled in a consecutive or random way71. The summary
estimates for sensitivity and specificity of the six studies
evaluating LAMP compared to microscopy were 98% (95%
CI: 94–99) and 97% (95% CI: 85–99), respectively (Figure 7
and Table 1).
When using PCR as reference standard, of four eligible
studies, two evaluated different extraction- and read-out
methods on the same sample set45,70. We chose to include
the comparisons that shared most characteristics between the
four studies in the meta-analysis. The comparisons using a
simple heat-treatment based extraction method and a visual
readout, either based on fluorescence or turbidity, were
therefore included. Evaluations using commercial extraction
kits and/or a read-out by gel-electrophoresis were excluded
from the meta-analysis when a test based on heat-treatment
extraction and/or a visual read-out was evaluated in the same
study (Figure 7). Summary estimates for sensitivity and
specificity of the four comparisons included in the meta-
analysis were 96% (95% CI: 79–99) and 91% (95% CI:
68–98), respectively.
The summary ROC curve in Figure 12 presents the
summary estimates of LAMP versus microscopy and PCR.
When choosing PCR as a reference standard, the confidence
interval is extremely broad, overlapping entirely with the
Figure 10. Forest plots of sensitivity and specificity of other molecular diagnostics with PCR as a reference standard. Squares represent values forsensitivity and specificity, bars show the 95% CI.
10 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015
Tab
le1
.W
hat
isth
ed
iag
no
stic
accu
racy
of
PC
R(c
onven
tio
nal
,n
este
d,
real
-tim
ean
dd
irec
t-o
n-b
loo
d)
and
LA
MP
toid
enti
fyP
lasm
od
ium
?
Pat
ien
ts/p
op
ula
tio
nP
atie
nts
inen
dem
icse
ttin
gs,
clin
ical
lysu
spec
ted
of
hav
ing
mal
aria
Pri
or
test
ing
Cli
nic
alh
isto
ry(m
ost
lyfe
ver
)an
dp
hysi
cal
exam
inat
ion
Ind
exte
sts
Any
mo
lecu
lar
mal
aria
dia
gn
ost
ic
Imp
ort
ance
Hig
hse
nsi
tiv
ity,
esp
ecia
lly
use
ful
for
det
ecti
ng
low
-den
sity
and
mix
edin
fect
ion
s
Ref
eren
cest
and
ard
sM
icro
sco
py,
PC
R
Stu
die
sC
ase–
con
tro
lst
ud
ies,
stu
die
so
np
reg
nan
tw
om
eno
nly
and
stu
die
sw
ith
hig
hri
sko
fb
ias
wer
eex
clu
ded
Ind
exte
stR
efer
ence
stan
dar
d
No
.o
fp
arti
cip
ants
(stu
die
s)P
reval
ence
a
med
ian
(ran
ge)
Imp
lica
tio
ns
Qu
alit
yan
dco
mm
ents
Co
nven
tio
nal
PC
RM
icro
sco
py
Sen
:0
.98
(0.9
0,
0.9
9)
Sp
ec:
0.9
4(0
.83
,0
.98
)2
34
6(1
4)
0.5
6(0
.07
,0
.70
)W
ith
ap
reval
ence
of
50
%,
50
of
10
0p
atie
nts
wil
lh
ave
mal
aria
,as
iden
tifi
edby
mic
rosc
op
y.O
fth
ese,
1w
ill
be
mis
sed
by
conven
tio
nal
PC
R(2
%o
f5
0).
Of
the
50
mic
rosc
op
yn
egat
ive
pat
ien
ts,
3w
ill
be
trea
ted
add
itio
nal
lyb
ased
on
PC
Rre
sult
s.
Rep
rese
nta
tive
pat
ien
tsp
ectr
um
;b
lin
din
gan
dqu
alit
yo
fm
icro
sco
py
po
orl
yd
escr
ibed
.
Nes
ted
PC
RM
icro
sco
py
Sen
:0
.99
(0.9
8,
1.0
0)
Sp
ec:
0.8
8(0
.80
,0
.93
)5
60
3(2
2)
0.4
8(0
.10
,0
.93
)W
ith
ap
reval
ence
of
50
%,
50
of
10
0p
atie
nts
wil
lh
ave
mal
aria
,as
iden
tifi
edby
mic
rosc
op
y.O
fth
ese,
1w
ill
be
mis
sed
by
nes
ted
PC
R.
Of
50
mic
ros-
cop
yn
egat
ive
pat
ien
ts,
7w
ill
be
trea
ted
add
itio
nal
lyb
ased
on
PC
Rre
sult
s.
Rep
rese
nta
tive
pat
ien
tsp
ectr
um
;b
lin
din
gp
oo
rly
des
crib
ed;
qu
alit
yo
fm
icro
s-co
py
po
orl
yd
escr
ibed
.
Rea
l-ti
me
PC
RM
icro
sco
py
Sen
:1
.00
(0.9
8,
1.0
0)
Sp
ec:
0.9
3(0
.87
,0
.96
)4
97
4(1
6)
0.4
8(0
.06
,0
.98
)W
ith
ap
reval
ence
of
50
%,
50
of
10
0p
atie
nts
wil
lh
ave
mal
aria
,as
iden
tifi
edby
mic
rosc
op
y.O
fth
ese,
no
ne
wil
lb
em
isse
dby
real
-tim
eP
CR
.O
f5
0m
icro
sco
py
neg
ativ
ep
atie
nts
,4
wil
lb
etr
eate
dad
dit
ion
ally
bas
edo
nP
CR
resu
lts.
Rep
rese
nta
tive
pat
ien
tsp
ectr
um
;b
lin
din
gp
oo
rly
des
crib
ed;
qu
alit
yo
fm
icro
s-co
py
po
orl
yd
escr
ibed
;cy
cle
thre
sho
ldp
oo
rly
des
crib
ed.
Dir
ect-
on
-blo
od
PC
RM
icro
sco
py
Sen
:0
.93
(0.7
2,
0.9
8)
Sp
ec:
0.9
0(0
.76
,0
.96
)1
40
4(4
)0
.25
(0.1
6,
0.6
4)
Wit
ha
pre
val
ence
of
25
%,
25
of
10
0p
atie
nts
wil
lh
ave
mal
aria
,as
iden
tifi
edby
mic
rosc
op
y.O
fth
ese,
2w
ill
be
mis
sed
by
dir
ect-
on
-blo
od
PC
R.
Of
75
mic
rosc
op
yn
egat
ive
pat
ien
ts,
8w
ill
be
trea
ted
add
itio
nal
lyb
ased
on
PC
Rre
sult
s.
Rep
rese
nta
tive
pat
ien
tsp
ectr
um
;b
lin
din
gp
oo
rly
des
crib
ed;
qu
alit
yo
fm
icro
s-co
py
po
orl
yd
escr
ibed
.N
ost
ud
ies
show
edh
igh
risk
of
bia
s.
LA
MP
Mic
rosc
op
yS
en:
0.9
8(0
.94
,0
.99
)S
pec
:0
.97
(0.8
5,
0.9
9)
14
49
(6)
0.6
0(0
.30
,0
.92
)W
ith
ap
reval
ence
of
60
%,
60
of
10
0p
atie
nts
wil
lh
ave
mal
aria
,as
iden
tifi
edby
mic
rosc
op
y.O
fth
ese,
1w
ill
be
mis
sed
by
LA
MP.
Of
40
mic
rosc
op
yn
egat
ive
pat
ien
ts,
1w
ill
be
trea
ted
add
itio
nal
lyb
ased
on
LA
MP
resu
lts.
Rep
rese
nta
tive
pat
ien
tsp
ectr
um
;qu
alit
yo
fm
icro
sco
py
po
orl
yd
escr
ibed
.
LA
MP
PC
RS
en:
0.9
6(0
.79
,0
.99
)S
pec
:0
.91
(0.6
8,
0.9
8)
60
4(4
)0
.61
(0.5
0,
0.7
3)
Wit
ha
pre
val
ence
of
60
%,
60
of
10
0p
atie
nts
wil
lh
ave
mal
aria
,as
iden
tifi
edby
PC
R.
Of
thes
e,2
wil
lb
em
isse
dby
LA
MP.
Of
40
PC
Rn
egat
ive
pat
ien
ts,
4w
ill
be
trea
ted
add
itio
nal
lyb
ased
on
LA
MP
resu
lts.
Rep
rese
nta
tive
pat
ien
tsp
ectr
um
.
Th
ere
sult
sin
this
tab
lesh
ou
ldn
ot
be
inte
rpre
ted
inis
ola
tio
nfr
om
the
resu
lts
of
the
ind
ivid
ual
incl
ud
edst
ud
ies
con
trib
uti
ng
toea
chsu
mm
ary
test
accu
racy
mea
sure
.T
hes
est
ud
ies
are
refe
rred
toin
the
mai
nb
od
yo
fth
ete
xt
of
the
revie
w.
aP
reval
ence
esti
mat
esar
eb
ased
on
the
med
ian
pre
val
ence
of
the
com
par
iso
ns
incl
ud
edin
each
met
a-an
alysi
s.
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 11
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

confidence interval of reference standard microscopy, indicat-
ing a vast amount of heterogeneity.
Other molecular diagnostics
Apart from the most commonly used PCR assays and LAMP,
other molecular tests have been developed and evaluated, but
meta-analysis could not be performed because of the limited
number of published papers on these techniques. Extracted
diagnostic accuracy data are presented in Figures 9 and 10.
Eight different assays were evaluated against microscopy, of
which three studies also compared the test under evaluation
with a PCR-based assay33,54,82.
The molecular tools in this section were developed to
simplify existing assays while not compromising on accuracy,
in an attempt to make them more suitable as (near) PoC
diagnostics or for screening asymptomatic individuals in
malaria control or elimination programs.
The PCR-NALFIA uses a lateral flow device as a read-out
system instead of gel-electrophoresis, thereby reducing
equipment requirements and hazardous waste. PCR-
NALFIA is available as a DNA- or direct-on-blood assay,
whereby the latter circumvents the need of DNA extrac-
tion9,55,56. Sensitivity ranges from 87% (95% CI: 79–93) to
95% (95% CI: 89–98), specificity from 82% (95% CI: 76–88)
to 95% (95% CI: 93–97).
A semi-nested multiplex PCR is a simplification of the
well-performing nested PCR, transforming it to a single-tube
assay detecting the main four Plasmodium species and
thereby reducing time and reagents. Sensitivity ranges from
94% (95% CI: 80–99) to 98% (95% CI: 93–100), specificity
from 98% (95% CI: 96–100) to 100% (95% CI: 92–100)26,29.
The RNA-hybridization assay is an isothermal direct-on-
blood assay in a 96-well format, with a chemiluminescence
based read-out. It requires an overnight incubation step.
Reported sensitivity and specificity, compared to microscopy,
are 100% (95% CI: 95–100) and 98% (95% CI: 94–100),
respectively. When using PCR as a reference standard,
sensitivity remains 100% (95% CI: 82–100) and specificity
increases to 100% (95% CI: 97–100)33. The possible appli-
cation of the RNA-hybridization assay for screening asymp-
tomatic populations in elimination settings is specifically
discussed by the authors.
The PCR-enzyme-linked immunosorbent assay (PCR-
ELISA) is a genus specific PCR-based assay, whereby the
target is immobilized by species-specific probes and semi-
quantitatively detected by a colorimetric assay. Assay time is
relatively short and no hazardous waste is produced. Reported
sensitivity and specificity are 97% (95% CI: 92–99) and 96%
(95% CI: 86–99), respectively50.
Nucleic acid sequence-based amplification (NASBA) is a
semi-quantitative isothermal amplification technique, with a
Figure 11. Summary ROC plot of sensitivityand specificity of conventional, real-time,nested and direct-on-blood PCR withmicroscopy as a reference standard.Sensitivity is plotted against 1-specificity,allowing for the comparison of both param-eters for multiple tests at the same time.Rounds represent summary estimates forsensitivity and specificity. Unbroken linesrepresent summary curves, dotted lines 95%CI around the summary estimates. The 95%CI for direct-on-blood PCR is large due to alimited number of studies. For conventionaland real-time PCR, the 95% CIs only justoverlap, while that of conventional PCR ismuch wider than that of real-time PCR,resulting in a significant difference in sensi-tivity (p¼ 0.02). Other summary estimates donot differ significantly.
12 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

fluorescence-based read-out. Compared to microscopy,
reported sensitivity and specificity are 100% (95% CI: 94–
100) and 90% (95% CI: 86–93), respectively. When using
PCR as a reference standard, reported sensitivity is 94% (95%
CI: 87–98) and specificity 99% (95% CI: 96–100)54.
Ligase detection reaction-fluorescent microsphere assay
(LDR-FMA) uses genus-specific PCR amplicons as input
material for a species-specific multiplex ligase detection
reaction with a fluorescence-based read-out. For a detailed
description of the method, see McNamara et al.97 Reported
sensitivity and specificity are 91% (95% CI: 83–96) and 71%
(95% CI: 65–76), respectively53. The possible application of
LDR-FMA for monitoring prevalence in low transmission
areas is specifically stated.
Photo-induced electron transfer-PCR (PET-PCR) is a real-
time PCR using self-quenching primers, which reduces the
number of reagents as compared to other real-time PCR
assays. Reported sensitivity and specificity compared to
microscopy are 100% (95% CI: 72–100) and 95% (95% CI:
91–97), respectively. When using nested PCR as a reference
standard, sensitivity remains 100% (95% CI: 87-100) and
specificity increases to 100% (95% CI: 97–100)82. The
authors specifically state the possible use of PET-PCR for
large-scale screening in control or elimination programs.
The reverse transcriptase PCR detects RNA next to
DNA, to increase sensitivity. Reported sensitivity and
specificity are 100% (95% CI: 94–100) and 6% (95%
CI: 3–12), respectively88. A possible application in detecting
the asymptomatic reservoir within a population is mentioned.
Discussion
Key findings
This review shows that conventional, nested and real-time
PCR all have a very high sensitivity for detecting malaria
when using microscopy as the reference standard (98%, 99%
and 100%, respectively). When comparing the summary
sensitivity of conventional PCR to that of real-time PCR, a
significant difference was found (p¼ 0.02). This can be
explained by the fact that the 95% CIs around the summary
estimates only just overlap, while real-time PCR has a very
narrow CI (98–100) compared to conventional PCR (90–99).
This difference is in most cases clinically negligible as both
sensitivities are very high and lie close together. Specificity
was lowest for nested PCR (88%) and slightly higher in
conventional and real-time PCR (94% and 93%, respectively).
Low-specificity values may partly be explained by the fact
that microscopy is considered to be an imperfect reference
standard, with a LoD higher than that of the molecular index
test. Some false positive test results may therefore actually be
true positives with sub-microscopic parasitaemia.
The sensitivity of the direct-on-blood PCR (93%) was
found to be slightly lower than that of the other PCRs, and
specificity was similar (90%). The input material could be a
Figure 12. Summary ROC plot of sensitivityand specificity of LAMP with microscopyand PCR as a reference standard. Sensitivityis plotted against 1-specificity, allowing forthe comparison of both parameters for mul-tiple tests at the same time. Open circles anddiamonds represent estimates for individualstudies with the size being proportional tosample size. Rounds represent summaryestimates for sensitivity and specificity.Unbroken lines represent summary curves,dotted lines 95% CI around the summaryestimates. The 95% CI for LAMP with PCRas a reference standard is large due to alimited number of, essentially heterogeneous,studies.
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 13
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

possible explanation for the lower sensitivity, as blood is
known to contain PCR inhibitors98 and DNA is likely to be
more concentrated in an extracted sample than in whole
blood. Direct-on-blood PCR has the valuable advantage that
no DNA extraction is required, saving both time and reagents
and making the step to molecular PoC diagnostics easier.
The sensitivity of LAMP versus microscopy (98%) was
comparable to that of LAMP versus PCR (96%). Specificity
was high when comparing LAMP to microscopy (97%), but
appeared to be somewhat lower when compared to PCR
(91%). LAMP was expected to show higher specificity using
PCR as a reference standard, as most sub-microscopic
infections will not be marked as false positive by PCR.
However, it should be taken into account that the meta-
analysis of LAMP versus PCR was based on only four,
extremely heterogeneous studies and that this analysis con-
sisted of comparisons using heat-treatment extraction and
visual read-out only. One study showed a high agreement
between the accuracy of PCR and LAMP when compared to
microscopy, with LAMP performed under field conditions83.
Other molecular tests that were not included in the meta-
analysis were: PCR-NALFIA, semi-nested multiplex PCR,
RNA hybridization assay, PCR-ELISA, NASBA, LDR-FMA,
PET-PCR and reverse transcriptase PCR. Sensitivity was
generally high, with a range of 87–100% when microscopy
was used as a reference standard and 94–100% with reference
standard PCR. Specificity was high with PCR as a refer-
ence standard (range 94–100%), but more variable for
reference standard microscopy, with an outlier of 6% for
reverse transcriptase PCR. This outlier could possibly be
explained by the detection of RNA next to DNA. NASBA, the
RNA-hybridization assay and PET-PCR were evaluated
against both microscopy and real-time or nested PCR. In all
three assays specificity was higher when using PCR as a
reference standard, compared to reference standard micros-
copy (Figures 9 and 10). This confirms that the detection of
sub-microscopic infections by molecular assays may explain
the larger proportion of false positive test results when using
microscopy as a reference standard.
Strengths and weaknesses
Taking into account that microscopy is an imperfect gold
standard, it is assumed that reference laboratory microscopy is
more suitable as a reference standard than routine microscopy
in field settings, due to its higher sensitivity. However, there is
currently no consensus in the reporting of microscopy quality,
and definitions of expert/research microscopy did not always
match the quality criteria as used in this review. Highly
similar quality criteria for microscopy have been used in a
systematic review on the accuracy of malaria RDTs using
microscopy and PCR as reference standards, with the
difference that the reference standard was qualified as poor
instead of unknown when the paper did not describe the use of
a second independent microscopist or when the number of
high power fields was not stated17. In the present review,
sufficient data were only available for real-time PCR to
investigate whether existing heterogeneity could be explained
by the quality of microscopy, which appeared not to be the
case. To determine the usefulness of microscopy as a
reference standard and to enable extensive subgroup analyses
to be done, there is a need for detailed reporting on the quality
of microscopy, describing the equipment and methods used,
the number of microscopists, their independency, training
level, and the procedure in case of discrepant results.
The low specificity of some molecular tools compared to
reference standard microscopy may be explained by the fact
that both types of tests aim to detect two different types of
biomarkers. For example, when parasites adhere to endothe-
lial cells (sequestration), microscopic detection may be
complicated by low levels of parasites in the circulation3,
whereas this should be less problematic for (molecular) tests
with a lower LoD. It can also be hypothesized that parasite
DNA persists in blood during or after treatment and that
therefore the detection of Plasmodium DNA does not
necessarily indicate active infection, but might as well
detect nuclear material from dead or drug-damaged parasites.
However, Jarra and Snounou showed that total DNA clear-
ance takes place between 24 and 48 h after injection of killed
parasites into mice and that nuclear material from dead or
drug-damaged parasites does not contribute significantly to
amplification99. This indicates that results from molecular
tests reflect the presence of living parasites.
While molecular tools are reported to be very sensitive in
detecting low parasite densities, there is some discussion
about the clinical relevance of detecting such low parasit-
aemias, as these infections are often asymptomatic. However,
they play an important role in transmission, especially in low
prevalence areas11. Furthermore, it has been found that the
high sensitivity of PCR also leads to the identification of
more patients with low parasitaemia in symptomatic micros-
copy-negative cases54. The chances of feeling ill due to a sub-
microscopic Plasmodium infection are therefore real, even
though the presence of another cause of fever cannot be
excluded. In this review, we did not assess the influence of
parasite density on accuracy and additional (real-time PCR)
data would be required to do so.
A possibly important confounder that was not taken into
account in this review may be the input volume of blood used
in the molecular assay, which is neither commonly described
nor standardized. This is especially important for correctly
diagnosing patients with low parasite densities, as chances of
not capturing a parasite in a particular sample increase with
decreasing parasitaemia. Recent research using high-volume
real-time PCR (�250 ml input material) shows a 50 times
increase in analytical sensitivity compared to other common
real-time PCR assays100.
Sensitivity of a molecular test is also impacted by copy
number, and stratification of data by DNA and total NA
amplification is therefore of potential interest. For example,
18S rRNA contains about 3500 copies/parasite101, which is
much more than the commonly used 18S rRNA-coding
genes (4–8 copies/parasite)102 or the mitochondrial cyto-
chrome b (20–150 copies/parasite)103, implying that RNA
potentially has a higher analytical sensitivity than DNA. Since
only one study using reverse-transcriptase PCR was included,
no such stratification could be done with the currently
available data.
Prevalence was highly variable between studies (Table 1).
This might have introduced bias in summary estimates of
14 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

sensitivity and specificity, as accuracy may vary with
prevalence104. The results of this review can therefore
not be extrapolated to accuracy in screening asymptom-
atic populations or in febrile non-immune returning travelers.
Most studies were conducted in Asia (58%) and Sub-
Saharan Africa (28%). No difference in accuracy between
continents was found. There was high variability in the
species detected by the index tests and no subgroup analysis
could be done to determine whether a difference in accuracy
exists, especially between P. falciparum and P. vivax. In line
with the presence of both P. falciparum and P. vivax in many
areas in the Asian-Pacific, most assays were multiplex
systems and some presented data in their 2� 2 tables for
each species separately. However, in most studies too few
samples per species were available to calculate sensitivity and
specificity individually and therefore a joined estimate for all
species together was given. Whether a difference in accuracy
between species exists can only be established by studies
designed to separate accuracy by species.
While some commercial real-time PCR kits are available,
thus far they do not appear to be widely used. Most laboratories
developed an in-house assay or used published protocols, often
with small changes to the original method. Therefore, very
little standardization of molecular malaria tests exists,
complicating data comparison between laboratories18. The
results of this review indicate that especially for conventional
and real-time PCR assays, many different protocols are in use.
Studies evaluating nested PCR, on the other hand, refer in most
cases to the method of Snounou et al.95,96 implying that some
of the outliers of low sensitivity cannot be explained by
differences in the original protocol used. Remarkably, espe-
cially for real-time PCR, the fact that many different protocols
are in use did not seem to influence sensitivity. Still,
standardization of commercial tests through FDA approval or
the WHO prequalification program of in vitro diagnostics
would enhance the reliability and comparability of assays and
would reduce the burden of quality assurance on individual
laboratories105. Additionally, even though accuracy of most
molecular assays presented in this review is high, the
experience of laboratory personnel is crucial in achieving
this. Proficiency testing/External Quality Assessment (EQA)
programs would provide insight in the quality of work of
laboratories routinely performing molecular malaria diagnos-
tics106,107. For real-time PCR, guidelines are available pre-
senting the minimum information for publication of
quantitative real-time PCR experiments (MIQE), specifically
addressing the potential to accurately quantify target nucleic
acids108. Their widespread use would increase experimental
transparency and consistency between laboratories performing
real-time PCR.
Implications for practice/further research
Even though it has been shown that PCR is highly sensitive
and specific, the required infrastructure, trained personnel and
costs hamper its implementation in resource-limited settings.
LAMP and other novel molecular tools under development, as
presented in this review, may be suitable alternatives to detect
low-density infections. The different characteristics of these
tests bring advantages for use in resource-limited settings,
related to sample preparation, the amplification process and/
or the read-out of the test.
Simplifying sample preparation reduces sample handling
time and the number of required reagents. There are several
assays that use whole blood or only require simple extraction
methods. PCR-NALFIA can use whole blood as input
material, whereby the need for sample preparation is
completely avoided56. The RNA-hybridization assay requires
lysed red blood cells (RBCs)33 and for LAMP several crude
extraction methods, like heat-treatment70,109 and boil-and-
spin methods45 have been compared to commercial extraction
kits. However, LAMP specificity appears to decrease when
using simplified extraction methods (see Figure 7), indicating
a need for improvement for use in field settings.
Using semi-isothermal amplification methods, LAMP,
NASBA and the RNA-hybridization assay only need two
temperatures for amplification, thereby circumventing the
need for expensive PCR-machines110. Instead, simple heat
blocks or water baths can be used. However, the RNA-
hybridization assay requires an overnight incubation step,
which makes the assay in its current format unsuitable to be
used in PoC settings, where results need to be produced as
soon as possible in order to initiate proper treatment. When
using LAMP or NASBA it would be possible to present
results within hours, but NASBA has the disadvantage that
RNA extraction is required, making it more suitable for
research purposes than as a PoC test.
Traditional gel-electrophoresis read-out systems have the
disadvantage that they need expensive equipment, produce
hazardous waste and usually take at least 45 min. For LAMP,
the read-out can be done visually using a UV-light, which
makes the detection simple and extremely fast. The lateral
flow device as a fast (10 min) read-out system in PCR-
NALFIA is similar to the one used for RDTs, but detects
amplicons instead of antibodies, enabling multiple species to
be detected at the same time using a simple visual read-out.
The detection system of PCR-ELISA is easy and fast, but
requires an ELISA plate reader.
Costs are an important factor when evaluating whether a
test is suitable for a particular purpose or not. This factor was
not included and additional data would be required to get a
complete overview of the costs per assay, including equip-
ment, reagents, labor, training and maintenance. Currently
available overviews mainly include equipment and reagent
costs12,30,109 and do not cover all tests presented in this
review.
The characteristics of a test that are most important in a
certain situation are determined by its intended use (clinical
practice or control/elimination programs) and setting (ranging
from field conditions to reference laboratories)105,111,112. For
clinical practice, besides high accuracy, it is important that
the test is fast, easy to perform on site and robust under
adverse environmental conditions. Currently, LAMP and
PCR-NALFIA are probably the most likely candidates to
meet these characteristics. LAMP for its semi-isothermal
amplification and PCR-NALFIA for using whole blood as
input material. Both have an easy and fast read-out system.
Preferably, no cold chain would be required to store reagents
in final test formats. For the smaller clinics, high-throughput
is less essential and tests will be done mostly for individual
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 15
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

(or small groups of) patients. Species differentiation may be
especially important in areas where P. vivax is present and
treatment regimens are based on the infecting species. Studies
on asymptomatic populations were excluded from this review,
but form an important subgroup for future reviews given the
current focus on malaria screening and elimination programs.
In such a review, it would be important to focus on the
relation between clinical and analytical sensitivity, as the
proportion of low-density infections is likely to be high in
asymptomatic populations and parasite levels below the LoD
of the test under evaluation will lead to false-negative test
results. In these populations, poor analytical sensitivity is
therefore a likely cause of poor clinical sensitivity. In the
present review, studies evaluating clinical accuracy of the
RNA-hybridization assay, LDR-FMA, PET-PCR and reverse
transcriptase PCR specifically mention a possible application
in screening programs in low transmission settings33,53,82,88.
For these programs, high-throughput and superior sensitivity
are crucial. Preferably, the test should be able to discriminate
between the five human infecting Plasmodium species.
However, the delay caused by shipment and analyses of
samples remains a challenge, as all positive cases need to be
traced back and receive treatment as soon as possible. For
elimination settings, portable equipment as described by
Canier et al.113 may therefore be an alternative.
Due to the apparent implementation difficulties associated
with molecular diagnostics, they are unlikely to replace
microscopy or RDTs as first line diagnostics in remote
settings in the near future. However, they may be a powerful
alternative, especially in areas where prevalence is declining,
which increases the need for more sensitive diagnostics, both
in clinical practice and for screening asymptomatic popula-
tions. The further development of (near) PoC diagnostics for
malaria could solve some of the implementation issues.
Conclusions
No important difference in accuracy was found between the
most commonly used PCRs, with most of them having high
sensitivity and specificity, implying that there are no reasons
other than practical ones to choose one technique over the
other. However, summary estimates should not be interpreted
in isolation from the results of the original paper, as
considerable heterogeneity exists, especially in the evalu-
ations of conventional PCR. Alternative diagnostics appear to
be highly accurate as well, with some offering potential to be
used in resource-limited settings.
Future diagnostic accuracy studies should be reported
according to Standards for the Reporting of Diagnostic
Accuracy Studies (STARD) guidelines114, to prevent inad-
equate reporting, maximize comparability and ensure inclu-
sion in the meta-analysis. Direct comparisons of molecular
tests (within-study) would facilitate stronger evidence of
differences in accuracy between tests. Further research on the
implementation of (near) PoC molecular diagnostics and their
potential roadblocks is essential.
Acknowledgements
We would like to thank all authors who kindly provided
additional data not published in the original papers.
Declaration of interest
This study was supported by EU FP7-Health-2013.0-1.
Project no.: 601714. Translation of the direct-on-blood
PCR-NALFIA system into an innovative near point-of-care
diagnostic for malaria (DIAGMAL). J.R. is working on the
development of the direct-on-blood PCR-NALFIA system.
The authors alone are responsible for the content and writing
of this article.
References
1. World Health Organization. Guidelines for the Treatment ofMalaria. 2nd ed. Geneva: World Health Organization, 2010.
2. Wongsrichanalai C, Barcus MJ, Muth S, et al. A review of malariadiagnostic tools: microscopy and rapid diagnostic test (RDT). AmJ Trop Med Hyg 2007;77:119–27.
3. Moody A. Rapid diagnostic tests for malaria parasites. ClinMicrobiol Rev 2002;15:66–78.
4. Murray CK, Gasser RA, Magill AJ, Miller RS. Update on rapiddiagnostic testing for malaria. Clin Microbiol Rev 2008;21:97–110.
5. Schneider P, Wolters L, Schoone G, et al. Real-time nucleic acidsequence-based amplification is more convenient than real-timePCR for quantification of Plasmodium falciparum. J ClinMicrobiol 2005;43:402–5.
6. Berry A, Benoit-Vical F, Fabre R, et al. PCR-based methods to thediagnosis of imported malaria. Parasite 2008;15:484–8.
7. Notomi T, Okayama H, Masubuchi H, et al. Loop-mediatedisothermal amplification of DNA. Nucleic Acids Res 2000;28:E63.
8. Mens PF, Schoone GJ, Kager PA, Schallig HD. Detection andidentification of human Plasmodium species with real-timequantitative nucleic acid sequence-based amplification. Malar J2006;80:5.
9. Mens PF, Amerongen A van, Sawa P, et al. Molecular diagnosis ofmalaria in the field: development of a novel 1-step nucleic acidlateral flow immunoassay for the detection of all 4 humanPlasmodium spp. and its evaluation in Mbita, Kenya. DiagnMicrobiol Infect Dis 2008;61:421–7.
10. Vasoo S, Pritt BS. Molecular diagnostics and parasitic disease.Clin Lab Med 2013;33:461–503.
11. Okell LC, Bousema T, Griffin JT, et al. Factors determining theoccurrence of submicroscopic malaria infections and theirrelevance for control. Nat Commun 2012;3:1–9.
12. Cordray MS, Richards-Kortum RR. Review: emerging nucleicacid-based tests for point-of-care detection of malaria. Am J TropMed Hyg 2012;87:223–30.
13. Desai M, ter Kuile FO, Nosten F, et al. Epidemiology and burdenof malaria in pregnancy. Lancet Infect Dis 2007;7:93–104.
14. Kattenberg JH, Ochodo EA, Boer KR, et al. Systematic review andmeta-analysis: rapid diagnostic tests versus placental histology,microscopy and PCR for malaria in pregnant women. Malar J2011;10:321.
15. Rutjes AWS, Reitsma JB, Di Nisio M, et al. Evidence of bias andvariation in diagnostic accuracy studies. Can Med Assoc J 2006;174:469–76.
16. World Health Organization. Basic Malaria Microscopy, Part ILearner’s Guide. 2nd ed. Geneva: World Health Organization,2010:1–88.
17. Abba K, Deeks J, Olliaro P, et al. Rapid diagnostic tests fordiagnosing uncomplicated P. falciparum malaria in endemiccountries (review). Cochrane Database Syst Rev 2012;7:1–275.
18. UNITAID. Malaria Diagnostic Technology Landscape. Geneva:UNITAID, 2011:1–96.
19. Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: arevised tool for the quality assessment of diagnostic accuracystudies. Ann Intern Med 2011;155:529–36.
20. Ebrahimzadeh A, Fazaeli A. The risk of re-emergence ofPlasmodium malariae in South-East of Iran as detected bynested polymerase chain reaction. Asian J Epidemiol 2008;1:47–52.
21. Alam MS, Mohon AN, Mustafa S, et al. Real-time PCR assay andrapid diagnostic tests for the diagnosis of clinically suspectedmalaria patients in Bangladesh. Malar J 2011;10:175.
16 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015
22. Al-Harthi SA, Jamjoom MB. PCR assay in malaria diagnosisusing filter paper samples from Jazan region, Saudi Arabia.J Egypt Soc Parasitol 2008;38:693–706.
23. Andrade BB, Reis-Filho A, Barros AM, et al. Towards a precisetest for malaria diagnosis in the Brazilian Amazon: comparisonamong field microscopy, a rapid diagnostic test, nested PCR, and acomputational expert system based on artificial neural networks.Malar J 2010;9:117.
24. Anthony C, Mahmud R, Lau Y, et al. Comparison of two nestedPCR methods for the detection of human malaria. Trop Biomed2013;30:459–66.
25. Aslan G, Seyrek A, Kocagoz T, et al. The diagnosis ofmalaria and identification of plasmodium species by poly-merase chain reaction in Turkey. Parasitol Int 2007;56:217–20.
26. Ataei S, Nateghpour M, Hajjaran AH, et al. High specificity ofsemi-nested multiplex PCR using dried blood spots on DNAbanking card in comparison with frozen liquid blood for detectionof Plasmodium falciparum and Plasmodium vivax. J Clin LabAnal 2011;25:185–90.
27. Barker RH, Banchongaksorn T, Courval JM, et al. A simplemethod to detect Plasmodium falciparum directly from bloodsamples using the polymerase chain reaction. Am J Trop Med Hyg1992;46:416–26.
28. Barman D, Mirdha B, Samantray J, et al. Evaluation ofquantitative buffy coat (QBC) assay and polymerase chainreaction (PCR) for diagnosis of malaria. J Commun Dis 2003;35:170–81.
29. Bendezu J, Rosas A, Grande T, et al. Field evaluation of a rapiddiagnostic test (Parascreen�) for malaria diagnosis in thePeruvian Amazon. Malar J 2010;9:154.
30. Boonma P, Christensen PR, Suwanarusk R, et al. Comparisonof three molecular methods for the detection and speciationof Plasmodium vivax and Plasmodium falciparum. Malar J 2007;6:124.
31. Carrasquilla G, Banguero M, Sanchez P, et al. Epidemiologic toolsfor malaria surveillance in an urban setting of low endemicityalong the colombian pacific coast. Am J Trop Med Hyg 2000;62:132–7.
32. Chaudry JZ, Ahmed S, Qureshi TZ, Ali N. Real time polymerasechain reaction for the detection of malarial parasite. J Coll PhysSurg Pak 2012;22:98–100.
33. Cheng Z, Sun X, Yang Y, Wang H. A novel, sensitive assay forhigh-throughput molecular detection of plasmodia for activescreening of malaria for elimination. J Clin Microbiol 2013;51:125–30.
34. Chou M, Kim S, Khim N, et al. Performance of ‘‘VIKIA MalariaAg Pf/Pan’’ (IMACCESS), a new malaria rapid diagnostic test fordetection of symptomatic malaria infections. Malar J 2012;11:295.
35. Costa M, Vieira P, de Oliveira Ferreira C, et al.Diagnostico molecular da malaria em uma unidade de atencaoterciaria na Amazonia Brasileira. Rev Soc Brasi Med Trop 2008;41:381–5.
36. Datta S, Basu B, Chandra CY, Nagendra BA. Newer versusconventional methods in the diagnosis of malaria: a comparison.Med J Armed Forces India 2010;66:129–33.
37. Dawoud H, Ageely H, Heiba A. Evaluation of a real-timepolymerase chain reaction assay for the diagnosis of malaria inpatients from Jazan area, Saudi Arabia. J Egypt Soc Parasitol2008;38:339–50.
38. Dawoud H, Ageely H, Heiba A. Comparison of two commercialassays and microscopy with PCR for diagnosis of malaria. J EgyptSoc Parasitol 2008;38:329–38.
39. Ebrahimzadeh A, Fouladi B, Fazaeli A. High rate of detection ofmixed infections of Plasmodium vivax and Plasmodium falcip-arum in South-East of Iran, using nested PCR. Parasitol Int 2007;56:61–4.
40. Elahi R, Mohon AN, Khan WA, et al. Performance of a HRP-2/pLDH based rapid diagnostic test at the Bangladesh–India–Myanmar border areas for diagnosis of clinical malaria. Malar J2013;12:378.
41. Fuehrer H, Fally MA, Habler VE, et al. Novel nested direct PCRtechnique for malaria diagnosis using filter paper samples. J ClinMicrobiol 2011;49:1628–30.
42. Gaye O, Diouf M, Diallo S. A comparison of thick smears, QBCMalaria, PCR and PATH falciparum Malaria test trip inPlasmodium falciparum diagnosis. Parasite 1999;6:273–5.
43. Genc A, Eroglu F, Koltas IS. Detection of Plasmodium vivax bynested PCR and real-time PCR. Korean J Parasitol 2010;48:99–103.
44. Haghdoost A, Mazhari S, Bahadini K. Comparing the results oflight microscopy with the results of PCR method in the diagnosisof Plasmodium vivax. J Vector Borne Dis 2006;43:53–7.
45. Hopkins H, Gonzalez IJ, Polley SD, et al. Highly Sensitivedetection of malaria parasitemia in a malaria-endemic setting:performance of a new loop-mediated isothermal amplification kitin a remote clinic in Uganda. J Infect Dis 2013;208:645–52.
46. Hwang S, Kim S, Lee G, et al. A novel real-time PCR assay for thedetection of Plasmodium falciparum and Plasmodium vivaxmalaria in low parasitized individuals. Acta Trop 2011;120:40–5.
47. Khan SA, Ahmed S, Mushahid N, et al. Comparison of real timepolymerase chain reaction with microscopy and antigen detectionassay for the diagnosis of malaria. J Coll Phys Surg Pak 2013;23:787–92.
48. Kuamsab N, Putaporntip C, Pattanawong U, Jongwutiwes S.Simultaneous detection of Plasmodium vivax and Plasmodiumfalciparum gametocytes in clinical isolates by multiplex-nestedRT-PCR. Malar J 2012;11:190.
49. Kumudunayana W, Gunasekera T de A, Abeyasinghe RR, et al.Usefulness of polymerase chain reaction to supplement fieldmicroscopy in a pre-selected population with a high probability ofmalaria infections. Am J Trop Med Hyg 2011;85:6–11.
50. Laoboonchai A, Kawamoto F, Thanoosingha N, et al. PCR-basedELISA technique for malaria diagnosis of specimens fromThailand. Trop Med Int Health 2001;6:458–62.
51. Laserson KF, Petralanda I, Hamlin DM, et al. Use of thepolymerase chain reaction to directly detect malaria parasites inblood samples from the Venezuelan Amazon. Am J Trop Med Hyg1994;50:169–80.
52. Lee P, Ji D, Liu C, et al. Application of loop-mediated isothermalamplification for malaria diagnosis during a follow-up study inSao Tome. Malar J 2012;11:408.
53. Menge DM, Ernst KC, Vulule JM, et al. Microscopy underesti-mates the frequency of Plasmodium falciparum infection insymptomatic individuals in a low transmission highland area. AmJ Trop Med Hyg 2008;79:173–7.
54. Mens P, Spieker N, Omar S, et al. Is molecular biology the bestalternative for diagnosis of malaria to microscopy? A comparisonbetween microscopy, antigen detection and molecular tests inrural Kenya and urban Tanzania. Trop Med Int Health 2007;12:238–44.
55. Mens PF, Moers AP, de Bes LM, et al. Development, validationand evaluation of a rapid PCR-nucleic acid lateral flow immuno-assay for the detection of Plasmodium and the differentiationbetween Plasmodium falciparum and Plasmodium vivax. Malar J2012;11:279.
56. Mens P, de Bes H, Sondo P, et al. Direct blood PCR incombination with nucleic acid lateral flow immunoassay fordetection of Plasmodium species in settings where malaria isendemic. J Clin Microbiol 2012;50:3520–5.
57. Montoya AE, Menco J, Osorio N, et al. Concordancia entre gotagruesa, inmunocromatografıa y reaccion en cadena de lapolimerasa para el diagnostico de malaria. Biomedica 2008;28:252–61.
58. Nandwani S, Mathur M, Rawat S. Evaluation of the polymerasechain reaction analysis for diagnosis of falciparum malaria inDelhi, India. Indian J Med Microbiol 2005;23:176–8.
59. Nicastri E, Bevilacqua N, Schepisi MS, et al. Accuracy of malariadiagnosis by microscopy, rapid diagnostic test, and PCR methodsand evidence of antimalarial overprescription in non-severe febrilepatients in two Tanzanian hospitals. Am J Trop Med Hyg 2009;80:712–17.
60. Nkrumah B, Agyekum A, Acquah SEK, et al. Comparison of thenovel partec rapid malaria test to the conventional Giemsa stainand the gold standard real-time PCR. J Clin Microbiol 2010;48:2925–8.
61. Nwakanma DC, Gomez-Escobar N, Walther M, et al. Quantitativedetection of Plasmodium falciparum DNA in saliva, blood, andurine. J Infect Dis 2009;199:1567–74.
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 17
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

62. Ogbolu D, Terry Alli O, Nassar A, Ajagbe O. Evaluation ofusefulness of polymerase chain reaction in the diagnosis ofmalaria in Nigeria. Afr J Clin Exp Microbiol 2012;13:127–34.
63. Ojurongbe O, Adegbosin OO, Taiwo SS, et al. Assessment ofclinical diagnosis, microscopy, rapid diagnostic tests, and poly-merase chain reaction in the diagnosis of Plasmodium falciparumin Nigeria. Malar Res Treat 2013;2013:1–5.
64. Osman MM, Nour BY, Sedig MF, et al. Informed decision-makingbefore changing to RDT: a comparison of microscopy, rapiddiagnostic test and molecular techniques for the diagnosis andidentification of malaria parasites in Kassala, eastern Sudan. TropMed Int Health 2010;15:1442–8.
65. Oster N, Abdel-aziz I, Stich A, et al. Comparison of different PCRprotocols for the detection and diagnosis of Plasmodium falcip-arum. Parasitol Res 2005;97:424–8.
66. Oyedeji SI, Awobode HO, Monday GC, et al. Comparison ofPCR-based detection of Plasmodium falciparum infections basedon single and multicopy genes. Malar J 2007;112:6.
67. Pakalapati D, Garg S, Middha S, et al. Development andevaluation of a 28S rRNA gene-based nested PCR assay forP. falciparum and P. vivax. Pathog Glob Health 2013;107:180–8.
68. Pakalapati D, Garg S, Middha S, et al. Comparative evaluation ofmicroscopy, OptiMAL and 18S rRNA gene based multiplex PCRfor detection of Plasmodium falciparum & Plasmodium vivaxfrom field isolates of Bikaner, India. Asian Pacif J Trop Med 2013;6:346–51.
69. Parajuli K, Hanchana S, Imwong M, et al. Comparative evaluationof microscopy and polymerase chain reaction (PCR) for thediagnosis in suspected malaria patients of Nepal. Nepal Med CollJ 2009;11:23–7.
70. Paris DH, Imwong M, Faiz AM, et al. Loop-mediated isothermalPCR (LAMP) for the diagnosis of Falciparum malaria. Am J TropMed Hyg 2007;77:972–6.
71. Poschl B, Waneesorn J, Thekisoe O, et al. Comparative diagnosisof malaria infections by microscopy, nested PCR, and LAMP inNorthern Thailand. Am J Trop Med Hyg 2010;83:56–60.
72. Postigo M, Mendoza-Leon A, Perez HA. Malaria diagnosis by thepolymerase chain reaction: a field study in south-easternVenezuela. Trans Roy Soc Trop Med Hyg 1998;92:509–11.
73. Puri B, Mehta P, Ingole N, et al. Laboratory tests for malaria: adiagnostic conundrum? South African Med J 2013;103:625–7.
74. Rakotonirina H, Barnadas C, Raherijafy R, et al. Accuracy andreliability of malaria diagnostic techniques for guiding febrileoutpatient treatment in malaria-endemic countries. Am J Trop MedHyg 2008;78:217–21.
75. Ratsimbasoa A, Ravony H, Vonimpaisomihanta J, et al.Management of uncomplicated malaria in febrile under five-year-old children by community health workers in Madagascar:reliability of malaria rapid diagnostic tests. Malar J 2012;85:11.
76. Runsewe-Abiodun IT, Efunsile M, Ghebremedhin B, et al. Malariadiagnostics: a comparative study of blood microscopy, a rapiddiagnostic test and polymerase chain reaction in the diagnosis ofmalaria. J Trop Pediatr 2011;58:163–4.
77. Sattabongkot J, Tsuboi T, Han E-T, et al. Evaluation of loop-mediated isothermal amplification (LAMP) assay for rapiddiagnosis of malaria infections in an endemic setting inThailand. J Clin Microbiol 2014;52:1471–7.
78. Singh R, Savargaonkar D. Rapid detection of Plasmodium vivax insaliva and blood using loop mediated isothermal amplification(LAMP) assay. J Infect 2013;67:245–7.
79. Sirichaisinthop J, Buates S, Watanabe R, et al. Short report:evaluation of loop-mediated isothermal amplification (LAMP) formalaria diagnosis in a field setting. Am J Trop Med Hyg 2011;85:594–6.
80. Strøm GE, Haanshuus CG, Fataki M, et al. Challenges indiagnosing paediatric malaria in Dar es Salaam, Tanzania.Malar J 2013;12:228.
81. Swan H, Sloan L, Muyombwe A, et al. Evaluation of a real-time polymerase chain reaction assay for the diagnosis ofmalaria in patients from Thailand. Am J Trop Med Hyg 2005;73:850–4.
82. Talundzic E, Maganga M, Masanja IM, et al. Field evaluation ofthe photo-induced electron transfer fluorogenic primers (PET)real-time PCR for the detection of Plasmodium falciparum inTanzania. Malar J 2014;13:31.
83. Tao Z, Zhou H, Xia H, et al. Adaptation of a visualized loop-mediated isothermal amplification technique for field detection ofPlasmodium vivax infection. Parasites Vect 2011;4:1–8.
84. Tirasophon W, Rajkulchai P, Ponglikitmongkol M, et al. A highlysensitive, rapid, and simple polymerase chain reaction-basedmethod to detect human malaria (Plasmodium falciparum andPlasmodium vivax) in blood samples. Am J Trop Med Hyg 1994;51:308–13.
85. Urdaneta L, Guevara P, Ramirez J. Evaluation of DNA recom-binant methodologies for the diagnosis of Plasmodium falciparumand their comparison with the microscopy assay. Mem InstOswaldo Cruz 1998;93:639–46.
86. Veron V, Simon S, Carme B. Multiplex real-time PCR detection ofP. falciparum, P. vivax and P. malariae in human blood samples.Exp Parasitol 2009;121:346–51.
87. Vo TKD, Bigot P, Gazin P, et al. Evaluation of a real-time PCRassay for malaria diagnosis in patients from Vietnam and inreturned travellers. Trans Roy Soc Trop Med Hyg 2007;101:422–8.
88. Waitumbi JN, Gerlach J, Afonina I, et al. Malaria prevalencedefined by microscopy, antigen detection, DNA amplification andtotal nucleic acid amplification in a malaria-endemic regionduring the peak malaria transmission season. Trop Med Int Health2011;16:786–93.
89. Wangai LN, Karau MG, Njiruh PN, et al. Sensitivity of microsopycompared to molecular diagnosis of P. falciparum: implications onmalaria treatment in epidemic areas in Kenya. Afr J Infect Dis2011;5:1–6.
90. Wu Y, Lei L, Li M. Evaluation of a parasite lactate dehydrogen-ase-based colloid gold-immunochromatography assay for diagno-sis of Plasmodium falciparum. J First Military Med Univ 2005;25:761–5.
91. Yamamura M, Makimura K, Ota Y. Evaluation of a new rapidmolecular diagnostic system for Plasmodium falciparum com-bined with DNA Filter paper, loop-mediated isothermal amplifi-cation, and melting curve analysis. Jpn J Infect Dis 2009;62:20–5.
92. Yan J, Li N, Wei X, et al. Performance of two rapid diagnostictests for malaria diagnosis at the China–Myanmar border area.Malar J 2013;12:73.
93. Zakeri S, Najafabadi ST, Zare A, Djadid ND. Detection of malariaparasites by nested PCR in south-eastern, Iran: evidence of highlymixed infections in Chahbahar district. Malar J 2002;1:2.
94. Zakeri S, Naimi P, Zare M, et al. Molecular evidence on changingpattern of mixed Plasmodium falciparum and P. vivax infectionsduring year-round transmission of malaria in Chahbahar, Iran. IranBiomed J 2004;8:89–93.
95. Snounou G, Viriyakosol S, Jarra W, et al. Identification of the fourhuman malaria parasite species in field samples by the polymerasechain reaction and detection of a high prevalence of mixedinfections. Mol Biochem Parasitol 1993;58:283–92.
96. Snounou G. Detection and identification of the four malariaparasite species infecting humans by PCR amplification. MethodsMol Biol 1996;50:263–91.
97. McNamara DT, Kasehagen LJ, Grimberg BT, et al. Diagnosinginfection levels of four human malaria parasite species by apolymerase chain reaction/ligase detection reaction fluorescentmicrosphere-based assay. Am J Trop Med Hyg 2006;74:413–21.
98. Akane A, Matsubara K, Nakamura H, et al. Identification of theHeme compound copurified with deoxyribonucleic acid (DNA)from bloodstains, a major inhibitor of polymerase chain reaction(PCR) amplification. J Forensic Sci 1994;39:362–72.
99. Jarra W, Snounou G. Only viable parasites are detected by PCRfollowing clearance of rodent malarial infections by drug treat-ment or immune responses. Infect Immun 1998;66:3783–7.
100. Imwong M, Hanchana S, Malleret B, et al. High-throughputultrasensitive molecular techniques for quantifying low-densitymalaria parasitemias. J Clin Microbiol 2014;52:3303–9.
101. Hodgson SH, Douglas AD, Edwards NJ, et al. Increased samplevolume and use of quantitative reverse-transcription PCR canimprove prediction of liver-to-blood inoculum size in controlledhuman malaria infection studies. Malar J 2015;14:33.
102. Mercereau-Puijalon O, Barale J, Bischoff E. Three multigenefamilies in Plasmodium parasites: facts and questions. Int JParasitol 2002;32:1323–44.
103. Xu W, Morris U, Aydin-schmidt B, et al. SYBR green real-time PCR-RFLP assay targeting the Plasmodium cytochrome B
18 J. M. Roth et al. Crit Rev Clin Lab Sci, Early Online: 1–19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015

gene – a highly sensitive molecular tool for malaria parasitedetection and species determination. PLoS One 2015;10:1–15.
104. Leeflang MMG, Bossuyt PMM, Irwig L. Diagnostic test accuracymay vary with prevalence: implications for evidence-baseddiagnosis. J Clin Epidemiol 2009;62:5–12.
105. UNITAID. Malaria Diagnostics Technology and MarketLandscape. 2nd ed. Geneva: UNITAID, 2014:1–140.
106. Holden MJ, Madej RM, Minor P, Kalman LV. Moleculardiagnostics: harmonization through reference materials, documen-tary standards and proficiency testing. Expert Rev Mol Diagn2011;11:741–55.
107. Miller WG, Jones GRD, Horowitz GL, Weykamp C. Proficiencytesting/external quality assessment: current challenges and futuredirections. Clin Chem 2011;57:1670–80.
108. Bustin SA, Benes V, Garson JA, et al. The MIQE guidelines:minimum information for publication of quantitative real-timePCR experiments. Clin Chem 2009;55:611–22.
109. Poon LL, Wong BW, Ma EH, et al. Sensitive and inexpensivemolecular test for falciparum malaria: detecting Plasmodium
falciparum DNA direclty from heat-treated blood byloop-mediated isothermal amplification. Clin Chem 2006;52:303–6.
110. Oriero EC, Jacobs J, Van Geertruyden J-P, et al. Molecular-basedisothermal tests for field diagnosis of malaria and their potentialcontribution to malaria elimination. J Antimicrob Chemother2014;70:1–12.
111. World Health Organization. Universal Access to MalariaDiagnostic Testing – An Operational Manual. Geneva: WorldHealth Organization, 2011:1–160.
112. Foundation for Innovative New Diagnostics (FIND). Malariastrategy. Geneva: FIND, 2012:1–44.
113. Canier L, Khim N, Kim S, et al. An innovative tool for movingmalaria PCR detection of parasite reservoir into the field. Malar J2013;12:405.
114. Bossuyt PM, Reitsma JB, Bruns DE, et al. TheSTARD statement for reporting studies of diagnosticaccuracy: explanation and elaboration. Acad Clinic 2003;138:1–12.
Supplementary material (Additional files 1 and 2) available online
DOI: 10.3109/10408363.2015.1084991 Molecular malaria diagnostics 19
Dow
nloa
ded
by [
77.1
68.1
3.16
7] a
t 11:
04 2
8 Se
ptem
ber
2015





























