Embed Size (px)
Citation preview

MOLECULAR GENETICS OF
ACUTE INTERMITTENT PORPHYRIA
IN FINLAND
SAMI MUSTAJOKI
Helsinki 1999

Division of Endocrinology, Department of Medicine, University of Helsinki and
Department of Human Molecular Genetics, National Public Health Institute, Finland
MOLECULAR GENETICS OF
ACUTE INTERMITTENT PORPHYRIA
IN FINLAND
SAMI MUSTAJOKI
To be presented, with the permission of
the Faculty of Medicine, University of Helsinki,
for public examination in auditorium 1,
Meilahti Hospital, on October 29th, 1999 at 12 noon.
Helsinki 1999

Supervisors Raili Kauppinen, M.D., Ph.D.
Department of Medicine, Division of Endocrinology
University of Helsinki, Finland
Professor Leena Peltonen-Palotie, M.D., Ph.D.
Department of Human Molecular Genetics
National Public Health Institute and
Department of Medical Genetics
University of Helsinki, Finland
Reviewers Professor Jean-Charles Deybach, M.D., Ph.D.
Hôpital L. Mourier and Faculté de Médecine X. Bichat
Université Paris 7, France
Professor Marja-Liisa Savontaus, Ph.D.
Department of Medical Genetics
University of Turku, Finland
Opponent Professor Juha Kere, M.D., Ph.D.
Finnish Genome Center
University of Helsinki, Finland
ISBN 951-45-8723-5 (PDF version)Helsinki 1999Helsingin yliopiston verkkojulkaisut

To Ulla

CONTENTS4
CONTENTS
ABBREVIATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
ORIGINAL PUBLICATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1. INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
2. REVIEW OF THE LITERATURE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102.1. Heme biosynthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102.2. The porphyrias . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122.3. Acute intermittent porphyria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
2.3.1. History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142.3.2. Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152.3.3. Clinical features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162.3.4. Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182.3.5. Biochemical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.3.6. CRIM subtypes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
2.4. Porphobilinogen deaminase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202.4.1. Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212.4.2. Structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
2.5. Molecular genetics of acute intermittent porphyria . . . . . . . . . . . . . . . . . . . . . . . . 232.5.1. The porphobilinogen deaminase gene . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232.5.2. Mutations resulting in AIP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3. AIMS OF THE PRESENT STUDY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
4. MATERIAL AND METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 314.1. Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 314.2. DNA and RNA isolation, and cDNA synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . 314.3. DNA amplification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 314.4. Subcloning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324.5. Mutation screening . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324.6. Sequencing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334.7. Solid-phase minisequencing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334.8. In vitro mutagenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34

CONTENTS 5
4.9. COS-1 cell culture and DNA transfection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 344.10. Enzyme activity assay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 344.11. Western blot . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 354.12. Pulse-chase and immunoprecipitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 354.13. Immunofluorescence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
5. RESULTS AND DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 375.1. Identified mutations (I, II, III) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 375.2. SSCP and DGGE in screening for novel mutations (I, II, III, IV) . . . . . . . . . . . . . 415.3. Monitoring the effect of mutations to allelic transcript levels (V) . . . . . . . . . . . . . 435.4. Expression of mutated polypeptides (III, VI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 475.5. Outcome of mutations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
5.5.1. Mutations resulting in premature termination codon . . . . . . . . . . . . . . . . . . . 525.5.2. Missense mutations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 535.5.3. Splicing mutations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 575.5.4. Other mutations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
5.6. Molecular genetics of AIP in the Finnish population . . . . . . . . . . . . . . . . . . . . . . . 615.5. DNA diagnosis of AIP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
6. SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
7. ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
8. REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
ORIGINAL ARTICLES I-VI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79

ABBREVIATIONS6
ABBREVIATIONS
aa Amino acid
AIP Acute intermittent porphyria
ALA Aminolevulinic acid
bp Base pair
BSA Bovine serum albumin
CYP Cytochrome P-450
DGGE Denaturing gradient gel electrophoresis
DNA Deoxyribonucleic acid
dNTP Deoxynucleotide triphosphate
EDTA Edetate disodium tetraacetic acid
IVS Intervening sequence
kb Kilobase
kD Kilodalton
mRNA Messenger ribonucleic acid
PBG Porphobilinogen
PBGD Porphobilinogen deaminase
PBS Phosphate buffered saline
PCR Polymerase chain reaction
RNA Ribonucleic acid
SDS Sodium dodecyl sulfate
SSCP Single-strand conformation polymorphism
Amino acids are abbreviated by one or three letter codes and nucleotides by one letter codes.

ORIGINAL PUBLICATIONS 7
LIST OF ORIGINAL PUBLICATIONS
I Kauppinen R, Mustajoki S, Pihlaja H, Peltonen L, Mustajoki P: Acute intermittent
porphyria in Finland: 19 mutations in the porphobilinogen deaminase gene. Hum Mol
Genet 4:215-222, 1995.
II Mustajoki S, Pihlaja H, Ahola H, Petersen NE, Mustajoki P, Kauppinen R: Three splicing
defects, an insertion, and two missense mutations responsible for acute intermittent
porphyria. Hum Genet 102:541-548, 1998.
III Mustajoki S, Ahola H, Mustajoki P, Kauppinen R: Insertion of Alu element responsible for
acute intermittent porphyria. Hum Mutat 13:431-438, 1999.
IV Nissen H, Petersen NE, Mustajoki S, Hansen TS, Mustajoki P, Kauppinen R, Hørder M:
Diagnostic strategy, genetic diagnosis and identification of new mutations in acute
intermittent porphyria by denaturing gradient gel electrophoresis. Hum Mutat 9:122-130,
1997.
V Mustajoki S, Kauppinen R, Mustajoki P, Suomalainen A, Peltonen L: Steady state
transcript levels of the porphobilinogen deaminase gene in patients with acute intermittent
porphyria. Genome Res 7:1054-1060, 1997.
VI Mustajoki S, Laine M, Lahtela M, Mustajoki P, Peltonen L, Kauppinen R: Acute
intermittent porphyria: expression of mutant and wild type porphobilinogen deaminase in
COS-1 cells. Manuscript submitted.
In addition, some unpublished data are presented.

INTRODUCTION8
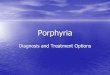
Figure 1.1. Heme biosynthesis pathway.
1. INTRODUCTION
Heme is synthesized in every eukaryotic and prokaryotic cell and it carries out many important
biologic functions. It is the prosthetic group of many hemeproteins. The best known function of
heme is its oxygen binding and transport in hemoglobin, and erythroblasts synthesize 85% of
the total body heme is the bone marrow (Berk et al. 1976). In addition, heme is involved in the
mitochondrial respiratory chain where it transports electrons to cytochromes. CYP enzymes,
which metabolize a large number of clinically important drugs as well as several endogenous
and exogenous substances, contain heme. Tryptophan pyrrolase, which catalyses the oxidation
of tryptophan, is also a heme-dependent enzyme.
Porphyrias are defects in heme biosynthesis. The heme biosynthesis pathway contains eight
steps and dysfunction in seven of them is associated with a specific porphyria (Figure 1);
defects in erythroid specific ALA synthase result in X-chromosome linked sideroblastic
anemia.

INTRODUCTION 9
Acute intermittent porphyria (AIP) is caused by a defect in the third enzyme in the heme
biosynthetic pathway, porphobilinogen deaminase (PBGD, also referred to as
hydroxymethylbilane synthase and uroporphyrinogen I synthase, EC 4.3.1.8). It is the most
common type of acute porphyria in Finland (Mustajoki and Koskelo 1976) and in most other
countries (Sassa and Kappas 1981). AIP is characterized by potentially lethal acute attacks with
abdominal pain, tachycardia and various other neuropsychiatric signs and symptoms (Kappas
et al. 1995).
The gene coding for human PBGD was characterized in 1986 (Raich et al. 1986) which enabled
the characterization of the molecular genetic background of AIP. The purpose of this series of
investigations was to identify the molecular defects in Finnish AIP patients and, furthermore,
to elucidate the mechanisms by which a mutation results in the deficient function of the
enzyme.

REVIEW OF THE LITERATURE10
2. REVIEW OF THE LITERATURE
2.1. Heme biosynthesis
All the enzymes and their genes in the heme biosynthetic pathway have been characterized
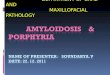
(Kappas et al. 1995, Nishimura et al. 1995). The biosynthesis pathway is illustrated in Figure
2.1. The first and the last three of the enzymes in the pathway are localized in mitochondria; the
intermediate enzymes are cytosolic. The precursors of heme are glycine and succinyl coenzyme
A which are combined by aminolevulinic acid (ALA) synthase to form 5-aminolevulinic acid
in the presence of the cofactor pyridoxal 5'-phosphate. Next, two molecules of ALA are
condensed to a monopyrrole porphobilinogen (PBG) by ALA dehydratase.
Porphobilinogen deaminase (PBGD) assembles the four rings of PBG in a stepwise fashion in
which the pyrrole ring A is first bound to the deaminase followed by rings B, C and finally D
(Figure 2.2.). The dipyrromethane cofactor, which arises from the autocatalytic coupling of two
molecules of PBG, is covalently linked to the enzyme. The cofactor functions as a primer to
which the four substrate molecules are sequentially attached but is not itself incorporated into
the product, hydroxymethylbilane.
The fourth enzyme, uroporphyrinogen III synthase, converts the highly unstable
hydroxymethylbilane to uroporphyrinogen III and in this reaction the linear tetrapyrrole
molecule is closed to form a ring. In the absence of uroporphyrinogen III synthase,
hydroxymethylbilane may non-enzymatically close to uroporphyrinogen I. In normal
circumstances, this isoform is present only in minute amounts.
The four carboxylic groups of the acetic acid chains in uroporphyrinogen are removed in the
reaction catalysed by cytosolic uroporphyrinogen decarboxylase. In the presence of oxygen
coproporphyrinogen oxidase catalyses the removal of the carboxyl group and the two
hydrogens from the propionic groups of the pyrrole rings and forms vinyl groups at these
positions resulting in protoporphyrinogen IX.

REVIEW OF THE LITERATURE11
Figure 2.1. Enzymes and intermediate products in the heme biosynthesis pathway.Ac= -CH2COOH; Pr= -CH2CH2COOH; Vi= -CH=CH2

REVIEW OF THE LITERATURE 12
In the seventh step of heme biosynthesis, six hydrogen atoms are removed from
protoporphyrinogen IX to form protoporphyrin IX, a reaction catalysed by protoporphyrinogen
oxidase. The oxidation of protoporphyrinogen may also occur non-enzymatically.
Finally, iron (Fe2+) is incorporated into protoporphyrin IX by a mitochondrial ferrochelatase,
also known as heme synthase.
The heme biosynthesis is regulated in distinctive manners in erythroid and non-erythroid tissues
but ALA synthase is the rate-limiting enzyme of heme biosynthesis in all tissues (Kappas et al.
1995). Two different genes code for ALA synthase: the nonspecific ALA synthase is ubiquitous
whereas the erythroid ALA synthase is expressed only in erythroid tissues (Kappas et al. 1995).
Biosynthesis of heme in the liver and in other non-erythroid tissues is regulated by a feedback
mechanism in which the end product heme regulates the synthesis of non-specific isoform of
ALA synthase at the transcriptional and translational level (Moore et al. 1987). The activity of
nonspecific ALA synthase may be also induced by various chemicals, drugs, lead, and alcohol
and reduced by glucose. The erythroid-specific isozyme of ALA synthase is, in contrast to the
nonspecific ALA synthase, upregulated by increased heme concentration (Fujita et al. 1991).
The ALA synthase activity is also regulated by many other factors, for example by
erythropoietin and by the availability of iron (May et al. 1995).
More detailed information about heme biosynthesis is available in the literature (e.g. Moore et
al. 1987, Kappas et al. 1995).
2.2. The porphyrias
The porphyrias are a heterogeneous group of metabolic disorders. They have been divided into
two groups, erythropoietic and hepatic porphyrias (Moore et al. 1987) according to the tissue
where the excess porphyrins or their precursors are mainly synthesized. In general, the clinical
m a n i f e s t a t i o n s o f p o r p h y r i a s a r e e i t h e r s k i n p h o t o s e n s i t i v i t y d u e t o

REV
IEW O
F THE LITER
ATU
RE
13
Table 2.1. Classification of porphyrias*Classification Deficient enzyme Manifestations Inheritance
Erythropoietic
Congenital erythropoietic porphyria Uroporphyrinogen III synthase Photosensitivity Autosomal recessive
Erythropoietic protoporphyria Ferrochelatase Photosensitivity Autosomal dominant/recessive
Hepatic
ALA dehydratase deficiency porphyria ALA dehydratase Chronic neurologic symptoms Autosomal recessive
Acute intermittent porphyria Porphobilinogen deaminase Acute attacks Autosomal dominant
Hereditary coproporphyria Coproporphyrinogen oxidase Acute attacks and/orexcessive skin fragility
Autosomal dominant
Variegate porphyria Protoporphyrinogen oxidase Acute attacks and/orexcessive skin fragility
Autosomal dominant
Porphyria cutanea tarda Uroporphyrinogen decarboxylase Excessive skin fragility Autosomal dominant/ sporadic
Hepatoerythropoietic porphyria Uroporphyrinogen decarboxylase Photosensitivity Autosomal recessive* Modified from Kappas et al. 1995

REVIEW OF THE LITERATURE 14
photoreactivity of porphyrins, neurovisceral dysfunction (acute attacks), or both (Kappas et al.
1995). Most of the porphyrias are inherited dominantly in autosomes. ALA dehydratase
deficiency and congenital erythropoietic porphyria have, however, autosomal recessive
inheritance. Furthermore, a significant number of patients with porphyria cutanea tarda are
sporadic cases (de Verneuil et al. 1978). Hepatoerythropoietic porphyria is a rare homozygous
form of the familial type of porphyria cutanea tarda (Toback et al. 1987). A summary of
different porphyria types is given in Table 2.1.
2.3. Acute intermittent porphyria
2.3.1. History
The modern history of acute porphyrias, reviewed extensively elsewhere (Goldberg and
Rimington 1962, Dean 1963, Tschudy et al. 1975), begins at the end of the 19th century, when
an increasing number of patients with abdominal pain and neurological symptoms was
described. The typical attacks of acute porphyria were associated already in these early days
with drug treatment.
Most of the porphyrin nomenclature is based on Hans Fischer's, a Nobel laureate in 1930,
studies on the heme biosynthesis in the 1920's. In 1937 Jan Waldenström, who had previously
worked in Fischer's laboratory, described over one hundred patients with acute porphyria, most
of whom originated from a small village in Northern Sweden (Waldenström 1937). In this study
the Mendelian dominant mode of inheritance in AIP was demonstrated for the first time. Later,
he proposed that porphyrias could result from enzyme defects in the heme pathway and was
also the first to use the term 'acute intermittent porphyria' (Waldenström 1957). A screening test
for porphobilinogen was introduced in 1941 by Watson, who also was Fischer's co-worker
(Watson and Schwartz 1941). He also introduced hematin for treatment of acute porphyrias
(Watson et al. 1978). In the 1960's Granick discovered that ALA synthase, the first step in heme
biosynthesis, is induced by chemicals which cause acute porphyria (Granick 1963, Granick
1966). This observation led to the concept that overproduction of ALA may represent the
primary genetic defect in all acute porphyrias (Granick 1966), but this hypothesis was soon

REVIEW OF THE LITERATURE15
found to be false because increased activity of this enzyme by itself could not account for the
distinct patterns of porphyrin precursors and porphyrin excretion. The biochemical background
of AIP was confirmed when it was demonstrated that the disease is due to a defect in PBGD
(Miyagi 1970, Meyer et al. 1972).
The characterization of the porphobilinogen deaminase gene (Raich et al. 1986, Grandchamp
et al. 1987, Chretien et al. 1988, Lee 1991a, Namba et al. 1991) initiated multiple investigations
of the molecular genetic background of AIP, and today several mutations responsible for AIP
have been identified (see chapter 2.5.2).
The first Finnish patient with acute porphyria was reported in 1928 (Langenskiöld 1928). The
first comprehensive study of the prevalence and clinical characteristics of acute porphyrias in
Finland was reported in 1976 by Pertti Mustajoki and Pentti Koskelo (Mustajoki and Koskelo
1976). The prognosis, precipitating factors and associated diseases in Finnish patients with
acute porphyrias have been investigated thoroughly by Raili Kauppinen and Pertti Mustajoki
(Kauppinen et al. 1992).
2.3.2. Prevalence
AIP is the most common type of acute porphyria in most countries (Kappas et al. 1995), only
in the Republic of South Africa is the prevalence of variegate porphyria higher than that of AIP.
The prevalence of AIP in Finland has been estimated to be 3:100000 (Mustajoki and Koskelo
1976). In other countries the reported prevalence figures are similar or slightly higher: 5-
10:100000 in the United States of America, in Western Australia 3:100000 (Tschudy et al.
1975). The highest prevalence of AIP has been described in northern Sweden where the
prevalence is 100:100000 and, furthermore, in two small municipalities the prevalence is as
high as 0.5-2%. However, the overall prevalence of AIP in Sweden is only 10:100000
(Andersson 1997). In a study of healthy Finnish blood donors the prevalence of low PBGD
activity was 1:500 (Mustajoki et al. 1992) and similar figures were obtained in a study which
consisted of healthy French blood donors (Nordmann et al. 1997). This implies that the
prevalence of AIP, though asymptomatic, may be much higher than previously estimated.

REVIEW OF THE LITERATURE 16
2.3.3. Clinical features
Approximately 10-20% of the affected individuals experience acute attacks during their
lifetime and 50% of patients have milder symptoms typical for AIP (Kauppinen and Mustajoki
1992). Half of the subjects with decreased PBGD activity remain, thus, asymptomatic
throughout their lifetimes. Acute attacks are extremely rare before puberty and the first acute
attack usually manifests at an age between 15 and 40 years (Mustajoki and Koskelo 1976).
Table 2.2. Symptoms and signs of an acute attack*Abdominal pain 90%Dark or red urine 89%Vomiting 61%Constipation 56%Extremity and/or back pain 53%Muscle weakness 53%Mental symptoms 46%Hypertension (diast. A100 mmHg) 42%Tachycardia 40%Fever 35%Sensory loss 19%Convulsions 14%Respiratory muscle paralysis 14%Diarrhea 9%*Total of 774 patients. Data combined from(Waldenström 1957, Goldberg 1959, Stein andTschudy 1970, Wetterberg 1974, Mustajoki andKoskelo 1976, Andersson 1997)
The symptoms during the acute attacks are mainly related to neurological dysfunctions. The
incidence of symptoms and physical signs are listed in Table 2.2. Abdominal pain is almost
invariably present and in severe cases it may mimic 'acute surgical abdomen'. Dark or red urine
is also frequently observed but the presence of other symptoms varies considerably which
sometimes causes difficulties in making the right diagnosis. Unless treated, the symptoms of an
acute attack may proceed to lethal respiratory paralysis. Nowadays, however, life-threatening
symptoms during acute attacks seldom occur because of increased knowledge of precipitating
factors and improved therapy (Kauppinen and Mustajoki 1992). The course of an acute attack
is variable and porphyric symptoms may last from a few days to several weeks (Kappas et al.
1995). Some patients may have symptoms almost continuously, but the majority of

REVIEW OF THE LITERATURE17
symptomatic patients have a few well-delineated attacks with relatively asymptomatic
intervening remissions (Kappas et al. 1995).
The porphyric attacks are often precipitated by environmental or endogenous factors, such as
changes in hormonal state (menstrual cycle and pregnancy), several therapeutic drugs (e.g.
barbiturates and sulphonamides), alcohol, infections, stress, and inadequate caloric intake
(Kauppinen and Mustajoki 1992, Kappas et al. 1995, Andersson 1997). According to a Finnish
survey, at present the most common cause for an acute attack is the menstrual cycle in females
and excessive alcohol consumption in males (Kauppinen and Mustajoki 1992). Avoiding the
precipitating factors usually decreases the incidence of attacks. Women at fertile age may need
hormonal therapy which suppresses their endogenous sex hormone production.
Some diseases are more common in patients with acute porphyria than in the normal
population. The risk for hepatocellular carcinoma is increased 61 to 114-fold (Kauppinen and
Mustajoki 1992, Andersson et al. 1996, Linet et al. 1999) and is the cause of death in about
one-quarter of AIP patients (Andersson et al. 1996). Chronic hypertension has been suggested
to be more common in patients with manifest AIP than in those with latent AIP or in healthy
controls in Swedish material of one large AIP family (Andersson and Lithner 1994): 56% of the
patients with manifest AIP had hypertension. However, the prevalence of chronic hypertension
was much lower (~24%) in the Finnish material which consisted of both AIP and variegate
porphyria patients from 53 families and, furthermore, the occurrence of hypertension did not
correlate with clinical manifestations (Kauppinen and Mustajoki 1992). When Finnish AIP
patients were compared to the general Finnish population, the prevalence rates of hypertension
with medication were higher only in two age-specific subgroups (Kauppinen and Mustajoki
1992). Cardiovascular mortality was not higher among AIP patients (Kauppinen and Mustajoki
1992, Andersson et al. 1996). The prevalence of chronic renal failure has been suggested to be
higher among AIP patients (Kauppinen and Mustajoki 1992, Andersson and Lithner 1994).

REVIEW OF THE LITERATURE 18
2.3.4. Pathogenesis
Under normal conditions, the heme biosynthesis pathway is able to fulfill its task inspite of
decreased PBGD activity. It is widely presumed that increased metabolic demand for heme in
the liver leads to an induction of ALA synthase expression (Kappas et al. 1995, Elder et al.
1997). This results in accumulation of intermediates of the heme biosynthesis pathway, namely
delta-aminolevulinic acid and porphobilinogen, since the defective enzyme is not able to
convert all the porphobilinogen to hydroxymethylbilane. The resulting deficiency of the final
product, heme, leads to further induction of ALA synthase provoking circulus vitiosus, an
escalating metabolic chain reaction.
About 65 percent of the aminolevulinic acid produced in the rat liver is utilized for the
formation of CYP isoenzymes (Sassa and Kappas 1981). Some drugs, alcoholic beverages and
steroid hormones, i.e. substances which are known to precipitate porphyric symptoms, are
known to induce or increase the inducibility of hepatic ALA synthase and may also increase the
intrahepatic requirement for heme by inducing the synthesis of CYP isoenzymes (Elder et al.
1997). This leads to the accumulation of delta- aminolevulinic acid and porphobilinogen
because the deficient PBGD cannot fulfill the requirements of the accelerated heme
biosynthesis.
The symptoms of AIP result from neurologic dysfunction and acute attacks are known to be
caused by the induction of ALA synthase. However, the details of molecular pathogenesis are
still obscure. Three major hypothesis has been proposed to explain the symptomatology of an
acute attack (Moore et al. 1987, Kappas et al. 1995):
1) depletion of heme in the cells of the central nervous system (Lindberg et al. 1996, Lindberg
et al. 1999),
2) neurotoxicity of accumulated intermediates, especially aminolevulinic acid (Bonkovsky
1993), and
3) neurotransmitter disturbance secondary to the deficiency of heme and tryptophan pyrrolase
(a heme dependent enzyme) in the liver (Litman and Correia 1983).

REVIEW OF THE LITERATURE19
Although all these theories are supported by some experimental findings, none of them can
explain all the various symptoms during an acute attack, and the pathogenetic mechanisms of
an acute attack remain, thus, unsolved.
The development of a transgenic porphobilinogen deaminase deficient mouse (Lindberg et al.
1996, Lindberg et al. 1999) is the first experimental model for acute porphyrias. Studies with
PBGD (-/-) mice suggest that heme deficiency and consequent dysfunction of hemeproteins
cause chronic and progressive neuropathy leading to impairment of motor coordination and
muscle weakness (Lindberg et al. 1999). However, the mouse model more resembles the
chronic neuropathy seen in some patients and it has not yet been able to elucidate the
pathogenetic mechanisms of acute attacks.
2.3.5. Biochemical findings
During an acute attack AIP patients always excrete increased amounts of the porphyrin
precursors, delta-aminolevulinic acid and porphobilinogen, in urine (Bissel 1982). Qualitative
tests, e.g. Watson-Schwartz and Hoesch tests (Bissel 1982), have been developed for rapid
confirmation of diagnosis, but sensitivity or specificity of these tests limit their usefulness
(Lamon et al. 1977). A quantitative assay (Mauzerall and Granick 1956) has been used for more
precise diagnosis. During the asymptomatic phase more than one half of AIP patients do not
excrete PBG in urine and these patients are less susceptible to acute attacks (Kauppinen and
Mustajoki 1992).
Biochemical diagnosis of acute intermittent porphyria is based on measurement of erythrocyte
porphobilinogen deaminase activity (Magnussen et al. 1974, Ford et al. 1980). In this assay,
porphobilinogen is used as a substrate and the uroporphyrin I formed is measured by
spectrofluorometry. In general, the erythrocyte PBGD activity in AIP patients is ~50% of that
found in normal subjects. Due to alternative splicing of the erythroid and wild type isoform
(Grandchamp et al. 1987), however, the erythrocyte PBGD activity is normal in the variant
form of AIP (Mustajoki 1981). Furthermore, there are wide individual variations of PBGD
activity among healthy controls (Mustajoki et al. 1992) and the normal and pathological values

REVIEW OF THE LITERATURE 20
have an overlapping zone. In addition, many diseases - for example renal insufficiency, iron
deficiency anemia and various malignancies - may affect PBGD activity (Moore et al. 1987).
These confounding factors limit the usefulness of biochemical methods in the diagnosis of AIP.
2.3.6. CRIM subtypes
Before the DNA era, AIP was divided into two major subtypes according to the ratio of enzyme
activity and the amount of immunoreactive protein in erythrocytes (Anderson et al. 1981,
Desnick et al. 1985, Lannfelt et al. 1989a). When the amount of immunoreactive protein
reflects the amount of enzymatically active protein, the patient is classified as cross-reactive
immunologic material (CRIM) negative. CRIM negative patients have been further divided into
two groups according to the PBGD activity in their erythrocytes: in type 1 the enzyme activity
is 50% of the normal activity whereas in type 2 the erythrocyte activity is normal. Several
explanations have been proposed for the absence of detectable mutant protein, i.e. CRIM
negativity (Mustajoki and Desnick 1985): instability of mutant mRNA, insufficient translation,
rapid intracellular decay of the mutant polypeptide, or due to an altered structure, the antibody
fails to detect the mutant polypeptide.
Enzymatically inactive but immunologically detectable protein is detected in erythrocytes of
CRIM positive patients. Two CRIM positive subtypes have been identified. In type 1 the ratio
of the protein and enzyme activity is ~1.6, i.e. the amount of inactive enzyme is 60-80% of that
of the active enzyme. In type 2 the CRIM/activity ratio is ~5.7, i.e. the amount of inactive
enzyme is 5.7-fold that of the active enzyme. In both CRIM positive subtypes the amount of
enzyme intermediates is increased (Anderson et al. 1981, Desnick et al. 1985), suggesting that
the enzyme protein is synthesized normally but it cannot catalyze deamination or elongate the
pyrrole chain normally.
2.4. Porphobilinogen deaminase
PBGD is a monomeric enzyme and in humans two isoforms are present: the 44 kD house-
keeping enzyme and the 42 kD erythroid-specific enzyme. The ubiquitous polypeptide, which

REVIEW OF THE LITERATURE21
consists of 361 amino acid residues, is encoded by a single gene on chromosome 11q, and the
two isoforms differ only in their N-terminal amino acid sequences; the first 17 amino acids of
the wild type enzyme are not present in the erythroid isoform (Grandchamp et al. 1989c). Since,
the deaminases show exceptional heat stability, their characterization has been very convenient
(Shoolingin-Jordan 1995).
2.4.1. Function
PBGD catalyzes the tetramerization of porphobilinogen. The reaction produces a highly
unstable 1-hydroxymethylbilane (preuroporphyrinogen) intermediate which is followed by the
formation of cyclic tetramere uroporphyrinogen by uroporphyrinogen III synthase. PBGD
assembles the four rings of PBG in a step-wise fashion, in which the pyrrole ring A is first
bound to the deaminase followed by rings B, C, D (Figure 2.2.) The dipyrromethane cofactor
anchors the substrate molecules at the catalytic center and directs the construction of the
tetrapyrrole (Jordan and Warren 1987). The cofactor is formed by autocatalytic coupling of two
molecules of PBG, the same molecule which also acts as the substrate for the reaction.
Figure 2.2. Reaction cascade catalyzed by porphobilinogen deaminase

REVIEW OF THE LITERATURE 22
Figure 2.3. Schematic representation of human PBGD secondary structural elements. Basedon a crystal structure of E. coli enzyme (Louie et al. 1992) and on a model of human PBGD(Brownlie et al. 1994).
The enzyme-intermediate complexes have been isolated and studied further (Warren and Jordan
1988). Of these, the first intermediate complex (i.e. the enzyme with one substrate molecule
bound) is the most labile and the second intermediate the most stable at 37oC. The last enzyme-
intermediate complex, in which all four porphobilinogen rings are attached to the enzyme via
the dipyrromethane cofactor, does not accumulate at all, presumably due to rapid release of the
tetrapyrrole from the enzyme.
PBGD has, thus, the ability to perform multiple chemical reactions despite its small size. The
enzyme catalyzes the repetitive condensation of PBG units with an acceptor pyrrole chain and
is able to 'count' precisely and terminate the reaction when the tetrapyrrole chain has been
assembled. In addition, the apoenzyme installs its own dipyrromethane cofactor to form the
holoenzyme.

REVIEW OF THE LITERATURE23
2.4.2. Structure
The structure of human PBGD has been predicted using the three-dimensional structure of
PBGD purified and crystallized from E. coli (Louie et al. 1992, Brownlie et al. 1994). The
molecule is composed of three domains of similar sizes linked together by flexible hinge
regions (Figure 2.3.). The enzyme possesses a single active site that is used for each
porphobilinogen condensation (Warren and Jordan 1988, Louie et al. 1992). In E. coli (the
corresponding human residues are in parenthesis), the dipyrromethane cofactor is covalently
bound to cysteine-242 (Cys261). In addition, residues aspartate-84 (Asp99), arginines 131, 132,
149, 155 (Arg149, 150, 167, 173), lysine-83 (Lys98), as well as some other residues form salt-
bridge and hydrogen bond interactions with the cofactor (Brownlie et al. 1994). The positively
charged side chains of Arg11, 132, and 155 (Arg26, 150, 173) are thought to interact with the
substrate (Lambert et al. 1994).
Fifty-eight residues in the PBGD polypeptide are invariant according to amino acid sequence
deduced from the nucleotide sequence determination from a wide range of organisms, and the
conserved amino acids are clustered in hydrophobic core of the molecule, in other
conformationally important locations, or at the active site. This suggests a similar structure and,
furthermore, similar mechanism of catalytic activity in organisms with different phylogenetic
age (Brownlie et al. 1994).
2.5. Molecular genetics of acute intermittent porphyria
2.5.1. The porphobilinogen deaminase gene
The gene coding for PBGD, which has been identified and thoroughly characterized (Raich et
al. 1986, Grandchamp et al. 1987, Chretien et al. 1988, Lee 1991a, Namba et al. 1991, Yoo et
al. 1993), is assigned to chromosome 11q24 (Namba et al. 1991). The size of the gene is 10 kb
of which 1.3 kb represents coding sequence. The genomic sequence is divided into 15 exons
ranging from 39 and 438 bp and 14 introns ranging from 87 to 2913 bp (Figure 2.4.).

REVIEW OF THE LITERATURE 24
Figure 2.4. The porphobilinogen deaminase gene and two mRNAs transcribed by alternativesplicing.
Two isoforms, arising from different promoters, are transcribed (Chretien et al. 1988). The
mRNA of the housekeeping (non-erythropoietic) isoform contains exons 1 and 3 to 15 coding
for an enzyme of 361 amino acids, whereas the erythroid isoform is encoded by exons 2 to 15
(Figure 2.4). The translation initiation codon for the housekeeping isoform is located in exon 1
and for the erythroid-specific isoform in exon 3. The erythroid isoform, thus, lacks the first 17
amino acids of the amino terminus.
The erythroid promoter region is located in intron 1 and its structure is very similar to that of
the β-globin gene (Chretien et al. 1988). The erythroid-specific transcript, thus, appears to be
regulated by similar set of transcription factors, suggesting that both genes are similarly
regulated during erythroid differentiation (Mignotte et al. 1989). The promoter region for the
housekeeping transcript is located upstream of exon 1 (Chretien et al. 1988, Yoo et al. 1993).
The minimal promoter sequence has been identified by deletion mapping (Lundin and Anvret
1997) and it is located between -243 and -115 nucleotides from the translation initiation codon.
This region contains two Sp1 consensus recognition sequences, a 13 bp repeat sequence, and an
AP1 consensus recognition sequence. In addition, sequence elements that have negative
regulatory function are located closer to the translational initiation site (Lundin and Anvret
1997).

REVIEW OF THE LITERATURE25
To date, thirteen intragenic polymorphisms have been identified in the PBGD gene (Lee and
Anvret 1987, Llewellyn et al. 1987, Lee et al. 1988, Gu et al. 1991, Lee 1991b, Picat et al.
1991, Daimon et al. 1993a, Yoo et al. 1993, Law et al. 1999, Whatley et al. 1999). One of the
polymorphisms is exonic, located in exon 10, but it does not alter the amino acid sequence.
Nine polymorphisms are located in intron regions of the gene; four of them are found in intron
1, the longest (2.9 kb) intron in the PBGD gene. In addition to the intragenic polymorphisms,
two polymorphisms have been identified in the non-erythroid promoter region (Picat et al.
1991, Schreiber et al. 1992, Lundin and Anvret 1997).
Six Alu elements have been found in the intronic sequences of the PBGD gene. Alu elements
are derived from 7SL RNA by internal deletions or point mutations of the 7SL sequence
followed by dimerization (Makalowski et al. 1994). They integrate throughout the primate
genomes via a process called retroposition (Rogers 1985) which involves generation of an RNA
polymerase III transcript, reverse transcription, and integration at staggered nicks within AT-
rich regions of the genome (Jagadeeswaran et al. 1981). A typical Alu element is 282
nucleotides long and it is composed of two homologous but distinct subunits. Alu repeats can
be divided into various subfamilies based on the presence of commonly shared diagnostic
mutations (Jurka 1993). Two of the Alu sequences in the PBGD gene are located in the 5'
flanking region, three in intron 1. The sixth Alu element is in intron 9 and is the only Alu in
sense orientation. Five of the Alu sequences belong to the relatively modern Sa subfamily
whereas one is homologous to the older J subfamily (Yoo et al. 1993).
2.5.2. Mutations resulting in AIP
Up to July 1999, 149 different mutations resulting in AIP had been identified in the PBGD gene
worldwide (Table 2.3.).
Of the mutations, 56 (38%) are substitutions of one amino acid and 37 (25%) mutations affect
splicing. Fifteen mutations result in an immediate termination codon and, furthermore, 36
mutations cause frame shifts which have been predicted to lead to a premature termination
codon after a variable number missense amino acids. One mutation hits the translation initiation

REVIEW OF THE LITERATURE 26
Figure 2.5. Location and type of identified mutations in the PBGD gene
codon and the remaining three mutations are deletions or insertions, which do not cause frame
shift.
Figure 2.5. shows the distribution of the mutations by location and mutation type. No mutations
causing AIP have been identified in exon 2 and its flanking sequences. This was somewhat
expected, because exon 2, transcribed only to the erythroid mRNA, does not code for
polypeptide since the initiation codon of this isoform is located in exon 3. Mutations
responsible for AIP are dispersed quite evenly in the PBGD gene and there is no hot spot for
the mutations. Twenty-nine (19%) of the mutations are located in exon 12, which is clearly the
highest number of all exons, but this exon the second longest exon in the PBGD gene and it is
almost twice as long as the majority of other exons (Figure 2.4.). Notably, six of eight residues
known to be crucial for the enzyme activity (R26, K93, D94, R149, R150, R167, R173, and
C261) are substituted resulting in AIP, only at positions K93 and R150 there are no reports of
mutations so far.
In the light of the mutations published in the PBGD gene so far, the molecular genetic
background is highly heterogeneous despite the rather uniform clinical manifestations of the
disease. Although studies of geno/phenotype comparisons have not yet been published, nothing

REVIEW OF THE LITERATURE27
implies that the type or the location of the mutation affects the clinical manifestations of the
disease. Furthermore, it seems that most of the mutations in the PBGD gene dramatically
decrease the enzymatic activity of the polypeptide encoded by the mutant allele.

REV
IEW O
F THE LITER
ATU
RE
28Table 2.3. Characterized mutations in the PBGD gene.Mutation Outcome Ref.* Mutation Outcome Ref.* Mutation Outcome Ref.*Exon 13G T translation defect (1)33G T splicing defect (2)Intron 1IVS1+1G A splicing defect (3)IVS1+2T A splicing defect (4)IVS1+5C G splicing defect (4)Exon 364C T R22C (5)66C G del exon 3 (6)70G A G24S (7)77G A R26H (8)83G A S28N (9)Intron 3IVS3+1G A splicing defect (10)Exon 491G A A31T (11)91G C A31P (12)100C A Q34K (13)125T A L42X (14)125T C L42S (12)158insA frame shift (7)Intron 4IVS4+1G A del exon 4 (12)IVS4+1G T del exon 4 (9)IVS4-6C G del exon 5 (12)IVS4-2A C del exon 5 (12)IVS4-1G C splicing defect (15)Exon 5163G T A55S (11)168delGT frame shift (16)174delC frame shift (11)181G A D61N (12)182insG frame shift (11)184delAA frame shift (12)206delCT S69X (9)
Intron 5IVS5+1G A del exon 5 (11)IVS5+2insG del exon 5 (9)IVS5+2T C del exon 5 (12)Exon 6218delAG frame shift (11)254T G L85R (12)Intron 6IVS6+1G C splicing defect (17)Exon 7269T G V90G (12)277G T V93F (1)287C T S96F (18)291delG frame shift (7)295G C D99H (18)314insC frame shift (16)323insT frame shift (12)331G A G111R (19)340insT frame shift (12)342C A C114X (9)Intron 7IVS7+33G T del exon 7 (12)IVS7-1G A del exon 8 (20)Exon 8346C T R116W (21)347G A R116Q (22)356C T P119L (10)365C G A122G (23)371T A V124D (9)del 704 bp frame shift (23)421delG del exon 8 (12)Intron 8IVS8+1G T splicing defect (10)Exon 9446G A R149Q (24)
446G T R149L (11)463C T Q155X (25)470insA frame shift (26)489insTCCT frame shift (12)Intron 9IVS9-1G A del exon 10 (27)Exon 10499C T R167W (28)500G A R167Q (29)500delG frame shift (9)517C T R173W (30)517del17bp frame shift (9)518G A R173Q (29)530T G L177R (13)532G A D178N (9)541C T Q181X (12)576del 19bp frame shift (9)589del 17bp frame shift (31)593G A W198X (32)601C T R201W (27)604delG frame shift (26)610C T Q204X (22)612G T del 3 aa (24)Intron 10IVS10+2TAGGG CCCTA
splicing defect (15)IVS10+2T C del exon 10 (9)IVS10-31A G del exon 11 (9)Exon 11625G A E209K (33)629delA frame shift (34)639T G Y213X (9)646G A G216D (17)650A T Q217L (35)651G T Q217H (9)

REV
IEW O
F THE LITER
ATU
RE
29
Mutation Outcome Ref.* Mutation Outcome Ref.* Mutation Outcome Ref.*Intron 11IVS11+1G C splicing defect (15)IVS11+2T C ins intron 11 (12)IVS11+3C G splicing defect (6)IVS11-2A G splicing defect (15)IVS11-1G C del exon 12 (9)IVS11-1delG del exon 12 (9)Exon 12656C A A219D (12)667G A E223K (11)678insAA frame shift (12)691del30bp truncated protein? (9)715delCA frame shift (14)716insC frame shift (31)721delC frame shift (12)723ins21bp 7 aa repeat (9)730delCT frame shift (36)734T G L245R (24)739T C C247R (36)742ins8bp frame shift (11)748G C E250A (10)748ins8bp frame shift (12)748G A E250K (11)749A T E250V (9)
749A C E250A (9)754G C A252T (37)754G A A252T (36)755C T A252V (36)761T C L254P (23)766C A H256N (13)766C T H256Y (9)771insT frame shift (38)771G A del exon 12 (39)771G C del exon 12 (40)Intron 12IVS12+1G A del exon 12 (14)IVS12+1G T del exon 12 (7)IVS12-1G A del exon 13 (9)Exon 13782G A C261Y (23)794insAGCC frame shift (12)799G A V267M (7)806C T T269I (22)809C A A270D (9)809C G A270G (31)820C A G274R (22)823C T Q275X (9)
Intron 13IVS13+1G A del exon 13 (6)Exon 14847delTG frame shift (17)848G A W283X (22)849G A W283X (16)854delTA frame shift (9)863C A S288X (9)863C G S288X (15)866delATAG frame shift (12)874C T Q292X (35)900insT frame shift (41)900delT frame shift (24)Intron 14IVS14+1G T del exon 14 (12)IVS14+1G A del exon 14 (19)Exon 15913insC frame shift (14)973C T R325X (42)982delG frame shift (12)986insT frame shift (15)1004delG frame shift (5)1004G A G335D (9)1062insC frame shift (43)
* 1, Chen et al. 1994; 2, Grandchamp et al. 1989c; 3, Grandchamp et al. 1989b, 4, Puy et al. 1998; 5, Ong et al. 1998; 6, Llewellyn et al. 1996; 7,Rosipal et al. 1997; 8, Llewellyn et al. 1993; 9, Puy et al. 1997b; 10, Lundin et al. 1995; 11, Gu et al. 1994; 12, Whatley et al. 1999; 13, Mgone et al.1992; 14, Puy et al. 1996; 15, Petersen et al. 1998; 16, Schreiber et al. 1995a; 17, Lundin et al. 1997; 18, Deybach and Puy 1995; 19, Gu et al. 1993a;20, Schreiber et al. 1994b; 21, Lee et al. 1990; 22, Mgone et al. 1994; 23, Brownlie et al. 1994; 24, Delfau et al. 1991; 25, Scobie et al. 1990; 26,Schreiber et al. 1994a; 27, Lundin et al. 1994; 28, Gu et al. 1992; 29, Delfau et al. 1990; 30, Lee 1991a; 31, Lee and Anvret 1991; 32, Puy et al.1997a; 33, Grandchamp et al. 1992; 34, Lee et al. 1994; 35, Schneider-Yin et al. 1999; 36, Mgone et al. 1993; 37, article IV; 38, Ong et al. 1996; 39,Grandchamp et al. 1989a; 40, Daimon et al. 1993b; 41, Schreiber et al. 1995b; 42, Petersen et al. 1996; 43, Daimon et al. 1994

AIMS OF THE STUDY 30
3. AIMS OF THE PRESENT STUDY
In the beginning of this study in 1993, the specific mutation resulting in AIP was identified only
in 9 (23%) of the 40 known Finnish AIP families. Furthermore, at that time very little was
known about the molecular mechanisms of how a mutation in the PBGD gene results in a
defective enzyme.
The aims of this study were:
1) To identify the gene defects resulting in AIP among Finnish patients.
2) To develop a method for screening of the PBGD gene for novel mutations and to develop
methods for DNA diagnostics of AIP for Finnish families.
3) To characterize the consequences of selected AIP mutations at the mRNA or polypeptide
and cellular level.

MATERIAL AND METHODS31
4. MATERIAL AND METHODS
4.1. Patients
A register for Finnish porphyria patients was established in 1966 and to date it comprises of
approximately 250 AIP patients belonging to 40 different families (Kauppinen and Mustajoki
1992). In the classical form of AIP the diagnosis has been based on typical clinical
manifestations or on increased excretion of porphobilinogen in urine (Mauzerall and Granick
1956) and on low PBGD activity in erythrocytes (Ford et al. 1980). In the majority of cases, the
pedigrees have been traced up to the 19th century and in some cases up to the 17th century
(Mustajoki and Koskelo 1976). According to this analysis, the families are not related to each
other. A DNA sample, and in most cases also a RNA sample, was available from at least one
patient from each family. In addition, DNA samples of healthy family members and healthy
unrelated controls have been available. The study protocol has been approved by the Ethics
Committee of the Third Department of Medicine, University of Helsinki.
4.2. DNA and RNA isolation, and cDNA synthesis
Leukocyte DNA was extracted from venous blood samples using the method described in
(Sambrook et al. 1989) or DNA was released from leukocytes as described by Higuchi (1989).
Total RNA was prepared from lymphoblastoid cells using the guanidium isothiocyanate method
(Chirgwin et al. 1979). Complementary DNA was synthesized from 2-5 µg of total RNA using
M-MuLV Reverse Transcriptase (New England Biolabs, ME, USA), RNase inhibitor (RNAsinR
Promega, WI, USA), dNTPs, and random hexanucleotide mix (Boehringer Mannheim,
Germany) or a specific primer for 3' untranslated region of the PBGD gene.
4.3. DNA amplification
Isolated DNA (final concentration 2-5 ng/µl), lysed leucocyte sample (1:10 v/v), or RT product
(3:20 v/v) was used as the template for polymerase chain reaction (PCR, Mullis and Faloona
1987). The PCR reaction mixture contained 16-23-mer primers (0.2-1 mM), dNTPs at 0.2 mM

MATERIAL AND METHODS 32
concentrations and 0.03 U/µl of DNA polymerase (DynazymeR, Finnzymes, Finland) in enzyme
buffer. The temperature profile for the PCR reactions was 2 min at 94oC for the first
denaturation step, followed by 30-60 s at 94oC, 30-60 s at 54-60oC, and 30-90 s at 72oC for 30
cycles. The other primer was biotinylated if the PCR product was used in sequencing or
minisequencing reactions. The primer sequences are given in original articles I-V.
4.4. Subcloning
When the consequences of mutations in the exon/intron boundaries (IVS1+3G T and IVS13-
2A G) were studied, the normal allele interfered with direct sequencing and both alleles were
studied separately by subcloning. In the case of Alu insertion, the normal allele and poly T
region interfered with direct sequencing of the branch points, and the 318 bp and 651 bp
fragments including exon 5 were amplified from a patient's genomic DNA sample. After
amplification, digestion and purification, the fragments were ligated into the corresponding
restriction sites of the pUC18 vector (Pharmacia, Sweden), transformed in E. coli and both
alleles were sequenced separately.
4.5. Mutation screening
Mutations were examined using two different screening methods: single-strand conformation
polymorphism (SSCP, Orita et al. 1989) and denaturing gradient gel electrophoresis (DGGE,
Myers et al. 1987, Nissen et al. 1995). Prior to SSCP, the 32P-labeled PCR products, which
covered exon 1 and exons 3 to 15 of the PBGD gene, were digested into shorter fragments
when longer than 500 bp. The primer sequences and restriction enzymes used are given in
article I. The samples were diluted 1:5 in 1% sodium dodecyl sulfate (SDS)/10mM edetate
disodium tetraacetic acid (EDTA), mixed with an equal volume (3 µl) of 95% (vol/vol)
formamide/20 mM EDTA containing 0.05% bromophenol blue and 0.05% xylene cyanol, and
denatured by heating. The diluted and denatured sample was electrophoresed in a 5%
bis/acrylamide (60:1) gel using different glycerol and TBE-buffer concentrations at 4oC or
room temperature. After drying the gels were autoradiographied at -70oC for 12-48 h.

MATERIAL AND METHODS33
For DGGE, to the 5' end of one of the PCR primers was attached a 40-50-bp-long stretch of
guanosine and cytidine nucleotides (GC-clamp) to increase the sensitivity of DGGE (Sheffield
et al. 1989). The GC-clamped PCR-products were run on linearly increasing denaturing
gradient polyacrylamide gels of 20%-60% denaturant at 60oC for 5 hours. After electrophoresis,
the gel was stained with ethidium bromide and visualized with ultraviolet translumination.
4.6. Sequencing
The PCR products were purified using the Qiagen Gel Purification Kit (Qiagen, CA, USA) or
Fluoricon avidin-polystyrene-assay particles (Idexx Laboratories, ME, USA), which was used
if PCR was performed with biotinylated primers. The DNA was sequenced in both sense and
antisense directions using the dideoxynucleotide chain termination method (Sanger et al. 1977)
with commercial kits (Sequenase 2.0 Sequencing Kit, USB, OH, USA or Amplicycle
Sequencing Kit, Perkin Elmer, CT, USA) according to the manufacturers' instructions.
4.7. Solid-phase minisequencing
The solid-phase minisequencing method (Syvänen et al. 1993) was used to identify the variable
nucleotide in the sample. Figure 1 in article V shows schematically the steps of solid-phase
minisequencing. The method is suitable for screening a previously identified mutation, and it
may also be used for quantitative measuring.
PCR was performed as described above with the exception that the PCR mixture contained
biotinylated and unbiotinylated primers in proportion of 1:5. For each minisequencing reaction
10 µl of the PCR product and 40 µl of sodium phosphate buffer were added to streptavidin-
coated microtiter wells and incubated at 37oC for 90 minutes. The wells were washed three
times and denatured twice with sodium hydroxide at room temperature. To each well was added
50 µl mixture containing specific primer, DNA polymerase, and [3H]dNTP. The labeled
nucleotide was hybridized next to the minisequencing primer during the 10-minute incubation
at 50oC. The nucleotides not incorporated were washed out as described above. The primer

MATERIAL AND METHODS 34
hybridized with labeled nucleotide was denatured with sodium hydroxide. The radioactivity
eluted with sodium hydroxide was counted in a liquid scintillation counter.
4.8. In vitro mutagenesis
Mutagenesis was performed using a Chameleon Double-Stranded Site-Directed Mutagenesis
Kit (Stratagene, CA, USA) according to the manufacturer's instructions. The full-length coding
region of the PBGD cDNA (Grandchamp et al. 1989a), used as a template, was ligated in
between the HindIII and EcoRI sites of mammalian expression vector SVpoly (Stacey and
Schnieke 1990). The oligonucleotides used in each mutagenesis reaction are given in
publication VI. The selection primer was located in the polylinker region of SVpoly which
removed the cleavage site for XbaI. Mutant clones were confirmed by sequencing.
4.9. COS-1 cell culture and DNA transfection
COS-1 cells were maintained in Dulbecco's modified Eagle's medium (Gibco-BRL, NY, USA)
supplemented with 10% fetal heat-inactivated bovine serum and antibiotics. For transfection,
the cells were seeded on a 3 cm 6-well plate at 4*105 cells/well and grown overnight. The cells
were transfected with 1.5 µg of the plasmid construct by lipofection (Felgner et al. 1987) using
FuGENE 6 transfection reagent (Boehringer Mannheim, Germany). Forty-eight hours post-
transfection the cells were either harvested for the PBGD activity and Western blot analyses, or
pulse-chase experiments were performed.
4.10. Enzyme activity assay
One hundred µl of the cell lysate in 1.0 ml of 1% Triton X-100 was pre-incubated at +37oC for
15 minutes prior to adding 500 µl of 1.4 mM porphobilinogen in phosphate-citrate buffer (Ford
et al. 1980). The mixture was incubated for 30 minutes at +37oC and the reaction was stopped
with 2.5 ml of 10% trichloride-acetatic acid. The fluorescence of the supernatant was measured
using 100 µg/l uroporphyrin I standard at the excitation wavelength of 407 nm and the emission
wavelength of 598 nm. Protein concentration in a cell lysate was determined by a dye-binding

MATERIAL AND METHODS35
reaction (Bio-Rad Protein Assay, CA USA). An expression vector control was used to monitor
the background expression of PBGD in COS-1 cells.
4.11. Western blot
A mixture of 20 µl of cell lysate in phosphate-buffered saline (PBS) containing 1% Triton X-
100, 5 µl of 5 x Laemmli’s reagent (Laemmli 1970), 1 µl dithiothreitol , and 1 µl of 20% SDS
was run a 14% SDS-polyacrylamide gel. The gel was electroblotted on a nitrocellulose filter.
The filter was filled with 5 % bovine milk proteins and reacted with a 1:2000 dilution of
polyclonal rabbit anti-human-PBGD antibody (Lannfelt et al. 1989b). Anti-rabbit IgG-Alkaline
Phosphatase conjugate (1:7500, Promega) was used as a secondary antibody and the proteins
were visualized using 0.66% nitro blue tetrazolium and 0.33% 5-bromo-4-chloro-3-indolyl-1-
phosphate (Promega).
4.12. Pulse-chase and immunoprecipitation
The cells were starved in a cysteine- and methionine-free medium for 60 min before labeling
with 200 µCi/ml Promix (35S-Cys + 35S-Met, Amersham, UK). A one-hour pulse was followed
by 1-23 hour chase in normal medium without bovine serum. After the chase period the cells
were harvested and resuspended in PBS containing 1% Triton X-100 and lysed by freeze-
thawing three times.
The PBGD proteins were immunoprecipitated from the cell lysates using polyclonal rabbit
PBGD antibodies (1:2000) and formalin-fixed Staphylococcus aureus cells (Pansorbin cells,
Calbiochem, CA, USA, Proia et al. 1984). The labeled and precipitated proteins were separated
by 14% SDS-polyacrylamide gel and visualized by autoradiography.
4.13. Immunofluorescence
For immunofluorescence staining the transfected COS-1 cells were grown on 12 mm coverslips
and fixed in 3% paraformaldehyde for 30 min at room temperature. After fixation the cells were

MATERIAL AND METHODS 36
washed in PBS and permeabilized in PBS containing 0.2% saponin, 0.5% bovine serum
albumin (BSA) for 30 min at room temperature. This was followed by incubation with a 1:2000
dilution of PBGD antibody for 30 min at room temperature. The cells were washed in PBS
containing 0.2% saponin and 0.5% BSA and incubated with 1:150 dilution of rhodamine-
conjugated secondary antibody against rabbit immunoglobulins (Immunotech, MA, USA) in the
same buffer for 45 min at room temperature. The cells were washed in PBS and mounted on
slides in 87% glycerol.

RESULTS AND DISCUSSION37
5. RESULTS AND DISCUSSION
Prior to this study 4 mutations in 9 Finnish AIP families had been identified (Kauppinen
1992a). The search for an underlying genetic defect in the remaining 31 families was begun
using SSCP analysis. The PCR fragments were designed to cover exons 1 and 3 to 15 of the
PBGD gene. Exon 2 was not analyzed, since it encodes only erythroid isoform. If a mobility
shift was detected in SSCP analysis, the corresponding PCR product was direct sequenced. The
identified mutations and their outcome are discussed in Chapters 5.1. and 5.5.
The sensitivity and specificity of the DGGE method for identifying mutations in the PBGD
gene was tested. Because two different screening methods - SSCP and DGGE - were used in
this series of investigation, their efficiency has been compared. However direct comparison was
not possible since the DGGE method was tested blindly and prospectively and the overall
sensitivity of SSCP method was analyzed retrospectively (Chapter 5.2.).
The steady state transcript levels of six different mutant alleles were accurately determined
using solid-phase minisequencing. In addition, whenever RNA isolated from the patient's
lymphoblastoid cell line was available, amplified cDNA was sequenced, which provides a
rough estimate of the transcript level of the mutant allele (Chapter 5.3.).
To study further the consequences of mutations in the PBGD gene, seven different mutant
cDNA constructs were produced and expressed in eukaryotic COS cells. The properties of
mutant proteins were investigated by PBGD activity measurements, and pulse-chase and
immunofluorescence studies (Chapter 5.4.).
5.1. Identified mutations (I, II, III)
The series of investigations presented here have revealed 22 additional defects in the PBGD
gene resulting in AIP (Table 5.1., Figure 5.1.). Combined with previously identified genetic
defects the 26 characterized mutations cover 38 (95%) of a total of 40 unrelated Finnish AIP
families.

RESULTS AND DISCUSSION 38
The mutation was always confirmed by direct sequencing the sample in the other direction or
by restriction enzyme analysis when available. When a mutation was identified and its
segregation with the disease was confirmed in the family, no further sequencing was performed.
In each patient, thus, one to 14 exons were sequenced before a mutation was identified. To
exclude a rare polymorphism, the nucleotide sequence of exons 12 and 14 in 50 Finnish
unrelated healthy controls was determined and this analysis revealed no sequence variations.
When performing the DGGE analysis of the patients’ genomic DNA samples, all mutations,
except the large insertion in exon 5, resulted in a deviated pattern in the corresponding exon.
None of the DGGE patterns similar to these mutations were observed when the DNA samples
of more than 50 Danish AIP patients were analyzed. In addition, a variable number of unrelated
healthy controls and healthy family members were analyzed for each mutation. Thus, a rare
polymorphism was considered very unlikely.
As in most other populations (Table 2.3.), also in Finland the AIP mutations are highly
heterogeneous both in their type and location. Furthermore, almost all mutations are family
specific. Thirteen (50%) mutations are located in exons 10, 12, and 14. Of the twelve missense
mutations (46% of all identified mutations), six are substitutions of an arginine residue. A
substitution of one base pair causes a nonsense codon in five cases. In addition, two deletions
and two insertions result in a frame shift leading to a premature termination codon after a
variable number of missense codons. Four mutations affect the splicing of the primary
transcript. As a consequence of two splicing mutations (IVS+3G T, IVS13-2A G), the intron
sequence is retented into the transcript and a premature termination codon is introduced. One
splicing mutation (86A T) was shown to result in exon skipping and a truncated protein, but
in the case of a splicing defect in exon 1 (33G T) no mutant transcript could be detected
(Kauppinen 1992b). Deletion of one nucleotide in the last exon results in a frame shift which
removes the normally utilized termination codon and no additional termination codon is
available before the polyadenylation signal.
In two (5% of all Finnish AIP families ) AIP patients the genetic defect causing AIP remains
unknown. In these patients, the diagnosis was based on typical clinical manifestations and on
increased excretion of porphobilinogen in urine and/or on low PBGD activity in erythrocytes.

RESULTS AND DISCUSSION39
Figure 5.1. Identifying the mutation bydirect sequencing. As an examplemutation 673C G.
Both patients are the only affected individuals in their families. In the one patient's sample there
was a mobility shift in exon 11 when DGGE analysis was performed, whereas the other
patient's DGGE analysis was negative. The entire coding sequence and flanking intronic
regions were sequenced and no nucleotide alteration was found in the genomic DNA samples
of these patients. Neither did the amplification of the PBGD gene in long fragments (3.4-4.5
kb) reveal additional information.
The genetic defect remained unsolved in some cases also in a French study, where the
mutations were systematically searched for using DGGE analysis and sequencing (Puy et al.
1997b). The patient material comprised of 405 patients from 121 unrelated AIP families, and in
1 2 ( 1 0 % ) f ami l i e s t he DGGE sc reen in g w a s n o r ma l a n d n o b a s e c h a n ge s
were identified despite sequencing all exons and exon/intron junctions. Based on the data from
Finland and France, sequencing only the coding areas and flanking intronic regions of the
PBGD gene does not seem to guarantee the detection of all mutations. In these patients the
underlying defect may be the in promoter region, in the middle of intronic sequence, or it may
be a large insertion or deletion which remains non-detectable with the methods used in these
s tud ie s . Because the en zyme a c t i v i t y me a s u r e me n t h as wide ove r l app ing
zone and urinary PBG and dALA are elevated also in other porphyrias, the subjects may also
have been misdiagnosed as AIP patients.

RESULTS AND DISCUSSION 40
Table 5.1. Identified mutations in Finnish AIP patients
Mutation Location Outcome cDNAa CRIMb Enzymec No. offamilies Ref.d
1 33G T 1 splicing defect - - HphI 1 (1)
2 IVS1+3G T intron 1 intron 1 retention + - HphI 1 II
3 76C T 3 Arg26 Cys + + BspMI 1 I
4 86A T 3 exon 3 skipping + - BstXI 1 II
5 97delA 4 frame shift + - 3 I
6 100C T 4 Gln34 Stop + - 1 I
7 Ins 332 bp 5 frame shift - - 1 III
8 293A G 7 Lys98 Arg n.d. - NlaIV 1 I
9 346C T 8 Arg116 Trp - - 1 (2)
10 417insCA 8 frame shift n.d. - 1 II
11 445C T 9 Arg149 Stop - - 2 I
12 499C T 10 Arg167 Trp + + 5 (3)
13 517C T 10 Arg173 Trp + -/(+) MspI 2 (4)
14 518G A 10 Arg173 Gln + + MspI 4 (5)
15 583C T 10 Arg195 Cys n.d. - HhaI 1 I
16 593G A 10 Trp198 Stop - - NheI 1 (6)
17 664G A 12 Val222 Met + - 1 II
18 673C G 12 Arg225 Gly + - NlaIV 1 I
19 673C T 12 Arg225 Stop - - 2 I
20 713T G 12 Leu238 Arg - - BbvI 1 I
21 740G T 12 Cys247 Phe + - Fnu4HI 1 I
22 IVS13-2A G intron 13 intron 13 retention + - MspI 1 II
23 833T C 14 Leu278 Pro + - BslI 1 II
24 838G A 14 Gly280 Arg - - MaeI 1 I
25 886C T 14 Gln296 Stop - - 1 I
26 1073delA 15 frame shift - - MseI 1 Ia +, mutation seen in cDNA; - mutation not seen in cDNA; n.d., not done.b CRIM, cross-reactive immunologic material; +, inactive protein detected;
-, no inactive protein detected.c Mutation specific restriction enzyme.d First described by: 1, Grandchamp et al. 1989b; 2, Lee et al. 1990; 3, Gu et al. 1992;
4, Lee 1991a; 5, Delfau et al. 1990; 6, Lee and Anvret 1991.

RESULTS AND DISCUSSION41
5.2. SSCP and DGGE in screening for novel mutations (I, II, III, IV)
Mutations were searched for using two different screening methods: single-strand conformation
polymorphism (SSCP, Orita et al. 1989) and denaturing gradient gel electrophoresis (DGGE,
Myers et al. 1987, Nissen et al. 1995). SSCP analysis is based on the mobility shifts of a single-
stranded DNA under renaturing conditions. During electrophoresis the single-stranded DNA
rehybridizes and the migration position is determined by the secondary structure, which is
influenced by the sequence variants. In DGGE analysis the amplified DNA samples are run on
a gel, in which the amount of denaturant is gradually increased. Sequence variation in the
sample has an effect on the melting point which alters the migration. Previously, both SSCP
(Kauppinen et al. 1992, Chen et al. 1994, Schreiber et al. 1994a, Schreiber et al. 1994b,
Schreiber et al. 1994c, Schreiber et al. 1995b) and DGGE (Gu et al. 1992, Gu et al. 1993b, Gu
et al. 1994, Petersen et al. 1996, Puy et al. 1996, Nordmann et al. 1997, Puy et al. 1997a, Puy
et al. 1997b, Rosipal et al. 1997, Petersen et al. 1998, Puy et al. 1998) have been used in
searching for mutations responsible for AIP.
The overall sensitivity of SSCP in screening mutations of the PBGD gene was 90%, i.e.18 of
the 20 identified mutations could be detected using this method when five different
electrophoretic conditions (glycerol concentration was 0%, 5%, or 10% and the gel was run at
+4oC or at room temperature) were used. However, the sensitivity of SSCP was significantly
lower if only a single electrophoretic condition was used: gel electrophoresis at room
temperature with 5% and 10% glycerol detected 12/20 (60%) and 14/19 (74%) of the
mutations, respectively, while gel electrophoresis at +4oC without glycerol detected 15/19
(79%) of the mutations. The length of the analyzed PCR fragment had a variable effect on the
sensitivity of the analysis: in the case of mutation 97delA both an increase and a decrease in the
size of the fragment (510 bpÏ446 bp 324 bp or 189 bp) from the original resulted in a shift
and in SSCP analysis of mutation 1073delA even minor changes in the size of the fragment
(192 bp or 197 bpÏ211 bp 228 bp) caused disappearance of the mobility shift. The specificity
of the SSCP method was not evaluated in this study.

RESULTS AND DISCUSSION 42
The efficacy of the DGGE method in detecting mutations causing AIP was evaluated by
analyzing blindly the DNA samples of 22 AIP patients and 6 healthy controls. As a result, the
correct mutation carrying region was found in samples of all 22 patients, but in two samples
two potential regions were initially highlighted. In both cases, the false positive pattern was
located in exon 7 and flanking intron sequencing, and sequence analysis revealed a previously
unknown polymorphism in intron 6. Common polymorphisms in the PBGD gene could easily
be distinguished from mutations because the number of analyzed samples was relatively high
and the location of polymorphic sequence variations was known. The DGGE patterns in all
healthy controls were normal, only common polymorphisms could be identified. In addition six
mutations described in article II, which were not included in the study with a blinded design,
resulted in a mobility shift in the corresponding region.
However, DGGE analysis could not identify the 333 bp Alu insertion located in exon 5. This
was expected since the length of the normal fragment covering exons 5 and 6 in DGGE analysis
is 393 bp and in the patient sample the PCR product is almost twice as long, 726 bp. The allele
with the insertion migrates more slowly and most probably will not reach the analytical area in
the gel by the end of the electrophoresis. When the results of these studies are combined, the
sensitivity of DGGE analysis was 96% (25/26 mutations could be identified with the method)
and the specificity was 94% (two false positive mobility shifts in 35 samples).
The DGGE and SSCP methods have previously been evaluated both in the screening of the
PBGD gene and several other genes, and the earlier results are in good agreement with the data
obtained from our experiments. When several sets of electrophoretic conditions is used, SSCP
detects 70-95% of mutations but using only one condition reduces the sensitivity considerably
(Michaud et al. 1992, Grompe 1993, Moyret et al. 1994). Furthermore, the sensitivity of this
method has been reported to be highest when the fragment size is below 200 bp (Grompe
1993), which limits the usefulness of the method when large genes are screened for mutations.
The sensitivity of DGGE has been estimated to be as high as 95-100% in several studies
(Grompe 1993, Moyret et al. 1994, Macek et al. 1997, Puy et al. 1997a, Puy et al. 1997b) and
single base differences can be detected with high accuracy in PCR products of up to 600 bp in
length.

RESULTS AND DISCUSSION43
DGGE appears, thus, to be superior in sensitivity when compared with SSCP. However, the
setup of the DGGE method is laborious: the running conditions of each fragment needs to be
optimized separately but tuning up of the system may be assisted by computer analysis. Once
conditions are finalized, the DGGE analysis proceeds rapidly. SSCP method has gained
popularity because of its simple and straightforward implementation. Although it is a powerful
method, the sensitivity of SSCP has not reached the same level as DGGE. Furthermore, the
method lacks guidelines for its optimization for a defined DNA sequence (Michaud et al. 1992,
Moyret et al. 1994) and it usually requires the use of radioactive nucleotides to label the
fragments to be analyzed.
5.3. Monitoring the effect of mutations to allelic transcript levels (V)
The steady state level of allelic transcripts in lymphoblasts of eight AIP patients were analyzed
using solid-phase minisequencing. The patients had the following mutations: 517C T
(R173W), 518G A (R173Q), 673C G (R225G), 673C T (R225X), 713T G (L278P) and
1073delA (frame shift). All mutations, except the missense mutation 517C T in exon 10,
affected the steady state transcript levels of the mutant allele (Table 5.2.). The mutant mRNA
levels in lymphocytes varied from 5 to 95% of the corresponding wild type allele levels. In
contrast to the CRIM negative mutation 517C T, the CRIM positive mutation in the same
codon 518G A resulted in reduction of the steady state transcript level of the mutant allele to
65% of that of the normal allele. Interestingly, the mutant transcript of the patient with mutation
517C T seemed to be more unstable than the normal transcript, because mutant transcript
seemed to degrade more rapidly during storage at -80oC. However, this preliminary finding was
not studied further.
Two of the mutations, 673C G or T (R225G or X), affecting the same nucleotide in exon 12
differed considerably in their effect on allelic transcript: the transcript level of the allele with
a missense mutation was decreased to 80% of that of the normal allele whereas the nonsense
mutation at the same position resulted in a dramatic decrease (5-fold) in the levels of the mutant
transcript. The mRNA samples of three subjects with the same nonsense mutation 673G T
(R225X) were also analyzed. Although clinical manifestations have been different in these

RESULTS AND DISCUSSION 44
patients, the steady state transcript levels were almost identical: 23%, 20%, and 24% of the
normal allele.
Even though the data showed variations between the levels of mutant transcript in AIP patients,
the mutant transcript level did not correlate to the CRIM class, to the location of the disease
causing mutation in the PBGD gene, or to the clinical phenotype of AIP.
Nonsense codons have been reported to dramatically decrease the mRNA levels of the mutant
allele and, typically, the closer the mutation is to 5' end of the transcript, the more dramatic is
the effect (Cooper 1993). Direct sequencing of amplified cDNA product gives in most cases a
rough estimation of the steady state transcript level of the mutant allele, since the mutant allele
is detected if its level is at least 30% of the normal allele. In our material the mutant allele
could be detected in sequenced cDNA in the case of four nonsense mutations: IVS1+3G T,
97delA, 100C T, and IVS13-2A G (Table 5.1.). Total RNA from the patient with mutation
417insCA was not available, and the remaining five nonsense mutations were not detected
when the corresponding cDNA was sequenced. This suggests that mutant allele gets transcribed
at least to some extent in the case of four nonsense mutations. Three of these four mutations are
located in exons 1 or 3 and one in intron 13. Those mutations which could not be detected by
sequencing of cDNA are located in exons 1, 5, 8, 10, 12 and 14 (Table 5.1.). Thus, our results
are not in agreement with the data obtained from mutations of other genes, since in those
mutant alleles that are transcribed the mutations are located closer to the 5' end of the PBGD
gene than those mutant alleles that are not transcribed. However, the low number of mutations
and the lack of accuracy of this method prevents us from drawing any definitive conclusions
concerning this finding.
Mutations resulting in premature termination codons do not decrease the rate of gene
transcription (Urlaub et al. 1989, Cheng and Maquat 1993). However, in the majority of cases
the levels of mutant mRNA, imposed by premature termination codon, are decreased (Cooper
1993, Peltz et al. 1994, Maquat 1995). Previously, it was anticipated that mRNA decay would
take place in the cytoplasm, because termination codon recognition requires cytoplasmic
ribosomes. Several pieces of evidence have, however, implied that the low levels of mutant

RESULTS AND DISCUSSION45
transcripts are due to nuclear events (Urlaub et al. 1989, Baserga and Benz 1992, Cheng and
Maquat 1993, Cooper 1993, Simpson and Stolzfus 1994, Carter et al. 1996)
The mechanisms of how premature termination codons reduce mutant mRNA levels are
obscure. Carter and co-workers (Carter et al. 1996) demonstrated that at least two signals are
required to trigger the down-regulation of mutant mRNA: a nonsense codon and a spliceable
downstream intron. According to this result, thus, premature termination codons in the last
exon would not affect the mutant RNA level.
The translational-translocation model (Urlaub et al. 1989) proposes that during mRNA export
from the nucleus to the cytoplasm, the 5' end of a transcript is scanned by cytoplasmic
translational machinery while the 3' end is still undergoing mRNA splicing, which is a nuclear
event. The premature nonsense codon in the nuclear pore-associated mRNA, scanned by a
cytoplasmic ribosome, would ultimately result in the decay of the mRNA. The length of the
nuclear pore has been estimated to be 15 nm or ~45 nucleotides of linear mRNA (Alberts et al.
1994). According to this model, hence, a nonsense codon should be at least 60 nucleotides (an
additional 15 nucleotides are required for the termination codon to be positioned at the P site of
the ribosome) from a downstream intron to be recognized in the cytoplasm before the intron is
spliced out in the nucleus. The studies on the T-cell receptor β-gene, however, suggested that
the border for nonsense-mediated mRNA down-regulation is below 10 nucleotides from the
exon/intron junction (Carter et al. 1996), and these data are inconsistent with the translational-
translocation model.
In the marker model (Carter et al. 1996) a downstream intron could act as a second signal to
trigger down-regulation. This model is based on the presumption that after splicing the previous
location of intron is marked on mature mRNA. The potential marker is a specific SR protein,
which remains bound to exons after RNA splicing, or the marker may be RNA which has
undergone post-transcriptional modification. This model allows the triggering of mRNA decay
before it has completely exited the nucleus, even if the premature termination was scanned by
a cytoplasmic termination codon.

RESULTS AND DISCUSSION 46
So far, the only known cellular structure that can scan codons is a cytoplasmic ribosome.
However, a model in which a nuclear component would recognize nonsense codon has been
proposed (Urlaub et al. 1989, Carter et al. 1996). Although there is no direct evidence for a
nuclear scanner, the model accounts for all the important features characterized in experiments:
mutant mRNA is destroyed in the nucleus, a spliceable intron acts as a second signal to trigger
mRNA down-regulation, and a nonsense codon may be located only 10 nucleotides upstream
of the last intron to trigger mRNA decay.
Unlike nonsense mutations, the effect of missense mutations on transcript levels has
characteristically been reported to be non-significant (Mustafa et al. 1995, Karttunen et al.
1996, Ploos van Amstel et al. 1996). In contrast, our results demonstrate that also missense
mutations can reduce the abundance of mutant mRNA. In our experiment we have used
Ebstein-Barr -virus infected lymphoblasts and the transcript levels in immortalized
lymphoblasts may differ from those in cells in vivo. However, an allele specific effect would be
unlikely and consequently we have here emphasized the relative ratios of mutant and wild type
allelic transcripts.
Table 5.2. Consequences of selected mutations on the steady-state transcript level andenzyme activity after eukaryotic expression.
Mutation Outcome CRIMMutant mRNA
as a ratio ofwild type mRNA
Enzyme activity±S.E. nmol/mg
prot/h b
76C T R26C + 105±17 (0%)
Alu insertion Trunc. protein - [270±80 (0%)]c
499C T R167W + 273±66 (5%)
517C T R173W - 0.97 173±33 (2%)
518G A R173Q + 0.66 140±11 (0%)
673C G R225G - 0.82 626±78 (16%)
673C T R225X - 0.22 142±9 (0%)
713T G L278P - <0.05
1073delA a frame shift - 0.72 1660±174 (50%)
Wild type 3173±507 (100%)

RESULTS AND DISCUSSION47
Control COS 127±7a Normally utilized termination codon abolished. The polypeptide synthesized by the
mutant construct differs from the predicted polypeptide in patients with thismutation.
b Mean value of four independent measurements. Percentage of mean normal activitycorrected with the endogenous COS-1 cell PBGD activity in parenthesis.
c Enzyme activity is not comparable because of separate assay.
5.4. Expression of mutated polypeptides (III, VI)
To analyze further the consequences of mutations on the function of PBGD enzyme, eight
mutations were introduced to PBGD cDNA and the mutated constructs were expressed in
eukaryotic COS cells. Six of the tested mutations (R26C, Alu insertion, R167W, R173W,
R173Q, R225X) resulted in the reduction of PBGD activity to the background level (0-5%).
These results confirm the assumed causality of the amino acid substitution and the low PBGD
activity measured in the patients’ erythrocytes. In two cases (R225G, 1073delA), however, the
enzyme activity was only partially disturbed and 16-50% residual activity could be detected
(Table 5.2.).
Western blot analysis shows that the mutant constructs R26C, R167W, R173W, R173Q, and
R225G expressed polypeptides which reacted with the antibodies directed against human
PBGD and the migration pattern was comparable with that of the normal enzyme (Figure 5.2.).
As predicted, the construct with mutation 1073delA removing the normally used termination
codon, produced a longer polypeptide. The constructs with R225X and Alu insertion, both of
which are predicted to result in a truncated protein, produced no detectable polypeptide in
Western blot analysis, suggesting that either the polyclonal antibody did not recognize the
truncated polypeptide or the polypeptide is very unstable.

RESULTS AND DISCUSSION 48
Figure 5.2. Western blot after expression of mutated PBGD constructs in COS cells.
The stability of mutant polypeptides R173W, R173Q, R225C, R225X, and 1073delA were
studied using a pulse-chase experiment. The construct with the mutation R225X did not
produce detectable polypeptide. The other mutated constructs were found to encode a
polypeptide with a stability comparable to the wild type polypeptide, since the signals of all
mutated polypeptides remained similar with the wild type polypeptide at all time points (Figure
5.3.). When polypeptides were chased for 23 hours, both mutant and wild type PBGD were
degraded based on a weaker signal in immunoprecipitation.

RESULTS AND DISCUSSION49
Figure 5.3. Pulse-chase experiment of wildtype and mutated PBGD
The half-life of the erythroid form of PBGD is approximately 24 hours if sufficient
porphobilinogen is present to form tetrapyrrole-bound intermediates which are less susceptible
to degrade than the free enzyme (Beaumont et al. 1986). When the amount of porphobilinogen
is inadequate, the polypeptide degrades more rapidly: half of the polypeptide is lost within 10
hours (Beaumont et al. 1986). The housekeeping isoform of PBGD appeared to be more stable
in the absence of substrate than the erythroid isoform, but the half-life of the housekeeping
isoform was not accurately determined (Beaumont et al. 1986). In COS-1 cells transfected with
PBGD cDNA, the enzyme is expressed without regulation and the amount of endogenous
porphobilinogen is probably not sufficient to bind to every molecule formed. In these
circumstances, thus, it is presumed that unbound PBGD is more prevalent than enzyme-
intermediate complex, leading to more instable polypeptide. This hypothesis supports the
results of our experiment, in which the PBGD were clearly degraded after a 23-hour chase.

RESULTS AND DISCUSSION 50
Figure 5.4. Immunofluorescence of mutated and wild type PBGD after expression.

RESULTS AND DISCUSSION 51
Based on the immunofluorescence staining, the transfection efficiency using lipofection method
was approximately 20% for each mutated cDNA studied (data not shown), and thus, it was
independent of the construct composition. The construct with the nonsense mutation R225X
was excluded from this experiment, since in the Western blot analysis or in the
immunoprecipitation assay no PBGD polypeptide could be detected. Figure 5.4. shows that in
the immunofluorescence staining the wild type polypeptide is diffusely dispersed in the
cytoplasm. The localization of the mutated polypeptides was indistinguishable from that of the
wild type. Thus, no abnormal accumulation or targeting of the mutated polypeptides was
observed. Moreover, the mutations representing different CRIM classes did not differ from
each other.
While this study is the first in which the properties of mutant PBGD were analyzed using in
vitro expression in eukaryotic cells, the effect of mutations in the PBGD gene on the enzyme
activity has been studied in three previous reports (Delfau et al. 1990, Chen et al. 1994, Ong et
al. 1997) These experiments were performed by expressing the mutated cDNAs of human
PBGD in E. coli. In these studies all mutations resulted in decreased enzyme activity and the
properties of mutant polypeptides were further analyzed by measuring the enzyme activity in
various pH environments (Delfau et al. 1990) or by determining the thermostability of the
polypeptides (Chen et al. 1994). Mutant PBGD appeared to have similar enzyme activities after
eukaryotic and prokaryotic expression, which was expected, since PBGD is a cytosolic enzyme
and is not further processed post-translationally.
Based on the studies of human PBGD mutants (Delfau et al. 1990, Chen et al. 1994, Ong et al.
1997), E. coli mutants (Jordan and Woodcock 1991, Lander et al. 1991), and the three-
dimensional model of the enzyme (Louie et al. 1992, Brownlie et al. 1994), mutations altering
the residues in the vicinity of the active site have always detrimental effect on the enzyme
activity. Amino acid substitutions located elsewhere in the polypeptide have variable
consequences. These mutations are thought either to destabilize the polypeptide or to alter the
protein structure in a way which prevents the substrate reaching the active site. In the present
study the mutant enzyme molecules were as stable as the normal polypeptide after pulse-chase
experiment. However, Chen et al. (1994) showed that mutations C247F and R201W lost half of

RESULTS AND DISCUSSION52
the enzyme activity in less than 30 minutes at 65oC while the T1/2 of normal PBGD was 120
minutes. Although this finding cannot be generalized to all the mutations in the PBGD gene, it
suggests that at least some amino acid substitutions actually both destabilize the polypeptide
and decrease enzymatic activity. Interestingly, four mutations located in domain 3 of the
polypeptide have been expressed and all of them had relatively high residual activity of 10-50%
(Chen et al. 1994, VI) after in vitro expression.
5.5. Outcome of mutations
The type and location of mutations resulting in AIP differ from each other considerably and
most of the mutations appear to have a detrimental effect on the normal function of the enzyme.
There is a wide range of mechanisms leading to an inactive enzyme and in this chapter the
potential mechanisms are discussed.
5.5.1. Mutations resulting in premature termination codon
In the case of ten mutations the predicted outcome would be the introduction of a premature
termination codon: IVS1+3G T (see chapter 5.5.3), 97delA, 100C T, insertion of 332 bp in
exon 5 (see chapter 5.5.4.), 417insCA, 445C T, 593G A, 673C T, IVS13-2G A (see
chapter 5.5.3.), and 886C T. The consequences of a premature termination codon on the
function of the enzyme are often dramatic. It is probable that the polypeptide encoded by the
mutant allele is enzymatically totally inactive, since many structures essential for the enzymatic
activity are not translated, and the stability of the polypeptide is probably also influenced by the
missing residues (Brownlie et al. 1994). In addition, the transcript level of the mutant allele is
often decreased (see chapter 5.2.). All nonsense mutations described here are found in CRIM
negative patients, which suggests that mutant polypeptide is not produced or the polypeptide is
unstable (Mustajoki and Desnick 1985).
The outcome of the nonsense mutation R225X (673C T) was studied in detail. The solid-
phase minisequencing method was used to determine the steady state transcript level of the
mutant allele, which was reduced to one fifth of that of normal allele (Table 5.2.). Furthermore,
the mutant transcript levels of the three clinically different patients with this mutation were

RESULTS AND DISCUSSION 53
similar. One of the patients has had acute attacks, her sister has experienced milder symptoms,
and their mother has always been asymptomatic. Thus, there was no correlation between the
phenotype and the mutant mRNA levels in patients' lymphoblasts. To study the consequences
of the mutation on protein level, the mutation was introduced in the human PBGD cDNA and
expressed in COS cells. The mutant enzyme was not detected by PBGD antibody (Figure 5.2.)
and it had no enzyme activity (Table 5.2.). In conclusion, the mutant transcript level is
remarkably decreased and even if mutant transcript was translated, the polypeptide would be
enzymatically inactive.
5.5.2. Missense mutations
Thirteen base changes were predicted to result in an amino acid substitution. The substituted
residues are highly conserved in different species (Grandchamp et al. 1984, Raich et al. 1986,
Thomas and Jordan 1986, Beaumont et al. 1989, Petricek et al. 1990, Keng et al. 1992, Mohr et
al. 1994, Abdelhak et al. 1997). Of the substituted residues all six arginines and lysine-98 are
invariant and thus completely conserved in the nine species studied (human, murine, rat, feline,
Saccharomyces cerevisiae, Escherichia coli, Pseudomonas aeruginosa, Bacillus subtilis, and
Euglena gracilis), and the remaining five residues are identical at least in mammalian species.
The invariance of the residues would suggest that they are crucial for the proper function of the
enzyme. The consequences of selected mutations were further characterized 1) by determining
the steady transcript level of the mutant allele and 2) in vitro expression of the mutagenized
cDNA construct and subsequent analyses of the polypeptide chains.
The three-dimensional model of PBGD polypeptide enables comparison of the mutant residues
with their corresponding normal residues in the E. coli crystal structure (Louie et al. 1992) and
provides information about the structural and functional consequences of the mutations in the
PBGD polypeptide (Brownlie et al. 1994). In addition, the mutagenesis studies of the E. coli
PBGD have provided valuable information about the function of the enzyme (Jordan and
Woodcock 1991, Lander et al. 1991, Woodcock and Jordan 1994). The consequences of the
missense mutations based on the information obtained from these studies are discussed below.

RESULTS AND DISCUSSION54
R26C (76C T). The arginine-26 is located in domain 1 of the PBGD (Figure 2.3.) in the
vicinity of the active cleft. The positively charged side chains of the residue are thought to
interact with the substrate (Lambert et al. 1994). In our expression studies the mutant C26
displayed no enzymatic activity (Table 5.2.). This result is consistent with the mutagenesis
studies in E. coli PBGD: substituting the corresponding residue (R11) results in complete
inactivation of the enzyme (Jordan and Woodcock 1991, Lander et al. 1991), because the
attachment of the first porphobilinogen ring of the substrate (E ES) is inhibited (Jordan and
Woodcock 1991). According to the pulse-chase experiment (Figure 5.2.) the mutant
polypeptide is as stable as the wild type enzyme, which is in agreement with the CRIM positive
status of the patients carrying this mutation.
R167W (499C T). Arginine167 (R149 in E. coli) interacts with the side chain of the cofactor.
Its modification to H149 in the E. coli enzyme leads to an accumulation of the ES intermediate
(enzyme with a single porphobilinogen attached) (Jordan and Woodcock 1991) and a similar
perturbation might also be expected for this mutation (Brownlie et al. 1994). In our expression
studies this mutation displayed a minimal residual activity of 5% (Table 5.2.). This mutation is
found in CRIM positive patients, which is consistent with the pulse-chase experiment, in which
the mutant enzyme was as stable as the wild type enzyme and folded normally, but lacking
function.
R173W (517C T) and R173Q (518G A). The side chain of arginine-173 interacts with the
cofactor and the residue also participates in substrate binding (Shoolingin-Jordan 1995). The
mutants W173 and Q173 were expressed in COS cells and the polypeptides synthesized had no
enzymatic activity even though both polypeptides were detected in the Western blot analysis by
the antibody and in pulse-chase experiments their stability was comparable to the wild type
PBGD (Table 5.2., Figures 5.2 and 5.3.). The mutagenesis studies in E. coli R155 (equivalent
to human R173) also led to severe impairment in substrate binding as well as the release of the
tetrapyrrole product (Jordan and Woodcock 1991, Lander et al. 1991). The mutant transcript
levels compared to the wild type allele in the case of mutations R173W and R173Q were 97%
and 66%, respectively (Table 5.2.).

RESULTS AND DISCUSSION 55
According to expression studies and determination of transcript levels, thus, the outcome of
mutations substituting R173 are quite similar. The Finnish patients carrying the mutation
R173W have previously been classified as CRIM negative or CRIM positive and patients with
the mutation R173Q as CRIM positive (Mustajoki and Desnick 1985). Our data suggests that
patients carrying the mutation R173W are weakly CRIM positive, i.e. inactive polypeptide is
present, but its amount is so low that it is hardly detectable by rocket immunoelectrophoresis.
This would give us satisfactory explanation for the different CRIM classes in different patients
with the same mutation.
R225G (673C G). Invariant arginine-225 is located on the outer surface of the enzyme (α4-
helix of the subunit 1) and its side chain forms hydrogen bonds to other side chains and also
hydrogen bond to main-chain carbonyl (Brownlie et al. 1994). Furthermore, substituting
arginine with glycine probably destabilizes the protein structure, since, unlike arginine, glycine
does not usually form α-helix structures (Branden and Tooze 1991). The transcript level of the
mutant allele was also determined and it was only slightly decreased (80% of the level of the
wild type allele). In in vitro expression the stability of the mutant polypeptide did not differ
from the wild type PBGD (Figure 5.3.) and, furthermore, the mutated enzyme displayed a
residual activity of 16% (Table 5.2.). Patients with this mutation are CRIM negative, i.e. there
is no inactive enzyme in patients' erythrocytes. The absence of inactive enzyme could be
explained by disruption of interactions and incomplete α-helix formation, which might
destabilize the polypeptide.
K98R (293A G).This highly invariant lysine interacts with dipyrromethane cofactor together
with the neighboring aspartate-99 and four arginines (R149, R150, R167, and R173).
Substitution of the corresponding lysine (K83) by various amino acids in E. coli resulted in an
enzyme that retains less than 1% of its activity (Woodcock and Jordan 1994) and presumably
the consequence of this mutation similar.
R116W (346C T). This substitution is the most common mutation causing AIP in the Dutch
population (Gu et al. 1993b). The arginine residue, located on a short strand linking domains 1
and 2, forms a salt bridge with glutamic acid in position 250 but is not involved in interactions

RESULTS AND DISCUSSION56
with the substrate or the cofactor. This mutation has been expressed in E. coli and the residual
PBGD activity was 3.4% (Ong et al. 1997). In addition, the mutagenesis study of the mutant
R101L in E. coli (equivalent to human position 116) displayed 37% residual activity and the
mutation had little effect on either the kinetic parameters of the enzyme or on the formation of
the substrate enzyme complexes (Lander et al. 1991). The patients with this mutation have
CRIM negative status, which is thought to have resulted from the loss of stabilizing interactions
to the glutamic acid residue in position 250 (Brownlie et al. 1994).
R195C (583C T). The patient carrying this mutation is the only affected individual in her
family. Neither parent was a carrier of the mutation and paternity was confirmed using DNA
fingerprint analysis, thus suggesting a de novo mutation. Substituting this arginine inhibits the
assembling of the third porphobilinogen unit to the growing chain (Lander et al. 1991).
C247F (740G T). The cysteine residue is buried in the hydrophobic core of the PBGD
polypeptide and its substitution is speculated to cause a steric disruption of the polypeptide
backbone (Brownlie et al. 1994).
V222M (664G A), L238R (713T G), L278P (833T G) and G280R (838G A). These
residues are conserved only in mammalian species and, furthermore, they do not appear to
interact with other amino acids in the polypeptide (Brownlie et al. 1994). Thus, the mechanism
of how these mutations cause inactivation of the enzyme is not thoroughly clarified. These
substitutions are, however, considered as causative agents for AIP, since 1) no other nucleotide
variation could be identified in the coding region of the PBGD gene by direct sequencing
and/or 2) the DNA analyses of the family members were in agreement with the pedigree
analysis and the results from biochemical analyses.
All mutations identified in CRIM positive patients were arginine substitutions. These arginine
residues form interactions with the substrate or the cofactor and are essential for enzymatic
activity. Minor changes in the polypeptide structure among CRIM positive patients were
expected, since CRIM positivity requires inactive but stable polypeptide which is detected by
a specific antibody. A truncated polypeptide, caused by a premature termination codon or larger

RESULTS AND DISCUSSION 57
disruption in the nucleotide sequence, would presumably be unstable. However, the possibility
exists that the antibody used in the immunological assays may not recognize it.
5.5.3. Splicing mutations
Four mutations interfere with the normal splicing pattern resulting in aberrant splicing. The
consensus sequence for RNA splicing is known (Table 5.3.) but mechanisms for a splicing
defect have not been thoroughly clarified. However, studies of different types of mutations at
the splice sites have provided useful information about aberrant splicing (Krawczak et al. 1992,
Nakai and Sakamoto 1994)
Table 5.3. Consensus sequences for RNA splicing.a
5'---CAGgu
aagt------a------
uuuuuuuuuuuuncag
G---3'
A g cccccccccccc u A
5' splice site (donor site) branch point A 3' splice site (acceptor site)a Adapted from (Alberts et al. 1994). Intronic sequence in lowercase and
exonic sequence in uppercase letters. n, any nucleotide
Three of the splicing mutations are located at the 5' donor splice site. In the case of the mutation
IVS1+3G T, the cryptic splice site is present 67 nucleotides away from the authentic splice
site. This finding is in agreement with the previous survey, in which most of the cryptic splice
sites activated by mutations are located relatively near, usually within 100 nucleotides, to the
authentic splice site (Nakai and Sakamoto 1994). The rest of the gene is transcribed normally,
but due to the uneven amount of nucleotides in the inserted fragment, a frame shift appears at
the beginning of exon 3 introducing a premature termination codon in exon 5. The length of the
predicted polypeptide is 73 amino acids and only the first exon would be translated normally.
Because the mutant polypeptide is dramatically truncated, it can be predicted to be
enzymatically inactive.
The mutation 33G T hits the last nucleotide of exon 1. The substitution does not modify the
amino acid and, although definitive proof is missing, it is thought to be responsible for
abnormal splicing (Grandchamp et al. 1989b, Kauppinen 1992b). Due to the tissue-specificity,

RESULTS AND DISCUSSION58
the erythrocyte PBGD activity in patients with mutations 33G T and IVS1+3G T is normal
and these mutations cause the variant form of AIP.
Exon skipping is the most frequent consequence of a splice mutation at either the 5' or 3' splice
site (Nakai and Sakamoto 1994), and it is also the predicted outcome of the mutation 86A T.
Interestingly, this base change would also result in the amino acid substitution Q29L if the
normal splicing was not affected. If no alternative sites with sufficient homology to the
consensus sequence exist in the vicinity, either exon skipping or greatly reduced production of
normal transcripts seem to be the predominant phenotypic consequences (Krawczak et al.
1992). In this case exon skipping is probably due to a lack of the potential cryptic splice site in
the vicinity of the 5' splice site of intron 3 and, as a result, 18 amino acids encoded by exon 3
are missing from the predicted PBGD polypeptide. The consequence of a missing exon 3 for
the function of the PBGD enzyme is most probably detrimental, since the exon codes for
residues (for example R26) which interact with the substrate (Jordan and Woodcock 1991,
Brownlie et al. 1994).
At the 3' splice site, the adenine at position -2 is highly conserved and this nucleotide is
significant for splicing events, since substitutions of this nucleotide are more frequent than
theoretical models predict (Krawczak et al. 1992). Intron retention, however, is the most
infrequent pattern of aberrant splicing (Nakai and Sakamoto 1994). According to the ’exon
definition hypothesis’, a model derived from experimental analyses (Niwa et al. 1992), intron
retention is permitted when the intron is small enough to satisfy the exon length limitation. In
the case of the mutation IVS13-2A G, the total length of exon 13, intron 13, and exon 14
includes only 204 nucleotides, which agrees well with this hypothesis. A premature termination
is introduced in intron 13 and the predicted polypeptide contains 275 normally translated amino
acids followed by 26 amino acids encoded by intron 13. In the PBGD polypeptide, exons 13
and 14 code for residues in the subunit β2 of the third domain (Brownlie et al. 1994). Similarly,
the nonsense mutation in exon 14 (W283X) deletes 78 residues from domain 3 and results in a
truncated polypeptide but yet retains ~10% of the normal expressed PBGD activity in E. coli
(Chen et al. 1994). The consequence of mutation IVS13-2A G on the enzyme properties may
be similar.

RESULTS AND DISCUSSION 59
5.5.4. Other mutations
Insertion of an Alu element. In SSCP analysis covering exons 5 to 7 a mobility shift was
identified in a sample of a patient belonging to a large AIP family (Figure 5.5.). The band
migrating more slowly than normal DNA strands was excised from the SSCP gel, diluted, and
reamplified. The PCR product was sequenced revealing a sequence homologous to an Alu
sequence. An extra fragment of 1019 bp in size could also be demonstrated in PCR covering
exons 5 to 7 from genomic DNA samples of five patients known to have low erythrocyte PBGD
activity, suggesting that an Alu insertion of ~350 bp in exon 5 of the PBGD gene was
responsible for AIP in this family. Simple amplification of exons 5 to 7 can easily be used in
the molecular diagnosis of this insertion (Figure 5.5.). It is of note that this additional fragment
could also be demonstrated by amplification of exon 5 alone but not in PCR reaction over
exons 3 to 5.
Figure 5.5. A) SSCP analysis showing an insertion which results in a mobility shift(arrow). B) PCR covering exons 5 to 7. Genomic DNA of the patients with Aluinsertation demonstrate both normal (687 bp) and inserted (1019 bp) alleles,whereas healthy controls demonstrate a normal allele. Leftmost lane, DNAmolecular weight maker VI (Boehringer Mannheim, Germany). N, healthy control,P, AIP patient.
A 333 bp Alu insertion in exon 5 was characterized after subcloning and sequencing the two
alleles of different size separately. The mutant allele included a 13 bp target site duplication and
3' terminal poly(A) tract in the antisense orientation. The sequence comparison of the inserted
Alu element with a database for repeated elements (Pythia, Jurka 1993) showed that it belongs
to the Ya5 subfamily. This subgroup is one of the youngest and currently most active Alu
subfamilies in evolution. There are no earlier reports of Alu insertions resulting in AIP and

RESULTS AND DISCUSSION60
none of the six Alu repeats located in the intronic areas of the PBGD gene belong to the same
subfamily (Yoo et al. 1993).
The predicted polypeptide contains 64 normally translated amino acids followed by 13 amino
acids not normally found in the PBGD polypeptide. A premature termination codon, which is
introduced at the beginning of the insertion, is located at the first codon after the 42 thymidines
which form the polyadenine tail of the Alu element. Amplification and sequencing of the
reverse transcribed total RNA extracted from a patient's lymphoblast cell line exposed only the
wild type allele.
The expression of the mutated and wild type PBGD constructs in COS-1 cells showed that the
insertion of the Alu element resulted in a total loss of the enzyme activity, which was expected
since nearly all structures crucial for the enzymatic function of the PBGD are missing
(Shoolingin-Jordan 1995). The TfiI restriction site located in exon 3 was removed from the
construct for the cloning purpose. This base change, however, did not alter the amino acid
sequence. The PBGD activity produced by this construct was close to normal, i.e. 88% of the
wild type activity. When the polyclonal rabbit anti-human-PBGD antibody was used to identify
the PBGD polypeptide in Western analysis, no mutant polypeptide could be detected. In
contrast, the wild type PBGD as well as the PBGD construct, in which the TfiI restriction site
was removed, produced a detectable polypeptide of normal size (42 kD).
Insertion of an Alu element into the coding sequence of a gene is an infrequent phenomenon:
only 17 coding sequences have been previous reported to be disrupted by an Alu repeat
(Makalowski et al. 1994). Furthermore, only eight of these Alu insertions have been associated
with a disease or a loss of biological activity. The disruption is most commonly caused by a
mutation splicing an intronic Alu sequence into the coding region of mRNA. Retroposition of
an Alu element into an exon occurs more rarely, and in that case, the Alu cassette is usually in
the sense orientation (Makalowski et al. 1994).
However, the PBGD Alu cassette is incorporated directly via retroposition into exon 5 in the
antisense orientation.

RESULTS AND DISCUSSION 61
1073delA. A deletion of one nucleotide is located 11 base pairs upstream of the termination.
The consequence of this deletion is a frame shift which removes the normally utilized
termination codon and does not create a new one before the polyadenylation signal. If the
translation stops at the polyadenylation signal, the length of the polypeptide would be 448
amino acids instead of the 361 of the wild type polypeptide. The first 357 amino acids of the
mutant polypeptide are predicted to be identical with the wild type enzyme and, thus, it
contains all the components known to be essential for the function of the PBGD.
When the transcript level of the mutant allele was determined, the results suggested that the
mutant allele is transcribed normally (Table 5.2.). However, the mutant mRNA appeared to get
degraded more rapidly than the transcript from the wild type allele during storage at -80oC. This
mutation was studied further by expressing the mutant PBGD-cDNA in COS cells. The mutant
clone displayed 50% residual activity (Table 5.2.). The non-coding region of the construct,
however, differed from the human PBGD gene. In the mutated construct the last 46 residues of
the synthesized polypeptide were encoded by the 3'-UTR region of the PBGD cDNA and the
vector sequence and a termination codon is introduced after 404 amino acids. This polypeptide
encoded by the construct is, thus, 44 amino acids shorter than the predicted mutant polypeptide
of the patient. The stability of the polypeptide encoded by the mutant construct was comparable
to the normal polypeptide in the pulse-chase experiment. However, this finding does not
exclude the possibility that mutant polypeptide would actually be more unstable in vivo.
5.6. Molecular genetics of AIP in the Finnish population
The population of Finland has been isolated during the past centuries and many diseases which
are rare in other countries are relatively common in Finland (de la Chapelle 1993).
Furthermore, there is an obvious founder effect in the case of many diseases; one mutation is
prevalent and is found in almost every affected individual. Studies from Sweden, the
Netherlands and Switzerland, suggest that a founder effect is present in these countries also in
the case of AIP (Lee and Anvret 1991, Gu et al. 1993b, Schneider-Yin et al. 1999). However,
the molecular defects are heterogeneous in the Finnish AIP patients, most of the identified
mutations are family specific (Table 5.1.). The R173Q mutation was the underlying reason for

RESULTS AND DISCUSSION62
AIP in four families. The pedigree of these families have been traced back for at least three
generations and no links could be identified between ancestors. However, three of the families,
originate from the same municipality (R173Q, number 14 in Figure 5.6.), implying that they
most probably are related to each other. In addition, the two families with mutation R149X are
originally from neighboring villages, which also suggests a common ancestor. Thus, there is a
minor founder effect among the Finnish AIP families. Also in France and in the United
Kingdom the molecular genetic background is highly heterogeneous and no founder effect has
been identified in these countries (Puy et al. 1997b, Whatley et al. 1999).

RESULTS AND DISCUSSION63
Figure 5.6. The origin of the Finnish AIP families. The numbers refer to mutations in Table 5.1.A and B: Origin of AIP families with yet unidentified genetic defect.

RESULTS AND DISCUSSION 64
The mutation 1073delA was found in a patient who belongs to the Skolt community. The Skolts
are Saamians who live in Northern Lappland. They have been very isolated for centuries and
form a homogenic population. Thus, it was possible, that the prevalence of AIP among Skolts
would be higher than in the rest of the Finnish population. To test this hypothesis, 94 DNA
samples from members of the Skolt community were screened for this mutation using the
minisequencing method (data not shown). As a result, the mutation could be identified in two
additional samples. These two individuals belonged to the same family as the index patient and,
furthermore, they were previously classified as AIP patients based on biochemical analyses. All
other samples were negative for this mutation and, thus, the conclusion was that prevalence of
AIP was not considerably higher in the Skolt community compared to the rest of the Finnish
population.
5.5. DNA diagnosis of AIP
The identification of underlying genetic defects now allows a reliable DNA-based diagnostics
of AIP in each family, which is in routine use when AIP status of asymptomatic family
members is determined. At least two separate analyses are carried out for each DNA sample.
Digestion with a restriction enzyme is used whenever possible, direct sequencing is performed
in both directions and minisequencing is also available in the case of some mutations.
The possibility of determining the genetic defect has also enabled the evaluation of the value of
biochemical methods in AIP diagnosis. Detailed screening for a mutation was tested in three
families representing different subtypes of AIP (Table 5.4.). The samples of a total of 81 family
members, among them 28 individuals with mutations were analyzed using both DNA and
biochemical methods. Biochemical methods (erythrocyte PBGD activity, urinary PBG and
ALA) failed to detect 25% (7/28) of patients. Furthermore, four out of 53 (8%) healthy family
members were falsely diagnosed as AIP carriers, but this may be due to the relatively low
PBGD activity from both parents' erythrocytes although the patients' father is apparently
healthy.

RESULTS AND DISCUSSION65
Table 5.4. Evaluation of biochemical methods in AIP diagnosis
Mutation a PBGDactivity b
Total number ofanalyzed family
members
No. ofmutationcarriers
False negativeresult in
biochemical tests
False positiveresult in
biochemical tests
33G T (-) N 30 10 2 0
499C T (+) V 28 12 3 4
673C T (-) V 23 6 2 0a CRIM status in parenthesisb PBGD activity in erythrocytes; N, normal activity; V, low activity
The feasibility of enzymatic screening in AIP diagnosis has also been evaluated in large
material of French AIP patients and their family members (Puy et al. 1997b). As a result,
determination of PBGD activity gave wrong diagnosis in 16% (45/280). However, if patients
with variant AIP were excluded from the analysis, the AIP gene-carrier status was correctly
stated in 240/252 (95%) cases. Thus, the biochemical methods have their limitations and DNA
analysis should be used whenever available in AIP diagnosis during the asymptomatic phase.

SUMMARY AND CONCLUSIONS 66
6. SUMMARY AND CONCLUSIONS
In the present work the molecular genetics of Finnish AIP patients was characterized. The
results of the studies and their conclusions can be summarized as follows:
• Twenty-two mutations were identified in the PBGD gene resulting in AIP. Together with
the previously identified genetic defects, the 26 characterized mutations cover 38 (95%)
of a total of 40 unrelated Finnish AIP families. Despite the heterogeneity at the molecular
level, the clinical manifestations of AIP are relatively uniform and no evidence emerged
for genotype-phenotype correlation.
• A specific diagnosing method based on DNA techniques was developed for each
mutation. The DNA diagnosis should always be used in screening of family members,
since biochemical methods fail to detect 10-20% of AIP patients.
• Mutations in the PBGD gene were screened using two different methods: DGGE and
SSCP. Both methods were useful and were able to detect most genetic defects, but the
sensitivity of DGGE was considerably higher.
• The steady state mRNA levels of six mutations were analyzed using solid-phase
minisequencing. The mutant mRNA levels in lymphocytes varied from 5 to 95% of the
corresponding wild type allele levels and all mutations, except the missense mutation
R173W in exon 10, affected the steady state transcript levels of the mutant allele. The
decreased mutant transcript level did not correlate either to CRIM class, to the location
of the disease causing mutation in the PBGD gene, or to the clinical phenotype of AIP.
• Using in vitro expression in COS-1 cells, eight mutations identified previously in Finnish
AIP patients were analyzed. All mutations resulted in a decrease in PBGD activity, and
six of the mutated enzymes displayed only minimal residual activity of 0-5%, confirming
the causality of the amino acid substitution and the low PBGD activity. The mutated
polypeptides were as stable as the normal PBGD, with the exception of truncated
polypeptide (mutation R225X) which could not be detected with the polyclonal antibody.
Furthermore, no abnormalities in the intracellular location of mutated polypeptides could
be observed by immuno-fluorescence.

ACKNOWLEDGEMENTS67
7. ACKNOWLEDGEMENTS
This study was carried out during years of 1993-1999 at the Department of Medicine, Divisionof Endocrinology, University of Helsinki and at the Department of Human Molecular Genetics,National Public Health Institute. Professor Marja-Riitta Taskinen, M.D., the Head of theDivision of Endocrinology is highly acknowledged for providing me excellent laboratoryfacilities and for continuous support in my efforts.
I express my greatest gratitude to my supervisors Raili Kauppinen and Leena Palotie-Peltonen.Raili has patiently taught me all the laboratory skills and the scientific way of thinking,although I was not always an especially quick learner. Her overwhelming enthusiasm towardsporphyrias and molecular genetics has been contagious. Leena amazes me time and time againwith her incredible memory and thorough knowledge of molecular genetics. Even though herschedule is very tight, she always found a time for me in her diary. After a meeting with Leenaall problems whatsoever seemed much smaller.
Professors Marja-Liisa Savontaus and Jean-Charles Deybach reviewed this thesis. They gaveconstructive criticism and noted important weaknesses in it. I appreciate their carefulexamination of this manuscript and most of all their positive attitude towards my work.
I am more than grateful to my uncle Pertti Mustajoki, M.D., who originally introduced me tothe world of porphyrias. Pertti's exceptionally wide perspective over the disorders of the hememetabolism is admirable. His supportive attitude towards my research has encouraged merepeatedly. Furthermore, our discussions have greatly influenced my way of working not onlyas a researcher but also as a practicing physician.
I would like to warmly thank all my collaborators Anu Wartiovaara (Suomalainen), M.D.,Minna Laine (Peltola), M.D., Maija Lahtela-Kakko, Ph.D., and the members of the DanishPorphyria Research Laboratory: Henrik Nissen, Ph.D., Niels Erik Petersen, Ph.D., TorbenHansen, Ph.D., and Mogens Hørder, Ph.D. Their excellent knowledge and skills haveconsiderably helped me during this study. Professor Bernard Grandchamp, M.D. isacknowledged for providing us with the PBGD cDNA and Dr. Ylva Floderus, PhD., providedus with PBGD antibody, which is also highly appreciated.
I warmly thank Ms. Hannele Pihlaja and Ms. Helena Ahola for their excellent technicalassistance and always positive and flexible attitude. The intensive moments of laboratory workwere made very pleasant when I could engage in interesting conversations concerning almosteverything in the whole wide world. Although I did not have any direct collaboration with Dr.Kaisa Timonen, M.D., I found her presence in the porphyria research group very pleasant.Professor Raimo Tenhunen, M.D. is acknowledged for providing the facilities for enzymeactivity measurements.
The colleagues and laboratory personnel in the Scientific Laboratory of the Helsinki UniversityCentral Hospital are warmly acknowledged for giving relaxing and hilarious company duringthe coffee-breaks, which too often were extended to coffee-hours. The atmosphere in thecoffee-room of the Scientific Laboratory was exceptional, and that repeatedly cheered me upafter an unsuccessful experiment. Especially I want to thank Ms. Sirkka-Liisa (Kikka)

ACKNOWLEDGEMENTS 68
Runeberg, whose sense of humor and exceptional ability to listen have made a deep and ever-lasting impact on me.
I want to express my warmest gratitude to my other uncle professor Arto Mustajoki, Ph.D. Theweekly squash matches, followed by the 'hair-drying', i.e. beer or two in the pub nearby, areunforgettable. Although the world did not become any better place to live despite our seriousefforts, our conversations offered me fresh perspectives to the scientific world, especially fromthe linguistic and administrative point of view.
I have spent many breathtaking moments with the running team of the Scientific laboratory.The gentle pressure of the other regular members of the team, Satu Vehkavaara, TatuMiettinen, Jaakko Kaukonen, Nina Lindbohm, and Heikki Relas, made me to take care of myphysical wellbeing. Besides, no one else but a young researcher can really understand thedifficulties of a young researcher, and our conversations during the weekly runs were often verytherapeutic. Furthermore, I am pleased that the Scientific Losers Club was finally founded,although the two founder members, Jaakko and I, do not actually meet the criteria for themembership any more.
I have a wonderful family. My parents Erkki Mustajoki and Päivi Lindstedt have given me allthe love and support I have ever needed. The importance of my two sisters, HenriikkaClarkeburn and Iida-Maaria Lindstedt, in my life cannot be exaggerated. The supportiveattitude of Risto Lindstedt, Jeffrey Clarkeburn and my parents-in-law, Anna-Liisa and OlliLaurila, is also highly appreciated.
Finally, I am more than grateful to my wife Ulla. She has been there during all the phases ofthis work. She has patiently tolerated me when all went wrong in the lab and with her I haveshared the moments of success. No words are sufficient to express my love to her.
This work was supported by grants from University of Helsinki, Academy of Finland, theResearch Funds and the Clinical Research Institute of the Helsinki University Central Hospital,Emil Aaltonen Foundation, the Paulo Foundation, the Instrumentarium Foundation, the Scienceand Research Foundation of Farmos Medical Company, the Aarne Koskelo Foundation, and theFinnish Medical Society Duodecim.
Helsinki, October 1999

REFERENCES69
8. REFERENCES
Abdelhak S, Kalatzis V, Heilig R, Compain S, Samson D, Vincent C, Levi-Acobas F, Cruaud C, Le Merrer M,Mathieu M, König R, Vigneron J, Weissenbach J, Petit C, Weil D. Clustering of mutations responsible for branchi-oto-renal (BOR) syndrome in the eyes absent homologous region (eyaHR) of EYA1. Hum Mol Genet 6:2247-2255,1997.
Alberts B, Bray D, Lewis J, Raff M, Roberts K, Watson JD. Molecular Biology of the Cell. Garland Publishing Inc.,New York, 1994.
Anderson PM, Reddy RM, Anderson KM, Desnick RJ. Characterization of the porphobilinogen deaminasedeficiency in acute intermittent porphyria. J Clin Invest 68:1-12, 1981.
Andersson C, Lithner F. Hypertension and renal disease in patients with acute intermittent porphyria. J Intern Med236:169-175, 1994.
Andersson C, Bjersing L, Lithner F. The epidemiology of hepatocellular carcinoma in patients with acute intermittentporphyria. J Int Med 240:195-201, 1996.
Andersson C. Acute intermittent porphyria in Northern Sweden. A population-based study. Academic dissertation.Departments of Family Medicine and Medicine, University of Umeå, Sweden. 1997.
Baserga SJ, Benz EJJ. Beta-globin nonsense mutation: deficient accumulation of mRNA occurs despite normalcytoplasmic stability. Proc Natl Acad Sci USA 90:482-486, 1992.
Beaumont C, Grandchamp B, Bogard M, de Verneuil H, Nordmann Y. Porphobilinogen deaminase is unstable in theabsence of its substrate. Biochim Biophys Acta 882:384-388, 1986.
Beaumont C, Porcher C, Picat C, Nordmann Y, Grandchamp B. The mouse porphobilinogen deaminase gene. J BiolChem 264:14829-14834, 1989.
Berk PD, Blaschke TF, Scharschmidt BF, Waggoner JG, Berlin NI. A new approach to quantitation of the varioussources of bilirubin in man. J Lab Clin Med 12:389-390, 1976.
Bissel L. Laboratory evaluation in porphyria. Semin Liv Dis 2:100-107, 1982.
Bonkovsky HL. Advances in understanding and treating 'The little imitator', acute porphyria. Gastroenterology105:590-594, 1993.
Branden C, Tooze J. Introduction to protein structure. Garland Publishing Inc., New York, 1991.
Brownlie PD, Lambert R, Louie GV, Jordan PM, Blundell TM, Warren MJ, Cooper JB, Wood SP. The three-dimensional structures of mutants of porphobilinogen deaminase: Toward an understanding of the structural basis ofacute intermittent porphyria. Prot Sci 3:1644-1650, 1994.
Carter MS, Li S, Wilkinson MF. A splicing-dependent regulatory mechanism that detects translation signal. EMBOJ 15:5965-5975, 1996.
de la Chapelle A. Disease gene mapping in isolated human populations: the example of Finland. J Hum Genet30:857-865, 1993.
Chen C-H, Astrin KH, Lee G, Anderson KE, Desnick RJ. Acute intermittent porphyria: identification and expressionof exonic mutations in the hydroxymethylbilane synthase gene. J Clin Invest 94:1927-1937, 1994.
Cheng J, Maquat LE. Nonsense codons can reduce the abundance of nuclear mRNA without affecting the abundanceof pre-mRNA or the half-life of cytoplasmic mRNA. Mol Cell Biol 10:5215-5225, 1993.

REFERENCES 70
Chirgwin JM, Przbyla AE, McDonald RJ, Rutter WJ. Isolation of biologically active ribonucleic acid from sourcesenriched in ribonuclease. Biochemistry 18:5294-5299, 1979.
Chretien S, Dubart A, Beaupain D, Raich N, Grandchamp B, Rosa J, Goossens M, Romeo PH. Alternativetranscription and splicing of the human porphobilinogen deaminase results either in tissue-specific or in house-keeping expression. Proc Natl Acad Sci USA 85:6-9, 1988.
Cooper DN. Human gene mutations affecting RNA processing and translation. Ann Med 25:11-17, 1993.
Daimon M, Morita Y, Yamatani K, Igarashi M, Fukase N, Ohnuma H, Sugiyama K, Ogawa A, Hideo M, Manaka H,Sasaki H. Two new polymorphisms in introns 2 and 3 of the human porphobilinogen deaminase gene. Hum Genet92:549-553, 1993a.
Daimon M, Yamatani K, Igarashi M, Fukase N, Morita Y, Ogawa A, Tominaga M, Sasaki H. Acute intermittentporphyria caused by a G to C mutation in exon 12 of the porphobilinogen deaminase gene that results in exonskipping. Hum Genet 92:549-553, 1993b.
Daimon M, Yamatani K, Igarashi M, Fukase N, Morita Y, Ogawa A, Tominaga M, Sasaki H. Acute intermittentporphyria caused by a single base insertion of C in exon 15 of the porphobilinogen deaminase gene that results in aframe shift and premature stopping of translation. Hum Genet 93:533-537, 1994.
Dean G. The porphyrias. A story of inheritance and environment. Pitman Medical Publishing Co., London, 1963.
Delfau M, Picat C, de Rooij F, Hamer K, Bogard M, Wilson J, Deybach J, Nordmann Y, Grandchamp B. Twodifferent point G to A mutations in exon 10 of the porphobilinogen deaminase gene are responsible for acuteintermittent porphyria. J Clin Invest 86:1511-1516, 1990.
Delfau M, Picat C, de Rooij F, Voortman G, Deybach J, Nordmann Y, Grandchamp B. Molecular heterogeneity ofacute intermittent porphyria: identification of four additional mutations resulting in the CRIM-negative subtype ofthe disease. Am J Hum Genet 49:421-428, 1991.
Desnick RJ, Ostasiewicz LT, Tishler PA, Mustajoki P. Acute intermittent porphyria: characterization of a novelmutation in the structural gene for porphobilinogen deaminase. J Clin Invest 76:865-874, 1985.
Deybach J-C, Puy H. Porphobilinogen deaminase gene structure and molecular defects. J Bioenerg Biomembr27:197-205, 1995.
Elder GH, Hift RJ, Meissner PN. The acute porphyrias. Lancet 349:1613-1617, 1997.
Felgner PL, Gadek TR, Holm M, Roman R, Chan HW, Wenz M, Northrop JP, Ringold GM, Danielsen M.Lipofection: a highly efficient, lipid mediated DNA-transfection procedure. Proc Natl Acad Sci USA 84:7413-7417,1987.
Ford RE, Ou C-N, Ellefson RD. Assay of erythrocyte uroporphyrinogen I synthase activity, with porphobilinogen assubstrate. Clin Chem 26:1182-1185, 1980.
Fujita H, Yamamoto M, Hayashi N, Sassa S. Erythroleukemia differentiation. Distinctive responses of the erythroid-specific and the nonspecific δ-aminolevulinate synthase mRNA. J Biol Chem 266:17494-17502, 1991.
Goldberg A. Acute intermittent porphyria: A study of 50 cases. Q J Med 28:183-209, 1959.
Goldberg A, Rimington C. Diseases of porphyrin metabolism. Charles C. Thomas Springfield, Illinois, 1962.
Grandchamp B, Romeo PH, Dubert A, Raich N, Rosa J, Nordmann Y, Goossens M. Molecular cloning of a cDNAsequence complementary to porphobilinogen deaminase mRNA from rat. Proc Natl Acad Sci USA 81:5036-5040,1984.

REFERENCES71
Grandchamp B, de Verneuil H, Beaumont C, Chretien S, Walter O, Nordmann Y. Tissue-specific expression ofporphobilinogen deaminase: two isoenzymes from a single gene. Eur J Biochem 162:105-110, 1987.
Grandchamp B, Picat C, de Rooij F, Beaumont C, Wilson P, Deybach J-C, Nordmann Y. A point mutation G-A inexon 12 of the porphobilinogen deaminase gene results in exon skipping and is responsible for acute intermittentporphyria. Nucleic Acids Res 17:6637-6649, 1989a.
Grandchamp B, Picat C, Kauppinen R, Mignotte V, Peltonen L, Mustajoki P, Romeo PH, Goossens M, NordmannY. Molecular analysis of acute intermittent porphyria in a Finnish family with normal erythrocyte porphobilinogendeaminase. Eur J Clin Invest 19:415-418, 1989b.
Grandchamp B, Picat C, Mignotte V, Wilson JHP, TeVelde K, Sandkuyl L, Romeo PH, Goossens M, Nordmann Y.Tissue-specific splicing mutation in acute intermittent porphyria. Proc Natl Acad Sci USA 86:661-664, 1989c.
Grandchamp B, Picat C, de Rooij F, Delfau MH, Gu XF, Deybach J-C, Wilson JPH, teVelde K, Nordmann Y.Porphobilinogen deaminase gene abnormalities in acute intermittent porphyria. International meeting on porphyrinmetabolism and iron metabolism, Papendal, the Netherlands, 1992.
Granick S. Induction of the synthesis of 5-ALA synthetase in liver parenchymal cells in culture by chemicalsinducing acute porphyria. J Biol Chem 238:2247-2250, 1963.
Granick S. The induction in vitro of the synthesis of delta-aminolevulinic acid synthetase in chemical porphyria: Aresponse to certain drugs, sex hormones and foreign chemicals. J Biol Chem 241:1359-1375, 1966.
Grompe M. The rapid detection of unknown mutations in nucleic acids. Nature Genet 5:111-117, 1993.
Gu XF, Lee JS, Delfau MH, Grandchamp B. PCR detection of a G/T polymorphism at exon 10 of theporphobilinogen deaminase gene (PBG-D). Nucleic Acids Res 19:1966, 1991.
Gu XF, de Rooij F, Voortman G, TeVelde K, Nordmann Y, Grandchamp B. High frequency of mutations in exon 10of the porphobilinogen deaminase gene in patients with a CRIM-positive subtype of acute intermittent porphyria. AmJ Hum Genet 51:660-665, 1992.
Gu XF, de Rooij F, de Baar E, Bruyland M, Lissens W, Nordmann Y, Grandchamp B. Two novel mutations of theporphobilinogen deaminase gene in acute intermittent porphyria. Hum Mol Genet 2:1735-1736, 1993a.
Gu XF, de Rooij F, Lee J-S, Te Velde K, Deybach JC, Nordmann Y, Grandchamp B. High prevalence of a pointmutation in the porphobilinogen deaminase gene in Dutch patients with acute intermittent porphyria. Hum Genet91:128-130, 1993b.
Gu XF, de Rooij F, Voortman G, TeVelde K, Deybach J-C, Nordmann Y, Grandchamp B. Detection of elevenmutations causing acute intermittent porphyria using denaturing gradient gel electrophoresis. Hum Genet 93:47-52,1994.
Higuchi R. Simple and rapid preparation of samples for PCR. In: Ehrlich HA, eds. PCR Technology. Principles andApplications for DNA Amplification. New York: Stockton Press. pp. 31-38, 1989.
Jagadeeswaran P, Forget BG, Weissman SM. Short interspersed repetitive DNA elements in eucaryotes: transposableDNA elements generated by reverse transcription of RNA pol III transcripts? Cell 26:141-142, 1981.
Jordan PM, Warren MJ. Evidence for a dipyrromethane cofactor at the catalytic site of E. coli porphobilinogendeaminase. FEBS Lett 225:87-92, 1987.
Jordan PM, Woodcock SC. Mutagenesis of arginine residues in the catalytic cleft of Escherichia coliporphobilinogen deaminase that affects dipyrromethane cofactor assembly and tetrapyrrole chain initiation andelongation. Biochem J 280:445-449, 1991.

REFERENCES 72
Jurka J. A new subfamily of recently retroposed human Alu repeats. Nucleic Acids Res 21:2252, 1993.
Kappas A, Sassa S, Galbraith RA, Nordmann Y. The porphyrias. In: Scriver CR, Beaudet A, Sly WS, Valle D, eds.The metabolic and molecular bases of inherited diseases. New York: McGraw-Hill. pp. 2116-2127, 1995.
Karttunen L, Lönnqvist L, Godfrey M, Peltonen L, Syvänen A-C. An accurate method for comparing transcript oftwo alleles or highly homologous genes: application to fibrillin transcripts in Marfan patients' fibroblasts. GenomeRes 6:392-403, 1996.
Kauppinen R. Prognosis of acute porphyrias and molecular genetics of acute intermittent porphyria in Finland.Academic dissertation. Department of Human Molecular Genetics, National Public Health Institute and ThirdDepartment of Medicine, University of Helsinki, Finland. 1992a.
Kauppinen R. Single-strand conformation polymorphism (SSCP) analysis applied to the diagnosis of acuteintermittent porphyria. Mol Cell Probes 6:527-530, 1992b.
Kauppinen R, Mustajoki P. Prognosis of acute intermittent porphyria: occurrence of acute attacks, precipitatingfactors and associated disease. Medicine 71:1-13, 1992.
Kauppinen R, Peltonen L, Pihlaja H, Mustajoki P. CRIM-positive mutations of acute intermittent porphyria inFinland. Hum Mutat 1:392-396, 1992.
Keng TC, Richard C, Larocque R. Structure and regulation of yeast HEM3, the gene for porphobilinogen deaminase.Mol Gen Genet 234:233-243, 1992.
Krawczak M, Reiss J, Cooper DN. The mutational spectrum of single base pair substitutions in mRNA splicejunctions of human genes: causes and consequences. Hum Genet 90:41-54, 1992.
Laemmli U. Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature 227:680-685, 1970.
Lambert R, Brownlie PD, Woodcock SC, Louie GV, Cooper JB, Warren MJ, Jordan PM, Blundell TL, Wood SP.Structural studies on porphobilinogen deaminase. In: Chadwick DJ, Ackrill K, eds. The Biosynthesis of thetetrapyrrole pigments. Ciba Foundation Symposium 180. Chichester: Wiley. pp. 97-110, 1994.
Lamon JM, Frykholm BC, Tschudy DP. Screening tests in acute porphyria. Arch Neurol 34:709-712, 1977.
Lander M, Pitt AR, Alefounder PR, Bardy D, Abell C, Battersby AR. Studies on the mechanism ofhydroxymethylbilane synthase concerning the role of arginine residues in substrate binding. Biochem J 275:447-452,1991.
Langenskiöld F. Om hematoporfyri med ileusliknande symtom. Finska Läk-Sällsk Handl 70:241, 1928.
Lannfelt L, Wetterberg L, Gellerfors P, Lilius L, Floderus Y, Thunell S. Mutations in acute intermittent porphyriadetected by ELISA measurement of porphobilinogen deaminase. J Clin Chem Clin Biochem 183:857-862, 1989a.
Lannfelt L, Wetterberg L, Lilius L, Thunell S, Gellefors P. ELISA for measuring porphobilinogen deaminase inhuman erythrocytes. Clin Chim Acta 183:227-238, 1989b.
Law WK, Choy KW, Lam CW. Novel single nucleotide polymorphism (9678G -> A) for linkage analysis of acuteintermittent porphyria. Clin Chem 45:308-309, 1999.
Lee GY, Astrin KH, Desnick RJ. Acute intermittent porphyria: A single-base deletion and a nonsense mutation in thehuman hydroxymethylbilane synthase gene, predicting truncations of the enzyme polypeptide. Am J Med Genet58:155-158, 1994.

REFERENCES73
Lee JS, Anvret M. A PstI polymorphism for the human porphobilinogen deaminase gene (PBG). Nucleic Acids Res15:6307, 1987.
Lee JS, Anvret M, Lindsten J, Lannfelt L, Gellerfors P, Wetterberg L, Floderus Y, Thunell S. DNA polymorphismswithin the porphobilinogen deaminase gene in two Swedish families with acute intermittent porphyria. Hum Genet79:379-381, 1988.
Lee J, Grandchamp B, Anvret M. A point mutation of the human porphobilinogen deaminase gene in a Swedishfamily with acute intermittent porphyria. Am J Hum Genet 47[Suppl]:A162, 1990.
Lee J. Molecular genetic investigation of the human porphobilinogen deaminase gene in acute intermittent porphyria.Academic dissertation. Karolinska Institute, Stockholm, Sweden. 1991a.
Lee JS. Alternative dideoxy sequencing of double-stranded DNA by cyclic reactions using Taq polymerase. DNACell Biol 10:67-73, 1991b.
Lee J, Anvret M. Identification of the most common mutation within the porphobilinogen deaminase gene in Swedishpatients with acute intermittent porphyria. Proc Natl Acad Sci USA 88:10912-10915, 1991.
Lindberg RLP, Porcher C, Grandchamp B, Ledermann B, Bürki K, Brandner S, Aguzzi A, Meyer UA.Porphobilinogen deaminase deficiency in mice causes a neuropathy resembling that of human hepatic porphyria.Nature Genet 12:195-199, 1996.
Lindberg RLP, Martini R, Bamgartner M, Erne B, Borg J, Zielasek J, Ricker K, Steck A, Toyka KV, Meyer UA.Motor neuropathy in porphobilinogen deaminase-deficient mice imitates neuropathy of human acute porphyria. JClin Invest 103:1127-1134, 1999.
Linet MS, Gridley G, Nyren O, Mellemkjaer L, Olsen JH, Keehm S, Adami HO, Fraumeni JF. Primary liver cancer,other malignancies, and mortality risks following porphyria: A cohort study in Denmark and Sweden. Am J Epidem149:1010-1015, 1999.
Litman DA, Correia MA. L-tryptophan: A common denominator of biochemical and neurological events of acutehepatic porphyria. Science 222:1031, 1983.
Llewellyn DH, Kalsheker NA, Elder GH, Harrison PR, Chretien S, Goossens M. A MspI polymorphism for thehuman porphobilinogen deaminase gene. Nucleic Acids Res 15:1349, 1987.
Llewellyn D, Whatley S, Elder G. Acute intermittent porphyria caused by an arginine to histidine substitution (R26H)in the cofactor-binding cleft of porphobilinogen deaminase. Hum Mol Genet 2:1315-1316, 1993.
Llewellyn DH, Scobie GA, Urquhart AJ, Whatley SD, Roberts AG, Harrison PR, Elder GH. Acute intermittentporphyria caused by defective splicing of porphobilinogen deaminase RNA: a synonymous codon mutation at -22 bpfrom the 5' splice site causes skipping of exon 3. J Med Genet 33:437-438, 1996.
Louie GV, Brownlie PD, Lambert R, Cooper JB, Blundell TL, Wood SP, Warren MJ, Woodcock SC, Jordan PM.Structure of porphobilinogen deaminase reveals a flexible multidomain polymerase with a single catalytic site. Nature359:33-39, 1992.
Lundin G, Wedell A, Thunell S, Anvret M. Two new mutations in the porphobilinogen deaminase gene and ascreening method using PCR amplification of specific alleles. Hum Genet 93:59-62, 1994.
Lundin G, Hashemi J, Floderus Y, Thunell S, Sagen E, Lægreid A, Wassif W, Peters T, Anvret M. Four mutationsin the porphobilinogen deaminase gene in patients with acute intermittent porphyria. J Med Genet 32:979-981, 1995.
Lundin G, Anvret M. Characterization and regulation of the nonerythroid porphobilinogen deaminase promoter.Biohem Biophys Res Comm 231:409-411, 1997.

REFERENCES 74
Lundin G, Lee JS, Thunell S, Anvret M. Genetic investigation of the porphobilinogen deaminase gene in Swedishacute intermittent porphyria families. Hum Genet 100:63-66, 1997.
Macek MJ, Mercier B, Macková A, Miller PW, Hamosh A, Férec C, Cutting GR. Sensitivity of the denaturinggradient gel electrophoresis technique in detection of known mutations and novel Asian mutations in the CFTR gene.Hum Mutat 9:136-147, 1997.
Magnussen CR, Levine JB, Doherty JM, Cheeseman JO, Tschudy DP. A red cell enzyme method for the diagnosisof acute intermittent porphyria. Blood 44:857-868, 1974.
Makalowski W, Mitchell GA, Labuda D. Alu sequences in the coding regions of mRNA: a source for proteinvariability. Trends Genet 10:188-193, 1994.
Maquat LE. When cells stop making sense: effects of nonsense codons on RNA metabolism in vertebrate cells. RNA1:453-465, 1995.
Mauzerall D, Granick S. The occurrence and determination of delta-aminolevulinic acid and porphobilinogen inurine. J Biol Chem 219:435-436, 1956.
May B, Dogra S, Sadlon T, Bhasker C, Cox T, Bottomley S. Molecular regulation of heme biosynthesis in highervertebrates. Prog Nucleic Acid Res Mol Biol 51:1-51, 1995.
Meyer UA, Strand LJ, Doss M, Rees C, Marver HS. Intermittent acute porphyria - demonstration of genetic defectin porphobilinogen metabolism. New Engl J Med 286:1277-1282, 1972.
Mgone C, Lanyon W, Moore M, Connor J. Detection of seven point mutations in the porphobilinogen deaminasegene in patients with acute intermittent porphyria, by direct sequencing of in vitro amplified cDNA. Hum Genet90:12-16, 1992.
Mgone C, Lanyon W, Moore M, Louie G, Connor J. Detection of high mutation frequency in exon 12 of theporphobilinogen deaminase gene in patients with acute intermittent porphyria. Hum Genet 92:619-622, 1993.
Mgone C, Lanyon W, Moore M, Louie G, Connor J. Identification of five novel mutations in the porphobilinogendeaminase gene. Hum Mol Genet 3:809-811, 1994.
Michaud J, Brody LC, Steel G, Fontaine G, Martin LS, Valle D, Mitchell G. Strand-separating conformationalpolymorphism analysis: efficacy of detection of point mutations in the human ornithine δ-aminotransferase gene.Genomics 13:389-394, 1992.
Mignotte V, Wall L, deBoer E, Grosveld F, Romeo P-H. Two tissue-specific factors bind the erythroid promoter ofhuman porphobilinogen deaminase gene. Nucl Acids Res 17:37-54, 1989.
Miyagi K. Deficiency of hepatic porphobilinogen deaminase in acute intermittent porphyria. J, Kyushu Haematol Soc20:190-203, 1970.
Mohr CD, Stonsteby SK, Deretic V. The Pseudomonas aeruginosa homologs of hemC and hemD are linked to thegene encoding the regulator of mucoidy AlgR. Mol Gen Genet 242:177-184, 1994.
Moore MR, McColl KEL, Rimington C, Goldberg A. Disorders of porphyrin metabolism. Plenum PublishingCorporation, New York, 1987.
Moyret C, Theillet C, Puig PL, Molés J-P, Thomas G, Hamelin R. Relative efficiency of denaturing gradient gelelectrophoresis and single strand conformation polymorphism in the detection of mutations exons 5 to 8 of the p53gene. Oncogene 9:1739-1743, 1994.
Mullis KB, Faloona F. Specific synthesis of DNA in vitro via a polymerase-catalyzed chain reaction. MethodsEnzymol 155:335-350, 1987.

REFERENCES75
Mustafa S, Pabinger I, Mannhalter C. Protein S deficiency type I: identification of point mutations in 9 of 10families. Blood 86:3444-3451, 1995.
Mustajoki P, Koskelo P. Hereditary hepatic porphyrias in Finland. Acta Med Scand 200:171-178, 1976.
Mustajoki P. Normal erythrocyte uroporphyrinogen I synthase in a kindred with acute intermittent porphyria. AnnIntern Med 95:162-166, 1981.
Mustajoki P, Desnick RJ. Genetic heterogeneity in acute intermittent porphyria: characterization and frequency ofporphobilinogen deaminase in Finland. Brit Med J 291:505-509, 1985.
Mustajoki P, Kauppinen R, Lannfelt L, Koistinen J. Frequency of low porphobilinogen deaminase activity inFinland. J Intern Med 231:3889-3395, 1992.
Myers RM, Maniatis T, Lerman LS. Denaturation and localization of single base changes by denaturing gradient gelelectrophoresis. Methods Enzymol 155:501-527, 1987.
Nakai K, Sakamoto H. Construction of a novel database containing aberrant splicing mutations of mammalian genes.Gene 141:171-177, 1994.
Namba H, Narahara K, Tsuji K, Yokoyama Y, Seino Y. Assignment of human porphobilinogen deaminase to11q24.1 - q24.2 by in situ hybridization and gene dosage studies. Cytogenet Cell Genet 57:105-108, 1991.
Nishimura K, Taketani S, Inokuchi H. Cloning of a human cDNA for protoporphyrinogen oxidase bycomplementation in vivo of a hemG mutant of Escherichia coli. J Biol Chem 270:8076-8080, 1995.
Nissen H, Hansen AB, Guldberg P, Petersen NE, Larsen ML, Haghfelt T, Kristiansen K, Hørder M. Cellular andmolecular cardiology: Genetic diagnosis with the denaturing gel electrophoresis technique improves diagnosticprecision in familial hypercholesterolemia. Circulation 91:1641-1646, 1995.
Niwa M, MacDonald CC, Berget SM. Are vertebrate exons scanned during splice-site selection? Nature 360:277-280, 1992.
Nordmann Y, Puy H, da Silva V, Simonin S, Robreau AM, Bonaiti C, Phung LN, Deybach JC. Acute intermittentporphyria: prevalence of mutations in the porphobilinogen deaminase gene in blood donors in France. J Int Med242:213-217, 1997.
Ong PM, Lanyon WG, Hift RJ, Halkett J, Moore MR, Mgone CS, Connor JM. Detection of four mutations in sixunrelated patients with acute intermittent porphyria. Mol Cell Probe 10:57-61, 1996.
Ong PML, Lanyon WG, Graham G, Hift RJ, Halkett J, Moore MR, Connor JM. Acute intermittent porphyria: the invitro expression of mutant hydroxymethylbilane synthase. Mol Cell Probe 11:293-296, 1997.
Ong PM, Lanyon WG, Hift RJ, Halkett J, Cramp CE, Moore MR, Connor JM. Identification of two novel mutationsin the hydroxymethylbilane synthase gene in three patients from two unrelated families with acute intermittentporphyria. Hum Hered 48:24-29, 1998.
Orita M, Suzuki Y, Sekiya T, Hayashi K. Rapid and sensitive detection of point mutations and DNA polymorphismsusing the polymerase chain reaction. Genomics 5:874-879, 1989.
Peltz SW, He F, Welch E, Jacobson A. Nonsense-mediated decay in yeast. In: eds. Progress in Nucleic AcidsResearch and Molecular Biology. New York: Academic Press. pp. 271-298, 1994.
Petersen NE, Nissen H, Hansen TS, Rasmussen K, Brock A, Hørder M. R235X mutation in exon 15 of theporphobilinogen deaminase gene identified in two Danish families with acute intermittent porphyria. Clin Chem42:106-107, 1996.

REFERENCES 76
Petersen NE, Nissen H, Hørder M, Senz J, Jamani A, Schreiber WE. Mutation screening by denaturing gradient gelelectrophoresis in North American patients with acute intermittent porphyria. Clin Chem 44:1766-1768, 1998.
Petricek M, Rutberg L, Schroder I, Hederstedt L. Cloning and characterization of the hemA region of the Bacillussubtilis chromosome. J Bacteriol 172:2250-2258, 1990.
Picat C, Bourgeois F, Grandchamp B. PCR detection of a C/T polymorphism in exon 1 of the porphobilinogendeaminase gene (PBGD). Nucleic Acids Res 19:5099, 1991.
Ploos van Amstel JK, Bergman AJIW, van Beurden EACM, Roijers JFM, Peelen T, van der Berg IET, Poll-The BT,Kvittingen EA, Berger R. Hereditary tyrosinemia type 1: novel missense, nonsense and splice consensus mutationsin the human fumarylacetoacetate hydrolase gene variability of the genotype-phenotype relationship. Hum Genet97:51-59, 1996.
Proia R, D'Azzo A, Neufeld EF. Association of alfa- and beta-subunits during biosynthesis of beta-hexosaminidasein cultured fibroblasts. J Biol Chem 259:3350-3354, 1984.
Puy H, Deybach J-C, Robreau AM, Lamoril L, Nordmann Y. Detection of four novel mutations in theporphobilinogen deaminase gene in French Caucasian patients with acute intermittent porphyria. Hum Hered 46:177-180, 1996.
Puy H, Aquaron R, Lamoril J, Robreau AM, Nordmann Y, Deybach JC. Acute intermittent porphyria: rapidmolecular diagnosis. Cell Mol Biol 43:37-45, 1997a.
Puy H, Deybach J-C, Lamoril J, Robreau AM, Da Silva V, Gouya L, Grandchamp B, Nordmann Y. Molecularepidemiology and diagnosis of PBG deaminase gene defects in acute intermittent porphyria. Am J Hum Genet60:1373-1383, 1997b.
Puy H, Gross U, Deybach JC, Robreau AM, Frank M, Nordmann Y, Doss M. Exon 1 donor splice site mutations inthe porphobilinogen deaminase gene in the non-erythroid variant form of acute intermittent porphyria. Hum Genet103:570-575, 1998.
Raich N, Romeo PH, Dubart A, Beaupain D, Cohen-Solal M, Goossens M. Molecular cloning and complete primarysequence of human erythrocyte PBG deaminase. Nucleic Acids Res 14:5955-5968, 1986.
Rogers J. The origin and evolution of retroposons. Int Rev Cytol 93:187-279, 1985.
Rosipal R, Puy H, Lamoril J, Martasek P, Nordmann Y, Deybach JC. Molecular analysis of porphobilinogen (PBG)deaminase gene mutations in acute intermittent porphyria: first study in patients of Slavic origin. Scand J Clin LabInv 57:217-224, 1997.
Sambrook J, Fritsch EF, Maniatis T. Molecular cloning: A laboratory manual. In: eds. Cold Spring Harbor, NewYork: Cold Spring Harbor Laboratory Press. pp. 9.16-19.19, 1989.
Sanger F, Nicklen S, Coulson AR. DNA sequencing with chain-termination inhibitors. Proc Natl Acad Sci USA74:5463-5467, 1977.
Sassa S, Kappas A. Genetic, metabolic, and biochemical aspects of the porphyrias. In: Harris H, Hirschhorn K, eds.Advances in Human Genetics. New York: Plenum. pp. 121-231, 1981.
Schneider-Yin X, Bogard C, Rüfenacht UB, Puy H, Nordmann Y, Minder EI, Deybach J-C. Identification of aprevalent nonsense mutation (W283X) and two novel mutations in the porphobilinogen deaminase gene of Swisspatients with acute intermittent porphyria. Hum Hered in press, 1999.
Schreiber WE, Jamani A, Ritchie B. Detection of a T/C polymorphism in the porphobilinogen deaminase gene bypolymerase chain reaction amplification of specific alleles. Clin Chem 38:2153-2155, 1992.

REFERENCES77
Schreiber W, Fong F, Jamani A. Frameshift mutations in exons 9 and 10 of the porphobilinogen deaminase geneproduce a cross reacting immunological material (CRIM)-negative form of acute intermittent porphyria. Hum Genet93:552-556, 1994a.
Schreiber WE, Fong F, Jamani A. Molecular diagnosis of acute intermittent porphyria by analysis of DNA extractedfrom hair roots. Clin Chem 40:1744-1748, 1994b.
Schreiber WE, Rozon C, Fong F, Jamani A. Detection of polymorphisms and mutations in the porphobilinogendeaminase gene by nonisotopic SSCP. Clin Chem 40:1982-1983, 1994c.
Schreiber WE, Fong F, Nassar BA, Jamani A. Heteroduplex analysis detects frameshift and point mutations inpatients with acute intermittent porphyria. Hum Genet 96:161-166, 1995a.
Schreiber WE, Jamani A, Armstrong JG. Acute intermittent porphyria in a native North American family.Biochemical and molecular analysis. Am J Clin Pathol 103:730-734, 1995b.
Scobie G, Llewellyn D, Urquhart A, Smyth S, Kalsheker N, Harrison P, Elder G. Acute intermittent porphyria causedby a C-T mutation that produces a stop codon in the porphobilinogen deaminase gene. Hum Genet 85:631-634, 1990.
Sheffield VC, Cox DR, Lerman LS, Myers RM. Attachment of a 40 base G + C rich sequence (GC-clamp) togenomic DNA fragments by the polymerase chain reaction results in improved detection of single base changes. ProcNatl Acad Sci USA 86:232-236, 1989.
Shoolingin-Jordan PM. Porphobilinogen deaminase and uroporphyrinogen III synthase: structure, molecular biology,and mechanism. J Bioenerg Biomembr 27:181-195, 1995.
Simpson SB, Stolzfus CM. Frameshift mutations in the v-src gene of avian sarcoma virus act in cis to specificallyreduce v-src mRNA levels. Mol Cell Biol 14:1835-1844, 1994.
Stacey A, Schnieke A. SVpoly: a versatile mammalian expression vector. Nucleic Acids Res 18:2829, 1990.
Stein JA, Tschudy DP. Acute intermittent porphyria: A clinical and biochemical study of 46 patients. Medicine 49:1-16, 1970.
Syvänen A-C, Sajantila A, Lukka M. Identification of individuals by analysis of biallelic DNA markers using PCRand solid-phase minisequencing. Am J Hum Genet 52:46-59, 1993.
Thomas SD, Jordan PM. Nucleotide sequence of the hemC locus encoding porphobilinogen deaminase ofEscherichia coli K12. Nucleic Acid Res 14:6215-6226, 1986.
Toback AC, Sassa S, Poh-Fitzpatrick MB, Schechter J, Zaider E, Harber LC, Kappas A. Hepatoerythropoieticporphyria: Clinical, biochemical and enzymatic studies in a three-generation family lineage. N Engl J Med 316:645-650, 1987.
Tschudy DP, Valsamis M, Magnussen CR. Acute intermittent porphyria: Clinical and selected research aspects. AnnIntern Med 83:851, 1975.
Urlaub G, Mitchell PJ, Ciudad CJ, Chasin LA. Nonsense mutations in the dihydrofolate reductase gene affect RNAprocessing. Mol Cell Biol 9:2868-2880, 1989.
de Verneuil H, Aitken G, Nordmann Y. Familial and sporadic porphyria cutanea: Two different diseases. Hum Genet44:145-151, 1978.
Waldenström J. Studien über porphyrie. Acta Med Scand Suppl 82:1-254, 1937.
Waldenström J. The porphyrias as inborn errors of metabolism. Am J Med 22:758-773, 1957.

REFERENCES 78
Warren MJ, Jordan PM. Investigation into the nature of substrate binding to the dipyrromethane cofactor ofEscherichia coli porphobilinogen deaminase. Biochemistry 27:9020-9030, 1988.
Watson CJ, Schwartz S. Simple test for urinary porphobilinogen. Proc Soc Exp Biol Med 47:393-394, 1941.
Watson CJ, Pierach CA, Bossenmaier I, Cardinal R. Use of haematin in the acute attack of the "inducible" hepaticporphyrias. Adv Intern Med 23:265-285, 1978.
Wetterberg L. Akut intermittent porfyri. Läkartidningen 71:2461-2465, 1974.
Whatley SD, Woolf JR, Elder GH. Comparison of complementary and genomic DNA sequencing for the detectionof mutations in the HMBS gene in British patients with acute intermittent porphyria: identification of twenty fivenovel mutations. Hum Genet 104:505-510, 1999.
Woodcock SC, Jordan PM. Evidence for participation of aspartate-84 as a catalytic group at the active site ofporphobilinogen deaminase obtained by site-directed mutagenesis of the hemC gene from Escherichia coli.Biochemistry 33:2688-2695, 1994.
Yoo HW, Warner CA, Chen CH, Desnick RJ. Hydroxymethylbilane synthase: complete genomic sequence andamplifiable polymorphisms in the human gene. Genomics 15:21-29, 1993.