Embed Size (px)
Citation preview
Modulatory role for B (and T) cells in ischemic reperfusion injury
Hamid Rabb MD Physician Director, Kidney Transplant Program
The Johns Hopkins Hospital

Acknowledgements
• Lorraine Racusen• Wink Baldwin• Robert Colvin• Dolores Ascon• Shannon Bevans• Roshni Molls• Manchang Liu
• Mark Haas• Melissa Burne-Taney • Naoko Yokota• Vladimir Savransky• Carmelo Mendiola• Gilbert Postler• Niamh Kieran

Outline
• Importance of ischemia reperfusion injury (IRI) in transplantation
• Cellular inflammation during IRI
• Role of T lymphocytes in kidney IRI
• Role of B lymphocytes in kidney IRI
• Role of B lymphocytes in intestinal IRI

High incidence of kidney ischemia reperfusion injury
Delayed graft function occurs in 30% of deceased donor (cadaver) kidney transplants (50% at Hopkins-ECD population), which predisposes to acute rejection and chronic allograft nephropathy (NEJM 1995)
All deceased donors have some degree of significant IRI
No specific therapy

ischemic injury
anti-donor Ab
(preexisting)
complement
platelets
toxins
NK cells
T cells
macrophages
pathogenic models
Endothelium + other cells
ischemia hypoxia
accommodation
acute humoral rejection
antigen
antibody
B cells T cells
Ischemia/hypoxia is a major pathophysiologic process during antibody mediated rejection
NIH antibody rejection workshop AJT 2004
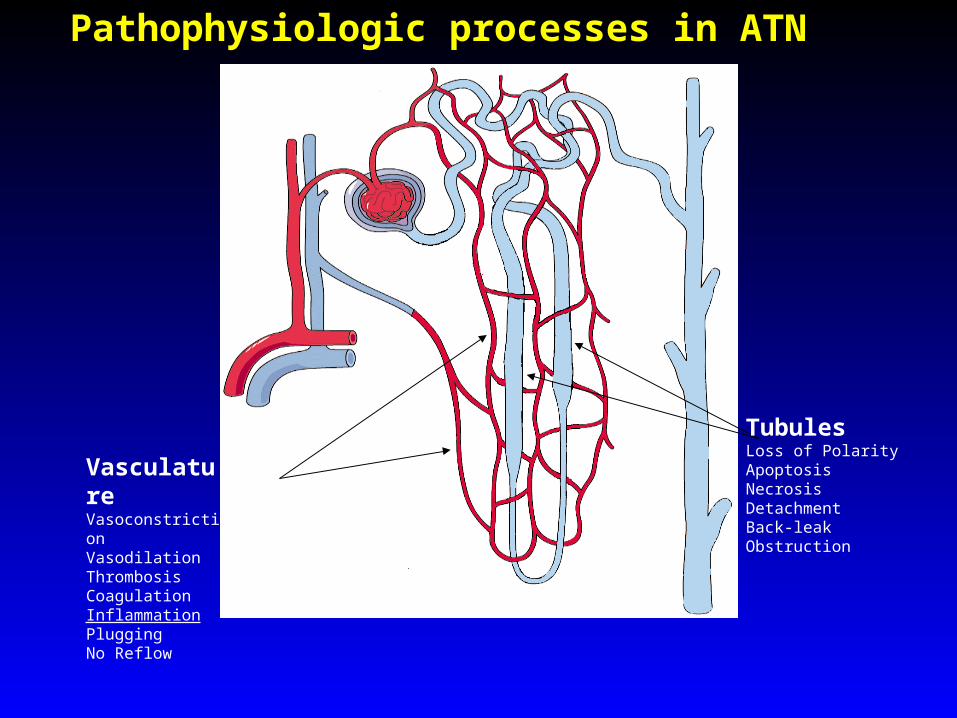
VasculatureVasoconstrictionVasodilationThrombosisCoagulationInflammationPluggingNo Reflow
TubulesLoss of PolarityApoptosisNecrosisDetachmentBack-leakObstruction
Pathophysiologic processes in ATN
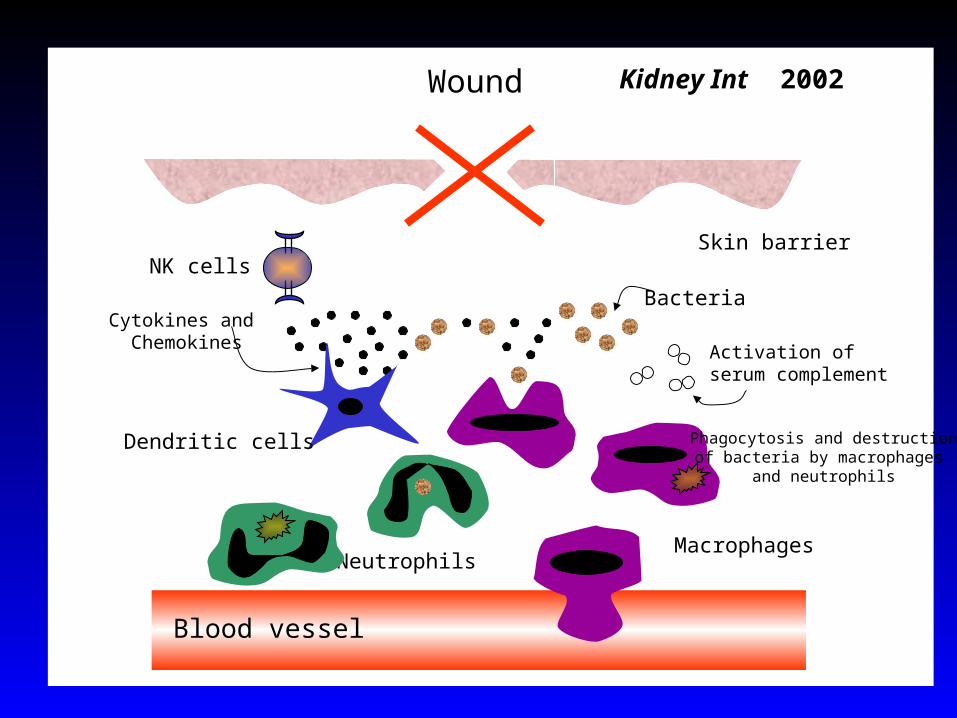
Wound
Bacteria
MacrophagesNeutrophils
Blood vessel
Skin barrierNK cells
Activation ofserum complement
Cytokines and Chemokines
Phagocytosis and destructionof bacteria by macrophages
and neutrophils
Dendritic cells
Kidney Int 2002

Leukocyte adhesion in renal IRI
CD11/CD18 - ICAM-1PNAS 94, Am J Physiol 94, BBRC 95, JCI 96, KI 97...
SelectinJASN 94, Am J Physiol 96, JCI 97, FASEB 2000,
KI 2001 (selectin ligand), J Immunol 2002(selectin ligand fucose groups)
Assumption: working solely via neutrophils

Role of CD11/CD18 and neutropenia on ischemic ARF.
Mendiola & Rabb, J Am Soc Nephrol 4:741 1993
Neutropenia induced to >98% depletion
No benefit on course of ARF with 60 min unilateral ischemia
CD11/CD18-ICAM-1 pathway blockade protective in same experiment
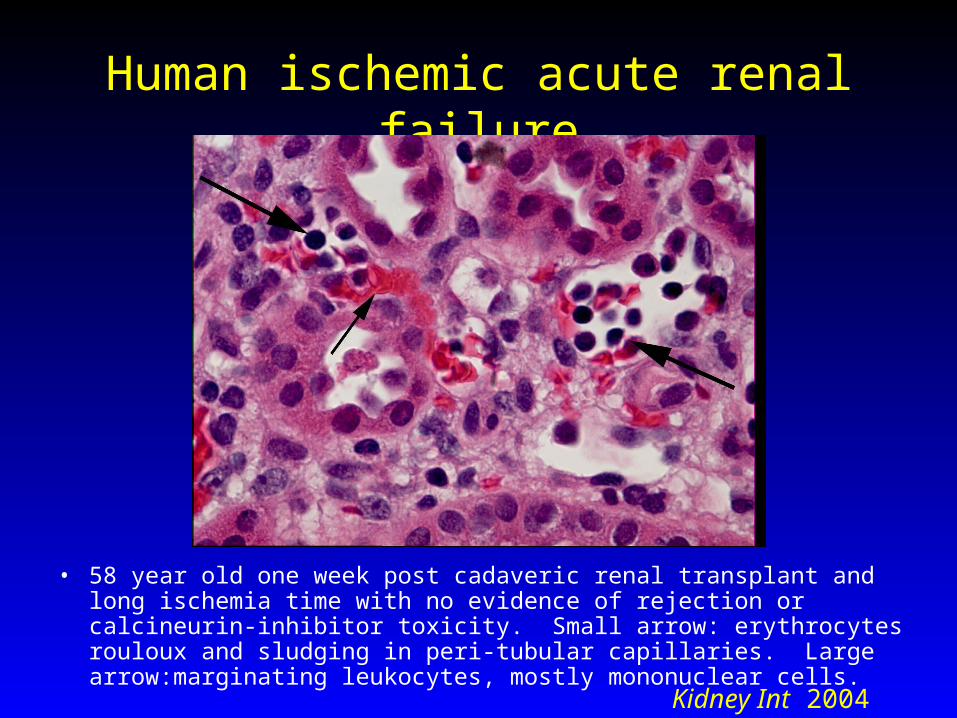
Human ischemic acute renal failure
• 58 year old one week post cadaveric renal transplant and long ischemia time with no evidence of rejection or calcineurin-inhibitor toxicity. Small arrow: erythrocytes rouloux and sludging in peri-tubular capillaries. Large arrow:marginating leukocytes, mostly mononuclear cells.
Kidney Int 2004
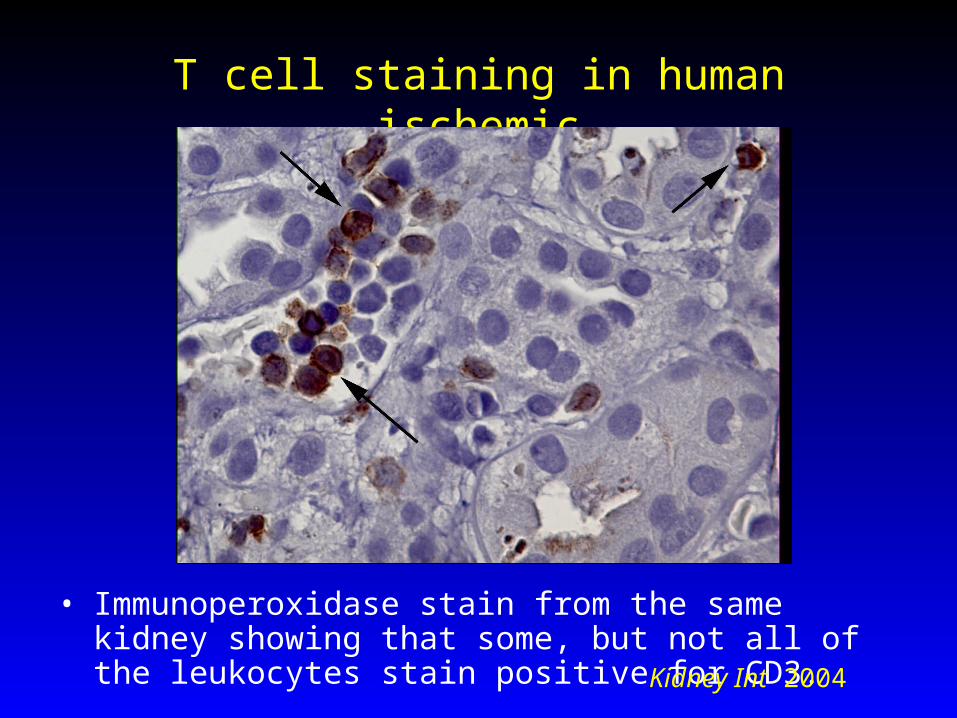
T cell staining in human ischemicacute renal failure
• Immunoperoxidase stain from the same kidney showing that some, but not all of the leukocytes stain positive for CD3.
Kidney Int 2004
Is there data to support the hypothesis that lymphocytes play an important role
in renal IRI?
Sparse lymphocytes are found in the postischemic kidney (Solez)
CTLA-4 Ig (against T cell costimulation) decreases cold ischemic injury (Takada J Clin Invest 1997, Chandraker Kidney Int 1997, B7-1 pathway important in rat model of ARF (DeGreef, Ysebart, De Broe Kidney Int 2001)
Lymphocyte related cytokines are upregulated in the postischemic kidney (Goes/Halloran et al: Transplantation 1995, Lemay et al: Transplantation 2000)
T lymphocytes mediate murine liver IRI (Zwacka et al: J Clin Invest 1997)

CD4 VLA-4CD3
T CELLRECEPTOR
HLAVCAM-1
ICAM-1
T Lymphocyte
Antigen Presenting CellSelectinLigand
SelectinLFA-1
Peptide
ICAM-1 and CD11/CD18 (LFA-1) also mediate T cell adhesion and function
Hours Postischemia
0 24 48
Se
rum
Cre
ati
nin
e (
mg
/dL
)
0
1
2
3
*
control C57 CD4/CD8 (-/-)
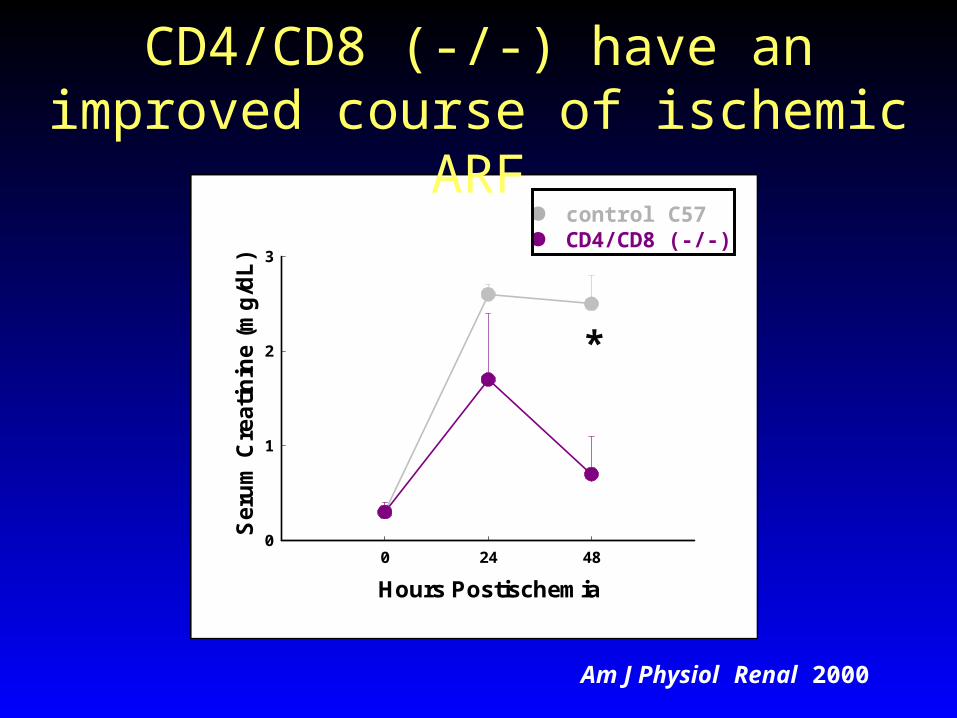
CD4/CD8 (-/-) have an improved course of ischemic ARF
Am J Physiol Renal 2000
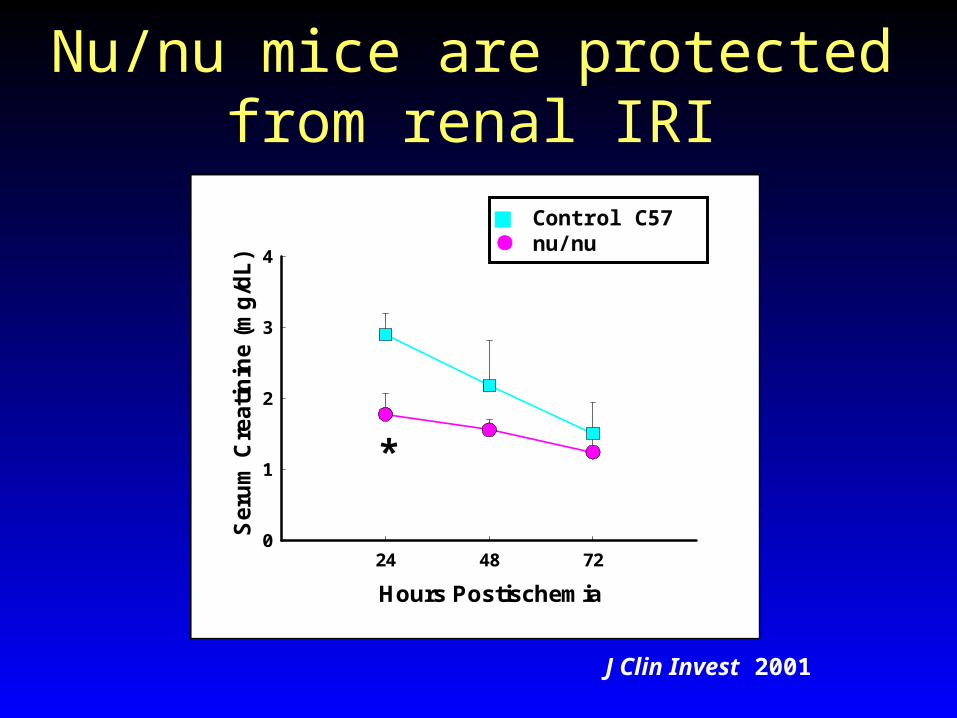
Nu/nu mice are protected from renal IRI
Hours Postischemia
24 48 72
Se
rum
Cre
ati
nin
e (
mg
/dL
)
0
1
2
3
4
*
Control C57 nu/nu
J Clin Invest 2001
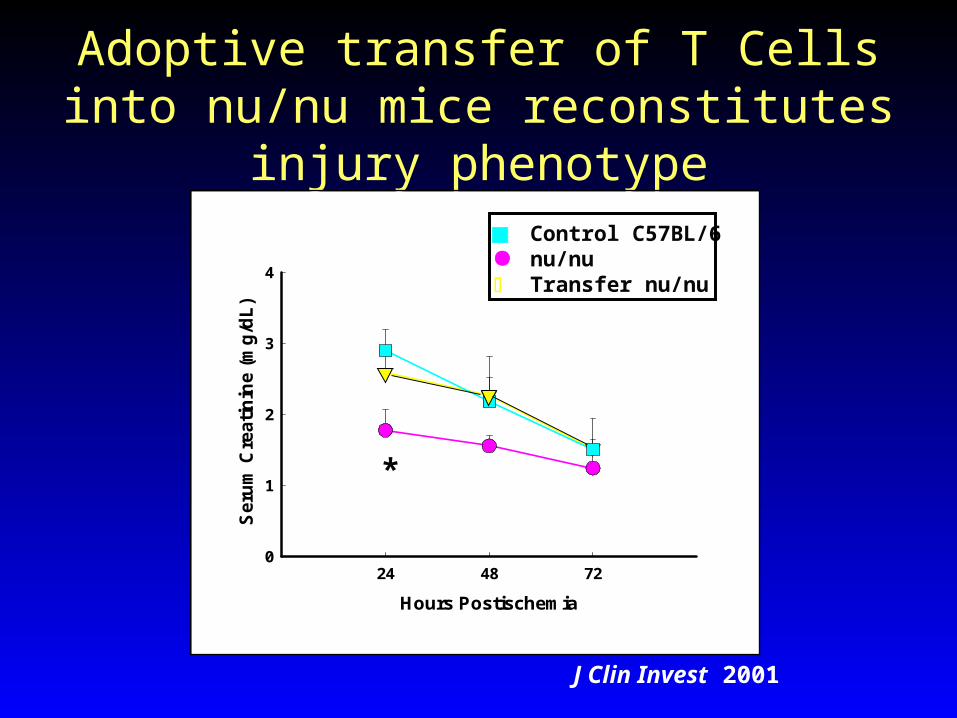
Adoptive transfer of T Cells into nu/nu mice reconstitutes injury phenotype
Hours Postischemia
24 48 72
Seru
m C
reati
nin
e (
mg
/dL
)
0
1
2
3
4
*
Control C57BL/6 nu/nu Transfer nu/nu
J Clin Invest 2001

Nu/nu mice have reduced tubular necrosis following renal IRI
A B
C D
J Clin Invest 2001
0
1
2
3
0 24 48 72
Hours postischemia
Ser
um
cre
ati
nin
e [m
g/d
L]
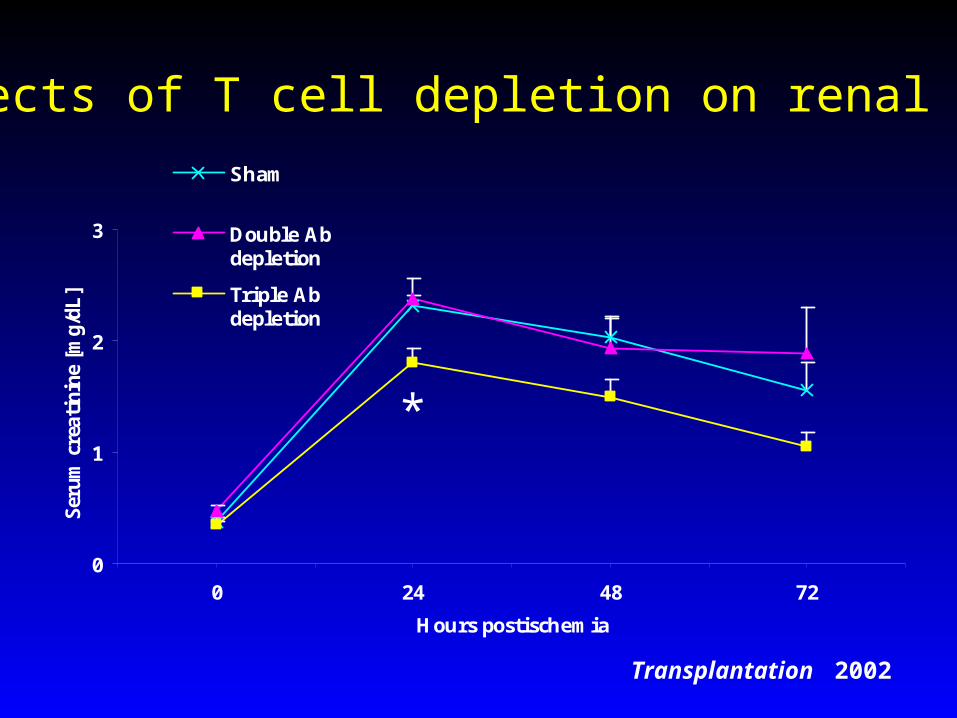
Sham
Double Abdepletion
Triple Abdepletion
*
Effects of T cell depletion on renal IRI
Transplantation 2002
0
20
40
60
80
100
120
140
-5 0 5 10 15 20 25 30min
Mea
n ar
teria
l blo
od p
ress
ure
(mm
Hg)
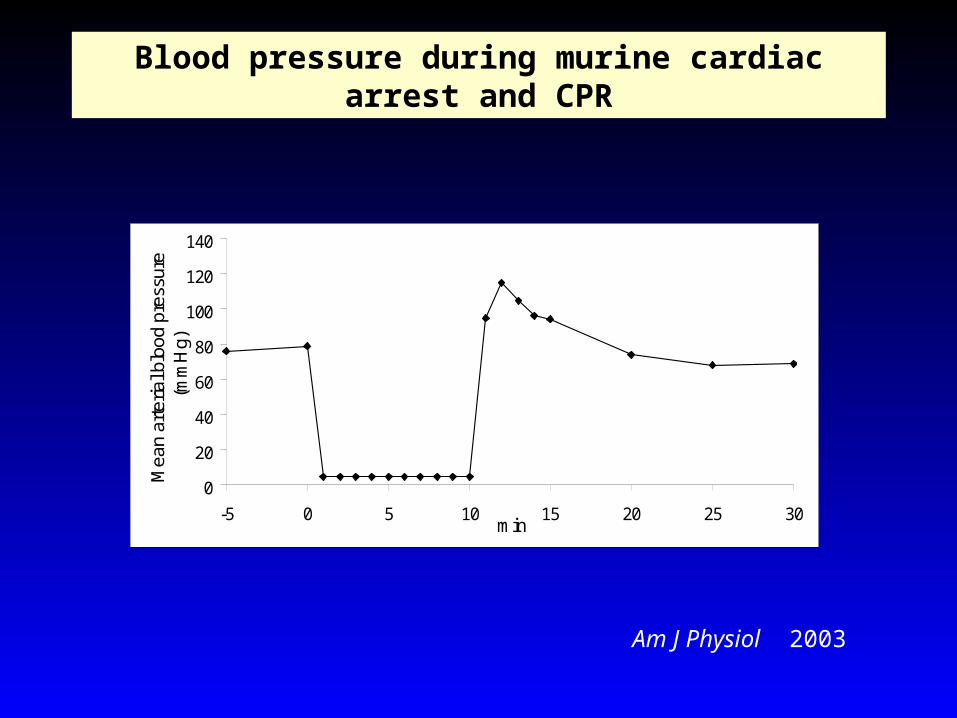
Blood pressure during murine cardiac arrest and CPR
Am J Physiol 2003

Hours Postischemia
0 24 48
Se
rum
Cre
atin
ine
(m
g/d
L)
0
1
2
3
4
**
T cell deficient mice have significant protection from acute renal failure after cardiac arrest and CPR
wild type CPR T cell deficient CPR wild type sham arrest T cell deficient sham arrest
Am J Physiol 2003
Evidence for T cell modulation of IRI in lung and liver
• Am J Transp 2002 FTY 720 liver
• Hepatology 2003 Stat 4 & Stat 6 liver
• Am J Path 2003 Fibronectin-VLA-4 liver
• Mol Ther 2004 CD40Ig liver
• J Immunol 2003 rat lung tx model

Hours Postischemia
0 24 48 720
1
2
3
4 C57BL/6 wild typeMu (B cell deficient)
Se
rum
Cre
atin
ine
(m
g/d
L)
B cell deficient mice are protected from renal injury following IRI
J Immunol 2003

Normal wild-type Wild-type B cell-deficient
J Immunol 2003

Hours after ischemia
0 72
Un
ite
s M
PO
/g p
rote
in
0
50
100
150
200
250
300
350
400Wild-type MT
Phagocyte Infiltration
J Immunol 2003
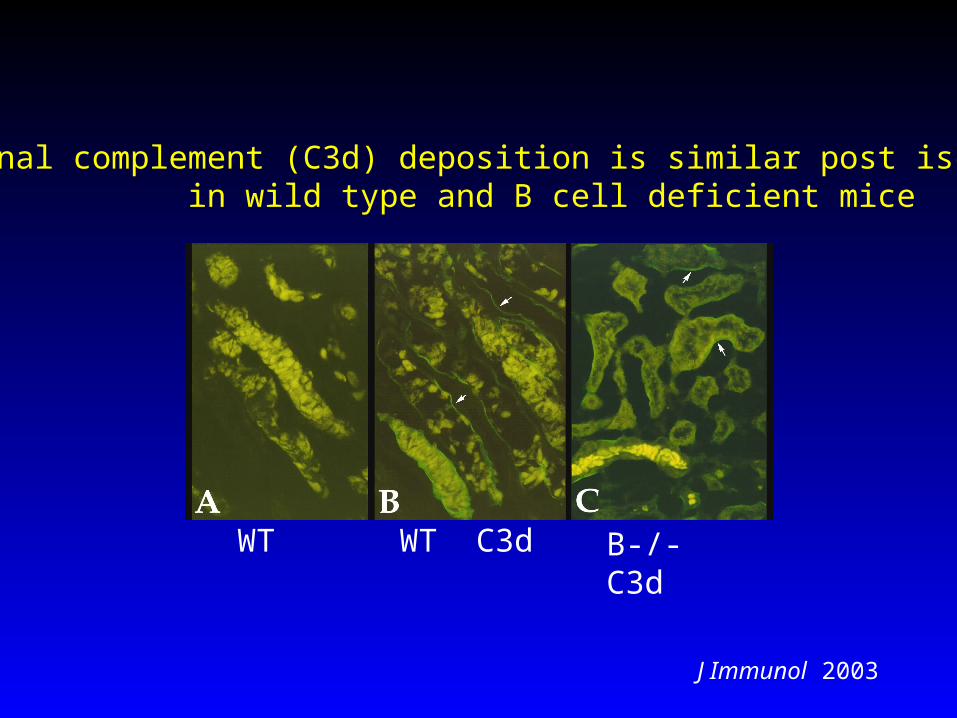
Renal complement (C3d) deposition is similar post ischemia in wild type and B cell deficient mice
WT WT C3d B-/- C3d
J Immunol 2003

Hours Postischemia
0 24 48 72
Ser
um C
reat
inin
e (m
g/dL
)
0.0
0.4
0.8
1.2
1.6
2.0
2.4
MTB cell transferWild-typeSerum transfer
#
* **
Serum transfer, but not B cell transfer, partially restores injury response in B cell deficiency
J Immunol 2003

Hours Postischemia
0 24 48 72
Se
rum
Cre
atin
ine
(m
g/d
L)
0.5
1.0
1.5
2.0
2.5
3.0
* **
Hours Postischemia
0 24 48 72
Se
rum
Cre
atin
ine
(m
g/d
L)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
* *
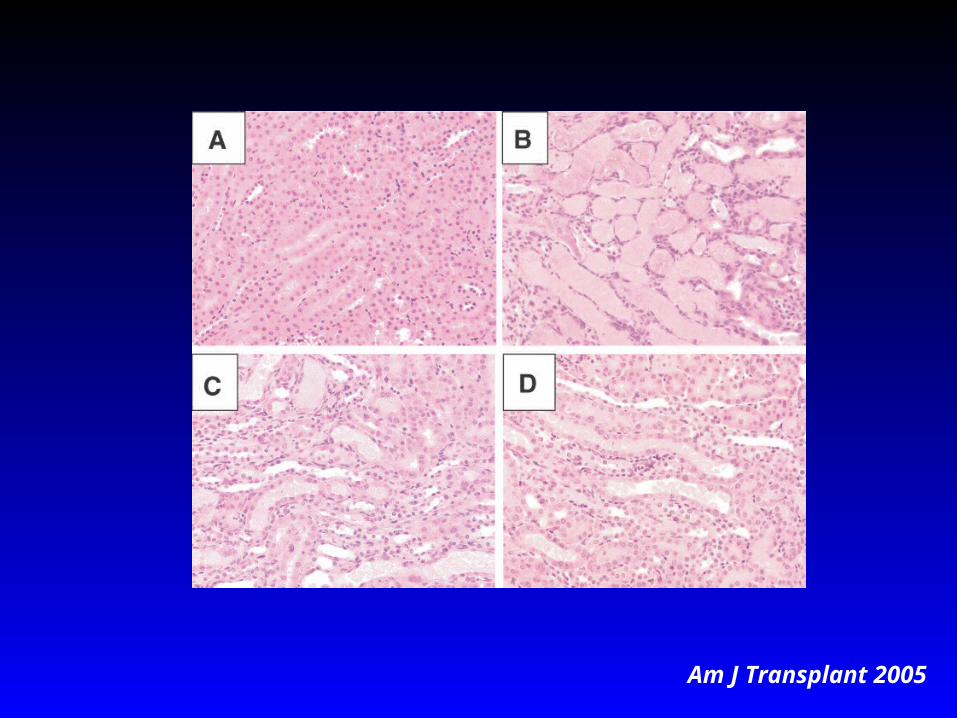
RAG-1 (T and B cell deficient) mice are not protected postischemia in both C57BL/6 and BALB/c background
strains
RAG-1 deficient mice Wild type mice T cell deficient (nude mice)
Am J Transplant 2005
Am J Transplant 2005

Am J Transplant 2005

Hours Postischemia
0 24 48 72
Seru
m C
reatin
ine (
mg/d
L)
0
1
2
3
4
*
**
B or T cell transferred RAG-1 deficient mice were protected from renal IRI compared to RAG-1 deficient mice that did not receive a
transfer of cells
RAG-1 deficient B cell transferred RAG-1 deficient T cell transferred RAG-1 deficient
wt mice Am J Transplant 2005

-+- RAG-1 + B cell
--+ RAG-1 + T cells
--- RAG-1 knockout
+-+ B cell deficient
++- T cell deficient
-++ Wild type
ProtectionB cellT cell Mouse strains
Am J Transplant 2005

Proc Natl Acad Sc 2004
Specific IgM mediates intestinal IRI in mice
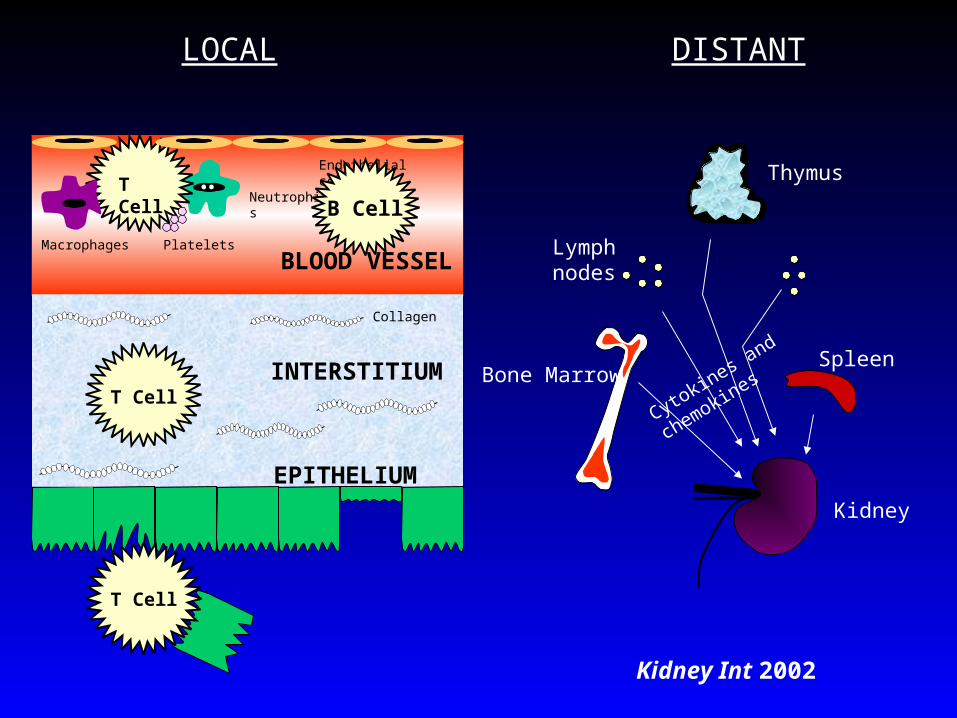
LOCAL DISTANT
Thymus
Lymphnodes
SpleenBone Marrow
Kidney
BLOOD VESSELMacrophages
Neutrophils
Endothelial cells
INTERSTITIUM
EPITHELIUM
Platelets
Collagen
T Cell
T Cell
T Cell
Cytokines and chemokines
Kidney Int 2002
B Cell

Summary
• IRI is a major cause of delayed graft function, increases graft immunogenicity, and decreases long term function
• Ischemic injury is a final mediator of antibody mediated rejection
• T cells are a newly identified mediator of IRI
• B cells are a newly identified mediator of IRI
• T and B cells may interact for full expression of IRI
• Role of T and B cells in IRI has similarities and differences between kidney and intestine
• B and T cells are a novel therapeutic target for IRI
• The mechanisms underlying the role for lymphocytes in IRI is largely unknown.





























