Embed Size (px)
Citation preview

_Journal of Epidemiology and Community Health 1990; 44: 307-312
Models for forecasting hospital bed requirementsin the acute sector
R D T Farmer, J Emami
AbstractStudy objective-The aim was to evaluate
the current approach to forecasting hospitalbed requirements.Design-The study was a time series and
regression analysis. The time series formean duration ofstay for general surgery inthe age group 15-44 years (1969-1982) wasused in the evaluation of different methodsof forecasting future values of meanduration of stay and its subsequent use inthe formation ofhospital bed requirements.Results-It has been suggested that the
simple trend fitting approach suffers frommodel specification error and imposesunjustified restrictions on the data. Timeseries approach (Box-Jenkins method) wasshown to be a more appropriate way ofmodelling the data.Conclusion-The simple trend fitting
approach is inferior to the time seriesapproach in modelling hospital bedrequirements.
Department ofCommunity Medicine,Charing Cross andWestminster MedicalSchool, 17 HorseferryRoad, London SWIP2ARR D T FarmerJ Emami
Correspondence to:Mr Emami
Accepted for publicationApril 1990
Over the past 25 years there have been substantialchanges in medical practice which have alteredgross demand for hospital facilities, the type offacilities required, and the ways they are used. Allthese changes have financial implications both interms of revenue requirements and capitalinvestment. During the same period there hasbeen a move to ensure that health care facilities aremore evenly distributed within the country as a
whole. Planning problems are compounded bythe fact that many hospitals are old and reachingthe end of their useful life. Thus planning ofhospital services is an important issue, yet themodels available to forecast facilities andmanpower are generally inadequate. There is a
need to develop a method whereby the optimumlevel ofprovision can be established and the likelyeffects of changes proposed can be assessed. Aplanning model should enable managers tomaximise the use of projected capital andinvestment and minimise cost.This paper is concerned with one aspect of the
development of such models, namely, obtainingshort term forecasts of future work loads in theacute hospital sector. It does not evaluate currentmethods for forecasting populations.The plan of this paper is as follows: the first
section considers the relationship used to forecasthospital bed needs and the data used for thispurpose; the second section introduces themethodology of forecasting used throughout thepaper; the third section is devoted to a criticalanalysis of the current method of forecasting
hospital bed requirements and illustrates the timeseries approach by applying it to a specific timeseries of Mean Duration of Stay (MDS); thefourth section considers the joint estimation oftheingredients of the relationship used for bedforecasting, Mean Duration of Stay, andAdmission Rate (AR) as part of multiequationmodel; the conclusion is presented in the finalsection.
DataHospital bed requirements are usually forecastwith the aid of the following relationship:
Beds= (Pop*AR*MDS*E)/365 (1)
where: Beds = forecast number of available beds;AR= projected admission rate (the forecastdischarge rate is usually used as a proxy);MDS =projected average duration of hospitalstay; Pop = projected population to be served; andE = projected efficiency factor. This may be thepercentage daily occupancy or the so calledturnover interval.The daily available beds are defined as those
beds available for the treatment of patients. Thebed complement is a higher number that takesaccount of the fact that additional beds will berequired because, for example, there will be aneed to refurbish and update hospital facilitiesand slack to allow for emergencies or disasters.Such changes will result in some of the bedsbeing unavailable most of the time. Sometimesan adjustment for the difference betweenthe required available beds and the requiredbed complement is incorporated in the basicmodel.The simple identity (equation 1) is usually
applied to different age, sex, and specialty groups.This is essential as the process determining theingredients of the identity changes between thesegroups. However, if disaggregation of the data istaken too far then the potential gain is lost due tolack of data.The efficiency factors used in forecasts are
essentially (but not necessarily) arbitrary. SinceMDS and AR are critical to the whole model it isessential to understand how they are derived.
MEAN DURATION OF STAYThe mean duration ofstay can be calculated in oneof two ways. It can either be generated from datacollected on discharge of patients from hospital(Hospital Activity Analysis data), referred to aspatient orientated data, or estimated fromstatistics on hospital bed utilisation (SH3 data)-bed orientated data.
on March 31, 2020 by guest. P
rotected by copyright.http://jech.bm
j.com/
J Epidem
iol Com
munity H
ealth: first published as 10.1136/jech.44.4.307 on 1 Decem
ber 1990. Dow
nloaded from

R D T Farmer, J Emami
Average lengths of stay are calculated frompatient orientated data as follows. A form iscompleted in respect of all patients admitted toand discharged from acute (and most other)hospitals administered by the NHS. Theadmission and discharge forms include personalidentification data to allow them to be linked.From these forms it is possible to establish thenumber of days spent in hospital by individualpatients during each episode of admission. Themean duration of stay is the sum of days spent inhospital by patients discharged during thatperiod. That is:
MDS = E(LOS)/P
Where: LOS = total number of days spent inhospital by each individual patient; and P =thetotal number of patients.The distribution of patients by exact length of
stay over time within most specialties and age andsex groups is unimodal and skewed to the right. Inmost age/sex/specialty groups the mode is aroundtwo to three days (figs 1 and 2). Thus changes overtime in the arithmetical mean length of stay tendto be caused by changes in the thickness of the tailrather than the location of the mode. It may bededuced that the mean is likely to be a relativelypoor indicator of the change. In view of thelimitations imposed by the distribution of lengthsof stay it is unlikely that the identity (equation 1)can be used with any degree of accuracy forforecasting the numbers of beds that may beacquired in some future year. However, despitethis reservation, it is possible to improve on thecurrent methods used in forecasting meanduration of stay.Bed orientated data are different and less
revealing of the underlying process. Here the
20
15
*C 10
Figure I Distribution ofpatients by length of stayand age (15-44 years):general surgery
toen.
Figure 2 Distribution ofpatients by length of stayand age (15-44 years, logpercentages): generalsurgery
Days of stay
Days of stay
mean duration of stay is estimated by dividing theproduct of the average number of beds occupieddaily during a period and the number of days inthat period by the number of discharges (anddeaths) that occurred. This method uses SH3 typedata. It tells us nothing about the distribution ofpatients by length of stay. A further majorproblem is that data on bed occupancy by age andsex of patients and precise specialty in which theywere treated are not normally available from thissource. There are important differences in theway certain manoeuvres within the hospital arehandled by the two information systems. InHospital Activity Analysis data, transfer of apatient from one doctor's care to another's isusually recorded as a discharge and immediatereadmission; the same is not true of SH3 data.
ADMISSION RATEThe hospital admission rate is not normallypresented in routine reports. Data are presentedas discharges (and deaths), and discharge (anddeath) rates. These are used as proxies foradmissions and admission rates. The potential forerror by using these proxies in the "acute"specialties is small. Few patients stay in hospitalfor over a year; and year to year changes inadmissions are not great. Rates are calculated bydividing the number of admissions by thecatchment population of the hospital, district,region, or the country as a whole. There is no realdenominator problem with national data. Withsubnational population groupings, the definitionof the denominator can present difficulties as thepopulation "at risk" to be admitted is hard todefine. There are frequent overlapping catchmentareas; the effective catchment population for onespecialty/age/sex group may differ from that foranother and confusion may arise regarding the useof the actual population or the theoretical (ordesirable) population base.
COMMENTS ON DATA USED IN THE PRESENT METHOD
At present national data are used to forecast theparameters (mean duration of stay and admissionrate) which are then applied at regional or districtlevels. The implicit assumption here is that, in anygiven year, the gross national provision ofhospitalbeds is optimal, although no assumption is maderegarding the distribution of this nationally"optimal" provision within the country. Thus theforecasts produced for a particular district (orregion) give an indication of what resources willbe required at some future time, assuming thefactors that determine the national optimumprovision will continue to be effective during theperiod of the forecast.
Moreover, it is assumed that the optimumadmission rate and mean duration of stay areuniform throughout the country. Underlying thisis an assumption that net morbidity is identicaland that the treatment requirements (in terms oflength of stay and numbers of admissions) do notvary from place to place. But there is muchevidence that patterns of morbidity vary betweenthe NE and SE of England45 and within regionsand that patients from different social andoccupational backgrounds vary in both thenumber of days they require in hospital for anepisode of illness and the numbers of admissions
308 on M
arch 31, 2020 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.44.4.307 on 1 D
ecember 1990. D
ownloaded from

Models for hospital bed requirements
that may be required per episode.6 The problemsof weighting forecasts, or even current provision,for variations in social circumstances andmorbidity7 have been addressed by manyinvestigators but to date no satisfactory methodhas been devised.
Forecasting methodologyIt is instructive to have a general overview of thetwo methods of forecasting referred to in thispaper, before discussing them in the context offorecasting of mean duration of stay andadmission rates, and their use in determination ofnumber of beds. The two methods are: (1)forecasting from a structural model; and (2) thetime series or Box-Jenkins' method.
FORECASTING FROM A STRUCTURAL MODELSuppose we are in year n, and we require theforecast of a quantity y, for year n + 1. The firststep in this method is to construct a model byrelating y to one or more variables x, for whichfuture values are more readily available. Let usdenote the relationship by a functionf. So that themodel can be written as:
Yt =f(xt) + st (2)
In this equation, E is an unobservable disturbanceterm, indicating that we do not expect data tosatisfy f exactly, and the subscript t refers to thevalue of the variables and disturbances at time t.Note that x, can be a vector of variables and caninclude past values ofy (ie, lags denoted by Yt - k,with k > = 1), as well as a trend t. The next step inthis procedure is to specify the relationship f interms of x, and some estimable parameters. Manymathematical functions can be used, for examplefcan be specified as a polynomial in x or as anexponential function of x. Finally using ourinformation (data) on x,y up to present time n, weestimate parameters determining f, using someappropriate estimation technique (eg, linear ornonlinear regression). To calculate the futurevalue ofy at year n + 1, given Xn + 1, we substitutex"+ 1, into the right hand side of equation (2), setEn+ , to zero (its expected value) and read therequired value of y, (ie, Yn+ i). Note that thedistribution of the disturbance term E in equation(2) enables us to put probability bounds for theestimated parameters off, as well as our forecastYn + 1. This is exactly what is currently being usedin forecasting mean duration of stay andadmission rate, with x, = t and f exponential (seebelow, "Present methods of forecasting"). It isalso instructive to bear in mind that equation (2)can be regarded as one equation of a system ofequations determining y, in which case we mayhave to use more sophisticated estimationprocedures such as two stage least squares, or twostage non-linear least squares, depending on thespecification off.This method has many advantages, the most
notable of which is that it implies a cause andeffect relationship which can be explored further.However from a forecasting point of view it hasthree major defects: (1) To obtain a forecast ofywe need future value ofx, so as Nelson2 puts it, "Itwould appear that the structural model hastransformed rather than solved the forecasting
problem, that is, it transformed it into theproblem offorecasting (exogeneous variables:x)".(2) The distribution of the disturbance termE in equation (2) may be wrongly specified, whichin turn induces error in estimated parameters offas well as forecasted values of y. Note thatmisspecification of the distribution of thedisturbance term in equation (2) is equivalent tomisspecifying distribution of y (see below,"Present methods offorecasting", on this point inrelation to mean duration of stay).3 Therelationship f may be inadequate and imposeunnecessary restriction on the data (see alsobelow).
TIME SERIES OR BOX-JENKINS METHOD OFFORECASTINGIt is important to realise that a time series oflength n is not n different observations ofa randomvariable, but one observation of a multivariaterandom variable. This dependence over time is amixed blessing. On the one hand, standardmethods requiring, independently, identicallydistributed observations cannot be used directly;on the other hand the dependence over time canbe exploited for several purposes, not the least ofwhich is forecasting.
Following our previous notation, in time seriesanalysis we are looking for the specification of thejoint probability distribution of the sequence ofobservations Y1V2,... , Yn: let us denote thisdistribution by P1 ... n(Y,Y2,,Yn) and note that ingeneral the parameter, or even the form of thisdensity, may depend on the time point inquestion. This means that a sequence ofobservations evolves through time, according to aprobability law P. Knowledge ofP will enable usto make inference about future likely values ofy.The Box-Jenkins method is a procedure foridentifying P. This is done in three stages:
(1) Identification-At this stage we entertain aset of possible models for the generating processofy, by comparison of the sample correlogram, ie,plot of covariance ofYt, and Yt - k (k> 0) against kfor a few lags (k); with the correlogram of someknown theoretical models.
(2) Estimation-In this stage we estimate themodels that are entertained in stage (1). The basicidea is to determine the parameter values thatminimise the sum of the squared residuals:
n
t=1
Where z,, is the residual of the model entertained.For example for theARMA (equation 1) model ofequation (2) below we have:
£t= Yt-cyt-I- O-1
This usually requires a non-linear optimisationroutine. The algorithm of Marquardt is amongthe most popular ones. To start the iterativeprocedure an initial estimate of the parameters(a, 0) as well as values for presample periodyo andSo are needed. There are many ways to assignthese values. One simple way is to set yo and co tozero and compute the initial values for parametersby equating the sample correlogram at different
309 on M
arch 31, 2020 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.44.4.307 on 1 D
ecember 1990. D
ownloaded from

R D T Farmer, J Emami
lags to their theoretical counterpart and solvingthe resulting equations. In practice Managerialand Statistical packages such as SAS,statgraphics, etc, take care of these problems andare easily accessible (see 1 2 for more details onthese issues; 2 is especially relevant to managers).(3) Diagnostic checking-This involves applyingtests to see if the model estimated in stage (2) fitsthe data well. One way to do this is to form thecorrelogram of the estimated residuals et:
E etet-kt
rk=
t
and compute the Box-Pierce statisticsQ= (r 2+r22+ ... +rm2)xT (T is the numberof observations) for say m = 8 to 10 for smallmodels. Then for an ARMA(p,q) model,Q-X2(m-p-q). Large values of Q reject thenull hypothesis ofno serial correlation (see 1 2 formore detail). Alternatively we may save fewobservation points in the estimation stage and seehow the estimated model predicts these values.
In the above discussion we assumed that theseries under investigation is stationary, ie, theextent to which two terms in the series are relateddepends only on the time interval between themand not on the time itself. Few series in practicesatisfy this condition, especially if they are levelsrather than rates of change. To overcome thisdifficulty we difference the series first beforeapplying the above procedures. (For an excellentnon-technical discussion of the Box-Jenkinsapproach for managerial purposes see Granger3.)Now suppose that the above procedure suggeststhe following simple model:
yt= + fit (6)
implies that:
Yr-Y - I = P, a constant (7)
If we rewrite equation (4) as:
Yo -ayt_ = ft +0, -I (8)
and compare it with equation (7) we see thatequation (8) uses the data to estimate a and 0,while (7) sets a=1 a priori, and makes no attemptto model the residuals, ie, (7) says that the timeseries is deterministic. The same argument alsoapplies to any polynomial trend.
Present methods of forecasting meanduration of stay and admission rateIn this section we discuss the limitation of thecurrently applied method of forecasting meanduration of stay and admission rate. We suggestthat these limitations are so substantial as toseriously limit their use in the managerial decisionmaking processes, and we apply the Box-Jenkinsmethod to a series of mean duration of stay forgeneral surgery.Within the simple identity (equation 1) the
mean duration of stay and admission rate areprojected separately. The limitations imposedthen are similar; throughout we use meanduration of stay to illustrate our points.
It is usual to arrive at projected values for meanduration of stay by first fitting historicalobservation to a log-linear curve using the methodof ordinary least squares, ie, estimating thecoefficient a and b of the following equation:
log (MDS) = a+ bt
(3)
This equation is known as a first orderautoregressive moving average model. It isautoregressive because it involves the term Yt -,and moving average because (st+ st_,) is amoving average. We first form the forecast ofyn + I(one step ahead forecast ofy), substitute n+1 for tin equation (3) to get:
Yn + I OtYn + en +I+ n (4)
Since we do not know En + I we set it to its expectedvalue zero, and n to the estimated residual fortime n. To obtain the forecast of Yn+ 1(l> 1),repeat the procedure by putting n +I for t inequation (2) to obtain the recursive formula:
Yn+l OYn+I- (5)
and use the value calculated from equation (4) asthe starting value. All this is readily available inmost managerial packages. It is the model weidentified below for mean duration of stay.
In conclusion it is important to realise thatmuch of the information content of data is used inequation (3) to form future forecasts than in asimple deterministic trend in t model. This isbecause a deterministic trend such as:
(9)
In so doing a and b are considered not to dependon time and t is time.The fitted curve is then extrapolated to give a
"value" for the desired year; this is then used inequation (1) to arrive at the forecast of bedsrequired.
Recall our discussion of single equationstructural forecasting; there we pointed out thatmisspecification of the distribution of thedisturbance term £ in equation (2) is equivalent tomisspecification of the distribution of thedependent variable y, ie, mean duration of stay inour context here. We have already pointed outthat the distribution of the dependent variable isskewed. This is not so important with admissionrate since admissions are observed numbers andthe variance accrues from the denominator (thepopulation). The size of the population isnormally so large that the variance of the ratewould be small. Skewing is much more importantwith mean duration of stay. Here the problemarises from the distribution from which the valueis derived.Log normal distribution for the error term may
not be the most suitable distribution as implied byequation (9), for the following reason: equation (9)can be rewritten as
y= a(l-g)t (10)
310
yt= Otyt- I+ Ft+ E)Ft- I
on March 31, 2020 by guest. P
rotected by copyright.http://jech.bm
j.com/
J Epidem
iol Com
munity H
ealth: first published as 10.1136/jech.44.4.307 on 1 Decem
ber 1990. Dow
nloaded from

Models for hospital bed requirements
where a and g are constants, and y = meanduration of stay, where 0<g< I and a > 0. Ifg> 1then (1 -g) < 0, which would contradict the factthaty must be greater than 0. On the other hand ifg<0 then (1-g)>1 and the process wouldexplode as time passes.The crucial point to note about equation (10) is
that whatever values are assigned to a and g, themodel assumes a constant decay rate over time forwhich there is neither a theoretical nor anempirical justification.Our next criticism of the simple model of
equation (10) relates to the fact that such a model(as shown earlier) implies that the processgenerating mean duration of stay is adeterministic function of time. This assumptioncannot be sustained by observations of the realsituation; indeed, at best, time can be viewed as aproxy for important determinants of admissionpolicy and length of stay. The length of time thatindividuals stay in hospital and their probabilityof admission will be affected by, amongst otherfactors, the availability of facilities, lengths ofwaiting lists, current medical practice, patterns ofmorbidity, and fashion. Moreover, within thelinear (or log-linear) static model, the assumptionis that each of the observations carries an equalweight. Thus the admission rate (or meanduration of stay) in year n -10 is accorded thesame importance as in year n-1. This is unlikelyto be a valid assumption. Last year's practices aremuch more relevant to this year because the styleof medical practice, patterns of morbidity,availability of treatments, etc, will have more incommon with those prevailing in the immediatepast than those of the more distant past.
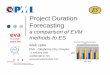
Thirdly any forecasting model must be stableover time, otherwise it is of little value. Thehistorical data on mean duration of stay show thatit fluctuates from year to year in many specialties.In a static regression model this will be reflectedby instability in the value of the coefficients,which will tend to make the forecast unstable.This is shown in fig 3 which gives the 1994"projection" derived from the 1969-77, 1971-79,1973-81, and 1977-85 data sets. Alternatively,this instability can be presiiend in a more compactand elegant way by plotting the coefficients overtime (fig 4).
Finally in most cases, although the value of R2obtained is impressive, the Durbin Watson (DW)statistic is very low. A low DW statistic indicatesthe presence ofautocorrelation in the residuals, ie,that there is systematic information that is notaccounted for by the regression. Since the usual
5-7- s,ss ~~~~1971 -79
5@2- sv ---1969-77o--1973-81
4-7 +
432
1971 1974 1977 1980 1983 19WFigure 4 Plot of regression coefficients over time
formula for the variance of the residuals appearsin the expression of R2, when there isautocorrelation in the residuals this formulaoverestimates or underestimates the true varianceeven in large samples, depending on positive ornegative correlation ofthe residuals. Thus R2 willoverestimate (underestimate) the proportion ofthe true variance which is taken account of by thelinear relationship.
In short the fitted data do not describe theprocess with an acceptable degree of accuracy.This is not surprising in view of our criticism ofthe applicability of specification (equation 9) tothe current problem and the fact that time isassumed to be the sole determinant of meanduration of stay or admission rate.To give a concrete example of our suggested
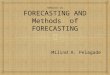
method of analysis we applied the Box-Jenkinsmethodology, outlined above, to the time series ofmean duration of stay for general surgery for agegroup 15-44 (1969-1982). Figure 5 compares thelog-linear trend and the Box-Jenkins fit of thedata. It is clear from the figure that the time seriesmodel mimics the movement of the series,
8.6
----Time trend
> 7-6- ........... Time series
°6-6^s ~ ~ Actual
C646.o * .
4' 4..
4-61969 1972 1975 1978 1981 1984
Figure S Plot of fitted and actual values for meanduration of stay (days): general surgery (age 15-44years)
whereas the log-linear model does not. This gainis mainly due to the fact that the informationcontent ofthe residuals from a log-linear trend hasbeen taken into account in the time seriesapproach.
Relationship between mean duration ofstayand admission rateWe have already drawn attention to the fact that,in forecasts of hospital bed requirements derivedfrom equation (1) by incorporating independent
Figure 3 1994projections: generalsurgery (age 15-44years)
311 on M
arch 31, 2020 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.44.4.307 on 1 D
ecember 1990. D
ownloaded from

R D T Farmer, J Emami
projections of mean duration of stay, admissionrate, and population to be served, the assumptionis that variations in each are not correlated. Frominspection of the past trends in both meanduration of stay and admission rate, it is clear thatchanges in some specialty, age, and sex groupstend to correlate. There are empirical reasons tosuppose that mean duration of stay and admissionrate will not be independently determined.Firstly, there tends to be a finite number of bedsand the demand for their use tends to be greaterthan their supply. Under these circumstances,hospital bed days vacated by a decrease in theaverage duration ofstay are likely to be filled by anincrease in the number of admissions to thosebeds. Secondly, even were there not to be a supplyconstraint, the policy in some specialties ofadmitting patients for part of the investigations ortreatments they require, discharging them, andthen readmitting them for completion of thetreatments, will result in a decrease in the meanduration of stay and an increase in admission rate,but will not necessarily effect any change in thegross number ofhospital days per patient episode.
If all of the principal components in equation(1) are projected under the assumption that eachvaries independently of the other, then the likelyresult will be misleading forecasts. Inadequacy ofthe forecast will be compounded by the fact thatnone of the parameters is weighted. The reasonsfor this are as follows. Equation (9) is concernedwith rate of change. Consider the situation where,over a long period, both mean duration of stay andadmission rate tend to decrease, but in which inthe immediate past admission rate increases andthere is an increase in the rate of decay of meanduration of stay. The regression will result in aglobal trend over the whole period and recentchanges will tend to be masked. Multiplying thetwo projections without correction forinterdependence will result in either an inflated ordeflated value for the bed forecasts.We conclude that a joint estimation of mean
duration of stay and admission rate is likely toresult in a more accurate forecast of beds. Theapproaches outlined above for single equationmodels can easily be generalised to amultiequation system or vector time series model.Here we attempt to discover the joint distributionof the three important variables involved, ie, thevector [MDS,AR,BEDS]. Such models estimatethe following general type of system:
MDS = f(BEDS,AR,MDS - 1,W) +F£1AR = f(BEDS,AR- 1,MDS,U)+s2BEDS = (AR*MDS*POP*F)/365
where W and U represent one or more exogenousvariables and s&,c2 are error terms which are notindependent ofeach other. In this system ifW andU were restricted to historical values of thevariables involved then the system would be avector time series model; if in addition theyinclude other exogenous variables, then thesystem would be a dynamic simultaneousstructural model. It is clear that the gain inforecast accuracy will be a consequence of thejoint estimation method, and the fact that thedisturbance term's correlation structures has beentaken into account. The type of data needed toestimate such models is no different to that of theunivariate case. Again many of the presentlyavailable statistical and managerial packages havefacilities to estimate such models.
ConclusionThere is no doubt that health service plannersrequire access to models for predicting futureneeds for health care facilities. Forecasting therequirements for acute hospital beds is ofparticular importance because of the substantialcapital and cost implications. Careful examinationof the most frequently used method indicates thatit does not describe historical patterns of hospitalbed utilisation accurately. When it is used toproject future requirements, it is inherentlyunstable. (The reasons for this instability arediscussed in detail.) Two alternative approachesto forecasting-time series and structuralmodels-have been discussed. The time seriesapproach seems to offer greater scope formanagerial forecasting.
1 Box GEP, Jenkins GM. Time series analysis-forecasting andcontrol. San Francisco: Holden-Day, 1976.
2 Nelson CR. Applied titne series analysis for managerialforecasting. San Francisco: Holden-Day, 1973.
3 Granger CWJ Forecasting in business and economics. NewYork: Academic Press, 1980.
4 Townsend P, Davidson N. Inequalities in health (The BlackReport). Harmondsworth, UK: Penguin Books, 1982.
5 Townsend P, Phillimore P, Beattie A. Health and deprivation.Inequality in the north. London: Croom Helm, 1988.
6 Jarman B. Identification of underprivileged areas. Br Med J1983; 286: 1705-8.
7 Department of Health and Social Security. Sharing resourcesfor health in England. Report of the Resource AllocationWorking Party (RAWP). London: HMSO, 1976.
312 on M
arch 31, 2020 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.44.4.307 on 1 D
ecember 1990. D
ownloaded from