Embed Size (px)
Citation preview
Mobilizing in the ICU: A Roadmap (for the rest of us)
Jeffrey M Singh, MD FRCPC MSc
Critical Care and Neurocritical Care
Toronto Western Hospital
and
Interdepartmental Division of Critical Care
University of Toronto
Disclosures
• I am the recipient of:
– unrestricted quality improvement
grants from Hospira
– honoraria from Snell Medical

Spot Quiz!
• How many PDSA cycle(s) are required
to implement an early mobility program
in the ICU with 75% compliance?
1. One cycle
2. Two cycles
3. Three cycles
4. Four cycles
Answer: TRICK QUESTION!
I don’t know… but it is ≥4!

Objectives
• Share a story of:
– Quality Improvement
– What we did
– Humility in acknowledging our
mistakes
– What worked and didn’t work
Toronto Western Hospital
• Part of UHN
• 236 beds
• 25 bed MSNICU – 40% neuroscience
• Specialty Programs – Neurosurgery / Spine
– Neurology / Stroke
– Ortho / Hand
– Bariatric
– Ophthalmology
ABCDE
Awake targeted sedation
and daily awakening
Breathing spontaneous
breathing trials
Coordination of SAT & SBT
Delirium Screening
Early Mobility

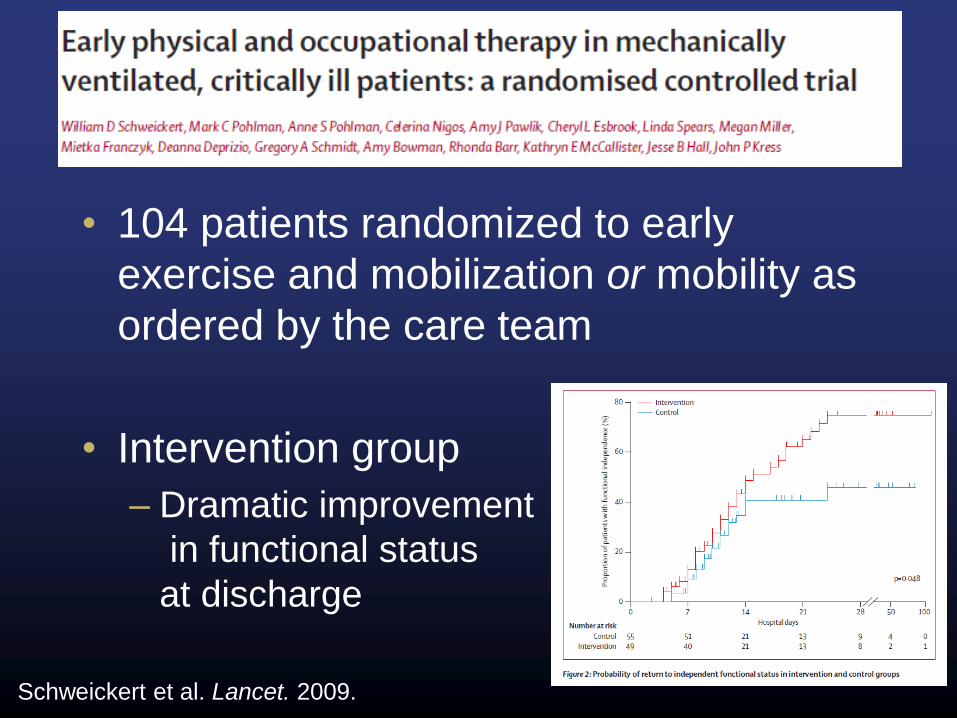
• 104 patients randomized to early
exercise and mobilization or mobility as
ordered by the care team
• Intervention group
– Dramatic improvement
in functional status
at discharge
Schweickert et al. Lancet. 2009.
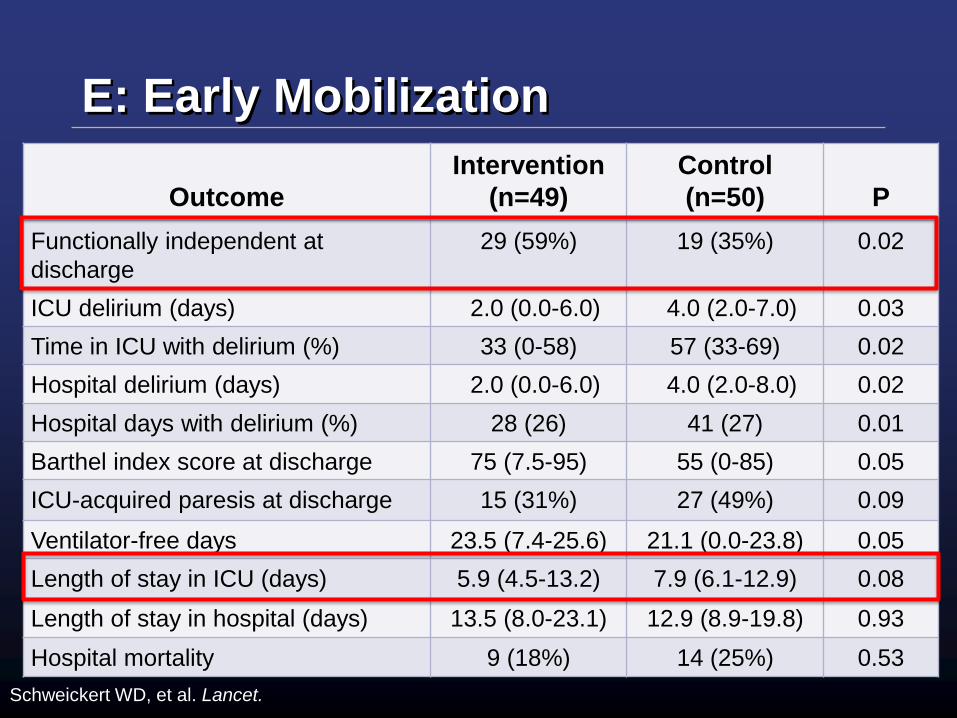
E: Early Mobilization
Outcome
Intervention
(n=49)
Control
(n=50)
P
Functionally independent at
discharge
29 (59%) 19 (35%) 0.02
ICU delirium (days) 2.0 (0.0-6.0) 4.0 (2.0-7.0) 0.03
Time in ICU with delirium (%) 33 (0-58) 57 (33-69) 0.02
Hospital delirium (days) 2.0 (0.0-6.0) 4.0 (2.0-8.0) 0.02
Hospital days with delirium (%) 28 (26) 41 (27) 0.01
Barthel index score at discharge 75 (7.5-95) 55 (0-85) 0.05
ICU-acquired paresis at discharge 15 (31%) 27 (49%) 0.09
Ventilator-free days 23.5 (7.4-25.6) 21.1 (0.0-23.8) 0.05
Length of stay in ICU (days) 5.9 (4.5-13.2) 7.9 (6.1-12.9) 0.08
Length of stay in hospital (days) 13.5 (8.0-23.1) 12.9 (8.9-19.8) 0.93
Hospital mortality 9 (18%) 14 (25%) 0.53
Schweickert WD, et al. Lancet.

The QI Plan
• Understand the local context
• Identify champions – get a team
• Identify barriers
• Develop a multifaceted intervention:
– Structure
– Process
– Outcomes
• Plan, Do, Study, Act cycles

(Perceived) Barriers to Mobilization
• Clinical instability
• Clinical inertia
• Lack of resources
• Lack of time / workload issues
• Safety
– Line / tubes / drain removal or
displacement
• Lack of physician orders / bedrest
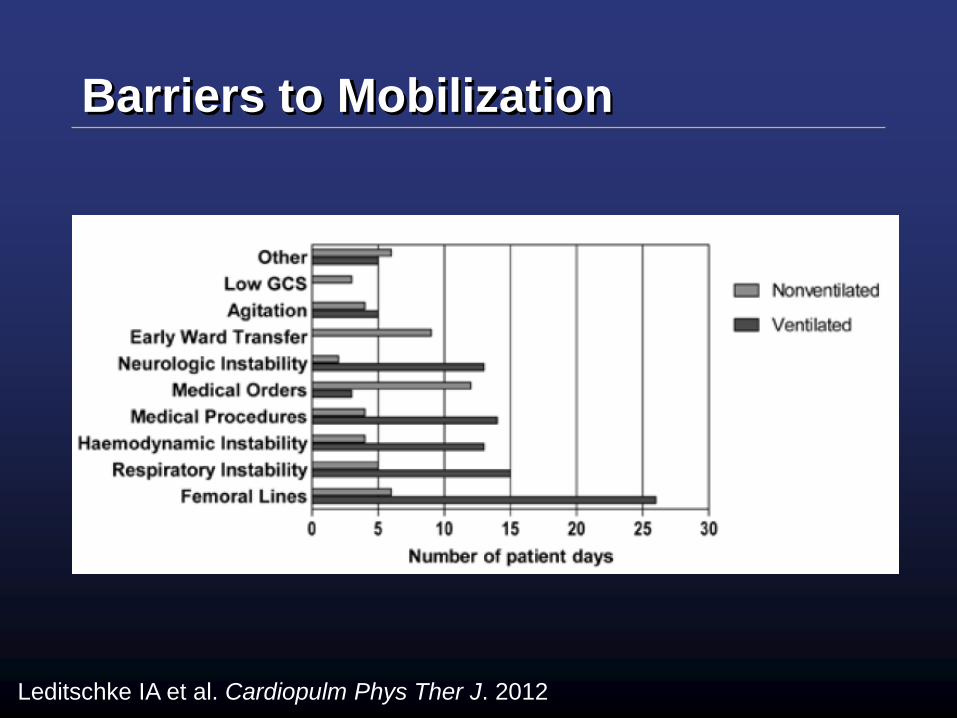
Barriers to Mobilization
Leditschke IA et al. Cardiopulm Phys Ther J. 2012
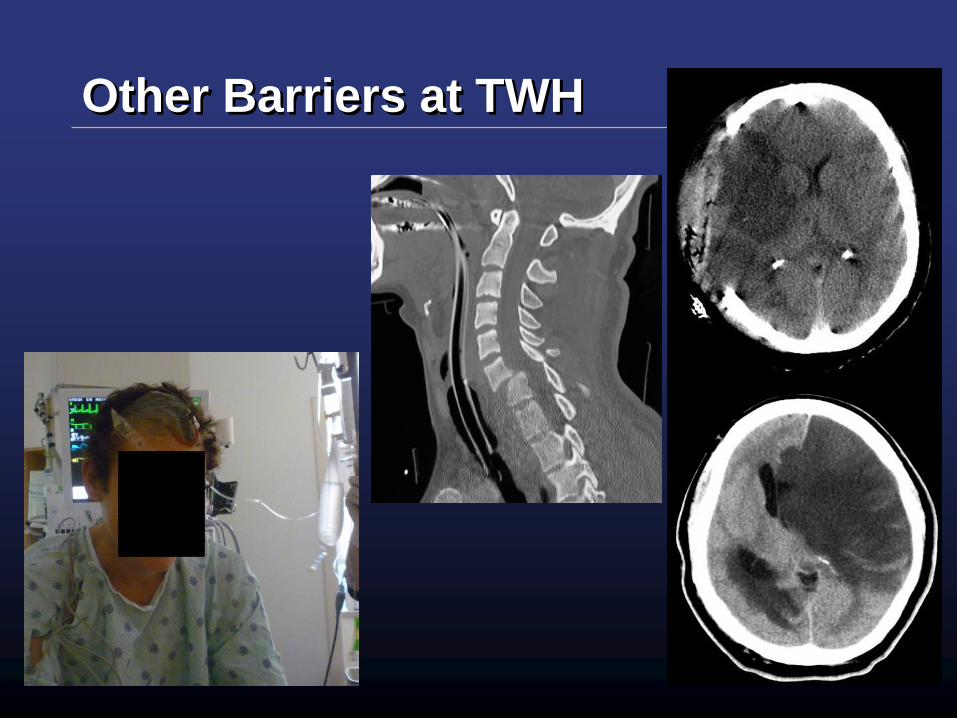
Other Barriers at TWH

Structure
• 1.5 Physiotherapy FTE
• 2 Personal Care Assistants
• Equipment
– Purchase of 2 new chairs
– Lifts & slings
– Walkers
• Medical directives
– Development of PT self-referral directive
• AAT orders

Process
• What do we want the team to do?
• Daily expectation for each eligible
patient to be mobilized
• Mobility target set by ICU
physiotherapist

Safety: Contraindications
• Receiving neuromuscular blockade
• SaO2 < 88% on FiO2 < 0.5
• Significant pressor/inotrope use
• Myocardial ischemia in last 24 hrs
• Raised ICP
• Unstable C-spine
• No arrhythmia requiring administration of new
antiarrhythmic agent in last 24 hrs

Safety: Screening
• Patients that require a PT consult prior
to mobilization:
– All SCI
– New neurological deficits
• Any new hemiparetic/hemiplegic patients
• Neurovascular disease
• Seizures
• All other patients receive safety screen
then mobilize
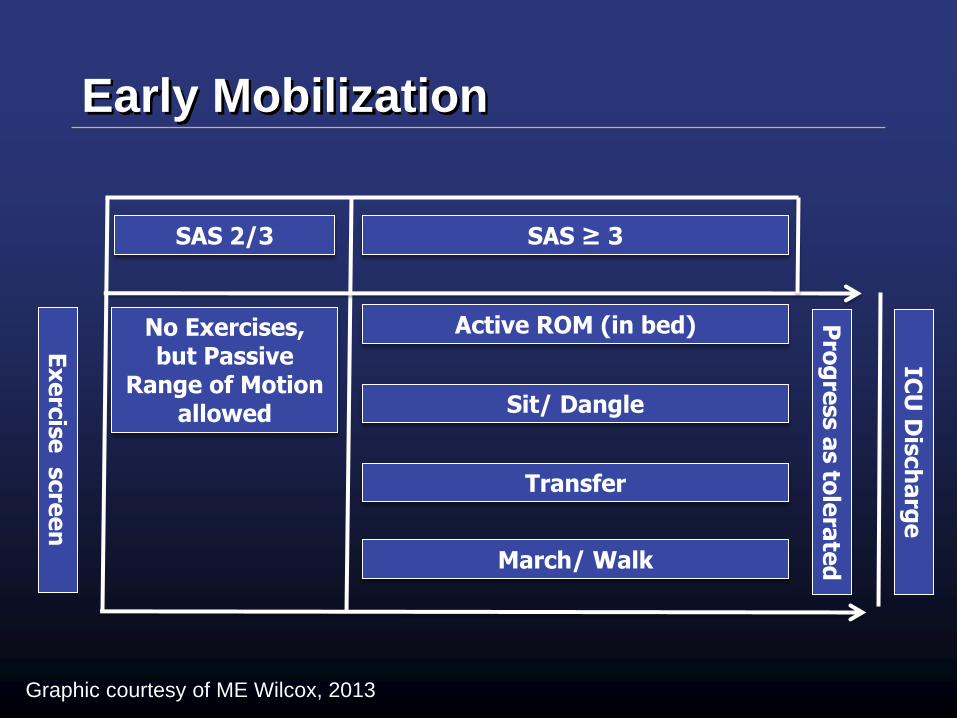
Active ROM (in bed)
Sit/ Dangle
March/ Walk
Transfer
No Exercises, but Passive
Range of Motion allowed
Pro
gre
ss a
s to
lera
ted
IC
U D
isch
arg
e
Ex
erc
ise
scre
en
SAS ≥ 3 SAS 2/3
Early Mobilization
Graphic courtesy of ME Wilcox, 2013

Courtesy of ME
Wilcox, 2013
Outcomes
• How are we going to measure our
progress?
• How do we measure mobility?
– Valid
– Responsive to changing behaviour
• ICU Mobility Scale
Hodgson CL. Am J Respir Crit Care Med 187;2013:A3123

Classification Definition
0 Nothing (lying in bed) Passively rolled or passively exercised by staff, but not actively moving
1 Sitting in bed, exercises in bed Any activity in bed, including rolling, bridging, active exercises, cycle ergometry and
active assisted exercises; not moving out of bed or over the edge of the bed
2 Passively moved to chair (no standing) Hoist, passive lift or slide transfer to the chair, with no standing or sitting on the edge
of the bed
3 Sitting over edge of bed May be assisted by staff, but involves actively sitting over the side of the bed with
some trunk control
4 Standing Weight bearing through the feet in the standing position, with or without assistance.
This may include use of a standing lifter device or tilt table.
5 Transferring bed to chair
Able to step or shuffle through standing to the chair. This involves actively
transferring weight from one leg to another to move to the chair. If the patient has
been stood with the assistance of a medical device, they must step to the chair (not
included if the patient is wheeled in a standing lifter device.)
6 Marching on spot (at bedside) Able to walk on the spot by lifting alternate feet (must be able to step at least 4 times,
twice on each foot), with or without assistance
7 Walking with assistance of 2 or more
people Walking away from the bed/chair by at least 5 metres (5 yards) assisted by 2 or more
people
8 Walking with assistance of 1 person Walking away from the bed/chair by at least 5 metres (5 yards) assisted by 1 person
9 Walking independently with a gait aid Walking away from the bed/chair by at least 5 metres (5 yards) with a gait aid, but no
assistance from another person. In a wheelchair bound person, this activity level
includes wheeling the chair independently 5 metres (5 years) away from the bed/chair
10 Walking independently without a gait aid Walking away from the bed/chair by at least 5 metres (5 yards) without a gait aid or
assistance from another person.

Outcomes
• PT recorded target mobility level for
each patient
• Actual activity level achieved was
recorded at end of day for each patient
• If activity done in evenings then data
revised the next morning.

False Start
• Educational Blitz:
– Inservices & Education
– Posters
– Daily Reminders
• But:
– Lacked total physician buy-in
– Nurses still not clear on what we expected
them to do
No Impact
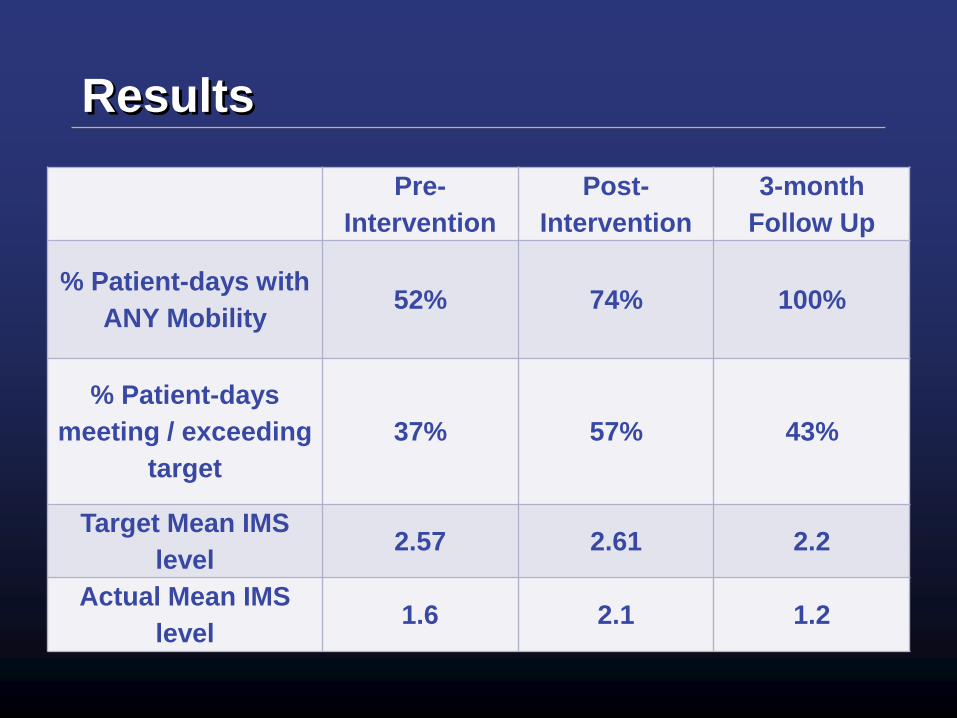
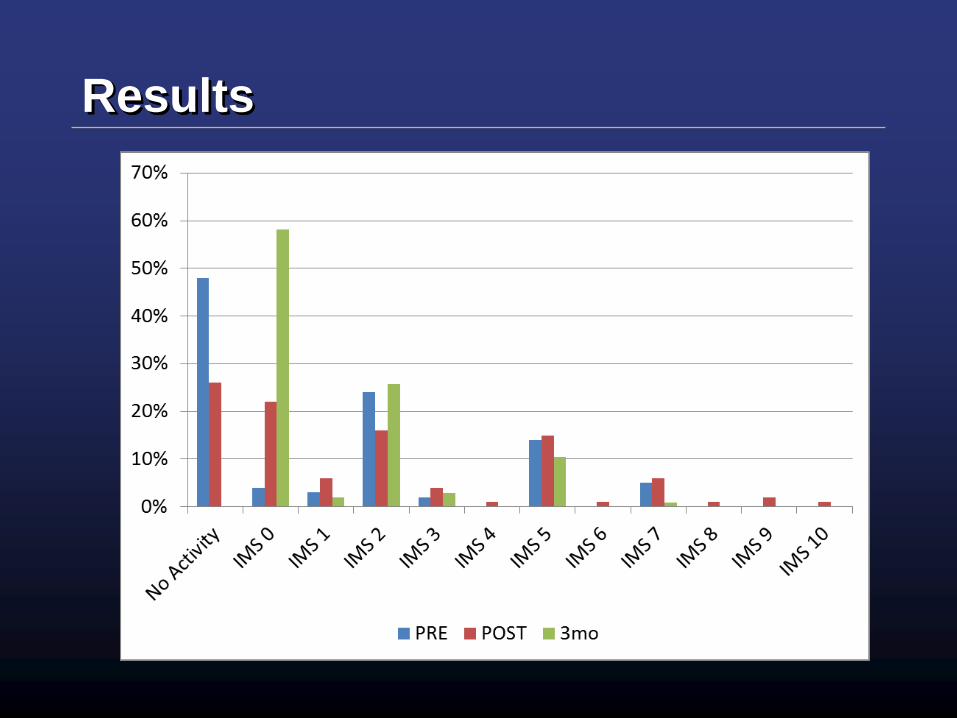
Results
Pre-
Intervention
Post-
Intervention
3-month
Follow Up
% Patient-days with
ANY Mobility 52% 74% 100%
% Patient-days
meeting / exceeding
target
37% 57% 43%
Target Mean IMS
level 2.57 2.61 2.2
Actual Mean IMS
level 1.6 2.1 1.2
Results
Results - Safety
• Consistent with published evidence –
very safe
– One NG tube displaced
– One patient fell to their knees from a chair
• Returned to chair actively with assistance
– External Ventricular Drains
Olkowski B et al.Physical Therapy. 2013
Hale et al. Physiotherapy Canada. 2013.

Comparisons
• Practice Audit
– 54% of patients received any mobilization
– 43% active
– 23% active transfer
– 34% passive
Leditschke IA et al. Cardiopulm Phys Ther J. 2012
Myths To Debunk
• All of this has to happen in the day shift
• You can’t mobilize neuro patients
• Every patient needs a PT assessment
before I start mobilizing
• Passive transfer into a chair is enough
Key Tips I Have Learned
• You must engage everyone
– Spend equal time on your biggest
supporter and biggest sceptic
• You must measure your progress
– It doesn’t have to be extensive /
complicated
• Feedback results to the team
– Seeing is believing!
• Not everyone is on a treadmill
Acknowledgements
• Lisa Muc PT
• Christopher Iacob PT
• Elizabeth Wilcox MD
• Emma Mew
• Mandy Ettinger
…and ALL of the interprofessional team







![SOLUTIONS FOR ICU & EMERGENCY CaRE ICU-UK-BD[1].pdf- SOLUTIONS FOR ICU & EMERGENCY CaRE - 3 Emergency Care NICU SURGIRIS is by your side We offer our know-how to support your project](https://img.dokumen.tips/doc/110x75/5d22d0a388c993f2168e102a/solutions-for-icu-emergency-care-icu-uk-bd1pdf-solutions-for-icu-emergency.jpg)






















