Embed Size (px)
Citation preview

ירמיהו הייניק' פרופח איכילוב"ביה, מרכז פסיכוגריאטרי מרגולץ
אביב-אוניברסיטת תל, הפקולטה לרפואה
מבחנים קוגניטיביים��DSM-5)פסיכיאטר של הזיקנה(קלינאי �
1
1) MMSE+
2) CDT
המבחנים הקוגניטיביים המובנים הנפוצים ביותר
“lingua franca” =MMSEשל הבדיקה הקוגניטיבית
3) Delayed word recall4) Verbal fluency test5) Similarities6) Trail Making Test (TMT)
No single test is adequate !
2
Item Max Score Actual Score Remarks
Day [1] 1
Date [1] 1
Month [1] 1 Orientation, time
Year [1] 1
Season [1] 1
County [1] 1
Town [1] 1
Streets [1] 1 Orientation, place
Floor [1] 1
Place [1] 1
Name Objects [2] 2 Language
Ifs [1] 1
Registration [3] 3 Registration
Serial sevens [5] 5 Attention/calculation
Recall objects [3] 2 Recall
Read: close eyes [1] 1 Language
Pentagon [1] 1
Write [1] 1* "שנת חיים ויצירה"
Paper folding [3] 3
Total 30 29* 28* 3 4

5 6
P15
DSM-5 Diagnosis
Frontotemporal Neurocognitive Disorder,
Language Variant
Semantic dementia
First described: Pick, 1904
Characterized: Warrington, 1975
Given name: Snowden et al. 1989
Associated with temporal lobe atrophy: Hodges et al. 1992
7
:מבוא קצר�הסתכלות של פסיכיאטר של הזיקנה על מבחנים קוגניטיביים מובנים�
ומה שקדם לה DSM-5הצעת �
בכל הסתכלות עכשוית טבועה פרספקטיבה היסטורית�
�MMSE
�CDT
�]MOCA[
אבחנה ולא /הפציינט מגיע למטרת אבחון�
screeningלשם �CAMCOG
�CAMCOG מורחב
דוגמאות�
8

המבחן הקוגניטיבי
תופס מקום מוגדר וחלקי1.
(Descriptive)הינו אירוע של פסיכופתולוגיה תיאורית 2.
תרומת הפרספקטיבה ההיסטורית3.
9 10
Family pedigree and genetic aspects
Patient Informant
Longitudinal
Physical aspects
Auxilliary tests Treatmentaspects
Patient Informant
Cross-sectional
Descriptive psychopathology
� Almost universally, a language (descriptive psychopathology) is now used to record the symptoms of mental disease
� …it consists of a vocabulary, a syntax, assumptions about the nature of behavior, and some application rules
� This language was composed in Europe during the first half of the 19th century, and has proved to be surprisingly stable
11
פסיכופאתולוגיה דסקריפטיבית הינה התיאור המדויק �
קוגניציות והתנהגויות , והקטגוריזציה של חוויות
הערכה (כפי שהן מדווחות על ידי הפציינט , אבנורמליות
וניצפות על ידי הקלינאי ) אמפטית של החוויה הסובייקטיבית
אובסרבציה דיסקריפטיבית
פנומנלוגיה
פסיכופאתולוגיה
פסיכודינמייםאינטרפרטיבית
התנהגותיים
קוגנטיביים
אקסיסטנציאליתNeuroscience???
12

Item Max Score Actual Score Remarks
Day [1] 0
Date [1] 0
Month [1] 0
Year [1] 0
Season [1] 0
County [1] 1
Town [1] 1
Streets [1] 1
Floor [1] 1
Place [1] 1
Name Objects [2] 2
Ifs [1] 1
Registration [3] 3
Serial sevens [5] 4
Recall objects [3] 1
Read: close eyes [1] 0 "שעון, עפרון"אומר
Pentagon [1] 0
Write [1] 1 "מה שצרתי זה מרובע"
Paper folding [3] 3
Total 30 2013 14
15 16

17
"חתך אורך"
חתך "
"רוחב
תובנה
ציור
שעון
; "בסדר"
מה "
שצרתי
זה "מרובע
אפקט אפאטי
הלך חשיבה פרסברטיבי
"הולך למשרד"קונפבולציות
אשתי בביקור "
אצל ההורים "באירופה
18
קלסיפיקציות
בפסיכיאטריה
קבוצת חוקרי�
אישיות
textbook
למטרות , מדינהארגו� מקצועי
מסוימות
פורמאליות
Alzheimer’s disease the flagship
Senile dementia (the prototype for the dementias)
Age and aging mechanisms important
Parenchymal and vascular hypotheses
Other etiologies
�1900מ
�בער
Dementia = Cognitive paradigm (essential features for dementia was intellectual impairment; delusions, hallucinations, mood, behavior - all epiphenomena)
Gradual attrition of the concept of
dementia
Localized memory impairment (amnesic synd.)
Vesanic/ defect statesStuporous states; acute
dementia____Dementia = psychosocial incompetence; cognitive impairment; delusions, hallucinations; NO irreversibility; NO old age; a terminal state to all sorts of mental, neurological and physical conditions; a wide range concept
1800
anatomic-pathological- clinical model
1900
1970
2000
Syndromic
Dementia syndrome of depression
Dementia is the clinical syndrome of mental life characterized by substantial global decline in cognitive function that is not attributable to alteration in consciousness
�The clinical syndrome of dementia
YES NO
�The clinical syndrome of dementia attributable to “organic” brain disease�Dementia carries the implication, the presumption of progression
Jaspers/Lewis/McHugh/Folstein An appeal to a presumed etiology
Roth

USA World
21
APA Standard Veterans’ Administration
Armed forces nomenclatureWorld War II
DSM-I (1952)
DSM-II (1968)
DSM-III (1980)
DSM-III-R (1987)
DSM-IV (1994)
DSM-IV-TR (2000)
DSM-V (2013?)
International list of causes of death – Paris 1900
Fifth Revision (1938) ללא סקציה
נפרדת להפרעות
נפשיות
ICD-6 (1948)לראשונה סקציה
נפרדת להפרעות
נפשיות
פיגור
סכיזופרניה
מניה דפרסיה
כל האחרי�ICD-7
ICD-8
ICD-9-CM (1978)בשימוש רשמי (
)בישראל
ICD-10! ! ! ! (1992)) בשימוש רשמי
)בישראל
ICD-11 (2015?)
The DSMs: Organic/cognitive disordersDSM-I 1952 Organic Mental Disorders
DSM-II 1968 Organic Brain Syndromes
DSM-III 1980 Organic Mental Disorders
DSM-III-R 1987 Organic Mental Disorders
DSM-IV 1994 Delirium, Dementia and Amnestic and Other Cognitive
Disorders
DSM-IV-TR 2000 Delirium, Dementia and Amnestic and Other Cognitive
Disorders
DSM-V 2013* Neurocognitive Disorders
• אנו מתבססי� על ה; 2013מיועד לצאת לאור במאי draft 2012של אפריל
�DSM-1
�DSM-3
�DSM-3-R
�DSM-4
�DSM-5
23
1. Impairment of orientation
2. Impairment of memory
3. Impairment of all intellectual functions (comprehension, calculation, knowledge, learning, etc.)
4. Impairment of judgment
5. Lability and shallowness of affect

1. A loss of intellectual abilities of sufficient severity to interfere with social or occupation functioning
2. Memory impairment and3. At lease one of the following:
a) Impairment of abstract thinkingb) Impaired judgmentc) Other disturbances of higher cortical function such
as aphasia, apraxia, agnosia, or constructional difficulty
d) Personality change
4. Change not attributable to alteration in consciousness
5. Evidence from history , physical examination , or laboratory of a specific etiological factor; or in the absence of such evidence, the presumption of such a factor
A. Demonstrable evidence of impairment in short- and long-term memory
B. At least one of the following:1) impairment in abstract thinking2) impaired judgment3) other disturbances of higher cortical function such as
� aphasia� apraxia� agnosia� “consructional difficulty”
C. The disturbances in A and B significantly interfere with work or usual social activities or relationships with others
D. Not ….. DeliriumE. Either (1) or (2):
(1)…..(2)….
A. The development of multiple cognitive deficitsmultiple cognitive deficitsmultiple cognitive deficitsmultiple cognitive deficitsmanifested by botha) Memory impairment
b) One (or more) of the following cognitive disturbances
a) Aphasia
b) Apraxia
c) Agnosia
d) Disturbance in executive functioning
B. A1 and A2 each cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning.
�Delirium�Mild Neurocognitive Disorder�Major Neurocognitive Disorder�NO dementia�NO Amnestic disorder�Other OMDs spread into other disorders(e.g., depressive disorder associated with medical condition)
�NO deficits, YES performance�NO DAT supremacy�NO memory impairment supremacy�No multiple cognitive deficits supremacy

Origins
Of terminology Of concept
Neuropsychology and Neurology
“MCI spectrum” research
Working groups and Task Forces on
specific disorders
Pre-senileAlzheimer
disease concept
Other
1.1.1.1. Complex attention: Complex attention: Complex attention: Complex attention: sustained attention, divided attention, selective attention, processing speed
2.2.2.2. Executive ability:Executive ability:Executive ability:Executive ability: planning, decision-making, working memory, responding to feedback/error correction, overriding habits, mental flexibility
3.3.3.3. Learning and memory: Learning and memory: Learning and memory: Learning and memory: immediate memory, recent memory (including free recall, cued recall, and recognition memory)
4.4.4.4. Language:Language:Language:Language: expressive language (including naming, fluency, grammar and syntax) and receptive language
5.5.5.5. VisuoconstructioalVisuoconstructioalVisuoconstructioalVisuoconstructioal----perceptual ability: perceptual ability: perceptual ability: perceptual ability: construction and visual perception
6.6.6.6. Social cognition:Social cognition:Social cognition:Social cognition: recognition of emotions, theory of mind, behavioral regulation

A. Evidence of modest decline modest decline modest decline modest decline from a previous level of performance in one or more of the domains outlined above based on:1. Concerns of the individual, a knowledgeable informant, or
the clinician that there has been a modest decline in cognitive function; and
2. A decline in neurocognitive performance, typically involving test performance in the range of 1 and 2 standard deviations below appropriate norms (i.e., between the 3rd and 16th percentile) on a formal testing or equivalent clinical evaluation.
B. The cognitive deficits are insufficient to interfere with independence (i.e. instrumental activities of daily living (more complex tasks such as paying bills or taking medications) are preserved, but greater effort, compensatory strategies, or accommodation may be required to maintain independence.
C. No Delirium
D. The cognitive deficits are not primarily attributable to another mental disorder (e.g., Major Depressive Disorder, Schizophrenia)
A. Evidence of substantial cognitive decline from a previous level of performancperformancperformancperformance in one or more of the domains outlined above based on:1. Concerns of the individual, a knowledgeable individual, or the
clinician that there has been a substantial decline substantial decline substantial decline substantial decline in cognitive function and
2. A decline in neurocognitive performanceperformanceperformanceperformance typically involving test performance in the range of two or more standard deviations below appropriate means (i.e., below the 3rd percentile) on formal testing or equivalent clinical evaluation
B. The cognitive deficits are sufficient to interfere with independence (i.e., requiring assistance at a minimum with instrumental activities of daily living [more complex tasks such as paying bills or managing medications])
C. The cognitive deficits do not occur exclusively in the context of a Delirium
D. The cognitive deficits are not primarilyprimarilyprimarilyprimarily attributable to another mental disorder (e.g. Major Depressive Disorder, Schizophrenia)
�Neurocognitive disorder due to Alzheimer’s disease
�Vascular neurocognitive disorder�Frontotemporal neurocognitive disorder
Neurocognitive disorder due to:
�Substance-induced neurocognitive disorder�Neurocognitive disorder not elsewhere classified
�Traumatic brain injury�Lewy body disease�Parkinson’s disease�HIV infection�Huntington’s disease�Prion disease�Another medical condition

37
MCI-Criteria for the clinical and cognitive syndrome cont’d
•Episodic memory tests
(immediate and delayed
recall; determine retention
over a delay)
Word list
learning testsOne trial
Multiple trials
•Free & Cued Selective Reminding Test
•Rey Auditory Verbal Learning Test
•California Verbal Learning Test
Delayed recall of a paragraph
•Wechsler Memory Scale Revised Logical Memory I and II
verbal materials-Immediate and delayed recall of a non
•Visual Reproduction labtests of WMS-Revised I and II
•Rey Osterieth Complex Figure
•Executive functions tests Trail Making Tests
•Language Boston Naming Test, Letter and Category Fluency
•Visuoconstuctional- perceptual Figure copying (RCF)
•Attention digit span
•If cognitive testing not feasible simple, informal
techniques
•Episodic memory tests
(immediate and delayed
recall; determine retention
over a delay)
listWord
testslearningOne trial
Multiple trials
•Free & Cued Selective Reminding Test
•Rey Auditory Verbal Learning Test
•California Verbal Learning Test
Delayed recall of a paragraph
•Wechsler Memory Scale Revised Logical Memory I and II
verbal materials-Immediate and delayed recall of a non
Cognitive assessments
� WAIS
� WMS
� Bender-Gestalt Test
� Halstead-Reitan Battery
� Rorschach
כללים(Slater and Roth 1977)
1. Behavior and talk2. Mood3. Preoccupation
morbid beliefs,disorders of perception
4. SensoriumOrientationMemoryAttention and concentrationGeneral informationIntelligence
5. Insight/judgment
38
נויר/פסיכולוגיהנוירולוגיהפסיכיאטריהפסיכולוגיה-ו
כ מכומתים"מבחנים בדלא מכומתים}מכומתים{
focal lesionמכוונים ל"”localizationך
(Mayer-Gross & Guttman, 1937)(Klein and Mayer-Gross, 1957)
1. Mood2. Orientation3. Attention and adaptability
4. Memory5. Use of numbers6. Speech7. Visual and related functions
8. Auditory perception9. Tactile perception and “body image”
10.Motility
39
מידע מדויק
,זמן
, מורכבות
, מומחיותתקציב
אוכלוסיית הפציינטים
רמה בסיסית
רמת ביניים
רמה מתקדמתרמה בסיסית�
�Brief cognitive tests�Screening tests
� CERAD
� MDRS/DRS
� ADAS - cog
� COGNISTAT
� RBANS
� CAMCOG/CAMCOG-R
� ACE
� Computerized cognitive testing
� MMSE� CDT� Mini-Cog� MIS� GPCOG� MoCA� FAB� Similarities� Trail tests� Verbal fluency
� ‘7MS� SASS� SPMSQ
40
רמת ביניים��Comprehensivecognitive screening
רמה מתקדמת�
הערכה נוירופסיכולוגית קלינית�

בודקים טווח מצומצם של תחומים קוגניטיביים�
נותנים אינדיקציה גסה למדי של הסטטוס הקוגניטיבי�
דורשים ידע תיאורטי ורמת הכשרה בסיסים ביותר �כאשר , מיושמים בקהילה או ברפואה ראשונית. להעברה
בן משפחה או כאשר מתעורר / מופיעות תלונות של פציינט חשד קליני אצל הרופא
אלא , מבחנים אלה אינם מובילים לדיאגנוזה�
צריכים לתת אינדיקציה לנוכחות של ליקוי מובהק קלינית �. ובהתאם הפניה למומחים
הם מייצגים את השלב הראשון בתהליך ההערכה ומסייעים �בזיהוי מוקדם של דמנציה
חלקם יעיל גם למעקב�
41
בודקים טווח רחב יותר של תפקודים קוגניטיביים�
חלקם מאפשרים להפיק ציוני אינדקס לתפקוד בתחומים שנבדקו�
נדרשים ידע תיאורטי ומומחיות מקצועית להעברת המבחן �
ולפרשנות נכונה של הממצאים
אשר לעיתים מתייחסים , חלקים מהווים בטריות נוירופסיכולוגיות�
אליהם ככלי סינון קוגניטיבי מקיפים
הם מתאימים יותר ליישום במסגרות מומחים שניוניות או �
שלישוניות
בחלק מהמקרים שימוש בכלים אלה יספיק לקביעת דיאגנוזה �
עשויה להידרש הפניה להערכה , כאשר הממצאים אינם ברורים�נוירופסיכולוגית מלאה
42
הערכה נוירופסיכולוגית קלינית הכוללת על פי הצורך כלי �
בטריות ומבחנים נוירופסיכולוגיים, סינון קצרים וארוכים
מורבידית-והערכה פרה, ראיונות קליניים, שאלונים, ייעודים
חולשות של היבטים /מאפשרת הפקת פרופיל חוזקים�
ולעיתים גם מוטורים , רגשיים, התנהגותיים, קוגניטיביים
תוך לקיחה בחשבון של , וסנסורים אצל הנבדק המסוים
.רמת התפקוד הפרה מורבידית המשוערת שלו
אינה מחליפה את ההערכה הרפואית הקלינית אלא �
במטרה לגבש חוות דעת דיאגנוסטית , משלימה אותה. והמלצות לניהול מחלה ולהתערבות
43
� Quick (less than 2 minutes)
� Well-tolerated, easy to administer and score
� Independent of culture, language, education
� IRR, test/re-test
� Sensitivity and specificity
� Predictive validity
� Casts a wide net
44

� Brief memory test
� Clock-drawing
� Verbal fluency
� MMSE
� informant
45 46
Mini-Cog
3-Item Recall=0 3-Item Recall=1-2 3-Item Recall=3
CDT Abnormal CDT Normal
Demented Non-Demented
Demented Non-Demented
Borson et al (2000)
Folstein _MMS1975
Shulman-CDT1986
Roth_CAMCOG1986
Nasredine-]MoCA[2005
47 48

49
� In 1972 Susan was pregnant with our first child and was a second year resident in psychiatry at NYH-WD
� On morning walk rounds, I would ask her to report on the patients’ mental states. Her reports were accurate and concise concerning vital signs and the presence or absence of delusions, hallucinations, and depression
� However, the cognitive state was not systematically or qualitatively reported
� I was always asking for more information
� Finally, she said, “Just write down the way you want it”. That night we conceived the MMS Examination
50
MMS items – taught to me by M. Victor and P. McHugh� derived from items found in textbooks such as Mayer-Gross Slater and Roth and Post
MMS item selection� those that had been clinically useful to me
� Those which I could remember and apply without any additional equipment at the bedside
� Those that could be scored with little interpretation
Weighting of scores (items): completely intuitive!!
No’s: � No grant
� No training in psychometrics/statistics
� No power analysis
� No factor analysis
Yes:� The power of youth!
PS No copyright!!!
51
The MMS was designed as a practical clinical assessment of change in cognitive impairment in geriatric inpatients
Maximum Maximum Maximum Maximum ScoreScoreScoreScore
ScoreScoreScoreScore
Orientation
5 ( ) What is the (year)(season)(date)(day)(month)?
5 ( ) Were are we (state)(county)(town)(hospital)(floor)
Registration
3 ( ) Name 3 objects: 1 second to say each. Then ask the patient all 3 after you have said them. Give 1 point for each correct answer. Then repeat them until he learns all 3. Count trials and record trials
Attention and Calculation
5 ( ) Serial 7’s. 1 point for each correct. Stop after 5 answers. Alternatively spell “world” backwards.
Recall
3 ( ) Ask for the 3 objects repeated above. Give 1 point for each correct answer
Language
9 ( ) Name a pencil and watch (2 points); Repeat the following “No ifs, ands or buts”(1 point)Follow a 3 stage comment: Take a paper in your right hand, fold it in half, and put it on the floor (3 points)Read and obey the following: CLOSE YOUR EYES ( 1 point) Write a sentence (1 point)Copy design (1 point)
30 ( ) Total score
ASSESS level of consciousness (alert, drowsy, stupor, coma)
52

Orientation
1. As for the date. Then ask specifically for parts omitted. e.g., “Can you also tell me what season it is?” One point for each correct.
2. As in turn “can You tell me the name of this hospital? (town, county, etc.). One point for each correct
Registration
Ask the patient if you may test his memory. Then say the names of 3 unrelated objects, clearly and slowly, about one second for each. After you have said all 3, ask him to repeat them. This first repetition determines his score (0-3) but keep saying them until he can repeat all 3, up to 6 trials. If he does not eventually learn all 3, recall cannot be meaningfully tested.
Attention and Calculation
Ask the patient to begin with 100 and count backwards by 7. Stop after 5 substractions (93, 86, 79, 72, 65). Score the total number of correct answers. If the patient cannot or will not perform this task, ask him to spell the word “world” backwards. The score is the number of letters in correct order. E.g. dlrow=5, dlorw=3.
Recall
Ask the patient if he can recall the 3 words you previously asked him to remember. Score 0-3
53
Naming: Show the patient a wrist watch and ask him what it is. Repeat for pencil. Score 0-2
Repetition: Ask the patient to repeat the sentence after you. Allow only one trial. Score 0 or 1
3-Stage Command: Give the patient a piece of plain blank paper and repeat the command. Score 1 point for each part correctly executed.
Reading: On a blank piece of paper print the sentence “CLOSE YOUR EYES” in letters large enough for the patient to see clearly. Ask him to read it and do what it says. Score 1 point only if he actually closes his eyes.
Writing: Give the patient a blank piece of paper and ask him to write a sentence for you. Do not dictate a sentence, it is to be written spontaneously. It must contain a subject and verb and be sensible. Correct grammar and punctuation are not necessary.
Copying: On a clean piece of paper, draw intersecting pentagons, each side about 1 inch, and ask him to copy it exactly as it is. All 10 angles must be present and 2 must intersect to score 1 point. Tremor and rotation are ignored. 54
�Dementia: a global deterioration of intellect in clear consciousness
�Affective disorder, depressed type, with cognitive impairment: A sustained feeling of depression with an attitude of hopelessness, worthlessness or guilt accompanied by disturbance in orientation and memory which occurred afterthe onset of the depression
�Affective disorder, depressed type uncomplicated: A sustained feeling of depression with an attitude of hopelessness, worthlessness or guilt and with no notable cognitive defect.
�Affective disorder, manic type: A sustained feeling of elevated mood with an attitude of overconfidence or exaggerated self-importance.
�Schizophrenia: Either Schneider’s first rank symptoms in the absence of affective symptoms or the presence of a personality deterioration associated with thought disorder and emotional incongruence without first rank symptoms
55
Syndromic
Dementia syndrome of depression
Dementia is the clinical syndrome of mental life characterized by substantial global decline in cognitive function that is not attributable to alteration in consciousness
�The clinical syndrome of dementia
YES NO
�The clinical syndrome of dementia attributable to “organic” brain disease�Dementia carries the implication, the presumption of progression
Jaspers/Lewis/McHugh/Folstein An appeal to a presumed etiology
Roth

Sample A Sample B
� 69 patients chosenspecifically as clear examples of clinical conditions
� Private psychiatric hospital
� 29-dementia syndromes due to a variety of brain diseases◦ 10-depression with cognitive impairment
◦ 30-depression, uncomplicated
� 63-normal subjects◦ Senior citizens center
◦ A retirement apartment complex
� 137 consecutive admissions to a private psychiatric hospital
57
DiagnosisDiagnosisDiagnosisDiagnosis AgeAgeAgeAge MMSMMSMMSMMS PPPP
X SD Range
Dementia 80.8 9.6 5.8 0-22 <.001
Depression with cognitive impairment
74.5 19.0 6.6 9-27 <.001
Affective DisorderDepressed
49.8 25.1 5.4 8-30 <.001
Normal 73.9 27.6 1.7 24-30
58
DiagnosisDiagnosisDiagnosisDiagnosis AgeAgeAgeAge MMSMMSMMSMMS
X SD Range
Dementia 74.4 12.2 6.7 1-22
Depression 50.7 25.9 4.2 9-30
Mania 39.5 26.6 3.5 20-30
Schizophrenia 44.6 24.6 6.6 1-30
Personality disorder with drug abuse
34.3 26.8 2.5 19-30
Neurosis 25.6 27.6 2.4 21-30
59
Concurrent validity was determined by correlating MMS scores with WAIS scores in a group of patients selected from Sample A and B because they had both a MMS and WAIS in the same week.
MMS and WAIS Verbal: Pearson r=0.776, p<0.0001
MMS and WAIS Performance: Pearson r=0.660 P<0.001
60

61
Mental state
Cognitive Dep, Hallu, Del
“Mini-Mental State”A practical method for grading the cognitive
State of patients for the clinician
Numerical scoring
•Folstein MF•Folstein SE•McHugh PRJ Psychiatr Res 1975
For clinical setting, not community
Just, cognitive state
•Quick•Easy to use•Acceptable (patients, testers)•Valid•Reliable
� The test was designed for use by clinicians who appreciate the need for gaining cooperation and maintaining a relationship with the subject that is supportive rather than confrontational
� When patients refuse, the clinician often has not gained the patient’s cooperation and should try again after a suitable delay
62
63
questionnaire
and blank paper
a pencil
� 3 sections to the test:1. Orientation – a traditional but poorly defined domain
2. Registration - the essential screener itemsattention and recall
3. Language comprehension –and expression
64
a diagnostic and management aid for clinicians and families

� The score is the number correct.Administer the items without regard to the many possible reasons for failure: e.g. deafness, blindness, paralysis, language fluency…23/30 23/28 23/26
YES NO
� Serial 7’s v WORLD:� The 7’s items are more difficult
� The 2 itms are not comparable
� My practice is only to administer 7’s unless the patient absolutely refuses to try
� “No ifs ands or buts”: was intended to be a series of short words of low probability of occuring together in a sentence!!
65
The range of scores is appropriate forinpatientinpatientinpatientinpatient or outpatientoutpatientoutpatientoutpatient practice
66
� MMS score is NOT:� A diagnosis, merely a dimension of cognitive impairment
� A measure of deterioration unless repeated over time
� A direct measure of defective brain structure “organicity” although it correlates with severity of pathological lesion
� A direct measure of disability or competence although it is correlated with disability measure
67
� Several variations have been created for particular purposes
� MMS is available in many translations of uncertain accuracy
� Therefore, it is important to specify the version!
68

� Age and education produce remarkable similar results across cultures
� I don’t know the meaning of scores in stone age cultures
69
The individual errors can indicate a syndrome
NO registrationNO attention/calculationNO recallNO copying....
70
Even when correctly administered and scored, the MMS has several limitation of sensitivity and specificity
�Age�Education�Cultural context�Diagnoses:
� Frontal subcortical conditions (e.g. Parkinson dis.� Lifelong impairment� Delirium� Depression� Schizophrenia
71 72
MMS
Other instruments
Increasing specificity
Bya complete mental state examination also adds time and requires
specialistic knowledge
Increasing sensitivityBy adding:
DSTCDT
Also adds time and requires additional equipment

� A collection of traditional items
� To grade the cognitive state (NO dementia)
� Practical
� NO cut-points, numbers for sensitivities/sensibilities
� NO general population studies mentioned
73 74
75
שעון נעשה שימוש למדידת הזמן מזה אלפי שניםב
שעון חול -8000 BC
מצרים העתיקה
יוון
שעון שמשרומא
0
ימי הביניים
2020
שעון מחוגים
שעון דיגיטלי
76
השעות
AMPM
הדקות
השניות
מחוג קטןמחוג גדול

:צריך להיות מסוגלשהתפתח באורח תקין כל ילד , לערך 15בגיל
לומר את השעה בשעון שלו או של אדם אחר�
להעתיק שעון�
לצייר שעון מהזיכרון ולהיות מסוגל לסמן כל מיני שעות �שמתבקש
77
מי שלא התפתח באופן תקיןלהיות פגועים אצל אלה עלולים
78
מסיבות רפואיות
)פיגור(פגיעה מוחית •
הפרעה נפשית•
פגיעה ממוקדת •ביכולת לימודית
סביבתיות-מסיבות תרבותיות
אי שימוש באוכלוסיה•אי לימוד•
הרפואה משתמשת בעקרונות ידיעת הזמן הכרונולוגי �
שנים לשם איתור של סימנים + 100-בעזרת שעון מזה כ
.קוגניטיבית מוחית/אשר נוכחותם מעידה על פגיעה אורגנית
הינו השם הניתן למכלול שיטות (clock test)מבחן השעון �
ניתן להבחין בכל מיני סוגים של , אך. הבדיקה הנהוגות.ולכל אחד ואריאנטים משלו, בדיקה
79
Clock Tests
Clock reading test
Clock setting testClock copying test
Clock drawing testCDT
� Clock drawing has been anecdotally in the neurology and psychology literature (Critchley, 1966; Albert and Kaplan, 1981;Goodglass & Kaplan, 1983, Boston Aphasia Battery; Soffer, 1984, The clock test in the differentiation of organic brain syndrome and schizophrenia. Dissertation abstract. Case Western Reserve University).
� In the clinical setting, the test could potentially be a simple and practical one that adds to the ability to screen for organic mental disorder and to monitor changes in cognitive status.
� To our knowledge, this is the first attempt to systematically validate the “clock test” and establish a scoring system to evaluate the qualitative aspects of clock-drawing 80

� Origins:
◦ Based on the clinical experienceclinical experienceclinical experienceclinical experience of a geriatric psychiatry service
◦ A hierarchical classification system hierarchical classification system hierarchical classification system hierarchical classification system of errors in clock-drawing was developed
◦ This includes a range of defects range of defects range of defects range of defects in:
� Visuospatial abilities
� Abstract thinking
� Neuropsychiatric manifestations of brain dysfunction such as perseveration, and right-left confusion
81
� Method◦ 75 persons < 65 years, no gross visual impairment◦ Inpatients and outpatients◦ Groups: organic mental disorder, major affective disorder; “normals” (from Family Practice Unit)◦ No attempt to use these groupings to establish the diagnostic usefulness of the clock test◦ Measures: MMSE, SMSQ, GDS
� Conclusion: Clock drawing appears to be a practical test which can be useful for clinicians as a screen for cognitive impairment in old age and possible as a marker of change marker of change marker of change marker of change in cognitive status
82
� Cognitive functions tapped:◦ Comprehension◦ Abstract thinking◦ Planning◦ Visual memory◦ Visuo-spatial abilities◦ Motivation◦ Concentration◦ Inhibition of stimulus pull to 10
� In all sensitivtity/specificity 85%� Correlations with MMSE and other cognitive tests – high� High inter-rater and test-retest reliability� Positive predictive value, sensitive to cognitive change� Simple is better
83
IdealIdealIdealIdeal, however in conjunction with:*MMSE, *verbal fluency test, *informant reports
84
MCI
AD, MID, Huntington,
etc.
DepressionSchizophrenia
Dementia
Organic Mental Disorder
Cognitive state
Tests of sensorium
Others
Others
•ROC curves•Cut-offs•Cut-points•Sensitivities•specificities
Shulman
Folstein
Roth
2012
2000
1990
1980
1970
1950

85
“Pathological” (errors, qualitative)
“Physiological” (process, [Kaplan, 1980] quantitative)
hierarchical non-hierarchicalMixed
(with errors)
“pure”
קרובבאמצע
86
Graphical difficulties
Stimulus bound response
Conceptual deficits
Spatial/planningdeficits
Perseveration
Size of the clock
� Critical clock-drawing errors for dementia screening
� Subjects > 5 years of education
87
Incorrect time setting No hands Missing numbers
Substitution Number repetitionRefusal to attempt clock drawing
� For dementia screening
� Population-based sample (CSHA)
� 356 participants (80 with dementia, 246 healthy controls
� 1 error=cut-off score, sensitivity 81%, specificity 68%clock
88

� Hierarchy of errors in dementia1. “Perfect”2. Minor visuospatial errors
a) Mildly impaired spacing of times
b) Draws times outside circle
c) Turns page – some numbers appear upside down
d) Draws in lines (spokes) to orient spacing
3. Innaccurate represntation of 10 after 11 when visuospatial organization is perfect or shows only minor deviations
4. Moderate visuospatial disorganization of times such that accurate denotation of 10 after 11 is impossible
a) Moderately poor spacing
b) Omits numbers
c) Perseveration
d) Right-left reversal
e) Dysgraphia
5. Severe level of disorganization as described in 46. No reasonable representation of a clock
a) Exclude severe depression or other psychotic states
b) No attempt at all
c) No semblance of a clock at all
d) Writes a word or name
89
� CDT-MIA is a:
◦ 4 step
◦ 20 item instrument
◦ Max score = 33
◦ Emphasizes differential scoring of
◦ Scoring
� Contour [max = 3]
� Numbers [max = 15]
� Hands [max = 12]
� Center [max = 3]
� Total [max = 33]
90
The higher the better
91 92

93 94
95
Freedman et alFree-drawn clock
(1994)
Paganini-Hill et al(2001)
Royall et alCLOX 1(1998)
Manos and WuPredrawn major
circle(1994)
CDT-MIA
CDT-MIA objectives
Conceptualized for the evaluation of early dementia and MCI in a specialized outpatient setting
� Page 1 – Bland sheet of paper (A4)
� Page 2 – Sheet of paper (A4) with a predrawn circle (8.3 cm adapted from Paganini-Hill et al (2000)
� Page 3 – Sheet of paper (A4), with a predrawn circle (11.3 cm diameter, adapted from Manos and Wu (1994), with designated place for the hours 12, 3, 6, and 9.
� Paganini-Hill et al’s template (2001)
� Ruler
� Pencil with eraser to be used by the participant
96
11.38.3
Page 1 Page 2 Page3

� Step Step Step Step 1 1 1 1 – Ask the participant to draw a clock face on page 1. The only initial instruction is “I would like you to draw a clock face”. Once the participant has finished drawing a contour, say “Thank you, this is enough. I would like you to move to the next page”
� Step Step Step Step 2 2 2 2 – Provide the participant with page 2 and say “This is the contour of a clock face. Please put in all the numbers”.
� Step Step Step Step 3333 – When the participant has done this, say “Now set the hands to 11 and 10 minutes”.
� Step Step Step Step 4444 – Provide the participant with page 3 and say “In this clock face please draw the hands at 6 and 45 minutes, without adding, the numbers themselves”. At this step, the patient is not requested to record numbers. This should be clarified again to the patient only if he or she asks if he or she should write down the numbers or if he or she begins to record numbers.
97
�NoteNoteNoteNote
� Successful completion of each step is not a prerequisite to moving to the next step, and each should be presented to the patient consecutively
� No time limit is imposed
� Erasures are permitted
� Best performance is scored
98
99
Actual score Max score___________ ___________
1. Acceptable contour drawn
2. Contour is not too small or too large
3. Contour is not overdrawn or reproduced repeatedly
Contour
01 [1]
01 [1]
01 [1]
4. Starting numbers
5. Direction of numbers
6. Only numbers 1-12
7. Only Arabic number representation or only Roman numerals should be used
8. Numbers are written in correct order
9. Tilt of numbers
100
Actual score Max score___________ ___________
Numbers
0123 [1]
01 [1]
01 [1]
01 [1]
01 [1]
01 [1]

10. 10. Numbers in correct position
11. All 12 numbers are located inside the contour
12. Position of numbers respect to contour
101
Actual score Max score___________ ___________
Numbers
0123 [3]
01 [1]
0123 [3]
Paganini-Hill et al’s template
Using a ruler
13. Clock has 2 hands or marks
14. Hour target indicated by hand/mark
15. Minute target indicated by hand/mark
16. Hands in correct proportion on both clocks
17. No superfluous markings
18. Hands are joined or within 12mm of joining
19. Hands set at 6:45
102
Actual score Max score___________ ___________
Hands
01 [1]
012 [2]
0123 [3]
01 [1]
01 [1]
01 [1]
0123 [3]
20. Clock has a center
103
Actual score Max score___________ ___________
Center
0123 [3]
Paganini-Hill et al’s template
� Dementia v non-dementia (mostly depressive and anxiety)
� Mean MMSE: dementia 18.5 v non MMSE = 28
� Cut-point 23; sensitivity 91%; specificity 80%
� High correlations with Freedman and Shulman’s clocks, moderate with MMSE
� Contributes to dementia diagnosis◦ Item 15 – minute target number indicated
◦ Item 16 – hands in correct proportion
◦ Item 19 – hands indicate 6:45
◦ Item 10 – numbers in correct position
� High internal consistency
� High inter-rater reliability104

� Participants with: dementia, MCI, not cognitively impaired (NCI)
� Mean MMSE: 25.55 v 26.50 v 28.26, respectively
� Mean CDT-MIA: 20.50 v 24.57 v 26.63, respectively
� Mean CAMCOG-R: 76.9 v 85.53 v 94.14, respectively
� CDT-MIA could discriminate dementia from NCI and dementia from MCI
� CDT MIA failed to appropriately discriminate MCI from NCI
� CDT-MIA/MMSE combined could discriminate dementia from MCI, dementia from NCI, MCI from NCI
� Best diagnostic accuracy obtained with CAMCOG-R
105
106
3=84.7%
1=27..7%
107
108

109
110
111
3/3
8/15
9/12
3/3
The Montreal Cognitive Assessment (MoCA):
A brief screening tool for mild cognitive impairment
112

� Short term memory (5 words)
� Visuospatial (CDT)
� Executive function
� trails B
� verbal fluency
� abstraction
� Attention
� Language – naming/fluency
� Orientation
113
Nasreddine et al (2005)
114
•Psychiatrist 1’ - Anamnesis (subject/relative)
- Status
- Mini-Mental State Examination (MMSE)
- Clock Drawing Test (CDT)
•Geriatrician - Anamnesis (subject/relative_
- Status
- Auxiliary tests (blood, imaging)
•Social Worker - Anamnesis (subject/relative)
- Status
•Nurse - Basic activities of daily living
- Instrumental Activities of Daily Living (IADL)
•Psychiatrist 2’ - Anamnesis (subject/relative)
- Status
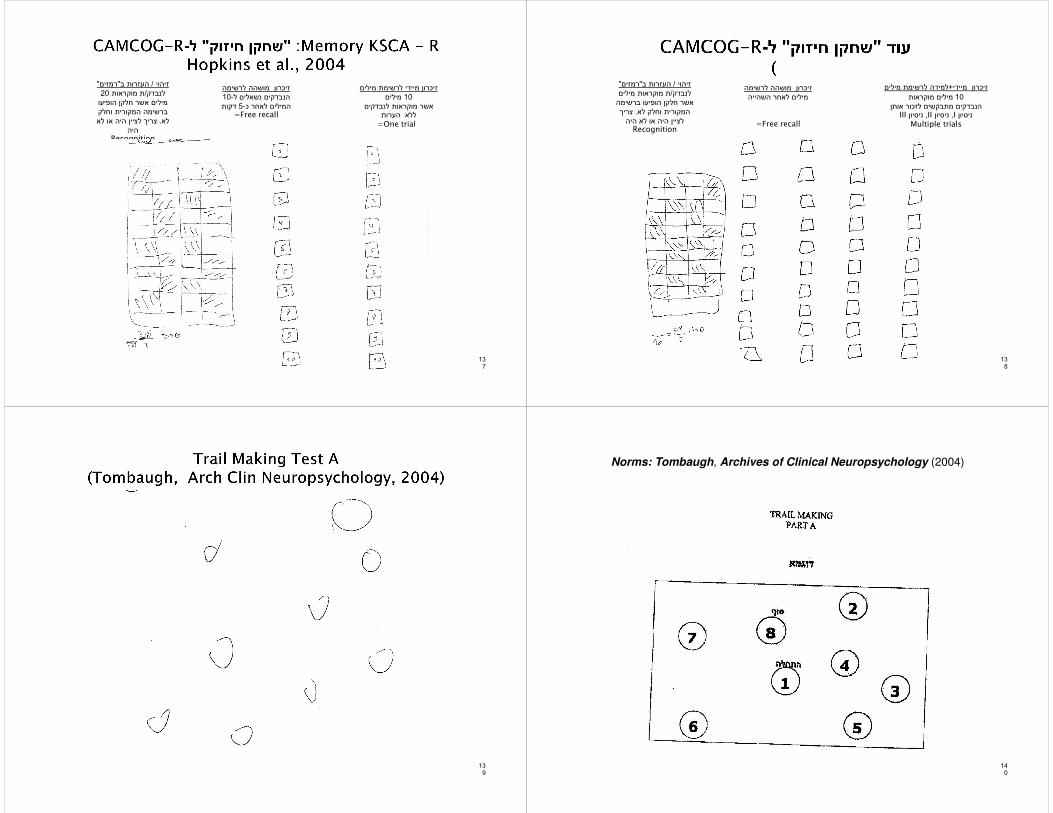
- KSCA-R memory 10 items
- Cambridge Cognitive Examination- Revised (CAMCOG-R)
- TMT- A
•Neuropsychologist - Anamnesis (subject/relative)
- Wechsler Adult Intelligence Scale – III (WAIS-III)
- Wechsler Memory Scale III (WMS-III)
- Rey-Auditory Verbal Learning Test (Rey-AVLT)
- Trail Making A and B
- Rey-Osterrieth Complex Figure
- Hooper
- Naming test
- Word Fluency Test
Clinical Dementia Rating
(CDR)

באותם המקרים בהם בבדיקת הפסיכיאטר קיימת
מוסר /עם או ללא אישור של קרוב, תלונה קוגניטיבית
עם , והתרשמות בבדיקה מירידה קוגניטיבית, מידע
אשר אינן מגיעות בחומרתן , אם ללא ירידה תפקודית
לכדי אבחנה של דמנציה או שקיים חשד מסוים .לקיומה
ביצוע בדיקות , השלמת הסבב(שיתוף פעולה �
)העזר
הפרעה נפשית�
שנים בארץ�
שפה�
קרוא וכתוב�
מוטוריקה/שמיעה/ראייה�
סיבות לא רפואיות לבדיקה�
)ועוד, חוסר שינה; מצב לאחר מחלה גופנית(שונות �
118
119
קמקוג
+
TMT-A
10 –words-learning
Memory – KSCA+ +
+� The Cambridge examination for mental disorders of the elderly (CAMDEX)
� The CAMDEX is a standardized, structured interview and examination for diagnosing common mental disorder in later life, with special reference to the dementias
Authors Roth et al
First edition 1988
Second edition 1998 = CAMDEX-R
120

Section A – Interview with patient/subject
Section B – Cognitive examination – CAMCOG
Section C – Interviewer observations
Section D – Physical examination
Section E – Investigations
Section F – List of current medications
Section G – Additional information
Section H – Interview with patient’s relative or other informant
Section I – Additional information from informant
121
122
123
Incorporated scales� Dementia Scale (Blessed et al, 1968)
� Ischaemia Score (Hachinski et al., 1975)
� Mini-Mental State Examination (Folstein et al, 1975)
� Abbreviated Mental Test (Hodkinson, 1972)
� CAMDEX operational diagnostic criteria◦ Primary and secondary psychiatric diagnoses◦ Clinical estimate of severity of dementia – if present◦ Clinical estimate of severity of depressive symptoms – if present◦ Other medical diagnoses◦ Items from CAMDEX-R for arriving at various diagnostic criteria and diagnostic scales
� DSM-4 – Delirium, DAT, VD, MDD� ICD – 10 – Dementia, dementia in AD, VD, MID, delirium, depressive episode, (mild, moderate, severe, with or without psychotic symptoms, somatic syndrome)
� Dementia with Lewy bodies (DLB) (McKeith et al, 1996)� Dementia of frontal type (Gregory and Hodges, 1993)� Frontotemporal dementia (The Lund and Manchester groups, 1994)
� Items relevant to the NINCDS-ADRDA criteria for Alzheimer’s disease (McKhann et al, 1984) and the NINDS-AIREN criteria for vascular dementia (Roman et al, 1995)
124

125
� The CAMCOG is a concise neuropsychological test for the assessment of cognitive impairment in elderly people
� It was designed specifically to assist in the diagnosis of dementia at an early stage
� CAMCOG assesses a broad range of cognitive functions, as is required for the diagnosis of dementia
� It minimizes floor and ceiling effects by covering a range of item difficulty
שאלון הקמקוג�
ספרון הקמקוג�
עפרון�
)עם מחוג שניות למדידת זמן(שעון יד �
)4A(דף נייר ריק �
מעטפה�
מטבעות בעלות ערך שונה 2: מטבעות�
�[Sport timer]
126
127
� Orientation
� Language
� Memory
� Attention/Calculation
� Praxis
� Abstract thinking
� Perception
128
Performance and normative values established in a large elderly
population sample (Williams et al., 2003)
CAMCOG
Validated in various patient groups
Translated into several languages: (Hebrew – Heinik, Werner et al., 1999)Research
Harmonized between seven European countries (Verhey et al., 2003)

Cognitive Cognitive Cognitive Cognitive functionfunctionfunctionfunction
Brief description of itemBrief description of itemBrief description of itemBrief description of item Maximum Maximum Maximum Maximum scorescorescorescore
Orientation =Day + Date + Month + Year + Season + County + Town + Streets + Floor + Place
10
Language = Nod + Touch + Ceiling +Tap + Hotel + Village + Radio + Read 1 + Read 2COMPREHENSIONHammer + Chemist + Bridge + Opinion + Name objects + Animals + Ifs + AddressEXPRESSION
9
30
21
Memory = First World War + Second World War+ German + Russia + Mae + Flyer = Remote + Queen + Heir + Prime Minister + News = Recent+ Recall pictures + Recognize pictures = Learning+ Recall address
64 2717
Attention / Calculation
= Count backwards + Serial sevens +Calculation 1 + Calculation 2
9
Praxis = Pentagon + Spiral + House + Clock + Envelope + Wave + Cut + Teeth
12
Abstract thinking
= Similarities 1 + Similarities 2 + Similarities 3 + Similarities 4 8
Perception = Faces + Views + Recognize person 9
Total 105 129
130
� DSM-III (1980)
� DSM-III-R (1987)
� ICD-10 draft (1988)
� CAMDEX operational criteria for dementia
No reference to No reference to No reference to No reference to “executive “executive “executive “executive dysfunction"dysfunction"dysfunction"dysfunction"
131
� Fluency item (animals in 1 minute) part of language functions
� Similarities item abstraction
132
� “executive function” increasingly seen as having at least a considerable degree of face validity and communication value (Tranel et al., 1994)
� Could be separated from the other specific cognitive domains (e.g., memory, language, praxis) used traditionally to assess patients (Royall et al., 2002)
� Added as Executive Control Function (ECF) to DSM-IV criteria for dementia (1994)
� ECF: a report from the Committee on Research of the American Neuropsychaitric Association (Royall et al., 2002)

133
narrower narrower narrower narrower sensesensesensesense
wider sense
In a wider sense, decision making, judgment and even creativity and artistic expression (Tranel et al., 1994)
•To describe a variety of high level cognitive processes including planning, organization, abstraction, categorization, initiation, reasoning, mental flexibility, sequencing, and the allocation of attentional resources [CAMCOG, (1998)]
•Cognitive processes that orchestrate complex goal-directed activities [Royall et al., 1996]
134
ECFECFECFECF
Vital to human autonomy Determinant of
problem behavior
Determinant of disability
in neuropsychiatric disorders
135
Executive Function Score (EFS)
Word List Generation [WLG]
Naming as many different animals in
1 minute as possible
Similarities [SIM]Apple-banana
Shirt-dressTable-chair
plant-animal
Ideational Fluency [IF]
How many different uses for a bottle in 90 seconds
Visual Reasoning [VR]
“Which of these objects
below should go in the
empty box?”
WLG=max 6 pts
SIM=max 8 pts
IF=max 8 pts
pts6 VR=max
Total EFS=max 28 pts
A B C D E F 136
� WLG = assesses initiation and categorization
� SIM = assess abstraction
� IF = assesses initiation and mental flexibility in the verbal domain
� VR = a non-verbal assessment of sequencing, categorization and abstraction
137
זיכרון מיידי לרשימת מילים
מילים 10
אשר מוקראות לנבדקים ללא הערות
=One trial
זיכרון מושהה לרשימה
10-הנבדקים נשאלים ל
דקות 5-המילים לאחר כ=Free recall
"רמזים"העזרות ב/ זיהוי
20ת מוקראות /לנבדק
מילים אשר חלקן הופיעו
ברשימה המקורית וחלק
צריך לציין היה או לא . לא
היהRecognition
138
למידה לרשימת מילים+מיידיזיכרון
מילים מוקראות 10
הנבדקים מתבקשים לזכור אותןIIIניסיון , IIניסיון , Iניסיון
Multiple trials
זיכרון מושהה לרשימה
מילים לאחר השהייה
=Free recall
"רמזים"העזרות ב/ זיהוי
ת מוקראות מילים /לנבדק
אשר חלקן הופיעו ברשימה
צריך . המקורית וחלק לא
לציין היה או לא היהRecognition
139
140
Norms: Tombaugh, Archives of Clinical Neuropsychology (2004)

141
Norms: Tombaugh, Archives of Clinical Neuropsychology (2004)
142
CAMCOG-R total score
and Sub-scores
גיל
שנות לימוד
מגדר
משלוח
/ יד
מעמד חברתי
ידיעת שפה
תרבות
143
Max value Mean (SD) Median Percent
obtaining
maximum
Range
Orientation 10 9.2(1.0) 10 51 3-10
Language 30 24.9 (2.6) 25 0 9-29
Memory 27 20.7(3.6) 21 0 4-26
Attention 7 5.1(1.9) 5 31 0-7
Praxis 12 10.1(2.0) 10 27 0-12
Calculation 2 1.8(0.4) 2 80 0-2
Abstract
thinking
8 5.2(2.3) 5 20 0-8
Perception 10* 7.8(1.8) 8 16 1-10
Total 106*144
CAMCOG-RTotal score
andsubscores
(UK)נורמות בקהילה
ממוצע: כ הניקוד"סה�Mean (SD) median range
•Sex•Age•Education•Social class
subscale-הניקוד ב�89-85 84-80 79-77גילאים
•Orientation•Language•memory
subscores-הניקוד ב�60
ממצאים בקליניקהsubscales+ כ הניקוד "סה
Non demented Minimal dementia Mild dementia9.73 (0.57) 9.03(0.36) 7.19(0.83)
•Orientation •Language•memory
Cutpoints/ sensitivity/specificityCutpoints/ sensitivity/specificityCutpoints/ sensitivity/specificityCutpoints/ sensitivity/specificity
79/80 90 8880/81 93 8781/82 93 86

145
0=impaired under 16th centile (-1SD) and under 2.5th centile (-2SD)
1=Not impaired
16th centile (-1 SD) 2.5th centile (-2 SD)
0/8=0 9/10=1 0/6=0 7/10=1
Orientation
Language comprehension
Language expression
Remote memory
Recent memory
Attention/calculation
Praxis
Abstract thinking
Perception
146
Cutoffs for < 69
Orientation (0/8=0) (9/10=1)
Cutoffs for 70-74
Cutoffs for 75-79
Cutoffs for 80-84
Cutoffs for 85-89
Orientation (0/7=0) (8/10=1)
Cutoffs for 90+
Orientation (0/6=0) (7/10=1)147 148
דמוגרפים-נתונים סוציו
81בן •
יליד מזרח אירופה•
)רוסיה(ניצול שואה •
20בארץ מגיל •
שנות לימוד 12השכלה •
מקצוע הדרכתי•
גר בביתו, 3+נ•
עבר פסיכיאטרי
נשלל
במשפחה
ADאולי , 62אמו נפטרה בגיל •
הפסיקה להכיר את הילדים•
שנים אחדות לפני 82.אחותו נפטרה בגיל •
מותה הייתה לא צלולה
אחות נוספת סבלה גם מירידה קוגניטיבית •
שנתיים שלוש לפני מותה
ובגיל 80בגיל ADאחים חלו ב 2עוד •
ADאחים נפטרו ללא 2. 84
תולדות חיים
עבודה במשרד ממשלתי
קידום
65יציאה לפנסיה בגיל
4עד , עבודה בנגרות
שנים לפני הבדיקה כאן
תרופות/ רקע גופני
וסקולאריים-גורמי סיכון קרדיו•
.ד.ל יתר•
כולסטרול•
,MIמצב לאחר , מחלת לב איסכמית•
)שנים קודם CABG )4ולאחר •
סכרת עם פגיעה באברי מטרה •
היפותירואידיזם•
שנים קודם TIA 2חשד ל•
ראייה סבירות/ שמיעה •
תרופות כולל סימבלטה 12•
•CT חדר שלישי ולטרליים מורחבים: מוח ,
: US; צ"מוקדי צפיפות נמוכה בגרעיני בסיס דו
של הקרוטידים 50%צ עד "היצרות דו

149
מחלה נוכחית
לאחר ניתוח מעקפים תלונה •
על ירידה קוגניטיבית =30/30MMSE
כ ירידה הדרגתית של "אח •
") לא"הוא , "כן"אשתו (הזיכרון
חודשים נפילה מסולם 4לפני •
ללא פגיעת (שבר בחוליה
מאז גם הוא מתלונן על ) ראש
אי , ירידה בתפקוד, קוגניציה
ישן , כאבים, שיווי משקלבמשך היום פחות טוב בלילה
תלונות
קושי בשליפת מילים•
גם של , שוכח שמות•
דברים , שוכח תאריכים,חברים
שצריך לעשות
לא חוזר על אותו סיפור •
פעמייםADמודאג שיש לו •
גופני/סטאטוס נפשי
מידי פעם , ללא ממצא חריג נפשי�חסרה מילה
28/30 MMSE ,ציור שעון תקין
,בדיקה גופנית ללא ממצא חריג�
הליכה עם הליכון
תפקוד
פעיל בעיקר במסגרת ; עצמאי•
הבית
עובד בגינה, נוהג•
אחראי על התרופות•
מטפל בענייניו הכספיים•
הלבשה /עזרה מסוימת ברחצה•
)מאז הנפילה(
נטלה על "מאז הנפילה אשתו •"עצמה חלק מהדברים
� MMSE� CDT-MIA� CAMCOG-R: Total◦ Orientation◦ LanguageComprehensionExpression
� Memory◦ Remote◦ Recent◦ Learning
◦ EFS
◦ TMT-A◦ Memory – KSCA-R
150
combined
• Attention/calculation
• Praxis
• Abstract thinking
• Perception
•Incidental
•Intentional
•Animals
•Similarities
•Ideational fluency•Visual reasoning
•Immediate word recall•Delayed word recall•Word recognition
� MMSE=29/30
� CDT-MIA=29/33
� CAMCOG-R: Total 91/103
151
Combined=58/63 (cutoff 51/63 Dementia v NDsensitivity 77.3%, specificity 75%)
Age 80-84Education L HMen5th 10th
25th 75th 80 89 83 91
152
SD 1- הנורמה 80-84גיל
Orientation 10/10 0/8=0 9/10=1
Language comprehension 9/9 0/6=0 7/9=1
Language expression 18/21 0/13=0 14/21=1
Remote memory 5/6 0/2=0 3/6=1
Recent memory 4/4 0/2=0 ¾=1
Learning memory 13/17 0/9=0 10/17=1
Attention/calculation 8/9 0/2=0 3/8=1
Praxis 12/12 0/7=0 8/12=1
Abstract thinking 7/8 0/2=0 3/8=1
Perception 5/9 0/3=0 4/8=1
מין, השכלה, בנורמה לפי גיל CAMCOGסך הכל ממצא
תחום-ללא פגיעה באף תת :ממצא

� EFS = 20/28 (cutoff 18= Dementia vs NDSensitivity 97%Specificity 56%ROC 0.844)
� TMT-A = ללא טעויות שניות 78 (20th to 10th percentile)� Memory – KSCA-R
153
----1111SDSDSDSD בנורמה
Immediate 4/10 0/3=0 4/10=1
Delayed 2/10 0000////2222====0000 3/10=1
Recognition 7.5/10 0.6=0 7/10=1
1SD delayed-רק לימוד רשימת מילים : ממצא
Immediate ו-recognition בנורמה
תיאור
מילולי
ציון בסקאלה
10הממוצע שבה
Zציון Tציון אחוזונים ציון בסקאלה שבה
100הממוצע
לקוי 0-3 2.8--2.1- 13-29 0.02-2 45-69
גבולי 4-5 2--1.4- 30-36 2-8 70-79
ממוצע
נמוך
6-7 1.3--0.7- 37-42 9-23 80-89
ממוצע 8-11 0.5--0.6 43-56 25-73 90-109
ממוצע
גבוה
12-13 0.6-1.2 57-62 75-90 110-119
מעולה 14-15 1.3-1.9 63-69 91-97 120-129
מעולה
במיוחד
16-20 2-2.8 70-86 98-100 130-155
*WMS
תת מבחנים של *
WAIS
*TMT
*Naming
*Fluency
*RAVLT
RCF* WAIS כל*
האינדקסים
FSIQ*
VIQ*
PIQ*
הוא היה במצב רוח טוב ולא ניכר : התנהגות במהלך האבחוןהוא לא התקשה לדווח על ההיסטוריה . שהאבחון מעייף אותו
הוא היה . היה צלול ושיתף פעולה באופן מלא, הרפואית בעצמומודע לקשיים שעלו במהלך האבחון
: סיכום
התפקוד האינטלקטואלי בתחום המעולה עם פער משמעותי בין �תפקוד מעולה במיוחד בתחום הויזואלי לבין תפקוד ממוצע גבוה
מוטורית-ככל הנראה עקב האטה פסיכו. בתחום הביצועי
ניכר קושי במבחן זיכרון לחומר מילולי נטול הקשר עם שיפור �משמעותי ביותר כאשר המידע מוצג בהקשר סיפורי
לא נמצא קושי בזיכרון חזותי�
שיום תמונות היה תקין�
שליפת מילים לפי אותיות הייתה נמוכה מהממוצע וכך גם מדד של �אך הביצוע היה בתחום התקין לגיל, מוטורי-קשב גרפו
דפוס הבצועים מצביע על ליקוי ממוקד בזיכרון לרשימת מילים �MCI 155שמתאים ל

157
Total assessments
N=286
Others
NCI
“strict”
N=75
RAVLT 8 1.3שווה או גדול מ-
WMS 2LM 6 -שווה או גדול מ
RCF delayed 10-שווה או גדול מ
NCI
Or
“normative”
sample
NCI
“clinical”
N=98
=
(z)-)ציון מתוקנן(
(percentile/z)
Mean SDMean SDMean SDMean SD MedianMedianMedianMedian RangeRangeRangeRange ModeModeModeMode
Age 75.08 6.37 76 61-88 83
Education 13.09 3.13 12 6-23 12
Gender (F%) 60
Aliyah 11.93 9.37 14 0-34 0
Years in Israel 63.14 9.49 63 44-84 63
159
Cognitive characteristics of an NCI Israeli Clinical Sample
29

2005200520052005 2007200720072007 2008200820082008 2009200920092009
MMSE 29 26 25 21
CDT-MIA 27 26 26 18
P15 P15





























