Embed Size (px)
Citation preview

Mitchell Wilson, MDMitchell Wilson, MDAssociate Professor of Medicine
Section Chief of Hospital MedicineDivision of General Medicine and Clinical Epidemiology
Department of MedicineUniversity of North Carolina School of Medicine
Co-Chair, SHM Non-Physician Provider Committee

PanelistsPanelists
Scarlett Blue, RNC, MSN, CNA
Ryan Genzink, PA-C
Jeanette Kalupa, MSN, APRN-BC, APNP

Working With Non Physician Working With Non Physician Practitioners: Risks, Benefits, Practitioners: Risks, Benefits,
Alternatives & IndicationsAlternatives & Indications

Learning ObjectivesLearning Objectives
Examine the potential disadvantages (risks) and advantages (benefits) of integrating PAs, NPs, and RN CCCs into hospitalist programs
Understand how skill mix can add valuevalue to hospitalist programs (alternatives)

Learning ObjectivesLearning Objectives
Determine if PAs, NPs, and RN CCCs are right for your practice (indications) by assessing opportunities & barriers
Perform a needs vs. barriers analysisDefine the factors critical to a
successful implementationLearn how to demonstrate ROI

1. Risks, Benefits, and Alternatives
2. Indications: Are PAs, NPs and RN CCCs Right For Us?
Panel Q & A (10 minutes)
3. Implementation: Critical Success Factors
Panel Q & A (10 minutes)
4. Return on Investment (and billing if we have time)
Panel Q & A (10 minutes)
Session OutlineSession Outline

Case StudyCase Study
Environment 250 bed suburban community non-teaching
hospital Open ICUs but not enough critical care
boarded MDs to staff patients Competitor hospitals within a 30 mile radius PAs successfully work with surgeons in case
study hospital NPs are in some of the PCP’s & cardiologist’s
offices and are well regarded

Case StudyCase Study
Hospitalist Program Structure Hospital employed, 18 months old Budgeted now for 8 physician FTE, 6 FTE currently:
• One dissatisfied doctor left one month ago citing excessive workload & slow recruiting
• 8th position open for 5 months 24/7 in-house, Code & Rapid Response Team (RRT) ED unassigned, many OBS patients Schedule
• 7 on/7 off block shift• Day (7am-7pm): 2 MDs• Night (7pm-7am): 1 MD

Case StudyCase Study
Programmatic issues: Ave. daily encounters/MD approx. 20,
sometimes more ICU with complex cases Admissions throughout the day due to ED
unassigned Delays in D/C’s & seeing patients, ALOS
increasing, case managers complaining Nurses complaining about hospitalist page
reply times Satisfaction scores not improving

Case StudyCase Study
Programmatic issues: Turning away patients from PCPs due to
census, acuity & workforce issues Cover one hospital, pressure to:
• Admit for more PCPs, specialists, including surgical co-management
• Consult on more inpatients• Cover hospitalist patients transferred to an
affiliated Skilled Nursing Facility Unable to attend committee meetings and no
QI/QA involvement

Case StudyCase Study
Culture One of the hospitalists worked with a PA/NP
in a practice before joining this one but it didn’t work out well
Another of the hospitalists just wants to hire someone—anyone—to make work life better so she can get out on-time (PAs will fix this)
Two of the other hospitalists, including the founding member, are in favor of trying a PA/NP and a third used to teach in a residency program before going private

Case StudyCase Study
Culture The program administrator worries the program will
collapse if another hospitalist leaves The CMO fears non-physicians may alienate referring
MDs The CNO is not a PA advocate due to some prior
nursing staff occurrences A couple of senior members of the medical staff have
never liked that the local practices work with PAs and NPs
The bulk of the medical staff are middle-aged or younger and express no firm objection

Partnering with NPPs in Hospitalist PracticesPartnering with NPPs in Hospitalist Practices
Identify the• Disadvantages and Advantages• Opportunities• Barriers
Perform a Needs-vs.-Barriers AnalysisPolling Question:Polling Question:
Is this case a “good-to-gogood-to-go” or “just-say-just-say-nono” to Partnering with NPPs?

Disadvantages(Risks)
NPPs in Hospital Medicine

Substituting for Residents: Substituting for Residents: Disadvantages of PAs and NPsDisadvantages of PAs and NPs
More expensive than residentsLoss of Medicare DME & IMEConflict with CMS cost reportsAcademic pay scales generally lower
than community competitionRole conflict: X vs YRedundancy?

Integrated Hospitalist Teams: Integrated Hospitalist Teams: Disadvantages of PAs and NPsDisadvantages of PAs and NPs
Stakeholder perceptions• PCPs• Referring physicians• Hospitalist group members• Hospital staff (Admin, Nursing, Ancillary)• Patients & family
Laws & Bylaws Physician supervision
• Especially for new grads Employment models & billing

Integrated Hospitalist Teams: Integrated Hospitalist Teams: Disadvantages of PAs and NPsDisadvantages of PAs and NPs
Will cost upwards of $80,000+ (plus benefits, recruitment, admin overhead, CME)
Medical liability for physician? ??Decreased “face time”?? Potential redundancy Competition?

Advantages(Benefits)
NPPs in Hospital Medicine

Silver et. al., Cawley et. al., Frick et. al., Jones et. al.
Substituting for Residents: Substituting for Residents: Advantages of PAs and NPsAdvantages of PAs and NPs
Greater consistency of ability More clinical experience Diminished supervision Better “systems” managers Enhanced efficiency Stronger staff affiliations Higher visibility and availability Improved continuity of care

Substituting for Residents: Substituting for Residents: Advantages of PAs and NPsAdvantages of PAs and NPs
Sometimes the one “constant”Not subject to RRC duty hour
restrictions!Can still serve as educators to
residents, nurses, and/or PAs & NPs in training
This is their career

Integrated Hospitalist Teams: Integrated Hospitalist Teams: Advantages of PAs and NPsAdvantages of PAs and NPs
Cost less than M.D. F.T.E. Manage the care of patients not requiring
direct physician care time Allows physician to:
• Focus on more difficult and complex cases• Provide access to services (program structure,
new business)• Participate in quality, safety & other hospital
initiatives• Still avail for PA/NP supervision & consultation• Share on-call time, cross-coverage• Colleague close at hand

Integrated Hospitalist Teams: Integrated Hospitalist Teams: Advantages of PAs and NPsAdvantages of PAs and NPs
Surge capacityProvide high-quality careFacilitate and coordinate care
processesEnhance efficiencyAugment practice productivityServe most specialties

Integrated Hospitalist Teams: Integrated Hospitalist Teams: Advantages of PAs and NPsAdvantages of PAs and NPs
Perform proceduresSpend more time with patients,
especially w.r.t. education, prevention, health maintenance
Interface with ancillary services and consultants & improves communication
Increase hospital staff satisfactionWrite prescriptionsMay lessen the liability risk

Integrated Hospitalist Teams: Integrated Hospitalist Teams: Advantages of PAs and NPsAdvantages of PAs and NPs
Services reimbursed by Medicare, Insurers
Makes a TEAM out of you and me!

Value-Added(Alternatives)
NPPs in Hospital Medicine

The Driver for PartneringThe Driver for Partnering
“Skill mix enables programs to deploy resources (physician and non-physician) in a way that matches skill set with skill need to optimize program performance and efficiency.”
--M.J. Wilson, M.D.

Cost Effective ModelCost Effective Model
Allows program to increase volume at less direct cost – PA and NP salaries & benefits less than that of the physician
Helps balance revenue versus expense with regard to:• Program mission• Payor mix• Patient population

Cost Effective ModelCost Effective Model
Promote uniformity & consistency of practice through the use of practice guidelines
Integrated teams maintain outcomes• Studies show reduced LOS, improved communication and
collaboration, and improved hospital profit without altering readmissions or mortality
More hospitalist positions than physicians which makes the PA and NP model a viable alternative to work force shortage issues

Cost Effective ModelCost Effective Model
Billing options allow for shared or independent visits
The same way that hospitalists add hospitalists add value*value* so too do PAs & NPs in hospitalist practices
*SHM special supplement "How Hospitalists Add Value"*SHM special supplement "How Hospitalists Add Value"

WhyWhyIntegrate
PAs, NPs, and RN CCCs
into
Hospitalist Practices?
BecauseBecauseThey
Add Value!

How Do NPPs Add Value?How Do NPPs Add Value?

The The MantraMantra of Hospitalists of Hospitalists
The purpose of admitting patients to the hospital is to discharge them
Discharge planning begins at the moment
of admissionThe average length of stay for most patients should not exceed three (3)
days.

The conundrum ofThe conundrum of
competingcompeting
congruentcongruent
contemporaneouscontemporaneous
care processescare processesOvernight hand-
offs
Admiss
ion
s
Follow up visits
Consults
Procedures
Family conferences
Quality Improvement projects
ICURRT
Codes Dis
charg
e
s

The The CompetitionCompetition for provider time… for provider time…
delaysdelays the continuum of care that culminates in the patient’s (un)timely
dischargedischarge.

Competition for Provider Time:Competition for Provider Time:
The The Ivory TowerIvory Tower Structure Structure
Academia ResidentsInterns Students
Residency Review CommitteeResidency Review Committee
Duty Hours RestrictionsDuty Hours Restrictions

Integrating PAs, NPs and RN CCCs in Acute CareIntegrating PAs, NPs and RN CCCs in Acute Care
The integrated model of medical practice, in which the patient care team is led by the medical managermedical manager (MD or DO), assisted by the patient care managerpatient care manager (PA or NP), and clinically coordinated by the CCCCCC (RN) is one solution to the competition for care processes in the management of inpatients.
Competition for Provider Time:A non-housestaff Solution

Integrating PAs, NPs and RN CCCs in Acute CareIntegrating PAs, NPs and RN CCCs in Acute Care
Physician Physician (medical manager) makes key medical decisions & follows medical progress
PA/NPPA/NP (patient care manager) implements decisions (dependent & independent), monitors care
Nurse CCCNurse CCC coordinates the clinical care processes culminating in discharge
Competition for Provider Time:A non-housestaff Solution

Physician Assistants,Nurse Practitioners,
and RN CCCs
Pitching the Value-AddedValue-Added Proposition

Wachter, "Hospital Medicine" p.33, Donabedian , "JAMA" 1988
Value = Value = QualityQuality // Cost Cost
The Health Care ValueThe Health Care ValueCascadeCascade
Health CareHealth Care == Clinical qualityClinical quality xx SatisfactionSatisfactionQualityQuality
Clinical Quality = structurestructure, process, outcomes

PAs, NPs, and RN CCCsPAs, NPs, and RN CCCsPitching the Value-Added PropositionPitching the Value-Added Proposition
Some Elements of Value:
Structure: Denotes the attributes of the setting
Process: Denotes action in giving & receiving care
Outcome: Denotes the effects of care on health
““How is care organized”How is care organized”
““What is done”What is done”
““What Happened”What Happened”

Value = ClinQual x Satisfaction
Cost
Evidence: Studies, Experience
StructureStructure
Processes
Outcomes
PAs, NPs, and RN CCCsPAs, NPs, and RN CCCsPitching the Value-Added PropositionPitching the Value-Added Proposition

Overnight hand-
offs
Admiss
ion
s
Follow up visits
Procedures
Family conferences
Dr Dr WilsonWilson
Quality Improvement projects
Disch
arge
s

Overnight hand-
offs
Admiss
ion
s
Disch
arges
Follow up visits
Consults
Procedures
Family conferences
Quality Improvement projects

Crane, S., "Physician Executive" 1995
Physician Assistants and Nurse PractitionersPhysician Assistants and Nurse Practitioners
Pitching the Value-Added PropositionPitching the Value-Added Proposition
“As these two major national advisory groups (Institute of Medicine and Pew Health Professions Commission) and other policy analysts have concluded, it is the integration it is the integration of care using a of care using a team of providersteam of providers, not the , not the fragmentation of care through the proliferation fragmentation of care through the proliferation of independent providers, that will be the of independent providers, that will be the model of high-quality and cost-effective model of high-quality and cost-effective health carehealth care in the future.” in the future.”

NPPs in Hospital Medicine
Indications:Are PAs, NPs, and RN CCCs
Right for Us?

NPPs in Hospital Medicine
Opportunities

Opportunities: ProgrammaticOpportunities: Programmatic
Hospitalist Resources• Recruiting• Retention• Satisfaction
Growth• Supply-Demand mismatch• Access to care• New business & market share
Structure• In-house vs. call• Single hospital vs. multi-site• Admitter vs. Rounder

Opportunities: ProgrammaticOpportunities: Programmatic
Program Performance**• Throughput• Hospital Cost & Utilization• Customer Satisfaction• Quality, Safety and Stewardship
Hospital specific needs• Code Team• RRT• Lines
• Restraints• ED Unassigned• ICU
*SHM white paper: “Measuring Hospitalist Performance"*SHM white paper: “Measuring Hospitalist Performance"

Opportunities: EnvironmentOpportunities: Environment
Are PAs & NPs already practicing:• Referring physician offices• Autonomously in clinics• Sub-specialist's practices• Hospital based
If so:• Is their work widely known?• How are they regarded generally?• What is their reputation specifically?• What do they do?

Opportunities: EnvironmentOpportunities: Environment
Are there PA & NP programs nearby? Competition
• Nearby hospitals• Nearby hospitalists
Location & Size• Urban• Rural and/or Critical Access• Less than 100 beds
ICU: Open or closed Teaching hospital

Opportunities: CultureOpportunities: Culture
Hospitalist• Worked successfully with PAs & NPs
before?• Advocates & Champions• Patriarch or Monarch—positive outlook• Musketeers versus Mercenaries
– all for one and one for all– every hospitalist for themselves

Opportunities: CultureOpportunities: Culture
Hospitalist (cont.)• Non physician group members• Clinician Educators, teacher-types• Mentor structure in place
Hospital• Nursing and NPs• Change oriented

OpportunitiesOpportunities
If you have seen one hospital medicine program you have seen one hospital medicine program – view this as an OPPORTUNITY to customize and tailor your collaborative PA and NP model to your practice
Proactive “planning mode” (instead of reactive “crisis mode”)

OpportunitiesOpportunities
Don’t reinvent the wheel – SHM experts are available to help

I was seldom able to see an opportunity until it had ceased to be one.
--Mark Twain's Autobiography

Barriers to SuccessBarriers to Success
NPPs in Hospital Medicine

The greatest barrier to someone achieving their potential is their denial of it.
--Simon Travaglia

Barriers: ProgrammaticBarriers: Programmatic
Hospitalist Resources• Different employers: Physician & PA/NP• Payroll rules• Human Resources• Low attrition• Hiring the wrong person
Growth• Unmotivated workforce• Lack of incentives• Restricted Access• Limitations on new business & market share• Flat line

Barriers: ProgrammaticBarriers: Programmatic
Structure• Lack of supervision• Poor role definition and/or lack of understanding
the role• Lack of preparedness• Lack of administrative & practice infrastructure &
support Program Performance
• Productivity tracking and/or incentive structure:– Doesn’t credit physician for the 15% shared-visit effort– doesn’t include PA & NP effort

Barriers: ProgrammaticBarriers: Programmatic
Program Performance (cont.)• No system in place to track
– PA & NP performance measures and outcomes
– patient satisfaction with PAs & NPs
• Failure to credential PAs & NPs with payors
• Billing system not ready to accommodate PA & NP charges

Barriers: EnvironmentBarriers: Environment
Are PAs & NPs new or novel?If PAs & NPs are already practicing:
• Is their work widely known?• How are they regarded generally?• What is their reputation specifically?• What do they do?

Barriers: EnvironmentBarriers: Environment
Unrealistic expectations• Hospital: “The hospitalists will fix our
problems”• Hospitalists: “The PA/NP will fix our
problems”
Perception that the driver (for integration) is increasing pressure to offset program cost

Barriers: EnvironmentBarriers: Environment
Perception that integration will alienate referral groups
Lack of environmental awareness• Perception• Reality
Laws & BylawsChanges in hospital leadership

Barriers: CultureBarriers: Culture
Hospitalist• Worked unsuccessfully with PAs & NPs
before• Naysayers• No Advocate or Champion• Patriarch or Monarch—ambivalent or worse• Mercenaries versus Musketeers
– every hospitalist for themselves– all for one and one for all

Barriers: CultureBarriers: Culture
Hospitalist• Unwillingness to:
– Teach– Mentor– Oversee & Review
• Unwillingness to change the culture• Polarized group

Barriers: CultureBarriers: Culture
General Attitude• Fear of competition• Only doctors can do the job• Diminishes physician importance
Bad Attitude• Not just no but “heck no”
Reactive “crisis mode” (instead of proactive “planning mode”)
A bad attitude is like a flat tire—you can’t get anywhere unless you change it!

Integrate
NPPs
Into Our
Hospitalist Practice?
AreAreNPPs
right for you?
Should WeShould We

Are NPPs right for your practice?Are NPPs right for your practice?
Environment is everything & culture is critical Not a “one size fits all” model Do your homework—data informs decisions
• Advantages• Disadvantages• Opportunities• Barriers
Practice SiteNeeds
vsBarriers to
Implementation

Are NPPs right for your practice?Are NPPs right for your practice?
Needs Versus Barriers Analysis
High Low
HighHigh HHH HHL
LowLow LLH LLL
Barriersto
Implementation
Practice SitePractice SiteNeedsNeeds

Case Study: Case Study: NeedsNeeds vs. Barriers vs. Barriers
Difficult & complex cases Access to service (PCPs, co-
management) Timeliness of care Surge capacity Interface issues with case
managers, staff nurses and ancillary care
Hospital & Patient satisfaction Committee & QI/QA
involvement Recruiting, Retention, &
hospitalist satisfaction Supply-Demand mismatch New business (including multi-
site) 24/7 in-house
Rounder is admitter structure Program performance Code/RRT ED Unassigned & OBS cases PAs & NPs known entities in
environment, well regarded Nearby competitor hospitals,
suburban Open ICU Advocates
• Founder• Two hospitalists• Teacher-type• +/-Program administrator
Medical Staff express no firm opposition

Case Study: Needs vs Case Study: Needs vs BarriersBarriers
No role definition as of yet Lack of preparedness
• Programmatic• Environmental
One hospitalist unsuccessful in past
Possible supervision issue with 1-2 hospitalists
“The PA/NP will fix things” attitude
Integration will alienate referring physicians (CMO)
Bias against PAs (CNO) Two senior medical staff
members not in favor

Are NPPs right for your practice?Are NPPs right for your practice?
Needs Versus Barriers Analysis
High Low
HighHigh HHH HHL
LowLow LLH LLL
Barriersto
Implementation
Practice SitePractice SiteNeedsNeeds
Case StudyCase Study

Barriers are merely opportunities waiting to be born.
--M. J. Wilson, M.D.

Panel DiscussionPanel Discussion

ImplementationImplementation
How can NPPs be Integrated Into the How can NPPs be Integrated Into the Hospitalist PracticeHospitalist Practice

Plan & Execute: Stakeholder Buy-inPlan & Execute: Stakeholder Buy-in
Do your homework, then lay the groundwork• Become an expert in PA and NP practice• Teach others what you’ve learned
Identify and survey all stakeholders, conduct focus groups in high barrier environments• Hospital Administration• PCPs• Referring Providers• Hospitalist Team• Patient care staff• Patients

Plan & Execute: Stakeholder Buy-inPlan & Execute: Stakeholder Buy-in
Use the information you receive in structuring PA and NP assignments & responsibilities
Provide feedback to stakeholders by letting them know:• That you were listening• What you did with their information
Communicate, Communicate, Communicate• Tell them what you are going to tell them, then tell
them, and then tell them what you told them

Plan & Execute: Stakeholder Buy-inPlan & Execute: Stakeholder Buy-in
Mitch, I can’t emphasize enough that if you are adding a first mid-level, there must be buy-in and support from the community and the group with very clear expectations.
The group has to want this and then back the mid-level up when his/her role is questioned or challenged.
--Lorraine Britting, MS, ANPSHM Non-Physician Provider Committee

Plan & Execute: Skill MixPlan & Execute: Skill Mix
Go with what your environment knows• Do PAs or NPs predominate?• In what setting?
Define the duties, then match the roles• Structure the advertising, interview, and hire
process to assure best practice fit– High acuity/ICU care = experienced PA or ACNP– Elderly population/MMM = experienced PA or GNP or
ACNP, +/- ANP (depending on experience)– OBS/CDU = PA or ANP, +/-FNP (depending on
experience) or ACNP

Plan & Execute: Skill MixPlan & Execute: Skill Mix
Define the duties, then match the roles, (cont.)• Start out with the best of the best—the microscope
will be on full power• Hire and pay for experience
– Invest in your start-up—you get what you pay for– Especially important for high barrier environments and
where immediate success is critical• Recruit local talent whenever possible
– Even if new to hospitalist role– A known and trusted provider new to the role may enable
early acceptance more than an unknown who knows how to do the job

Plan & Execute: Structure ServicesPlan & Execute: Structure Services
Tailor supervision and assignments to experience and skill set:• Evaluate individual physician characteristics and
partner physician and PAs/NPs based on best fit• Tailor physician supervision to the experience and
skills of the PA and NP• Capitalize on PA and NP past experiences and
strengths
Use a mentoring process

Plan & Execute: Structure ServicesPlan & Execute: Structure Services
Make team assignments: Less experienced PA/NPWorked successfully with PA/NP beforeTeacher-typesAdvocates and ChampionsMusketeersPatriarch, Monarch—positive outlook Worked unsuccessfully Naysayers Mercenary Patriarch, Monarch—ambivalent or worse Unwilling to teach

Plan & Execute: Structure ServicesPlan & Execute: Structure Services
Make team assignments: More experienced PA/NPWorked successfully with PA/NP beforePatriarch, Monarch—positive outlookAdvocates and ChampionsMusketeersTeacher-types Worked unsuccessfully Naysayers Mercenary Patriarch, Monarch—ambivalent or worse Unwilling to teach

Plan & Execute: Structure ServicesPlan & Execute: Structure Services
Make work assignments:• Less experience
– Protocol, pathway, guideline driven DRGs– Low acuity (chest pain, mild pulmonary, GU)– Direct supervision, more shared-visits
• More experience– Protocol, pathway, guideline driven DRGs to start,
transition quickly to non-pathway DRGs– Higher acuity– Indirect supervision, fewer shared-visits

Plan & Execute: Structure ServicesPlan & Execute: Structure Services
Make work assignments (cont.):• All experience levels
– Touch-base “card-flip” daily—late morning & afternoon
• Referring Physicians– Preferentially assign by buy-in versus opt-out
Stagger the on-service start dates• On-service/off-service rotation dates differ for
physicians & PAs/NPs• Overlap allows for more continuity of care &
slightly eases the first day on

Plan & Execute: Structure ServicesPlan & Execute: Structure Services
Check-out process for PAs/NPs going off—coming on service• Mirror physician process if possible
Stagger the new-hire start dates Start out slow and gradually increase patient
load and assignments

Plan & Execute: Leadership Plan & Execute: Leadership PearlsPearls
Debrief with:• PAs/NPs often (daily, qod, biweekly, etc.) during
start-up• Hospitalists per above• Meet with both groups together at least once
during each rotation• Nurses & nurse administration• Key Stakeholders
Actively engage feedback Actively resolve turbulence

Plan & Execute: Leadership Plan & Execute: Leadership PearlsPearls
Rewards for:• Buy-in• Enablers of success• Teams making it work
Consequences for:• Opt-out• Obstruction• Subversion• Sabotage
Move towards a single-tiered schedule

Plan & Execute: Leadership Plan & Execute: Leadership PearlsPearls
Stick to the play book• Assignments to create “go-do” not “go-for”• Encourage flexibility and interdependence• Develop dynamic, cross-functional teamwork
Don’t allow a second-class citizen culture to emerge• Equal voice, equal vote at team meetings and
practice related activities• Reserve agenda space and discussion time for
PA/NP issues Create early wins and publicize to stakeholders

Plan & Execute: Leadership Plan & Execute: Leadership PearlsPearls
Make sure you have baseline data – performance measures
Track outcomes and performance measures from pre-PA and NP structure to post- PA and NP implementation
Work with hospital administration & program management• Determine what is most important to funding source • Stratify needs by priority & importance• Align goals• Develop services to achieve greatest gains for the effort
Capitalize on “real time service” delivery

Plan & Execute: Leadership Plan & Execute: Leadership PearlsPearls
Know the rules:• State regulations, registration, certification• Institutional bylaws and privileges• Documentation, billing, and reimbursement
Don’t be afraid to “drop back and punt” Keep working it until you get it “right” Remember there is no “I” in TEAM! Provide a career path and incentives Keep the key stakeholders in mind when:
• Sharing your results• Developing your marketing plan

Critical Success FactorsCritical Success Factors
Delineations of duties: What the PA, NP, and RN CCC can and cannot do
Hire for fit (not for fill) Key stake-holder buy-in Hospitalist Advocates & Champions Hospitalist group culture of equality Preparedness in planning and execution Marketing

Michael Collins, "From Good to Great"
Critical Failure FactorsCritical Failure Factors
The opposite of success factors!• Poor role delineation• Wrong person/wrong seat on the bus*
(poor fit)• Lack of mentoring tailored to experience• Pervasive opt-out• Billing & performance monitoring absent
Taking on “too much, too fast”

Panel DiscussionPanel Discussion

The Bottom LineThe Bottom Line
Demonstrating ROIDemonstrating ROI

E&M Code DescriptionMedicare
Allowable/MD
Medicare Allowable
PA/NP % 85%# of
EncountersPA/NP
Collection RatePA/NP
Collection Rate# of
EncountersPA/NP
Collection RatePA/NP
Collection Rate
30% 46% 30% 46%Admit
99221 low $82.49 $70.1299222 intermed $113.41 $96.4099223 complex $166.87 $141.84
F/U99231 low $34.33 $29.18 10 $31,952.65 $48,994.06 7 $26,313.95 $40,348.0599232 intermed $61.49 $52.2799233 complex $88.16 $74.94
DC99238 l.t. 30 $62.52 $53.14 5 $29,095.25 $44,612.71 3 $20,537.82 $31,491.3299239 g.t. 30 $89.90 $76.42
OBS99218 low $58.90 $50.0799219 intermed $96.86 $82.3399220 complex $136.23 $115.80
OBS99217 D/C $62.41 $53.05
OBS Same Date99234 low $118.00 $100.3099235 intermed $155.73 $132.3799236 complex $193.80 $164.73
Total $61,047.89 $93,606.77 $46,851.77 $71,839.37
Demonstrating ROIDemonstrating ROI

Demonstrating ROIDemonstrating ROI
High (15) Productivity High (15) ProductivityHigh Collection Low Collection
Incremental Net Revenue Incremental Net Revenue$93,606.77 PA/NP $61,047.89
$107,647.78 MD $70,205.07
Average (10) Productivity Average (10) ProductivityHigh Collection Low Collection
Incremental Net Revenue Incremental Net Revenue$71,839.37 PA/NP $46,851.77$82,615.27 MD $53,879.53
46% 30%
Collections
P
rod
uct
ivit
y

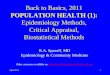
Demonstrating ROIDemonstrating ROIValue of a PA/NP
Increase in Patients/Day 15 10
Increase in Net Professional Revenue/Patient Day (46% Collection Rate) $93,606.77 $71,839.37
PA/NP Cost ($80K/yr, 26% fringe) $201,600.00 $201,600.00
PA/NP Net Incremental Cost ($107,993.23) ($129,760.63)

Demonstrating ROIDemonstrating ROIValue of a PA/NP
Increase in Patients/Day 15 10
Increase in Net Professional Revenue/Patient Day (46% Collection Rate) $93,606.77 $71,839.37
PA/NP Cost ($80K/yr, 26% fringe) $201,600.00 $201,600.00
PA/NP Net Incremental Cost ($107,993.23) ($129,760.63)
MD Net Incremental Cost ($157.5K/yr, 26%) ($289,252.22) ($314,284.72)

Demonstrating ROIDemonstrating ROIValue of a PA/NP
Increase in Patients/Day 15 10
Increase in Net Professional Revenue/Patient Day (46% Collection Rate) $93,606.77 $71,839.37
PA/NP Cost ($80K/yr, 26% fringe) $201,600.00 $201,600.00
PA/NP Net Incremental Cost ($107,993.23) ($129,760.63)
MD Net Incremental Cost ($157.5K/yr, 26%) ($289,252.22) ($314,284.72)
Net Incremental Increase in Loss MD vs PA ($181,258.98) ($184,524.09)

Billing Medicare:Billing Medicare:
Hospital SettingsHospital Settings
Shared VisitsShared Visits
Remember the “33 SamesSames and a SomeSome” rule:
SameSame employerSameSame patientSameSame daySomeSome face-to-face time with the patient

Panel DiscussionPanel Discussion