Embed Size (px)
Citation preview

Allan Garland, MD, MA
Associate Professor of Medicine & Community Health Sciences
University of Manitoba
Long-term versus Short-term
Prognostication in Critical Illness

Conflicts of Interest
Nothing to declare

Introduction & Rationale - 1
Prognosticating, to inform discussing achievable treatment plans and goals with patients/surrogates is one of the most important things we do in the ICU
The usual ICU risk stratification systems only address short-term outcomes, while patients care more about long-term survival (JGIM 5:402,1990)
In the absence of established quantitative approaches to prognosticating, physicians commonly use gestalt
Trainees consistently report that they receive inadequate training and feel ill-prepared for prognosticating (J Palliative Med 1:347,1998; CCM 30:290,2002)

Introduction & Rationale - 2
SO -- it’s important to better understand the main determinants of long-term mortality in critical illness
Hypothesis: The determinants of long-term mortality differ from the main determinants of short-term mortality
A necessity in addressing this question is to separately analyze the short-term and long-term phases
Identifying the determinants of long-term mortality requires analysis that starts after the short-term phase has ended
– prior studies assessing long-term survival failed to do this

Methods
Data: linked provincial administrative data + clinical database covering all Winnipeg ICUs
All adults admitted to all ICUs in the Winnipeg Regional Health Authority of Manitoba over 11 years, 1999-2010
– only included each person’s first ICU episode
Preliminary step: Kaplan-Meier survival curve
3 multivariable mortality regression models
– short-term -- logistic model; death to 30 days after ICU admit
– long-term -- Cox model; time to death >90 days after ICU admission among those who survived to day#90
– both -- Cox model; time to death starting from ICU admission

Covariates for Mortality Models
Age, sex, residency location (in vs. outside Winnipeg), SES (average household income by postal code); comorbidities
ICU admission details: year; timing (weekday vs. weekend, days vs. nights); pre-ICU location (ED, ward, OR/PACU); hospital type (community vs. tertiary)
ICU admission diagnosis category
Severity of illness: GCS; APACHE II APS excluding neurologic subscore; use of life support during first 2 ICU days (invasive MV, vasoactive agents, dialysis)
Cubic splines to allow for nonlinear relationships between of mortality with age, APS

Evaluation of Impact of Groups of Variables
Quantified the predictive power of five clusters of variables
– age
– sex and SES
– comorbid conditions
– acute illness characteristics (diagnosis, GCS, APS, pre-ICU location, need for MV ventilation, vasoactive drugs, dialysis)
– remaining model variables (admission timing, admission year, hospital type, residency location)
For this used Akaike’s Information Criterion (AIC)
– a goodness-of-fit measure for these models
– within each model -- evaluated DAIC when one of the variable clusters was omitted from the model

Patients & Illnesses
Variable
N 33,324
Female sex (%) 40.5%
Age (yrs), mean ± SD 63.5 ± 16.2
ICU admit diagnosis category (%)
Circulatory System 60.4
Symptoms, Signs (includes sepsis) 11.8
Respiratory System 10.7
Injury and Poisoning 7.6
Digestive System 3.4
APACHE II score, mean ± SD 15.3 ± 7.9
Mechanical ventilation ICU days 1-2 (%) 57.3
Vasoactive drugs ICU days 1-2 (%) 46.2
Renal dialysis ICU days 1-2 (%) 5.4

Results
Median lengths-of-stay:
– ICU: 2.4 days (IQR 1.1-4.6)
– hospital: 11 days (IQR 6-24)
Mortality (after ICU admission)
– 15.9% died within 30 days
– 19.5% died by 90 days

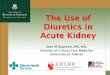
Kaplan-Meier Survival Curve (unadjusted)
0 2 4 6 8 10 120.00
0.25
0.50
0.75
1.00
30 days
90 days
S
urv
iva
l F
ract
ion
Years after ICU Admission
2 phases of
mortality
associated with
critical illness
Early high rate
of death
Later lower rate
of dying that is
clearly
established a few
months after
ICU admission

Independent variable
Death at 30 days
after ICU admission
Odds Ratio
Death >90 days
after ICU admission,
among 90 day survivors
Hazard Ratio
Age asymptotic rise * asymptotic rise *
Female sex 1.00 0.85 *
Socioeconomic status
Lowest urban income (reference) -- --
Highest urban income 0.83 * 0.72 *
Institutionalized 0.62 * 1.40 *
Regression Results - Demographics

Regression Results - Selected items
Death at 30 days
Odds Ratio
Death >90 days
Hazard Ratio
Comorbid conditions
Metastatic cancer 3.44 * 4.68 *
Liver disease 2.87 * 1.72 *
Congestive heart failure 1.17 * 1.61 *
Chronic pulmonary disease 1.12 * 1.51 *
Diabetes 0.93 1.39 *
Obesity 0.79 * 0.97
Drug abuse 0.71 * 1.42 *
Admission diagnoses
Circulatory System (reference) -- --
Respiratory System 1.23 * 1.55 *
Genitourinary System 0.46 * 1.38 *

Regression Results - Severity of Illness
Variable Death at 30 days
Odds Ratio
Death >90 days
Hazard Ratio
APS-Neurologic subscore asymptotic rise * rise then plateau*
Glasgow Coma Scale score
3-5 21.02 * 0.98
15 (reference) -- --
Mechanical ventilation ICU days 1/2 1.51 * 0.99
Vasoactive drugs ICU days 1/2 1.42 * 0.95
Dialysis ICU days 1/2 1.13 1.36 *

BUT
The magnitude and p-values of coefficients
in regression equations do not directly
indicate their predictive power

Death to
30 days after
ICU admission
Acute illness characteristics 1.00
Age 0.14
Comorbid conditions 0.09
Admission year, admission timing,
hospital type, residency location 0.002
Sex, socioeconomic status 0.001
Details of the acute illness are the dominant factor relating to short-term mortality
Relative Predictive Value of Variables

Post-90 day survival,
among 90 day
survivors
Acute illness characteristics 0.26
Age 1.00
Comorbid conditions 0.93
Admission year, admission timing,
hospital type, residency location 0.04
Sex, socioeconomic status 0.07
Relative Predictive Value of Variables
Age and comorbid conditions are the dominant determinants of long-term mortality, among short-term survivors
– same as for the general population

Death to
30 days after
ICU admission
Post-90 day survival,
among 90 day
survivors
Survival from
ICU admission
Acute illness characteristics 1.00
Age 0.69
Comorbid conditions 0.55
Admission year, admission timing,
hospital type, residency location 0.04
Sex, socioeconomic status 0.03
Relative Predictive Value of Variables
Main determinants of long-term mortality starting from onset of critical illness, are acute illness, age and comorbid conditions

Relative Predictive Value of Variables
Death to
30 days after
ICU admission
Post-90 day survival,
among 90 day
survivors
Survival from
ICU admission
Acute illness characteristics 1.00 (ref) 0.26 1.00 (ref)
Age 0.14 1.000 (ref) 0.69
Comorbid conditions 0.09 0.93 0.55
Admission year, admission timing,
hospital type, residency location 0.002 0.04 0.04
Sex, socioeconomic status 0.001 0.07 0.03
--------------- Regression models ---------------
Long-term mortality starting from onset of critical illness, is determined by a mixture of the main determinants of short-term and long-term mortality -- as expected

Summary: Main Findings
There are 2 distinct phases of survival related to critical illness
Death in the month after onset mainly determined by the type and severity of acute illness, but this influence decayed relatively rapidly -- age and comorbidity were only minor contributors to short-term survival
Among those who survived to 90 days after illness onset, subsequent survival was mainly determined by comorbid conditions and age, as in the general population

Discussion - 1
Appreciation of these phases is relevant, and can be helpful in discussing achievable goals and care plans
People generally place more value on long-term than short-term survival conversations focused only on the chance of surviving the acute illness are inadequate
Clarity may be improved by explicitly framing these discussions around short-term followed by long-term considerations:
– first discuss the chances of short-term survival from the critical illness, as determined by its type and severity
– then, if short-term survival seems sufficiently possible discuss long-term survival, as mainly related to age and the burden of comorbid conditions

Discussion - 2
Strengths
– large, population-based study assessing consecutive, unselected patients admitted over a substantial timespan to all types of ICUs
– assessed a wide and robust range of potential determinants of mortality
– first study whose methodology allowed for clear delineation of short-term from long-term influences on outcome, and did so on the same patient cohort
Limitation
– some known determinants of mortality were not contained in our data -- prehospital living site, prehospital functional status, post-hospital discharge location

Collaborators
Randy Fransoo, PhD
Kendiss Olafson, MD, MPH
Clare Ramsey, MD, MSC
Marina Yogendran, MSc