Embed Size (px)
Citation preview

Miriam Koopman, L Simkens, A ten Tije, G Creemers, O Loosveld, F de Jongh, F Erdkamp, Z Erjavec, A van der Torren, J van der Hoeven, P Nieboer, J Braun, R Jansen, J Haasjes, A Cats, J Wals, L Mol, O Dalesio, H van Tinteren, C Punt
Maintenance treatment with capecitabine + bevacizumab versus observation after induction treatment with chemotherapy + bevacizumab in
metastatic colorectal cancer
Phase 3 CAIRO3 study of the Dutch Colorectal Cancer Group (DCCG)

Background
• The value of chemotherapy-free intervals has been tested in the OPTIMOX2, COIN and GISCAD studies, and is still a matter of debate1-3
• The optimal duration of chemotherapy and bevacizumab in metastatic colorectal cancer (mCRC) is unknown
• The benefit of bevacizumab added to chemotherapy in the NO16966 study (FOLFOX/CAPOX +/- bevacizumab) may have been compromised due to the low percentage of patients that received treatment until disease progression4
• Drug holidays are preferred by many patients 1Chibaudel et al. J Clin Oncol 20092Adams et al. Lancet Oncol 20113Labianca et al. Ann Oncol 20114Saltz et al. J Clin Oncol 2008

Study rationale
CAIRO3 study was designed to investigate the efficacy of
observation
versus
maintenance treatment with capecitabine + bevacizumab
after induction treatment with 6 cycles of capecitabine, oxaliplatin + bevacizumab (CAPOX-B)

CAIRO3 treatment
Pre-study induction treatment with 6 cycles of 3-weekly CAPOX- B• Capecitabine 1000 mg/m2 b.i.d. orally day 1 – 14• Oxaliplatin 130 mg/m2 i.v. day 1• Bevacizumab 7.5 mg/kg i.v. day 1
Maintenance treatment• Capecitabine 625 mg/m2 b.i.d. orally continuously• Bevacizumab 7.5 mg/kg i.v. day 1, 3-weekly

CAIRO3 main inclusion criteria
• Histological proof of metastatic CRC
• Age 18 years, WHO PS 0-1
• Stable disease or better after first-line treatment with 6 cycles of CAPOX- B
• Eligible for further treatment with CAPOX- B
• No intention of radical resection of metastases
• Adequate organ functions
• Written informed consent

Study design
SD or better after 6 cycles CAPOX- B
observation
R
capecitabine + bevacizumab
PD PDRe-introduction
CAPOX-B
PFS1 PFS2

SD or better after 6 cycles CAPOX- B
observation
R
capecitabine + bevacizumab
Re-introductionCAPOX-BPD
PFS1
PD
• PFS1: time from randomization until first progression after observation or maintenance treatment
Definition of PFS1

Definition of PFS2primary endpoint
SD or better after 6 cycles CAPOX- B
observation
R
capecitabine + bevacizumab
PD
PFS2
Primary endpoint: PFS2 • time from randomization to progression upon re-introduction of CAPOX- B• PFS2 is considered to be equal to PFS1 for patients in whom CAPOX- B is not
reintroduced after PFS1 for any reason
PD
PFS1
Re-introductionCAPOX-B

Definition of TT2PD
SD or better after 6 cycles CAPOX- B
observation
R
capecitabine + bevacizumab
PD
TT2PD
PD
PFS1
any treatmentincl. CAPOX-B
• TT2PD = time to second progression of disease, time from randomization to progression upon any treatment including CAPOX-B, given after PFS1

Statistical design
• Endpoints were calculated from time of randomization upon progression/death (i.e. not including 6 x CAPOX-B induction)
• Sample size was calculated to detect a hazard ratio of 0.78 which translates into an increase of PFS2 from 9 to 11.5 months
• 525 events were required, providing 80% power to detect a decrease of 22% in the hazard of progression (α=0.05, 2-tailed test)
• Stratified as well as adjusted HR's with corresponding p-values will be shown using stratified cox proportional hazard models adjusting for covariates with imbalances at baseline

Duration and evaluation of treatment
• Treatment was to be continued until progression, unless:– unacceptable toxicity– patient refusal – continuation not considered in the interest of the patient
• Evaluation of tumor response and toxicity every 9 weeks (RECIST, NCI-CTC criteria, 3.0)

Accrual and follow-up
• 74 Dutch hospitals
• 558 patients were randomized between May 2007 and June 2012
• Cut-off data 19-04-2013 (updated from abstract)
• Median duration of follow-up is 40 months
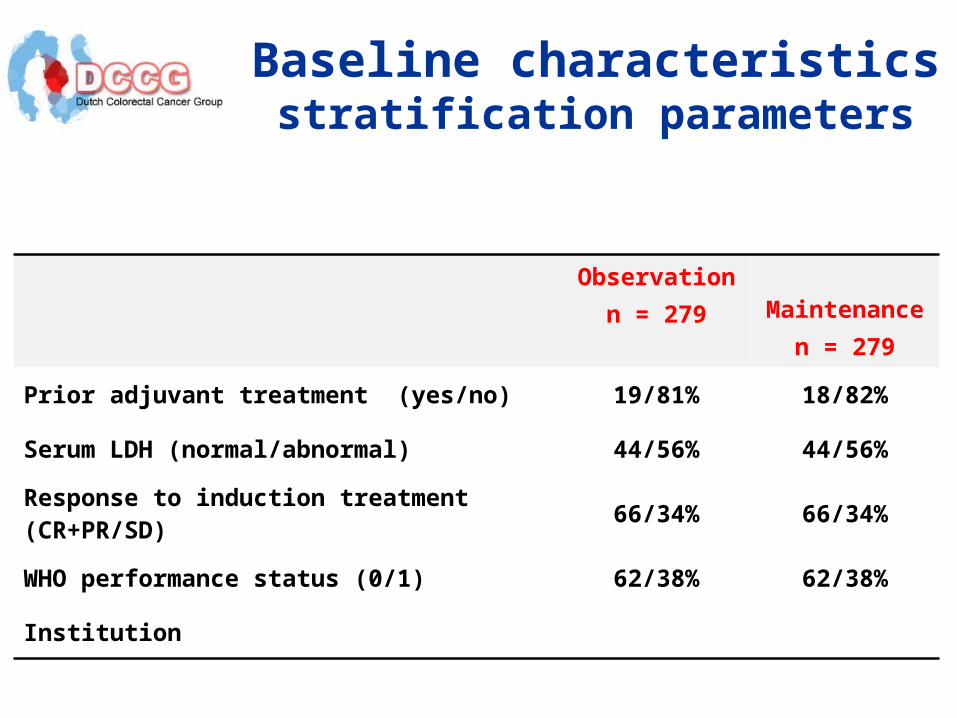
Observationn = 279
Maintenance n = 279
Prior adjuvant treatment (yes/no) 19/81% 18/82%
Serum LDH (normal/abnormal) 44/56% 44/56%
Response to induction treatment (CR+PR/SD) 66/34% 66/34%
WHO performance status (0/1) 62/38% 62/38%
Institution
Baseline characteristicsstratification parameters

Observationn = 279
Maintenance n = 279
Age (median, range) 64 (31-81) 63 (26-81)
Gender (male / female) 64/36% 66/34%
Number of metastatic sites (1 / >1) 46/54% 48/52%
Interval between primary diagnosis and randomization in the study (mean in months) *
19 14
Stage of disease (I-III / IV) * 33/67% 23/76%
Baseline characteristicsother
* Covariates of which the differences are statistically significant

CAIRO3 study profile
558 patients enrolled
279 patientsobservation
279 patientsmaintenance
212 patients(76%)
re-introductionCAPOX-B
131 patients(47%)
re-introductionCAPOX-B
67 patients(24%)
- ongoing obs.- no treatment- other treatment
148 patients(53%)
- ongoing maint.- no treatment- other treatment

SD or better after 6 cycles CAPOX- B
observation
R
capecitabine + bevacizumab
Re-introductionCAPOX-BPD
PFS1
PD
• PFS1: time from randomization until first progression
Results: PFS1

Time (mths)
PF
S1
Pro
ba
bili
ty
0 6 12 18 24 30 36
0.0
0.2
0.4
0.6
0.8
1.0
279 85 18 9 6 6 3 Observation
279 172 89 44 29 15 9 Maintenance
Observation
Maintenance
median PFS1 - Observation : 4.1 (95% CI: 3.9 - 4.4 )
median PFS1 - Maintenance : 8.5 (95% CI: 6.9 - 10.2 )
ITT, events/n ( 256 / 279 - 266 / 279 )
HR= 0.44 ( 95% CI: 0.36 - 0.53 )
stratified log-rank p-value 0
Median PFS1
Observation 4.1 m [95%CI: 3.9-4.4]
Maintenance 8.5 m [95%CI: 6.9-10.2]
Stratified HR 0.44 [95%CI: 0.36-0.53]
p value < 0.00001
PFS1
adjusted HR 0.41, p <0.001

Observation n=279
Maintenance n=279
Observation/maintenance ongoing 13 (5%) 20 (7%)
Treatment discontinuation 266 (95%) 256 (92%)
No follow up 0 3 (1%)
Reasons for discontinuation n=266 n=256
disease progression/death 264 (95%) 214 (77%)
toxicity 0 25 (10%)
refusal 0 5 (2%)
other 2 (1%) 12 (5%)
Median number of cycles (range)
Capecitabine - 9 (1-85)
Bevacizumab - 10 (1-88)
Treatment until PFS1

Results: PFS2primary endpoint
SD or better after 6 cycles CAPOX- B
observation
R
capecitabine + bevacizumab
PD
PFS2
PD
PFS1
Re-introductionCAPOX-B
Primary endpoint: PFS2 • time from randomization to progression upon re-introduction of CAPOX- B• PFS2 is considered to be equal to PFS1 for patients in whom CAPOX- B is not
reintroduced after PFS1 for any reason

Time (mths)
PF
S2
Pro
ba
bili
ty
0 6 12 18 24 30 36
0.0
0.2
0.4
0.6
0.8
1.0
279 207 111 42 16 11 4 Observation
279 207 130 66 38 23 12 Maintenance
Observation
Maintenance
median PFS2 - Observation : 10.5 (95% CI: 9.3 - 12.3 )
median PFS2 - Maintenance : 11.8 (95% CI: 10.2 - 13.3 )
ITT, events/n ( 246 / 279 - 243 / 279 )
HR= 0.81 ( 95% CI: 0.67 - 0.98 )
stratified log-rank p-value 0.028
Primary endpoint PFS2
Median PFS2
Observation 10.5 m [95%CI: 9.3-12.3]
Maintenance 11.8 m [95%CI: 10.2-13.3]
Stratified HR 0.81 [95%CI: 0.67-0.98]
p value 0.028
adjusted HR 0.77, p 0.007

Observationn=279
Maintenancen=279
Observation/maintenance ongoing 13 (5%) 20 (7%)
No re-introduction CAPOX-B 54 (19%) 125 (45%)
Re-introduction CAPOX-B 212 (76%) 131 (47%)
No follow-up 0 3 (1%)
Reasons for discontinuation CAPOX-B n=212 n=131
Ongoing CAPOX- B 13 (6%) 8 (6%)
Disease progression/death 137 (65%) 97 (74%)
Toxicity 30 (14%) 18 (14%)
Patient refusal 11 (5%) 1 (1%)
Other 21 (10%) 7 (5%)
Treatment until PFS2

Observationn=279
Maintenancen=279
Observation/maintenance ongoing 13 (5%) 20 (7%)
No re-introduction CAPOX-B 54 (19%) 125 (45%)
Re-introduction CAPOX-B 212 (76%) 131 (47%)
No follow-up 0 3 (1%)
Reasons CAPOX-B was not re-introduced n=54 n=125
Persisting neurotoxicity 3 (6%) 15 (12%)
Other toxicities - 26 (21%)
Poor clinical condition 15 (28%) 19 (15%)
Patient refusal 8 (15%) 13 (10%)
Other 28 (52%) 52 (42%)
Treatment until PFS2

Results: TT2PD
SD or better after 6 cycles CAPOX- B
observation
R
capecitabine + bevacizumab
PD
TT2PD
PD
PFS1
any treatmentincl. CAPOX-B
• TT2PD = time to second progression of disease, time from randomization to progression upon any treatment given after PFS1

Observationn=279
Maintenancen=279
Observation/maintenance ongoing 13 (5%) 20 (7%)
No re-introduction CAPOX-B 54 (19%) 125 (45%)
Re-introduction CAPOX-B 212 (76%) 131 (47%)
No follow-up 0 3 (1%)
Treatment other than re-introduction CAPOX-B after PFS1
n=54 n=125
No treatment 29 (54%) 46 (37%)
Irinotecan 18 (33%) 53 (42%)
Anti-EGFR 0 10 (8%)
5FU-bevacizumab 4 (7%) 11 (9%)
Other 3 (6%) 5 (4%)
Treatment until 2nd progressionother than CAPOX-B

Time (mths)
TT
2P
D P
rob
ab
ility
0 6 12 18 24 30 36
0.0
0.2
0.4
0.6
0.8
1.0
279 247 174 97 52 36 13 Observation
279 251 187 134 87 52 31 Maintenance
Observation
Maintenance
median TT2PD - Observation : 15.0 (95% CI: 13.6 - 16.4 )
median TT2PD - Maintenance : 19.8 (95% CI: 18.0 - 21.9 )
ITT, events/n ( 223 / 279 - 251 / 279 )
HR= 0.67 ( 95% CI: 0.55 - 0.81 )
stratified log-rank p-value 0
TT2PD
Median TT2PD
Observation 15.0 m [95%CI:13.6-16.4]
Maintenance 19.8 m [95%CI: 18.0-21.9]
Stratified HR 0.67 [95%CI: 0.55-0.81]
p value < 0.00001
adjusted HR 0.63, p <0.001

Time (mths)
OS
Pro
ba
bili
ty
0 6 12 18 24 30 36
0.0
0.2
0.4
0.6
0.8
1.0
279 248 184 122 78 53 28 Observation
279 252 192 143 95 58 33 Maintenance
Observation
Maintenance
median OS - Observation : 18.2 (95% CI: 16.3 - 20.8 )
median OS - Maintenance : 21.7 (95% CI: 19.4 - 24.0 )
ITT, events/n ( 204 / 279 - 217 / 279 )
HR= 0.87 ( 95% CI: 0.71 - 1.06 )
stratified log-rank p-value 0.156
Overall SurvivalMedian OS
Observation 18.2 m [95%CI: 16.3-20.8]
Maintenance 21.7 m [95%CI: 19.4-24.0]
Stratified HR 0.87 [95%CI: 0.71-1.06]
p value 0.156
adjusted HR 0.80, p 0.035
preliminary survival analysis

Observationn = 279
Maintenancen = 279
Hypertension 18% 24%
Hematological toxicity NeutropeniaTrombocytopenia
00
2%1%
Diarrhea 1% 3%
Vomiting 1% 0.4%
Nausea 0 2%
Hand-foot syndrome 0 22%
Neurotoxicity 5% 10%
GI perforation 0 1%
Venous thromboembolic events 2% 3%
Fatigue 2% 4%
Toxicity (grade 3-4)during observation/maintenance

Observation
n=279Maintenance
n=279
4 drugs
capecitabine, oxaliplatin, bevacizumab, irinotecan
138 (49%) 136 (49%)
5 drugs
capecitabine, oxaliplatin, bevacizumab, irinotecan, anti-EGFR
34 (12%) 32 (11%)
Drugs administered during metastatic disease

Conclusions - I• Maintenance treatment with capecitabine plus
bevacizumab after 6 cycles CAPOX-B is feasible, and significantly prolongs PFS1 and PFS2
• The number of patients that was eligible for re-introduction of CAPOX-B is lower than expected
• When any treatment after PFS1 is considered, maintenance treatment also significantly prolongs the time to second progression (TT2PD)
• There is a non-significant benefit in median OS for maintenance treatment, which is significant in the adjusted analysis

Conclusions - II
• The percentage of patients that received 4 or 5 effective drugs during their metastatic disease is comparable in both treatment arms
• Therefore, time on treatment appears to be an additional relevant factor for overall survival in this study
• Our data support the use of maintenance treatment with capecitabine plus bevacizumab until progression or unacceptable toxicity after induction treatment of 6 cycles with CAPOX-B

DCCG CAIRO3 study - acknowledgementsInvestigators: C. Smorenburg, Alkmaar; R.Hoekstra, Almelo; C.Rodenburg, Amersfoort; G.Timmers, Amstelveen; A.Cats, M.Geenen, W. van Leeuwen, D.Richel, C.Punt, O.Leeksma, J.Otten Amsterdam; J.Douma, Arnhem; P.Nieboer,Assen; F.Valster, Bergen op Zoom; P. van den Berg Blaricum; O.Loosveld, A.Ten Tije Breda; D.Kehrer, Capelle a/d IJssel; M.Bos, Delft; Z.Erjavec,Delfzijl; H.Sinnige, Den Bosch; H.Sleeboom Den Haag; J.Berends, Den Helder; A.Imholz, Deventer; S.Hovenga, Drachten; E.Balk, Ede; G.Creemers, M.Dercksen, Eindhoven; M.Legdeur, Enschede; A.Smals, Geldrop; M. van Hennik, Gorinchem; A.van der Torren, Gouda; G.Hospers, R.de Jong, Groningen; M.Temizkan, Harderwijk; J.Wals, Heerlen; V.Derleyn, Helmond; E. Siemerink, Hengelo;J.Schrama, Hoofddorp; J.Haasjes, Hoogeveen; M.Polee, Leeuwarden;E. Batman, A.Gelderblom, J. van der Hoeven Leiden; R.Jansen, Maastricht; M.Los, Nieuwegein; C.Punt, C.Mandigers, Nijmegen; A.Vos, Oss; M.den Boer, Roermond; F.de Jongh, Rotterdam; J.Braun, Schiedam; F.Erdkamp, Sittard; G.Veldhuis, Sneek; C.Kruijtzer, Tiel; H.Roerdink, J. van Riel, Tilburg; S.van der Vegt, E.Voest, Utrecht; G.Vreugdenhil, Veldhoven; M.Werter, Venlo; P.Schiphorst, Winterswijk; A.van Bochove, Zaandam; H.Seinen, Zevenaar; A.Honkoop, Zwolle Statisticians: H, van Tinteren, O.Dalesio, Amsterdam Central Datamanagement: L.Mol, F.van Leeuwen, IKNL Nijmegen Independent Data Monitoring Committee: E. de Vries, E. vd Wall, J. Nortier, M. Buyse, K. Roest Supported by: Dutch Cancer Foundation, and unrestricted scientific grants from Roche, Sanofi-Aventis
Contact: email-address: [email protected]