Embed Size (px)
Citation preview
Student no: _____________ TALMID
Questionnaire no: ________ SHELON
Date: ___/______/_______ INTDATE
Ministry of Health Israel Center for Disease Control
Food and Nutrition Services
School: ________________ SCHOOL
Grade: ________________ CLASS
Sex: __________________ SEX 1=male, 2=female
1=present, 2=absent ABSENT Student present/absent: -
Reason for absence: free text ABSTXT
2
Hello.
The Ministry of Health is carrying out a national survey on the subject of health and nutrition among children
and adolescents. The aims of the survey are to assess the food intake and nutrition habits of Israeli children,
their health status and their views on nutrition–related topics. The information received from the survey will
serve as a basis for developing health promotion activities. Participation in the survey is not compulsory. We
thank you for your cooperation.
Instructions for completing the questionnaire:
1. The questionnaire is written in the male gender, but is intended for girls as well (unless stated
otherwise).
2. The questionnaire is for self-completion. The questions are numbered, and divided into sections. Each
section begins with a heading.
3. Please answer each question precisely according to the instructions.
If a question is not clear, please refer to the teacher/interviewer present in the class.
FOOD FREQUENCY QUESTIONNAIRE:
INSTRUCTIONS FOR FILLING OUT THE QUESTIONNAIRE:
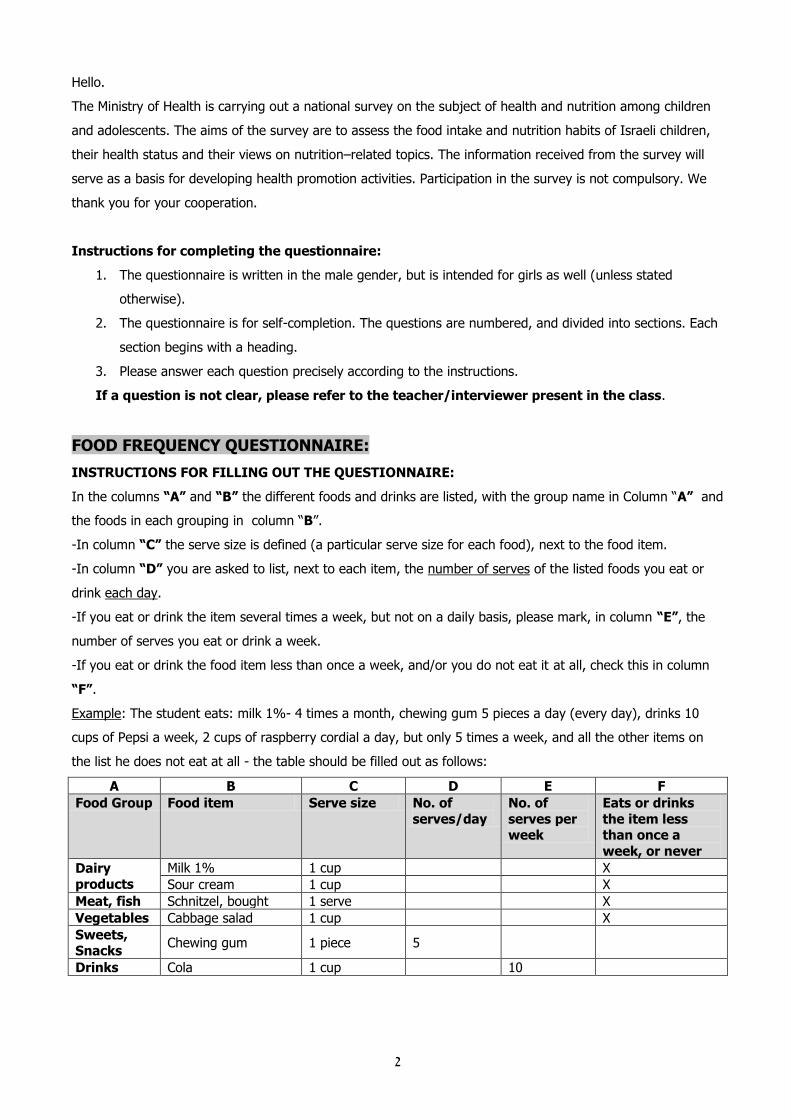
In the columns “A” and “B” the different foods and drinks are listed, with the group name in Column “A” and
the foods in each grouping in column “B”.
-In column “C” the serve size is defined (a particular serve size for each food), next to the food item.
-In column “D” you are asked to list, next to each item, the number of serves of the listed foods you eat or
drink each day.
-If you eat or drink the item several times a week, but not on a daily basis, please mark, in column “E”, the
number of serves you eat or drink a week.
-If you eat or drink the food item less than once a week, and/or you do not eat it at all, check this in column
“F”.
Example: The student eats: milk 1%- 4 times a month, chewing gum 5 pieces a day (every day), drinks 10
cups of Pepsi a week, 2 cups of raspberry cordial a day, but only 5 times a week, and all the other items on
the list he does not eat at all - the table should be filled out as follows:
A B C D E F
Food Group Food item Serve size No. of
serves/day
No. of
serves per week
Eats or drinks
the item less than once a
week, or never
Dairy products
Milk 1% 1 cup X
Sour cream 1 cup X
Meat, fish Schnitzel, bought 1 serve X
Vegetables Cabbage salad 1 cup X
Sweets, Snacks
Chewing gum 1 piece 5
Drinks Cola 1 cup 10
3
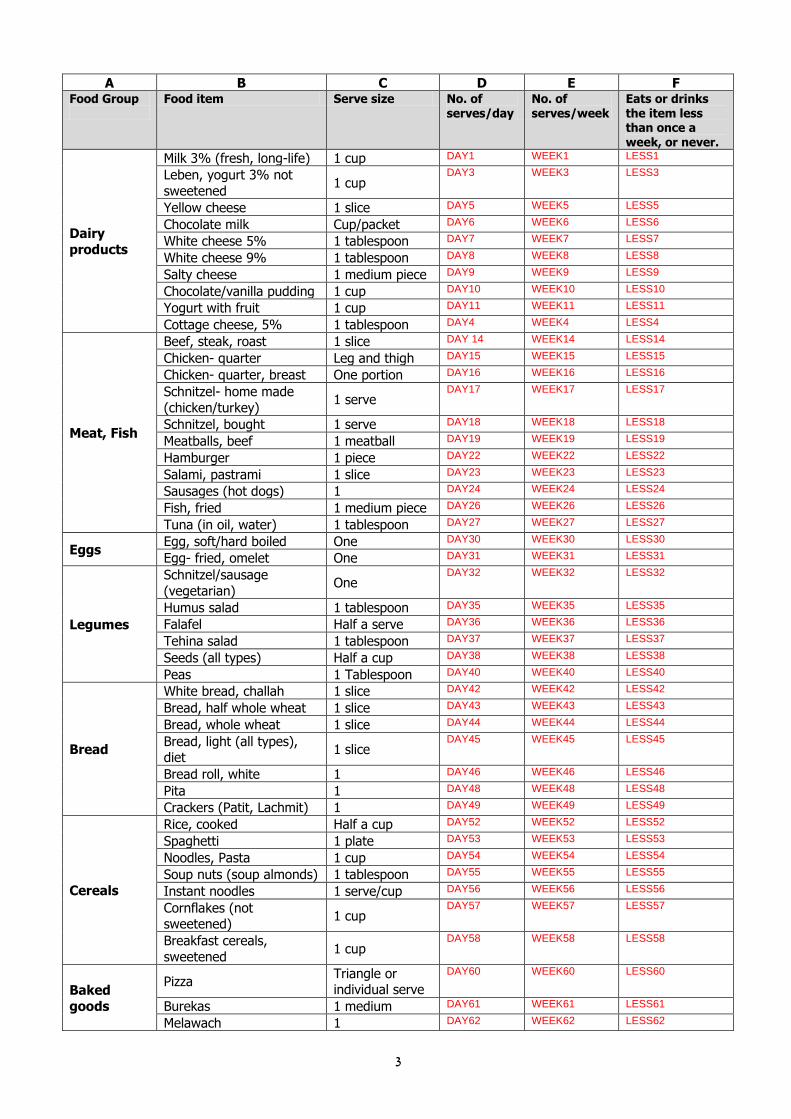
A B C D E F Food Group
Food item Serve size No. of serves/day
No. of serves/week
Eats or drinks the item less than once a week, or never.
Dairy
products
Milk 3% (fresh, long-life) 1 cup DAY1 WEEK1 LESS1
Leben, yogurt 3% not
sweetened 1 cup
DAY3 WEEK3 LESS3
Yellow cheese 1 slice DAY5 WEEK5 LESS5
Chocolate milk Cup/packet DAY6 WEEK6 LESS6
White cheese 5% 1 tablespoon DAY7 WEEK7 LESS7
White cheese 9% 1 tablespoon DAY8 WEEK8 LESS8
Salty cheese 1 medium piece DAY9 WEEK9 LESS9
Chocolate/vanilla pudding 1 cup DAY10 WEEK10 LESS10
Yogurt with fruit 1 cup DAY11 WEEK11 LESS11
Cottage cheese, 5% 1 tablespoon DAY4 WEEK4 LESS4
Meat, Fish
Beef, steak, roast 1 slice DAY 14 WEEK14 LESS14
Chicken- quarter Leg and thigh DAY15 WEEK15 LESS15
Chicken- quarter, breast One portion DAY16 WEEK16 LESS16
Schnitzel- home made
(chicken/turkey) 1 serve
DAY17 WEEK17 LESS17
Schnitzel, bought 1 serve DAY18 WEEK18 LESS18
Meatballs, beef 1 meatball DAY19 WEEK19 LESS19
Hamburger 1 piece DAY22 WEEK22 LESS22
Salami, pastrami 1 slice DAY23 WEEK23 LESS23
Sausages (hot dogs) 1 DAY24 WEEK24 LESS24
Fish, fried 1 medium piece DAY26 WEEK26 LESS26
Tuna (in oil, water) 1 tablespoon DAY27 WEEK27 LESS27
Eggs Egg, soft/hard boiled One DAY30 WEEK30 LESS30
Egg- fried, omelet One DAY31 WEEK31 LESS31
Legumes
Schnitzel/sausage
(vegetarian) One
DAY32 WEEK32 LESS32
Humus salad 1 tablespoon DAY35 WEEK35 LESS35
Falafel Half a serve DAY36 WEEK36 LESS36
Tehina salad 1 tablespoon DAY37 WEEK37 LESS37
Seeds (all types) Half a cup DAY38 WEEK38 LESS38
Peas 1 Tablespoon DAY40 WEEK40 LESS40
Bread
White bread, challah 1 slice DAY42 WEEK42 LESS42
Bread, half whole wheat 1 slice DAY43 WEEK43 LESS43
Bread, whole wheat 1 slice DAY44 WEEK44 LESS44
Bread, light (all types), diet
1 slice DAY45 WEEK45 LESS45
Bread roll, white 1 DAY46 WEEK46 LESS46
Pita 1 DAY48 WEEK48 LESS48
Crackers (Patit, Lachmit) 1 DAY49 WEEK49 LESS49
Cereals
Rice, cooked Half a cup DAY52 WEEK52 LESS52
Spaghetti 1 plate DAY53 WEEK53 LESS53
Noodles, Pasta 1 cup DAY54 WEEK54 LESS54
Soup nuts (soup almonds) 1 tablespoon DAY55 WEEK55 LESS55
Instant noodles 1 serve/cup DAY56 WEEK56 LESS56
Cornflakes (not sweetened)
1 cup DAY57 WEEK57 LESS57
Breakfast cereals,
sweetened 1 cup
DAY58 WEEK58 LESS58
Baked
goods
Pizza Triangle or individual serve
DAY60 WEEK60 LESS60
Burekas 1 medium DAY61 WEEK61 LESS61
Melawach 1 DAY62 WEEK62 LESS62

4
A B C D E F Food Group
Food item Serve size No. of serves/day
No. of serves/week
Eats or drinks the item less than once a week, or never.
Cookies 1 medium DAY63 WEEK63 LESS63
Chocolate cake 1 slice DAY64 WEEK64 LESS64
Chocolate yeast rolls One DAY65 WEEK65 LESS65
Wafers 1 wafer DAY66 WEEK66 LESS66
Fruit
Apple 1 DAY69 WEEK69 LESS69
Orange 1 DAY70 WEEK70 LESS70
Banana 1 DAY71 WEEK71 LESS71
Plums, peaches 2 DAY72 WEEK72 LESS72
Grapes 1 cup DAY73 WEEK73 LESS73
Fruit, dried 4 pieces DAY74 WEEK74 LESS74
Melon 1/4 melon DAY75 WEEK75 LESS75
Watermelon 1 slice DAY76 WEEK76 LESS76
Vegetables
French fries 1 cup DAY79 WEEK79 LESS79
Potato, mashed 1 cup DAY80 WEEK80 LESS80
Potatoes, baked 1 medium piece DAY81 WEEK81 LESS81
Green beans, cooked Half a cup DAY82 WEEK82 LESS82
Carrot, cooked Half a cup DAY83 WEEK83 LESS83
Sweet corn Half a cob or 3
tablespoons
DAY84 WEEK84 LESS84
Olives 1 DAY85 WEEK85 LESS85
Tomato 1 DAY86 WEEK86 LESS86
Cucumber 1 DAY87 WEEK87 LESS87
Fresh Vegetable salad 1 cup DAY88 WEEK88 LESS88
Cabbage salad 1 cup DAY89 WEEK89 LESS89
Pickled vegetables 3 pieces DAY90 WEEK90 LESS90
Vegetable soup 1 cup DAY91 WEEK91 LESS91
Fats, sauces
spreads
Margarine, butter 1 teaspoon DAY92 WEEK92 LESS92
Mayonnaise 1 tablespoon DAY94 WEEK94 LESS94
Chocolate spread 1 teaspoon DAY95 WEEK95 LESS95
Ketchup 1 tablespoon DAY97 WEEK97 LESS97
Sweeteners Sugar 1 teaspoon DAY98 WEEK98 LESS98
Honey/Jam 1 teaspoon DAY99 WEEK99 LESS99
Sweets, snacks
Bissli (extruded salty snack)
Small packet DAY102 WEEK102 LESS102
Bamba (extruded corn
snack) Small packet
DAY103 WEEK103 LESS103
Ice cream (on stick)-dairy 1 DAY104 WEEK104 LESS104
Popsicle 1 DAY105 WEEK105 LESS105
Ice cream 1 ball/scoop DAY106 WEEK106 LESS106
Chocolate 4 squares or 1 row
DAY107 WEEK107 LESS107
Chocolate bar - Pesek zman etc…..
1 DAY108 WEEK108 LESS108
Chewing gum 1 pellet/stick DAY109 WEEK109 LESS109
Candies 1 DAY110 WEEK110 LESS110
Beverages
Cola 1 cup DAY112 WEEK112 LESS112
Soft drink (not cola) 1 cup (1/4 liter) DAY113 WEEK113 LESS113
Soft drink, artificially
sweetened 1 cup (1/4 liter)
DAY114 WEEK114 LESS114
Beer 1 cup DAY115 WEEK115 LESS115
Wine 1 glass DAY116 WEEK116 LESS116
Tea 1 cup DAY117 WEEK117 LESS117
5
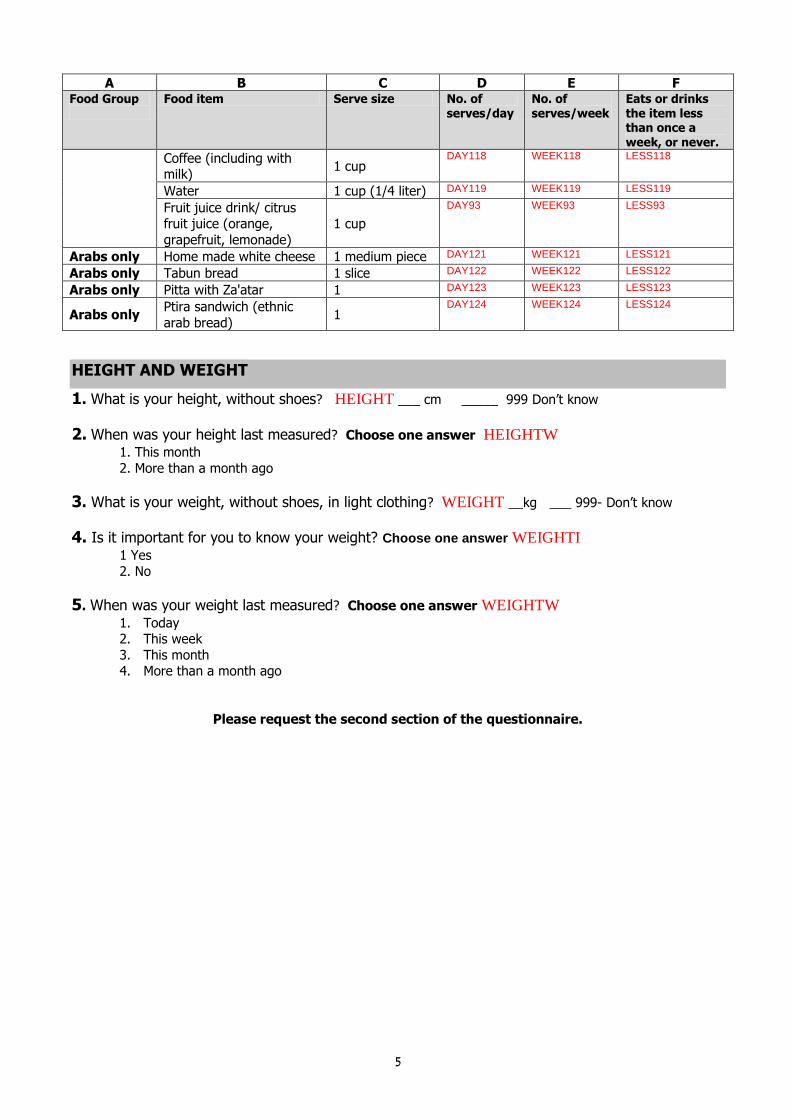
A B C D E F Food Group
Food item Serve size No. of serves/day
No. of serves/week
Eats or drinks the item less than once a week, or never.
Coffee (including with milk)
1 cup DAY118 WEEK118 LESS118
Water 1 cup (1/4 liter) DAY119 WEEK119 LESS119
Fruit juice drink/ citrus fruit juice (orange,
grapefruit, lemonade)
1 cup
DAY93 WEEK93 LESS93
Arabs only Home made white cheese 1 medium piece DAY121 WEEK121 LESS121
Arabs only Tabun bread 1 slice DAY122 WEEK122 LESS122
Arabs only Pitta with Za'atar 1 DAY123 WEEK123 LESS123
Arabs only Ptira sandwich (ethnic
arab bread) 1
DAY124 WEEK124 LESS124
HEIGHT AND WEIGHT
1. What is your height, without shoes? HEIGHT ___ cm _____ 999 Don’t know
2. When was your height last measured? Choose one answer HEIGHTW
1. This month
2. More than a month ago
3. What is your weight, without shoes, in light clothing? WEIGHT __kg ___ 999- Don’t know
4. Is it important for you to know your weight? Choose one answer WEIGHTI 1 Yes
2. No
5. When was your weight last measured? Choose one answer WEIGHTW
1. Today 2. This week
3. This month 4. More than a month ago
Please request the second section of the questionnaire.

6
SECTION 2 Class name _____Student no. _____questionnaire____
MEALS
6. Where did you eat yesterday? Check the appropriate box -one answer for each line.
At home Outside of home
Didn’t eat
Don’t remember
With
parent/ family
Alone At
school
Not at
school
Breakfast Y1_1 1 2 3 4 6 5
In between snack (morning snack) Y1_2
Lunch Y1_3
In between snack (afternoon snack) Y1_4
Dinner Y1_5
Night snack Y1_6
Other meal Y1_7 specify_______ Y1TXT
7. How many times a month do you eat fast food at home or away (falafel, hamburger, pizza)? Y2 _____times number
8. When do you usually eat your main meal (a large cooked meal)? Choose one answer Y3
1. In the morning
2. At lunchtime 3. In the evening
4. At lunchtime and in the evening 5. I don’t eat a main meal go to question 11
6. Other, specify: __________________________________ Y3 TXT
999. Don’t know
9. How many times a week do you eat your main meal in the company of an adult?number __ Y4
times
10. How many times a week do you sit alone (without adult company) to eat your main meal?
number__Y5 times
11. Does the quantity you eat usually change if you are with others? Choose one answer Y6
1. I eat less 2. I eat more
3. Sometimes I eat less, sometimes I eat more 4. I don’t eat less, and I don’t eat more
5. Don’t know
12. Do you eat at school? Choose one answer Y7
1. Yes, every day or almost every day go to question 13 2. Yes, occasionally go to question 13
3. No go to question 14
13. Who prepares the food you eat at school? You may choose more than one answer
1=yes 2=no to all answers 1. I myself Y8_1
2. Father/mother/ some other family member prepares for me Y8_2
3. I buy at school Y8_3 4. I buy outside school Y8_4
5. The school provides Y8_5

7
14. If you do not eat at school, what are the reasons? You may choose more than one answer
1=yes 2=no to all answers
1. I don’t have the time Y10_1
2. I am not hungry Y10_2
3. I don’t have any food with me Y10_3
4. They don’t prepare for me Y10_4
5. There is no cafeteria, kiosk Y10_5
6. I don't have money to buy in the cafeteria, kiosk Y10_6
7. Other Y10_7 specify: ____________ Y10txt ________
15. Does your school have? You may choose more than one answer 1=yes 2=no to all answers
1. A cafeteria or kiosk Y9_1 2. Organized catering, organized meals Y9_2 3. None of these Y9_3
16. In the last week, did you go to bed at night hungry (not because of dieting)? Y11
1. Yes 2. No
999. Don’t know
(If you answered “ yes”, go on to section ”Vegetarianism, Veganism”)
17. In the last month, did you go to bed hungry (not because of dieting)? Y12
1. Yes
2. No 999. Don’t know
VEGETARIANISM, VEGANISM 18. Do you avoid the following foods? Circle the appropriate answer
I avoid
1. Meat (beef, lamb, etc.) V4_1 Yes No
2. Chicken, turkey V4_2 Yes No
3. Fish V4_3 Yes No
4. Dairy products (including cheese, yogurt, puddings) V4_4 Yes No
5. Eggs V4_5 Yes No
6. Other V4_6 specify:__________ V4TXT Yes No
If you answered “no” to all the foods, go to the section “Body Image and Dieting”.
19. Why do you avoid these foods? You may choose more than one answer 1=yes 2=no to all
answers
1. I am a vegetarian or vegan V5_1 go to question 20
2. Family habit V5_2 3. I don’t like to eat them V5_3 go to the section “Body Image and Dieting”.
4. For health reasons V5_4 5. Other V5_5 specify: ____ V5TXT
20. From what age are you vegetarian or a vegan? (List your age in years) from age_______
V3 or 999 Don't know

8
BODY IMAGE AND DIETING
21. The following table relates to your attitudes regarding your body shape. Check the appropriate
box.
1. Fine 2.Too fat 3.Too thin
In my opinion, I am D1_1
In my opinion, others think I am D1_2
22. Here are a number of pictures, which depict different body shapes.
Boys
Girls
Please write, next to each question, the number of the picture you have selected as your answer. 1. How I currently see myself. picture number D2_1____number 1-5 or 999 Don't know
2. How my parents currently see me. picture number D2_2____ number 1-5 or 999 Don't know
3. How my friends currently see me. picture number D2_3___ number 1-5 or 999 Don't know
23. Have you ever made yourself vomit when you had a feeling of fullness/satiety? D3
1. Yes 2. No
3. Don’t know
24. Are you sometimes worried that you will lose control over the quantity of food you eat? D4
1. Yes 2. No
3. Don’t know
25. Have you ever reduced more than 3 kg in weight over a three-month period? D5
1. Yes 2. No
3. Don’t know
26. Do you think that you should be on any type of diet? D6
1. Yes 2. No
3. Don’t know
27.Are you currently on any type of diet such as for weight loss, weight maintenance, weight gain
for a medical reason (such as diabetes, growth problems, celiac, etc), or for another reason? D7
1. Yes 2. No
999. Don’t know
9
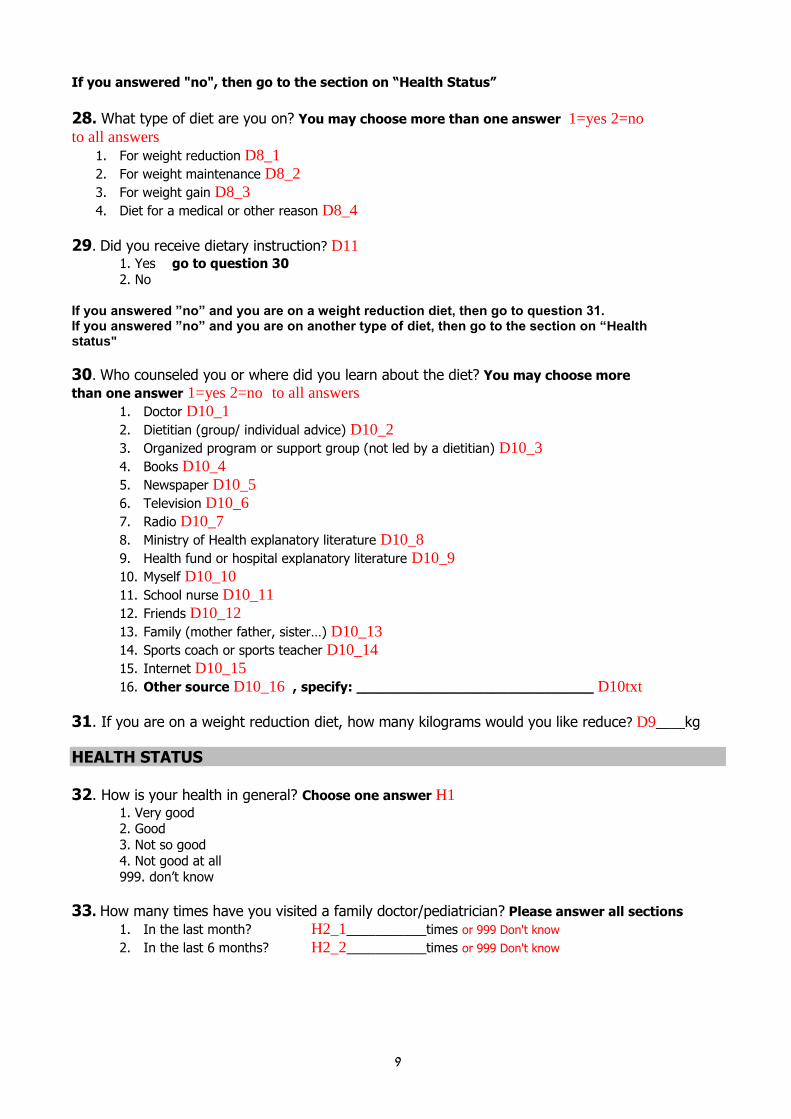
If you answered "no", then go to the section on “Health Status”
28. What type of diet are you on? You may choose more than one answer 1=yes 2=no
to all answers
1. For weight reduction D8_1
2. For weight maintenance D8_2
3. For weight gain D8_3
4. Diet for a medical or other reason D8_4
29. Did you receive dietary instruction? D11
1. Yes go to question 30
2. No If you answered ”no” and you are on a weight reduction diet, then go to question 31. If you answered ”no” and you are on another type of diet, then go to the section on “Health status"
30. Who counseled you or where did you learn about the diet? You may choose more
than one answer 1=yes 2=no to all answers
1. Doctor D10_1
2. Dietitian (group/ individual advice) D10_2
3. Organized program or support group (not led by a dietitian) D10_3
4. Books D10_4
5. Newspaper D10_5
6. Television D10_6
7. Radio D10_7
8. Ministry of Health explanatory literature D10_8
9. Health fund or hospital explanatory literature D10_9
10. Myself D10_10
11. School nurse D10_11
12. Friends D10_12
13. Family (mother father, sister…) D10_13
14. Sports coach or sports teacher D10_14
15. Internet D10_15
16. Other source D10_16 , specify: ____________________________ D10txt
31. If you are on a weight reduction diet, how many kilograms would you like reduce? D9____kg
HEALTH STATUS
32. How is your health in general? Choose one answer H1 1. Very good 2. Good
3. Not so good
4. Not good at all 999. don’t know
33. How many times have you visited a family doctor/pediatrician? Please answer all sections
1. In the last month? H2_1___________times or 999 Don't know
2. In the last 6 months? H2_2___________times or 999 Don't know
01
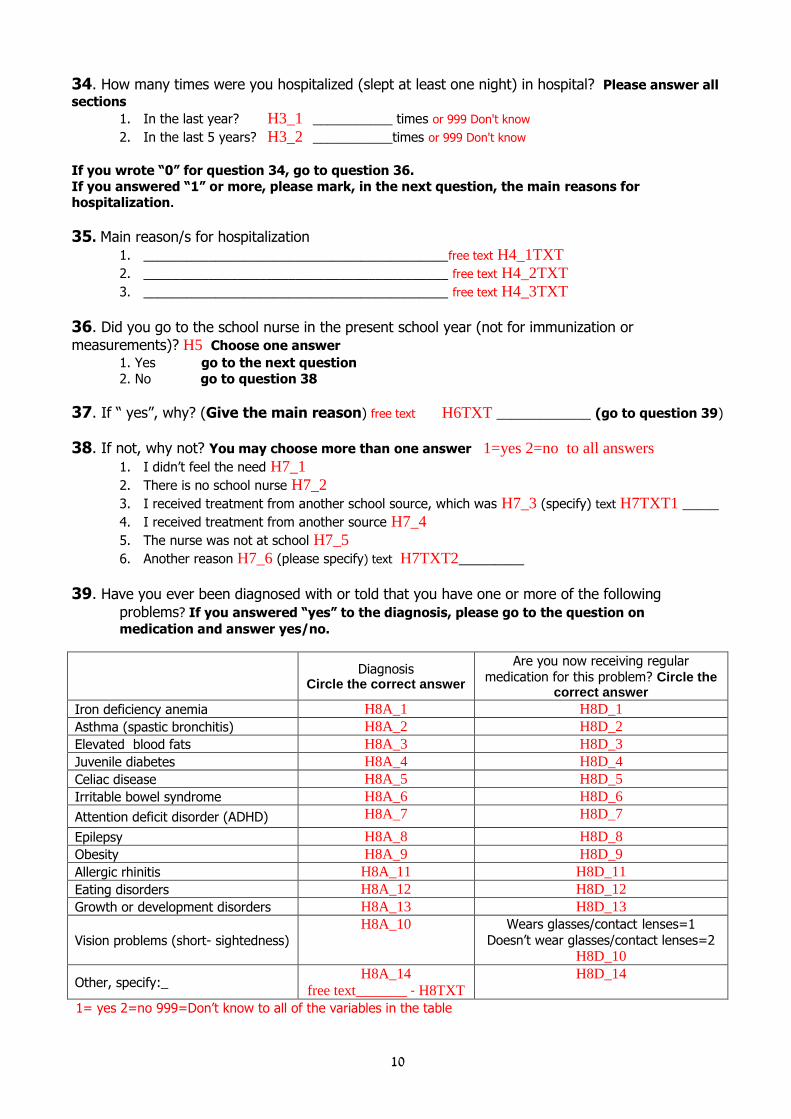
34. How many times were you hospitalized (slept at least one night) in hospital? Please answer all
sections
1. In the last year? H3_1 ___________ times or 999 Don't know
2. In the last 5 years? H3_2 ___________times or 999 Don't know
If you wrote “0” for question 34, go to question 36.
If you answered “1” or more, please mark, in the next question, the main reasons for hospitalization.
35. Main reason/s for hospitalization
1. __________________________________________free text H4_1TXT 2. __________________________________________ free text H4_2TXT 3. __________________________________________ free text H4_3TXT
36. Did you go to the school nurse in the present school year (not for immunization or
measurements)? H5 Choose one answer
1. Yes go to the next question
2. No go to question 38
37. If “ yes”, why? (Give the main reason) free text H6TXT _____________ (go to question 39)
38. If not, why not? You may choose more than one answer 1=yes 2=no to all answers
1. I didn’t feel the need H7_1
2. There is no school nurse H7_2
3. I received treatment from another school source, which was H7_3 (specify) text H7TXT1 _____
4. I received treatment from another source H7_4
5. The nurse was not at school H7_5
6. Another reason H7_6 (please specify) text H7TXT2_________
39. Have you ever been diagnosed with or told that you have one or more of the following
problems? If you answered “yes” to the diagnosis, please go to the question on
medication and answer yes/no.
Diagnosis
Circle the correct answer
Are you now receiving regular medication for this problem? Circle the
correct answer
Iron deficiency anemia H8A_1 H8D_1
Asthma (spastic bronchitis) H8A_2 H8D_2
Elevated blood fats H8A_3 H8D_3
Juvenile diabetes H8A_4 H8D_4
Celiac disease H8A_5 H8D_5
Irritable bowel syndrome H8A_6 H8D_6
Attention deficit disorder (ADHD) H8A_7 H8D_7
Epilepsy H8A_8 H8D_8
Obesity H8A_9 H8D_9
Allergic rhinitis H8A_11 H8D_11
Eating disorders H8A_12 H8D_12
Growth or development disorders H8A_13 H8D_13
Vision problems (short- sightedness)
H8A_10 Wears glasses/contact lenses=1
Doesn’t wear glasses/contact lenses=2 H8D_10
Other, specify:_ H8A_14
free text_______ - H8TXT
H8D_14
1= yes 2=no 999=Don’t know to all of the variables in the table

00
40. How many days were you absent from school in the past 4 weeks (not including Shabbat,
holidays)? H9 number_______days or 999= Don't know (If answered ”0”, move to the next section)
41. What were the main reasons for the absence? You may choose more than one answer
1=yes 2=no to all answers
1. Illness H10_1
2. Didn’t feel like going to school H10_2
3. Tiredness H10_3
4. Trip or family celebration, event H10_4
5. Other H10_5 , specify: free text ______________ H10TXT
Boys: go to the section “ Questions for Boys” on the next page.
QUESTIONS FOR GIRLS 42. Have you started to menstruate? F1
1. Yes
2. No If you answered "no" go to the section on “Smoking”
43. At what age did you start to menstruate? At age: F2______________
44. Is your monthly period regular every 21-35 days? F3
1. Yes go to question 46 2. No
999. Don’t know
45. How many monthly periods have you had in the last year? Choose one answer F4
1. 0 2. 1-2
3. 3-6 4. 7 or more
999. Don’t know
46. Are you currently taking oral contraceptives (also for treatment of skin conditions or as other
treatment)? F5
1. Yes 2. No
999. Don’t know
Girls - go on to the section on ”Smoking”
QUESTIONS FOR BOYS
47. At what age did your voice change? Number B2 __________years or 999 Don't know
SMOKING 48. In your opinion, should cigarette smoking under the age of 18 be banned?Choose one answer S1
1. Yes
2. No
3. I don’t have an opinion
02
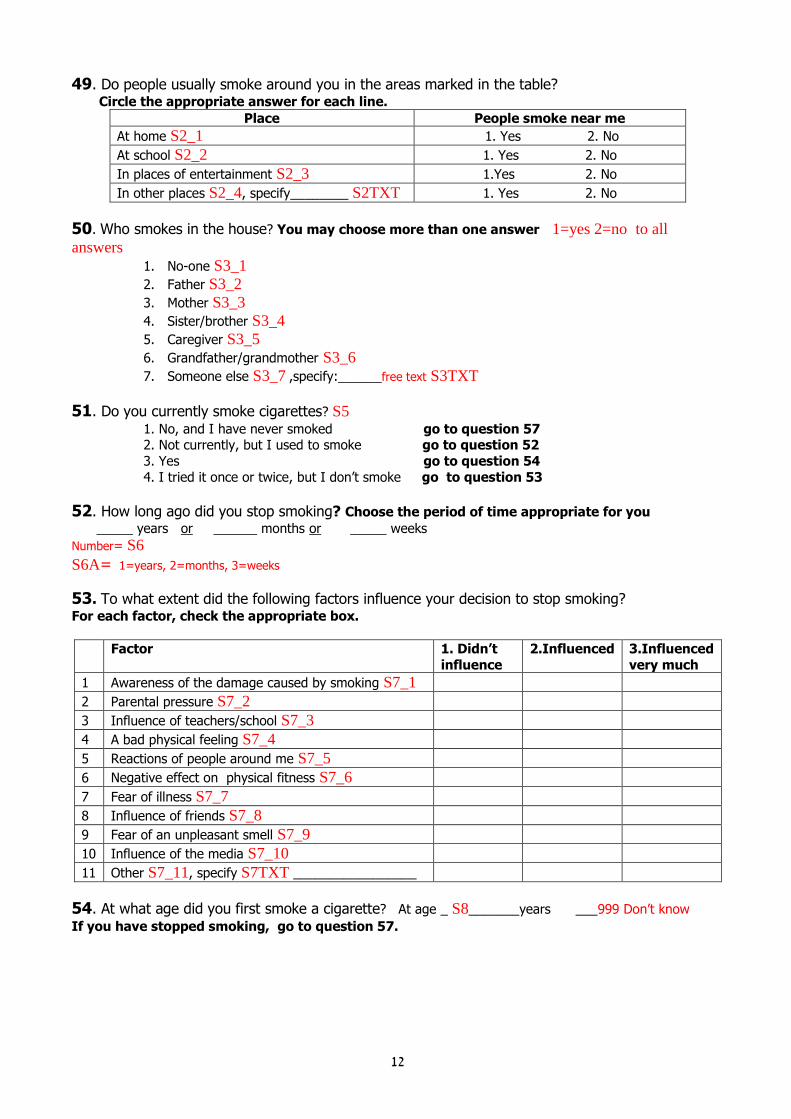
49. Do people usually smoke around you in the areas marked in the table?
Circle the appropriate answer for each line.
Place People smoke near me
At home S2_1 1. Yes 2. No
At school S2_2 1. Yes 2. No
In places of entertainment S2_3 1.Yes 2. No
In other places S2_4, specify________ S2TXT 1. Yes 2. No
50. Who smokes in the house? You may choose more than one answer 1=yes 2=no to all
answers 1. No-one S3_1
2. Father S3_2
3. Mother S3_3
4. Sister/brother S3_4
5. Caregiver S3_5
6. Grandfather/grandmother S3_6
7. Someone else S3_7 ,specify:______free text S3TXT
51. Do you currently smoke cigarettes? S5
1. No, and I have never smoked go to question 57
2. Not currently, but I used to smoke go to question 52
3. Yes go to question 54
4. I tried it once or twice, but I don’t smoke go to question 53
52. How long ago did you stop smoking? Choose the period of time appropriate for you _____ years or ______ months or _____ weeks
Number= S6
S6A= 1=years, 2=months, 3=weeks
53. To what extent did the following factors influence your decision to stop smoking?
For each factor, check the appropriate box.
Factor 1. Didn’t
influence
2.Influenced 3.Influenced
very much
1 Awareness of the damage caused by smoking S7_1
2 Parental pressure S7_2
3 Influence of teachers/school S7_3
4 A bad physical feeling S7_4
5 Reactions of people around me S7_5
6 Negative effect on physical fitness S7_6
7 Fear of illness S7_7
8 Influence of friends S7_8
9 Fear of an unpleasant smell S7_9
10 Influence of the media S7_10
11 Other S7_11, specify S7TXT _________________
54. At what age did you first smoke a cigarette? At age _ S8_______years ___999 Don’t know
If you have stopped smoking, go to question 57.

03
55. Mark the reason/s you smoke. You may choose more than one answer 1=yes 2=no to all
answers
1. I enjoy smoking S9_1 2. In order to be accepted by my friends S9_2 3. They smoke at home S9_3 4. Smoking helps me slim down/ not gain weight S9_4 5. My friends smoke S9_5
6. A feeling of maturity S9_6 7. Other S9_7 , specify:free text ____________ S9TXT
56. How many cigarettes do you usually smoke? (Mark the number per day or per week)
S10 (number of cigarettes) _________ per day OR _________per week
S10A: 1= day 2= week
57. Do you currently smoke a hookah? S11
1. No, and I have never smoked
2. Not currently, but I used to smoke 3. Yes
4. I tried once or twice, but I don’t smoke
ALCOHOL INTAKE
58. Have you ever drunk an alcoholic drink? C1
1. Yes
2. No
If you answered “no” go to the section on “Activity”
59. During the past month, did you drink any alcoholic drink? C2 Choose one answer
1. Yes
2. No
If you answered “no” go to the section on “Activity”
60. What do you usually drink, and in what setting? Check the appropriate boxes. If in “another
setting”, please write when and where.
Type of drink
On Shabbat/
festivals as kiddush
Weekdays at
home
At a
discotheque/club
With friends
(not in a club)
Other, specify:
_______
Beer C3A_1 C3B_1 C3C_1 C3D_1
C3TXT1text
Red wine C3A_2 C3B_2 C3C_2
C3D_2
C3TXT2 text
White wine C3A_3 C3B_3 C3C_3
C3D_3
C3TXT3 text
Other drink text
C3TXT01,_______
C3A_4 C3B_4 C3C_4
C3D_4
C3TXT4 text
Other drink text
C3TXT02,______ C3A_5 C3B_5 C3C_5
C3D_5
C3TXT5 text
Other drink text
C3TXT03,_______ C3A_6 C3B_6 C3C_6
C3D_6
C3TXT6 text
1= yes to all of the variables in the table
If you only drink within the Kiddush setting, then go to the section on “Activity”

04
If you drink outside of the Kiddush setting, then go on to question 61, and in each box, write the
name of one of the types of drink you mentioned in question 60, and continue to fill out the table
with questions 62,63.
61.How much did you drink?
Note each separate type of drink you
mentioned in question 60 in a separate line, and then go onto
questions 62 and 63.
62. How often did you
drink the drink? Choose
one answer
63. How much on average did you
drink each time? Write the amount
on one line
Type of drink _______ Text C4TXT1 1. 4-7 times a week
2. 1-3 times a week 3. 1-3 times a month
4. Less than once a month 5. Don’t know
C5_1
1= Sips 2= Small glasses 3= Glasses 4= Other, specify: ____ text C6TXT1
5= Don’t know C6A_1= number of drinks
C6B_1= drink/serve size (1-5 from the
above)
Type of drink _______ Text C4TXT2
1. 4-7 times a week
2. 1-3 times a week 3. 1-3 times a month
4. Less than once a month
5. Don’t know C5_2
____Sips (1) ____Small glasses (2) ____Glasses (3)
____Other,(4) specify: _____ text C6TXT2
____Don’t know (5) C6A_2 = number of drinks
C6B_2 = drink/serve size (1-5 from the
above)
Type of drink _______ Text C4TXT3 1. 4-7 times a week
2. 1-3 times a week
3. 1-3 times a month
4. Less than once a month 5. Don’t know
C5_3
____ Sips (1) ____ Small glasses (2) _____Glasses (3) _____Other, (4) specify: ____ text C6TXT3
_____Don’t know (5) C6A_3 = number of drinks
C6B_3= drink/serve size (1-5 from the
above)
ACTIVITY 64. How many times a day are you usually involved in the following activities? Check the appropriate box for each line
1.Up to
½ hour
2.Between ½-2
hours
3.More than 2
hours
4.Not at
all
Watching television or video, or listening to music P1_1
Working on the computer P1_2
Preparing homework or reading P1_3
Talking on the telephone P1_4
Playing a musical instrument or singing P1_5

05
65. How often do you take part in the following activities? On each line, write the number of times
a week or month. ( If you don’t engage in this activity, check “ don’t do”)
No. of times/ week No. of times/ month Don’t do
Sport, exercise P2A_1 _____times P2B_1 ____times P2C_1 Trips, hikes P2A_2 ______times P2B_2 _____times P2C_2 Youth movement P2A_3 ______times P2B_3 _____times P2C_3 At a club P2A_4 ______times P2B_4 _____times P2C_4 Work in the home (specify type: text___) P2TXT5 P2A_5 ______times P2B_5 _____times P2C_5 Work outside home (specify type: text __) P2TXT6 P2A_6 ______times P2B_6 _____times P2C_6 Other, specify: text _________ P2TXT7 P2A_7 ______times P2B_7 _____times P2C_7 In the following table, you are asked to specify all the physical activity you do at school and
outside of school, such as running, swimming, football, walking/cycling to school and others.
66. Which
activity do you do?
67. Where
does the activity take
place?
68. How often do
you do this activity?
69. How long does
the activity last each time?
70. What is
the degree of difficulty of the
activity?
71. How many
years have you engaged in this
activity?
Type: ________
Text P4TXT1
Text_________ PWHR1
1.4 times/week or more
2.1-3 times/week
3.2-3 times/month 4.Once a month or Less P5_1
Number of minutes_____ P6_1
1. Difficult 2.Moderate
3. Easy P7_1
1.Less than 1 year
2.Between 1-5
years 3.More than 5 years P8_1
Type: _________
Text P4TXT2
Text_________ PWHR2
1. 4 times/week or more
2. 1-3 times/week
3. 2-3 times/month 4. Once a month or less P5_2
Number of minutes_____ P6_2
1. Difficult 2.Moderate
3. Easy P7_2
1. Less than 1 year
2. Between 1-5
years 3. More than 5 years P8_2
Type:
_________
Text P4TXT3
Text_________
PWHR3
1. 4 times/week or
more
2. 1-3 times/week 3. 2-3 times/month
4. Once a month or less P5_3
Number of
minutes_____ P6_3
1. Difficult
2.Moderate
3. Easy P7_3
1. Less than 1
year
2. Between 1-5 years
3. More than 5 years P8_3
Type: _________
Text P4TXT4
Text_________ PWHR4
1. 4 times/week or more
2. 1-3 times/week
3. 2-3 times/month 4. Once a month or less P5_4
Number of minutes_____ P6_4
1. Difficult 2.Moderate
3. Easy P7_4
1. Less than 1 year
2. Between 1-5
years 3. More than 5 years P8_4
72. Why do you exercise? You may choose more than one answer 1=yes 2=no to all answers
1. It’s fun, I enjoy it P9_1
2. It is healthy P9_2
3. My friends are there P9_3
4. My parents want it P9_4
5. I want to be a sportsman P9_5
6. I want to be physically fit P9_6
7. Other P9_7, specify:text _____________________________ P9TXT
06
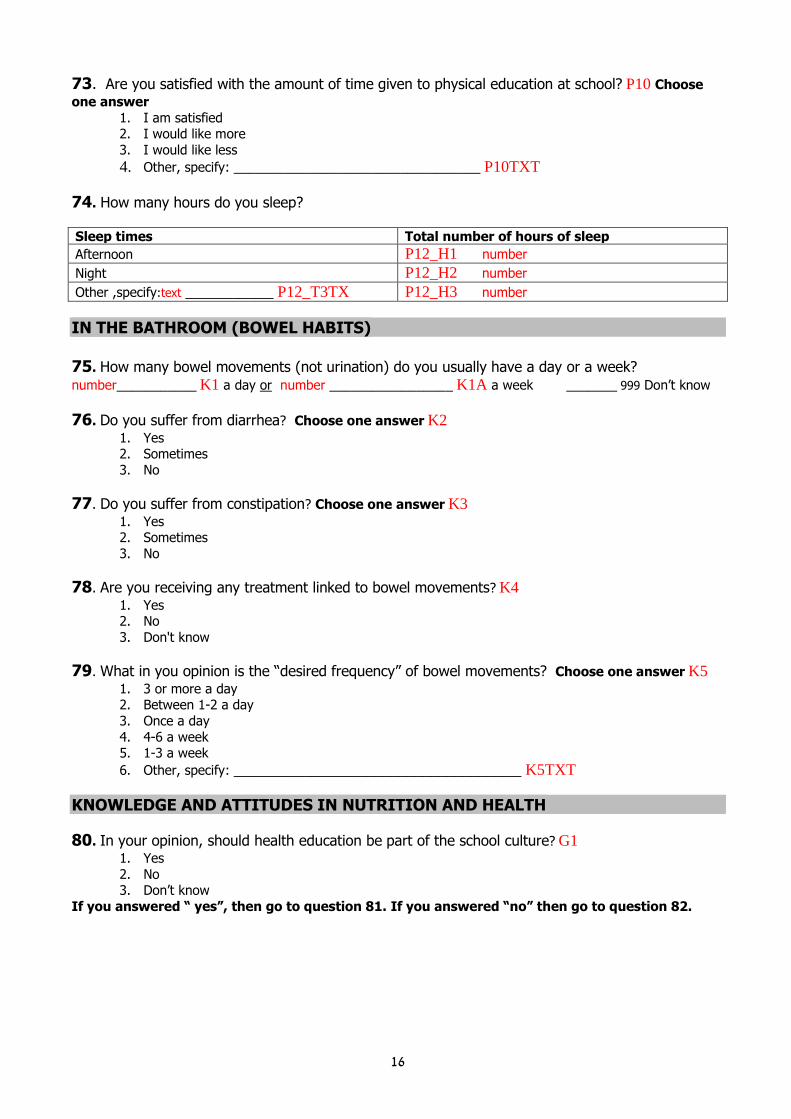
73. Are you satisfied with the amount of time given to physical education at school? P10 Choose
one answer
1. I am satisfied 2. I would like more
3. I would like less
4. Other, specify: __________________________________ P10TXT
74. How many hours do you sleep?
Sleep times Total number of hours of sleep
Afternoon P12_H1 number
Night P12_H2 number
Other ,specify:text ___________ P12_T3TX P12_H3 number
IN THE BATHROOM (BOWEL HABITS) 75. How many bowel movements (not urination) do you usually have a day or a week? number___________ K1 a day or number _________________ K1A a week _______ 999 Don’t know
76. Do you suffer from diarrhea? Choose one answer K2
1. Yes 2. Sometimes
3. No
77. Do you suffer from constipation? Choose one answer K3
1. Yes 2. Sometimes
3. No
78. Are you receiving any treatment linked to bowel movements? K4
1. Yes 2. No
3. Don't know
79. What in you opinion is the “desired frequency” of bowel movements? Choose one answer K5
1. 3 or more a day 2. Between 1-2 a day
3. Once a day
4. 4-6 a week 5. 1-3 a week
6. Other, specify: ____________________________________ K5TXT
KNOWLEDGE AND ATTITUDES IN NUTRITION AND HEALTH
80. In your opinion, should health education be part of the school culture? G1
1. Yes
2. No 3. Don’t know
If you answered “ yes”, then go to question 81. If you answered “no” then go to question 82.
07
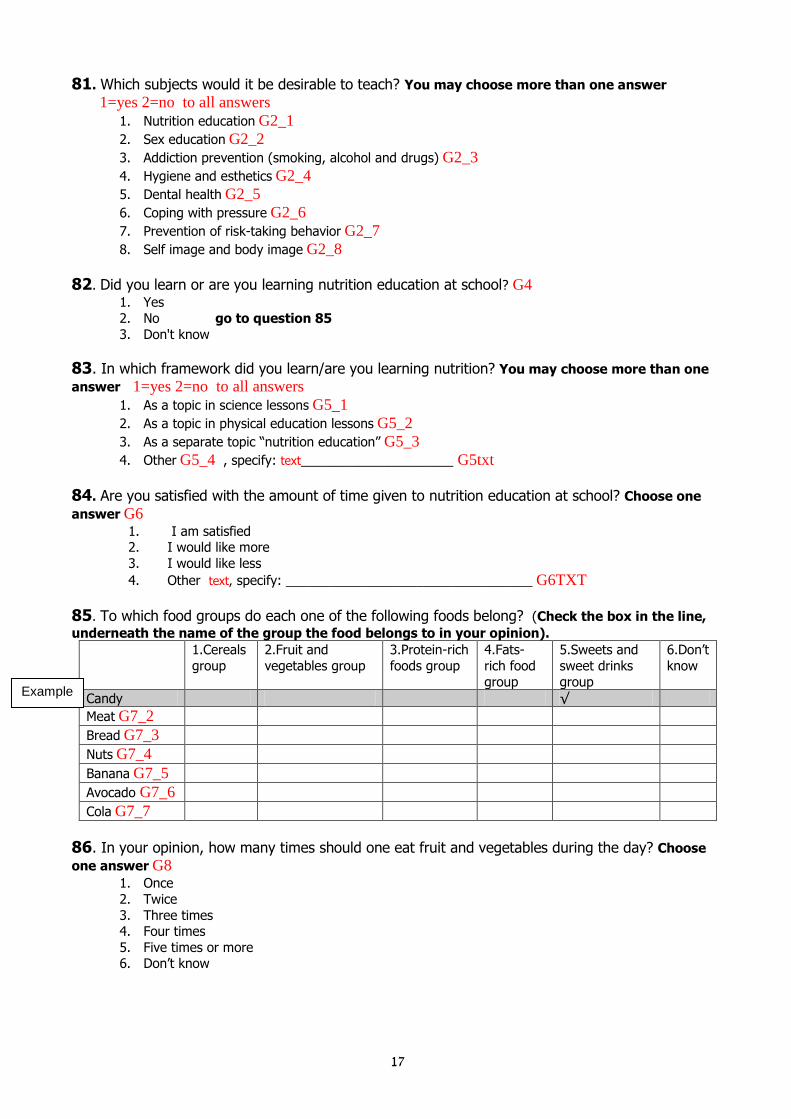
81. Which subjects would it be desirable to teach? You may choose more than one answer 1=yes 2=no to all answers
1. Nutrition education G2_1
2. Sex education G2_2
3. Addiction prevention (smoking, alcohol and drugs) G2_3
4. Hygiene and esthetics G2_4
5. Dental health G2_5
6. Coping with pressure G2_6
7. Prevention of risk-taking behavior G2_7
8. Self image and body image G2_8
82. Did you learn or are you learning nutrition education at school? G4
1. Yes
2. No go to question 85
3. Don't know
83. In which framework did you learn/are you learning nutrition? You may choose more than one
answer 1=yes 2=no to all answers
1. As a topic in science lessons G5_1
2. As a topic in physical education lessons G5_2
3. As a separate topic “nutrition education” G5_3
4. Other G5_4 , specify: text_____________________ G5txt
84. Are you satisfied with the amount of time given to nutrition education at school? Choose one
answer G6
1. I am satisfied 2. I would like more
3. I would like less
4. Other text, specify: __________________________________ G6TXT
85. To which food groups do each one of the following foods belong? (Check the box in the line,
underneath the name of the group the food belongs to in your opinion).
1.Cereals
group
2.Fruit and
vegetables group
3.Protein-rich
foods group
4.Fats-
rich food
group
5.Sweets and
sweet drinks
group
6.Don’t
know
Candy √
Meat G7_2
Bread G7_3
Nuts G7_4
Banana G7_5
Avocado G7_6
Cola G7_7
86. In your opinion, how many times should one eat fruit and vegetables during the day? Choose
one answer G8
1. Once
2. Twice
3. Three times 4. Four times
5. Five times or more 6. Don’t know
Example
08
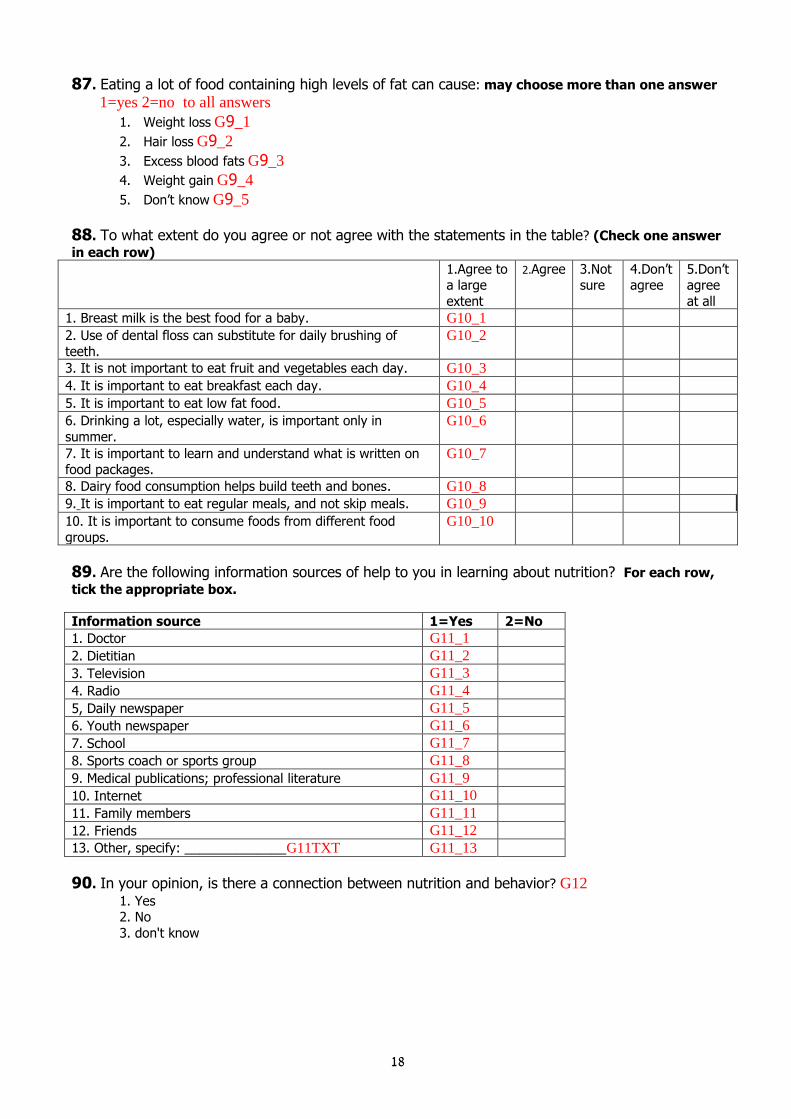
87. Eating a lot of food containing high levels of fat can cause: may choose more than one answer
1=yes 2=no to all answers
1. Weight loss G9_1
2. Hair loss G9_2
3. Excess blood fats G9_3
4. Weight gain G9_4
5. Don’t know G9_5
88. To what extent do you agree or not agree with the statements in the table? (Check one answer
in each row)
1.Agree to a large
extent
2.Agree 3.Not sure
4.Don’t agree
5.Don’t agree
at all
1. Breast milk is the best food for a baby. G10_1
2. Use of dental floss can substitute for daily brushing of
teeth.
G10_2
3. It is not important to eat fruit and vegetables each day. G10_3
4. It is important to eat breakfast each day. G10_4
5. It is important to eat low fat food. G10_5
6. Drinking a lot, especially water, is important only in
summer.
G10_6
7. It is important to learn and understand what is written on food packages.
G10_7
8. Dairy food consumption helps build teeth and bones. G10_8
9. It is important to eat regular meals, and not skip meals. G10_9
10. It is important to consume foods from different food
groups.
G10_10
89. Are the following information sources of help to you in learning about nutrition? For each row,
tick the appropriate box.
Information source 1=Yes 2=No
1. Doctor G11_1
2. Dietitian G11_2
3. Television G11_3
4. Radio G11_4
5, Daily newspaper G11_5
6. Youth newspaper G11_6
7. School G11_7
8. Sports coach or sports group G11_8
9. Medical publications; professional literature G11_9
10. Internet G11_10
11. Family members G11_11
12. Friends G11_12
13. Other, specify: ______________G11TXT G11_13
90. In your opinion, is there a connection between nutrition and behavior? G12
1. Yes 2. No
3. don't know

09
91. When you are stressed or irritable, does this affect the amount you eat? Choose one answer
G13
1. Yes
2. No 3. Don’t know
If you answered “no” or “ don’t know” then go to question 93.
92. Do you eat less or more when you are stressed or irritable? Choose one answer G14
1. I eat less
2. I eat more
3. Some times I eat more, sometimes less
93. Do you read the food label on food and drink containers? Choose one answer G15
1. Always
2. Often
3. Sometimes 4. Never If you answered “never” then go onto the next section “ General Questions”
94. Do you usually check the presence of the following components of the food label? (Check the
appropriate box, for each row.)
1=Yes 2=No
List of ingredients (flour, eggs… ) G16_1
Preservatives G16_2
Food colors G16_3
Nutrition claims (low fat, low sugar, lite….) G16_4
Nutrition labelling (calories, protein, etc per 100 gram) G16_5
Prizes or presents G16_6
Another component:___________________________________ G16TXT G16_7
GENERAL QUESTIONS
95. How old are you?number of years and number of months _______agen (write number of years and
months)
96. In which country were you born? If not in Israel, please write the name of the country BORN
1. Israel =1
2. Other country, specify_____ number, according to country code 3. Don’t know=3
If you answered “Israel”, then go to question 98.
97. What year did you immigrate to Israel? ___ year If you don't know, pick “ Don’t know” 999 __
ALIYAY
21
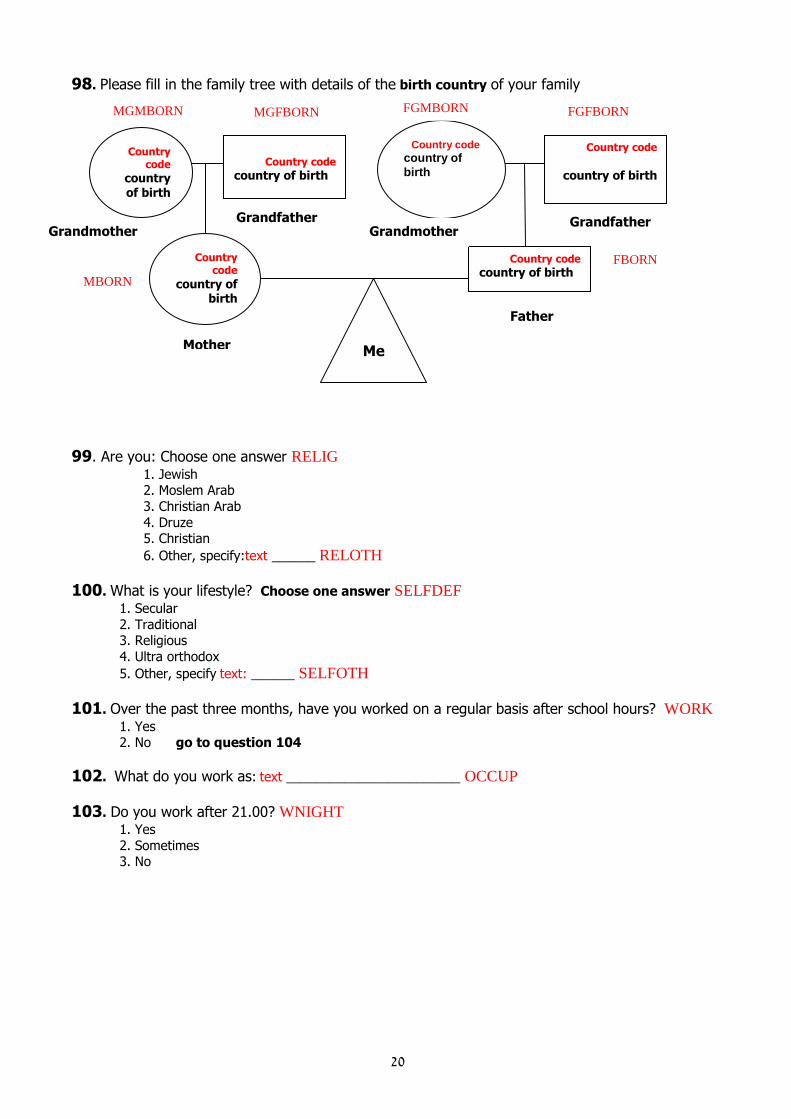
98. Please fill in the family tree with details of the birth country of your family
99. Are you: Choose one answer RELIG
1. Jewish 2. Moslem Arab
3. Christian Arab
4. Druze 5. Christian
6. Other, specify:text ______ RELOTH
100. What is your lifestyle? Choose one answer SELFDEF
1. Secular
2. Traditional 3. Religious
4. Ultra orthodox
5. Other, specify text: ______ SELFOTH
101. Over the past three months, have you worked on a regular basis after school hours? WORK
1. Yes 2. No go to question 104
102. What do you work as: text ________________________ OCCUP
103. Do you work after 21.00? WNIGHT
1. Yes
2. Sometimes 3. No
Country code
country of
birth
Country code
country of birth
Country code
country of birth
Country code
country of birth
Country code
country of birth
Country code
country of birth
_____
___
Grandfather Grandmother
Grandfather
Grandmother
Mother
Father
Me
FGMBORN FGFBORN
MGMBORN MGFBORN
FBORN
MBORN
20
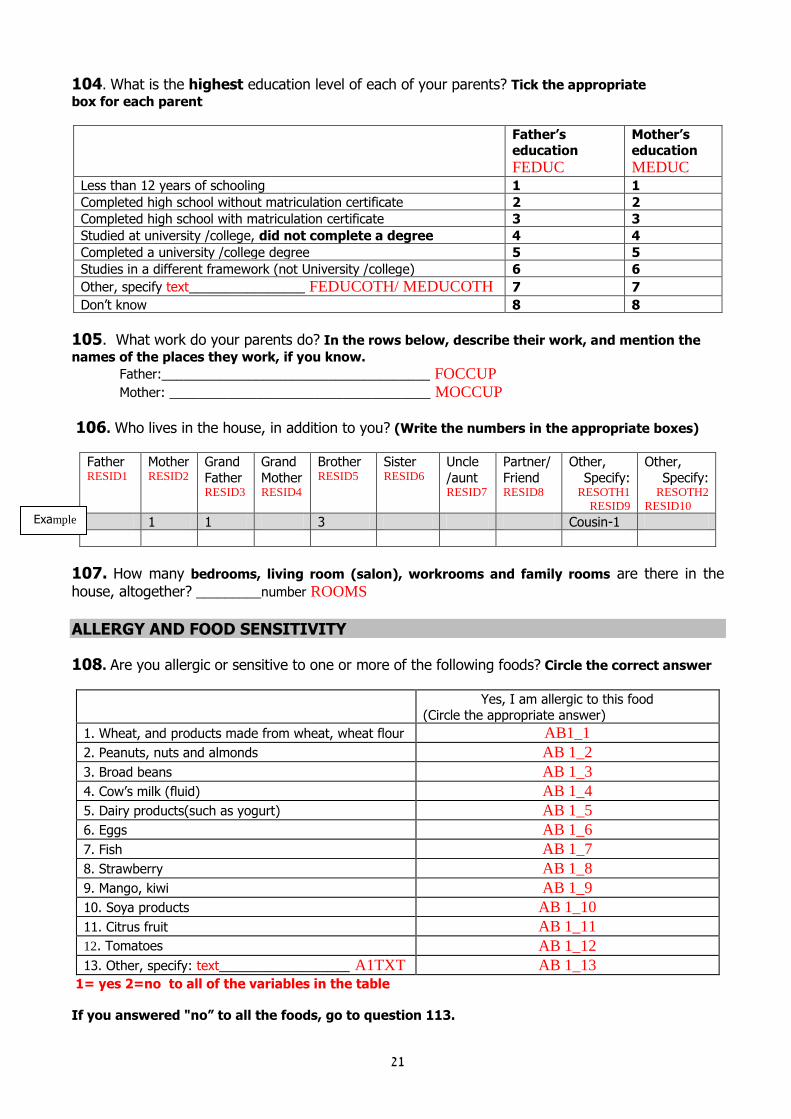
104. What is the highest education level of each of your parents? Tick the appropriate
box for each parent
Father’s education FEDUC
Mother’s education MEDUC
Less than 12 years of schooling 1 1
Completed high school without matriculation certificate 2 2
Completed high school with matriculation certificate 3 3
Studied at university /college, did not complete a degree 4 4
Completed a university /college degree 5 5
Studies in a different framework (not University /college) 6 6
Other, specify text________________ FEDUCOTH/ MEDUCOTH 7 7
Don’t know 8 8
105. What work do your parents do? In the rows below, describe their work, and mention the
names of the places they work, if you know.
Father:_____________________________________ FOCCUP
Mother: ____________________________________ MOCCUP
106. Who lives in the house, in addition to you? (Write the numbers in the appropriate boxes)
Father RESID1
Mother RESID2
Grand
Father RESID3
Grand
Mother RESID4
Brother RESID5
Sister RESID6
Uncle
/aunt RESID7
Partner/
Friend RESID8
Other,
Specify: RESOTH1
RESID9
Other,
Specify: RESOTH2
RESID10
1 1 3 Cousin-1
107. How many bedrooms, living room (salon), workrooms and family rooms are there in the
house, altogether? _________number ROOMS
ALLERGY AND FOOD SENSITIVITY
108. Are you allergic or sensitive to one or more of the following foods? Circle the correct answer
Yes, I am allergic to this food (Circle the appropriate answer)
1. Wheat, and products made from wheat, wheat flour AB1_1
2. Peanuts, nuts and almonds AB 1_2
3. Broad beans AB 1_3
4. Cow’s milk (fluid) AB 1_4
5. Dairy products(such as yogurt) AB 1_5
6. Eggs AB 1_6
7. Fish AB 1_7
8. Strawberry AB 1_8
9. Mango, kiwi AB 1_9
10. Soya products AB 1_10
11. Citrus fruit AB 1_11
12. Tomatoes AB 1_12
13. Other, specify: text__________________ A1TXT AB 1_13
1= yes 2=no to all of the variables in the table
If you answered "no” to all the foods, go to question 113.
Example

22
109. Who told you that you are allergic or sensitive to food? You can choose more than one
answer 1=yes 2=no to all answers
1. Doctor A2_1
2. Dietitian A2_2
3. Nurse A2_3
4. Alternative practitioner or homeopath A2_4
5. I myself A2_5
6. Parents, family members A2_6
7. Friends A2_7
8. Other A2_8, specify:text________________________ A2TXT
9. Don’t know/don’t remember A2_9
110. Which tests did you undergo for the diagnosis of the allergy or food sensitivity? You can
choose more than one answer 1=yes 2=no to all answers
1. Skin tests A3_1
2. Blood tests (RAST) A3_2
3. Other A3_3 , specify: ____________________________________ A3TXT
4. I did not undergo tests for diagnosis A3_4
111. At what age was your allergy/sensitivity diagnosed? At age number A4 _____ don’t know 999 Please note the age or check “Don’t know”.
112. Who checks that you don’t eat food to which you are sensitive or allergic? You can choose
more than one answer 1=yes 2=no to all answers
1. I myself A5_1
2. Mother, father A5_2
3. Someone else A5_3 , specify: A5TXT _____________________________________
4. No-one (I also don’t check) A5_4
113. Are you allergic or sensitive to one or more of the following factors?
Factor Yes, I am allergic to this factor (Circle the appropriate answer)
1. Dust, dust mites A6_1
2. Household pets such as a cat, dog A6_2
3. Grass A6_3
4. Olive trees A6_4
* 1= yes 2=no 3= don’t know to all of the variables in the table If you marked “no” for all the factors, then go on to the next section “ Nutrition Supplements”
114. Which tests did you undergo for the diagnosis of the allergy or sensitivity to the factors
mentioned in Table 113? You can choose more than one answer 1=yes 2=no to all answers
1. Skin tests A7_1
2. Blood tests (RAST) A7_2
3. Other A7_3 , specify: _____________________________________ A7TXT
4. I did not undergo tests for diagnosis A7_4
115. At what age was your allergy/sensitivity diagnosed? At age number A8 _____ don’t know999
Please note the age or check “ don’t know
23
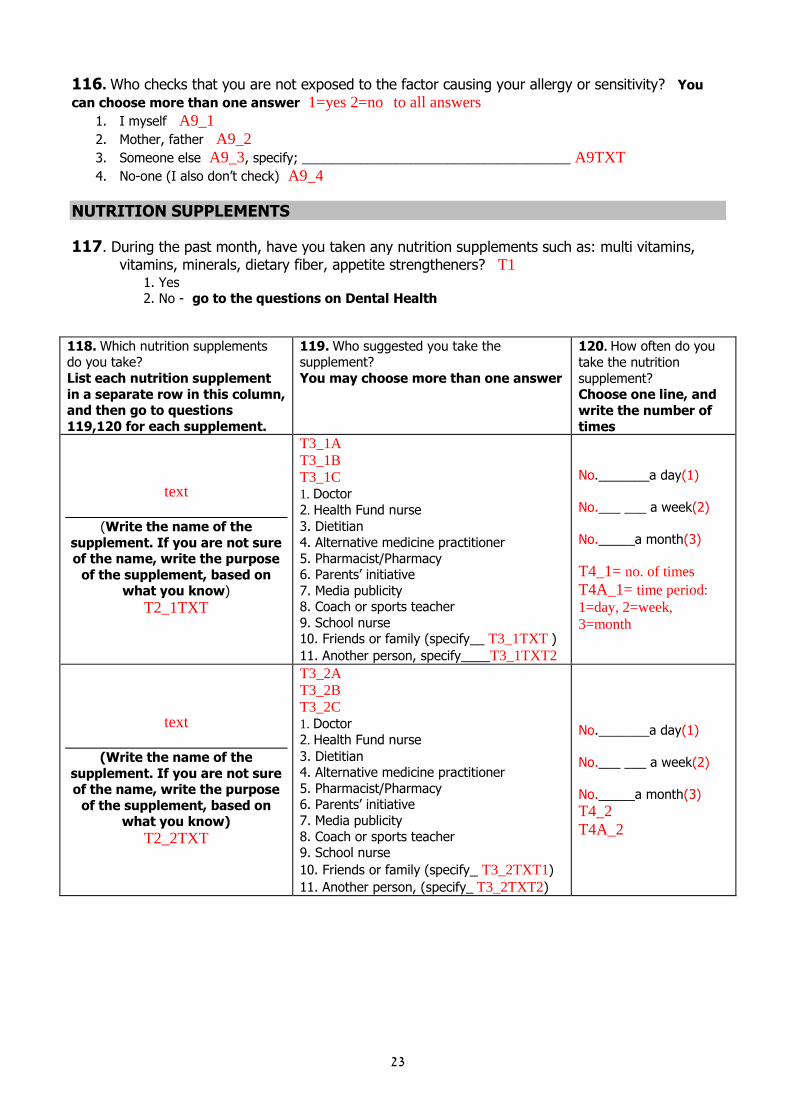
116. Who checks that you are not exposed to the factor causing your allergy or sensitivity? You
can choose more than one answer 1=yes 2=no to all answers
1. I myself A9_1
2. Mother, father A9_2
3. Someone else A9_3, specify; _____________________________________ A9TXT
4. No-one (I also don’t check) A9_4
NUTRITION SUPPLEMENTS
117. During the past month, have you taken any nutrition supplements such as: multi vitamins,
vitamins, minerals, dietary fiber, appetite strengtheners? T1
1. Yes 2. No - go to the questions on Dental Health
118. Which nutrition supplements do you take?
List each nutrition supplement
in a separate row in this column, and then go to questions
119,120 for each supplement.
119. Who suggested you take the supplement?
You may choose more than one answer
120. How often do you
take the nutrition
supplement? Choose one line, and
write the number of
times
text
(Write the name of the
supplement. If you are not sure of the name, write the purpose
of the supplement, based on what you know)
T2_1TXT
T3_1A
T3_1B
T3_1C 1. Doctor 2. Health Fund nurse
3. Dietitian
4. Alternative medicine practitioner
5. Pharmacist/Pharmacy 6. Parents’ initiative
7. Media publicity 8. Coach or sports teacher
9. School nurse 10. Friends or family (specify__ T3_1TXT )
11. Another person, specify____T3_1TXT2
No._______a day (1)
No.___ ___ a week (2)
No._____a month (3)
T4_1= no. of times
T4A_1= time period: 1=day, 2=week, 3=month
text
(Write the name of the
supplement. If you are not sure of the name, write the purpose
of the supplement, based on what you know)
T2_2TXT
T3_2A
T3_2B
T3_2C
1. Doctor
2. Health Fund nurse
3. Dietitian 4. Alternative medicine practitioner
5. Pharmacist/Pharmacy 6. Parents’ initiative
7. Media publicity
8. Coach or sports teacher 9. School nurse
10. Friends or family (specify_ T3_2TXT1)
11. Another person, (specify_ T3_2TXT2)
No._______a day (1)
No.___ ___ a week (2)
No._____a month (3)
T4_2
T4A_2
24
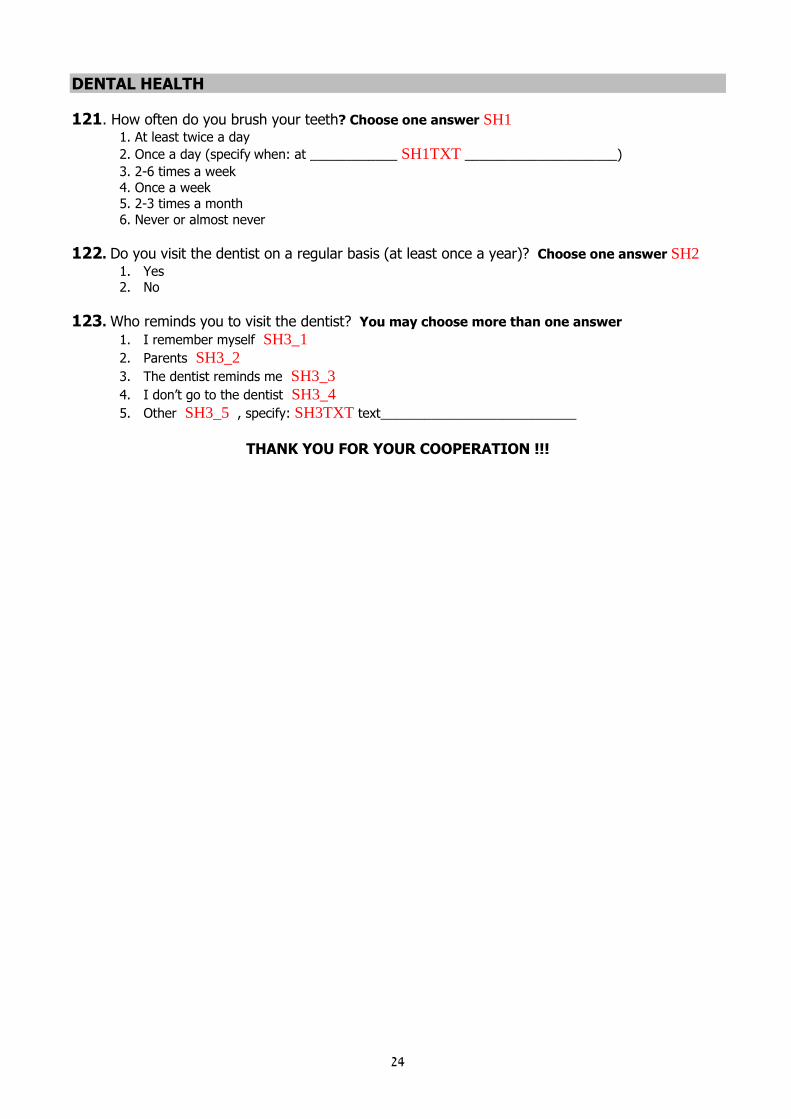
DENTAL HEALTH
121. How often do you brush your teeth? Choose one answer SH1
1. At least twice a day
2. Once a day (specify when: at ____________ SH1TXT _____________________)
3. 2-6 times a week
4. Once a week 5. 2-3 times a month
6. Never or almost never
122. Do you visit the dentist on a regular basis (at least once a year)? Choose one answer SH2
1. Yes 2. No
123. Who reminds you to visit the dentist? You may choose more than one answer
1. I remember myself SH3_1
2. Parents SH3_2
3. The dentist reminds me SH3_3
4. I don’t go to the dentist SH3_4
5. Other SH3_5 , specify: SH3TXT text___________________________
THANK YOU FOR YOUR COOPERATION !!!
25
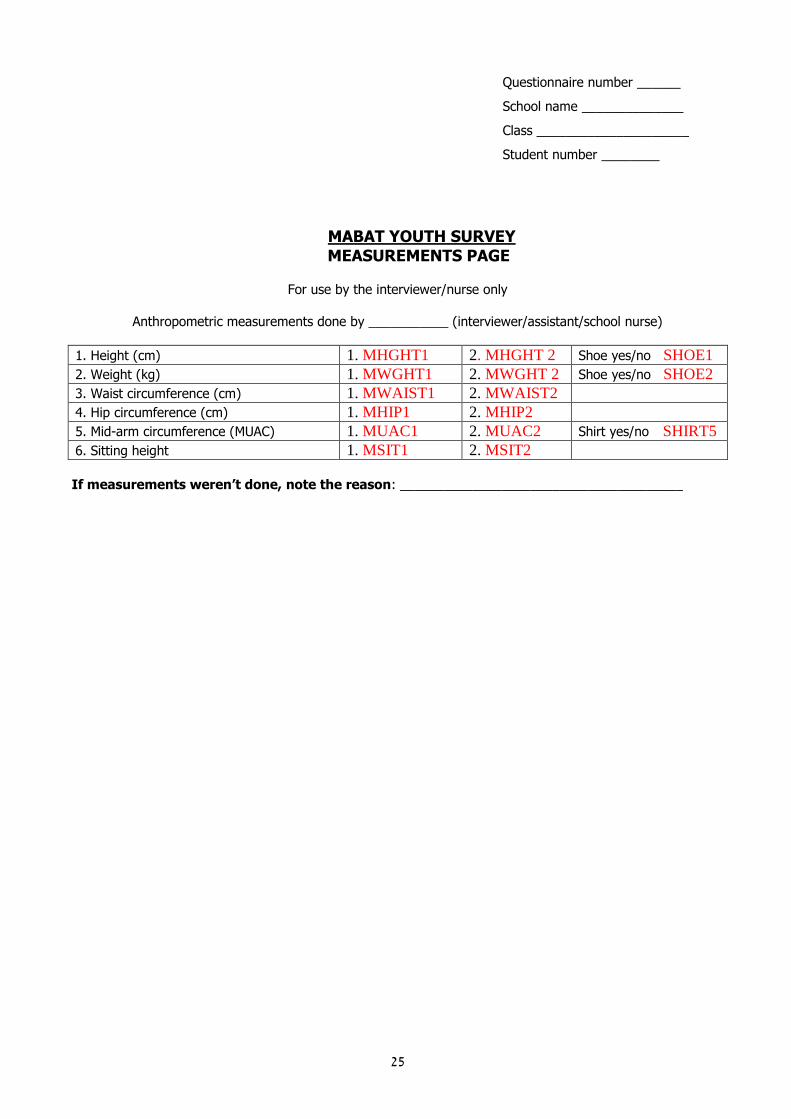
Questionnaire number ______
School name ______________
Class _____________________
Student number ________
MABAT YOUTH SURVEY MEASUREMENTS PAGE
For use by the interviewer/nurse only
Anthropometric measurements done by ___________ (interviewer/assistant/school nurse)
1. Height (cm) 1. MHGHT1 2. MHGHT 2 Shoe yes/no SHOE1
2. Weight (kg) 1. MWGHT1 2. MWGHT 2 Shoe yes/no SHOE2
3. Waist circumference (cm) 1. MWAIST1 2. MWAIST2
4. Hip circumference (cm) 1. MHIP1 2. MHIP2
5. Mid-arm circumference (MUAC) 1. MUAC1 2. MUAC2 Shirt yes/no SHIRT5
6. Sitting height 1. MSIT1 2. MSIT2
If measurements weren’t done, note the reason: _______________________________________

26
MABAT YOUTH SURVEY Name of school:__________
Student number; ________ questionnaire number: ___
24 HOUR FOOD RECALL On day (circle the day) 1 2 3 4 5 6 7
Interviewer: Read: Now let’s go over what you ate yesterday? Yesterday was __________ (interviewer-
state the day). Please tell me everything you ate and drank at home and away from home, during meals and between meals, including snacks, sweets and drink. (Interviewer - write each item on a separate line, and when you have completed this, go to the question on time.
Item
When did you begin
to eat /drink the
item?
The quick list √ Where did you eat?
A 1. At home (home cooked food)
B 2. Home (ready made/bought food)
C 3. At school (food from home)
D 4. At school (bought food, cafeteria)
E 5. At home of friends, family
F 6. Away from home (cinema, group activity, game)
G 7. Restaurant
H 8. At an event (party, wedding)
I 9. While traveling (car, bus, train)
J 10. At work (home prepared food)
K 11. At work (ready made/bought food)
L 12. Summer camp, hike, trip
M 13. Other, specify:________________
N
O Which meal?
P 1. Before breakfast
Q 2. Breakfast
R 3. Morning snack
S 4. Lunch
T 5. Afternoon snack
U 6. Dinner
V 7. Late night snack
W 8. drink/non-specified meal – (snack)
X 9. Food/drink over a period of some
hours/all day)
Y 10. Other, specify_____________
Z
Interviewer - read: Is there something you’ve forgotten? I will read you a short list- if you remember other
foods or drinks, please tell me: hot drinks, cold drinks (including water), alcoholic drinks, candy, sweet and salty snacks, seeds, nuts, fruits including dried, vegetables, bread, dairy products.
27
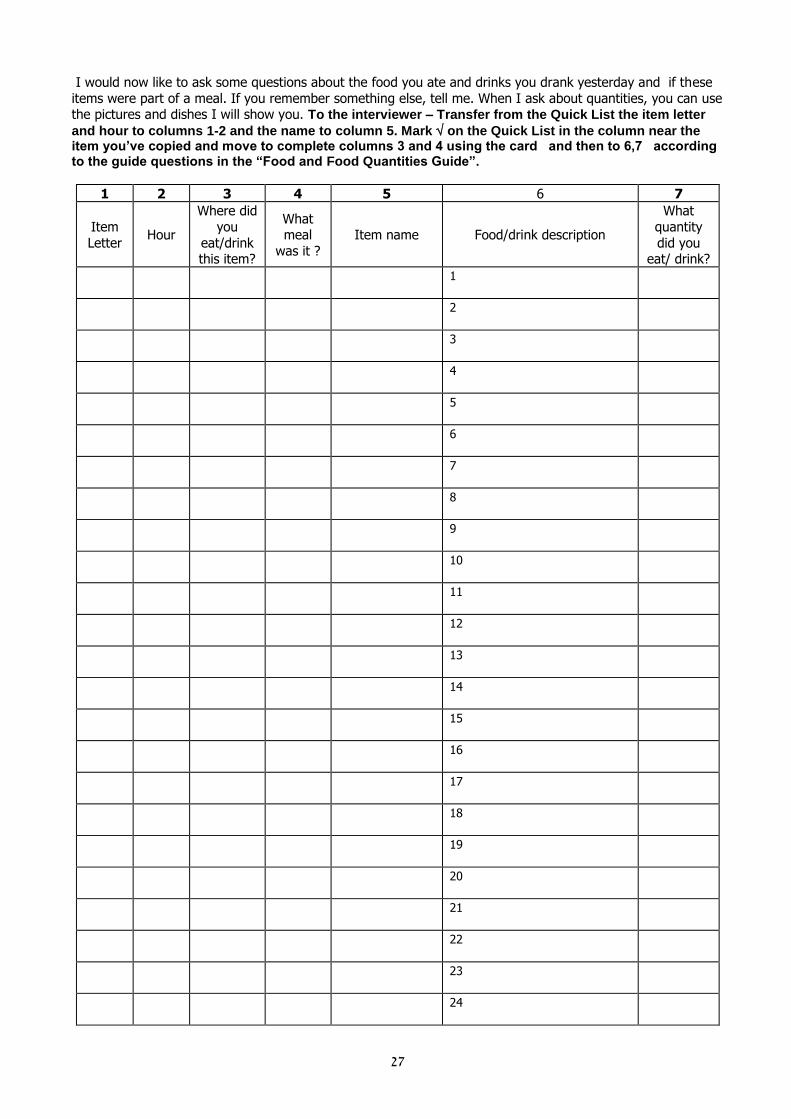
I would now like to ask some questions about the food you ate and drinks you drank yesterday and if these
items were part of a meal. If you remember something else, tell me. When I ask about quantities, you can use the pictures and dishes I will show you. To the interviewer – Transfer from the Quick List the item letter
and hour to columns 1-2 and the name to column 5. Mark on the Quick List in the column near the item you’ve copied and move to complete columns 3 and 4 using the card and then to 6,7 according to the guide questions in the “Food and Food Quantities Guide”.
1 2 3 4 5 6 7
Item
Letter Hour
Where did
you
eat/drink this item?
What meal
was it ?
Item name Food/drink description
What
quantity
did you eat/ drink?
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
28
1 2 3 4 5 6 7
Item
Letter Hour
Where did you
eat/drink this item?
What meal
was it ?
Item name Food/drink description
What quantity
did you eat/ drink?
25
26
27
28
29
30
31
32
33
34
35
1. Was the amount you ate yesterday similar to the amount you usually eat? Z1
1. Yes, the same - go to question 3
2. No, yesterday I ate less than usual 3. No, yesterday I ate more than usual go to question 2 999. Don’t know
2. What is the main reason you ate an amount yesterday that was different to what you usually eat? Z2
1. There was food I liked
2. There was food I didn’t like 3. Vacation, trip, travel
4. Religious holiday, Shabbat
5. Family celebration, social occasion 6. Stress
7. Boredom 8. Illness, not feeling well
9. Different mood to usual
10. I was at a friend’s home
11. Other, specify: _____________________________________ Z2TXT
3. What was your mood yesterday? Choose one answer Z3
1. Very good
2. Good 3. Average
4. Not so good 5. Not good at all
Now, I will ask you some specific questions about dairy products, fruit and vegetables.

29
4. When do you prefer to eat the following foods? (Check the appropriate box- you can pick
several times for each food)
With breakfast
Morning, between
meals
With lunch
After lunch (before the
evening meal)
Dinner (evening
meal)
Before going to
sleep, or during the
evening
No preferred
time
I don’t eat
this food
Fruit Z4F1 Z4F2 Z4F3 Z4F4 Z4F5 Z4F6 Z4F7 Z4F8
Vegetables Z4V1 Z4V2 Z4V3 Z4V4 Z4V5 Z4V6 Z4V7 Z4V8
Dairy
products
Z4D1 Z4D2 Z4D3 Z4D4 Z4D5 Z4D6 Z4D7 Z4D8
5. Do you take a fruit or vegetables to school or eat at school the foods listed? Check the
appropriate boxes.
Food Take to school Buy on the way/buy at school
Fruit Z5F1
Vegetables Z5V1
Dairy products Z5D1
1. Take to school
2. Buy on the way/buy at school
3. Don’t take
If you don’t take any fruits and vegetables, go to question 7
6. Who mostly picks the fruit or vegetables that you take? Z6
1. I myself, and I like what I choose 2. I myself, and I don’t always like what I choose
3. Someone else, and I mostly like what they choose for me
4. Someone else, and I mostly don’t like what they choose for me
7. Which fruits do you like to eat, and are they usually available? You can list up to 5 fruits. For
each fruit you have listed, check the appropriate box, if it is available or not available to you.
Fruit I like to eat, and it is always
available to me
I like to eat, but it is not
always available to me
Z7TXT1 Z7B1
Z7TXT2 Z7B2
Z7TXT3 Z7B3
Z7TXT4 Z7B4
Z7TXT5 Z7B5
1. I like to eat it and it is always available
2. I like to eat it and it is not always available
8. Are there fruits you prefer to eat alone, and those you prefer to eat with others?
(There are 2 lists- you can list up to 5 types of fruit in each list.)
Fruits I prefer to eat alone: Z8ATXT1__________________________to_ Z8ATXT5_____________________________
____________________________ ___________________________
Fruits I prefer to eat in company of others: Z8BTXT1 ___________________________to Z8BTXT5_____________________________
____________________________ ___________________________

31
9. Do you consider fruit to be a snack item? Choose one answer Z9
1. Yes, mainly
2. Sometimes
3. No, mainly not 4. No, not at all





























