Embed Size (px)
Citation preview

Am J Drug Deliv 2003; 1 (2): 103-112HEALTHCARE TECHNOLOGY REVIEW 1175-9038/03/0002-0103/$30.00/0
© Adis Data Information BV 2003. All rights reserved.
Minimizing Bioavailability Variations with OralControlled Release FormulationsWhat is Possible?
Aditya Mohan Kaushal and Sanjay Garg
Department of Pharmaceutics, National Institute of Pharmaceutical Education and Research, SAS Nagar, Punjab, India
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
1. Bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
1.1 Types of Bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
1.2 Quantitation of Bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
1.3 Variations in Bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
1.4 Problems with Bioavailability Variations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
2. Minimization of Bioavailability Variations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
2.1 Reducing Fluctuations With Continuous Release Controlled Drug Delivery Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
2.2 Reduction in Metabolism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
2.3 Overcoming Chronopharmacokinetic Variation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108
2.4 Gastro Retentive Systems for Site-Specific Absorption . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 109
2.5 Food Induced Variability and Controlled Release Products . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
3. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
Despite various routes of drug delivery being explored, the oral route has continued to be the most popularAbstractroute of drug administration. However, the complexities associated with the gastrointestinal tract lead to
variations in the rate and extent of bioavailability of drugs administered as oral dosage forms. This variation in
the bioavailability of drugs is responsible for the majority of adverse effects, lack of efficacy, and development
of tolerance, etc.
This review explores the possibilities of minimizing these bioavailability variations with the use of oral
controlled release (CR) dosage forms. The use of CR preparations, in lieu of the immediate preparations in itself,
leads to better control over plasma levels. Furthermore, the additional benefits offered by CR products, such as
the reduction in first-pass metabolism, enhanced and reproducible bioavailability with gastro retentive prepara-
tions, overcoming circadian rhythm variations, and the lesser effect of fed condition on bioavailability, can be
effectively utilized for bioavailability variation minimization. However, CR products cannot be use indiscrimi-
nately. The use of CR products to serve the purpose of bioavailability variation minimization should be based on
due consideration to the role of metabolizing enzymes, the permeability variations, and the area available for
absorption.

104 Kaushal & Garg
The oral route of drug administration has traditionally been the drug absorbed of the total amount of drug administered. Since the
preferred route of administration for most therapeutic agents and, assessment of absolute bioavailability necessitates the use of an
in general, is the first avenue investigated in the discovery and administration route that excludes doubt on the amount of drug
development of new drug candidates and formulations. Patient reaching the systemic circulation, the drug is also administered
acceptance, convenience of administration, cost of manufacturing, intravenously. The calculations involve the comparison of the area
etc., are some of the factors that have ensured a continued empha- under the curve (AUC) for the two routes of drug administration.
sis on the development of oral formulations. Among the oral On the other hand, the relative bioavailability is the extent and rate
formulations, for most of the drugs and therapeutic indications, the of bioavailability of a drug from one or more dosage forms given
conventional immediate release (IR) forms suffice. However, in by the same route of administration. One of the dosage forms
some conditions, the controlled release (CR) systems are superi- administered when relative bioavailability is measured is the refer-
or.[1] ence product and the rest are test formulations.[4]
The diversity and complexity of the gastrointestinal tract pro-
vides for a much greater flexibility in the design of oral drug 1.2 Quantitation of Bioavailabilitydelivery systems, than for other routes of drug delivery.[2] At the
same time, this very diversity and complexity can lead to differ- Mathematical parameters are required to quantitate andences in the behavior of the dosage form in the gastrointestinal compare the bioavailability of different formulations. In the caseenvironment. This can lead to differences in the bioavailability of of single dose studies, the parameters used are AUC, peak plasmadrugs from one patient to another, and within the same patient on concentration (Cmax), and the time to reach peak plasma concen-two different occasions or in different gastrointestinal conditions. tration (Tmax). To characterize the rate and extent of bioavailabil-Although bioavailability is not a direct measure of the therapeutic ity in multiple dose studies, AUC during an administration inter-efficacy per se, the variations in the bioavailability (in rate or val, and the percentage fluctuation, or the fluctuation index, areextent) are more likely to have an effect on therapeutic response most commonly used:than not have an effect. Hence, a predictable and reproducible
bioavailability is very much a desired attribute of an orally admin-Fluctuation C C C
Fluctuatio
ss ss ss(%) {( ) / }[max] [min] (min)� �100
nn index C C AUCss ss� � �( ) /( / )[max] [min] 0 � �istered dosage form. In light of all this, the use of CR drug delivery
where Css (max) and Css (min) are the maximum and minimumstrategies for the minimization of the bioavailability variations ofconcentrations at steady state, respectively, AUC0–τ is the areaorally administered products is explored in this manuscript.under the curve during an administration interval, and τ is the
1. Bioavailability administration interval.[4,5]
Bioavailability is defined in the US Code of Federal Regula-1.3 Variations in Bioavailability
tions as ‘the rate and extent to which the active ingredient or active
moiety is absorbed from a drug product and becomes available atA variety of factors can lead to differences in the bioavailability
the site of action. For drug products that are not intended to beof orally administered products.[6] A few of the important factors
absorbed into the bloodstream, bioavailability may be assessed bythat lead to variations in bioavailability include:
measurements intended to reflect the rate and extent to which the• Blood flow: Blood flow or perfusion to the site of drug absorp-
active ingredient or active moiety becomes available at the site oftion varies during the day, as a result of movement, food intake,
action.’[3] This definition focuses on the processes by which theetc. The absorption of drugs that are perfusion rate-limited,
active ingredients or moieties are released from an oral dosagesuch as the small hydrophilic molecules, is greatly influenced
form and move to the site of action.[3]
relative to the diffusion rate-limited lipophilic molecules.[6]
• pH: The pH of the gastrointestinal tract is variable in the1.1 Types of Bioavailabilitydifferent regions, and also varies according to the time of the
Bioavailability can be expressed as either absolute or relative day, the food intake, and the type of food taken. The pH at the
bioavailability. The absolute bioavailability is the fraction of the site of release and absorption determines the amount of drug
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

Bioavailability Variation with Oral CR Formulations 105
present as the un-ionized moiety that is essential for passive 2. Minimization of Bioavailability Variationsdrug absorption.[6]
By definition, CR dosage forms release the drug at a planned,• Food and fluid volume: The amount and type of food influences
predictable, and lower rate than immediate-release formulations.the gastric motility cycle and the gastric retention time. In
On the other hand, the IR dosage forms are designed to release theaddition, the blood flow, acid and bile secretion, and change in
drug immediately upon ingestion, with no intended lag in thethe absorption of the drug in the presence of food components
release of the drug.[8] The rate of release of the drug from these twomay occur. All these indirectly lead to variations in rate and/or
types of dosage forms is thus very different, and this translates intoextent of bioavailability.[6]
a difference in the plasma profiles, or in other terms, the bioavaila-Thus, the sources of variation in bioavailability can either be
bility of these two types of dosage forms. The factors that affectthe physiologic factors such as blood flow, pH and, food and fluid
the bioavailability of the orally administered dosage forms canvolume, or the dosage form related factors. An understanding of
affect the IR and CR in different ways and to different extents.these factors is essential to minimize variations in bioavailability
The biopharmaceutics classification system (BCS) divides theof orally administered products. The physiologic factors are relat-
drugs into four categories, based on their solubility and permeabil-ed to the patient and are beyond the control of a formulation
ity characteristics.[9] Class I includes drugs with high solubilityscientist; at best, they can be well understood and minimized, if
and high permeability; class II drugs have low solubility but highpossible, by suitable formulation approaches. The influence of
permeability; class III drugs have high solubility but low permea-these factors is avoided while carrying out a bioavailability or
bility; and class IV drugs have both low solubility and lowbioequivalence study by proper design of the study.[4] However,
permeability. This classification is used by the US FDA to providewhen the product reaches the market, it is subject to intra- and
less stringent conditions for bioequivalence of oral drug productsinter-patient variability. The possibility of overcoming these fac-
for class 1 drugs. Although the drugs belonging to class 1 of thetors by the use of CR products is explored in the present manu-
BCS are considered to present minimal problems in their absorp-script. The second type of factors is the dosage form related
tion, due to the wide array of factors discussed earlier, variations infactors. Strictly considering, any bioavailability variations due to
the bioavailability may still arise. Hence, problems of variation informulation related factors should be intended and controllable.
the bioavailability can arise for any BCS class of drugs.For example, the rate of bioavailability is deliberately desired to be
Oral controlled drug delivery can be used in more than one waylower in the case of CR products.
to minimize the variations associated with conventional IR prod-The variations in bioavailability can be quantified in terms of
ucts. The basic approach in making a CR system is to provide athe parameters discussed earlier, i.e. AUC, Cmax, Cmin, percentage
slower, preprogrammed rate of delivery compared with IR. Thefluctuation, etc.
controlled drug delivery systems can be designed as:[2]
• continuous release systems, e.g. diffusion, dissolution, and1.4 Problems with Bioavailability Variations
osmosis controlled systems
• delayed transit and CR systems, e.g. density altered and bioad-Bioavailability variations are manifested in terms of nonrepro-
hesive systemsducible plasma drug profiles, from one patient to another, as well
• delayed release systems, e.g. intestinal or colon release.as within the same patient from one time to another. The plasma
The following subsections discuss the opportunities whereinprofiles of a drug moiety administered as an oral dosage form
CR products can minimize variations and lead to better therapeuticfluctuate as per the properties of the drug and dosage form. The
efficacy.additional variations in the profiles, as a result of the above-
discussed factors, can lead to problems of loss of efficacy (due to2.1 Reducing Fluctuations With Continuous Release
fall of plasma levels below minimum effective level), and toxicityControlled Drug Delivery Systems
(higher peaks crossing toxic levels). In addition, specific problems
such as the development of tolerance against antibacterials, or Among the variety of CR dosage forms delivering drugs in
compliance problems due to severe adverse effects, may devel- pulsatile, delayed, timed release, and colon targeted fashion, the
op.[7] continuous CR dosage forms are by far the most common. These
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

106 Kaushal & Garg
dosage forms release the drug in a continuous fashion all along the
gastrointestinal tract. Belonging to this category of dosage forms
are the matrix tablets, multiparticulate systems, and the osmotic
pumps.[7] Among all these, OROS®1 systems have proven to be the
most reliable and predictable over the years, and hence are dis-
cussed as representative examples of the class of continuous
release controlled drug delivery systems.[10] The reduction in
bioavailability variabilities is mainly due to the change of rate-
limiting step from absorption to drug release. Hence, the bioavail-
ability is controlled by dosage form rather than by the physiologic
factors. Some of the examples of studies carried out with these
systems are discussed below.
Methylphenidate is used for the treatment of attention deficit
hyperactivity disorder (ADHD). The OROS® system for methyl-
phenidate HCl is an osmotic CR delivery system designed for once
daily oral administration. The pharmacokinetics of this system
were compared against sustained-release and the IR formulation.
The dose-normalized methylphenidate Cmax for the OROS®
800
700
600
500
400
300
200
100
96 120 128 136 144 152 160 168
Time after first dose (h)
Pla
sma
conc
entr
atio
n (n
mol
/L)
Day 5 Day 6 Day 7 Day 8
Conventional metoprolol tabletsMetoprolol CR/ZOKMetoprolol OROS®
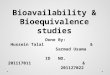
Fig. 1. Mean plasma concentrations of metoprolol on days 5 through 8following once daily administration of metoprolol controlled-release/zero-order kinetics (CR/ZOK), metoprolol OROS®, and conventional (immediaterelease) metoprolol tablets (reproduced from Sandberg et al.,[13] with per-mission from Kluwer Academic/Plenum Publishers).
methylphenidate HCl system was significantly lower than for IR
and sustained release methylphenidate.[11] At the same time, the 2.2 Reduction in Metabolismbioavailability of methylphenidate from OROS® compared to the
Metabolism of the drug released from an oral system in theIR and sustained release formulations was complete.[11]
gastrointestinal tract is one of the factors affecting the ultimateIn another study with the OROS® system, for amitriptyline
bioavailability. The drugs that are metabolized to inactive metabo-hydrochloride, the mean maximal plasma amitriptyline concentra-
lites present the greatest problem since metabolism results in a losstion Cmax was lower, and the mean tmax was longer than that
of activity. Of concern here is metabolism due to the luminalassociated with the equivalent IR dose administered at night-
enzymes, and the first-pass metabolism (both metabolism in thetime.[12] The relative bioavailability of amitriptyline via OROS®
gut wall and liver).[6] The concentration of gut wall enzymes thatversus IR administration was 95%. The metabolite-to-drug ratios
belong to the category of cytochrome oxidase is variable throughafter the OROS® and IR administration were similar, suggesting
the gastrointestinal tract, with concentrations decreasing fromno change in metabolism between treatments.
proximal to distal intestine.[14] The conventional controlled drugIn yet another study, the steady-state bioavailability and day-to- delivery systems release the drugs from the system at a continuous
day variability of plasma levels were evaluated for two novel oral rate (with or without a lag time). In these systems, the position ofdrug delivery systems (OROS® and a multi-unit system) of meto- release of the drug from the system is not controlled, and aprolol and an immediate release tablet. The extended drug release substantial part of the drug is released in the lower intestine (as aand absorption observed after administration of metoprolol CR/ result of normal gastrointestinal transit). Hence, a greater percent-zero-order kinetics (ZOK) and metoprolol OROS®, resulted in age of the drug released (compared with IR oral dosage forms)similar steady-state plasma concentrations after once daily admin- from these systems is presented to a lower concentration of drugistration. Compared with the IR tablet, they produced considerably metabolizing enzymes. The bioavailability of drugs that are me-lower plasma peaks, 3- to 4-fold higher trough concentrations, 8–9 tabolized by the gut wall enzymes can, therefore, be increased by
hours longer mean residence times, and 20% lower relative bio- their incorporation into CR systems (single- or multi-layer matrix
availability.[13] Figure 1 shows the comparative plasma profiles. tablets, multiparticulate systems, OROS® system, etc.). Further-
1 The use of tradenames is for product identification purposes only and does not imply endorsement.
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

Bioavailability Variation with Oral CR Formulations 107
more, the application of a mechanism that introduces an even rious dosage forms (including a transdermal system) are given in
greater delay in the start of drug release, such as enteric coatings table I. The results demonstrate the metabolism of oxybutynin by
on the CR dosage forms, can protect the drug from a hostile gut wall enzymes, and a consequently improved bioavailability
environment in the stomach, and further enhance the bioavailabil- and reduced adverse effects by CR dosage forms.
ity. A few examples that exhibit this are discussed below. In another study, a novel once daily ‘coat-core’ formulation of
the calcium channel antagonist nisoldipine was compared againstOxybutynin is a muscarinic receptor antagonist that has beenIR or intravenous formulations.[20] The mean residence time andavailable for a number of years in its original IR formulation.apparent terminal half-life of nisoldipine in the coat-core formula-While oxybutynin IR has proven effective for the treatment oftion were significantly increased compared with administration viaoveractive bladder, its extended use can be limited by adversethe intravenous route or the oral IR formulation. At steady-state,effects, particularly dry mouth. The CR formulation of oxybuty-the coat-core formulation produced a plateau-shaped profile ofnin, based on the OROS® system, allows once daily administra-nisoldipine plasma concentrations throughout the 24-hour admin-tion. In a comparative in vivo study of the immediate and OROS®
istration interval, and the peak-trough fluctuation was reduced byforms of oxybutynin, the mean oxybutynin degree of fluctuationapproximately 4-fold, compared with the IR tablet in a twice dailywas much lower for OROS® oxybutynin chloride (78%) than forregimen. The relative bioavailability of the novel formulation wasIR oxybutynin (371%).[15] Furthermore, with OROS® oxybutyningreater by 1.5-fold compared with the IR tablet. This was attribut-chloride, mean relative bioavailability was higher (153%) fored to release of the drug in the colon where the contribution of theoxybutynin, and lower (69%) for N-desethyloxybutynin, com-gut wall to presystemic metabolism is reduced, resulting in anpared with IR oxybutynin.[16] The latter has been implicated inincrease in bioavailability compared with the stomach and smallmediating a major part of the adverse effects of oxybutyninintestine.treatment.[16] This increased bioavailability may be due to reduced
first-pass metabolism. The OROS® systems are thought to reach Yet another study compared the pharmacokinetics of intrave-
the colon within 3–5 hours after administration, where cytochrome nous, oral IR, and oral OROS® formulations of hydromor-
P450-mediated oxidation (the primary metabolic pathway for oxy- phone.[21] The mean absolute bioavailability for the 8mg OROS®
butynin) is less extensive than in the small intestine.[15] The formulation was significantly larger than for the 8mg IR formula-
comparative pharmacokinetic parameters of oxybutynin from va- tion. The CR formulation of hydromorphone produced less fluctu-
Table I. Comparative pharmacokinetic parameters of oxybutynin using different systems[17-19]
Cmax (μg/L) tmax (h) AUC0–t (μg • h/L) AUC0–∝ (μg • h/L)
Immediate release tablets (5mg)
R-oxybutynin 2.2 ± 1.7 1.0 3.8 ± 3.1 3.8 ± 3.1
R-N-desethyloxybutynin 15.5 ± 3.7 1.0 45.7 ± 17.1 62.3 ± 30.8
S-oxybutynin B 4.1 ± 0.7 0.8 5.5 ± 3.3 5.5 ± 3.3
S-N-desethyloxybutynin 10.9 ± 3.1 1.0 31.8 ± 11.7 42.2 ± 19.4
Controlled release OROS® tablets (10mg)
Oxybutynin 2.5 2.0 30 ND
N-desethyloxybutynin 43.2 2.0 39.1 ND
Transdermal system (36mg)
R-oxybutynin 1.2 ± 0.3 48.0 85.8 ± 26.4 ND
R-N-desethyloxybutynin 1.2 ± 0.5 48.0 83.9 ± 43.0 ND
S-oxybutynin 1.6 ± 0.4 48.0 121.4 ± 34.0 ND
S-N-desethyloxybutynin 1.4 ± 0.7 48.0 101.1 ± 52.6 ND
AUC = area under the concentration-time curve; Cmax = maximum plasma drug concentration after single-dose administration; ND = no data; tmax = time to
reach maximum concentration following drug administration.
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

108 Kaushal & Garg
ation of plasma concentrations compared with IR formulations. 2.3 Overcoming Chronopharmacokinetic Variation
The increased bioavailability from the OROS® formulation was
attributed to decreased metabolism by a first-pass effect. The temporal difference in the absorption, distribution, meta-
bolism, and elimination lead to differences in the bioavailabilityMany of the drugs are metabolized by hepatic first-pass meta-and pharmacologic response of drugs. Out of all of these, thebolism, leading to a lower bioavailability for the parent molecule.differences in absorption and metabolism can possibly be over-
A subcase of such a phenomenon could involve drugs that primari-come by use of CR dosage forms. Although a number of mechan-
ly act in the liver. The use of oral CR dosage forms could offer isms, such as passive or facilitated diffusion, active transport, anddose-sparing advantages. Lovastatin is a HMG-CoA reductase filtration through pores, etc., are involved in the absorptive pro-inhibitor indicated for lowering of cholesterol. A study was under- cess, passive diffusion is by far the most important. The differ-
ences in absorption result from differences in the perfusion, gastrictaken to compare the short-term pharmacodynamics and pharm-pH, acid secretion, motility, and gastric emptying.[23] Lipophilicacokinetics of multiple doses of lovastatin extended release (ER)drugs have been shown to be absorbed faster in the morning than
with those of lovastatin IR in patients with hypercholesterolemia.the evening.[24]
Compared with lovastatin IR, lovastatin ER produced a 3.9%A small number of studies have demonstrated that the differ-
greater reduction in low-density lipoprotein-cholesterol. The Cmaxences in the absorption process over the 24-hour period can be
values for lovastatin, lovastatin acid, and inhibitors of HMG-CoAovercome by use of oral CR dosage forms. Examples where the
reductase were lower at day 28 with lovastatin ER than with variations in the bioavailability seen with IR products was over-lovastatin IR. The AUC0–24 ratio for lovastatin was 1.91, reflect- come with CR dosage forms include preparations of nifedipine,[25]
isosorbide mononitrate,[26] and theophylline.[27] In the latter study,ing higher bioavailability of the prodrug with lovastatin ER; in
a proprietary once daily oral CR beadlet technology for theophyl-contrast, the ratios for lovastatin acid, and active and total inhibi-line was compared with a twice daily preparation. It was found thattors of HMG-CoA reductase were <1. Because lovastatin is effi-the diurnal variation associated with theophylline could be over-
ciently extracted by the liver, and because its administration income by a formulation approach. Figure 2 shows the comparative
divided doses is associated with increased efficacy, ER formula- profiles of theophylline once daily formulation, given in the morn-tion was suggested to have the potential for a dose-sparing advan- ing and evening. The observed circadian rhythm was due to thetage relative to the IR formulation in the treatment of hypercholes- slower absorption of theophylline when the body was at rest.
Similar results were reported for another CR theophylline prepara-terolemia.[22]
tion that was prepared using acrylic resins. The study concluded
that there was a lower risk of toxic plasma concentrations, or
concentrations under the therapeutic level, than with formulations
that exhibit circadian rhythm.[28]
In the case of nifedipine, IR, sustained-release, and intravenous
solution were studied in healthy volunteers and patients with
hypertension.[25] The pharmacokinetics of IR, but not sustained-
release and intravenous nifedipine, were dependent on the time of
day. IR nifedipine had a higher Cmax and shorter tmax after the
morning application compared with the evening application, and
bioavailability in the evening was reduced by about 40%.
A similar possibility of decreasing the variability seen with
metabolism (due to variations in hepatic blood flow) remains with
the use of CR products. The effects of hepatic blood flow are most
relevant for high extraction ratio drugs.[23]
12
10
9
7
5
3
2
00 5 10 15 20 25
Time (h)
Ser
um le
vel (
μg/m
L)
Administered in the morning
Administered in the evening
Fig. 2. Mean serum theophylline concentrations on day 5 in patients given900mg of a once daily, controlled release formulation in the morning orevening (reproduced from Harrison et al.,[27] with permission from JohnWiley & Sons, Inc., and the copyright© holder Wiley-Liss, Inc.)
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

Bioavailability Variation with Oral CR Formulations 109
hours post-administration, and then releases the drug at a zero
order rate for 16 hours.[31]
2.4 Gastro Retentive Systems for Site-Specific Absorption
The phenomenon of drugs being preferentially absorbed from a
specific area of the gastrointestinal tract is termed as absorption
window. The existence of the absorption window is considered to
be a rational against the development of CR dosage forms, since
the criteria of general absorption throughout the gastrointestinal
tract is considered to be a prerequisite for CR form develop-
ment.[32] The variation in the bioavailability of an IR preparation
could result from the existence of an absorption window. CR
dosage forms utilizing the principle of gastro retention have been
reported for drugs having an absorption window in the upper
gastrointestinal tract. One such study reported enhanced bioavaila-
bility of furosemide (frusemide) from a floating dosage form.[33]
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.00 4 8 12 16 20 24 28 32 36
Time (h)
Sal
iva
theo
phyl
line
(μg/
mL)
Nonfloating CR tablets (TheoDur™) - fasting Nonfloating CR tablets (TheoDur™) - nonfastingFloating CR tablets - fastingFloating CR tablets - nonfasting
Fig. 3. Comparative plasma profiles of floating and nonfloating theophyllinecontrolled release (CR) tablets given under fasted and nonfasted states(reproduced from Desai and Bolton,[35] with permission from Kluwer Aca-demic/Plenum Publishers).
The solubility of the drug was first enhanced by preparing an
inclusion complex of furosemide with β-cyclodextrin in a 1 : 1In addition to decreasing the variability associated with chro-
proportion. The values of plasma AUC obtained with the floatingnopharmacokinetics, CR dosage forms can be formulated accord-
dosage form were about 1.8 times those of the conventional tablet.ing to the circadian need of the body in the disease condition. Similar results were obtained in another study employing bufferedExamples of diseases where chronotherapy is most desired are buoyant furosemide capsule formulations.[34]
cardiovascular complications (hypertension), cancer, arthritis, and In another study, a floating CR oral tablet containing 300mg
theophylline was compared with a conventional tablet.[35] Scin-asthma. The chronotherapy involves either changing the time oftigraphic studies of floating and nonfloating tablets, under fastingadministration or altering the release pattern of the drug from theand nonfasting conditions, showed that food significantly in-dosage form. A number of attempts have been made to preparecreased gastric retention time and tablet density did not affect
timed-release dosage forms.[29,30] The systems utilize a variety ofretention time. However, positions of floating and nonfloating
formulation strategies to provide a delayed release of the drug. Thetablets in the stomach were different. Bioavailability studies under
delayed release dose could either be IR or CR. One of the success- fasting and nonfasting conditions showed results comparable toful dosage forms for hypertension control is verapamil in a con- those of the conventional tablet. The floating tablet maintained
trolled onset ER system. The system starts to deliver the drug 5 constant theophylline levels of about 2 mg/ml for 24 hours. It was
Table II. Pharmacokinetic parameters for oxycodone hydrochloride controlled release (CR) tablet and immediate release (IR) solution (reproduced from
Benziger et al.,[37] with permission from from John Wiley & Sons, Inc., and the copyright© holder Wiley-Liss, Inc.)
Pharmacokinetic CR tablet (40mg) IR solution (20mg)
parameters fasted state fed state fasted/fed (%) fasted state fed state fasted/fed (%)
Cmax (μg/L) 18.8 17.1 92 36.7 30.3 82
AUC0–36 201 195 97 174 209 120
AUC0–∞ 203 4.8 97 174 209 120
tmax (h) 3.1 4.5 159 1.1 1.4 120
AUC = area under the concentration-time curve; Cmax = maximum plasma drug concentration after single-dose administration; tmax = time to reach
maximum concentration following drug administration.
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

110 Kaushal & Garg
system employed and the drug meant to be delivered. Some of the
examples where the effect of food on the bioavailability of CR
products was investigated are given below.
The effects of a high-fat meal on the bioavailability of oxyco-
done hydrochloride, administered as a 40mg CR tablet or a 20mg
IR solution, were evaluated. There was no significant food effect
with CR oxycodone, as judged by the analysis of AUC0–∞ and
Cmax values under fed and fasted conditions. However, for the IR
solution, both the bioavailability and peak plasma oxycodone
concentration were significantly altered by consumption of the
high-fat meal.[37] Table II summarizes these results.
100
80
60
40
20
00 5 10 15 20 25
Time (h)
nmol
/L
Extended release matrix tabletProcardia XL®
Fig. 4. Mean nifedipine plasma concentrations for extended release matrixtablet and Procardia XL® at steady state after administration under fastingconditions (reproduced from Abrahamsson et al.,[38] with permission fromElsevier Science). In another study on nifedipine, the hydrophilic matrix tablet
(ER) and a push-pull osmotic pump tablet (Procardia XL®) wereconcluded that the floating theophylline tablet floats in the stom-
compared for bioavailability with and without food.[38] Althoughach and provides a gradual release profile (figure 3).
both the ER and XL formulations provided almost constant drug
delivery over 24 hours after administration under fasting condi-2.5 Food Induced Variability and Controlled
tions, and were found to be bioequivalent, food significantlyRelease Products
increased the AUC for ER. The rate of absorption was increased to
a higher degree for ER than XL, as indicated by a Cmax that wasThe administration of food can result in marked differences inalmost twice as high for ER compared with XL. This finding wasthe bioavailability of orally administered drug products. This isshown to be related to an increased tablet-erosion rate for ER,also considered by the regulatory agencies, which recommend aleading to more rapid drug release.[38] Figure 4 and figure 5 showfood effect study of orally administered products. Food, compared
with fasting conditions, can change the bioavailability of a drug
and can influence the bioequivalence between test and reference
products. Food effects on bioavailability can have clinically sig-
nificant consequences. Food can alter bioavailability by a change
in the following:
• delay of gastric emptying
• stimulation of bile flow
• changes in gastrointestinal pH
• increase in blood flow
• changes in luminal metabolism of a drug substance
• physical or chemical interactions with a dosage form or drug
substance.
Depending on the drug substance, the drug product, and the
characteristics of the meal taken, a more or less pronounced effect
may be observed. Drug absorption may be decreased, delayed,
increased, or remain unaffected upon taking with food.[36] The CR
dosage forms normally contain a greater amount of the drug
loaded on to a single dose, and a dose dump could result in
toxicity. One of the objectives of a food study for CR products is to
rule out the possibility of dose dumping. The CR products differ
with regard to the effect the food has on them, depending upon the
1.0
0.8
0.6
0.4
0.2
0.00 10 20 30 40
Time (h)
Frac
tion
abso
rbed
ER fed-study IIER fed-study IIIER fasting-study IIER fasting-study IIIProcardia XL®-fed
Fig. 5. Mean absorption time profile of nifedipine for ER and Procardia XL®
after administration with food, and ER without food (reproduced fromAbrahamsson et al.,[38] with permission from Elsevier Science). ER = ex-tended release.
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

Bioavailability Variation with Oral CR Formulations 111
the nifedipine plasma profiles for ER and XL formulations under indiscriminately used for the above purpose. In many cases they
fasted and fed conditions. can themselves be a cause of decreased or variable bioavailability
due to the variable nature of the gastrointestinal tract with respectIn two independent studies with different CR systems forto the metabolizing enzymes, permeability, and area available foroxybutynin delivery, Lukkari and co workers[39] observed that theabsorption. It is important, therefore, to understand the gastroin-food did not change the AUC of oxybutynin, but increased thetestinal physiology, and design the CR systems accordingly to turnAUC of N-desethyloxybutynin (the metabolite) by about 20%.this limitation to our advantage.The Cmax values for oxybutynin and N-desethyloxybutynin were
2-fold higher when the drug was administered after breakfast,
compared with the fasting state. On the other hand, Gupta and AcknowledgementsSathyan[15] reported that the bioavailability of oxybutynin from the
The authors gratefully acknowledge CSIR, New Delhi, for providingOROS® system was unaffected when taken with food.funding for research project no. 01(1712)/01/EMR-II. The views expressed by
A new dosage form of carbamazepine was developed consist- the authors do not necessarily reflect the views of CSIR. The authors have noing of three different types of pellets (IR, CR, and enteric release). conflicts of interest that are directly relevant to the content of this manuscript.
To explore the influence of food on the absorption of carbamaze-
pine, the dosage form was taken with a high-fat meal, in a fasting Referencesstate, or sprinkled over food. The bioequivalence was established 1. Fix J. Oral drug delivery, small intestine and colon. In: Mathowitz E, editor.
Encyclopedia of controlled drug delivery. Vol. 2. New York: John Wiley &based on the equivalence of AUC (extent of absorption) in all threeSons, 1999: 698-728
conditions.[40]2. Gupta PK, Robinson JR. Oral controlled release delivery. In: Kydonieus A, editor.
Treatise on controlled drug delivery: fundamentals, optimization, application.Clarithromycin, a semisynthetic macrolide, was studied as anNew York: Marcel Dekker, 1992: 255-313oral once daily dose of 500mg CR clarithromycin tablets. The
3. Food and Drug Administration, Center for Drug Evaluation and Research. Gui-administration with food led to an increase in the extent of bio- dance for industry: bioavailability and bioequivalence studies for orally admin-
istered drug products – general considerations, 1st revision, March 2003availability.[41] As a result of the study, it was recommended that[online]. Available from URL: http://www.fda.gov/cder/guidance/5356fnl.pdf
the CR tablet should be taken with food to maximize bioavailabil- [Accessed 2003 Apr 1]
ity. 4. Ritschel WA, Kearns GL. Handbook of basic pharmacokinetics including clinicalapplications. 5th ed. Washington, DC: American Pharmaceutical Association,1999
5. Malinowski HJ, Henderon JD. Bioavailability and bioequivalence of oral con-3. Conclusionstrolled release products: a regulatory perspective. In: Welling PG, Tse FLS,editors. Pharmacokinetics: regulatory-industrial-academic perspectives. New
The ultimate target of oral therapy is to derive therapeutic York: Marcel Dekker, 1995: 451-78
6. Selen A. Factors influencing bioavailability and bioequivalence. In: Welling PG,efficacy. Although the bioavailability is not a direct marker of theTse FLS, Dighe SV, editors. Pharmaceutical bioequivalence. New York: Mar-
efficacy per se, bioavailability measurement can serve as ancel Dekker, 1991: 117-48
indicator of the drug availability at the site of action. Variations in 7. Welling PG, Dobrinska MR. Dosing considerations and bioavailability assessmentof controlled drug delivery systems. In: Robinson RJ, Lee VHL, editors.the bioavailability of orally administered products could resultControlled drug delivery fundamentals and applications. New York: Marcel
from a variety of controllable and uncontrollable factors, such as Dekker, 1987: 253-91
8. Malinowski HJ, Marroum PJ. Food and drug administration requirements forthose related to the patient, the dosage form, etc. With the use ofcontrolled release products. In: Mathowitz E, editor. Encyclopedia of controlledoral controlled preparations, these variations can be minimized indrug delivery. Vol. 1. New York: John Wiley & Sons, 1999: 381-95
at least a few, if not all, of the cases. The use of CR preparations in 9. Amidon GL, Lennernas H, Shah VP, et al. A theoretical basis for a biopharmaceu-tic drug classification: the correlation of in vitro drug product dissolution and inlieu of IR preparations in itself leads to better control over thevivo bioavailability. Pharm Res 1995; 12 (3): 413-20
plasma levels. Furthermore, the additional benefits offered by CR 10. Verma RK, Krishna DM, Garg S. Formulation aspects in the development ofosmotically controlled oral drug delivery systems. J Control Release 2002; 79:products, such as the reduction in first-pass metabolism, enhanced7-27and reproducible bioavailability with gastro retentive preparations
11. Modi NB, Lindemulder B, Gupta SK. Single- and multiple-dose pharmacokinetics(for absorption window drugs), overcoming circadian rhythm vari- of an oral once-a-day osmotic controlled-release OROS (methylphenidate HCl)
formulation. J Clin Pharmacol 2000; 40 (4): 379-88ations, and the lesser effect of fed condition on bioavailability, can12. Gupta SK, Shah JC, Hwang SS. Pharmacokinetic and pharmacodynamic character-
be effectively utilized for bioavailability variation minimization.ization of OROS and immediate-release amitriptyline. Br J Clin Pharmacol
However, it is important to note that the CR preparations cannot be 1999; 48 (1): 71-8
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)

112 Kaushal & Garg
13. Sandberg A, Abrahamsson B, Svenheden A, et al. Steady-state bioavailability and 29. Krogel I, Bodmeier R. Pulsatile drug release from an insoluble capsule bodyday-to-day variability of a multiple-unit (CR/ZOK) and a single-unit (OROS) controlled by an erodible plug. Pharm Res 1998; 15 (3): 474-81delivery system of metoprolol after once-daily dosing. Pharm Res 1993; 10 (1):
30. Krogel I, Bodmeier R. Evaluation of an enzyme-containing capsular shaped28-34
pulsatile drug delivery system. Pharm Res 1999; 16 (9): 1424-914. Paine MF, Khalighi M, Fisher JM, et al. Characterization of interintestinal and
31. Prisant LM. Verapamil revisited: a transition in novel drug delivery systems andintraintestinal variabilities in human CYP3A-dependent metabolism. J Pharma-outcomes. Heart Dis 2001; 3 (1): 55-62col Exp Ther 1997; 283: 1552-62
32. Ritchel WA. Pharmacokinetic and biopharmaceutical aspects in drug delivery. In:15. Gupta SK, Sathyan G. Pharmacokinetics of an oral once-a-day controlled-releaseTyle P, editor. Drug delivery devices. New York: Marcel Dekker Inc, 1988:oxybutynin formulation compared with immediate-release oxybutynin. J Clin
Pharmacol 1999; 39 (3): 289-96 17-79
16. Michel MC. A benefit-risk assessment of extended-release oxybutynin. Drug Saf 33. Ozdemir N, Ordu S, Ozkan Y. Studies of floating dosage forms of furosemide: in2002; 25 (12): 867-76 vitro and in vivo evaluations of bilayer tablet formulations. Drug Dev Ind
Pharm 2000; 26 (8): 857-6617. Ditropan XL prescribing information [online]. Available from URL: http://www.ditropanxl.com/professional/prescribe_info [Accessed 2003 Apr 1] 34. Gabr KE, Borg TM. Formulation and evaluation of buffered floating furosemide
18. Zobrist RH, Schmind B, Feick A, et al. Pharmacokinetics of the R- and S- delivery systems. STP Pharma Sci 2000; 10 (2): 181-6enantiomers of oxybutynin and N-desethyloxybutynin following oral and trans- 35. Desai S, Bolton S. Floating controlled-release drug delivery system: in vitro-indermal administration of the racemate in healthy volunteers. Pharmacol Res
vivo evaluation. Pharm Res 1993; 10: 1321-52001; 18 (7): 1029-3336. Food and Drug Administration, Center for Drug Evaluation and Research. Gui-
19. Lukkari E, Hakonen T, Neuvonen PJ. The pharmacokinetics of oxybutynin isdance for industry: food-effect bioavailability and fed bioequivalence studies,unaffected by gender and contraceptive steroids. Eur J Clin Pharmacol 1998; 53December 2002 [online]. Available from URL: http://www.fda.gov/cder/gui-(5): 351-4
dance/5194fnl.pdf [Accessed 2003 Apr 1]20. Heinig R. Clinical pharmacokinetics of nisoldipine coat-core. Clin Pharmacokinet1998; 35 (3): 191-208 37. Benziger DP, Kaiko RF, Miotto JB, et al. Differential effects of food on the
bioavailability of controlled-release oxycodone tablets and immediate-release21. Drover DR, Angst MS, Valle M, et al. Input characteristics and bioavailabilityoxycodone solution. J Pharm Sci 1996; 85 (4): 407-10after administration of immediate and a new extended-release formulation of
hydromorphone in healthy volunteers. Anesthesiology 2002; 97 (4): 827-36 38. Abrahamsson B, Alpsten M, Bake B, et al. Drug absorption from nifedipine
22. Davidson MH, Lukacsko P, Sun JX, et al. A multiple-dose pharmacodynamic, hydrophilic matrix extended-release (ER) tablet-comparison with an osmoticsafety, and pharmacokinetic comparison of extended- and immediate-release pump tablet and effect of food. J Control Release 1998; 52 (3): 301-10formulations of lovastatin. Clin Ther 2002; 24 (1): 112-25
39. Lukkari E, Castren-Kortekangas P, Juhakoski A, et al. Effect of food on the23. Bruguerolle B, Lemmer B. Recent advances in chronopharmacokinetics: method- bioavailability of oxybutynin from a controlled release tablet. Eur J Clin
ological problems. Life Sci 1993; 52: 1809-24Pharmacol 1996; 50 (3): 221-3
24. Lemmer B. Chronopharmacokinetics: implications for drug treatment. J Pharm40. McLean A, Browne S, Zhang Y, et al. The influence of food on the bioavailability
Pharmacol 1999; 51: 887-90of a twice-daily controlled release carbamazepine formulation. J Clin Pharma-
25. Lemmer B, Nold G, Behne S, et al. Chronopharmacokinetics and cardiovascular col 2001; 41 (2): 183-6effects of nifedipine. Chronobiol Int 1991; 8 (6): 485-94
41. Guay DR, Gustavson LE, Devcich KJ, et al. Pharmacokinetics and tolerability of26. Scheidel B, Lemmer B. Chronopharmacology of oral nitrates in healthy subjects.
extended-release clarithromycin. Clin Ther 2001; 23 (4): 566-77Chronobiol Int 1991; 8 (5): 409-19
27. Harrison LI, Kehe CR, Ekholm BP, et al. Comparative pharmacokinetics ofmorning and evening doses of once-a-day theophylline capsules. J Pharm Sci Correspondence and offprints: Dr Sanjay Garg, Department of Pharmaceu-1994; 83 (8): 1171-4
tics, National Institute of Pharmaceutical Education and Research (NIPER),28. Thielemann AM, Manquez N, Pinilla E. Chronopharmacokinetics of theophylline
Sector 67, Phase X, SAS Nagar, Punjab 160062, India.administered as a controlled-release tablet. Int J Clin Pharmacol Ther 1996; 34(3): 130-3 E-mail: [email protected]
© Adis Data Information BV 2003. All rights reserved. Am J Drug Deliv 2003; 1 (2)