Embed Size (px)
Citation preview

Minimally Invasive Bone Graft Delivery SystemMinimally Invasive Bone Graft Delivery SystemJon Witten, Lauren Burdock, Frank ZhaoJon Witten, Lauren Burdock, Frank Zhao
Advisors: Paul King, Ph. D.1, Prasad Shastri, Ph.D1, Robert Burden2, Michael Voor, Ph.D2
1: Department of Biomedical Engineering, Vanderbilt University, Nashville, TN2: Department of Orthopaedic Surgery, University of Louisville School of Medicine, Louisville, KY
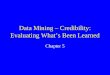
Figure 10: The forces required for the application of the bone graft substitute versus the ratio of the mixture are shown. The average maximum force exerted by the human thumb was found to be 10 lbs. Therefore, the highest usable ratio of plaster to water was 2.1:1.
Results and Discussion
Viscosity vs Ratio
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
1.10
1.7 1.8 1.9 2 2.1 2.2 2.3
Ratio of Plaster to Water
Vis
cosity (K
g/m
s) l
Ratio of Plaster vs Force
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
0 2 4 6 8
Time(s)
Forc
e(lbs) l
2.2
2.1
2
1.9
1.8
Phase I: Viscosity Determination
Figure 11: The viscosity of the bone graft substitute at different ratios of plaster to water is shown. In the subsequent phases of testing, the 2.1:1 mixture with a viscosity of 0.540 kg/m-s was used. This is the optimum viscosity for University of Louisville’s bone graft material.
Phase II: Plug FormationFigure 12: This figure shows the bone graft plug that was formed using the bidirectional injection pin. Bone graft substitute (plaster) was injected into the centrifuge tube filled with a bone marrow substitute (jelly). All three pin designs were tested with the optimum viscosity of plaster. The unidirectional-elongated port pin left voids in the plug while the straight pin required movement in order to create an acceptable plug. The bidirectional pin was the only design to create a uniform plug in the cross-section of the centrifuge tube. Therefore, we chose the bidirectional pin design for Phase III testing in the porcine femur.
1
2
3
4
5
Phase III: Porcine Femur Analysis
A-P
M-L
Conclusion:A minimally invasive method for delivering bone graft material has been achieved. The design can be incorporated into an external fixation system for use in treating long bone fractures. Through testing, the optimum viscosity for the bone graft under development by University of Louisville was determined to be 0.540 kg/m-s. The accuracy of the delivery system can be improved by further testing under optimized physiological conditions. The quality of the bone graft plug can be improved by increasing the volume of bone graft material delivered into the bone.
Figure 13: The A-P figure shows an x-ray image of the porcine femur in the anterior-posterior orientation. The M-L figure shows the femur in the medial-lateral orientation. The dark regions of the images show the presence of the plaster plug. The arrows denote the area of best plug formation.
Figure 14: Section 1 of the femur shows a cross-section of the injection site. The plaster distribution in this section shows almost no lateral movement from the injection port. The plaster traveled along the longitudinal axis of the femur.
Figure 15: Section 2 of the femur shows a lateral expansion of the plaster at the base. but an absence of plaster at the top. At this point the plaster shows 30 percent cross-sectional coverage.
Figure 16: Section 3 of the femur shows further lateral expansion of the plaster at the base. At this point the plaster shows 50 percent cross-sectional coverage. The top of the femur section still lacks plaster, making plug formation incomplete.
Figure 17: Section 4 of the femur shows further lateral expansion of the plaster at the base. At this point the plaster has traveled along the sides of the wall and shows 65 percent cross-sectional coverage of the interior. This section corresponds to the arrows in the x-ray images.
Figure 18: Section 5 of the femur bone shows a severe decrease in the presence of the plaster. The pressure release can be clearly seen in the picture. The coverage of the plaster is now 5 percent of the cross sectional area. The entire 10cc syringe load had been injected. A larger syringe may be needed to provide more material for better coverage.
Prototype Designs
MethodsPhase I: Viscosity Determination
Phase II: Plug Creation
Phase III: Analysis in a Porcine Femur
Since the device must fit into an external fixation configuration, the delivery system was modeled after external fixation pins, which are 15cm in length and 3-5mm in diameter. The pin (Figure 4) is hollow and capable of passing bone graft through the lumen of the pin to the interior of the bone. It will not be used to stabilize the bone like traditional pins.
For ease of machining and reduced cost, the length of the prototype was shortened to 10cm and constructed from aluminum instead of surgical grade stainless steel. The pin has an outer diameter of 5mm for the upper half and 3mm for the lower half. The inner diameter is a constant 2mm.
Figure 6: Bidirectional circular port pin
Three output ports were designed for testing to ensure complete bone graft plug creation (Figures 5-7).
Figure 5: Straight pin.
A standard 12cc syringe will provide the force for application. A plastic interface secures the syringe and pin forming an air tight seal. The syringe is loaded with 20cc of bone graft. Then the plastic interface and the desired pin are attached (Figure 8). In order to minimize the introduction of air into the system, the pin must be primed by pushing bone graft through until it emerges from the output port. After the pin is inserted into the bone, the output ports are aligned in a favorable position and force is applied to empty the contents of the syringe. Once this is complete, the pin system can be removed.
In the third phase of testing, the best pin design was used to pass the optimum viscosity into a porcine femur. The plug was then analyzed using X-ray imaging and manual sectioning.
The highest viscosity of Plaster of Paris that can be manually passed through the straight pin was tested with the different pin designs in plastic centrifuge tubes. The centrifuge tubes were filled with jelly to simulate bone
Different mixtures of Plaster of Paris were tested to determine which could be passed through the straight pin at forces less than 10lbs (the maximum force a surgeon can manually apply to the syringe). We experimented with Plaster of Paris (the bone graft substitute) at plaster to water ratios of 1.8:1, 1.9:1 (recommended by manufacturer), 2:1, 2.1:1, and 2.2:1. The Plaster of Paris was first mixed to the desired ratio and then the syringe was loaded with approximately 10cc. Once the pin was primed, the device was positioned under the Materials Testing System (Figure 9) which was programmed with a flow rate of 1cc/second. The MTS software recorded the displacement, time, and force. Using Poiseuille's Law and the known variables, viscosity () was calculated:
P = pressureF = force applied by the MTS machineA = surface area of the syringe plungerr = inner diameter of the pin (2mm)Q = flow rate
L = length from the opening of the syringe to the end of the pin
Figure 9: MTS set-up for Phase I
LQ8
rAF
LQ8
rP44
Test Pin designMovement/Alignment of Pin
During Plaster Delivery
1Straight pin
Held steady in center of bone
2 Slowly moved out
3 Bidirectional circular ports Held steady with ports pointed at walls
4 Unidirectional elongated portHeld Steady with port pointed along
length of tubeTable 1: Phase II of Methods: Testing for complete plug formation using the highest viscosity of Plaster of Paris that can manually be passed through the pin
marrow and to provide high contrast to the Plaster of Paris. A break was not created to imitate a fracture since well-reduced fractures in the human body are surrounded by fascia, which keep the marrow and grafting material in the bone. Two holes were drilled approximately 3cm apart (1.5cm on either side of the imaginary fracture). One hole allowed the insertion of the pin for testing while the other acted as a pressure release. Testing was performed with the different pins as explained in Table 1 and then the plug formation was examined.
Pin Plastic Interface
Syringe
Figure 7: Unidirectional elongated port pin
Delivery Protocol
Figure 4: Wire frame of pin device
Figure 8: Bone graft delivery system
Acknowledgements: This project was facilitated with contributions by Dr. Ginger Holt, Dr. Franklin Shuler, Chrissy Marasco, Seid Waddell, and Dr. Joseph Cheng
Overview
• Approximately 6 million fractures occur each year in the United States, of which 1.5 million involve long bones. These injuries produce considerable morbidity and impairment in individuals of both genders and all age groups, regardless of socioeconomic circumstances. • On an annual basis, fractures account for over 36 million lost days from work, more than 7 million days missed from school, approximately 6.4 million days of hospitalization, nearly 9.4 million visits to healthcare providers, and cost society an estimated $21 billion. • Among the most problematic and burdensome fractures are those 5-10% that demonstrate delayed healing, mal-union, and non-union.
The physiology of bone presents unique characteristics when the normal loading effects encountered during daily life are exceeded. If a bone fractures during a traumatic event, the outcome and future health of the patient can be positively affected by operative means. At the root of the healing process is a fundamental mechanism by which bone tissues interact to restore a bone’s structural properties. One surgical technique that has exploited this natural healing process is the application of a bone graft material to the fracture site with the aim of facilitating the natural repair and eventual return of healthy bone structure. Figure 1: Immobilization of fracture
Introduction
Physiology of Fracture Healing
Design Objectives• This project is a proof-of-concept endeavor.
• The goal of this project is to develop a minimally invasive delivery system for a proprietary bone graft material. This bone graft material is currently under investigation at the Orthopaedic Bioengineering Laboratory of the University of Louisville.
• The delivery device should provide accurate delivery of bone graft material, forming a ‘plug’ of material filling the Medullary cavity. The plug will exist between points above and below the fracture site.
• The design should integrate with contemporary external fixation devices used on human patients.
• When testing the prototype device, viscosity parameters will be determined for manual application of a bone graft substitute.
• The maximum allowable viscosity measured during testing of the device will dictate characteristics of the bone graft material being developed by the Orthopaedic Bioengineering Laboratory.
Figure 3: Contemporary External Fixation Device from Stryker applied to model tibia
• There are many different bone graft materials and implantation methods. • Bone graft materials can be divided into four groups: autograft, allograft, xenograft, and synthetic compounds.
Bone Graft Research
• The most effective treatment is to replace the tissues in the fracture site with a bone graft, which essentially initiates an entirely new repair process. The preventative application of a bone graft material to qualifying fractures promises significant reduction in morbidity experienced by fracture patients.
Natural fracture healing may be divided into inflammatory, reparative, and remodeling phases. The initial inflammatory phase serves to immobilize the fractured bone and activate the cells responsible for repair. Once set in motion, the subsequent steps in the reparative and remodeling phases are initiated.
• If a mistake is made, the process may take a wrong turn rather than stopping, with no way to recover the conditions at the point of the error.
• Delayed-union, non-union, and mal-union are conditions caused by a defect in the initial mobilization of the repair process, and once the problem becomes apparent, there is no way to correct it by manipulating the current group of cells.
Figure 2: Sample synthetic bone graft material
• Autograft is material harvested from the patient; allograft comes from a different member of the same species; xenograft is material obtained from a different species; synthetic compounds comprise polymers that mimic the properties of bone.• Used separately and in combinations, these sources of graft provide varying degrees of positive biological incorporation and stability when grafting is indicated. Previous bone grafting techniques work; however, different materials require different methods of application. Often these methods require open reduction followed by application of bone graft. • In an effort to reduce morbidity issues and improve healing efforts in fracture patients, research continues to focus on both the quality and the delivery method of bone graft.
Market Analysis