Embed Size (px)
Citation preview

Milder phenotypes of glucose transporter type 1 deficiency syndrome
GEETHA ANAND1 | ANURUDDHA PADENIYA1 | DONNCHA HANRAHAN2 | HANS SCHEFFER3 |ZENOBIA ZAIWALLA1 | DEBBIE COX1 | NICHOLAS MANN4 | JOHN HEWERTSON5 | SUE PRICE5 |ANDREA NEMETH6 | TODOR ARSOV7 | INGRID SCHEFFER8 | SANDEEP JAYAWANT1 | MICHAEL PIKE1 |TONY MCSHANE1
1 Department of Paediatric Neurology, John Radcliffe Hospital, Oxford, UK. 2 Department of Paediatric Neurology, Royal Belfast Hospital for Sick Children, Belfast, NorthernIreland, UK. 3 Division of DNA-diagnostics, Department of Human Genetics, Radboud University Nijmegen Medical Centre, the Netherlands. 4 Department of Paediatrics, RoyalBerkshire Hospital, Reading, UK. 5 Department of Paediatrics, Northampton General Hospital, Northampton, UK. 6 Department of Genetics, Churchill Hospital, Oxford, UK.7 Molecular Genetics Laboratory, Department of Medicine, The University of Melbourne, Australia. 8 Royal Children's Hospital, The University of Melbourne, Australia.
Correspondence to Dr Geetha Anand, Department of Paediatric Neurology, John Radcliffe Hospital, Oxford, UK. E-mail: [email protected]
PUBLICATION DATA
Accepted for publication 1st February 2011Published online 24th March 2011.
ABBREVIATIONGLUT1DS Glucose transporter type 1
deficiency syndrome
Glucose transporter type 1 deficiency syndrome (GLUT1DS) is a treatable condition resulting
from impaired glucose transport into the brain. The classical presentation is with infantile-onset
epilepsy and severe developmental delay. Non-classical phenotypes with movement disorders
and early-onset absence epilepsy are increasingly recognized and the clinical spectrum is expand-
ing. The hallmark is hypoglycorrhachia (cerebrospinal fluid [CSF] glucose<2.2mmol ⁄ l) in the pres-
ence of normoglycaemia with a CSF ⁄ blood glucose ratio of less than 0.4. GLUT1DS is due to a
mutation in the solute carrier family 2, member 1 gene (SLC2A1). We present five individuals (four
males, one female), all of whom had a mild phenotype, highlighting the importance of considering
this diagnosis in unexplained neurological disorders associated with mild learning difficulties,
subtle motor delay, early-onset absence epilepsy, fluctuating gait disorders, and ⁄ or dystonia. The
mean age at diagnosis was 8 years 8 months. This paper also shows phenotypical parallels
between GLUT1DS and paroxysmal exertion-induced dyskinesia.
Glucose transporter type 1 deficiency syndrome (GLUT1DS)is a treatable neurometabolic disorder that was first describedby De Vivo et al. in 1991.1 The classic phenotype that consti-tutes 80% of the cases so far described presents with infantileseizures, severe developmental delay, acquired microcephaly,and a varying degree of spasticity.2–4 It is the non-classicalphenotype, accounting for the remaining 15 to 20% of cases,that has attracted attention in recent years.4 This groupincludes movement disorders without epilepsy, early-onsetabsence epilepsy, paroxysmal exertion-induced dyskinesia, andvarious carbohydrate-responsive symptoms.2,3 Brockmannreported an impressive correlation between food intake andmotor and cognitive performance in patients withGLUT1DS.3 We present a series of five individuals, four ofwhom were diagnosed in the year 2009 to 2010 and one in1999. All five had a milder phenotype than classical GLUT1encephalopathy. Informed consent for the publication of thesereports was obtained from all the families.
CASE REPORTCase 1An 8-year-old female was referred with pharmacoresistant,early-onset absence epilepsy; pre- and perinatal history werenormal. There were no developmental concerns and her head
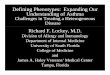
circumference followed the 25th centile. At the age of 2 yearsshe developed absence seizures. Her electroencephalogram(EEG) on three occasions showed 3–4 Hz spike-and-wave dis-charges (Fig. 1) with clinical absences accompanied by a myo-clonic element in the form of a head drop. She was treatedwith six anticonvulsants: sodium valproate, ethosuximide,lamotrigine, clobazam, acetazolamide, and topiramate. Shehad mild learning difficulties and attended a mainstreamschool. Magnetic resonance imaging (MRI) of her brain wasnormal. At the age of 15 her parents mentioned that her sei-zures were better after meals and sugary drinks. Using thisinformation, 7 years after her initial presentation, a diagnosisof GLUT1DS was made following a lumbar puncture(Table I). She had a heterozygous mutation in the exon 4 ofthe SLC2A1 gene (c.464C>T p.Ala155Val). She was started ona ketogenic diet and within weeks had complete resolution ofabsence seizures.
Case 2A 2-year-old male presented with delayed motor milestones;pre- and perinatal history were normal. He sat without sup-port at 9 months and at 2 years was cruising around furniturebut not walking. His head circumference was on the 0.4th cen-tile at the age of 2; previous measurements were not available.
664 DOI: 10.1111/j.1469-8749.2011.03949.x ª The Authors. Developmental Medicine & Child Neurology ª 2011 Mac Keith Press
DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY CASE REPORT

He had hyperreflexia and dystonic posturing. Brain MRI wasnormal. Genetic analysis showed a heterozygous mutation inthe exon 9 of SLC2A1 gene (c.1227_1230delCTCCp.Phe409fs). He was started on a ketogenic diet and within amonth his parents reported improved concentration, mobility,and energy levels. He started walking, though with anunsteady gait, within 3 months of starting a ketogenic diet.(See Video S1, supporting material published online.).
Case 3A 10-year-old male presented with a fluctuating gait disorder,which was worse on exertion. His pre- and perinatal historywere normal. He started walking at 15 months but was knownto have frequent falls. On walking for longer than 10 minuteshis gait was became unsteady, associated with dystonia oflimbs. He also had learning difficulties and went to a specialschool from the age of 5 years. His head circumference wasless than 2nd centile (mother’s head circumference, 25th cen-tile; father’s head circumference, 50th centile). He had anabnormal gait with dystonic posturing and was unsteady withinvoluntary movements. His brain MRI was normal. Geneticanalysis showed a heterozygous mutation in SLC2A gene(c.[880T>G (+) 881C>T] p.Ser294Val). He was started on amodified Atkins diet as he found it difficult to comply with theketogenic diet. When ketosis was adequate, which was rare,there was some improvement in gait and he did not have falls.
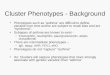
Case 4A 7-year-old male was referred with a fluctuating gait disorderand ‘clumsiness’. He had initially been seen at age 2 years withmild motor delay and absence seizures. His EEG showed 2–3 Hz spike-and-wave discharges with clinical absence seizuresand myoclonus (Fig. 2). He responded well to valproate and
treatment was withdrawn at 5 years. Absence seizures recurredat 7 years. He was clumsy, with a dystonic gait abnormalitythat was most obvious after exertion. He had mild learningdifficulties and attended mainstream school, with a few hoursof extra support every week. He had a wide-based gait thatwas difficult to categorize. An MRI of his brain was normalapart from slightly prominent CSF spaces. An EEG againshowed generalized 2–4 Hz spike-and-wave discharges associ-ated with clinical absence seizures. Genetic analysis showed aheterozygous mutation in SLC2A1 gene (c.506T>C p.Leu169-Pro). A ketogenic diet was tried for 12 weeks, but both patientand family abandoned the diet because they found it too diffi-cult and there was no symptom improvement. Seizures werecontrolled with lamotrigine. (See Video S2, supporting mate-rial published online.)
Case 5A 9-year-old male presented with myoclonus, atypical absenceseizures, and a fluctuating gait disorder. After a normal pre-and perinatal history, he was well for 1 year, after which hestarted having myoclonic seizures and subsequently atypicalabsence seizures which were difficult to manage with antiepi-leptic drugs. They were worse in the early morning andimproved with food. Later in childhood he developed a parox-ysmal gait disorder, which had both ataxic and dystonic ele-ments. His gait disorder was worse with exertion. His IQ was
Figure 1: Electroencephalogram showing 3–4 Hz spike-and-wave discharges associated with absence seizures.18
What this paper adds• GLUT1DS is possibly an under-diagnosed condition.• Diagnosis of GLUT1DS in children with early-onset absence epilepsy and ⁄ or
movement disorders should be considered even if there are only mild learningdifficulties.
• This paper reports phenotypical parallels between GLUT1DS and paroxysmalexertion-induced dyskinesia.
Case Report 665

in the average range and his head circumference rangedbetween the 9th and 25th centiles. He had a heterozygousmissense mutation in exon 7 of SLC2A1 gene (c.884C>Tp.Thr295Met). He was started on a ketogenic diet. His gaitproblem improved initially but then recurred and was lesssevere than before treatment. On the diet, seizure frequencyreduced significantly from a frequency of 10 per day to 1 orfewer per week.
DISCUSSIONThe constellation of infantile epilepsy, movement disorders,acquired microcephaly, and hypoglycorrhachia is characteris-tic of GLUT1DS. Owing to improved awareness of the condi-tion, milder phenotypes are increasingly recognized.5 Since1991, about 100 patients have been identified worldwide.6
Here we describe five cases of GLUT1DS with phenotypesmilder than the classical GLUT1 encephalopathy. Of the five,three SLC2A1 mutations have been described before4,7–10 andtwo are new (cases 2 and 3). Parental testing was available inall but one case (case 1), and the mutations in those cases wereall found to be de novo.
The phenotypes of the patients described in the literaturesharing mutations with case 1 and case 5 are very similar towhat was seen in our patients.8 They had early-onset pharma-coresistant absence seizures and myoclonic epilepsy and ataxiawith microcephaly respectively. A frameshift mutation involv-ing the same nucleotide (c.506) seen in case 4 has also beendescribed before.7 However, that patient presented with infan-tile seizures, developmental delay, and microcephaly, whereasin our patient a fluctuating gait disorder with clumsiness that
Table I: Summary of clinical, molecular, and biochemical features of patients with GLUT1DS
Patient number
1 2 3 4 5
Phenotype Early-onsetresistant atypicalabsences normaldevelopment,mild learningdifficulties.IQ: NAb
Mild motor delay,dystonia,developmentalquotient: 72 at 3y6mo
Fluctuating gaitdisorder,dystonia, mildlearningdifficulties. IQ: 84
Clumsiness,atypical absenceseizures,fluctuating gaitdisorder, mildlearningdifficulties. IQ: 85
Myoclonus,atypical absenceseizures,fluctuating gaitdisorder, mildcognitive problems.IQ: 100
Head circumference,cm (age atmeasurement)
54; 25th centile(15y)
46; 0.4th centile(2y)
50.5; 0.4th–2ndcentile (9y 6mo)
54; 50–75th centile(9y 6mo)
50.2; 9–25th centile(7y)
Mutation in SLC2A1 c.464C>Tp.Ala155Val
c.1227_1230delCTCC p.Phe409fs
c.[880T>G (+)881C>T] p.Ser294Val
c.506T>Cp.Leu169Pro
c.884C>Tp.Thr295Met
Parental phenotype ⁄genotype
Asymptomatic ⁄ NA Asymptomatic ⁄ normal Asymptomatic ⁄ normal Asymptomatic ⁄ normal Asymptomatic ⁄ normal
Age at symptomonset, y
2 2 3 2 1
Age at diagnosis, y 15 2y 11mo 10 7 9
Fasting CSF glucose,mmol ⁄ l
2.3 2 2 2.1 2.1
Paired blood glucose,mmol ⁄ l
5.3 Not done 5 4.4 5.1
CSF ⁄ blood glucoseratio
0.43 – 0.4 0.47 0.41
CSF lactate, mmol ⁄ l 0.9 0.9 0.9 0.8 0.96
EEG 3–4 Hz spike-and-wave dischargeswith absenceseizures
Not done Normal 2–3 Hz spike-and-wave activity withfrequent absenceseizures
Generalizedpolyspike-and-wavedischarges
Response to ketogenicdiet
Excellent seizurecontrol
Improved mobility When ketosis isadequate,improvement ingait andreduction in fallsa
No response tobrief trial ofketogenic diet;a
seizurescontrolled withlamotrigine
Very goodresponse of allsymptoms
aDifficulty in adhering to ketogenic diet. bSchool performance was a year behind in some subjects (mainstream). NA, not available; CSF,cerebrospinal fluid; EEG, electroencephalogram.
666 Developmental Medicine & Child Neurology 2011, 53: 664–668

was worse on exertion was a key feature, along with atypicalabsences. There was also no microcephaly (Table I).
Leen et al. described two different phenotypes: (1) theclassical phenotype (84%) with seizures, subdivided into early-onset (<2y; 65%) and late-onset (18%); (2) a non-classicalphenotype, with developmental delay and movement disorder,without epilepsy (15%).8 Various other authors have alsodescribed the latter phenotype.4,7,11–13 SLC2A1 mutationscausing sporadic paroxysmal exertion-induced dyskinesia withor without epilepsy have been reported.14–16 In our series, case1 had milder forms of the late-onset classical phenotype withlate-onset seizures.8 Case 2 was a non-classical phenotype withdevelopment delay and dystonia but without seizures.8 Cases3, 4, and 5 fitted the phenotypes described by Schneider et al.,Suls et al., and Weber et al.14–16 with paroxysmal exertion-induced dyskinesia with or without epilepsy.
Atypical absence seizures with myoclonus seen in three ofthe five patients (cases 1, 4, and 5) in this series is in keepingwith the reports in the literature,17–20 where similar cases havebeen treated for several years as generalized epilepsy. Interest-ingly, although sodium valproate has been shown to inhibitGLUT1 in vitro,21 in our patient (case 4) there was completeresolution of absence seizures initially using this drug. Thishas been reported in one patient in the recent series by Sulset al.22 The clue to diagnosis of GLUT1DS is the early onsetof absence seizures. The absence seizures are usually drugresistant, and EEG shows generalized 2.5–4 Hz spike-and-wave discharges.7
Leary et al.18 described EEG features in 20 children withGLUT1DS. In all ages a normal interictal EEG was the mostcommon EEG finding. When abnormalities occurred, focal
slowing or epileptiform discharges were seen in infants, but inolder children a generalized 2.5–4 Hz spike-and-wave patternwas observed. Seizure types were absences, myoclonic, partial,and astatic.18 Both electrographically (Figs. 1 and 2) and clini-cally (cases 1, 4, and 5), this is very similar to what we observed.
A fluctuating gait disorder made worse by exertion was seenin three patients in our series (cases 3, 4, and 5); all had dysto-nia. This was similar to paroxysmal exertion-induced dyskine-sia that has been described with Glut-1 gene mutations.14–16 Itis yet unclear whether paroxysmal exertion-induced dyskinesiais a separate adult entity allelic with GLUT1DS or an atypicaladult presentation of GLUT1DS. Our paper suggests pheno-typical parallels between both diseases.
Three of our four children of school age had low averageIQ or mild learning difficulties but were attending mainstreamschool, reflecting their mild phenotype.
The diagnosis of GLUT 1 is currently made using a combi-nation of hypoglycorrhachia (fasting CSF glucose <2.2mmol ⁄ land CSF ⁄ plasma glucose ratio <0.4; Klepper and Voit23) andmutational analysis of the SLC2A1 gene. When feasible, it isrecommended that the red blood cell glucose uptake assay isperformed. It is reduced to half of the control values inGLUT1DS.24 Klepper et al. showed that sensitivity of thisassay was 86% and specificity was 97%.24 Although perform-ing a lumbar puncture in children with milder phenotypesmay be a difficult undertaking, the danger of just relying onthe mutational analysis alone is that we run the risk of missingaround 30% of cases that are negative for the mutation.7
However, it is worth proceeding to lumbar puncture in sus-pected cases where SLC2A1 mutational analysis has first beenshown to be negative.
Figure 2: Electroencephalogram showing 2–3 Hz spike-and-wave activity associated with absence seizures.18
Case Report 667

The CSF ⁄ plasma glucose ratio in our series was slightlyhigher than that normally described in children withGLUT1DS: 0.33, SD 0.01.25 This confirms the view thatmilder phenotypes may have higher ratios.3,20,21 The normalCSF ⁄ plasma glucose ratio described in controls is 0.65, SD0.01.23,26
The treatment currently recommended for GLUT1DS is aketogenic diet. It works by providing ketones as an alternativefuel for the brain. The ketogenic diet does not influence theimpaired glucose transport. The effect of the diet on seizurecontrol is more impressive than the effect on cognitive difficul-ties.7 The seizures in two of the three patients in our seriesresponded well but in one case (case 4) there was no responsedespite good compliance and adequate ketosis for 12 weeks.In the series reported by Klepper et al.,27 two of the 15patients had seizure recurrence after 2½ years, despiteadequate ketosis. We have not followed up our patients forlong enough to comment on the impact of the diet on cogni-
tion. Recently, the modified Atkins diet, which is much lessrestrictive than the ketogenic diet in terms of total calories andprotein, has been shown to be effective and well tolerated.28–30
GLUT1DS should be considered in children presentingwith mild motor delay, dystonia, fluctuating gait abnormali-ties, or early-onset absence epilepsy, even in the absence ofsignificant learning difficulties.7,8 It is important to obtainpaired CSF ⁄ plasma glucose measurements. In the absence ofsimultaneous blood glucose, an absolute low-fasting CSF glu-cose of less than 2.2mmol ⁄ l suggests this diagnosis. A lumbarpuncture provides the clue to the diagnosis of GLUT1DS andsignificantly reduces the time to starting a ketogenic diet.22
Genetic analysis is currently not undertaken in the UK but isavailable in the Netherlands and USA.
ONLINE MATERIAL ⁄ SUPPORTING INFORMATIONAdditional material and supporting information for this paper may be
found online.
REFERENCES
1. De Vivo DC, Trifiletti RR, Jacobson RI, Ronen GM, Beh-
mand RA, Harik SI. Defective glucose transport across the
blood–brain barrier as a cause of persistent hypoglycorrha-
chia, seizures and developmental delay. N Engl J Med 1991;
325: 703–9.
2. Klepper J. Impaired glucose transport into the brain: the
expanding spectrum of glucose transporter type 1 deficiency
syndrome. Curr Opin Neurol 2004; 17: 193–6.
3. Brockmann K. The expanding phenotype of GLUT 1 defi-
ciency syndrome. Brain Dev 2009; 31: 545–52.
4. Wang D, Pascual JM, Yang H, et al. Glut-1 deficiency syn-
drome: clinical, genetic, and therapeutic aspects. Ann Neurol
2005; 57: 111–8.
5. Pascual JM, Lecumberri B, Wang D, Yang R, Engelstad K,
De Vivo DC. Type 1 glucose transporter (Glut1) deficiency:
manifestations of a hereditary neurological syndrome.
Rev Neurol 2004; 38: 860–4.
6. Klepper J. Glucose transporter 1 deficiency syndrome. J
Pediatr Neurol 2010; 8: 107–8.
7. Klepper J, Leiendecker B. Glut 1 deficiency syndrome –
2007 update. Dev Med Child Neurol 2007; 49: 707–16.
8. Leen WG, Klepper J, Verbeek MM, et al. Glucose trans-
porter-1 deficiency syndrome: the expanding clinical and
genetic spectrum of a treatable disorder. Brain 2010; 133:
655–70.
9. Wang D, Yang H, Shi L, et al. Functional studies of the
T295M mutation causing Glut1 deficiency: glucose efflux
preferentially affected by T295M. Pediatr Res 2008; 64:
538–43.
10. Fujii T, Morimoto M, Yoshioka H, et al. T295M-associated
Glut1 deficiency syndrome with normal erythrocyte 3-OMG
uptake. Brain and Development 2011; 33: 4: 316–320.
doi:10.1016 ⁄ j.braindev.2010.06.012 (Published online
12th July 2010).
11. Overweg-Plandsoen WC, Groener JE, Wang D, et al.
GLUT-1 deficiency without epilepsy—an exceptional case.
J Inherit Metab Dis 2003; 26: 559–63.
12. Hennecke M, Wang D, Korinthenberg R, et al. GLUT1
deficiency syndrome with ataxia, acquired microcephaly and
leukoencephalopathy in monozygotic twins. Neuropediatrics
2005; 36: 140. (Abstract).
13. Friedman JR, Thiele EA, Wang D, et al. Atypical GLUT1
deficiency with prominent movement disorder responsive to
ketogenic diet. Mov Disord 2006; 21: 241–5.
14. Schneider SA, Paisan-Ruiz C, Garcia-Gorostiaga I, et al.
GLUT 1 Gene mutations cause sporadic paroxysmal exer-
cise-induced dyskinesias. Mov Disord 2009; 24: 1684–96.
15. Suls A, Dedeken P, Goffin K, et al. Paroxysmal exercise-
induced dyskinesia and epilepsy is due to mutations in
SLC2A1, encoding the glucose transporter GLUT1. Brain
2008; 131: 1831–44.
16. Weber YG, Storch A, Wuttke TV, et al. GLUT1 mutations
are a cause of paroxysmal exertion-induced dyskinesias and
induce hemolytic anemia by a cation leak. J Clin Invest 2008;
118: 2157–68.
17. Roulet-Perez E, Ballhausen D, Bonafe L, et al. Glut 1 defi-
ciency syndrome masquerading as idiopathic generalised epi-
lepsy. Epilepsia 2008; 49: 1955–8.
18. Leary LD, Wang D, Nordli DR Jr, et al. Seizure characteri-
sation and electroencephalographic features in Glut 1 defi-
ciency syndrome. Epilepsia 2003; 44: 701–7.
19. Hirsch LJ. Absence epilepsy with onset before three years:
could this be Glut 1 deficiency syndrome (De Vivo
syndrome)? Epilepsia 2004; 45: 92. (Letter)
20. Ito S, Oguni H, Ito Y, Ishigaki K, Ohinata J, Osawa M. Mod-
ified Atkins diet therapy for a case with glucose transporter
type 1 deficiency syndrome. Brain Dev 2008; 30: 226–8.
21. Wong HY, Chu TS, Lai JC, et al. Sodium valproate inhibits
glucose transport and exacerbates Glut 1 deficiency in vitro.
J Cell Biochem 2005; 96: 775–85.
22. Suls A, Mullen A, Weber YG, et al. Early onset absence epi-
lepsy caused by mutations in glucose transporter GLUT1.
Ann Neurol 2009; 66: 415–9.
23. Klepper J, Voit T. Facilitated glucose transporter protein
type 1 (Glut 1) deficiency syndrome: impaired glucose trans-
port into brain – a review. Eur J Pediatr 2002; 161: 295–304.
24. Klepper J, Garcia-Alvarez M, O’Driscoll KR, et al. Erythro-
cyte 3-O-methyl-D-glucose uptake assay for diagnosis of glu-
cose-transporter-protein syndrome. J Clin Lab Anal 1999;
13: 116–21.
25. Wang D, Pascual JM, De Vivo DC. Glucose transporter type
1 deficiency syndrome. Gene Reviews. Bookshelf ID:
NBK1430 PMID: 20301603 (Published online 30th July
2002; last update 7th July 2009).
26. Klepper J, Willemsen M, Verrips A, et al. Autosomal domi-
nant transmission of GLUT 1 deficiency. Hum Mol Genet
2001; 10: 63–8.
27. Klepper J, Scheffer H, Leiendecker B, et al. Seizure control
and acceptance of the ketogenic diet in GLUT1 deficiency
syndrome: a 2- to 5-year follow up of 15 children enrolled
prospectively. Neuropediatrics 2005; 36: 302–8.
28. Ito Y, Gerstsen E, Oguni H, et al. Clinical presentation,
EEG studies, and novel mutations in two cases of GLUT 1
deficiency syndrome in Japan. Brain Dev 2005; 27: 311–7.
29. Kossoff EH, Krauss GL, McGrogan JR, Freeman JM. Effi-
cacy of the Atkins diet as therapy for intractable epilepsy.
Neurology 2003; 61: 1789–91.
30. Kang HC, Lee HS, You SJ, Kang du C, Ko TS, Kim HD.
Use of a modified Atkins diet in intractable childhood epi-
lepsy. Epilepsia 2007; 48: 182–6.
668 Developmental Medicine & Child Neurology 2011, 53: 664–668