Embed Size (px)
Citation preview

Esercizi callistenici e precoce mobilizzazione in TI
Ft Piaggi Giancarlo Fondazione Salvatore Maugeri – Istituto Scientifico di Pavia
U.O. Pneumologia Riabilitativa
Milano 25 Ottobre 2014 - GIORNATA ARIR: falsi miti in riabilitazione respiratoria Fondazione IRCCS Ca’ Granda – Ospedale Maggiore Policlinico
Sfatare ……
SIGNIFICATO: Dimostrare inconsistente o falsa una credenza o un’opinione radicate nella massa SINONIMI: demolire, screditare, smentire, smascherare, scoprire, distruggere, ridimensionare, demitizzare, smitizzare, contraddire, esautorare, disconoscere

Il mito
Indica qualcosa di favoloso o di irraggiungibile, che viene in qualche modo amplificato e allontanato dal reale. Un aspetto/persona che catalizza l’attenzione del mondo intero e per molto tempo. Si pensi ad espressioni come 'il mito dei Rolling Stones‘.

Il mito
39.200.000 risultati

Esercizi callistenici
Sono veramente un mito?

Callistenici: Definizione
La parola deriva da due termini greci, “kalos” che significa bellezza e “sthenos” ovvero forza. Calisthenics è un termine inglese che identifica un insieme di esercizi fisici (di forza e di allungamento/stretching) a corpo libero o con utilizzo di attrezzatura molto semplice. A volte si trovano anche i termini calisthenic e callisthenic che di fatto identificano lo stesso concetto.
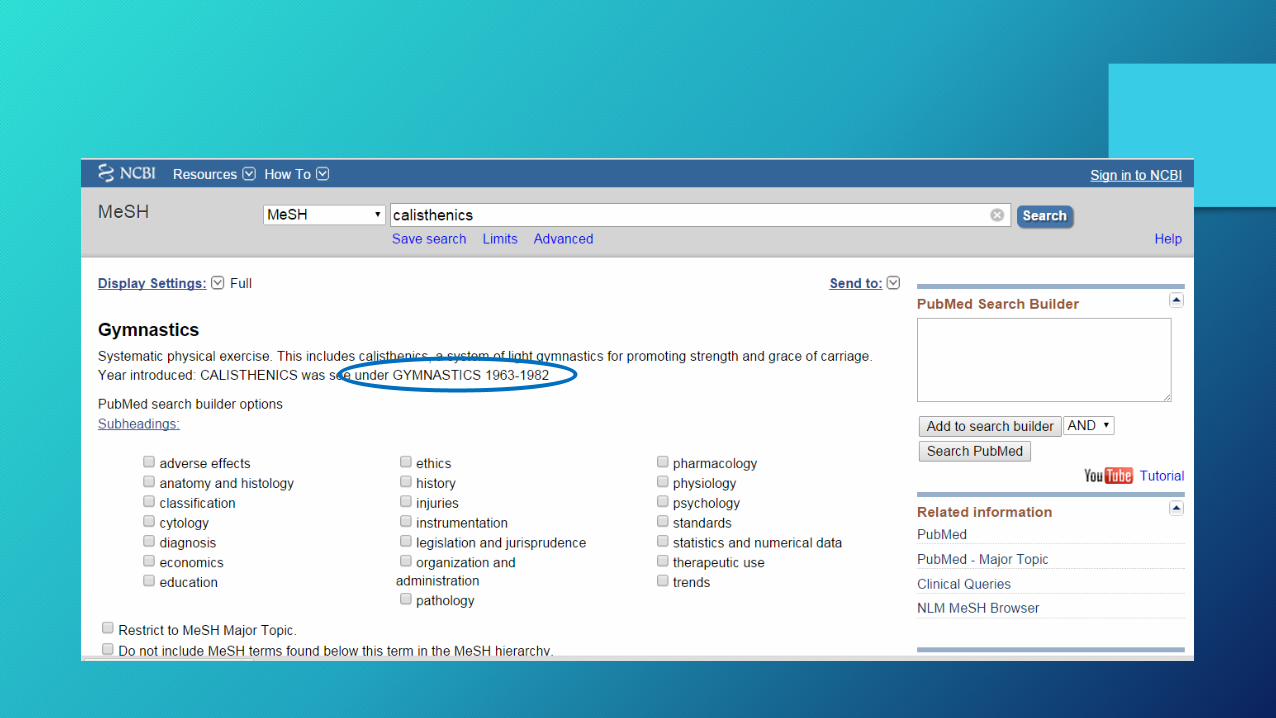

Esercizi callistenici in letteratura
14 articoli

Esercizi callistenici
Probabilmente il termine «esercizi callistenici» in Riabilitazione respiratoria è molto più in uso in Italia
rispetto al resto del mondo


The results of this study demonstrate that no difference in Vo2 exists
between healthy women and women with CAD when they are performing
calisthenics in the range of 1.6 to 2.9 METS
1,2
2,0
1,6
1,3
METS

Takahashi et al. Japanese Journal of Comprehensive Rehabilitation Science (2011)
67 males with stable COPD undergoing outpatient treatment. They were randomly assigned to either a calisthenics group (n = 35), performed at home for 3 months and an educational program at the outpatient department, or a control group (n = 32) that underwent only a monthly outpatient educational program.
The CSC is a program of low-intensity calisthenics that consists of stretches, strength training, and aerobic exercises. The purpose of this study was to investigate the effectiveness of PR consisting of CSC in patients with stable COPD undergoing outpatient treatment.
We advocated a program of COPD sitting calisthenics (CSC) that could be performed while being seated in an ordinary chair.
The exercise intensity of the aerobic exercises was set using target dyspnea ratings (TDR), and the exercises were performed at low intensity, rated as 2 (weak level) on the 10-level Borg scale

5 ripetizioni
3 ripetizioni per lato
3 ripetizioni per lato
Takahashi et al. Japanese Journal of Comprehensive Rehabilitation Science (2011)

Per ognuno dei 4 esercizi: 5 contrazioni isometriche da 6’’ l’una
Takahashi et al. Japanese Journal of Comprehensive Rehabilitation Science (2011)

Durata di ogni esercizio 2’ 30’’, serie per ogni esercizio 2 = 20 minuti di lavoro
Takahashi et al. Japanese Journal of Comprehensive Rehabilitation Science (2011)
The exercise intensity of the aerobic exercises was set using target dyspnea ratings (TDR), and the exercises were performed at low intensity, rated as 2 (weak level) on the 10-level Borg scale

1,6 METS 1,7 METS
2,1 METS
1,9 METS
Takahashi et al. Japanese Journal of Comprehensive Rehabilitation Science (2011)
Aderenza alla terapia domiciliare

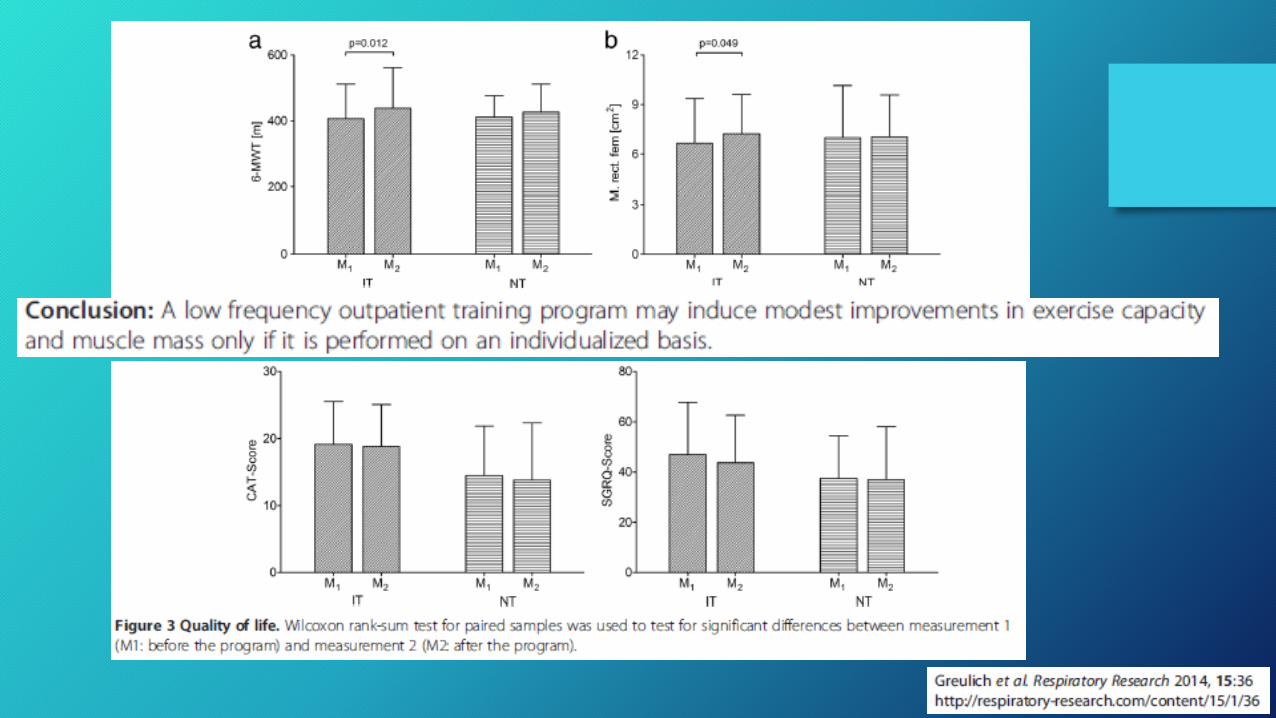
61 stable COPD: - 31 “Individualized Training” (IT) - 30 “Non-individualized Training” (NT)
IT: Each patient received an individual training schedule at the beginning of the training period based on his maximal force and endurance time in different approaches.
NT: The training unit was divided into three parts: warm-up (free movements, stretching) for ten minutes; the main part was a forty minute training which included collectively performed exercises like ball games, stepping, thera-band training and dumbbells. The training period was finalized by a ten minute relaxing exercises period.
Frequenza dell’allenamento: 1 seduta a settimana
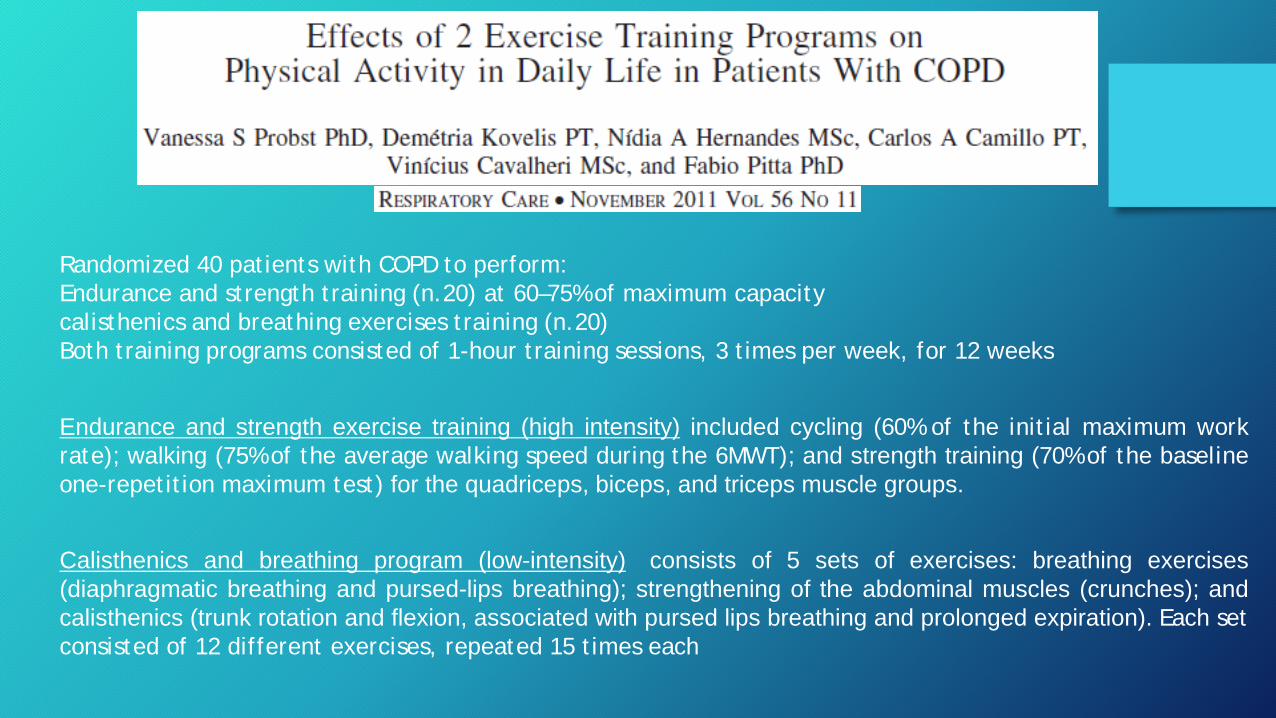
Randomized 40 patients with COPD to perform: Endurance and strength training (n.20) at 60–75% of maximum capacity calisthenics and breathing exercises training (n.20) Both training programs consisted of 1-hour training sessions, 3 times per week, for 12 weeks
Calisthenics and breathing program (low-intensity) consists of 5 sets of exercises: breathing exercises (diaphragmatic breathing and pursed-lips breathing); strengthening of the abdominal muscles (crunches); and calisthenics (trunk rotation and flexion, associated with pursed lips breathing and prolonged expiration). Each set consisted of 12 different exercises, repeated 15 times each
Endurance and strength exercise training (high intensity) included cycling (60% of the initial maximum work rate); walking (75% of the average walking speed during the 6MWT); and strength training (70% of the baseline one-repetition maximum test) for the quadriceps, biceps, and triceps muscle groups.
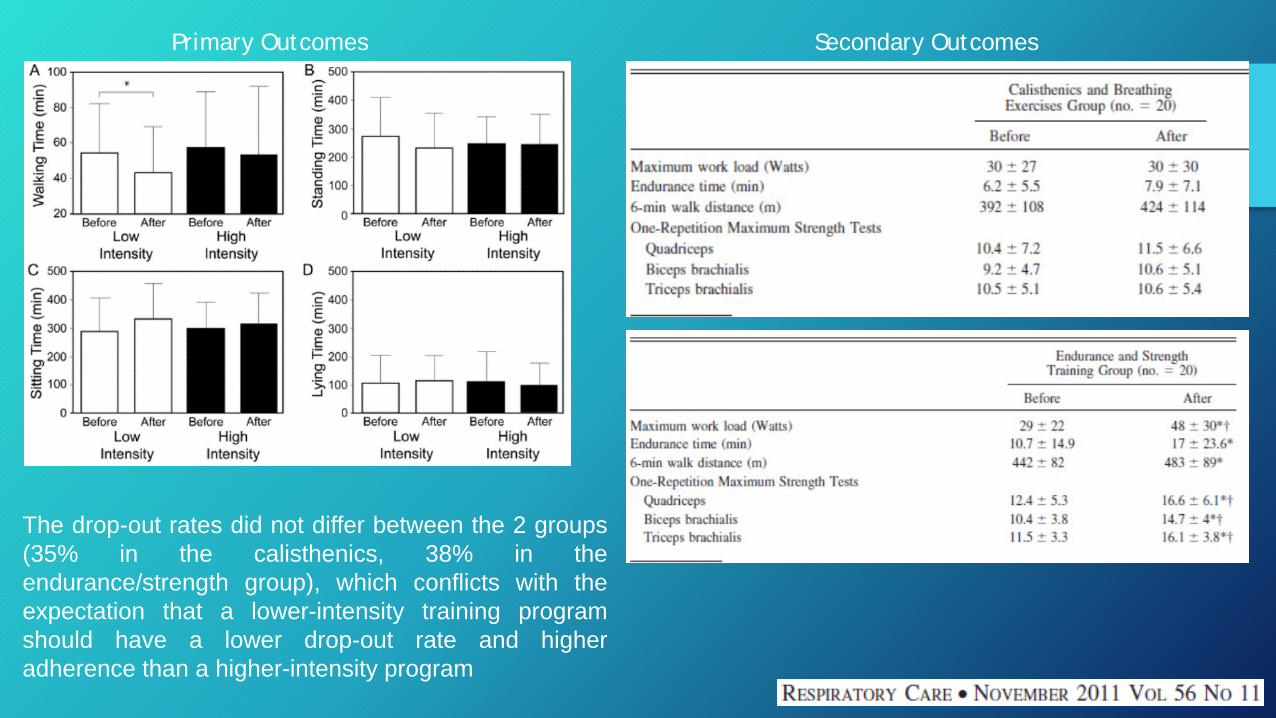
Primary Outcomes Secondary Outcomes
The drop-out rates did not differ between the 2 groups (35% in the calisthenics, 38% in the endurance/strength group), which conflicts with the expectation that a lower-intensity training program should have a lower drop-out rate and higher adherence than a higher-intensity program


L’utilizzo del termine «esercizi callistenici» andrebbe ridimensionato perché:
• Esiste una variabilità dei contenuti che non permette di utilizzare il termine in maniera chiara ed univoca
• Il termine «esercizi callistenici» è stato gradualmente sostituto
con termini più specifici quali esercizi di endurance, di forza, di stretching
• In letteratura le evidenze di efficacia per i callistenici sono molto
deboli (per non dire nulle)

Precoce mobilizzazione in TI

• Il progresso della medicina intensivistica ha portato ad un significativo aumento della sopravvivenza del paziente critico
• Migliore sopravvivenza spesso significa aumento della degenza in Terapia Intensiva
• L’aumento della degenza in Terapia Intensiva spesso implica un incremento del rischio di complicanze associate alle cure intensive e all’allettamento
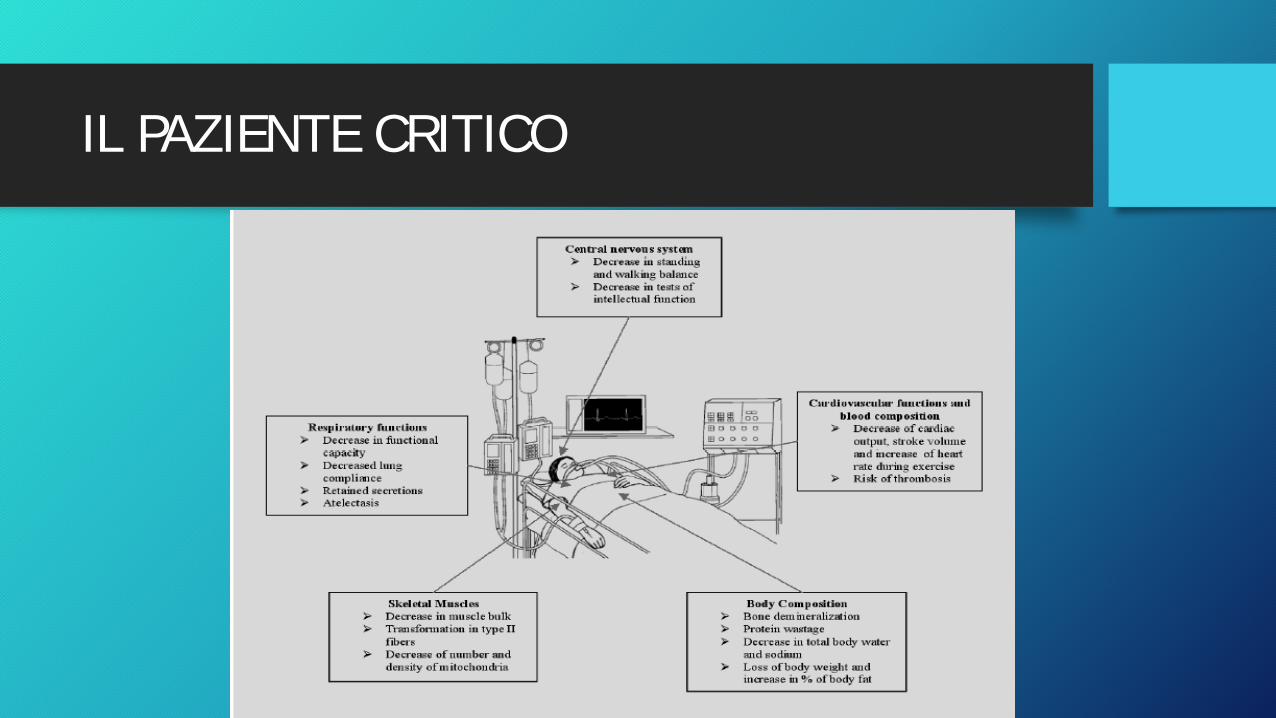
IL PAZIENTE CRITICO

IL PAZIENTE CRITICO

Lasciamolo tranquillo, quando starà meglio inizieremo a trattarlo……………..

• 49%: è ritornato al lavoro • 100%: riferisce limitazioni funzionali, debolezza e fatica muscolare • 7%: neuropatie da intrappolamento • 5%: ossificazione ectopica • 4%: contratture alle dita e spalla congelata • 7%: problemi nella zona della tracheotomia
Herridge et al. N. Engl. J. Med. 348:683-693, 2003
PROBLEMI CLINICI (ad 1 anno)


La mobilizzazione precoce
Migliora la capacità funzionale del paziente
Bailey et al., 2009; Morris et al., 2008; Needham et al.,2010
Riduce la durata del ricovero in TI fino a 3 giorni
Morris et al., 2008; Needham et al., 2010
Riduce l’incidenza del delirio Needham et al., 2010; Schweickert et al., 2009
Migliora l’autonomia del paziente Needham et al., 2010; Schweickert et al., 2009

Che cosa volete farmi?? Non vorrete mica muovermi? Non vedete come sono ridotto?

INSTABILE, ALLETTATO, POCO COLLABORANTE
STABILE, COLLABORANTE
• RIALLENAMENTO
• DEAMBULAZIONE • ESERCIZI CONTRO RESISTENZA • MOBILIZZAZIONI ATTIVE
• ELETTROSTIMOLAZIONE • POSTURE MOBILIZZAZIONI PASSIVE

MOBILIZZAZIONE PASSIVA
Il 99% dei fisioterapisti la utilizza per: Valutazione, Prevenzione, Mantenimento e Ripristino
C’è una debole evidenza sull’efficacia della mobilizzazione passiva (MP) sul paziente critico (e non solo). Gli unici lavori che supportano l’evidenza della MP hanno trattato i pazienti mediante sedute giornaliere prolungate (9 h/die) e con apparecchiature.
? ? ?

La precoce mobilizzazione del paziente critico è pericolosa?

593 701
1550
100
200
300
400
500
600
700
800
ET tubo Non intubati
Tracheo
0,96 % effetti avversi
Num
ero
at
tivi
tà
1449 attività (233 seduto sul letto, 454 seduto sulla sedia, 762 Deambulazione)

0,6% di eventi avversi

La mobilizzazione precoce viene utilizzata comunemente nel paziente critico?
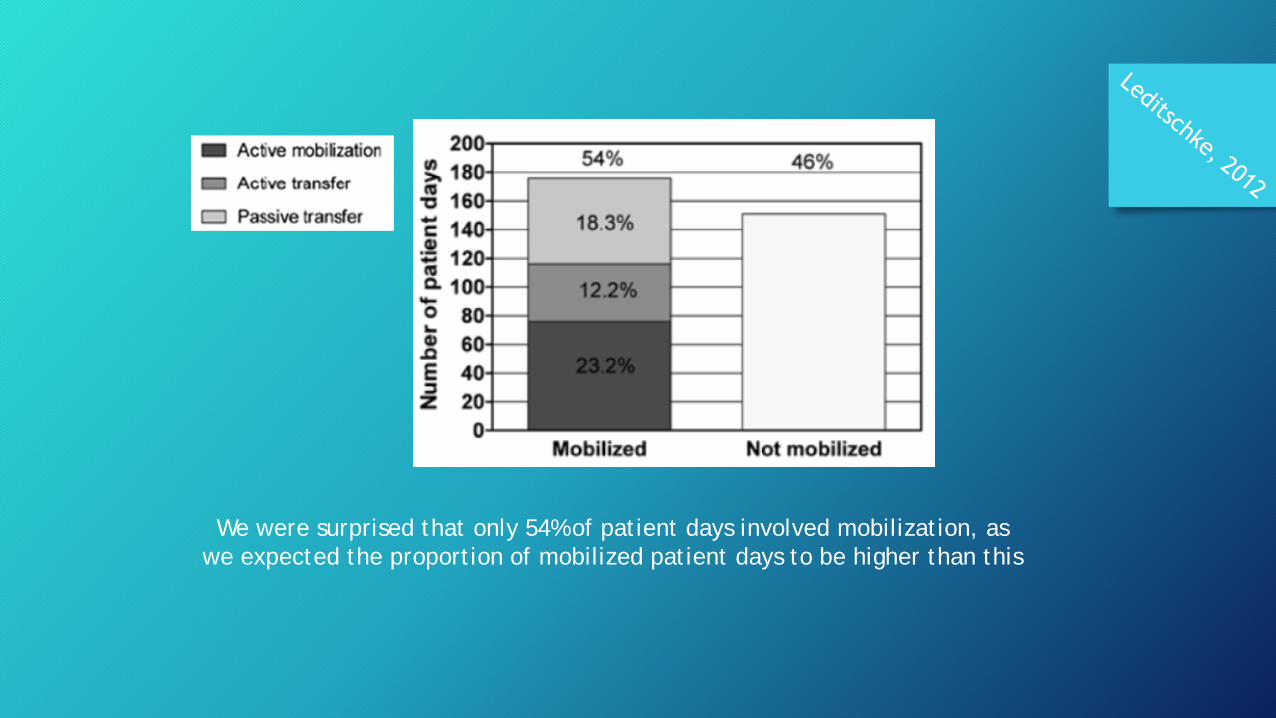
We were surprised that only 54% of patient days involved mobilization, as we expected the proportion of mobilized patient days to be higher than this

Critical Care Medicine May 2014 • Volume 42 • Number 5

Ostacoli alla mobilizzazione precoce

MEDICO INFERMIERE FISIOTERAPISTA
Risolvere gli ostacoli
• Lavoro in team (es. mobility team, ma anche solo maggior
collaborazione tra le figure)
• Utilizzo di protocolli di mobilizzazione (valutazione e monitoraggio
pre mobilizzazione, durante mobilizzazione e post mobilizzazione)
• Ottimizzazione delle risorse

3 operatori per 1 paziente
FT FT
IP
FT
1 operatore per 18 pazienti
MOBILIZZAZIONE PRECOCE ESERCIZI CALLISTENICI





























