Embed Size (px)
Citation preview

MIGRAINE: PAST, CURRENT AND FUTUREKevin M Kapadia, MD
Meriter Medical Group Neurology
Madison, WI

Objectives
Headache Disorders comprise a large portion of inpatient and outpatient primary care, pain medicine, and neurologic care, of which migraine headache disorders are one of the most common.
• To review the epidemiology, theoretical pathophysiology and broad clinical presentation of migraine
• To review the current evidence-based treatment therapies for migraine prevention and abortive therapies
• To become familiar with new targeted therapies being trialed for migraine

Epidemiology of Migraine• Most common form of disabling headache for patients
seeking medical treatment.
• >38 million people (between 10% - 15% of US population)
• Onset ages 10 - 45, most commonly recurring during ages 15 - 55.
• Yet…Underdiagnosed and Undertreated: • American Migraine Prevalence and Prevention Study:
• ½ of severe migraineurs based on questionnaire never had a formal diagnosis
• Only 12% were on dedicated preventive management

Acquiring Migraines• Lifetime Prevalence
• 43% in women• 18% in men
• Childhood migraines 4-5%; equal in boys and girls• By Puberty women twice as likely to develop migraines
• Estrogen increases Nitric Oxide (NO) Synthase activity
• Polygenic Inheritance• Rare Autosomal Dominant monogenic forms
• Head Trauma

Societal Cost of Migraine Headache
• Direct costs (prescriptions, outpatient expenses, ED and inpatient care) ~$11 billion/year
• Indirect costs (missed work days) >$12 billion/year
• Annual loss of 160 million workdays

Prototypical Case: ‘Julie’40 yo F episodic migraines for 20 years.
Typical Headache: visual aura of flashing lights followed by unilateral left sided headache, photosensitivity, and nausea.
• Headaches became more frequent in her 30's. • Takes OTC medications Tylenol and ibuprofen now to the
point of 8-12 pills per day. • She reports having a headache starting last Christmas Eve
that lasted for 1 full month.
• On continuous birth control given that she has worsening headaches around the time of her menses.

Defining Migraine• Derived from Greek ‘hemi’ and ‘kranion’
• (though up to 40% are bilateral)
• Recurrent primary headache disorder commonly associated with sensory symptoms (photophobia, phonophobia, osmophobia, nausea, vomiting, disability) with aura (20%) or without aura.
• Episodic (<15 headache days per month)• Chronic (>15 headache days per month)

Migraines of the Past
• 9,000 years ago (cave drawings) to 17th century Europe: trepanation of skulls to release ‘evil spirits’ to escape.
• 400 BC: Hippocrates: described visual auras and relief after vomiting ‘to release bad vapors’
• 2nd Century AD: Aretaeus of Cappadocia ‘discoverer of migraines’ described symptoms of unilateral headache associated with vomiting and headache-free intervals between attacks
• Hua T’o: Chinese surgeon Han Dynasty: acupuncture to treat recurrent migraines of King

More Headache History• Middle Ages: unorthodox treatments:
• Hot irons• Blood Letting• Insertion of Garlic into an incision• Witchcraft• Opium and vinegar solutions to skull for ‘directed pain relief’
• 800’s: Persian physician recognized hormonal role of migraines in women
• Islamic scientist of 900’s recognized the irritation of light and sound in patients
• 1712: London published Headache 5 major types; including ‘megrim’: classic migraine with aura.
Primary Headaches:International Classification of Headache Disorders (ICHD-II/III)
• Migraine: • Migraine w/o aura and Migraine w/ aura• Hemiplegic Migraine• Basilar-Type Migraine • Menstrual Migraine• Chronic Migraine
• Non-Migrainous Primary Headache Disorders:• Tension-type• Trigeminal Autonomic Cephalgias• Primary Stabbing Headache• Hypnic Headache (alarm clock headache)• Nummular Headache

Laying Down the Blueprints• 1938: Graham and Wolff: ergotamines effective for
stopping migraine• 1948: The Wolff’s Headache ‘Headache Bible’ 1st Edition
published:
‘Headache may be equally intense, whether its implications are malignant or benign, and though there are few instances in human experience where so much pain may mean so little in terms of tissue injury, failure to separate the ominous from the trivial may cost life or create paralyzing fear.’

Vascular Pathophysiology Dogma• 1938 Graham and Wolff:
• Headache pain reduced coinciding with reduced amplitude of arterial pulsations due to IV ergotamine treatments.
Vascular Theory:• Humoral mediated intracerebral arterial vasoconstriction causing aura
followed by extracerebral vasodilation causing headache.

Cortical Spreading Depression• 1938 Leao: Cortical Spreading Depression (CSD); wave of
neuronal depolarization followed by suppression of neuronal activity with corresponding blood flow changes (hyperemia followed by oligemia) moving across the cerebral cortex at 3mm/min.
• Lashley documented his own visual aura moving across the occipital lobe at same speed
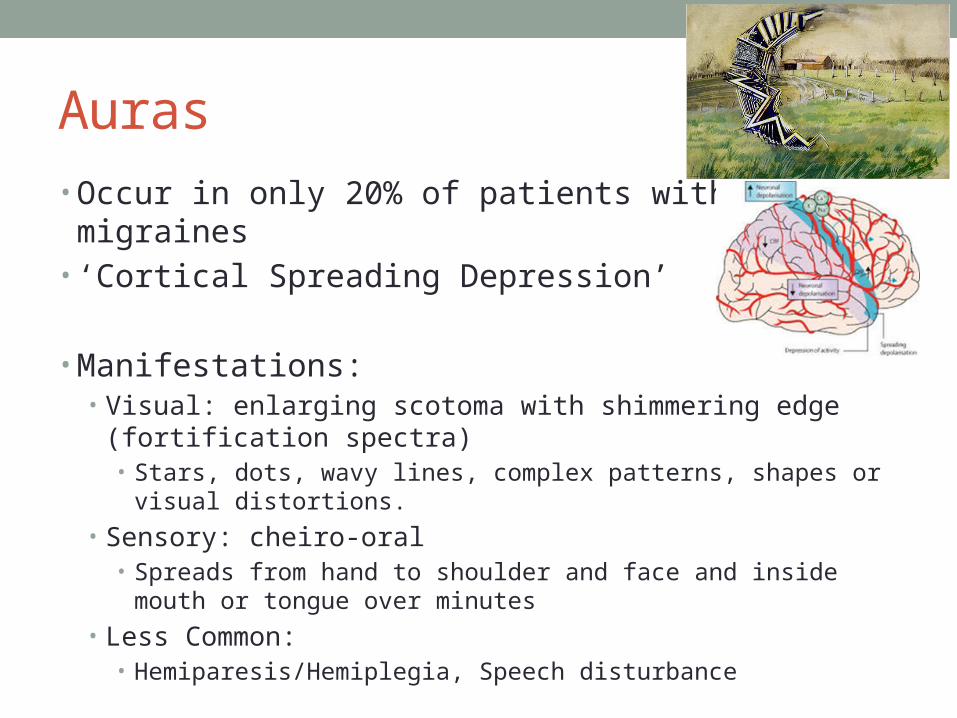
Auras• Occur in only 20% of patients with migraines• ‘Cortical Spreading Depression’
• Manifestations:• Visual: enlarging scotoma with shimmering edge (fortification
spectra)• Stars, dots, wavy lines, complex patterns, shapes or visual distortions.
• Sensory: cheiro-oral • Spreads from hand to shoulder and face and inside mouth or tongue
over minutes
• Less Common:• Hemiparesis/Hemiplegia, Speech disturbance

Migraine and White Matter Lesions• Increased prevalence of ‘silent brain lesions’: cerebral
white matter hyperintense lesions in migraine patients; pooled increased risk of 3.9 (95% CI 2.3–6.7).
• Recent systematic review and meta-analysis showed an increased risk for lesions in Migraine with Aura (OR = 1.68; 95% CI 1.07–2.65), no association found for migraine without aura.
Incidental white matter lesions
Guidetti,D et al. Front Neurol. 2014.

Rare Complication of Migraine
Migrainous Infarction:• Mostly occurs in the posterior circulation, in younger
women with a history of migraine with aura.
• Large clinical series reported prevalence of migrainous infarction varies between 0.5 and 1.5% of all ischemic strokes, ranging up to 10–14% of ischemic strokes in young patients
Guidetti,D et al. Front Neurol. 2014.

Migraine and Stroke Risk: 9 Study Review
• Relative risk (RR) for ischemic stroke with any type of migraine: 1.73 (95% CI 1.31-2.29).
• Increased risk migraine with aura (RR 2.16, 95% CI 1.53-3.03).
• In contrast, increased risk migraine without aura was not statistically significant (RR 1.23, 95% CI 0.90-1.69).
• Risk of ischemic stroke was significantly increased for certain subgroups:• Women with migraine (RR 2.08, 95% CI 1.13-3.84) but not men (RR
1.37, 95% CI 0.89-2.11)• Subjects with migraine <45 years of age (RR 2.65, 95% CI 1.41-4.97)• Smokers who had migraine with aura (RR 9, 95% CI 4.2-19.3)• Women currently using oral contraceptives who had migraine with aura
(RR 7, 95% CI 1.5-32.7)

Case: Migraines and Stroke Risk• ‘Julie’ has migraines with aura.
• What is her risk for stroke?• Oral Contraceptives, women with aura: RR 7.
• Recommendations for smoking cessation, avoid OCPs in women with migraine with aura.
• Use of Triptans?• Contraindicated in patients with Cardiovascular Disease, Hemiplegic
Migraine, Basilar Migraine due to theoretical increased risk of stroke.• Also relative contraindication in pre-menopausal women with migraine
with aura.

Anatomy of Headache PainBrain itself does not feel pain.
Dura Mater, Meninges and Blood vessels carry pain fibers to the cranial nerves, specifically CN V (Trigeminal Nerve).

Migraine Cascade• Trigeminal Reflex is activated:
• Trigeminal neurons supplying the dural vessels release calcitonin gene-related peptide (CGRP), substance P, neurokinin A.• Vessels dilate and become inflamed, plasma
protein extravasation occurs (sterile neurogenic inflammation)
• Result is peripheral sensitization of the first-order neuron innervating the dural blood vessels (explaining the pounding pain)
• With prolonged duration: second and third-order neurons become activated, resulting in central sensitization.

Therapeutic Goal: Avoid Central Sensitization
• Central Sensitization occurs and abortives like triptans are much less likely to be effective.
• Treating the headache early prevents central sensitization
• May also be seen more frequently in chronic migraine than episodic migraine.

Anatomy of Headache Pain• Pain from face and head can be
referred to the neck and vice versa.
• Ipsilateral Greater Occipital Nerve formed by C2 often is tender during an attack of migraine. • Neural Blockade (occipital nerve
block) may terminate an attack.
• Periaqueductal Gray, Locus Ceruleus in the midbrain connects with TNC to inhibit pathways (target of some medications)

Migraines and Hormones• Menstrual migraines, increased headache frequency in
peri-menopausal women
• 25 year old F with migraines around her menstrual cycle. Infrequent migraines the rest of the month
• What medications to trial?• Hormonal therapy (if migraines without aura)• Long-Acting Triptan• Daily Preventive

Ideal Migraine Acute TreatmentGoal: functional headache-free state in 2 hours with no recurrence in 24 hours.• No more than 2-3 times per week to avoid medication overuse• Non-oral formulas should be made available if nausea is severe
High-quality evidence from placebo-controlled randomized trials:
• NSAIDs: aspirin, ibuprofen, naproxen, and diclofenac
• Triptans: sumatriptan
• Combination: sumatriptan and naproxen
• Antiemetic/dopamine receptor antagonists: chlorpromazine, prochlorperazine, and metoclopramide
Treating the Headache Early
Early treatment reduces overall burden of migraine
Challenges: • Prodromal symptoms prior to headache:
• Mood change, fatigue, muscle tension, yawning, cognitive dysfunction
• 50% of patients will delay treatment in order to see if presentation really represented migraine
• Some avoid medication unless headache is severe• Some with frequent attacks limit acute medication for fear
of overuse
Hu et al.

Triptans• Short-acting: sumatriptan (Imitrex), rizatriptan (Maxalt),
eletriptan (Relpax), almotriptan (Axert), zolmitriptan (Zomig),
• Long-acting: naratriptan (Amerge), and frovatriptan (Frova)
• Discovered in the 1990’s• 5-HT1B, 5-HT1D Receptor agonist• Mechanism of action in migraine unclear
• Vasconstrictor but also inhibits neurogenic inflammation peripherally• Prevents Central Sensitization
• Contraindicated in patients with CAD

Dihydroergotamine (DHE)• Nasal Spray: 1 puff (0.5mg) each nostril repeat in 15
minutes, 2 mg max daily dose
• Injectable: (0.5mg to 1mg) repeat in 1 hour, max of 3mg daily
• Inpatient Raskin Protocol (IV DHE + antiemetic) repeatedly for status migranosis.

Acute Medications to Avoid• Fiorinal (Fioricet): Contains Butalbital (notorious for
rebound headaches)
• Opioids for migraine (Majority of Neurologists do not prescribe narcotics) Ideal limitation is maximum of 2 days per week

Medication Overuse Headaches
Regular overuse for more than >3 months of one or more drugs that can be taken for symptomatic treatment of headache:
• ≥10 days per month for >3 months: ergotamines, triptans, opioids
• ≥15 days per month for >3 months, of simple analgesics (ie, acetaminophen, aspirin, or NSAID)

Medication Overuse Headaches: Culprits

Migraine Prevention• Theories of mechanism of action:
• Enhancement of anti-nociceptive pathways• Inhibition of central and peripheral sensitization• Inhibition of cortical spreading depression
• Goals: reduce attack frequency and severity, reduce associated disability
• Only 12% of patients taking migraine preventive therapy where up to 40% may be indicated

Evidence-based Medications:
B-Blockers: Metoprolol, propranolol, and timolol
Anti-depressants: Amitriptyline and venlafaxine
Anti-epileptics: Valproate and topiramate
Herbals: Butterbur
Alternatives include calcium channel blockers including verapamil and flunarizine

Starting Preventive Therapy• Start low and build slowly (make adjustments every 2 weeks)
• Adequate trial duration 2-3 months
• Headache calendar or diary
• Consider tapering of medication after 6 months is feasible

Anti-Epileptic Drugs• Valproate: effective
• Contraindicated in pregnancy, nausea, weight gain, alopecia, transaminitis, pancreatitis, agranulocytosis
• Topiramate: effective• Titrate slowly from 15-25mg daily up to 100-200mg daily• Paresthesias, change in taste, cognitive side effects, category D in
pregnancy
• Gabapentin: efficacy unclear• Generally well-tolerated but somnolence is common

Anti-Hypertensives
First Line: • B-Blockers: Propranolol and Timolol are FDA approved
Second Line:• Calcium Channel Antagonists: Verapamil: may be
indicated for those with prolonged aura or vestibular migraine
• ACE inhibitors and ARBs: Lisinopril, Candesartan

Anti-Depressants• Tricyclic Antidepressants (amitriptyline)
• Effective at low doses 10-25mg• Blocks neuronal uptake of both serotonin and norepinephrine;
resulting in anti-nociceptive effects• Helpful in sleep disruption

Multi-Disciplinary Treatments• Psychological Approaches:
• Acceptance and Commitment Therapy• Cognitive-Behavioral Therapy• Biofeedback techniques
• Exercise:• 40 minutes, 3 times weekly of aerobic exercise as effective as relaxation
techniques and topiramate
• Neck Pain/Cervicogenic Headaches: • Isometric neck exercises effective treatment of cervicogenic migraines
(strengthens neck muscles thus less likely to spasm)• Improvement after 2 weeks of diligent exercise
• Acupuncture: Benefit exceeds placebo (widely practiced and studied in Germany)
Neurology Continuum, Vol 18 No. 4, 2012

Supplements• Magnesium oral supplementation (magnesium oxide
400mg daily) or IV infusion 1g
• CoEnzymeQ10 300mg daily
• Riboflavin (Vitamin B2) 400mg daily
• Butterbur (plant derivative) 75mg twice daily
• Feverfew (plant extract) products in US may not have same quality or consistency

Nonpharmacologic Migraine Prevention
Adequate Hydration
Adequate Restorative Sleep
Managing Stress, Anxiety, Depression
Avoidance of Known Triggers
Aerobic exercise
Biofeedback
Other forms of relaxation training
Cognitive-behavioral therapies
Acupuncture
Transcutaneous electrical nerve stimulation (TENS)

Dietary Changes• Caffeine: helpful or harmful
2-3 cups of coffee can trigger withdrawal headaches
• Gluten Sensitivity/Celiac Disease association
• Skipping Meals
• Tyramine-rich foods (wines and cheeses)

Common Migraine Headache Triggers
• Caffeine withdrawal• Alcohol (red wine)• Changes in sleep patterns• Bright lights, loud noises, strong odors or perfumes• Exercise or other physical stress or anxiety• Missed meals• Smoking or exposure to cigarette smoke• Weather changes• Foods that contain MSG (monosodium glutamate)• Meats with nitrates and nitrites (bacon, hot dogs, salami, cured meats)• Foods with tyramine, such as aged cheeses, soy products, fava beans, hard
sausages, smoked fish, and red wine• Baked goods, chocolate, nuts, peanut butter, and dairy products• Aspartame (NutraSweet, Equal)• Fruits (avocado, banana, citrus fruit, figs)• Gluten Sensitivity/Celiac Disease• Hormonal changes during the menstrual cycle

Case: ‘Julie’ and Preventives
Past Preventive Medications:
Topiramate: felt 'dopey' memory and balance issues. Effective for migraine at higher doses but side effects were too much.
Amitriptyline (failed)
Propranolol (gave her headaches)
Magnesium caused GI effects

Chronic Migraine
15 headache days per month for >3 months with migraine headaches >7 days per month
3% Annual Risk of transformation from episodic migraine to chronic migraine
Comorbid Disorders:63% with chronic fatigue syndrome36% with fibromyalgia57% with major depression

Chronic Migraine• Very Poor Acute Migraine Treatment has a >2 fold risk of
new-onset Chronic Migraine after 1 year.
• PREEMPT2 Trial: OnobotulinumtoxinA (Botox) for Chronic Migraine• large mean decrease in frequency of headache days over placebo
at 24 weeks (-8.4 vs -6.6; P < .001) and at all other time points.
• Botox for Chronic Migraine FDA Approved
Lipton, RB et al. Neurology 2015
Dodick, DW et al. Headache 2010

Mechanism of Botox for Chronic Migraine
Aside from reducing wrinkles
(neuromuscular junction blockade)…
Decreases nociceptor pathways:• C and A delta fibers• Mechano- and chemo-nociceptors• Substance P• Calcitonin Gene Related Peptide (CGRP)• Glutamate Release
BoTox for Migraines 2013 Moulton-Barrett, R.

Case ‘Julie’• Initiated on Botox therapy. Responded well, with reduced
headache frequency.
• 4 treatments so far and reports 5 headache days per month on average. Her headaches typically last 1-2 days. She takes rizatriptan (Maxalt) as an abortive.

©2013 American Academy of Neurology. Published by LWW_American Academy of Neurology. 2
Migraine prevention with a supraorbital transcutaneous stimulator: A randomized controlled trial.Schoenen, Jean; MD, PhD; Vandersmissen, Bart; Jeangette, Sandrine; Herroelen, Luc; Vandenheede, Michel; Gerard, Pascale; Magis, Delphine; MD, PhD
Neurology. 80(8):697-704, February 19, 2013.DOI: 10.1212/WNL.0b013e3182825055
The stimulation electrode placed on the forehead covers the supratrochlear and supraorbital nervesFigure 1. Reproduced with permission from STX-Med.
The FUTURE

CEFALY: Transcutaneous Supraorbital Neurostimulation (tSNS)
• Cefaly Device: FDA Approved 2014• ‘first transcutaneous electrical nerve stimulation (TENS) device specifically
authorized for use prior to the onset of pain’
• tSNS external self adhesive electrode placed on the forehead Cefaly® device Belgium
• Bipolar electrode covers origins of the supraorbital nerves (branches of 1st trigeminal division)
• PREMICE Trial:• At least once daily 20 minutes for 3 months
Schoenen, J et al. Neurology 2013

©2013 American Academy of Neurology. Published by LWW_American Academy of Neurology. 2
Migraine prevention with a supraorbital transcutaneous stimulator: A randomized controlled trial.Schoenen, Jean; MD, PhD; Vandersmissen, Bart; Jeangette, Sandrine; Herroelen, Luc; Vandenheede, Michel; Gerard, Pascale; Magis, Delphine; MD, PhD
Neurology. 80(8):697-704, February 19, 2013.DOI: 10.1212/WNL.0b013e3182825055
Study outcomesFigure 3. (A) Decrease in number of migraine days over the trial duration compared to run-in in verum and sham groups. (B) Percentage decrease at end of trial compared to run-in for the various outcome measures in verum and sham groups.

Mechanism of Migraine: Understanding through Genetics• Primary Migraine pathology: state of hyper-responsiveness• Genetic discoveries step to understanding migraine• Initially considered a cerebrovascular condition, then a
neuro-inflammatory process, and now primarily a neurogenic disorder.
• Genetic findings revealed ion channels and transporter mutations, powerful argument for the neurogenic basis of migraine.
• Modulations of ion channels leading to amelioration of the migraine “hyper-responsive” brain targets for drug research
Weir and Cader (2011)

Migraine Genetics: Polygenic
Studying of rare monogenic causes:• Familial Hemiplegic Migraine (FHM) (multiple rare genotypes)
• FHM1: Increased Ca2+ influx into presynaptic terminals, increase of glutamate
• FHM2: Mutation Na+/K+ ATPase decreased clearance of synaptic glutamate
• FHM3: Mutation voltage-gated Na+ channels, increased glutamate
Low Brain Magnesium Levels (inhibitory ion for Calcium channels that inhibit CSD)
All result in hyperexcitable brain

Migraine-Associated Genetics
Recently Identified:• LRP1 Locus: cell surface receptor for neurons and vasculature:
vascular smooth muscle• TRPM8 Locus: associated with both migraine w/ and w/o aura.
Also cutaneous allodynia, skin hypersensitivity• MTDH gene: migraine with aura only• MEF2D Locus: survival of newly formed neurons. Dysregulation in
migraine by this transcription factor may cause hyperexcitability (also associated with epilepsy)
• TGFBR2 Locus: transforming growth factor beta receptor 2; cell proliferation and differentiation and extracellular matrix. Familial aortic dissection. May explain two fold risk increase for cervical artery dissection in migraine.
Freilinger et al, 2012.

Investigative Acute Agents
CGRP receptor antagonists • Randomized Phase III trials CGRP receptor antagonists
telcagepant and olcegepant beneficial for acute migraine • Telcagepant stopped due to hepatotoxicity• Olcegepant stopped due to poor oral bioavailability.
Selective Serotonin 1F receptor agonist• Lasmiditan lacks vasoconstrictor activity, effective in
randomized placebo-controlled trial • high rate of serious adverse events, particularly at higher doses;
the most common were dizziness, fatigue, vertigo, paresthesia, and somnolence.
• Ongoing studies to determine lasmiditan tolerability
Alternative Non-Pharmacologic Investigation: Transcranial Magnetic Stimulation (TMS)
• Efficacy of transcranial magnetic stimulation (TMS) demonstrated in randomized controlled trial
• 164 patients at least one attack of migraine treated during aura
• Pain free at 2 hours post-treatment greater with TMS compared with sham (39% vs 22%, absolute risk reduction 17%)
• Sustained pain-free response at 24 and 48 hours• No serious adverse events

Debated Invasive Procedures
PFO Closure • PFO: 25% general population, 50% of patients with migraine with
aura.• Theory that right to left shunt may circumvent the filtering function of
lung and allow microemboli or other neurotransmitters to affect the intracranial blood vessels, triggering migraine attacks.
• Recent trial with PFO Closure in migraine with aura patients showed no benefit.
Migraine Decompression Surgery
Neurologists Don't Buy 'Facelift Treatment' for Migraine Pauline Anderson July 05, 2013
• "Let's face it: migraine is a very complex disease of the brain; how could surgery affect the epigenetics of 22 different genes?"
• “Biological plausibility" and "experimental evidence" are "totally absent" in the studies of the procedure.

Take Away Points• Be MINDFUL: Cost and Morbidity
• Be WATCHFUL: Underdiagnosed, undertreated: good to ask during ROS (especially men)
• Be PROACTIVE: Failing to treat early increases risk for evolution to chronic migraine
• Be CAUTIOUS: Medication overuse headaches
• Be RESOURCEFUL: Multidisciplinary approach to headache treatment: medical and psycho-social aspects

Thank You!





























