-
8/12/2019 microvascular dysfunction in RA.docx
1/14
1
CHAPTER 1
INTRODUCTION
Patients with Rheumatoid Arthritis (RA) have a reduced life
expectancy which is
predominantly due to cardiovascular disease (CVD).(1,2) The
reason for this excess risk is not
clear. Evidence supporting an increased prevalence of
hypertension and dyslipidaemia in RA
is now available, but when adjustment is made for these risk
factors, the risk ratio is only
minimally attenuated , suggesting that mechanisms other than the
conventional vascular risk
factors may contribute to this excess CV risk.
Recently, similarities have been found between the inflammatory
process seen in RA
and atherosclerosis. These features include raised plasma levels
of TNF-_, IL-6,
concentrations of CRP and local expression of adhesion
molecules. It is now recognized that
the inflammatory process is a major contributor to the
pathological processes seen in CVD,
and may play an aetiopathogenic role. It seems likely therefore
that the deleterious effect to
the CV system in RA could be mediated by the inflammation
associated with the disease
itself, a process we already know is involved in
atherogenesis.
The vascular endothelium plays an essential role in maintaining
blood vessel health
by releasing a variety of vasoactive substances and mediators of
inflammation and
coagulation. When the endothelial function is impaired, there is
an imbalance in these
substances resulting in a vasoconstrictor, pro-inflammatory and
pro-coagulant endothelium
that may lead to both thrombosis and atherosclerotic disease.
Changes in endothelial function
occur early in the development of CVD and are found in
asymptomatic subjects with CV risk
factors. In RA, impaired endothelial function has been observed
in the macrocirculation, butless is known about microvascular
function. The microvasculature is an important vascular
bed to study as it is affected early in the development of
endothelialdysfunction and
abnormalities here have been shown to correlate with CV risk
factors and established
coronary artery disease. (3,4)
.
-
8/12/2019 microvascular dysfunction in RA.docx
2/14
2
CHAPTER II
RHEUMATOID ARTHRITIS
1. DefinitionRheumatoid arthritis (RA) is an autoimmune disease
that causes chronic
inflammation of the joints. While inflammation of the tissue
around the joints and
inflammatory arthritis are characteristic features of rheumatoid
arthritis, the disease
can also cause inflammation and injury in other organs in the
body. Autoimmune
diseases are illnesses that occur when the body's tissues are
mistakenly attacked by
their own immune system. The immune system contains a complex
organization of
cells and antibodies designed normally to "seek and destroy"
invaders of the body,
particularly infections. Patients with autoimmune diseases have
antibodies in their
blood that target their own body tissues, where they can be
associated with
inflammation. Because it can affect multiple other organs of the
body, rheumatoid
arthritis is referred to as a systemic illness and is sometimes
called rheumatoid
disease.(8)
2. Epidemiology Prevalence varies from 0,5% to 1,5% ofthe
population RA affects more woman than man ( ratio 3:1) The age of
onset is between 3055 years
3. EtiologyGenetic susceptibility:
HLA DR4 with Rheumatoid Arthritis, type I diabetes HLA DR2 with
lupus
Environmental Factors:
Infections Overexposure to pesticides and toxins Stress
4. Pathophysiology(6)The autoimmune inflammatory process in RA
involves a complex cascade of
cells, including T cells, B cells, macrophages, mast cells, and
fibroblasts, that
infiltrate the synovial tissues. Macrophage activation occurs,
stimulating the release ofproinflammatory cytokines such as
interleukin-1 (IL-1), IL-6, IL-8, IL-12, IL-16, IL-
-
8/12/2019 microvascular dysfunction in RA.docx
3/14
3
18, IL-32, and tumor necrosis factor-alpha (TNF-alpha). These
cytokines stimulate
synovial fibroblasts and chondrocytes in the nearby articular
cartilage to secrete
enzymes that degrade proteoglycans and collagen, leading to
tissue destruction. This
results in inflammation of the synovial membrane, increased
vascularity, hyperplasia
of the synovial cells, joint effusion, and the growth of a
fibrovascular granulation
tissue called "pannus" which infiltrates contiguous bone and
cartilage. Bone erosion
and degradation of the cartilage matrix ensue, due to the
activation of osteoclasts and
invasion of aggressive synoviocytes, cytokine-activated
chondrocytes, and neutrophils
Picture 1 : patophysiology of rheumatoid arthritis
5. Sign and symptoms(7)
-
8/12/2019 microvascular dysfunction in RA.docx
4/14
4
Rheumatoid arthritis is a long-term disease - a chronic disease.
Symptoms can
come and go and each patient is affected differently. While some
patents may have
long periods of remission, when the rheumatoid arthritis is
inactive and few or no
symptoms are felt, others may have virtually constant symptoms
for long periods.
Classic features:
Joint pain, typically symmetric Morning joint stiffness ( 1
hour) Joint swelling Constitutional symptoms (fever, fatigue,
weight loss, etc.)
Although the joints are almost always the principal focus of RA,
other organ
systems may also be involved. Extra-articular manifestations of
RA occur most often
in seropositive patients with more severe joint disease.
Extra-articular manifestations
can develop even in disease when there is little active joint
involvement.
Extraarticular manifestation :
Rhematoid noduleThe subcutaneous nodule is the most
characteristic extra-articular lesion of the
disease. Nodules occur in 20 to 30% of cases, almost exclusively
in
seropositive patients. They are located most commonly on the
extensor
surfaces of the arms and elbowsbut are also prone to develop at
pressure
points on the feet and knees. Rarely, nodules may arise in
visceral organs,
such as the lungs, the heart, or the sclera of the eye.
Cardiopulmonary Disease.There are several pulmonary
manifestations of rheumatoid arthritis, including
pleurisy with or without effusion, intrapulmonary nodules, and
diffuse
interstitial fibrosis. On pulmonary function testing, there
commonly is arestrictive ventilatory defect with reduced lung
volumes and a decreased
diffusing capacity for carbon monoxide. Although mostly
asymptomatic, of
greatest concern is distinguishing these manifestations from
infection and
tumor. Atherosclerosis is the most common cardiovascular
manifestation in
rheumatoid arthritis. It is also the leading cause of death in
the RA patient.
Because chronic inflammation may be the cause of
atherosclerosis, it is
possible that early aggressive treatment of RA may reduce the
incidence or
severity of heart disease. Pericarditis also seen with RA.
-
8/12/2019 microvascular dysfunction in RA.docx
5/14
5
Eye Disease.Keratoconjunctivitis of Sjogrens syndrome is the
most common ocular
manifestation of rheumatoid arthritis. Sicca (dry eyes) is a
common
complaint. Episcleritis occurs occasionally and is manifested by
mild pain and
intense redness of the affected eye. Scleritis and corneal
ulcerations are rare
but more serious problems.
Sjogrens Syndrome.Approximately 10 to 15% of patients with
rheumatoid arthritis
develop Sjogrens syndrome. Sjogrens syndrome is an autoimmune
condition
that affects exocrine gland function, leading to a reduction in
tear production
(keratoconjunctivitis sicca), oral dryness (xerostomia) with
decreased saliva of
poor quality, and reduced vaginal secretions.
Rheumatoid Vasculitis. Neurologic Disease.
The most common neurologic manifestation of rheumatoid arthritis
is a mild,
primarily sensory peripheral neuropathy, usually more marked in
the lower
extremities. Entrapment neuropathies (e.g., carpal tunnel
syndrome and tarsal
tunnel syndrome) sometimes occur in patients with rheumatoid
arthritis
because of compression of a peripheral nerve by inflamed
edematous tissue.
6. Diagnosis
-
8/12/2019 microvascular dysfunction in RA.docx
6/14
6
CHAPTER III
CREACTIVE PROTEIN (CRP) & NITRIT OXIDE (NO)
1. CReactive Protein (CRP)a) Definition
CRP is a protein that produced in the liver as respon from
inflammatory
cytokines, but based on recent studies show that CRP can also be
produced by
extrahepatic tissues such as adipose cells and vascular smooth
muscle cells.
b) Function(5)The acute phase response develops in a wide range
of acute and chronic
inflammatory conditions like bacterial, viral, or fungal
infections; rheumatic and other
inflammatory diseases; malignancy; and tissue injury or
necrosis. These conditions
cause release of interleukin-6 and other cytokines that trigger
the synthesis of CRP
and fibrinogen by the liver. During the acute phase response,
levels of CRP rapidly
increase within 2 hours of acute insult, reaching a peak at 48
hours. With resolution of
the acute phase response, CRP declines with a relatively short
half-life of 18 hours.
Measuring CRP level is a screen for infectious and inflammatory
diseases. Rapid,
marked increases in CRP occur with inflammation, infection,
trauma and tissue
necrosis, malignancies, and autoimmune disorders. Because there
are a large number
of disparate conditions that can increase CRP production, an
elevated CRP level does
not diagnose a specific disease. An elevated CRP level can
provide support for the
presence of an inflammatory disease, such as rheumatoid
arthritis, polymyalgia
rheumatica orgiant-cell arteritis.
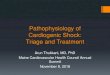
picture 2 : Stimulation and synthesis of positive
acute-phase
reactants during inflammation. Inflammation caused by
infection or tissue damage stimulates the circulating
inflammation-associated cytokines, including interleukin-1
(IL-1), interleukin-6 (IL-6), and tumor necrosis factor
(TNF)- . These cytokines stimulate hepatocytes to
increase the synthesis and release of positive acute-phase
proteins, including CRP. IL-6 is the major cytokine
stimulus for CRP production
http://en.wikipedia.org/wiki/Giant-cell_arteritishttp://en.wikipedia.org/wiki/Giant-cell_arteritis
-
8/12/2019 microvascular dysfunction in RA.docx
7/14
7
The physiological role of CRP is to bind to phosphocholine
expressed on the
surface of dead or dying cells (and some types of bacteria) in
order to activate the
complement system. CRP binds to phosphocholine on microbes and
damaged cells
and enhances phagocytosis by macrophages. Thus, CRP participates
in the clearance
of necrotic and apoptotic cells.
CRP is a member of the class of acute-phase reactants, as its
levels rise
dramatically duringinflammatoryprocesses occurring in the body.
This increment is
due to a rise in the plasma concentration ofIL-6,which is
produced predominantly
bymacrophagesas well asadipocytes.CRP binds tophosphocholine on
microbes. It
is thought to assist incomplementbinding to foreign and damaged
cells and enhances
phagocytosis by macrophages (opsonin mediated phagocytosis),
which express a
receptor for CRP. It is also believed to play another important
role ininnate
immunity,as an early defense system against infections. Serum
amyloid A is a related
acute-phase marker that responds rapidly in similar
circumstances.
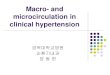
Picture 3 : Key functions of CRP within the innate
immune system include the ability to (1) recognize andbind to
phosphocholine exposed in damaged cell walls
and found in many bacteria, fungi, and parasites; (2)
act like an opsonin, marking bacteria, damaged cell
walls, and nuclear debris for phagocytosis; (3) bind to
Cl, the first component of the classical pathway of the
complement system that triggers phagocytic activity;
and (4) bind to polymorphonuclear leukocytes (PMNs)
and monocytes, which stimulate the production of
inflammatory cytokines
CRP rises up to 50,000-fold in acute inflammation, such as
infection. It rises
above normal limits within 6 hours, and peaks at 48 hours. Its
half-life is constant, and
therefore its level is mainly determined by the rate of
production (and hence the
severity of the precipitating cause).
2.
Nitric Oxide (NO)
http://en.wikipedia.org/wiki/Inflammationhttp://en.wikipedia.org/wiki/Interleukin-6http://en.wikipedia.org/wiki/Macrophagehttp://en.wikipedia.org/wiki/Macrophagehttp://en.wikipedia.org/wiki/Adipocytehttp://en.wikipedia.org/wiki/Phosphocholinehttp://en.wikipedia.org/wiki/Complement_systemhttp://en.wikipedia.org/wiki/Opsoninhttp://en.wikipedia.org/wiki/Innate_immunityhttp://en.wikipedia.org/wiki/Innate_immunityhttp://en.wikipedia.org/wiki/Innate_immunityhttp://en.wikipedia.org/wiki/Innate_immunityhttp://en.wikipedia.org/wiki/Opsoninhttp://en.wikipedia.org/wiki/Complement_systemhttp://en.wikipedia.org/wiki/Phosphocholinehttp://en.wikipedia.org/wiki/Adipocytehttp://en.wikipedia.org/wiki/Macrophagehttp://en.wikipedia.org/wiki/Interleukin-6http://en.wikipedia.org/wiki/Inflammation
-
8/12/2019 microvascular dysfunction in RA.docx
8/14
8
Nitric Oxide is derived endhotelial releasing factor (EDRF) that
synthesized and released
by endothelial cells and serves as a potent vasodilator. The
release of NO stimulated by
bradykinin. Endothelium derived nitric oxide is synthesised from
the amino acid L-arginine
by the endothelial isoform of nitric oxide synthase
NO is isoenzymes in the body and there are 3 types:
Enzyme Endhotelial syntase NO (eNOS), an enzyme that has the
propertiesdependent on Ca, the enzyme is found in many types of
cells and are responsible for
most of the NO production in healthy blood vessels and released
continuously by
arterial and venous endothelial cells and platelets.
Neuronal NO synthase (nNOS), which is a special form of eNOS
function of nerves. inducible NO synthase (iNOS), an enzyme that
can be induced form, can be found
and removed by myocytes, macrophages and endothelial cells of
small blood vessels
that are enabled and can be induced by immunological stimuli by
cytokines and
endotoxin.
In normal circumstances, NO produced by eNOS which is activated
by blood vessels, but
in a state of inflammation, inducible NO (iNOS) is expressed by
macrophages and smooth
muscle cells that affect the production of NO. Increased
production of iNOS, leading to
consumption of L - arginine increased so that the substrate for
eNOS and iNOS decreased
and resulted in a decrease in the number of endothelial NO and
trigger endothelial
dysfunction.
NO is a major factor in maintaining endothelial function. Low
concentrations correlated
with decreased endothelial NO endothelial function. NO is an
important mediator in
endhotelium dependent vasodilation. In addition, NO also plays a
role in platelet aggregation
and regulating the growth and differentiation of smooth muscle
cells.
-
8/12/2019 microvascular dysfunction in RA.docx
9/14
9
CHAPTER IV
DISCUSSION
Atherosclerosis is the most common cardiovascular manifestation
in rheumatoid
arthritis. Inflammation plays an important role in the
development and progression of
atherosclerosis and congestive heart failure (CHF) . The
inflammatory process contributes to
the formation of early atherosclerotic plaques in the form of
lipid-laden macrophages and
induces plaque weakening and rupture leading to acute coronary
syndromes and sudden death
. Furthermore, many circulating markers of inflammation,
particularly C-reactive protein
(CRP), are associated with increased morbidity and mortality in
asymptomatic individuals
and in patients with cardiovascular disease and CHF .
Picture 5: correlation crp and chf
risk
Picture 4: prevalence atherosclerosis in rheumatoid
arthritis
Rheumatoid arthritis is autoimune disease. Autoimmune diseases
are illnesses that
occur when the body's tissues are mistakenly attacked by their
own immune system.When
antigen entry, it will activate macrophages to secrete
inflammatory cytokines. IL6 and TNF-a
will stimulate hepatocyt to secrete CRP, it causes increased
levels of CRP in rheumatic
arthritis patients. Rheumatoid arthritis also stimulates
limfosit B cells to produce
autoantibody. Autoantibodies to form immune complexes and will
attack the target cell,
where that target is their own body tissues.
-
8/12/2019 microvascular dysfunction in RA.docx
10/14
10
Increased CRP levels is important in endothelial dysfunction
because CRP can reduce
the synthesis of Nitric Oxide. NO is a major factor in
maintaining endothelial function. Low
concentrations correlated with decreased endothelial function.
NO is an important mediator in
endhotelium dependent vasodilation. Beside that, it can
stimulate secretion of CD4 from T
lymphocytes to damage endothelial cells. In addition, CRP also
stimulates LDL to get into
the macrophages forming foam cells that will eventually become
atherosclerotic plaques. (9,10)
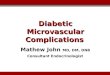
Picture 6 :Mechanisms relating C-reactive protein (CRP) to the
development and progression
of atherothrombosis. eNOS, endothelial nitric oxide
synthase;ET-1, endothelin 1;LDL, low-
density lipoprotein;MCP-1, monocyte chemoattractant protein
1;PAI-1, plasminogen
activator inhibitor-1
PreventionCorticosteroid are often used in the treatment of SLE.
RA and other inflammatory
disorder. High dose treatment with corticosteroid has adverse
effect on the cardiovascular
system, including endothelial dysfunction, hypertension, and
dysregulated glucose
metabolism. But, there is no evidence for similiar clinical
effects in patients treated with
low dose (< 7,5 mg/day). In the other hand, a protective
effect from CVD ( cardiovascular
disease) could be postulated based on control inflammation, so
it has been suggested that
corticosteroid treatment may be associated with a reduce risk of
atherosclerosis. MTX
(methothrexate) is today the anchor DMARDs for RA treatment;
this suggests that
-
8/12/2019 microvascular dysfunction in RA.docx
11/14
11
reducing RA inflammation, MTX may also reduce collateral damage
such as
atherosclerosis. (11)
Recently, treatment with TNF inhibitors was associated with a
lower risk of CVD
agents in a study of community based RA registers in Sweden.
These drugs act through
the inhibition of TNF alpha, a
proinflammatory cytokine
playing a primary role in RA
appearance, however, as
previously described, TNF
alpha has been implicated
also in the pathogenesis of
RA related atherosclerosis.
The cardioprotective effect of
TNF inhibition in RA may be
related to several factors, as,
for example, the increase of
HDL levels; therefore, these
drugs do not affect LDL
levels or atherosclerotic index
(i.e., TC/HDL ratio). On the other hand, these drugs may reduce
significantly insulin
levels and the insulin/glucose index, as well as improve insulin
resistance and also a
dramatic reduction of resistin, an adipokine that showed strong
correlation with C
reactive protein, was observed following infliximab infusion in
RA patients undergoing
this therapy because of severedisease Likewise, improvement of
endothelial function
following anti-TNF-alpha administration has been observed in RA
patients with severe
disease refractory to conventional DMARDs therapy.(13,14,15)
Statin reduce CVD morbidity and mortality. although they were
originally used in
this contect because of their effect in lipid level, it has
become increasingly evident that
they have other actionswhich may diminish CVD risk.(12) The anti
inflammatory and
immunomodulating effects of statin include supression of
leucocyte cytocine release.
Reduce MHC class II expression and reduced production of
reactive oxygen species.(16)
-
8/12/2019 microvascular dysfunction in RA.docx
12/14
12
CHAPTER V
CONCLUSION
Systemic inflammation (CRP) is associated with microvascular
dysfunction in
patients with RA. Rheumatoid arthritis and atherosclerosis are
strictly linked, this link is so
strong that atherosclerosis may be considered an extra-articular
manifestation of the
disease, leading to an increased risk of CVD. Moreover, the
impact of this extra -articular
manifestation on patients survival is of primary importance,
being in fact CVD, the
main prognostic factor in this setting. So it is important to
screen and monitor RA patients
to reduce the impact on cardiovascular system. To prevent the
occurrence of atherosclerosis
in patients with rheumatoid arthritis, the pateints can do
traditional form like physical
exercise and for medikamentosa treatment can use anti
inflamatory drugs for decrease CRP
serum, like methotrexate low dosage and TNF alfa inhibitor.
-
8/12/2019 microvascular dysfunction in RA.docx
13/14
-
8/12/2019 microvascular dysfunction in RA.docx
14/14
14
13.F. Atzeni, M. Turiel, R. Caporali et al., The effect of
pharmacological therapy on thecardiovascular system of patients
with systemic rheumatic diseases, Autoimmunity
Reviews, vol.9, no. 12, pp. 835839, 2010.
14.M. A. Gonzalez-Gay, C. Gonzalez-Juanatey, T. R. Vazquez-
Rodriguez, J. A.Miranda-Filloy, and J. Llorca, Insulin resistance
in rheumatoid arthritis: the impact
of the anti- TNF- therapy: annals of the New York Academy of
Sciences, Annals of
the New York Academy of Sciences, vol. 1193, pp. 153159,
2010.
15.C. I. Daen, Y. Duny, T. Barnetche, J.-P. Daur`es, B. Combe,
and J. Morel, Effect ofTNF inhibitors on lipid profile in
rheumatoid arthritis: a systematic review with meta-
analysis,Annals of the Rheumatic Diseases, vol. 71, no. 6, pp.
862868, 2012.
16.Palinski W, Napoli C. 2002. Untravelling Pleotropic Effects
of Statin on PlaqueRupture. Artherioscler Thromb Vasc Biol, 22:
1745 - 50