Embed Size (px)
Citation preview

Microsatellite instability and other molecularmarkers: how useful are they ?
Pr Frédéric Bibeau, MD, PhD
Head, Pathology department
CHU de Caen,
Normandy University,
France
ESMO preceptorship, Barcelona, 20.10.17
Content
- Colorectal cancer context
- CRC molecular classification
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion

Content
- Colorectal cancer context
- CRC molecular classification
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion

Tis T1 T2 T3 T4
MUCOSA
SUB-MUCOSA
MUSCULARIS
SUB-SEROSA -->SEROSA -->
pT
pN
pM
Muscularis Muscosae -->
N0 : no positive lymph node (LN)N1 : 3 positive LNN2 : ≥ 4 positive LN
M0 : No distant metastasisM1 : Distant metastasis
Organe infiltrationand / or visceral
peritoneal perforation
TNM UICC 2016 8thClassification
pTNM CRC classification

Early CRC treatment
N+Stage III
Chemotherapy(FOLFOX, 5-FU)
pT3-4 N0 Stage II
No chemotherapyBut rate of relapses: 20%
Need for additionnal prognostic factors
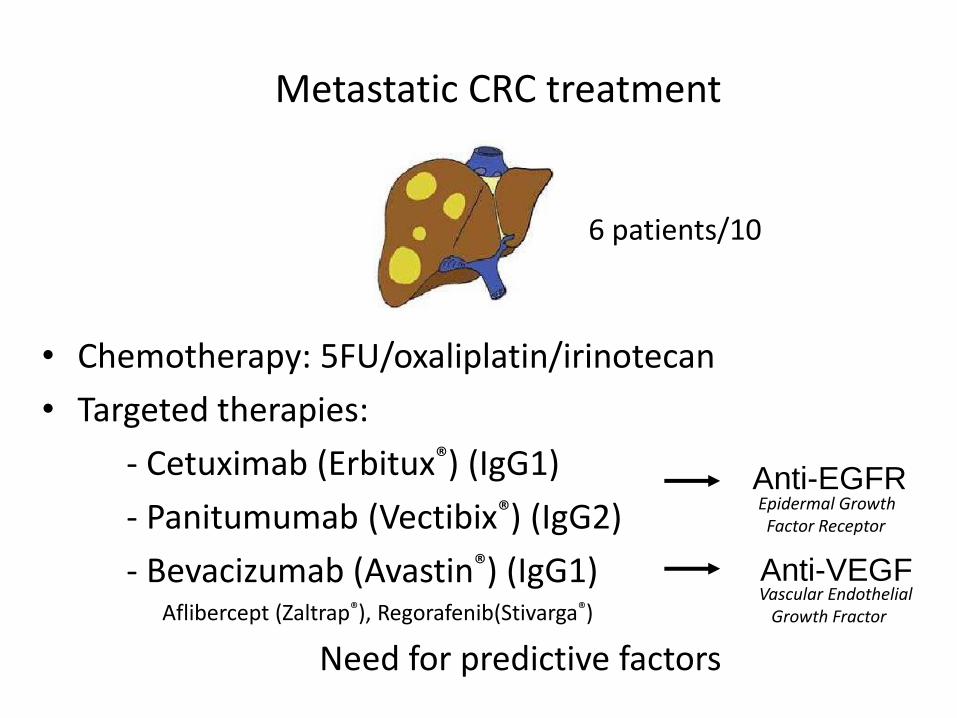
• Chemotherapy: 5FU/oxaliplatin/irinotecan
• Targeted therapies:
- Cetuximab (Erbitux®) (IgG1)
- Panitumumab (Vectibix®) (IgG2)
- Bevacizumab (Avastin®) (IgG1)Aflibercept (Zaltrap®), Regorafenib(Stivarga®)
Anti-EGFR
Anti-VEGF
Metastatic CRC treatment
Epidermal GrowthFactor Receptor
Vascular EndothelialGrowth Fractor
Need for predictive factors
6 patients/10

Sporadic(majority of cases)
Hereditary(6 % of cases)
CRC context
Screening toolsOptimal management

Content
- Colorectal cancer context
- CRC molecular classification
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion

small polype advanced polypavancé
cancer metastasesAberrant
crypts
CRC tumour progression

Voies d’oncogenèse CCR
CIN pathway MSI pathwayCIMP pathway
≈20 % 15- 20 %80-85 %
CRC carcinogenesis
Chromosomic Instabilty CpG Island Methylator Phenotype
Epigenetic instability
MicroSatellite Instabilty
KRAS, TP53 mutation
hMLH1, p16, MGMT methylation
BRAF mutation

Molecular profileMicrosatellite Instability
(ou soustraction)
Normal DNA
MSI tumour
NucleotidesLoss or gain

MSI CRC carcinogenesis
4 proteinsfor DNA reparation
Deficient MMR system

MSI (microsatellite instable)
Terminology
dMMR(deficient mismatch repair)
pMMR(proficient mismatch repair)
MSS (microsatellite stable)
RER+ Phenotype (Replication Error+)
RER- Phenotype(Replication Error-)

Stable tumour (MSS): 4 MMR proteins expressed
Immunohistochemistry

Loss of hML1 hMSH2 +
hMSH6 + Parallel loss of PMS2
Negative tumour Positive tumour
perso
nn
al caselF. B
ibeau
*MisMatch Repair
Instable tumour(MSI): extinction of MMR proteins
Immunohistochemistry

CIN pathway MSI pathwayCIMP pathway≈20 % 15- 20 %80-85 %
Lynch syndromeSerratedtumours
Conventionnal carcinomaCancer of the elderly
CRC molecular classification
Lieberkühnian Serrated Médullary/ lymphocytes
Chromosomic instability Epigenetic instability Microsatellite instability
Content
- Colorectal cancer context
- CRC molecular classifications
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion
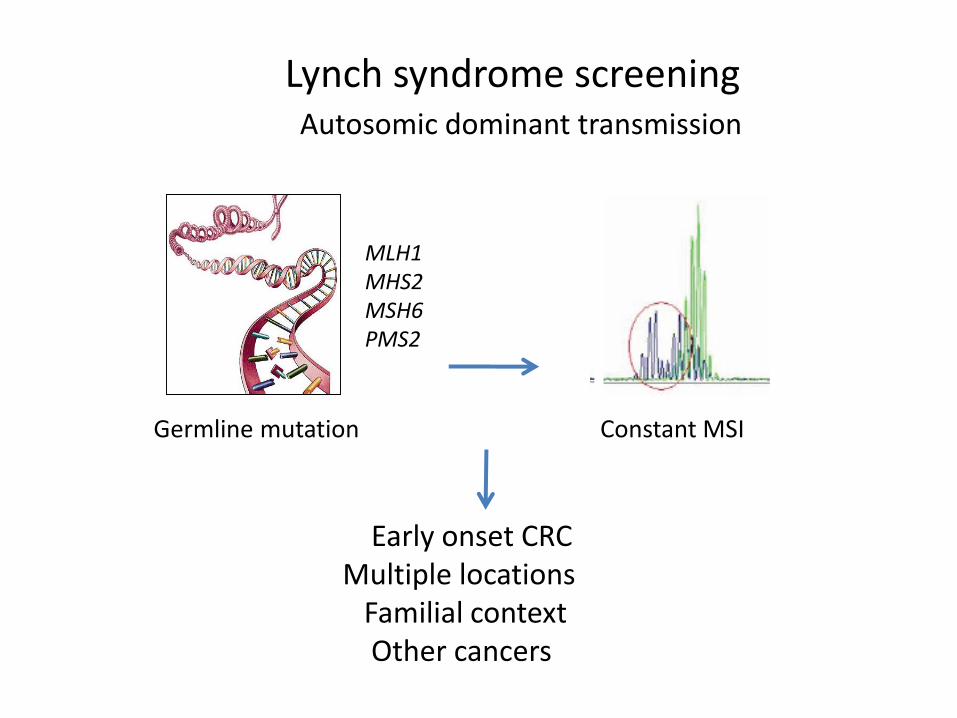
Autosomic dominant transmission
MLH1MHS2MSH6PMS2
Germline mutation Constant MSI
Early onset CRC Multiple locations
Familial contextOther cancers
Lynch syndrome screening

Lynch syndrome spectrum HNPCC: Hereditary Non Polyposis Colorectal Cancer
Other cancers
Cancer risk : 75% CCR, 50% endometrium, 15% others
Lynch syndrome screening
Colorectal
Small bowelUrinary tract
Endometrium

MLH1MSH2MSH6PMS2
Germile mutation Constant MSI
Mutation of thecorresponding gene
DNA
RNA
PROTEINS
Lynch syndrome screening
Time consumingHighly specialized laboratories

Oncogenetics team consultationGermline mutation determination
Prophylactic surgery …
Clinical, endoscopic, and US(if woman) follow-up
Lynch diagnosis
Familial investigation
+
CRC < 60 ansPersonal CRC historyCRC familial context
MSI +
Lynch syndrome screening

MSI and hMLH1 loss
Lynch syndrome (2%)Sporadic cancer (15%)
HypermethylationMLH1 promotor
BRAF mutation
Microsatellite instability context
Absent
Absent
Elderly patient Young patient

Content
- Colorectal cancer context
- CRC molecular classifications
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion

Identification of favorable stage II CRC
No adjuvant chemotherapy (5-FU)Lack of 5-FU efficacy
MSI Normal DNA
MSI tumour
Loss or
gain of
nucleotides
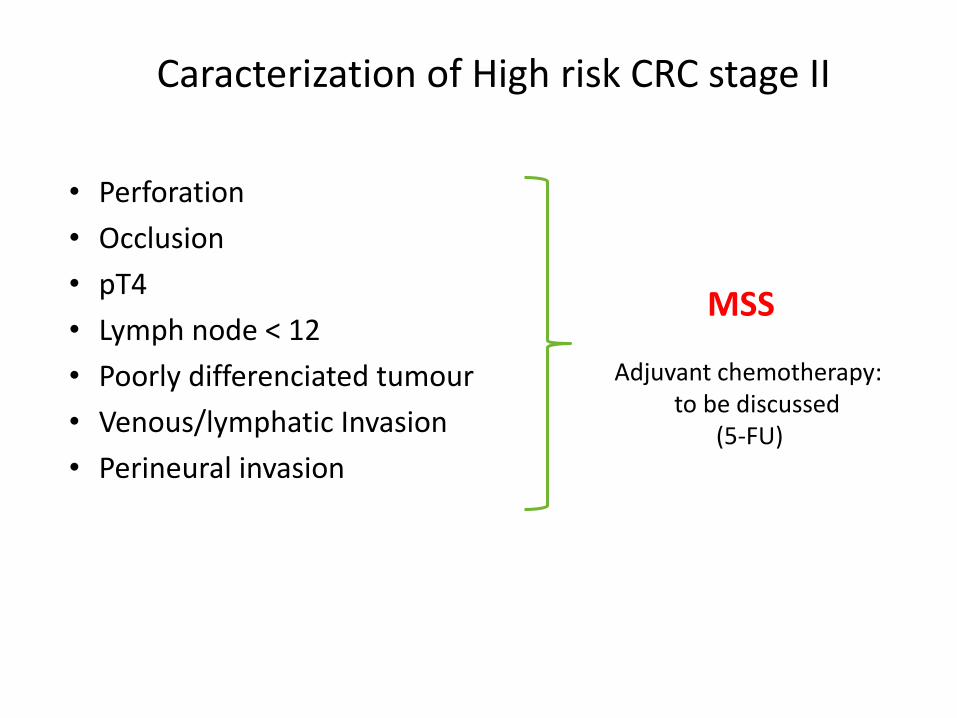
• Perforation
• Occlusion
• pT4
• Lymph node < 12
• Poorly differenciated tumour
• Venous/lymphatic Invasion
• Perineural invasion
Adjuvant chemotherapy: to be discussed
(5-FU)
Caracterization of High risk CRC stage II
MSS

Caracterization of agressive stage III CRC
MSSKRAS mut.BRAF mut.
*Taieb et al JAMA Oncol 2016
Intensified chemotherapy: clinical trials Stratification according mutations ?

Identification of agressive stage IV CRC
MSSKRAS mut.BRAF mut.
Metastatic setting
Intensified chemotherapy: FOLFIRINOX+ Bevacizumab (BRAF mut.)Ongoing clinical trials (combined targeted therapies)

Content
- Colorectal cancer context
- CRC molecular classifications
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion

RAS mutations = marker of resistance
Anti-EGFR targeted therapies
Cetuximab
PanitumumabAnti-EGFR antibodies
Angiogenesis
Growth
MotilityMetastases
ChemotherapyRadiotherapy
Cell cycle activation
RAS

Résistance: mutations KRAS
Normal différenciation, proliferationand growth
Adapté de Van Krieken et al. Virchows 2008;453:417-431
abnormal différenciation, proliferationand growth

Recommendations
Primary CRC Metastasis
RAS testing mandatory before anti-EGFR therapy on
Or

Molecular techniques

Selection Macrodissection Mutation ?
Quality of the pre-analytique step

Quality of the pre-analytique step
Use the pretreatment biopsy

RAS and BRAF WT
Mutation KRAS exon 2
Mut KRAS ex 3, 4
Mut NRAS
50%
RAS mutated
HER-2
BRAF
10%
Amplifications: 2,5%Mutations: 1,9%
Anti-HER2Targeted
therapies?
Anti-EGFR resistance ?
SPECTAcolor: Folprecht ESMO 2016, abst 4580
Sartore-Bianchi Lancet Oncol 2016Hurwitz ASCO GI 2016Marsoni AACR 2017
Trastuzumab + lapatinib(HERACLES)
Trastuzumab + pertuzumab
Raghac ASCO 2016
40%
CRCm molecular biomarkers and targets
MSI5%

Immunotherapy
MSI CRC : immunogenic tumour Metastatic MSI CRC
Immuneescape
Crohn like reaction
Lymphocytic infiltrate

ImmunotherapyCheck-points immunity
inhibitors
High response rate(anti-PD1 pembrolizumab)
Immune enhancement
Le DT et al. N Eng J Med 2015;372:2509-20
MSI CRC : immunogenic tumourT lymphocyte receptor
T lymphocyte receptor
Antigen
Antigen
Tumor cell
Tumor cell
PDL1 inhibitor
PD1inhibitor

ImmunotherapyAnti-PD-1 treatment: overall survival
Selection of patients based on MSI status
CCR MSI
CCR MSS
Mois

Content
- Colorectal cancer context
- CRC molecular classification
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion

Content
- Colorectal cancer context
- CRC molecular classification
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion
RAS and BRAF mutationnal status determination
Circulating tumour DNA ?
- Non invasive technique- Monitoring(cf Pierre Laurent PuigLecture)
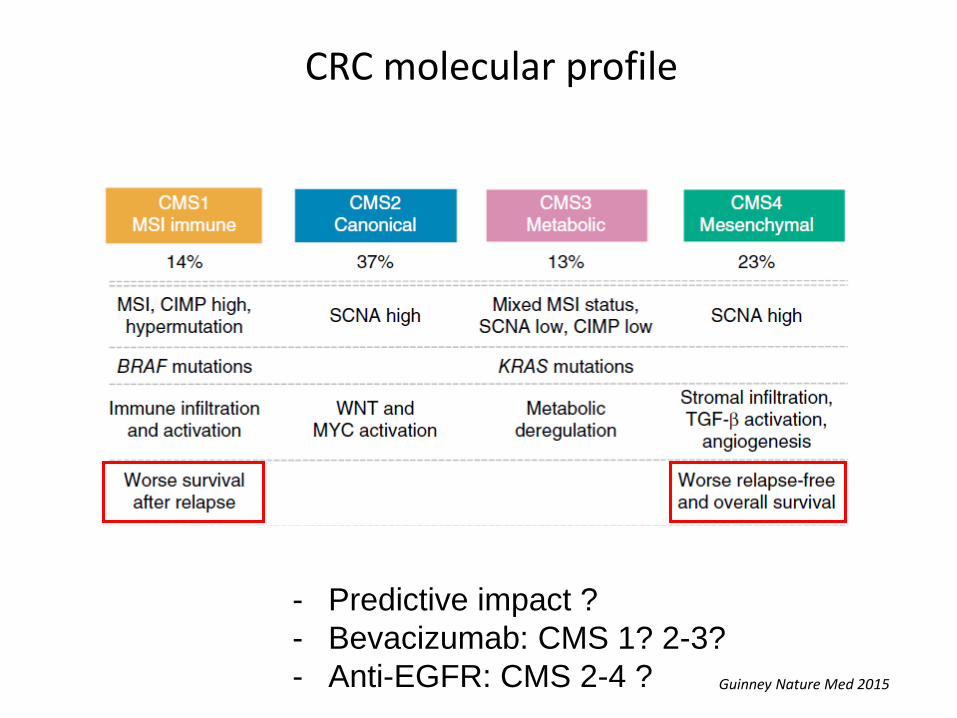
CRC molecular profile
- Predictive impact ?
- Bevacizumab: CMS 1? 2-3?
- Anti-EGFR: CMS 2-4 ? Guinney Nature Med 2015

Quality control

Content
- Colorectal cancer context
- CRC molecular classification
- Diagnostic value
- Prognostic value
- Therapeutic value
- Perspectives
- Conclusion

CIN pathway MSI pathwayCIMP pathway≈20 % 15- 20 %80-85 %
Lynch syndromeSerratedtumours
Conventional carcinomaCancer of the elderly
Molecular CRC classification- Useful biomarkers
BRAFmutation
RASmutation
Anti-EGFR resistance(predictive factor
Pronosticfactor
Lynch diagnosis
No 5-FU efficacy
Anti-PD-1 efficacy
PronosticMSI


MLH1MSH2MSH6PMS2
Germile mutation Constant MSI
Time consumingHighly specialized laboratories
Lynch syndrome screening

Microsatellite instability
Diploidy
No /or few loss of heterozygocity
(ou soustraction)
Normal DNA
MSI tumour
Loss or
gain of
nucleotides

Molecular profileMicrosatellite Instability
(ou soustraction)
Normal DNA
MSI tumour
NucleotidesLoss or gain

MisMatch Repair system (MMR)
4 proteinsfor DNA reparation

*Marisa et al. Plos One 2016, * * Guinney Nature Med 2015
Molecular profile
Signatures
Poor pronosis
Addition of immune signature ?
Adapté de Pagès et al., New Engl J Med 2005
CMS**ConsensusMolecularsignature

*Marisa et al. Plos One 2016, * * Guinney Nature Med 2015
Molecular profile
Signatures
Adapté de Pagès et al., New Engl J Med 2005
CMS**ConsensusMolecularsignature
Reliable on fixed tissue ? Reliable by using immunohistochimistry ?
Prediction of response to FOLFIRI, Cetuximab ?

Quality control

Quality control

Quality control




























