Embed Size (px)
Citation preview

Ultrasound in Med. & Biol., Vol. 40, No. 9, pp. 2321–2324, 2014Copyright � 2014 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/$ - see front matter
/j.ultrasmedbio.2014.04.008
http://dx.doi.org/10.1016d Clinical Note
MICROCALCIFICATIONS VERSUS ARTIFACTS: INITIAL EVALUATION OFANEW ULTRASOUND IMAGE PROCESSING TECHNIQUE TO IDENTIFY BREAST
MICROCALCIFICATIONS IN A SCREENING POPULATION
PRISCILLA MACHADO, JOHN R. EISENBREY, BARBARA CAVANAUGH, and FLEMMING FORSBERGDepartment of Radiology, Thomas Jefferson University, Philadelphia, Pennsylvania, USA
(Received 5 December 2013; revised 20 February 2014; in final form 15 April 2014)
ARadioldelphia
Abstract—A new commercial image processing technique (MicroPure, Toshiba AmericaMedical Systems, Tustin,CA, USA) that identifies breast microcalcifications was evaluated at the time of patients’ annual screening mam-mograms. Twenty women scheduled for annual screening mammography were enrolled in the study. Patients un-derwent bilateral outer-upper-quadrant real-time dual gray scale ultrasound and MicroPure imaging using anAplio XG scanner (Toshiba). MicroPure combines non-linear imaging and speckle suppression to mark suspectedcalcifications as white spots in a blue overlay image. Four independent and blinded readers analyzed digital clips todetermine the presence or absence of microcalcifications and artifacts. The presence of microcalcifications deter-mined by readers was not significantly different from that of mammography (p5 0.57). However, the accuracy waslow overall (52%) and also in younger women (,50 years, 54%). In conclusion, althoughmicrocalcifications can beidentified using MicroPure imaging, this method is not currently appropriate for a screening population andshould be used in more focused applications. (E-mail: [email protected]) � 2014 World Feder-ation for Ultrasound in Medicine & Biology.
Key Words: Ultrasound, Breast, Microcalcifications, Image processing, Mammography.
INTRODUCTION
Mammography is an X-ray imaging method for breastcancer screening. Its ability to evaluate microcalcifica-tions in detail is an important asset, because microcalcifi-cations are considered an important finding in thediagnosis of breast cancer. This method is used to differ-entiate possible benign from suspicious microcalcifica-tions that require further examination for a definitediagnosis (Huang et al. 1999; Moon et al. 2002;Nagashima et al. 2005; Park et al. 2010; Soo et al.2002; Yang et al. 1997). Mammography has highsensitivity and specificity for the screening of breastcancer, varying from 77% to 95% and from 94% to97%, respectively (Nelson et al. 2009).
Gray scale ultrasound (US) imaging is not currentlyperformed for the clinical evaluation of breast microcal-cifications because of the limitations of this techniquein identifying microcalcifications (Huang et al. 1999;Moon et al. 2002; Nagashima et al. 2005; Park et al.
ddress correspondence to: Flemming Forsberg, Department ofogy, Thomas Jefferson University, 132 South 10th Street, Phila-, PA 19107, USA. E-mail: [email protected]
2321
2010; Soo et al. 2002; Yang et al. 1997). Researchershave attempted to use gray scale US to identify microcal-cifications with some promising results, but results to datedo not support the clinical use of gray scale breast US forthis application (Huang et al. 1999; Moon et al. 2002;Nagashima et al. 2005; Park et al. 2010; Soo et al.2002; Yang et al. 1997).
MicroPure is a new commercial US image process-ing technique (Toshiba America Medical Systems, Tus-tin, CA, USA) that processes US images to improve thevisualization of breast microcalcifications. MicroPurecombines non-linear imaging and speckle suppressionto mark suspected calcifications as white spots in a blueoverlay image (Kamiyama et al. 2008). A pilot study byMachado et al. (2012) that focused on the evaluation ofMicroPure for the identification of breast microcalcifica-tions obtained promising results, with an increase in themean number of microcalcifications seen on MicroPurewhen compared with gray scale US. The study also indi-cated that MicroPure artifacts, which can be confusedwith microcalcifications, are usually due to Cooper’sligaments.
The purpose of this study was to determine if Micro-Pure can identify breast microcalcifications in patients

2322 Ultrasound in Medicine and Biology Volume 40, Number 9, 2014
scheduled for their annual screening mammograms andto establish whether artifacts can be confused with micro-calcifications in this mode.
METHODS
SubjectsThis study was a prospective clinical trial conducted
from January to July of 2013 and involving 20 adult fe-male patients who were approached when they went tothe Breast Imaging Center at Thomas Jefferson Univer-sity Hospital for their scheduled annual mammogram.The mean age of the patients participating in the studywas 55.3 years (range: 35–73 years, with 7 subjects,50 years), and all women provided written informedconsent. The study was approved by the University’sinstitutional review board and was compliant with theHealth Insurance Portability and Accountability Act.
This study was supported by Toshiba AmericaMedical Systems, which provided grant support and
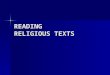
Fig. 1. Real-time dual images obtained with gray scale ultr(b) Artifacts and microca
equipment. However, the authors of this article had solecontrol of the data generated by this trial and the informa-tion provided for publication.
Data acquisitionSubjects underwent bilateral outer-upper-quadrant
real-time dual imaging with gray scale US and Micro-Pure. An Aplio XG scanner (Toshiba America MedicalSystems) with a 14 MHz broad bandwidth linear arraywas used. No compounding or other image processingtechniques were applied. The time-gain compensationand 2-D gain setting were optimized for each subject indi-vidually. Sagittal and transverse still images as well asdigital clips of the area were obtained in all subjects.Example images are provided in Figure 1.
Mammographic images were acquired in two stan-dard image planes: mediolateral oblique and craniocau-dal. Additional views were acquired when necessary tomake a diagnosis. Mammography was performed using
asound (left) and MicroPure (right). (a) Only artifacts.lcifications (arrow).

Breast microcalcification screening with MicroPure d P. MACHADO et al. 2323
a Senographe Essential or Senographe DS unit (GEHealthcare, Milwaukee, WI, USA). One radiologistdetermined the presence or absence of microcalcifica-tions on mammography, and these data were used as thereference standard. Microcalcifications were consideredpresent when they were seen in the outer upper quadranton both mammographic views (mediolateral oblique andcraniocaudal). Each breast was analyzed separately.
Data analysesFour independent, blinded readers—two radiolo-
gists (20 and 10 years of experience, respectively) andtwo physicists (20 and 7 years of experience, respec-tively)—analyzed 40 digital clips to determine the pres-ence or absence of microcalcifications and artifacts.The artifacts were considered to be Cooper’s ligaments,which can appear as white spots in the MicroPuremode. The data were analyzed in three groups: all pa-tients, patients ,50 years old and patients .50 yearsold. All three groups were compared separately withrespect to the presence of microcalcifications and arti-facts using a c2 test. All tests were performed using Stata12.0 (Stata Corp, College Station, TX, USA) with p-values ,0.05 indicating statistical significance.
RESULTS
The population studied was a screening population,and for that reason, it was not surprising that all micro-calcifications seen on mammography were scatteredmicrocalcifications considered to be benign. Microcalci-fications were seen in 18 of the 40 breasts analyzed, bilat-erally in 6 patients and unilaterally in 6 patients. Readers’evaluations of the presence or absence of microcalcifica-tions did not significantly differ from those of mammog-raphy, with a p-value of 0.57 for all patients (,50 yearsold, p 5 0.43; .50 years old, p 5 0.87). Table 1 com-pares the accuracy of the readers for the three groups. Ac-curacy was low overall, with mean values of 52% (range:47%–56%) for all patients; 54% (range: 36%–64%) foryounger women (,50 years old); and 50% (range:42%–58%) for older women (.50 years old).
When artifacts were analyzed, radiologists andphysicists disagreed. Radiologists saw artifacts in the
Table 1. Percentage of agreement between MicroPureand mammography on the presence of
microcalcifications
Patients ,50 y Patients .50 y All patients
Reader 1 57% 46% 52%Reader 2 64% 42% 53%Reader 3 36% 58% 47%Reader 4 57% 54% 56%Total 54% 50% 52%
majority of the cases, whereas the physicists did not agreewith the radiologists or among themselves. The presenceof artifacts had no effect on the accuracy of identificationof microcalcifications, meaning that the presence orabsence of artifacts does not interfere with the ability toidentify microcalcifications (Fig. 1).
DISCUSSION
The visualization and analysis of breast microcalci-fications are crucial, because these are an importantfinding in the diagnosis of breast cancer (Huang et al.1999; Moon et al. 2002; Nagashima et al. 2005; Parket al. 2010; Soo et al. 2002; Yang et al. 1997).Mammography is currently the only reliable methodthat can identify and classify microcalcifications in ascreening population (Huang et al. 1999; Moon et al.2002; Nagashima et al. 2005; Soo et al. 2002; Yanget al. 1997). The US technology currently in clinicaluse cannot reliably detect or evaluate breast microcalci-fications. Prior studies indicated that microcalcificationsare seen on US when they are located inside hypo-echoic solid masses, because the solid masses provide ahypo-echoic background that improves visualization ofthe bright microcalcification echoes (Huang et al. 1999;Moon et al. 2002; Nagashima et al. 2005; Park et al.2010; Soo et al. 2002; Yang et al. 1997). Hence, theevaluation of isolated microcalcifications, often benign,within normal breast tissue is considered to be moredifficult with US, because of the lack of contrastbetween normal parenchyma and the microcalcifications(Huang et al. 1999; Moon et al. 2002; Nagashima et al.2005; Park et al. 2010; Soo et al. 2002; Yang et al. 1997).
A recent pilot study on the use of MicroPure for theidentification of clusters or isolated microcalcifications inpatients whose mammograms revealed microcalcifica-tions reported promising results, with a statisticallysignificant increase in the mean number of microcalcifi-cations seen on MicroPure images compared with thaton gray scale US, using mammography as the referencestandard (on average 1.9 6 1.70 vs 0.7 6 1.10;p , 0.009) (Machado et al. 2012). That study also foundthat MicroPure artifacts, which can be confused with mi-crocalcifications, are usually due to Cooper’s ligaments.MicroPure is currently being investigated for the identifi-cation of breast microcalcifications in patients undergo-ing stereotactic or US-guided biopsies compared withX-ray of the tissue retrieved (Machado et al. 2013a). Inthat study, all patients have suspicious microcalcifica-tions that are going to be analyzed by pathology.Although that study is ongoing, the results to date areencouraging, indicating good agreement between themean number of microcalcifications seen on MicroPureand the mean number of microcalcifications seen on

2324 Ultrasound in Medicine and Biology Volume 40, Number 9, 2014
X-ray images of the tissue, with a p-value of 0.29(Machado et al. 2013a).
The accuracy of Micropure in identifying microcal-cifications in this screening population was low overall(36%–64%). This indicates that MicroPure is not usefulas a screening method. It should be noted that this wasa small pilot study performed in only 20 subjects. Instead,MicroPure should be used for more focused clinical ap-plications, such as ultrasound-guided biopsy procedures,when microcalcifications are known to be present. Initialresults in this application are encouraging: in four lesionsthat underwent US-guided biopsy using MicroPure, theduration was the same as that for regular US-guided bi-opsy with gray scale imaging, and the performing radiol-ogist had confidence in the images. Most importantly,MicroPure and X-ray images of the retrieved tissue re-vealed microcalcifications in all lesions, confirmingthat the images seen during the procedure (i.e., withMicroPure) did indeed represent microcalcifications(Machado et al. 2013b).
CONCLUSIONS
MicroPure does not seem to be reliable as ascreening tool to identify microcalcifications. Instead,MicroPure imaging should be used for more focused clin-ical applications, such as real-time US-guided biopsy.
Acknowledgments—We gratefully acknowledge that Toshiba AmericaMedical Systems provided grant support and equipment for this study.
REFERENCES
Huang CS, Wu CY, Chu JS, Lin JH, Hsu SM, Chang KJ. Microcalcifi-cations of non-palpable breast lesions detected by ultrasonography:Correlation with mammography and histopathology. UltrasoundObstet Gynecol 1999;13:431–436.
Kamiyama N, Okamura Y, Kakee A, Hashimoto H. Investigation ofultrasound image processing to improve perceptibility of microcal-cifications. J Med Ultrason 2008;35:97–105.
Machado P, Eisenbrey JR, Cavanaugh BC, Forsberg F. New imageprocessing technique for evaluating breast microcalcifications:A comparative study. J Ultrasound Med 2012;31:885–893.
Machado P, Eisenbrey JR, Cavanaugh B, Forsberg F. Identification ofbreast microcalcifications using a new ultrasound image processingtechnique on patients prior to biopsy [abstract]. Ultrasound MedBiol 2013a;39:S87.
Machado P, Eisenbrey JR, Cavanaugh B, Forsberg F. Ultrasound guidedbiopsy of breast microcalcifications with a new ultrasound imageprocessing technique [abstract]. Ultrasound Med Biol 2013b;39:S41.
Moon WK, Myung JS, Lee YF, Park IA, Noh DY, Im JG. US in ductalcarcinoma in situ. RadioGraphics 2002;22:269–281.
Nagashima T, Hashimoto H, Oshida K, Nakano S, Tanabe N, Nikaido T,Koda K, Miyasaki M. Ultrasound demonstration of mammographi-cally detected microcalcifications in patients with ductal carcinomain situ of the breast. Breast Cancer 2005;12:216–220.
Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L.Screening for breast cancer: Systematic evidence review updatefor the U.S. preventive services task force. Ann Intern Med 2009;151:727–737.
Park JS, Park YM, Kim EK, Kim SJ, Han SS, Lee SJ, In HS,Ryu JH. Sonographic findings of high-grade and non-high-grade ductal carcinoma in situ of the breast. J Ultrasound Med2010;29:1687–1697.
Soo MS, Baker JA, Rosen EL, Vo TT. Sonographically guided biopsy ofsuspicious microcalcifications of the breast: A pilot study. AJR Am JRoentgenol 2002;178:1007–1015.
Yang WT, Suen M, Ahuja A, Metreweli C. In vivo demonstration of mi-crocalcification in breast cancer using high resolution ultrasound.Br J Radiol 1997;70:685–690.