Embed Size (px)
Citation preview

Microbiology 261 –Lecture NotesMicrobes and Hosts: Infection, Disease and Defenses
Dr. Gary G. Andersen

We make contact! Resident flora – (skin, upper respiratory
tract, gastro-intestinal tract, urethra, genitalia, vagina, external ear canal, external eye) (Note: All internal tissues and organs are sterile)
Birth is a microbe event See pg 388 for microbes established on
humans.
Flora Locations and Types Transient – (variable) such as on skin surface Resident – (stable populations) Skin - deeper layers of skin (stable populations of
Staphlococcus, Corynebacterium, & Yeasts) GI tract: Mouth – Streptococcus species GI tract: Intestine – Anaerobes such as
Bacteroides, Bifidobacterium, Fusobacterium, Clostridium and Coliforms

Flora Locations and Types (cont.) Respiratory Tract – upper nasal passages and
throat (Staphylococcus aureus) Genitourinary Tract – eurethral opening and
vagina (Lactobacillus, Steptococcus, Corynebacterium, Escherichia, Mycobacterium)
Germ-free animals are healthier as long as they remain in a sterile environment

Host Parasite RelationshipsA. Symbiosis – the relationship between bacteria (microbiota)
and us (the host!).1. Parasitism – pathogenic, harmful to the host.2. Mutualism – both microbe and host benefit. Bacteria in the colon release Vitamin K as a waste product. Vitamin K is used in clotting. 3. Commensalism – microbe benefits by absorbing nutrients released from sloughed dead cells.

Normal Microbiota Mutualists and commensalists comprise the
normal microbiota of the host. Normal microbiota can be permanent (resident), or transient bacteria. Opportunistic bacteria are normal microbiota that may cause disease when the immune system is depressed from cold or flu viruses. It has been estimated 1015 bacteria live in or on the human body. (500 – 1000 species) Yet, the human body itself comprises only 1014 eukaryotic cells in the adult!
The disruption of Normal Microbiota1. Vaginal Bacteria
pH 4.0 birth - 2-3 wks. Lactobacilli (residual estrogen)
pH 7.5 2-3 wks. – puberty Various Microbes
(no estrogen) ex. Staph & Strep.
pH 4.0 puberty – menopause Lactobacilli
(estrogen levels high)
pH 5.0 Oral contraceptives, broad spectrum antibiotics, or frequently douching may cause: Opportunistic infections may arise causing vaginosis: ex. Candida albicans (yeast), Gardenerella vaginalis (bacteria), or Trichomonas vaginalis (protozoan)
pH 7.5 postmenopausal Various Microbes: Staph & Strep.
GA f07

Infectious Disease ClassificationsA. Symptomology – changes in body function
resulting from infectious diseases.
1. asymptomatic – without symptoms. Detection based on positive blood test indicating presence of antibodies. Inapparent, subclinical and carrier are synonyms. Insidious infection if damaging host tissues without symptoms, Ex. Pelvic Inflammatory Disease. Etiology: Chlamydia, or Neisseria gonorrhea.
2. Subjective symptoms – malaise, a general feeling of discomfort.
3. Objective symptoms – observable and measured conditions. Ex. Rash size and color, body temperature, and extent of lymphadenopathy (lymph node swelling).
Infectious Disease Stages p 402
1. Incubation Period – no symptoms
2. Prodromal period – subjective symptoms
3. Period of Invasion – objective symptoms
4. Convalescence – decrease to subjective or no symptoms.

Modes of Transmission MOTYe’ ole 6 F’s: feces, flies, fingers, fomites,
food and fornication!1. Contact Transmission
a. Direct contact – STD’s, or vertical (prenatal and perinatal).b. Indirect contact – fomites: ex.
money, catheter, syringe, eating utensils.
c. Droplet contact – within 1 meter zone!

2. Vehicle Transmission a. Water – raw sewage in water results
in fecal-oral cycle.
b. Food – poisoning via bacterial toxins as with botulism (ex. Clostridium botulinum), or gastroenteritis from bacteria (ex. Salmonella typhi) or viruses (ex Rotavirus) that invade the colon.
c. Airborne – greater than 1 meter in extreme wind blown conditions such as
in military settings. 747 airlines recirculate air.
GA f 07
Vectors3. Vector Transmission
a. Mechanical – the feet of flies
b. Biological – insect bites
ex. Anopheles mosquito transmits malaria, etiology:
Plasmodium vivax.
ex. Rat Flea transmits bubonic plague,
etiology: Pasteurella pestis
ex. Tick transmits Lymes disease,
etiology: Borrelia burgdorferi

Flies defecate, vomit, feed
Zoonoses (pl.)– diseases transmitted directly from animals to humans, or indirectly from animals by insect vectors. ex. Malaria and Yellow Fever have a monkey reservoir. Wild and domestic animals are carriers for many human infectious diseases. Zoonoses include diseases transmitted by feathers, hides, or furs to humans.
ex. Tularemia – “rabbit fever” etiology: Francisella tularensis (Gram – bacteria)
ex. Toxoplasmosis – etiology: Toxoplasma gondii. A protozoan parasite found in cat litter boxes. Beware if pregnant or with reduced immunity.
ex. Rabies – etiology; Rhabdovirus. A virus transmitted by skunks and raccoon.

Rabies (Dog and restrained man)
GA sp07

Epidemiology
1. Definition – the study of the incidence, transmission and frequency of a disease.
2. Centers for Disease Control and Prevention (the CDC) in Atlanta, MMWR, the Morbidity and Mortality Weekly Report. Provides cumulative statistical public health information. http://www.cdc.gov/mmwr/
3. The World Health Organization (W.H.O.) in Geneva, Switzerland. Conducts international epidemiological research.

4. Communicable disease – direct contact 5. Non-communicable disease – vehicle,
vector or indirect contact transmission. ex. Bacillus anthracis endospores in the mail!
6. Endemic – a disease that is constantly present in a local population. Ex. malaria
7. Epidemic – many people contracting a disease in a short period of time. Ex. Lyme disease
8. Pandemic – global spread of pathogen.
NOSOCOMIAL INFECTIONS p433
Nosocomial def. – from the Greek word for “hospital” A. The CDC claims that ~8% of all inpatients acquire new
infections while in the hospital. ~ 20,000 deaths/year.
B. Three reasons for nosocomial infections:
1. There is a concentration of virulent, antibiotic resistant microbes in hospitals.
2. Patients are normally immunocompromised from chemotherapy, radiation, malnutrition, and psychological or physiological stress.
3. Chain of Transmission – from patients to doctors to other patients. Lack of handwashing!

What Normal Microbiota become Nosocomial Infections
1. E. coli, Enterococcus faecalis, and Staph. saprophyticus cause roughly ~50% of all nosocomial infections. Due to urinary catheterizations that push fecal bacteria into the bladder (bladder infection- cystitis) High mortality rate.
2. E. coli causes roughly ~25% of all nosocomial infections due to colon surgery. Clostridium difficile from prolonged use of antibiotics which destroys normal bacterial communities.
3. Lower respiratory tract pneumonia causing microbes. ~12% of all nosocomial infections. Pneumocystis carinii is the most common opportunist in AIDS patients.
4. Cutaneous (skin) infections, ~ 8% of all nosocomial infxns. Staph. aureus outbreaks in nurseries and bedsores in long term care patients. Ex. Methicillin Resistant Staph aureus (MRSA).
5. Bacteriemia – bacteria accidentally introduced into blood stream by contaminated intravenous fluids. Ex. portacaths (implanted caths) or dialysis.

Portacaths
What makes microbes pathogenic or virulent?
SEVEN MECHANISMS OF PATHOGENESIS
1. Maintain a reservoir – in humans (carriers), animals (zooneses), water, soil, dust etc.
2. Adherance hooks, spikes, tacky chems
3. Anti-phagocytic properties: capsule, Wax D, M-protein in Streptococcus pyogenes, and antigenic drift in Influenza (virus), Neisseria (bacteria), and Trypanosomes (protozoan).

Adhesion: How do pathogens stick? Fimbriae (bacterial
projections) Capsules (bacterial
coatings) Spikes (viral
particles) Hooks
(Treponema) or flagella (Salmonella)
Vibro cholerae attaching to intestinal cells

4. EXOENZYMES – secreted by pathogens
a. Hemolysin – lysis of erythrocytes (RBC)
b. Leukocidin – degrades lysosomes, the digestive vacuole found in phagocytes. Staph. aureus.
c. Coagulase – clots blood Staph aureus.
d. Streptokinase – dissolves clots ex. Strep. and Staph.
e. Hyaluronidase –hydrolyzes the “glue” that holds cells together, I.e. the dermis to the epidermis. Leaves tissues black. ex. Clostridium perfringens causes gas gangrene.
f. Collagenase – degrades collagen, Strep. pyogenes (necrotizing faciitis)
g. Urease – ex. Helicobacter pylori survives at low stomach pH. Causes ulcers. http://www.bact.wisc.edu/Bact330/lecturehelico2
h. Neisseria gonorrhea degrades imunoglobulin (IgA) found in mucous rendering its antibody activity to be lost.

5. SIDEROPHORES Most pathogens obtain iron from the host
by secreting these low molecular weight proteins into the blood which strip iron from transferrin, a glycoprotein in the blood.
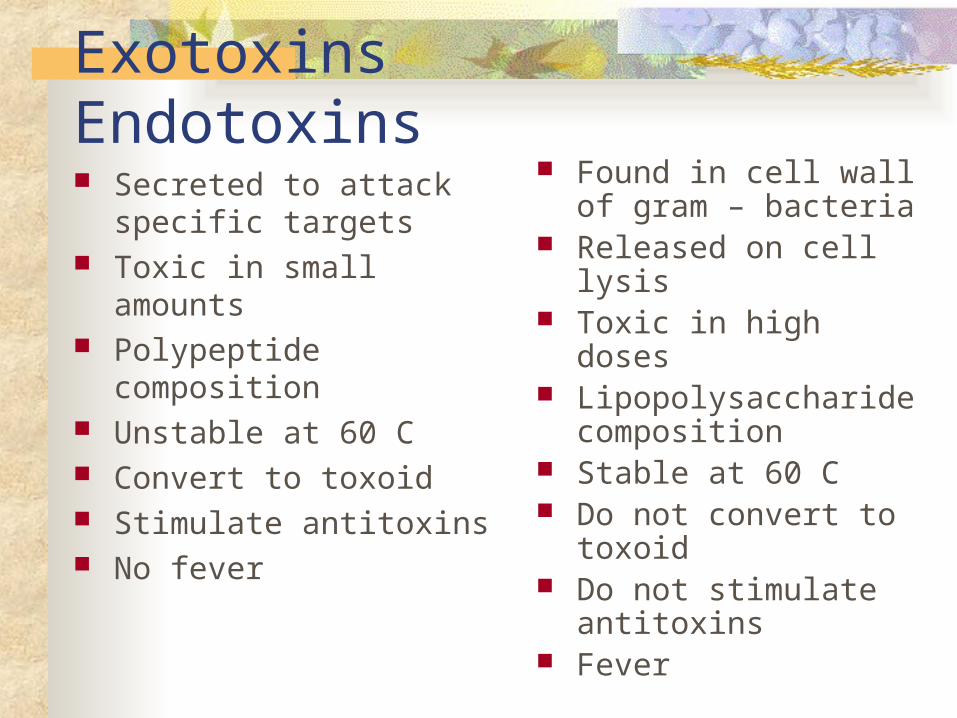
Exotoxins Endotoxins Secreted to attack
specific targets Toxic in small amounts Polypeptide composition Unstable at 60 C Convert to toxoid Stimulate antitoxins No fever
Found in cell wall of gram – bacteria
Released on cell lysis Toxic in high doses Lipopolysaccharide
composition Stable at 60 C Do not convert to
toxoid Do not stimulate
antitoxins Fever
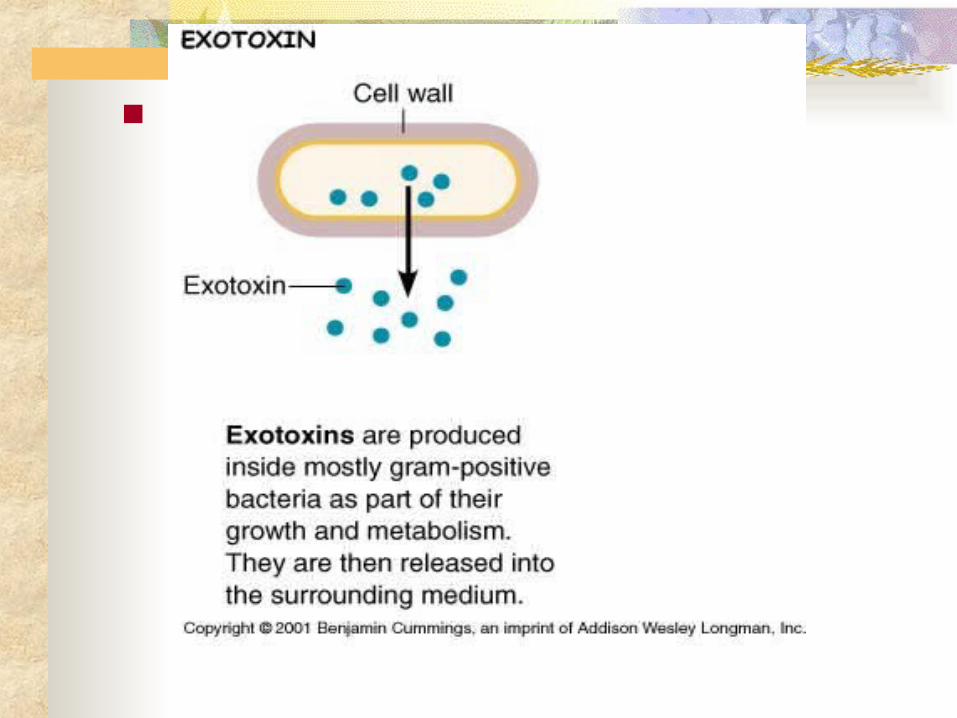
6. EXOTOXINSa. Toxic proteins secreted by bacteria that
disrupt cell membranes. b. Toxemia – exotoxins in blood or lymph.c. Toxoid – inactivated altered exotoxins
used for vaccination. d. Exotoxins are toxic in small quantities.e. Exotoxins are heat labile (sensitive) if
treated at 60 degrees Celsius for 30 minutes.


f. Three examples of powerful exotoxins:1. Cytotoxins – kill host cells by disrupting protein synthesis. Toxoid used in “D” part of the DTP vaccine. ex. Corynebacterium diphtheriae2. Neurotoxins – act on nerve cells
ex. Clostridium tetani – (tetanus) blocks Ach inhibitors and leaves ACh on. Spastic paralysis.
ex. Clostridium botulinum – (botulism) binds ACh receptors blocking them. Flaccid paralysis. 3. Enterotoxins – binds to villus cells causes excess loss of water and electrolytes (gastroenteritis). ex. Vibrio cholerae.

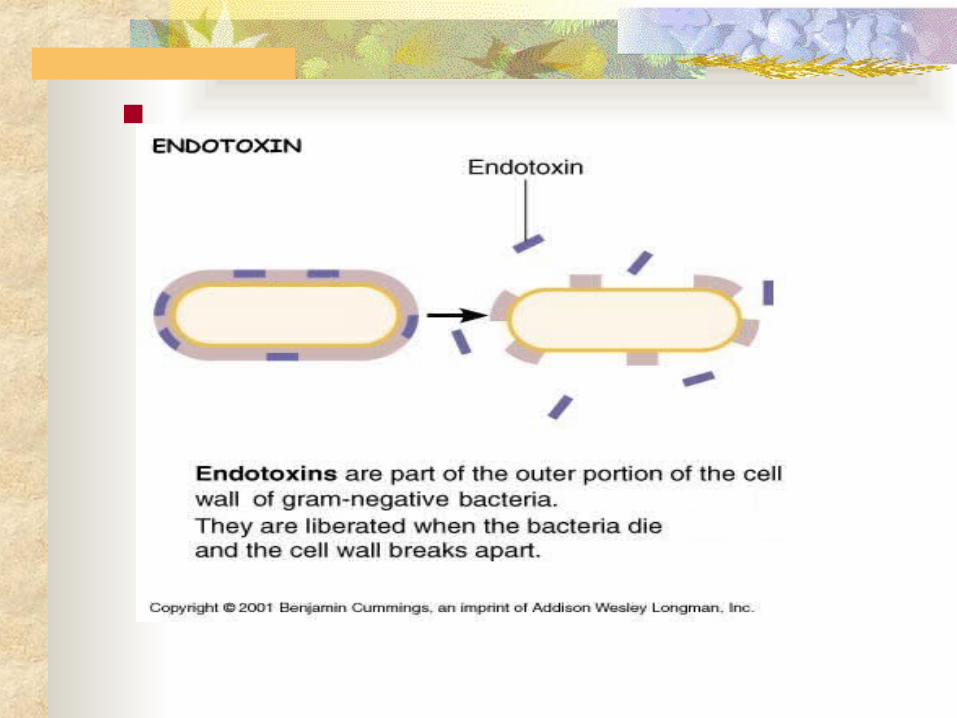
7. ENDOTOXIN – also known as “Lipid A”
a. Found in lipopolysaccharide of Gram – cell wall.
b. Heat resistant.
c. Toxic only in large quantities
d. No toxoid (vaccine) available
e. Limulus test – an industrial Lipid A detection method used by manufacturers of IV fluids. (Came from horsehoe crab)

f. PHYSIOLOGICAL EFFECTS OF LIPID A
In Six Easy Steps! Causes Endotoxic Shock, synonymous with Blood Poisoning, and Sepsis Shock.
1. Originates with lysed Gram – bacteria in blood (bacteremia). Lipid A fragments of Gram - cell wall are scattered throughout cardiovascular system, and becomes lodged in the capillary network of vital organs.
2. Prostaglandins are released by endothelial cells in contact with Gram – bacteria causing vasodilation.
3. Macrophage (MP) phagocytize some Gram – bacteria. MP release IL-1 signals the hypothalamus to produce fever. Fever has 3 benefits: Inactivates bacterial enzymes, hides iron from bacteria, and increases leukocytic infiltration.
4. Neutrophils cannot squeeze through endothelial cells to reach lipid A lodged in basement membrane of capillaries. “Frustrated” neutrophils release digestive enzymes on endothelial cells.

5. On massive scale causes Disseminated Intravascular Coagulation (D.I.C.).
6. Result: Endotoxic Shock. Impaired oxygen exchange in lungs leads to coma, and death. ~ 175,000 deaths per year in the U.S.
7. Diseases that cause Endotoxic Shock:
a. Neisseria meningitidis meningitis
b. Salmonella typhi – typhoid fever
c. Nosocomial infections (cystitis)
Opportunistic Gram - (E. coli)
Application of Pathogenesis: Bioterror
NOVA “Bioterrorism” http://www.pbs.org/wgbh/nova/bioterror/biowarriors.html

Body Defenses Overview 1st line of defense (physical, chemical and
genetic barriers) 2nd line of defense (Inflammation,
Interferons, Phagocytosis) (linked to 3rd) 3rd line of defense (Immune response)

Nonspecific Immunity (Innate) offers general protection from all pathogens.
I. Skin - the largest organ of the body in terms of surface area.
A. Epidermis - outer thin layer contains stratified squamous epithelium. Forms a barrier against most pathogens. Keratinocytes secrete keratin, a type of wax. Most microbiota is located here.
Body Defenses

B.Dermis – skin’s inner thicker part composed of connective tissue made of collagen.
1. Dendritic cells are a type of phagocyte found in the skin derived from monocytes. These cells migrate to the lymph nodes after phagocytosis.
2. Mast cells release histamine during inflammation. Not normally in circulation but in the skin.
3. Suderiferous glands produce sweat. Sweat contains lysozyme and NaCl which inhibits most bacteria except - Staphylococcus epidermidis
4. Sebacous glands produce sebum, an unsaturated fatty acid, lowers skin pH to 4.0.
Body Defenses cont.
GA f 07

Dendritic Cell

Dendritic Cells
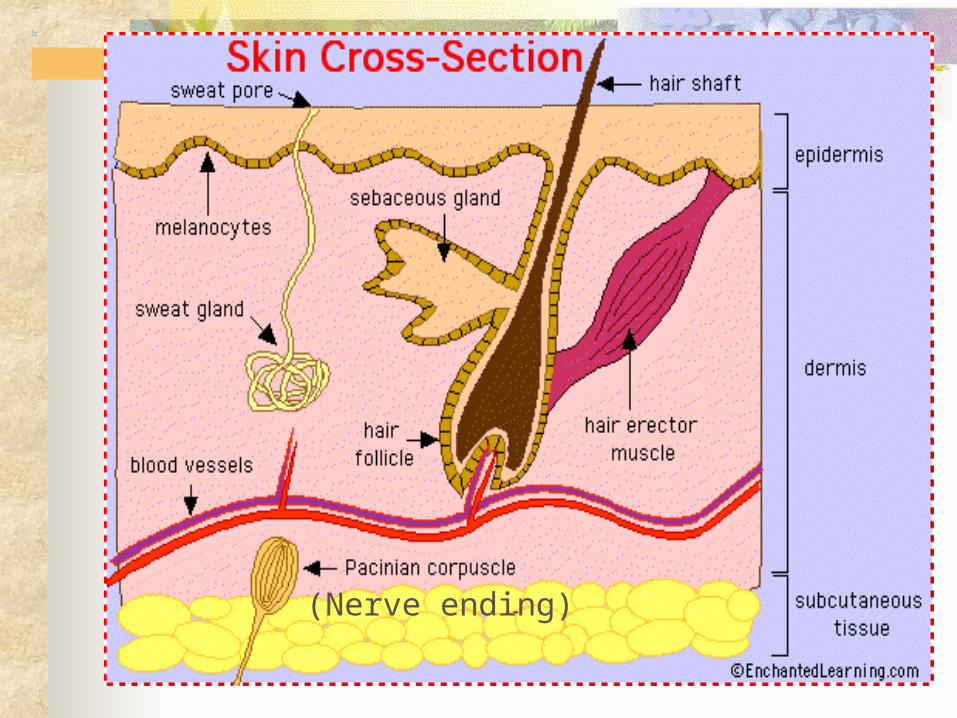
Skin Diagram (Cross Section)
(Nerve ending)

C. Subcutaneous Tissue – mostly the membranes that line the G.I.T., G.U.T., and R.T! 1. Goblet cells secrete mucus. Prevent cells from drying out and cracking. Keeps bacteria flowing over the surface of cells lining tracts of the body. 2. Ciliated columnar cells wave dirt, dust and bacteria out of the body. In the R.T., cilia wave particles up toward the epiglottis where they are swallowed. The "muco-ciliary escalator." 3. Hydrochloric Acid (HCl) pH 1.8 stomach 4. Salivary glands 1 liter of saliva per day.
Bathes teeth with lysozyme (destroys peptidoglycan layer ).
5. Lacrimal glands produce tears, contain lysozyme.
Body Defenses cont.

Mucous membranes
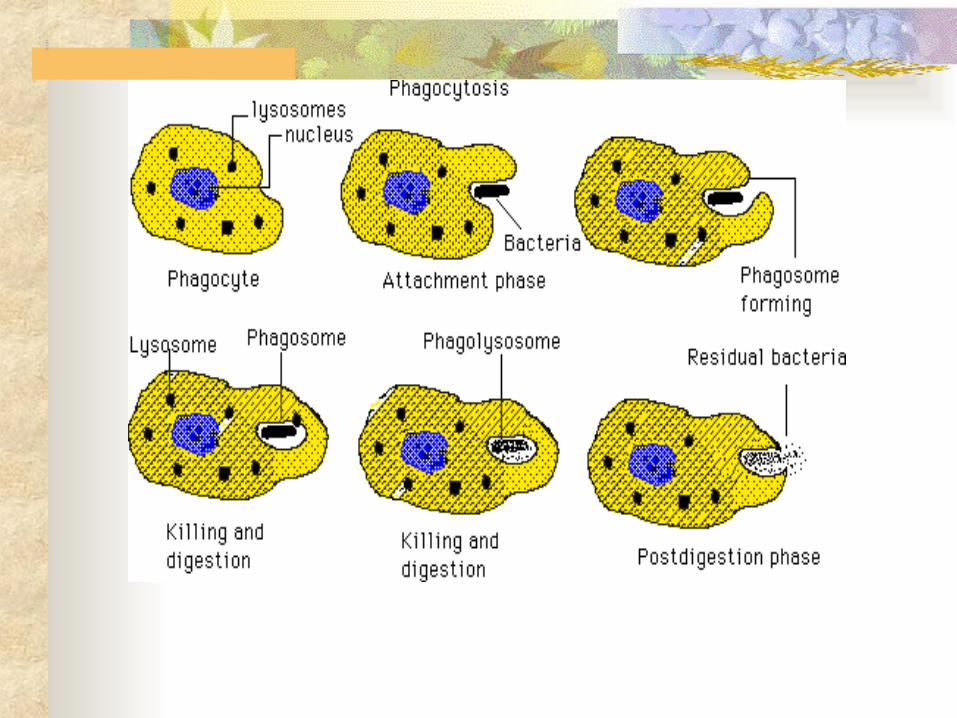
II. Phagocytic System - Phagocytosis (to eat) A. Mechanism Fig. 16.3
1. Chemotaxis - chemical attraction of phagocytes to a microbe.
2. Adherence - attachment 3. Ingestion - pseudopods extend
around microbe. 4. Digestion - the plasma membrane
of a phagocytic cell pinches off into the cell and forms a vacuole (phagosome). Lysosomes fuse
with phagosome. Contain nitric oxide and lysozyme which kills microbes, and digestive enzymes that degrade microbes.
Phagocytic System
Phagocytosis diagram

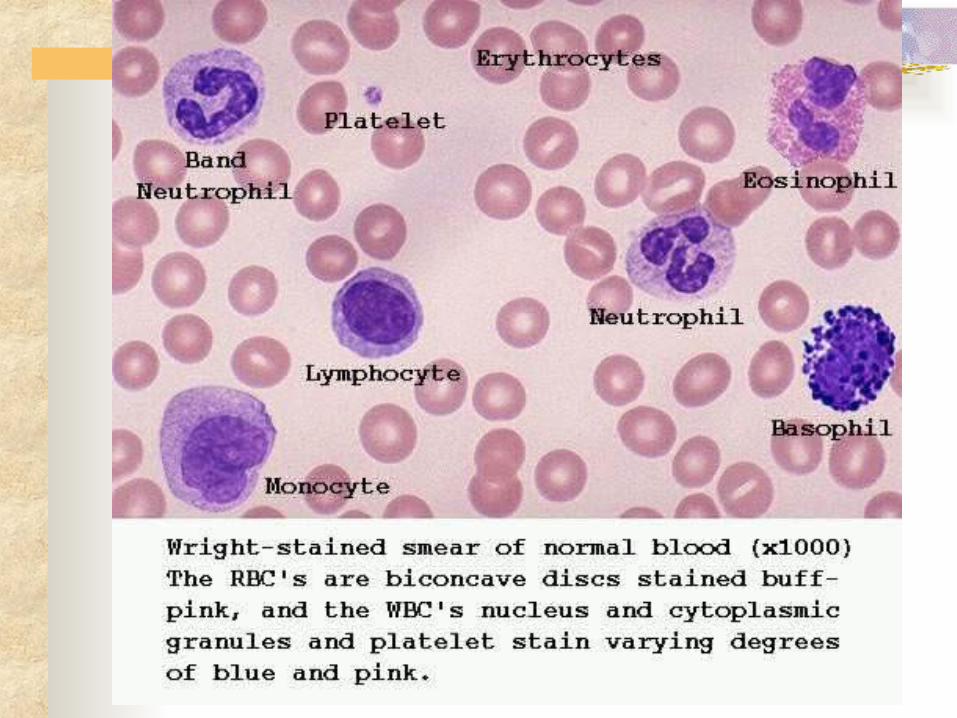
B. Five Types of Leukocytes (wbc’s)- made in the bone marrow (Figure 16.1 p. 448). 3 Granulocytes- with granules in cytoplasm.
1. Neutrophils stain poorly and have 2- 7 nuclei. 1st phagocytes to arrive at site of inflammation. 60% of blood leukoctyes.
2. Eosinophils stain red have 2 nuclei and phagocytize large parasites (protozoans, worms and fungi).2-4%.
3. Basophils stain blue and release histamine during
inflammation. Non- phagocytic. < 1%.
Five Leukocytes
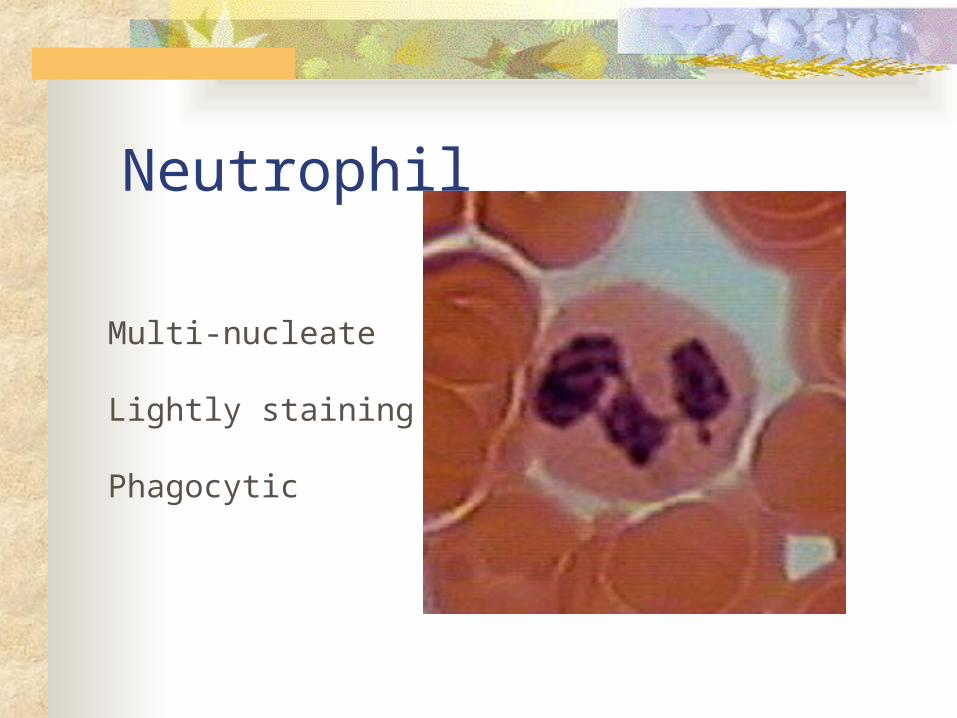
Neutrophil
Multi-nucleate
Lightly staining
Phagocytic
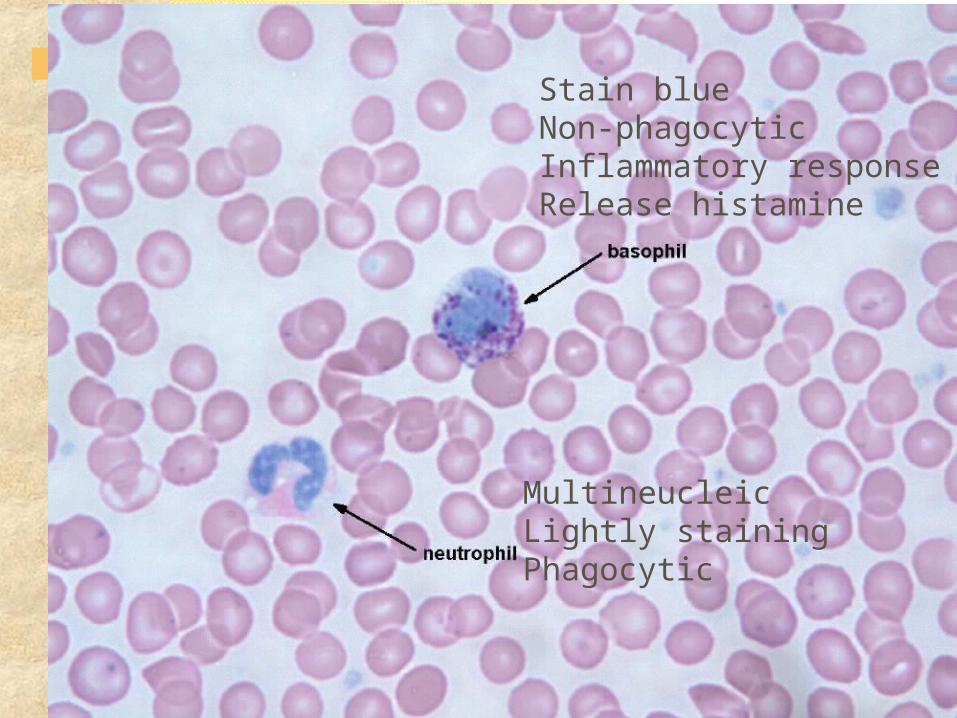
Stain blueNon-phagocyticInflammatory responseRelease histamine
MultineucleicLightly stainingPhagocytic
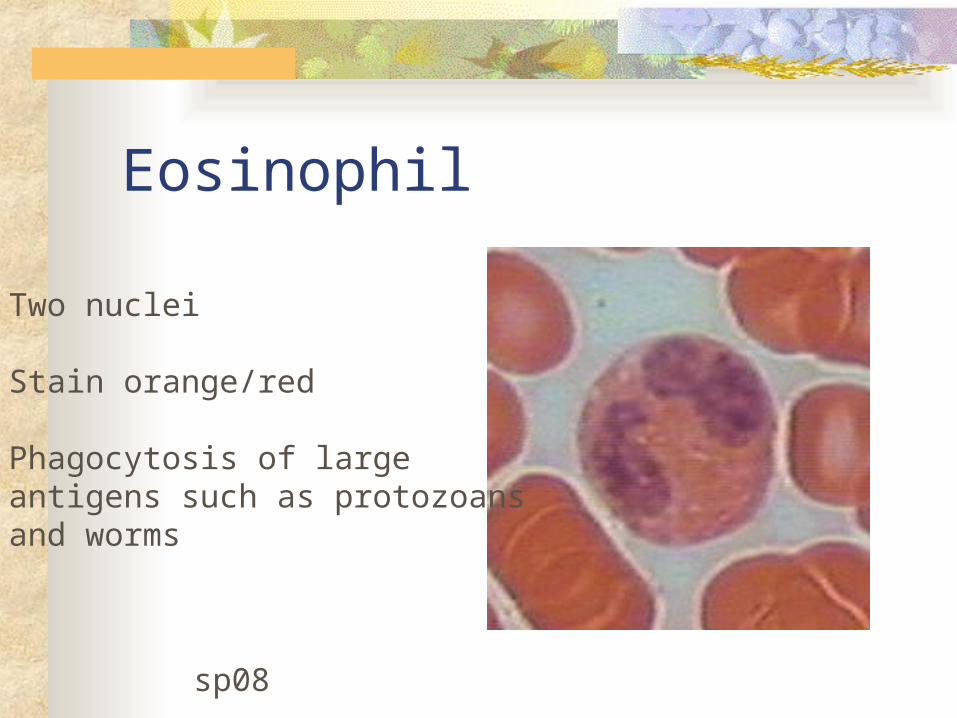
Eosinophil
Two nuclei
Stain orange/red
Phagocytosis of largeantigens such as protozoansand worms
sp08

Two nuclei
Stain orange/red
Phagocytosis of largeantigens

Basophil
Stain darkly (blue)Non-phagocyticInflammatory responseRelease histamine

MonocyteAgranulocyteNotched nucleusBecome macrophages when out of circulation
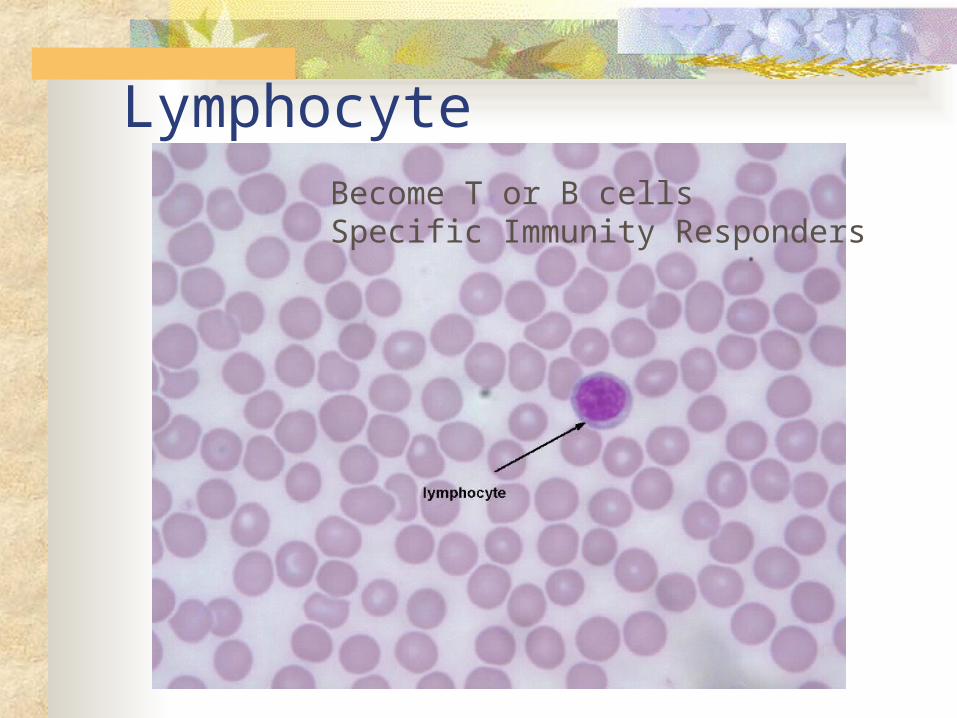
LymphocyteBecome T or B cellsSpecific Immunity Responders
Two Agranulocytes-no granules in cytoplasm. 4. Monocytes --horseshoe shaped nucleus. Largest leukocyte. Migrate out of the circulatory system and wander into any tissue of the body scavenging for foreign substances. If out of the circulation, they are called macrophage (MP). Ingest 100 bacteria at once.
3-8% of all wbc’s in blood.5. Lymphocytes - make up 20% of all
leukocytes. Function in specific immunity. There are basically two types: T cells and B cells. C. Platelets, or thrombocytes, are small
cells that form blood clots.
Agranulocytes (Monocytes & Lymphocytes)
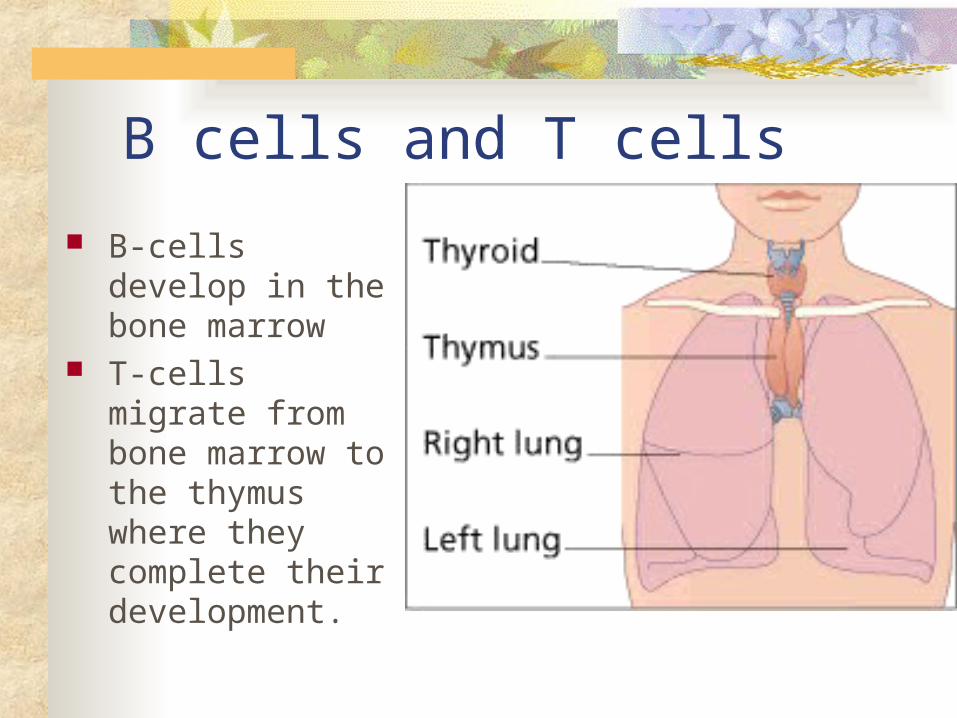
B cells and T cells
B-cells develop in the bone marrow
T-cells migrate from bone marrow to the thymus where they complete their development.

Platelets
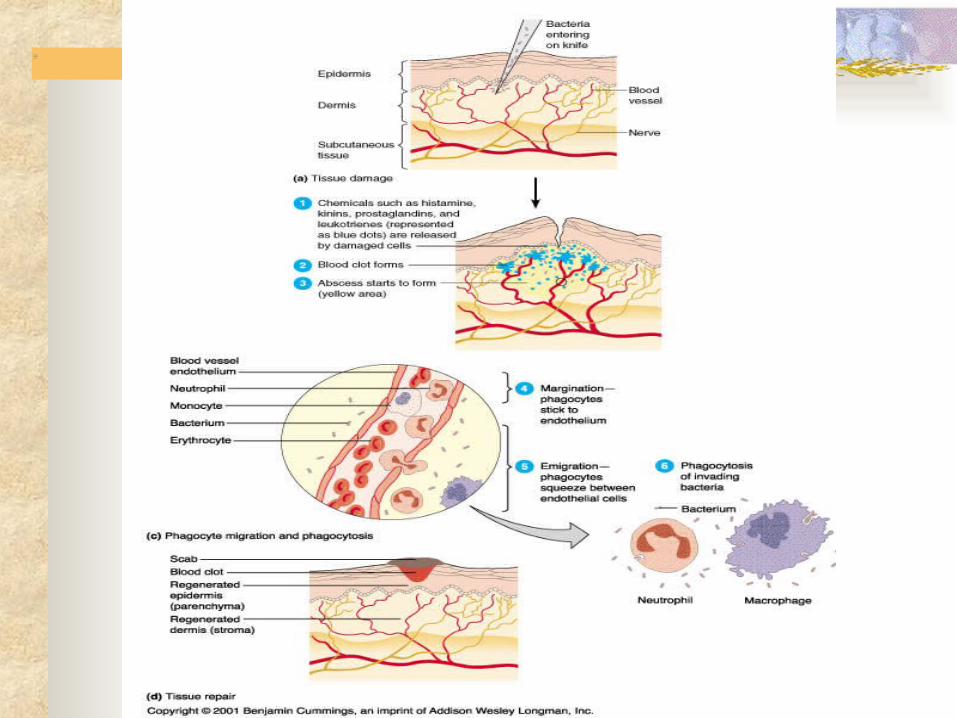
III. Inflammation is a nonspecific host defense mechanism designed to mobilize components to the site of injury, destroy microbes, and set repair processes into motion.
A. 4 Cardinal Signs of Inflammation
1. Rubor - redness or erythema2. Dolar - pain3. Calor - heat4. Halor - swelling, can be fluid
(edema) or cellular (tumor).
Inflammation
Five Patterns of Inflammation
B. 5 Patterns of Inflammation 1. Serous – water blister, mild burns 2. Fibrinous – scar tissue formation 3. Pseudomembrane – new
membrane formed over the old.
4. Suppurative – pus formation, dead neutrophils and target
bacteria within an abscess. 5. Ulcer – crater from inflammed
tissue.C. Inflammatory Response consists of
three phases; Fluid, Cellular, and Healing
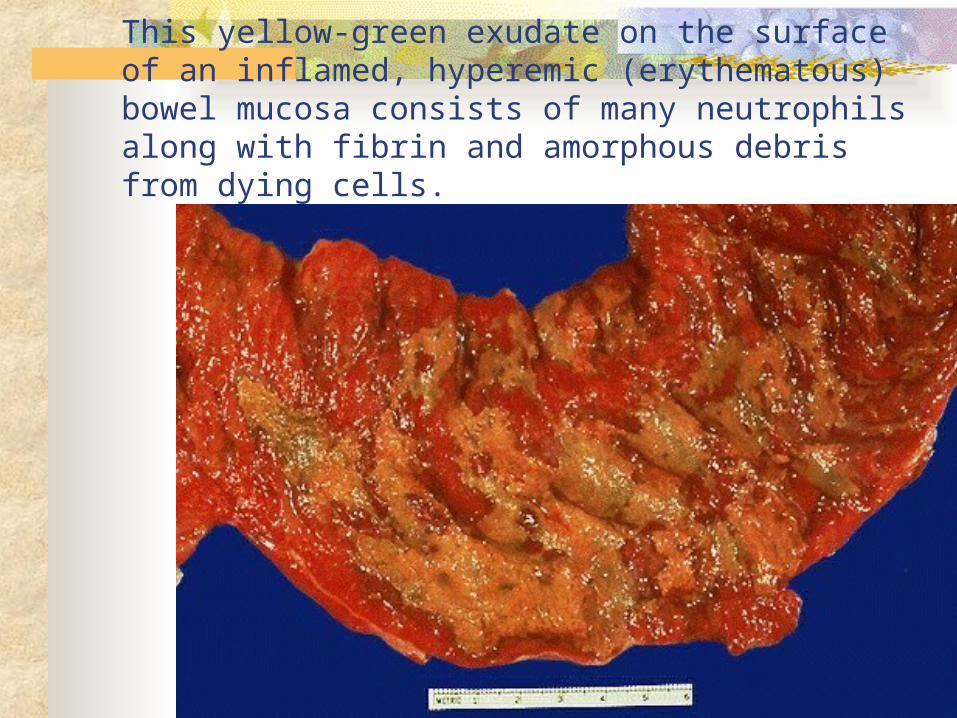
This yellow-green exudate on the surface of an inflamed, hyperemic (erythematous) bowel mucosa consists of many neutrophils along with fibrin and amorphous debris from dying cells.

Here is a purulent exudate in which the exuded fluid also contains a large number of acute inflammatory cells. Thus, the yellowish fluid in this opened pericardial cavity is a purulent exudate.
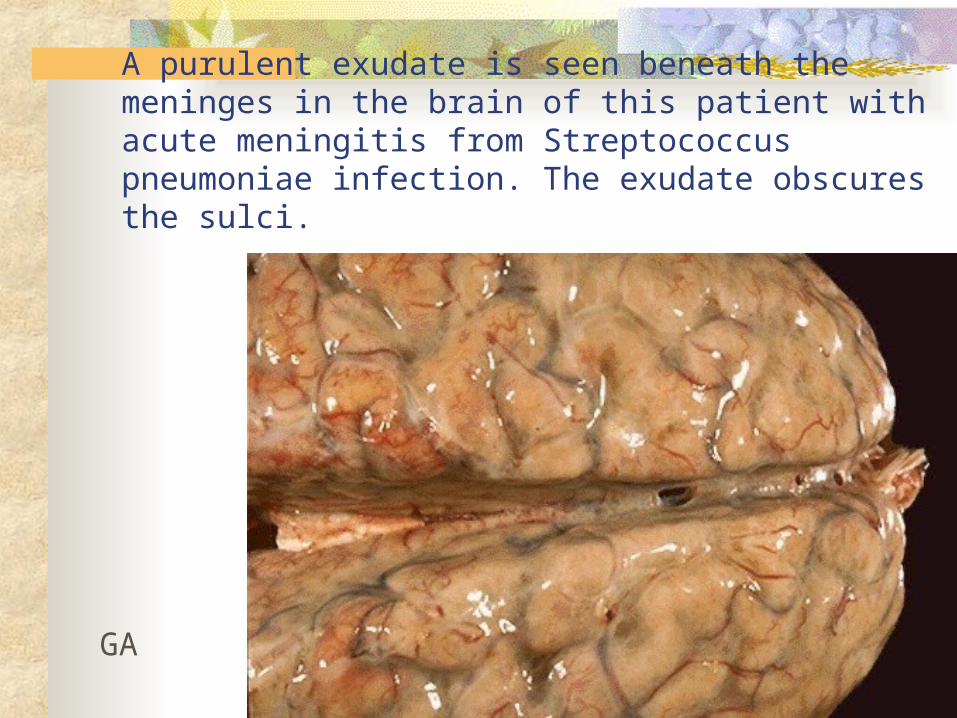
A purulent exudate is seen beneath the meninges in the brain of this patient with acute meningitis from Streptococcus pneumoniae infection. The exudate obscures the sulci.
GA
1. Fluid Phase (Chemical Mediators)
a. Bradykinin produced in kidney, causes pain and vasodilation. (found in bee venom)
b. Histamine-released by mast cells causes vasodilation and smooth muscle contraction. (problem- asthma)
c. Prostaglandin –lipid released by somatic (body) and mast cells, causes vasodilation
d. Heparin - by mast cells, anticoagulant
e. Leukotrienes - by leukocytes, squeezing effect on capillaries +(bronchial constriction)
Fluid Phase
f. Seratonin – released by platelets causes vasodilation.
g. Histamine – released by Basophils.(vasodilation)
h. Complement - consists of 20 serum proteins that bind to antibody in an ordered sequence, or cascade. Pg 462
C3a - interacts with mast cells causes release of histamineC3b - enhances phagocytosis by coating (process called opsonization) C5a - chemotactic for neutrophils
i. LPf - leukocytosis promotion factor by mast cells, chemotactic for neutrophils.
Fluid Phase (cont.)

Compliment Pathway
AttractsNeutrophils
With mast cells releaseHistamine

Complement End Results
Cytolysis

h. Hemostasis - clotting begins within 15-20 seconds if there is a severe cut. and 1-2 minutes if minor. 12 clotting factors found in serum. Activated when they leave the circulatory system.
Ex. Prothrombin -----------> thrombin (in blood) (out of
circulation) thrombin (enzyme)
Ex. Fibrinogen ------------> fibrin (in blood) (out of
circ.) Fibrin enmeshes platelets.These two substances form the clot.
Clotting
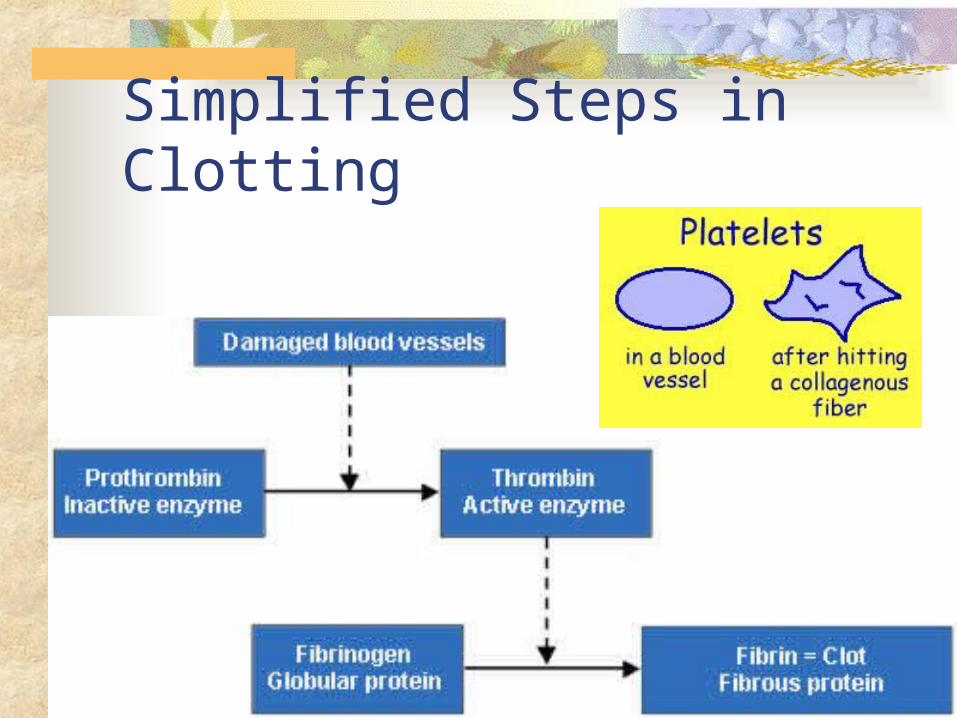
Simplified Steps in Clotting
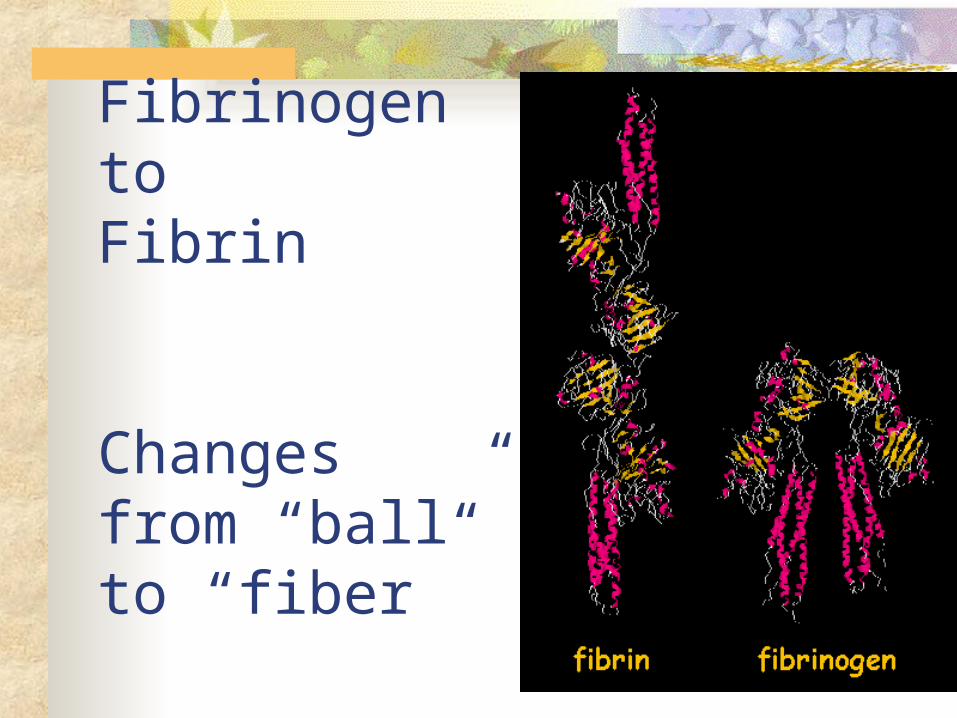
Fibrinogen to Fibrin
Changes from “ball” to “fiber”

2. Cellular Phase - occurs within 1 hour and involves phagocytic cell infiltration. Occurs within an abscess in supparative pattern of inflammation.
a. low pH kills microbesb. macrophages attack escaping microbes c. body temperature increases due to macrophage signaling the hypothalamus with lymphokine (a chemical secreted by white blood cells that regulates the immune response) called IL-1
(interleukin I). Note: Specific Immunity begins here!
Cellular Phase

a. Fibroblast cells produce beta interferon (a lymphokine secreted by cells of the body that regulates the immune response). This chemical signals the immune system to stop.
b. Fibroblasts proliferate and produce collagen fibers.
c. Macrophage also produce collagen.
d. Intact connective tissue reforms.
3. Healing Phase
CytokinesCytokines are chemicals secreted by cells of the body
that regulate the immune response. “Chemical messengers” Cytokines produced by leukocytes are lymphokines.
Wound Infections

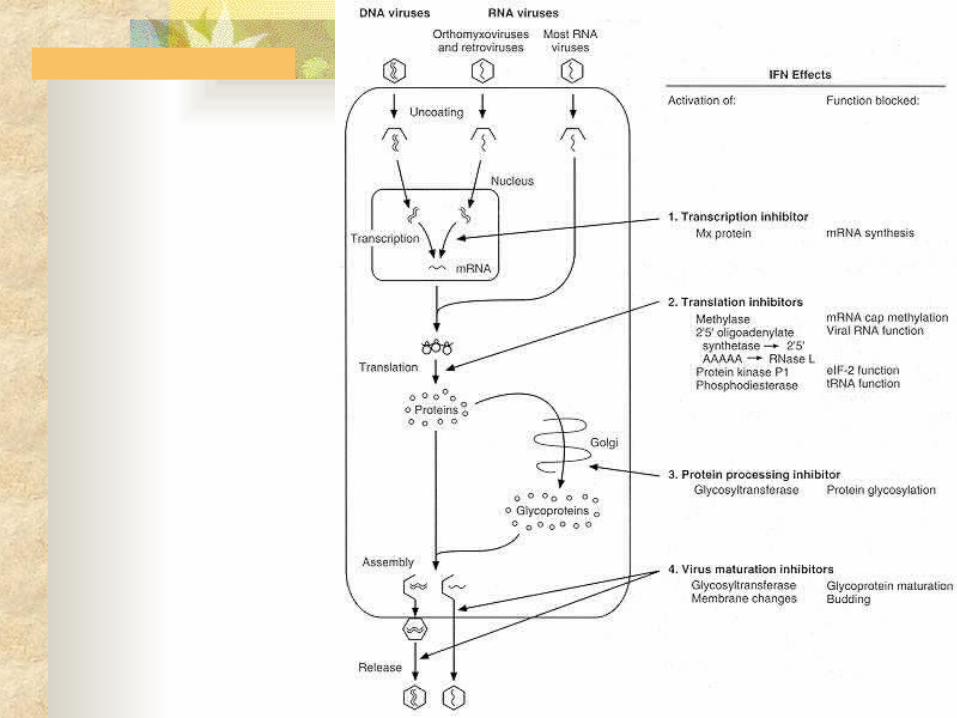
IV.Interferon (abbrev. IFN) Discovered in 1957. A. Beta Interferon - produced by
fibroblasts. Activates T suppressor (TS) cells to end the inflammatory response.
B. Alpha Interferon – viruses trigger neighboring cells to produce antiviral proteins. Used to treat symptoms of ovarian cancer, multiple sclerosis, Kaposi's Sarcoma and HCV.
C. Gamma Interferon - produced by T helper cells (TH1) in response to viruses. Gamma-IFN activates macrophages (MP) and Natural Killer
(NK) cells for specific immunity.
Interferon























![Bioactive Powerpoint Microbes fighting microbes [Read-Only]](https://img.dokumen.tips/doc/110x75/625e85126147534db333a997/bioactive-powerpoint-microbes-fighting-microbes-read-only.jpg)