Embed Size (px)
Citation preview

M I C H E L L E P E A H O TA , P H A R M D , B C P S
Incorporating Rapid Diagnostic Microbiology Testing into
Antimicrobial Stewardship

Objectives
1. Describe recent advancements in microbiology rapid diagnostic testing
2. Review current literature describing the impact of rapid diagnostic testing on antimicrobial stewardship and patient outcomes
3. Evaluate the incorporation of rapid diagnostics into an antimicrobial stewardship program to identify positive blood cultures
Case 1
HPI: MJ is a 68 YO M end stage renal disease (ESRD) on hemodialysis (HD) (MWF) presents to ER from HD clinic after he was noted to have chills, rigors, and a fever of 102.1. In the ER he is lethargic and febrile. The ER sent 2 sets of blood cultures.
PMH: ESRD on HD (HD catheter), Diabetes, Hypertension
Allergy: penicillin (GI upset)
Medications: Insulin glargine, metoprolol, zolpidem prn, docusate, senna
Social history: Denies IVDA, no tobacco, no alcohol

The microbiology lab performed a gram stain and notifies the ER that both sets of MJ’s blood cultures have gram positive cocci in clusters. Which empiric antibiotic should be started?
The microbiology lab set up MJ’s blood cultures on the BioFire FilmArray. The team was notified that the patient’s blood cultures are growing Staphylococcus aureus mecA negative. What (if any) changes should be made to MJ’s antibiotic
regimen?
Case 1

Antimicrobial Stewardship Program (ASP)
ID Physician Clinical Pharmacist Microbiology
Information Systems Specialist
Epidemiologist

Early Antibiotic Administration
Septic shock Acute organ dysfunction secondary to documented or
suspected infection Major health care issue
Effective antimicrobial administration Impact on mortality Timing is important Selection is important
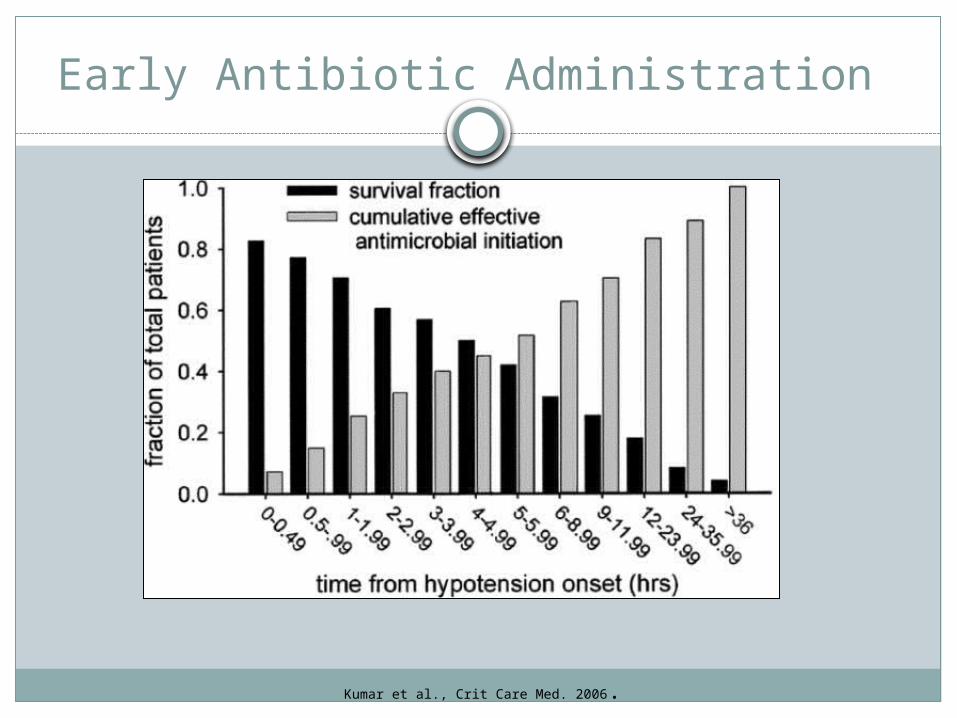
Early Antibiotic Administration
Kumar et al., Crit Care Med. 2006.

Antibiotic Selection
Drug allergies
Patient history
Antimicrobial
ExposureComorbidities
Local susceptibility
patterns
Initial selection should be broad enough to cover all likely pathogens
Empiric therapy should be tailored to local susceptibility patterns
De-escalate when causative pathogen has been identified

Microbiology
Alert of positive culture
Organism identification (ID)
Antimicrobial susceptibility
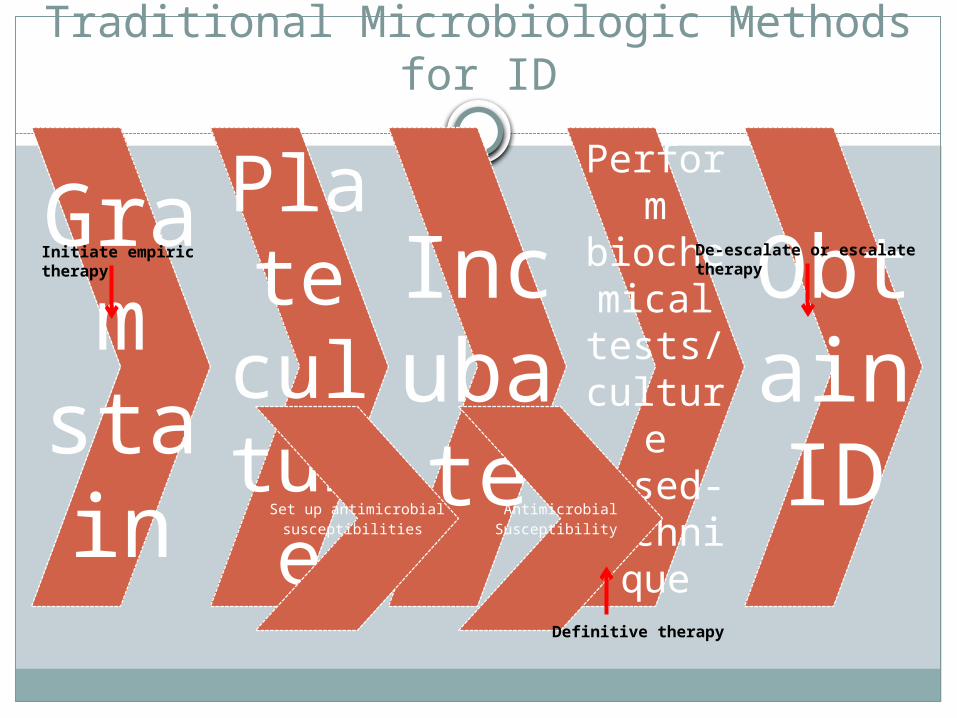
Traditional Microbiologic Methods for ID
Gram
stain
Plate
culture
Incubate
Perform
biochemical
tests/culture
based-techniq
ue
Obtain ID
Set up antimicrobial susceptibilities Antimicrobial Susceptibility
Initiate empiric therapy De-escalate or escalate therapy
Definitive therapy

Time Required to Deliver Routine Bacterial Culture Results
Goff DA, et al. Pharmacother. 2012.

Rapid Molecular Identification Methods
Rapid methods that can deliver results minutes to a few short hours
Several commercially available tests
Enable timely antimicrobial optimization
“Game changer”

Polymerase chain reaction (PCR)
Multiplex PCR
Nanoparticle Probe Technology (Nucleic Acid Extraction and PCR Amplification)
Peptide Nucleic Acid Fluorescent In Situ Hybridization
Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF)
Rapid Molecular Identification Methods

MALDI-TOF
Matrix-assisted laser desorbtion/ionization time-of-flight mass spectrometry
Ability to analyze thousands of samples per day
Multiple sources: blood, respiratory, urine, wound
Identifies bacteria based on unique protein sequences Ionization and disintegration of target molecule Mass/charge ratio analyzed Mass spectrum provides a profile of the organism compared to those of well-
characterized organism in a library
Process ~1 hour

MALDI-TOF

Able to reduce time to organism ID by 24-36 hoursCan not detect resistance mechanisms Limitation in organism ID at species level
Streptococci, Shigella, Propionibacterim
MALDI-TOF

Peptide Nucleic Acid Fluorescent In Situ Hybridization
PNA-FISH
One of the first commercially available rapid diagnostic tests for blood
Synthetic oligonucleotide fluorescence-labeled probes Hybridization to species-specific ribosomal RNA Fluorescence is detected using a fluorescence microscope

Organism detection S. aureus, coagulase-negative staphylococci (CoNS) Enterococci Gram negative rods (Pseudomonas, Klebsiella, E.coli) Candida (C. albicans, glabrata, C. parapsilosis, C. krusei, C.
tropicalis) mecA probe (MRSA)
Peptide Nucleic Acid Fluorescent In Situ Hybridization

Testing time 20 minutes - 2 hours
Robust clinical experience
Limited targets
Limited detection of resistance mechanisms
Peptide Nucleic Acid Fluorescent In Situ Hybridization

Polymerase Chain Reaction
PCR
Uses fluorescent probe with 2 primers
Amplify target DNA
Amplification and detection in 1 process
Multiplex PCR >1 set of primers Simultaneous detection of multiple organism and resistance patterns

Polymerase Chain Reaction (PCR)
https://www.youtube.com/watch?v=0HCWmD7Mv8U

Nucleic Acid Amplification
Utilizes a fluorescently labeled piece of target DNA Use of 2 primers Amplify a piece of target DNA
Amplification and detectionNanosphere VerigeneTM
BioFire FilmArrayTM Blood culture identification (BCID) panel
FilmArray BCID tests for 24 organims Gram positive Gram negative Yeast

BioFire FilmArrayTM
Micro Organism
Gram positive Enterococcus, L. monocytogenes, Staphylococcus, S. aureus, Streptococcus, S. agalactiae, S. pyogenes, S. pneumoniae
Gram Negative Acinetobacter baumanni, Haemophilus influenzae, Nisseria meningitidis, Pseudomonas aeruginosa, Enterobacter cloacae, Escherichia coli, Klebsiella oxytoca, K. pneumoniae, Proteus, Serratia marcescens
Yeast Candida albicans, C. glabrata, C. krusei, C. parapsilosis, C. tropicalis
Antibiotic resistance genes-mecA – methicillin resistance-vanA/B- vancomycin resistance -KPC- carbapenem resistance
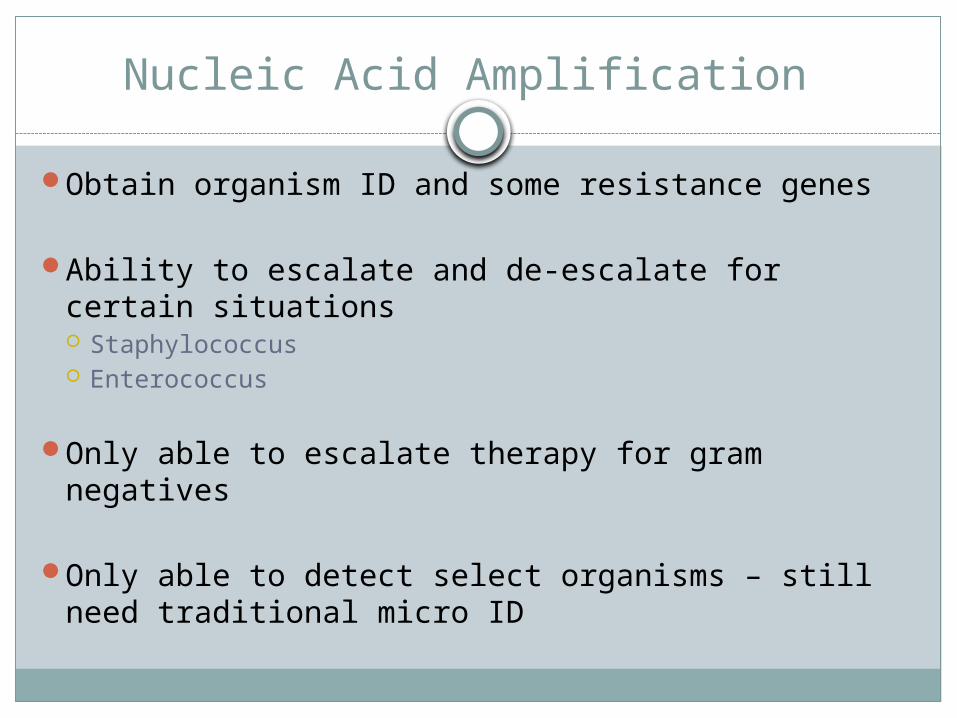
Obtain organism ID and some resistance genes
Ability to escalate and de-escalate for certain situations Staphylococcus Enterococcus
Only able to escalate therapy for gram negatives
Only able to detect select organisms – still need traditional micro ID
Nucleic Acid Amplification

What next?
Action to results Decreased time to ID Decreased time to detection of select resistance genes Opportunity to improve patient care
Timing
S. aureus
MRSA vs. MSSA mecA gene encodes for methicillin resistance (PBP-2a) Vancomycin for MRSA
Vancomycin less active against MSSA than anti-staph β-lactams Increased failure rates Higher risk of relapse
MSSA bacteremia Drug of choice
Nafcillin or oxacillin Cefazolin

Detection of S. aureus bacteremia with PCR and ASP’s Impact
Clinical and economic outcomes
Xpert MRSA kit (Cepheid) and GeneXpert realtime-PCR platform: MRSA vs. MSSA
Single Center study Compared patients with S. aureus bacteremia Intervention arm:
Microlab notified ID pharmacist and treating physician ID pharmacist paged treating physician and communicated lab results and
recommendations Targeted therapy Antibiotic optimization Infectious Diseases Consult
Bauer, et al. CID 2010.

ResultsMean time to switch to optimal antibiotic
Mean time to switch from empiric vancomycin to β-lactam for MSSA decreased by 1.7 days (P=0.002)
LOS 6.2 days shorter (P=0.07)
Hospital costs decreased $21,387 less per patient (P=0.02)
Detection of S. aureus bacteremia with PCR and ASP’s Impact
Bauer, et al. CID 2010.

Coagulase-Negative Staphylococcus
CoNS
Common pathogen associated with hospital-acquired central line infection
Commonly isolated as a contaminant from blood culture Bacteremia vs. contamination
True bacteremia = treat Contaminant = discontinue antibiotics

Impact of ASP Intervention on CoNS Blood Cultures in Conjunction with Rapid Diagnostics
Analyzed the impact of rapid diagnostics with MALDI–TOF plus ASP intervention
Single center, quasiexperimental study Historical control – CoNS identified by conventional methods Intervention – CoNS blood culture ID’ed vial MALDI in
conjunction with ASP intervention
Nagel JL, et al, J Clin Microbiol. 2014.

Impact of ASP Intervention on CoNS Blood Cultures in Conjunction with Rapid Diagnostics
Nagel JL, et al, J Clin Microbiol. 2014.

MALDI ID CoNS quicker than traditional methods (83.4 vs 57 h, P=0.001)
Antibiotics No difference in time to effective therapy Decrease in time to optimal therapy (58.7 vs 34.4h, P=0.03)
Similar LOS, ICU stay, recurrent bacteremia and hospital readmission
Intervention group had lower mortality rate (21.7% vs 3.1%, P=0.023)
Decreased duration of inappropriate antibiotic administration with vancomycin and daptomycin (4.4 vs 3 days, P=0.015)
Impact of ASP Intervention on CoNS Blood Cultures in Conjunction with Rapid Diagnostics

Enterococci
Enterococcal bacteremia is the 4th most common cause of hospital-acquired bacteremia in the US Most common species E. faecium and E. faecalis
Vancomycin resistant enterococci (VRE) Most commonly E. faecium Daptomycin Linezolid
Early appropriate antimicrobial therapy has shown to improve patient outcomes in the ICU

PNA-FISH and Enterococcus
Blood culture with gram positive cocci in chains (GPCC)
PNA-FISH E. faecalis Other enterococci (which include E. faecium) No detection Streptococci
Use information to guide antimicrobial therapy

PNA-FISH for Enterococcal Bacteremia
Quasiexperimental study
Control group E. faecium and E. faecalis
were ID using conventional methods
ASP intervened by clinical factors and final susceptibility
Intervention Group
PNA-FISH ASP intervened at time of
PNA-FISH results
Forrest GN, et al. Antimicrob Agents Chemother. 2008.

PNA-FISH ID E. faecalis 3 days and E. faecium 2.3 days earlier than conventional methods (P<0.001)
Reduction in time to initiating effective therapy (1.3 vs 3.1 days, P<0.001)
Decreased 30 day mortality (26% vs 45%)
PNA-FISH in conjunction with ASP treatment algorithm decreased time to appropriate empiric therapy
Forrest GN, et al. Antimicrob Agents Chemother. 2008.
PNA-FISH and Enterococcus
Integrating Rapid Diagnostics and ASP to Improve Outcomes in Patients with Gram-Negative Bacteremia
Impact of rapid ID (MALDI-TOF) and susceptibility testing coupled with ASP on patients with resistant gram-negative bacteremia
Control group: conventional ID and susceptibility
Intervention group: MALDI ID Simultaneous set up for susceptibility testing Results sent to ASP ASP contacted team to discuss results and provide evidence based
recommendations when appropriate
Perez KK. J Infect. 2014.

MALDI reduced time to ID (40.9±15.1 h to 14.5±12.3 h, P<0.001)
Susceptibility testing (46.7±12.9 h to 29.3±14.7, P<0.001)
Decreased time to optimal antibiotics (80.9±63 h to 23.2 ±19.9 h, P<0.001)
Decreased LOS
Decreased mortality
Decreased hospital costs $26,298 per each bacteremic patient
Perez KK. J Infect. 2014.
Integrating Rapid Diagnostics and ASP to Improve Outcomes in Patients with Gram-Negative Bacteremia

Timeline Comparison
Perez KK. J Infect. 2014.

Rapid Diagnostic Testing in Conjunction with ASP
Case 1
HPI: MJ is a 68 YO M end stage renal disease (ESRD) on hemodialysis (HD) (MWF) presents to ER from HD clinic after he was noted to have chills, rigors, and a fever of 102.1. In the ER he is lethargic and febrile. The ER sent 2 sets of blood cultures.
PMH: ESRD on HD (HD catheter), Diabetes, Hypertension
Allergy: penicillin (GI upset)
Medications: Insulin glargine, metoprolol, docusate, senna, zolpidem prn
Social history: Denies IVDA, no tobacco, no alcohol

The microbiology lab performed a gram stain and notifies the ER that both sets of MJ’s blood cultures have gram positive cocci in clusters. Which empiric antibiotic should be started?
The microbiology lab set up MJ’s blood cultures on the BioFire FilmArray™. The team was notified that the patient’s blood cultures are growing Staphylococcus aureus mecA gene negative What (if any) changes should be made to MJ’s antibiotic
regimen?
Case 1

The microbiology lab performed a gram stain and notifies the ER that both sets of MJ’s blood cultures have gram positive cocci in clusters.
Which antibiotic is most appropriate to start given the available information?
a) Cefazolin
b) Vancomycin
c) Linezolid
d) Cephalexin
Case 1

The microbiology lab performed a gram stain and notifies the ER that both sets of MJ’s blood cultures have gram positive cocci in clusters.
Which antibiotic is most appropriate to start given the available information?
a) Cefazolin
b) Vancomycin
c) Linezolid
d) Cephalexin
Case 1

Case 1
The microbiology lab set up MJ’s blood cultures on the BioFire FilmArray™. The team was notified that the patient’s blood cultures are growing Staphylococcus aureus mecA gene negative
Which antibiotic is most appropriate for MJ’s infection?
a) Cefazolin
b) Vancomycin
c) Linezolid
d) Cephalexin
e) Daptomycin

Case 1
The microbiology lab set up MJ’s blood cultures on the BioFire FilmArray™. The team was notified that the patient’s blood cultures are growing Staphylococcus aureus mecA gene negative
Which antibiotic is most appropriate for MJ’s infection?
a) Cefazolin
b) Vancomycin
c) Linezolid
d) Cephalexin
e) Daptomycin

Case 2
LT is a 30 YO M with no significant PMH presents to the ER with fevers, SOB, and productive cough.
PMH: depression
Allergies: ciprofloxacin (hives/urticaria)
Social History: denies IVDA, +EtOH, no tobacco
Medications: sertraline
CXR: patchy airspace opacities concerning for pneumonia
The ER sent 2 sets of blood and sputum cultures and started IV azithromycin and ceftriaxone for CAP

The lab performed a gram stain and notifies the ER that 1 blood culture bottle has gram positive cocci in clusters on gram stain
The ER added vancomycin to LT’s antibiotic regimen
Case 2
LT is admitted to the observation unit
LT is clinically stable, SOB and cough resolving
Temp 98.9, HR 65 BMP, BP 132/80
WBC 12
Blood cultures: 1 out of 2 sets growing Coagulase negative Staphylococcus (from anaerobic bottle only), repeat blood cultures are negative
Sputum culture: rejected due to poor sample collection
Case 2
Given the available information, what is the most appropriate action?
a) Continue vancomycin IV for 14 days, goal trough 15-20 mg/L
b) Discontinue vancomycin and narrow to cefazolin for 14 days
c) Discontinue vancomycin and discharge patient on oral course of antibiotics for CAP
d) Discontinue vancomycin and start daptomycin since CoNS is likely vancomycin resistant
Case 2

Given the available information, what is the most appropriate action?
a) Continue vancomycin IV for 14 days, goal trough 15-20
b) Discontinue vancomycin and narrow to cefazolin for 14 days
c) Discontinue vancomycin and discharge patient on oral
course of antibiotics for CAP
d) Discontinue vancomycin and start daptomycin since CoNS is likely vancomycin resistant
Case 2

Thomas Jefferson University Hospital
Large academic medical center 951 acute care beds 45,131 admissions per year Wide range of clinical specialties
Microbiology Lab Services 3 hospital campuses Over 10,000 specimens per month ~4,000 blood specimens per month

Thomas Jefferson University Hospital
Antimicrobial stewardship program Prospective audit with feedback and intervention ICU stewardship rounds Treatment guideline development
Infectious Diseases Subcommittee Members include pharmacists, ID physicians, and
microbiologist Drug policy Guidelines

MALDI-TOF Direct from blood Urine Sputum Tissue
Biofire FilmArray Direct from blood
Rapid Diagnostic Testing at TJUH
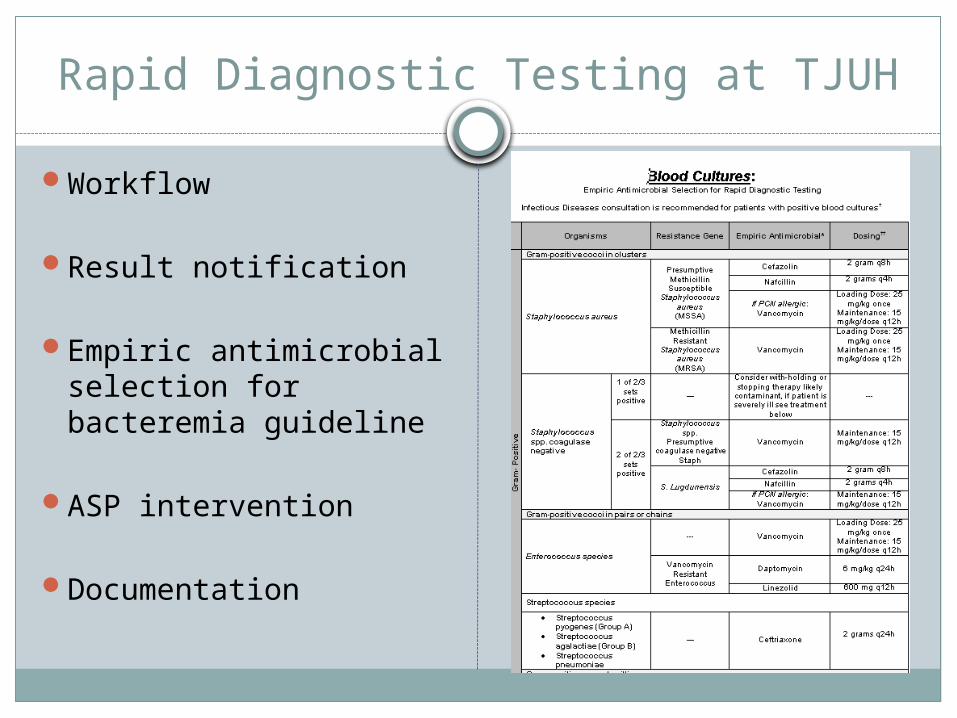
Workflow
Result notification
Empiric antimicrobial selection for bacteremia guideline
ASP intervention
Documentation
Rapid Diagnostic Testing at TJUH
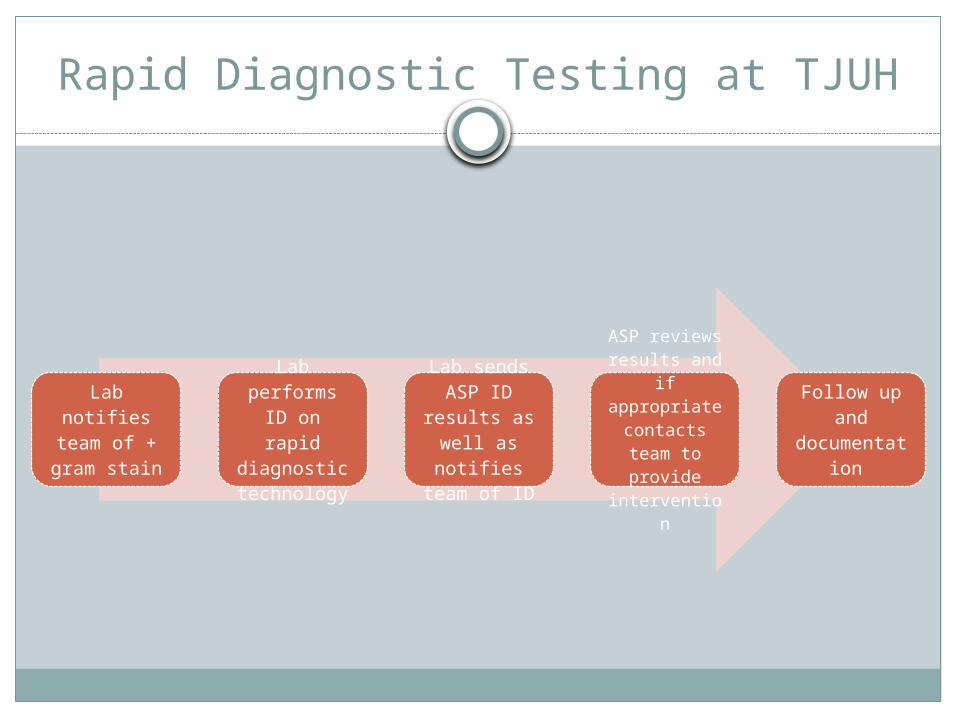
Rapid Diagnostic Testing at TJUH
Lab notifies team of +
gram stain
Lab performs ID on rapid diagnostic
technology
Lab sends ASP ID
results as well as notifies team of ID
ASP reviews results and if appropriate
contacts team to provide
intervention
Follow up and documentatio
n

TJUH Future Directives
Bacteremia bundles
Data collection
Outcomes research
Economic impact evaluation

Conclusion
Timely administration of optimal antimicrobial therapy is essential to improving patient outcomes
Rapid diagnostic testing in conjunction with ASP efforts have demonstrated positive results
New technologies in combination with ASP will likely continue to demonstrate improvements in antimicrobial use and patient care

References
1. Dellit T, Owens R, McGowan J, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. CID. 2007;44:159-77.
2. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006; 34:1589-96.
3. Goff DA, Jankowski C, Tenover FC. Using rapid diagnostic tests to optimize antimicrobial selection in antimicrobial stewardship programs. Pharmacother. 2012;32(8):677-87.
4. Bauer KA, West JE, Balada-Llasat JM, et al. An antimicrobial stewardship program’s impact with rapid polymerase chain reaction methicillin-resistant Satphylococcus aureus/S. aureus blood culture test in patients with S. aureus bacteremia. Clin Infect Dis. 2010;51:10174-80.
5. Nagel JL, Huang AM, Kunapuli A, et al. Impact of antimicrobial stewardship intervention on Coagulase-Negative Staphylococcus Blood Cultures in Conjunction with Rapid Diagnostic Testing. J Clin Microbiol. 2014;52(8):2849-54.
6. Forrest GN, Roghmann MC, Toombs LS, et al. Peptide nucleic acid fluorescent in situ hybridiazation for hospital-aquired enterococcal bacteremia: delivering earlier effective antimicrobial therapy. Antimicrob Agents Chemother. 2008; 52:3558-63.
7. Perez KK, Olsen RJ, Musick WL, et al. Integrating rapid pathogen identification and antimicrobial stewardship improves outcomes in patients with antibiotic resistant gram-negative bacteremia.
8. Wong JR, Bauer KA, Mangino JE, et al. Antimicrobials tewardship pharmacist interventions for coagulase-negative staphylococcus positive blood cultures using rapid polymerase chain reaction. Ann Pharmacother. 2012;46:1484-90.

![Teresa M. [Breslin] DeLellis, PharmD, BCPS, BCGPatomalliance.org/.../2019/01/DeLellis_CV_11_2018.pdf · DeLellis 1 Teresa M. [Breslin] DeLellis, PharmD, BCPS, BCGP 1021 Woodland Pass](https://img.dokumen.tips/doc/110x75/5fba322bc915c30e9e04ab57/teresa-m-breslin-delellis-pharmd-bcps-delellis-1-teresa-m-breslin-delellis.jpg)



























