Embed Size (px)
Citation preview
Michael Holden FRPharmSNPA Chief Executive
Pharmacy and Public Health Forum
• Background• Healthy Living Pharmacy• National Roll-out• Evaluation outcomes


Community Pharmacy
• Over 11,000 community pharmacies in England
• 99% of the population can get to a pharmacy within 20min by car
• 96% by walking or using public transport
• Estimated 1.6 million visits a day
• Average 14 visits per year


PATIENT and
PUBLIC
Self care & Healthy lifestyle interventions
Making Every Contact Count
Medicines Optimisation

Why use pharmacy?

Healthy Living Pharmacy backgroundApril 2008
June 2009
Sept 2010
March 2011
April 2013

Consistently delivers broad range of high quality commissioned services
Quality, innovation and productivity
Proactive team ethos
Health Champion
Identifiable
What distinguishes a Healthy Living Pharmacy?

Key question
Can the results seen in Portsmouth be replicated elsewhere with different demography and
geography?

National roll-out

National roll-out
• Pathfinder Support Group – all pharmacy organisations
• Generate evidence and further develop the concept
• Pharmacy and Public Health Forum HLP task group• Influencing policy
– NHS Plan 2010-2015– Public Health White Paper– Respiratory Strategy– NHS Future Forum report– Public Health Workforce Development consultation
Evaluation aims
• Is there better uptake and delivery of services in HLPs compared to baseline (i.e. before being an HLP or against other non-HLP pharmacies)?
• Does geography and demography impact on HLP performance?
• What is the effect of HLP services on public-reported experiences?
• What are the benefits of HLP for public, commissioner, contractor, employees?
• Is each individual service delivered through HLP cost-effective?
Service evaluation

Service outcomes: overall

Service outcomes: stop smoking

Service outcomes: sexual health
• Buckinghamshire:– Pre-HLP, 75% of EHC through pharmacy– Post-HLP, 86% through pharmacy– Increase in condom distribution by 13%– Increase in Chlamydia screening discussion by 6%
• Stoke on Trent: – Increase in EHC consultations from 1600 to 1848– 29% increase in chlamydia screening
• East Riding and Hull– Average EHC consultations in HLP 123, non-HLP 73 – Increased condom distribution (22.6% vs. 16.1%)
• Portsmouth– Average EHC consultations in HLP 160, non-HLP 85
19

Service outcomes: alcohol awareness
• Dudley– 55 interventions prior to HLP; 280 after
• Milton Keynes– Non-HLP 31 per pharmacy– Working towards HLP 38 per pharmacy– HLPs 59 per pharmacy
• Portsmouth– Non-HLP 90 per pharmacy– HLPs 218 per pharmacy
20

Service outcomes: alcohol awareness
• Pharmacy London initiative– 24,000 scratch cards– >43% high risk
21
Service outcomes: Substance misuse
• Blackburn with Darwen and East Lancs– 328 interactions over 4 months
• 35.7% made by pharmacist• 26.8% made by Health Champion• 20% counter assistants• 13% technicians
– 60% clients signposted to other services• 34.5% to pharmacist• 10.1% to NHS dentist
– 72% of advice was for needle exchange
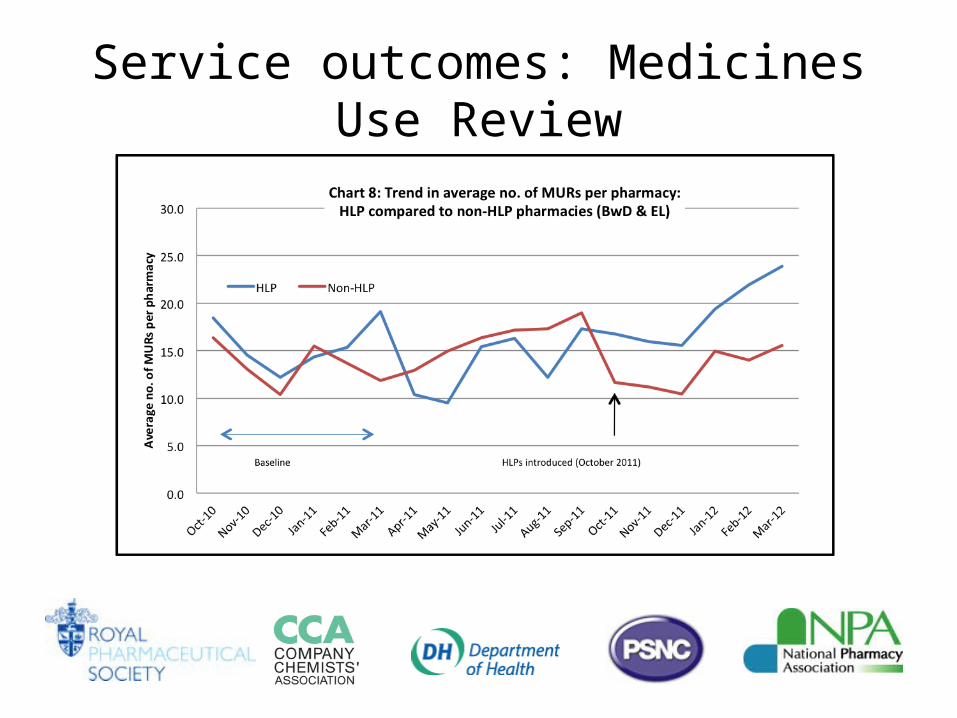
Service outcomes: Medicines Use Review

Service outcomes: New Medicine Service

Cost effectiveness
Cost effectiveness• Contractor survey gives rich insight into how PH services are delivered• Evaluation has affirmed important role of non-pharmacist staff in delivery• Clear evidence that pharmacy staff are engaged and enthused by
opportunities to make a difference; potential to spill over to better service outcomes
• Stop smoking services delivered by non-pharmacist staff perform at least as well as pharmacists– Service can be delivered more effectively i.e. making best use of each staff
member’s skills– And more cost effectively i.e. pharmacist’s time has a higher business cost– Academic evidence shows that stop smoking services are cost effective
Making optimal use of each staff member’s time, without necessarily risking ability to generate positive health outcomes, indicates the potential of service delivery in the HLP context

Public reported experiences

Public satisfaction (n = 1034)
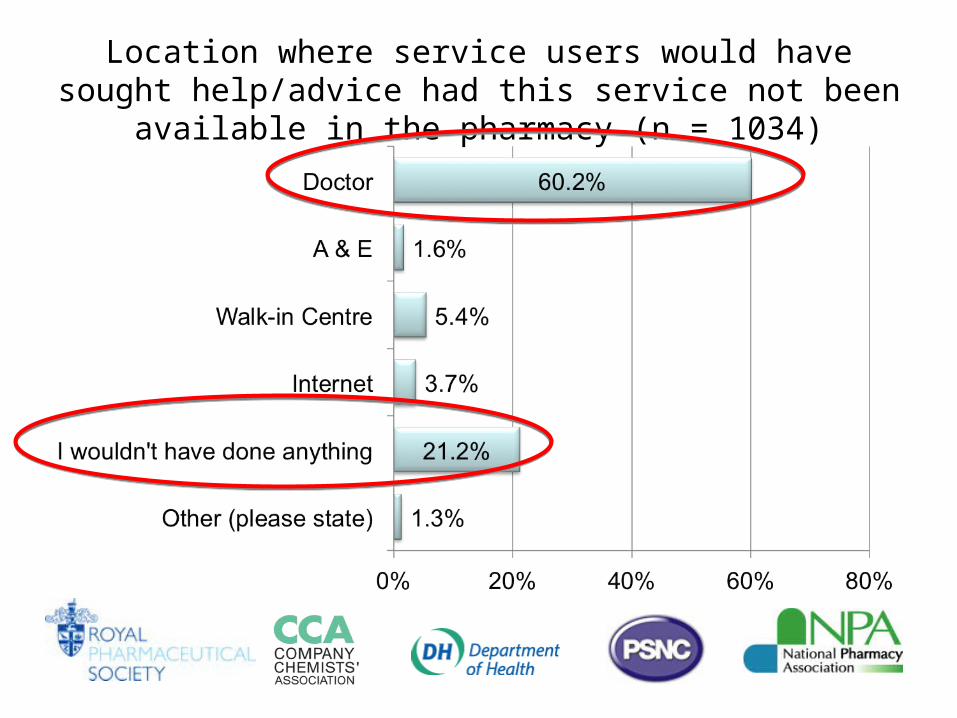
Location where service users would have sought help/advice had this service not been available in the pharmacy (n = 1034)
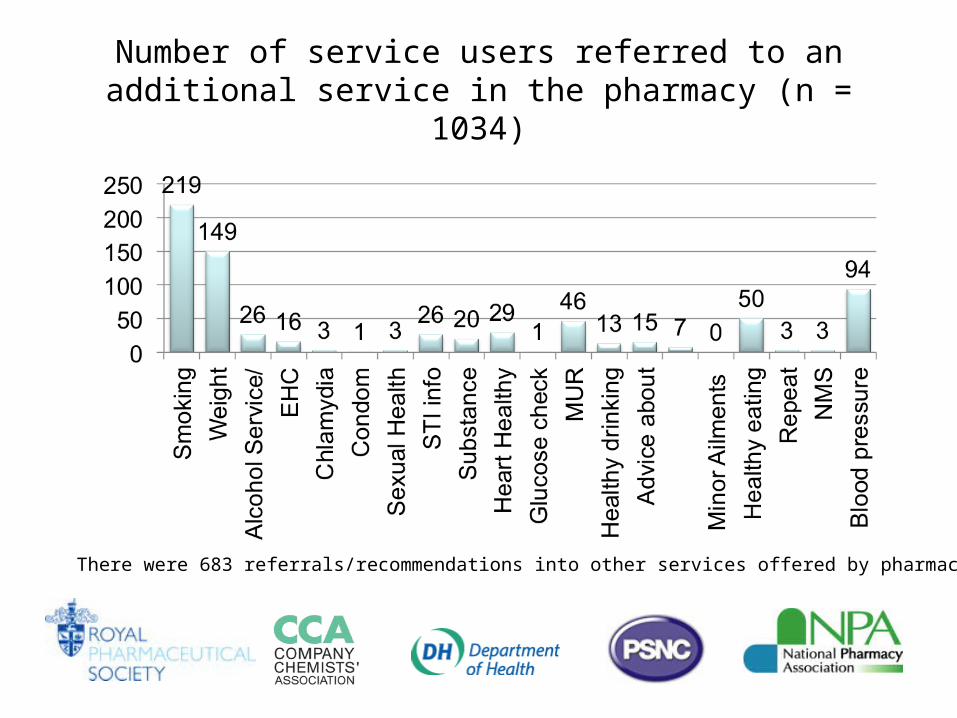
Number of service users referred to an additional service in the pharmacy (n = 1034)
There were 683 referrals/recommendations into other services offered by pharmacy.

Commissioners’ views
• “Becoming an HLP will display to commissioners pharmacy’s commitment to delivering cost effective and high quality services” [Birmingham tPCT and Solihull]
• “Future commissioning can be targeted and offered to those pharmacies that we know will deliver. So this has become a great organisational tool to target commissioning more cost effectively” [Portsmouth]
• “Public health commissioners see the HLP initiative in a very positive manner, public health teams are now keen to involve community pharmacies and in particular the HLPs in their service developments. They have volunteered to give on-going training to HLCs re information and signposting” [Dudley]

What made the difference?


The Enablers
Quality Criteria

2000+ qualified Health Champions
1400+ leadership development
500+ Healthy Living Pharmacies

What next?

Recommendations • Continued local and national support and leadership• Potential link with national contract• Recognition of HLP status by local commissioners• National consistency and quality assurance of HLP status• Consideration for establishment of national awarding body• National service frameworks• Common performance measures including public reported experiences• Resources to support pharmacists and their teams• Workforce development• Consideration for extending role e.g. Dementia, early detection of cancers

Summary
• Provides a commissioning framework
• Is an organisational development tool
• Is a Quality mark
• Is about the pharmacy team
• Has a common vision & goal
• Has a brand the public can
recognise
• Is a means to the end