Embed Size (px)
Citation preview
![Page 1: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/1.jpg)
6Prodrugs Designed to Target Transporters for Oral Drug DeliveryMark S. Warren and Jarkko Rautio
6.1Introduction
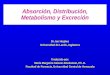
In drug discovery, many drug candidates show effective therapeutic promise but aredropped prior to development because they do not possess the optimal physiochemi-cal properties needed to overcome biological barriers. For orally administered drugs,the intestinal epithelial cells constitute the principal barrier that limits uptake andbioavailability (Figure 6.1). These cells form tight junctions that limit the paracellularflux of drug molecules. In addition, a variety of efflux pumps, such as P-glycoproteinandseveralmultidrug-resistanceproteins intheABCtransporter family,areexpressedon the apical side of these epithelial cells, limiting uptake into these epithelial cells. Inorder for a drug to be well absorbed from the gastrointestinal tract, researchers havetraditionally focused on optimizing the physiochemical properties that allow it topermeate the epithelial cells by transcellular diffusion [1]. One way this can beaccomplished is by masking polar and/or ionizable functional groups with lipophilicmoieties, increasing passive diffusion while trying to avoid recognition by biologicalprocesses such as metabolizing enzymes and efflux transporters [61]. However, thepharmacokinetic properties of drugs are also partly determined by their interactionwith transporters, both efflux pumps that remove them from cells and solute carriersthat expedite their transport into cells.Many nutrients are recognized and absorbed bymembrane transporters expressed by the epithelial cells of the GI tract [2]. Instead oftrying to avoid recognition by these transporters, onemay be able to take advantage ofthem. Drug analogues or prodrugs that are targeted toward these transporters may beable to significantly enhance the absorption of poorly permeating therapeutic agents.
6.2Serendipity: An Actively Transported Prodrug
The antiviral drug acyclovir (2) was approved as an oral medication in 1985, althoughit suffered from limited and variable oral bioavailability due to its high polarity. In
Prodrugs and Targeted Delivery: Towards Better ADME Properties. Edited by Jarkko RautioCopyright � 2011 WILEY-VCH Verlag GmbH & Co. KGaA, WeinheimISBN: 978-3-527-32603-7
j133
![Page 2: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/2.jpg)
Transcellularlipophilicdiffusion
Paracellularhydrophilicdiffusion
Transporter‐mediatedtransport
Efflux�transport
Receptor-mediatedtransport
Lumen�(Apical)
Cellularbarrier
Basolateral
Figure 6.1 Drug transport routes across the intestinal epithelial cell monolayer.
order to circumvent these problems, Beauchamp et al. synthesized and tested 18amino acid esters of acyclovir as potential prodrugs [3]. None of these esters showedmore activity than the parent compound using in vitro antiviral assays against herpessimplex virus type 1.However, whenorally administered to rats, 10 of the compoundsproduced greater amounts of acyclovir in rat urine than the parent compound itself.Their quest to create a prodrug was thus successful: 10 compounds that had no orlimited activity until they had been absorbed and converted to the active phosphor-ylated species in vivo. The L-valyl ester (1) was shown to be the best prodrug of thegroup, with 63% of the administered dose excreted as acyclovir in the urine –
a considerable improvement over the 19% observed for acyclovir itself. Since thisL-valyl ester prodrug of acyclovir was shown to be stable in aqueous solutions, theauthors concluded that the conversion of acyclovir was likely enzyme catalyzed.Clinical evaluation showed that this prodrug (valacyclovir) also had three to five timeshigher systemic availability compared to acyclovir in humans [4]. After clinicalevaluation, valacyclovir was approved as an oral medication and is used for thetreatment of several viral infections. Although the original goal of this studywasmostlikely to simply improve the bioavailability of acyclovir by creating a prodrug withgreater passive permeability, these researchers had, by serendipity, created a prodrugthat was actively absorbed in the intestine.
Further evaluation of the amino acid esters of acyclovir showed that the L-aminoacids were better prodrugs than either the D-amino acids or mixtures of the D- andL-isomers, suggesting the involvement of a stereoselective transporter [3]. It was latersuggested that human peptide transporter 1 (hPEPT1)-mediated uptake of valacy-clovir into intestinal cells could be the underlying mechanism for this elevatedabsorption [5].Other reports suggested thatmultiplemembrane transporters, includ-ing PEPT1, could be involved in valacyclovir uptake [6], and the transport kinetics ofvalacyclovir were concentration dependent and saturable [7]. However, these studiesused rat tissue or Caco-2 cells, where numerous transporters potentially involved invalacyclovir transport are found.Moredefinitive studiesusingChinesehamster ovary(CHO) cells transfected with hPEPT1 followed, providing direct evidence that (1)valacyclovir uptakewas higher in hPEPT1-transfectedCHOcells than in control cells;(2) valacyclovir uptake was concentration dependent and saturable with a Michae-lis–Menten constant around 1mM; and (3) known PEPT1 substrates, such as variousdipeptides and b-lactam antibiotics, could block valacyclovir uptake [8, 9]. Afterabsorption, valacyclovir is then hydrolyzed to acyclovir by �human valacyclovirase,�an alpha-amino acid ester hydrolase capable of activating valacyclovir and other
134j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 3: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/3.jpg)
prodrugs [10, 11]. Furthermore, acyclovir is converted to its active phosphorylatedform (3) by various kinases, thus being a prodrug in its own right.
HN
N
N
NH2N
O
OO
O
NH2
HN
N
N
NH2N
O
OOH
HN
N
N
NH2N
O
OO-P-P-P
Phosphorylation by kinasesHydrolysis
Valacyclovir (1)Substrate of PEPT1
Oral bioavailability 3-5 fold higher than acyclovir
Acyclovir (2)Not substrate of PEPT1
Active triphosphorylated form (3)
6.3Requirements for Actively Transported Prodrugs
Although valacyclovir was not necessarily designed to take advantage of activetransport mechanisms, it did raise the possibility of using such mechanisms indrug design. Indeed, it has been shown in many cases that it is possible to improveoral absorption substantially by chemicallymodifying the drug to forma prodrug thatcan act as a substrate for a known transport system. This is particularly important forpolar or charged drugs that may have negligible passive absorption.
Obviously, not every transporter is suitable for prodrug uptake. Transporters thatare optimal for prodrug uptake have several properties: First, transporters used fororally administered prodrugsmust be expressed in the gastrointestinal tract. Second,the transporter must not be too specific in its recognition of substrates; otherwise itwould be very difficult to design prodrugs that could be recognized. In addition, thetransporter should be expressed at relatively high levels in order to facilitate rapiddrug uptake. Finally, the candidate transporter should have a relatively high capacityin order to avoid being inhibited by an excess of prodrug molecules, which couldblock uptake of the normal nutrients recognized by that transporter. Fortunately,several different classes of transporters appear to satisfy all of these criteria andmanyof them have successfully been used (either by design or by serendipity) to enhancethe uptake of prodrugs. Examples of uptake transporters found in the intestine areprovided in Table 6.1.
In this chapter, only uptake transporters that have been active prodrug targets, forexample, peptide,monocarboxylate, and bile acid transporters, are discussed inmoredetail.
6.4Peptide Transporters: PEPT1 and PEPT2
Members of the oligopeptide transporter family (SLC15) mediate proton-coupledcotransport of many diverse peptide and peptidomimetic substrates. Well-characterized familymembers are PEPT1 (SLC15A1) and PEPT2 (SLC15A2). PEPT1
6.4 Peptide Transporters: PEPT1 and PEPT2 j135
![Page 4: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/4.jpg)
is highly expressed in the absorptive cells of the intestinal epithelium, whereas cellsof the renal epithelium express predominantly PEPT2 and also PEPT1. Bothtransporters have been cloned in mammals [12, 13], but their three-dimensionalstructure has not been elucidated due to the difficulty in purifying and crystallizingmembrane proteins. Therefore, the structural requirements for molecular recog-nition have been based both on uptake or transport studies and on computationalmodeling. Both transporters differ in their substrate specificity, affinity, andtransport capacity.
The intestinal PEPT1 is perhaps the drug transporter that has captured the mostrecent attention in oral drug delivery. The expression of PEPT1 increases from theduodenum to the ileum [14], and at the villus level ismore abundant at the tip. Almostall 400 dipeptides and 8000 tripeptides derived from the common protein-formingamino acids, but not free amino acids or peptides with more than 3 amino acidresidues, are substrates for PEPT1. A detailed characterization of its substrates hasbeen performed [15], demonstrating that it has a particular affinity for molecules inwhich the amino and carboxylic acid groups are separated by about 6A
�, even in
nonpeptidic substrates. The PEPT1 substrate recognition site is proposed to have thefollowing characteristics: (1) a strong binding site for N-terminal NH3
þ , (2) ahydrogen bond to the carbonyl group of the first peptide bond, (3) a carboxylatebinding site, and (4) a hydrophobic pocket for the side chain of an amino acid(Figure 6.2). Moreover, PEPT1 is stereospecific and it prefers L-L-di- and L-L-L-tripeptides over their D-enantiomers.
Comparatively, PEPT1 is considered a low-affinity (Km of 200 mM–10mM), high-capacity transporter, while PEPT2 has higher substrate affinity (Km of 5–500 mM) andlower transport capacity. Taken together, peptide transporters are capable of medi-ating the transport of a huge variety of molecules, from endogenous peptides tovarious therapeutic drugs, including nonpeptidyl drugs, with a large diversity ofphysicochemical properties (Figure 6.3). The substrates of peptide transportersinclude several b-lactam antibiotics, angiotensin-converting enzyme inhibitors suchas captopril, enalapril, and fosinopril, as well as bestatin and antibacterial peptideanalogues such as alafosfalin. Even compounds without an obvious peptide bond,
Table 6.1 Uptake transporters affecting intestinal absorption of drugs and their representative drugsubstrates.
Transporter Examples of drugs with active uptake transport
Oligopeptide transporter (PEPT1) ACE inhibitors (e.g., captopril, enalapril, and fosinopril),b-lactam antibiotics (e.g., penicillins andcephalosporins), valacyclovir, valganciclovir
Monocarboxylate transporters Salicylic acid, b-lactam antibiotics, statinsBile acid transporters (ASBT/IBAT) Various drugs conjugated to bile saltsOrganic anion transporter polypep-tide (OATP1)
Fexofenadine
136j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 5: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/5.jpg)
N
R
XO
O
+H3N
R1
H
CO2-R3
R2
HisXH
1
2
3
4
Figure 6.2 PEPT1 substrate recognition site contains four key structural characteristics (modifiedfrom Ref. [15]).
Dipeptide
NH
H2N
R1
O
COOH
R2
NH
H2N
R1
O R2
HN
O
R3
COOH
H2N OH
O
O
Tripeptide
Aminolevulinic acid
R NH
O
N
O
S
COOH
N
O
R1
R2
COOH
beta-Lactam antibiotic (penicillins)
ACE inhibitor
Figure 6.3 Substrates of peptide transporters.
6.4 Peptide Transporters: PEPT1 and PEPT2 j137
![Page 6: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/6.jpg)
such as d-aminolevulinic acid, possessing a ketomethylene group, are transported bypeptide transporters.
Its broad substrate specificity, reasonable high capacity, and high level ofexpression in the intestinal epithelium make PEPT1 an attractive target forprodrug design. As seen earlier in the case of valacyclovir, by engineering theprodrug to be recognized by PEPT1, a low permeability drug can obtain signifi-cantly higher oral absorption. Like valacyclovir, a valine ester prodrug of ganci-clovir (4), namely, valganciclovir (5), is actively transported by PEPT1, whichresults in approximately 60% oral bioavailability of ganciclovir in humans, whilethe oral bioavailability of ganciclovir itself is less than 10% [16]. The transportmechanism was confirmed in studies using Caco-2 cell monolayers where thetransport of valganciclovir was inhibited by a dipeptide, Gly-Phe [17]. In the sametransport studies, the bis-valine ester of ganciclovir and ganciclovir itself provednot to be PEPT1 substrates. Valganciclovir has also been shown to be a substrateof the PEPT2 transporter, which is mainly present in the kidney [17], and theamino acid transporter ATB0,þ , expressed primarily in the colon, lung, andeye [18]. Only very low levels of the prodrug can be detected in the systemiccirculation after oral administration, suggesting a rapid and complete hydrolysisto ganciclovir in vivo. Recently, it has been demonstrated that conversion ofvalganciclovir is due to the biphenyl hydrolase-like protein, valacyclovirase [10].Valganciclovir has been approved as an oral prodrug for the treatment ofcytomegalovirus (CMV).
HN
N
N
NH2N
O
OO
O
NH2
HN
N
N
NH2N
O
O
Ganciclovir (4)
Oral bioavailability 6%
Not substrate of PEPT1
Valganciclovir (5)
Oral bioavailability 60%
Substrate of PEPT1
OH
OH
OH
The pioneering success with valacyclovir and valganciclovir in the clinic paved theway for the development of several L-valine prodrugs of other poorly absorbed drugs,especially various nucleoside analogues. Levovirin valinate (6), valopicitabine (7), andvaltorcitabine (8) are prodrugs of levovirin, 20-C-methylcytidine and 20-deoxy-b-L-cytidine, respectively, and their improved oral absorption may be attributed to theinvolvement of PEPT1-mediated transport. All these L-valine prodrugs, includingvalomaciclovir stearate (9), which is a valyl/stearyl diester prodrug of H2G (omaci-clovir), are undergoing clinical trials. Therefore, the L-valine monoester concept hasproved to be an important landmark in the development of PEPT1-targeted oralprodrugs.
138j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 7: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/7.jpg)
ON
OH OH
N
N
O
NH2
O
O
NH2
Levovirin valinate (6)
O
N
HO
O OH
O
NH2
N
O
NH2
CH3
Valopitacitabine (7)
O
HO
O
O
NH2
N
O
NH2
Valtorcitabine (8)
NH
NN
N
O
NH2
O
H2N
O
OH3C(H2C)16
O
Valomaciclovir stearate (9)
The prodrug strategy targeting PEPT1 has also been effective in improving oralabsorption of polar parent drugs using amino acids other than valine. The peptidylprodrugs such as L-a-methyldopa-L-Phe, L-Phe-L-a-methyldopa, and L-a-methyldopa-L-Pro achieved 4–20 times higher intestinal wall permeability than a-methyldopaitself in a rat ileum perfusionmodel [19, 20]. While a-methyldopa is itself a relativelypoor substrate for the L-aromatic amino acid transporter, the uptake of the a-meth-yldopa prodrugs was inhibited by known PEPT1 substrates, thus demonstratingpeptide transporter-mediated absorption. Similarly, L-dopa-L-Phe showed peptidetransporter-mediated uptake that was 40-fold higher than that of L-dopa acrossCaco-2cell monolayers [21].
Recently, an L-alanylamide prodrug (LY544344 or talaglumetad, 11) emerged froma series of C-2, C-6, and N peptides derived from an agonist of the metabolicglutamate receptor 2 (LY354740, 10), with a variety of amino acids and dipeptidesas promoieties. The prodrug was selected on the basis of its effective active
6.4 Peptide Transporters: PEPT1 and PEPT2 j139
![Page 8: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/8.jpg)
transport [22]. In subsequent assays, this prodrug not only showed high affinity toPEPT1 in Caco-2 cells and hPEPT1-transfected CHO cells but also significantlyreduced permeability in the presence of the knownPEPT1 substrate Gly-Sar in in siturat intestinal perfusion studies [22, 23]. The prodrug also underwent extensivepresystemic intestinal activation, with more than 97% of prodrug hydrolysis occur-ring before its appearance in the hepatic portal vein [24]. In clinical studies, theprodrug has been shown to increase systemic LY354740 exposure by approximately13-fold compared to equivalent LY544344 doses.
HNH
H
O
NH2
O
HOO
OH
H2NH
H
O
HOO
OH
LY544344 (11)
LY354740 (10)
6.5Monocarboxylate Transporters
The monocarboxylate transporter (MCT) family (SLC16) is comprised of 14 mem-bers, although only the first 4 members have been shown to transport monocarbox-ylates [25, 26]. These four transporters, MCT1 (SLC16A1), MCT2 (SLC16A7), MCT3(SLC16A8), and MCT4 (SLC16A3), have been shown to transport a diverse group ofaliphatic monocarboxylates in a process that does not require ATP, but is insteadcontrolled by proton and substrate gradients [26]. For proper localization andfunctional expression of these transporters in the membrane, coexpression of anaccessory protein is also required. CD147, also known as basigin, has been shown toserve this role forMCT1,MCT3, andMCT4 [27], while gp70, also known as embigin,is used by MCT2 [28].
Of these four MCT transporters, only MCT3 has relatively restricted tissueexpression, primarily being expressed in the retinal pigment epithelium and choroidplexus epithelium [29]. The other MCTs are expressed in a variety of tissues,demonstrating high expression in the gastrointestinal tract [26], with MCT1 andMCT4 being the predominant isoforms expressed in the human colon [30]. Since thetransit time is longer in the colon than in the rest of the gastrointestinal tract, MCT1and MCT4 may be ideal candidates for use as prodrug transporters.
Using immunoblotting studies on purified apical and basolateral membranesisolated from different regions of the small and large intestines, Gill et al. reported
140j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 9: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/9.jpg)
that MCT1 was localized apically, with increasing abundance along the gastroin-testinal tract and predominant expression in the colon [30]. In addition, theyperformed immunohistochemical studies on colonic crypts obtained from humanbiopsy samples to confirm that MCT1 was predominantly confined to the apicalmembranes. Similar studies by Iwanaga et al. using mouse, rat, and human tissuesconfirmed the broad expression of MCT1 throughout the gastrointestinal tract,with greater expression in the large intestine than in the stomach or smallintestine; however, in contrast to the results obtained by Gill et al., they showedMCT1 expression to be on the basolateral cell membranes [31]. In addition, theyused immunoelectron microscopy to confirm the subcellular localization of MCT1in the cecum of mice, showing that MCT1 was present only in the basolateralmembranes of enterocytes and not in the microvillous region. The differencesreported by these two groups may be a result of differences in the antibodyrecognition sites, which could indicate that MCT1 is actually expressed on bothsides of the membrane.
Immunoblotting studies of MCT4 demonstrated that this transporter islocalized to the basolateral colonic membranes [30], with highest expression inthe distal colon, followed by the proximal colon, and followed by the ileum. TheMCT4 antibody was unsuitable for immunohistochemical studies [30], and otherstudies also failed to detect any visible signals for MCT4 in the digestive tract ofmice [31].
Lactate (12) and pyruvate (13) are natural substrates for MCT1 and MCT4. Inaddition, both MCT1 and MCT4 transport the short-chain fatty acids acetate,propionate, and butyrate, which collectively represent the most abundant anionsin the colon [30]. However, the specificity ofMCT1 andMCT4 is not limited to thesemolecules. Both proteins have been shown to transport a variety of small carbox-ylates, such as chloropropionate, hydroxybutyrate, alpha-ketoisocaproate, andalpha-ketoisovalerate [32, 33]. In fact, whenMCT1was first cloned, it was identifiedas �MEV,� a protein facilitating high uptake of the cholesterol precursor mevalonicacid [34].
MCT1 and MCT4 can also transport pharmaceutical agents. Gamma-hydroxybu-tyrate (GHB, 14), a naturally occurring metabolite of gamma-aminobutyric acid, isfound in mammalian brain, heart, liver, and kidney [35]. While GHB is usedtherapeutically for treating narcolepsy [36] and alcohol and heroin withdrawal [37],it is also widely abused by body builders for its growth hormone releasing proper-ties [38], as well as drug abusers for its euphoric effects and for drug-facilitated sexualassault [39, 40].
OH
O
OH
OH
O
O
HO
OH
O
γ -Hydroxybutyrate (14)Lactate (12) Pyruvate (13)
6.5 Monocarboxylate Transporters j141
![Page 10: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/10.jpg)
In addition to endogenous substrates, MCT1 has also been shown to transport avariety of xenobiotic compounds. Using tissue-specific cell lines, membranevesicles, Caco-2 cells, NBL-2 cells, MDCK cells, or in vivo investigations, MCTshave been demonstrated to transport compounds as diverse as b-lactam antibioticscarindacillin [41, 42] and cefdinir [43], valproic acid [44, 45], salicylic acid [46],fluorescein [47], ferulic acid [48], pravastatin [49], simvastatin [50], and ator-vastatin [51]. However, while the statins are substrates of MCT1, they are alsoinhibitors of MCT4, with the more lipophilic statins demonstrating the strongestinhibition [52].
With the wide variety of structures recognized by MCT1, as well as the highexpression in the gastrointestinal tract, it should be possible to design prodrugs totake advantage of MCT1. One such first prodrug was the b-lactam antibiotic prodrugcarindacillin (15), which is converted to carbenicillin (16) [53], although it was notspecifically designed to take advantage ofMCT1 (which itself would not be describedfor another 20 years). However, the role of MCT1 in the intestinal uptake ofcarindacillin has been confirmed in rat intestinal brush border membrane vesicles,and this MCT1-dependent uptake is believed to contribute to improved exposure tocarbenicillin [41, 42].
N
SNH
O
O
COOH
OO
N
SNH
COOH
O
O
COOH
Carindacillin (15) Carbenicillin (16)
This concept has also been used in the design of a gabapentin prodrug,XP13512 (or gabapentin enacarbil, 17), which was designed to overcome the poorintestinal absorption of gabapentin in part by taking advantage of MCT1 andanother transporter, the sodium-dependent multivitamin transporter SMVT. Theuptake of XP13512 was shown to be MCT1 mediated both in HEK-derived cellsand in MCT1-expressing oocytes [54]. While gabapentin (18) absorption occurs inonly a limited region of the small intestine and saturates at doses used clinically,resulting in dose-dependent pharmacokinetics, high interpatient variability, andpotentially ineffective drug exposure, XP13512 is absorbed throughout the entirelength of the intestine. In vivo studies on XP13512 demonstrated predictabledose-proportional bioavailability of gabapentin from XP13512 compared tothat resulting from gabapentin itself, as well as improved colonic absorption[55–58].
142j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 11: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/11.jpg)
XP13512 (17)
NH
OH
O
O
O
O
O
H2N
OH
O
Gabapentin (18)
A prodrug of R-baclofen, arbaclofen placarbil (19), has also been designed to takeadvantage of MCT1 [57, 58]. The prodrug was shown to compete with the naturalMCT1 substrate lactate in LLC-PK1-derived cells expressing high levels ofMCT1 anddemonstrated increased uptake in MCT1-expressing oocytes compared to controloocytes. In contrast, R-baclofen (20) itself did not show any significant interactionwith MCT1 [57, 58]. Arbaclofen placarbil has demonstrated enhanced colonicabsorption with 5-fold higher R-baclofen exposure in rats and 12-fold higher inmonkeys compared to intracolonic administration of R-baclofen. Sustained releaseformulations of arbaclofen placarbil demonstrated sustained R-baclofen exposure indogs with bioavailability up to 68%.
Arbaclofen placarbil (19)
NH
OH
O
O
O
O
O
R-Baclofen (20)
Cl
H2N
OH
O
Cl
With numerous endogenous and exogenous compounds, including prodrugs,already known to be recognized by MCT1, this transporter shows considerablepromise as a target for future prodrugs that can be designed to take advantage of itsbroad substrate recognition, high capacity, and high colonic expression.
6.6Bile Acid Transporters
Bile, consisting of bile acids, phospholipids, cholesterol, biliary pigments, andproteins, is concentrated and stored in the gall bladder. During digestion, bile issecreted into the small intestine. As they travel through the gastrointestinal tract, the
6.6 Bile Acid Transporters j143
![Page 12: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/12.jpg)
bile acids are nearly completely reabsorbed by both active and passive mechanisms.Bile acids then recirculate to the liver via the portal vein.
Inhumans, the primary bile acids, cholate and chenodeoxycholate, are synthesizedin hepatocytes from cholesterol, while secondary bile acids (such as deoxycholate andlithocholate) are formed via bacterial metabolism in the small intestine [59]. Theprincipal bile acids in human bile aremainly conjugated cholic acid and chenodeoxy-cholic acid [60]. Conjugation increases bile acid polarity and lowers passive transport,resulting in most bile acid reabsorption being controlled by the human apicalsodium-dependent bile acid transporter hASBT (SLC10A2, also known as IBAT forileal/intestinal bile acid transporter). This situation facilitates high intraluminal bileacid concentration to aid in lipid absorption. Conjugation also improves bile acidsolubility, helping to decrease any precipitation in the presence of high calcium ionconcentrations found in the gall bladder [61].
The enterohepatic circulation of bile acids occurs repeatedly (6–15 times/day) [62].The bile acid pool in humans is about 3–5 g, resulting in a turnover of 12–18 g of bileacid each day [60]. In spite of this repeated cycling, the loss of bile acid in the feces isless than 0.5 g/day, reflecting the tremendous capacity and efficiency of hASBT [63].
ASBT is expressed on the apical membrane of enterocytes in the terminal ileum,and mediates the reabsorption of bile acids into the ileum. The second bile acidtransporter, the sodium-dependent hepatocyte bile salt uptake transporter (NTCP,SLC10A1, also known as LBAT for liver bile acid transporter), is expressed inhepatocytes and localized on the basolateral (sinusoidal) domain to reabsorb bilesalts from the portal circulation. These two transporters have broad substratespecificity, high affinity for efficient absorption, and very high capacity, makingthem excellent targets for designing prodrugs [59].
Bile acids are versatile building blocks. Drug substances may be attached todifferent positions of the steroidal skeleton or to the side chain using differentchemical bonds, or by linkers with different structures, lengths, stereochemistries,polarities, and functional groups. The carboxylic acid group of the bile acid moleculemay be esterified, amidated, or reduced, while the steroidal hydroxyl groups can beused to make esters and ethers, or can be oxidized or reduced [62].
Pioneering work in developing bile acid-derived prodrugs came from the researchgroup of Kramer and Wess, who synthesized conjugates of bile acids containingdrugs such as chlorambucil, oxaprolyl peptide, HR780, and lovastatin (Figure 6.4)[64–71]. Their work on chlorambucil–bile acid conjugates showed that these com-pounds were absorbed from the ileum and secreted by the liver, as demonstrated byin situperfusion experiments of rat liver and ileal segments. In contrast, chlorambucilitself is cleared by the kidney. These intact bile acid conjugates retain the alkylatingactivity of chlorambucil. Later studies showed that humanhepatocellular carcinomaswere capable of mediating the uptake of a chlorambucil–taurocholate conjugate withhigh affinity, demonstrating the feasibility of bile acid–drug conjugates in liver-specific drug targeting [70].
A prime target for a liver-specific drug would be the statins, which are widely usedin efforts to lower plasma cholesterol levels.Drugs such as pravastatin, lovastatin, andsimvastatin inhibit the activity of HMG-CoA reductase, which is responsible for the
144j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 13: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/13.jpg)
Oxap
roli
ne
pep
tide
H
O
OH
OH
R1
O
(CH
2) n
H NCO
DR
UG
R1
= O
H, O
Me,
NH
CH
2CO
OH
, NH
CH
2CH
2SO
3HR
2 =
H, t
-Bu
H NH N
O
O
N
OH N
O
CO
2R
2
NO
NO
2N
N
F
O
HO
O
HR
780
N
Cl
Cl
O
OH
Chlo
ram
buci
l
Figu
re6.4
Bile
acid-derived
prod
rugs.
6.6 Bile Acid Transporters j145
![Page 14: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/14.jpg)
rate-limiting step in cholesterol biosynthesis, the transformation of b-hydroxy-b-methylglutaryl-CoA (HMG-CoA) to mevalonate [65, 66]. Since bile acids undergoenterohepatic circulation restricting them to the liver and small intestine, a statin-bileacid prodrug that specifically targeted cholesterol biosynthesis in the liver andintestines could reduce potential side effects due to cholesterol biosynthesis in othertissues.
Kramer et al. utilized two approaches: combining structural features ofHMG-CoAreductase inhibitors with bile acids to create hybrid molecules (22) and creation ofprodrugs by conjugation of the HMG-CoA reductase inhibitors to the bile acid(21) [65, 66]. The hybrid molecules were able to inhibit HMG-CoA reductase, whilethe prodrugs, prior to hydrolysis from the bile acid promoiety, could not. However,the prodrugs did release the active inhibitor, as evident by the presence of a majormetabolite, and the concentration of the conjugated drug in extrahepatic tissues inrats was considerably lower than the concentration in liver, demonstrating tissueselectivity. In vivo experiments also showed an inhibition of hepatic cholesterolbiosynthesis after oral dosage of the prodrugs, whereas the hybrid molecules wereinactive after oral dosing [65, 66].
HO
OH
OH
OH
O
DRUGH
HO
OH
OH
OH
HO
COOH
HMG-CoA reductase inhibitor prodrug (21) HMG-CoA reductase inhibitor hybrids (22)
Proof-of-concept studies using a series of drug-conjugated and drug–surrogate-conjugated steroidal pyrazoles were also performed to explore the potential of ASBTandNTCP [72]. Most of these conjugates showed better affinity for NTCP than ASBT,although several of them did demonstrate transport by ASBT in an oocyte electro-physiology assay [72].
Another proof-of-concept study, designed to take advantage of ASBT, createdacyclovir prodrugs by conjugation to a variety of bile acids [73]. Affinities wereassessed by measuring inhibition of taurocholate uptake in ASBT-transfected COS-7 cells, and the prodrug with the highest affinity was further evaluated in vitro andin vivo. This prodrug, acyclovir valylchenodeoxycholate (23), was cleaved by anesterase to release acyclovir, and resulted in greater acyclovir accumulation fromthe prodrug than could be obtained from the drug alone due to a combination of
146j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 15: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/15.jpg)
active uptake by ASBT and increased passive permeability. Oral administration ofthe prodrug in rats resulted in a twofold increase in acyclovir bioavailabilitycompared to acyclovir itself, demonstrating that a bile acid prodrug strategy couldbe useful in improving the oral bioavailability of compounds with limited intestinalpermeability [73].
Acyclovir valylchenodeoxycholate (23)
NH
O
OHHO
H
O
O
O N
N
NH
N
NH2
O
AcyclovirValine
Chenodeoxycholate
6.7Conclusions
Druguptake transporters in the intestinal tract play amajor role in the absorption anddisposition of some drugs. They also offer an intriguing target in designing prodrugswith a view to improving intestinal absorption of poorly absorbed drugs, as can beseen from successful prodrug examples discussed in this chapter.Moreover, in somecases, membrane transporters may also enable selective drug uptake to the targetorgan or tissue, or utilize the genetic polymorphism of drug transporters bydesigning drugs toward a specific portion of the patient population. Challengeswith relying on drug transporters in drug absorption include transport capacitybecoming rate limiting or saturable, susceptibility to drug–drug and drug–endo-genous ligand interactions, and genetic variability in a population. The prodrugapproach targeting intestinal uptake transporters is now widely exploited as dem-onstrated by themany novel prodrugs that are under investigation and development.
References
1 Martinez, M.N. and Amidon, G.L. (2002)Amechanistic approach to understandingthe factors affecting drug absorption: areview of fundamentals. Journal of ClinicalPharmacology, 42 (6), 620–643.
2 Dobson, P.D. and Kell, D.B. (2008)Carrier-mediated cellular uptake ofpharmaceutical drugs: an exception or therule? Nature Reviews. Drug Discovery,7 (3), 205–220.
References j147
![Page 16: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/16.jpg)
3 Beauchamp, L.M., Orr, G.F., De Miranda,P., Burnette, T., and Krenitsky, T.A.(1992) Amino acid ester prodrugs ofacyclovir. Antiviral Chemistry andChemotherapy, 3 (3), 157–164.
4 Weller, S., Blum, M.R. et al. (1993)Pharmacokinetics of the acyclovir pro-drug valaciclovir after escalating single-and multiple-dose administration tonormal volunteers. Clinical Pharmacologyand Therapeutics, 54 (6), 595–605.
5 Lee, C.-P., De Vrueh, R. L. A., and Smith,P. L. (1996) Transport of a prodrug ofAcyclovir, L-val-acyclovir, via theoligopeptide transporter. Proc. Int. Symp.Control. Release. Bioact. Mater., 23, 47–48.
6 Sinko, P.J. and Balimane, P.V. (1998)Carrier-mediated intestinal absorption ofvalacyclovir, the L-valyl ester prodrug ofacyclovir: 1. Interactions withpeptides, organic anions and organiccations in rats. Biopharmaceutics & DrugDisposition, 19 (4), 209–217.
7 de Vrueh, R.L., Smith, P.L. et al. (1998)Transport of L-valine-acyclovir via theoligopeptide transporter in thehuman intestinal cell line, Caco-2.The Journal of Pharmacology andExperimental Therapeutics, 286 (3),1166–1170.
8 Han, H., de Vrueh, R.L. et al. (1998) 50-Amino acid esters of antiviral nucleosides,acyclovir, and AZT are absorbed by theintestinal PEPT1 peptide transporter.Pharmaceutical Research, 15 (8),1154–1159.
9 Guo, A.,Hu, P. et al. (1999) Interactions ofa nonpeptidic drug, valacyclovir, with thehuman intestinal peptide transporter(hPEPT1) expressed in a mammalian cellline. The Journal of Pharmacology andExperimental Therapeutics, 289 (1),448–454.
10 Kim, I., Chu, X.Y. et al. (2003)Identification of a human valacyclovirase:biphenyl hydrolase-like protein asvalacyclovir hydrolase. The Journal ofBiological Chemistry, 278 (28),25348–25356.
11 Lai, L., Xu, Z. et al. (2008) Molecular basisof prodrug activation by humanvalacyclovirase, an alpha-aminoacid ester hydrolase. The Journal of
Biological Chemistry, 283 (14),9318–9327.
12 Fei, Y.J., Kanai, Y. et al. (1994) Expressioncloning of a mammalian proton-coupledoligopeptide transporter. Nature,368 (6471), 563–566.
13 Liu, W., Liang, R. et al. (1995) Molecularcloning of PEPT 2, a new member of theHþ/peptide cotransporter family, fromhuman kidney. Biochimica et BiophysicaActa, 1235 (2), 461–466.
14 Tanaka, H., Miyamoto, K.I. et al. (1998)Regulation of the PEPT1 peptidetransporter in the rat small intestine inresponse to 5-fluorouracil-inducedinjury. Gastroenterology, 114 (4),714–723.
15 Bailey, P.D., Boyd, C.A. et al. (2000)How to make drugs orally active: asubstrate template for peptidetransporter PEPT1. Angewandte Chemie.International Edition in English, 39 (3),505–508.
16 Brown, F., Banken, L. et al. (1999)Pharmacokinetics of valganciclovir andganciclovir following multiple oraldosages of valganciclovir in HIV- andCMV-seropositive volunteers. ClinicalPharmacokinetics, 37 (2), 167–176.
17 Sugawara, M., Huang, W. et al. (2000)Transport of valganciclovir, a ganciclovirprodrug, via peptide transporters PEPT1and PEPT2. Journal of PharmaceuticalSciences, 89 (6), 781–789.
18 Umapathy, N.S.,Ganapathy, V. et al. (2004)Transport of amino acid esters and theamino-acid-based prodrug valganciclovirby the amino acid transporter ATB(0,þ ).Pharmaceutical Research, 21 (7),1303–1310.
19 Hu, M., Subramanian, P. et al. (1989) Useof the peptide carrier system to improvethe intestinal absorption of L-alpha-methyldopa: carrier kinetics, intestinalpermeabilities, and in vitro hydrolysis ofdipeptidyl derivatives of L-alpha-methyldopa. Pharmaceutical Research,6 (1), 66–70.
20 Bai, J.P., Hu, M. et al. (1992) Utilization ofpeptide carrier system to improveintestinal absorption: targeting prolidaseas a prodrug-converting enzyme. Journalof Pharmaceutical Sciences, 81 (2), 113–116.
148j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 17: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/17.jpg)
21 Tamai, I., Nakanishi, T. et al. (1998)Improvement of L-dopa absorption bydipeptidyl derivation, utilizing peptidetransporter PEPT1. Journal ofPharmaceutical Sciences, 87 (12),1542–1546.
22 Bueno, A.B., Collado, I. et al. (2005)Dipeptides as effective prodrugs of theunnatural amino acid (þ )-2-aminobicyclo[3.1.0]hexane-2,6-dicarboxylic acid(LY354740), a selective group IImetabotropic glutamate receptor agonist.Journal of Medicinal Chemistry, 48 (16),5305–5320.
23 Eriksson, A.H., Varma, M.V. et al. (2010)The intestinal absorption of a prodrug ofthe mGlu2/3 receptor agonist LY354740is mediated by PEPT1: in situ ratintestinal perfusion studies. Journal ofPharmaceutical Sciences, 99 (3),1574–1581.
24 Perkins, E.J. and Abraham, T. (2007)Pharmacokinetics, metabolism, andexcretion of the intestinal peptidetransporter 1 (SLC15A1)-targetedprodrug (1S,2S,5R,6S)-2-[(20S)-(2-amino)propionyl]aminobicyclo[3.1.0.]hexen-2,6-di carboxylic acid (LY544344) in ratsand dogs: assessment of first-passbioactivation and dose linearity. DrugMetabolism and Disposition: TheBiological Fate of Chemicals, 35 (10),1903–1909.
25 Meredith, D. and Christian, H.C. (2008)The SLC16 monocaboxylate transporterfamily. Xenobiotica; The Fate of ForeignCompounds in Biological Systems, 38 (7–8),1072–1106.
26 Merezhinskaya, N. and Fishbein, W.N.(2009) Monocarboxylate transporters:past, present, and future. Histology andHistopathology, 24 (2), 243–264.
27 Kirk, P., Wilson, M.C. et al. (2000) CD147is tightly associated with lactatetransporters MCT1 and MCT4 andfacilitates their cell surface expression.EMBO Journal, 19 (15), 3896–3904.
28 Wilson, M.C., Meredith, D. et al. (2005)Basigin (CD147) is the target fororganomercurial inhibition ofmonocarboxylate transporter isoforms 1and 4: the ancillary protein for theinsensitive MCT2 is EMBIGIN (gp70).
The Journal of Biological Chemistry,280 (29), 27213–27221.
29 Yoon, H., Fanelli, A. et al. (1997)Identification of a uniquemonocarboxylate transporter (MCT3) inretinal pigment epithelium. Biochemicaland Biophysical Research Communications,234 (1), 90–94.
30 Gill, R.K., Saksena, S. et al. (2005)Expression and membrane localization ofMCT isoforms along the length of thehuman intestine. American Journal ofPhysiology. Cell Physiology, 289 (4),C846–C852.
31 Iwanaga, T., Takebe, K. et al. (2006)Cellular expression of monocarboxylatetransporters (MCT) in the digestive tractof the mouse, rat, and humans, withspecial reference to SLC5A8. BiomedicalResearch (Tokyo, Japan), 27 (5), 243–254.
32 Manning Fox, J.E., Meredith, D. et al.(2000) Characterisation of humanmonocarboxylate transporter 4substantiates its role in lactic acid effluxfrom skeletal muscle. The Journal ofPhysiology, 529 (Pt 2), 285–293.
33 Morris, M.E. and Felmlee, M.A. (2008)Overview of the proton-coupled MCT(SLC16A) family of transporters:characterization, function and role in thetransport of the drug of abuse gamma-hydroxybutyric acid. AAPS Journal, 10 (2),311–321.
34 Kim, C.M., Goldstein, J.L. et al. (1992)cDNA cloning of MEV, a mutant proteinthat facilitates cellular uptake ofmevalonate, and identification of the pointmutation responsible for its gain offunction. The Journal of BiologicalChemistry, 267 (32), 23113–23121.
35 Maitre, M. (1997) The gamma-hydroxybutyrate signalling system inbrain: organization and functionalimplications. Progress in Neurobiology,51 (3), 337–361.
36 Mamelak, M., Scharf, M.B. et al. (1986)Treatment of narcolepsy with gamma-hydroxybutyrate. A review of clinical andsleep laboratory findings. Sleep, 91 Pt (2),285–289.
37 Gallimberti, L., Spella, M.R. et al. (2000)Gamma-hydroxybutyric acid in thetreatment of alcohol and heroin
References j149
![Page 18: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/18.jpg)
dependence. Alcohol (Fayetteville, NY),20 (3), 257–262.
38 Okun, M.S., Boothby, L.A. et al. (2001)GHB: an important pharmacologic andclinical update. Journal of Pharmacy &Pharmaceutical Sciences: A Publication ofthe Canadian Society for PharmaceuticalSciences, 4 (2), 167–175.
39 Schwartz, R.H., Milteer, R. et al. (2000)Drug-facilitated sexual assault (�daterape�). Southern Medical Journal, 93 (6),558–561.
40 Wong, C.G., Chan, K.F. et al. (2004)Gamma-hydroxybutyric acid: neurobiologyand toxicology of a recreational drug.Toxicology Review, 23 (1), 3–20.
41 Li, Y.H., Ito, K. et al. (1999) Mechanism ofintestinal absorption of an orally activebeta-lactamprodrug: uptake and transportof carindacillin in Caco-2 cells.The Journalof Pharmacology and ExperimentalTherapeutics, 290 (3), 958–964.
42 Li, Y.H., Tanno, M. et al. (1999) Role of themonocarboxylic acid transport system inthe intestinal absorption of an orally activebeta-lactam prodrug: carindacillin as amodel. International Journal ofPharmaceutics, 191 (2), 151–159.
43 Tsuji, A., Tamai, I. et al. (1993) Intestinalbrush-border transport of the oralcephalosporin antibiotic, cefdinir,mediated by dipeptide andmonocarboxylic acid transport systems inrabbits. The Journal of Pharmacy andPharmacology, 45 (11), 996–998.
44 Utoguchi, N. and Audus, K.L. (2000)Carrier-mediated transport of valproic acidin BeWo cells, a human trophoblast cellline. International Journal ofPharmaceutics, 195 (1–2), 115–124.
45 Hosoya, K. and Kondo, T. et al. (2001)MCT1-mediated transport of L-lactic acidat the inner blood–retinal barrier: apossible route for delivery ofmonocarboxylic acid drugs to the retina.Pharmaceutical Research, 18 (12),1669–1676.
46 Neuhoff, S., Ungell, A.L. et al. (2005) pH-Dependent passive and active transportof acidic drugs across Caco-2 cellmonolayers. European Journal ofPharmaceutical Sciences, 25 (2–3),211–220.
47 Konishi, Y., Hagiwara, K. et al. (2002)Transepithelial transport of fluorescein inCaco-2 cell monolayers and use of suchtransport in in vitro evaluation of phenolicacid availability. Bioscience, Biotechnology,and Biochemistry, 66 (11), 2449–2457.
48 Konishi, Y. and Shimizu, M. (2003)Transepithelial transport of ferulic acid bymonocarboxylic acid transporter in Caco-2cell monolayers. Bioscience, Biotechnology,and Biochemistry, 67 (4), 856–862.
49 Tamai, I., Takanaga, H. et al. (1995)Proton-cotransport of pravastatin acrossintestinal brush-border membrane.Pharmaceutical Research, 12 (11),1727–1732.
50 Tsuji, A., Saheki, A. et al. (1993)Transport mechanism of 3-hydroxy-3-methylglutaryl coenzyme A reductaseinhibitors at the blood–brain barrier.The Journal of Pharmacology andExperimental Therapeutics, 267 (3),1085–1090.
51 Wu, X., Whitfield, L.R. et al. (2000)Atorvastatin transport in the Caco-2 cellmodel: contributions of P-glycoproteinand the proton-monocarboxylic acid co-transporter. Pharmaceutical Research,17 (2), 209–215.
52 Kobayashi, M., Otsuka, Y. et al. (2006)Inhibitory effects of statins on humanmonocarboxylate transporter 4.International Journal of Pharmaceutics,317 (1), 19–25.
53 English, A.R., Retsema, J.A. et al. (1972)Carbenicillin indanyl sodium, an orallyactive derivative of carbenicillin.Antimicrobial Agents and Chemotherapy,1 (3), 185–191.
54 Cundy, K.C., Branch, R. et al. (2004)XP13512 [(þ /�)-1-([(alpha-isobutanoyloxyethoxy)carbonyl]aminomethyl)-1-cyclohexane acetic acid],a novel gabapentin prodrug: I.Design, synthesis, enzymatic conversionto gabapentin, and transport byintestinal solute transporters.The Journal of Pharmacology andExperimental Therapeutics, 311 (1),315–323.
55 Cundy, K.C., Annamalai, T. et al. (2004)XP13512 [(þ /�)-1-([(alpha-isobutanoyloxyethoxy)carbonyl]
150j 6 Prodrugs Designed to Target Transporters for Oral Drug Delivery
![Page 19: [Methods and Principles in Medicinal Chemistry] Prodrugs and Targeted Delivery (Towards Better ADME Properties) || Prodrugs Designed to Target Transporters for Oral Drug Delivery](https://reader040.dokumen.tips/reader040/viewer/2022020408/5750928c1a28abbf6ba83942/html5/page/19.jpg)
aminomethyl)-1-cyclohexane acetic acid],a novel gabapentin prodrug: II. Improvedoral bioavailability, dose proportionality,and colonic absorption compared withgabapentin in rats and monkeys. TheJournal of Pharmacology and ExperimentalTherapeutics, 311 (1), 324–333.
56 Cundy, K.C., Sastry, S. et al. (2008) Clinicalpharmacokinetics of XP13512, a noveltransported prodrug of gabapentin.Journal of Clinical Pharmacology, 48 (12),1378–1388.
57 Lal, R., Sukbuntherng, J. et al. (2009)Pharmacokinetics and tolerability ofsingle escalating doses of gabapentinenacarbil: a randomized-sequence,double-blind, placebo-controlledcrossover study in healthy volunteers.Clinical Therapeutics, 31 (8), 1776–1786.
58 Lal, R., Sukbuntherng, J. et al. (2009)Arbaclofen placarbil, a novel R-baclofenprodrug: improved absorption,distribution,metabolism, and eliminationproperties compared with R-baclofen. TheJournal of Pharmacology and ExperimentalTherapeutics, 330 (3), 911–921.
59 Balakrishnan, A. and Polli, J.E. (2006)Apical sodium dependent bile acidtransporter (ASBT, SLC10A2): a potentialprodrug target. Molecular Pharmacology,3 (3), 223–230.
60 Hofmann, A.F. (1999) The continuingimportance of bile acids in liver andintestinal disease. Archives of InternalMedicine, 159 (22), 2647–2658.
61 Hofmann, A.F. and Mysels, K.J. (1992)Bile acid solubility and precipitation invitro and in vivo: the role of conjugation,pH, and Ca2
þ ions. Journal of LipidResearch, 33 (5), 617–626.
62 Sievanen, E. (2007) Exploitation of bileacid transport systems in prodrug design.Molecules, 12 (8), 1859–1889.
63 St-Pierre, M.V., Kullak-Ublick, G.A. et al.(2001) Transport of bile acids in hepaticand non-hepatic tissues. The Journal ofExperimental Biology, 204 (Pt 10),1673–1686.
64 Kramer, W., Wess, G. et al. (1992) Liver-specific drug targeting by coupling to bileacids. The Journal of Biological Chemistry,267 (26), 18598–18604.
65 Kramer, W.,Wess, G. et al. (1994) Bile acidderived HMG-CoA reductase inhibitors.Biochimica et Biophysica Acta, 1227 (3),137–154.
66 Kramer, W., Wess, G. et al. (1994)Intestinal absorption of peptides bycoupling to bile acids. The Journal ofBiological Chemistry, 269 (14),10621–10627.
67 Wess, G., Kramer, W. et al. (1994) Specificinhibitors of ileal bile acid transport.Journal of Medicinal Chemistry, 37 (7),873–875.
68 Wess, G., Kramer, W. et al. (1994)Synthesis and biological activity of bileacid-derived HMG-CoA reductaseinhibitors. The role of 21-methyl inrecognition of HMG-CoA reductase andthe ileal bile acid transport system.Journal of Medicinal Chemistry, 37 (20),3240–3246.
69 Kramer, W. and Wess, G. (1996) Bile acidtransport systems as pharmaceuticaltargets. European Journal of ClinicalInvestigation, 26 (9), 715–732.
70 Kullak-Ublick, G.A., Glasa, J. et al. (1997)Chlorambucil-taurocholate is transportedby bile acid carriers expressed in humanhepatocellular carcinomas.Gastroenterology, 113 (4), 1295–1305.
71 Starke, D., Lischka, K. et al. (2001) Bileacid-oligodeoxynucleotide conjugates:synthesis and liver excretion in rats.Bioorganic & Medicinal Chemistry Letters,11 (7), 945–949.
72 Bhat, L., Jandeleit, B. et al. (2005)Synthesis and biological evaluation ofnovel steroidal pyrazoles as substrates forbile acid transporters. Bioorganic &Medicinal Chemistry Letters, 15 (1), 85–87.
73 Tolle-Sander, S., Lentz, K.A. et al. (2004)Increased acyclovir oral bioavailability viaa bile acid conjugate. MolecularPharmacology, 1 (1), 40–48.
References j151