Embed Size (px)
Citation preview
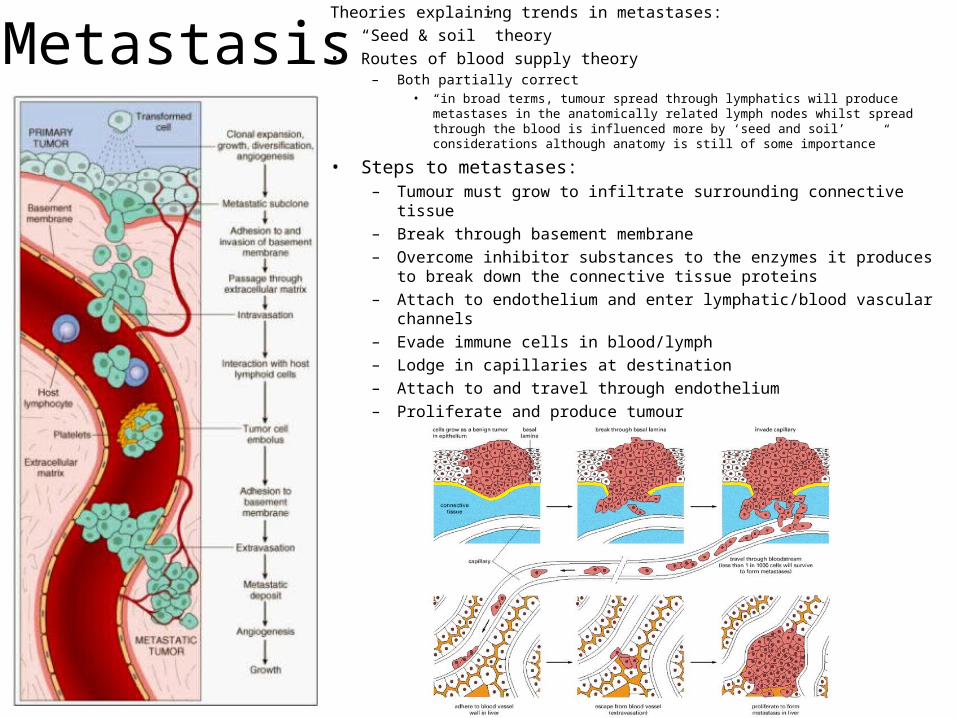
MetastasisTheories explaining trends in metastases:• “Seed & soil” theory• Routes of blood supply theory
– Both partially correct• “in broad terms, tumour spread through lymphatics will produce metastases in the
anatomically related lymph nodes whilst spread through the blood is influenced more by ‘seed and soil’ considerations although anatomy is still of some importance”
• Steps to metastases:– Tumour must grow to infiltrate surrounding connective tissue– Break through basement membrane– Overcome inhibitor substances to the enzymes it produces to break
down the connective tissue proteins– Attach to endothelium and enter lymphatic/blood vascular channels– Evade immune cells in blood/lymph– Lodge in capillaries at destination– Attach to and travel through endothelium– Proliferate and produce tumour
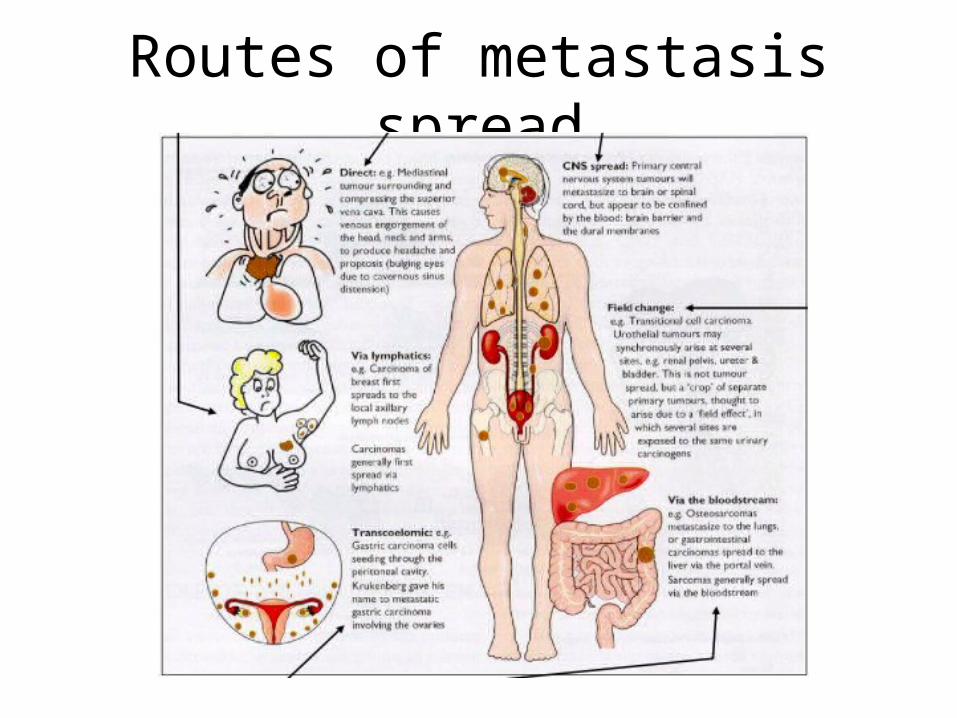
Routes of metastasis spread
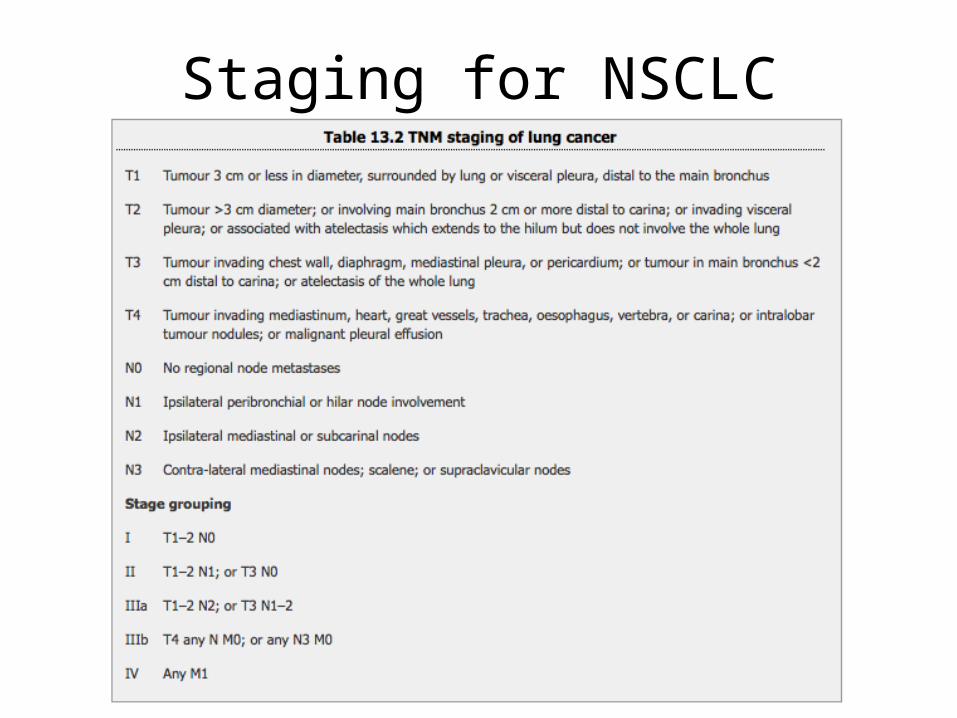
Staging for NSCLC
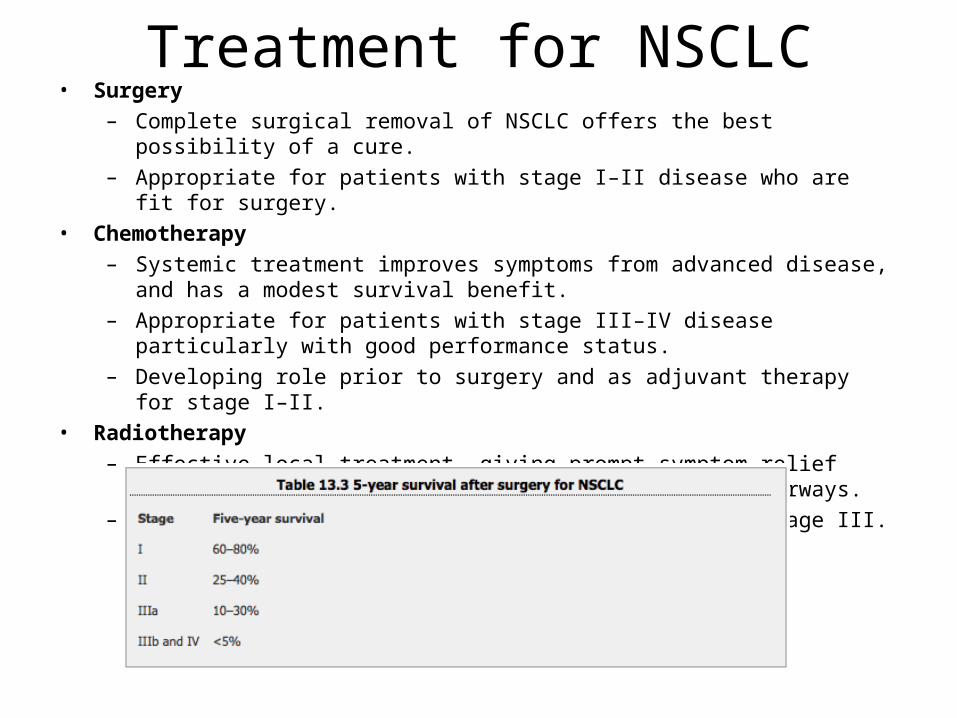
Treatment for NSCLC• Surgery
– Complete surgical removal of NSCLC offers the best possibility of a cure. – Appropriate for patients with stage I–II disease who are fit for surgery.
• Chemotherapy– Systemic treatment improves symptoms from advanced disease, and has a modest
survival benefit. – Appropriate for patients with stage III–IV disease particularly with good performance
status. – Developing role prior to surgery and as adjuvant therapy for stage I–II.
• Radiotherapy– Effective local treatment, giving prompt symptom relief from advanced disease
especially involving large airways. – Can be curative in stage I–II and, infrequently, stage III.
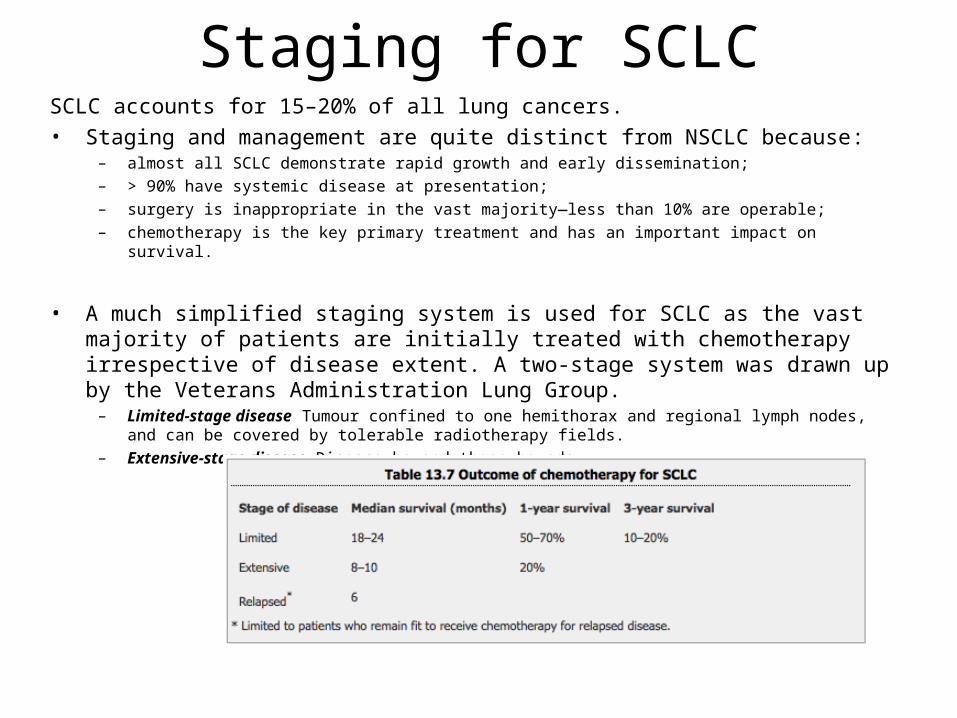
Staging for SCLCSCLC accounts for 15–20% of all lung cancers.• Staging and management are quite distinct from NSCLC because:
– almost all SCLC demonstrate rapid growth and early dissemination; – > 90% have systemic disease at presentation; – surgery is inappropriate in the vast majority—less than 10% are operable; – chemotherapy is the key primary treatment and has an important impact on survival.
• A much simplified staging system is used for SCLC as the vast majority of patients are initially treated with chemotherapy irrespective of disease extent. A two-stage system was drawn up by the Veterans Administration Lung Group.– Limited-stage disease Tumour confined to one hemithorax and regional lymph nodes, and can be covered by
tolerable radiotherapy fields. – Extensive-stage disease Disease beyond these bounds.











![Port-SiteMetastasisafterLaparoscopicSurgeryfor ...downloads.hindawi.com/journals/au/2012/609531.pdfport-site metastasis remain a concern [4]. Port-site metastases, though rare, have](https://img.dokumen.tips/doc/110x75/5ece8781bd73eb5762772a91/port-sitemetastasisafterlaparoscopicsurgeryfor-port-site-metastasis-remain-a.jpg)

![Isolated splenic metastasis from colon cancer: Case report › 18418cf... · for metastases[2]. We report a case of isolated splenic metastasis 16 mo after right Hemicolectomy for](https://img.dokumen.tips/doc/110x75/5f1d45c997812b30ff0f5c8d/isolated-splenic-metastasis-from-colon-cancer-case-report-a-18418cf-for.jpg)















