Embed Size (px)
Citation preview
Metabolic Abnormalities and Mitochondrial Function in Children with Perinatally-Acquired HIV Infection in the
Pediatric HIV/AIDS Cohort Study (PHACS)
Mariana Gerschenson, Ph.D.Tracie L. Miller MD, Jiajia Wang MS, Denise L. Jacobson PhD, MPH, Jody K. Takemoto PhD, Tanvi Sharma MD, Mitchell Geffner MD, Daniel E. Libutti BS,
Susanne Siminski MS, MBA, Gabriel Somarriba DPT, and Patricia Graham MSfor the Pediatric HIV/AIDS Cohort Study
July 23, 2012XIX International AIDS Conference

Background
• Insulin resistance is common among perinatally HIV-infected children (HIV+)
• Mitochondrial dysfunction, induced by antiretroviral therapy (ARV) or chronic viral infection, is a possible mechanism for metabolic dysfunction
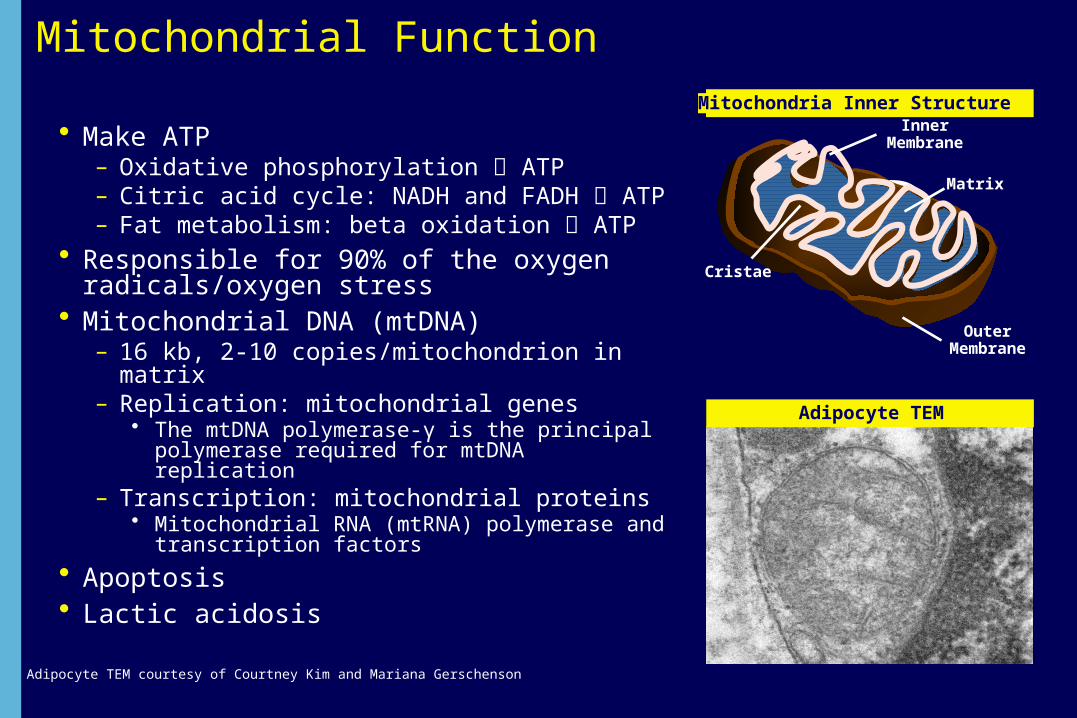
Mitochondrial Function
• Make ATP– Oxidative phosphorylation ATP– Citric acid cycle: NADH and FADH ATP – Fat metabolism: beta oxidation ATP
• Responsible for 90% of the oxygen radicals/oxygen stress
• Mitochondrial DNA (mtDNA)– 16 kb, 2-10 copies/mitochondrion in matrix– Replication: mitochondrial genes
• The mtDNA polymerase-γ is the principal polymerase required for mtDNA replication
– Transcription: mitochondrial proteins• Mitochondrial RNA (mtRNA) polymerase and
transcription factors
• Apoptosis• Lactic acidosis
Adipocyte TEM courtesy of Courtney Kim and Mariana Gerschenson
Mitochondria Inner Structure
HIV
InnerMembrane
OuterMembrane
Cristae
Matrix
Adipocyte TEM
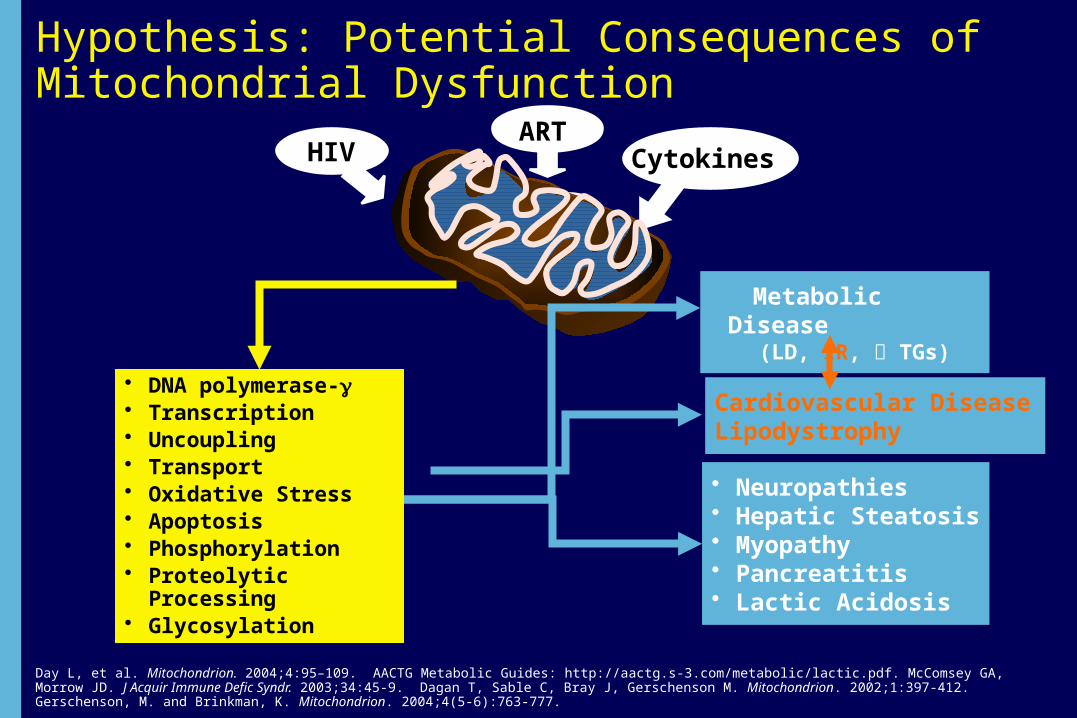
Hypothesis: Potential Consequences of Mitochondrial Dysfunction
Cardiovascular DiseaseLipodystrophy
• Neuropathies• Hepatic Steatosis• Myopathy• Pancreatitis• Lactic Acidosis
Metabolic Disease (LD, IR, TGs)
ARTCytokines
Day L, et al. Mitochondrion. 2004;4:95–109. AACTG Metabolic Guides: http://aactg.s-3.com/metabolic/lactic.pdf. McComsey GA, Morrow JD. J Acquir Immune Defic Syndr. 2003;34:45-9. Dagan T, Sable C, Bray J, Gerschenson M. Mitochondrion. 2002;1:397-412. Gerschenson, M. and Brinkman, K. Mitochondrion. 2004;4(5-6):763-777.
HIV
HIV
• DNA polymerase-g• Transcription• Uncoupling• Transport• Oxidative Stress• Apoptosis• Phosphorylation• Proteolytic Processing• Glycosylation
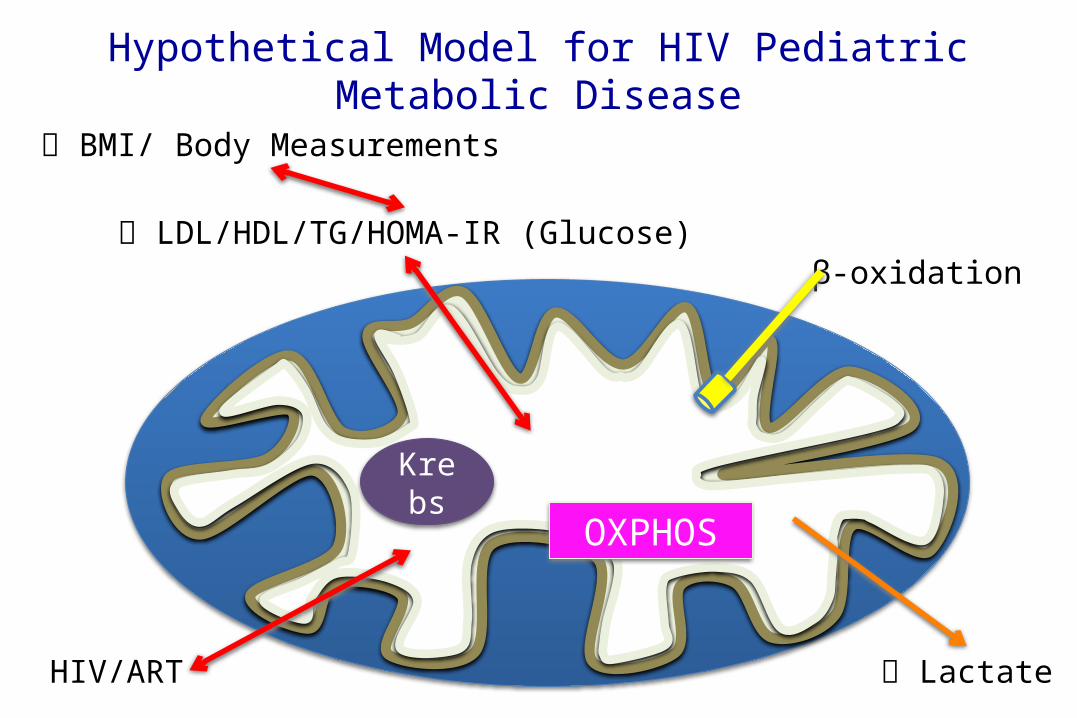
Hypothetical Model for HIV Pediatric Metabolic Disease
BMI/ Body Measurements
LDL/HDL/TG/HOMA-IR (Glucose)
OXPHOSKrebs
β-oxidation
LactateHIV/ART

Objectives
• To compare mitochondrial function [oxidative phosphorylation (OXPHOS) enzyme activities and lactate levels] of 191 HIV+ and 117 HIV-exposed, uninfected (HEU) children and among HIV+, determine associations with homeostatic model assessment of insulin resistance (IR) (HOMA-IR) and hyperlipidemia
• In HIV+ children, to determine if mitochondrial function (oxidative phosphorylation [OXPHOS] enzyme activities and lactate and pyruvate levels) are associated with metabolic abnormalities (IR and hyperlipidemia)

Mitochondrial Determinant Component of PHACS
• The Adolescent Master Protocol (AMP), a part of the Pediatric HIV/AIDS Cohort Study (PHACS), is a prospective cohort study conducted at 12 US sites designed to define the impact of HIV infection and ARV on pre-adolescents and adolescents with perinatal HIV infection.
• The Mitochondrial Determinants Component (MDC) is a separately funded study (R01 NR12885) that has co-enrolled AMP participants since May 2011.
• The objective of MDC is to determine the influence of mitochondrial abnormalities on metabolic outcomes in HIV+ children who were previously enrolled in AMP from 7 years of age until their 16th birthday. HIV-exposed, uninfected children (HEU) are also enrolled to serve as controls.
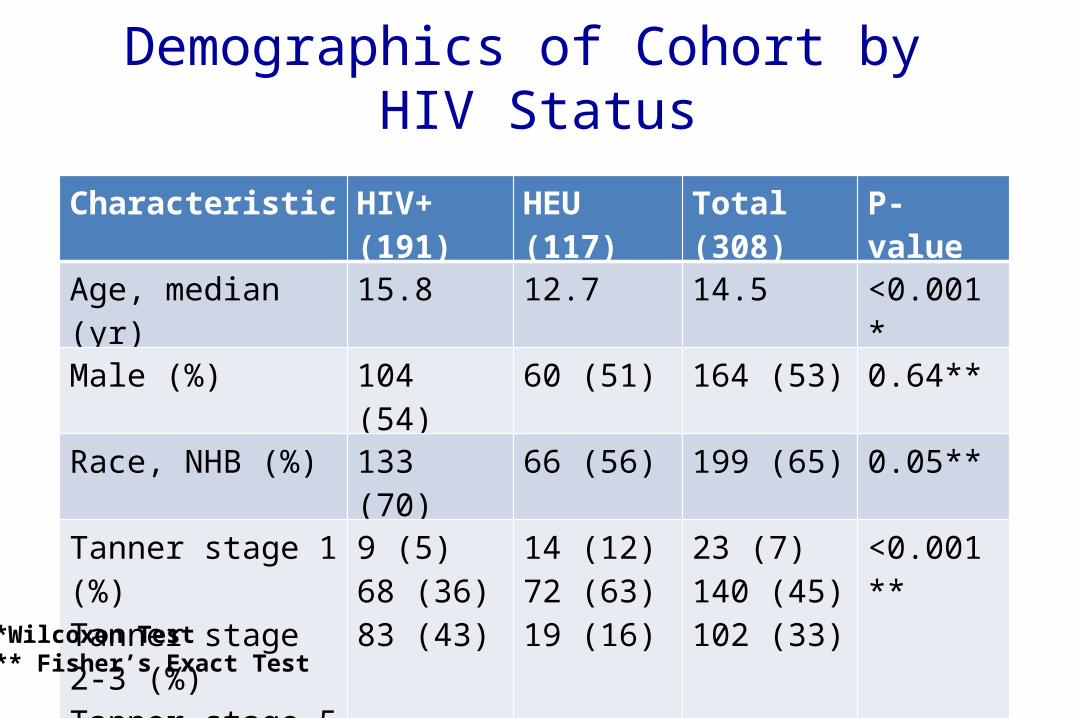
Demographics of Cohort by HIV Status
Characteristic HIV+ (191) HEU (117) Total (308) P-valueAge, median (yr) 15.8 12.7 14.5 <0.001*Male (%) 104 (54) 60 (51) 164 (53) 0.64**Race, NHB (%) 133 (70) 66 (56) 199 (65) 0.05**Tanner stage 1 (%)Tanner stage 2-3 (%)Tanner stage 5 (%)
9 (5)68 (36)83 (43)
14 (12)72 (63)19 (16)
23 (7)140 (45)102 (33)
<0.001**
BMI Z-score, median 0.46 0.91 0.59 0.005*
*Wilcoxon Test** Fisher’s Exact Test

Clinical Characteristics of HIV+ Children at Study Entry
Characteristic ValueCDC Stage, N (%) N/A 84 (44)
B 55 (29)
C 41 (21)
CD4 Count, cell/mm3 Median (IQR) 624 (463, 859)
Viral load, copies/mL (%) >5000 34 (18)
401-5000 40 (21)
<400 61 (11)
ARV Regimens (%)
HAART with PI 111 (58)
HAART without PI 30 (16)
Non-HAART ARV 10 (5)
No ARV 10 (5)

Baseline Metabolic Outcomes in HIV-Infected Children
Metabolic Outcome N Abnormal (%) Median IQR
Fasting Glucose (mg/dL) 153 86.0 81, 91
Fasting Insulin (mu/mL) 150 12.1 8.0, 20.9
HOMA-IR (normal <2.5 for Tanner 1 or <4 for Tanner 2-5)
151 29 2.5 1.7, 4.5
Total cholesterol (mg/dL) 189 15 159 137, 186
HDL-cholesterol (mg/dL) 187 10 49 41, 58
LDL-cholesterol (mg/dL) 186 11 87 72, 112
Triglycerides (mg/dL) 188 15 86.5 63, 116

Mitochondrial Function by HIV Status
Median Outcome HIV+ HEU P-value
POC lactate (mg/dL) [IQR]
1.45 [1.00, 1.90]
1.40[1.10, 1.90]
0.98
Venous lactate (mg/dL) [IQR]
1.0[0.78, 1.40]
1.26 [0.89, 1.70]
<0.001
Venous pyruvate (mg/dL) [IQR]
0.09[0.05, 0.11]
0.10[0.07, 0.13]
0.005
CI enzyme activity PBMC (OD/min/mg e-6) [IQR]
37.92 [27.73, 58.50]
36.87 [29.69, 56.87] 0.71
CIV enzyme activity PBMC (OD/min/mg e-6) [IQR]
69.38 [52.13, 83,34]
60.83 [50.59, 72.21]
0.048
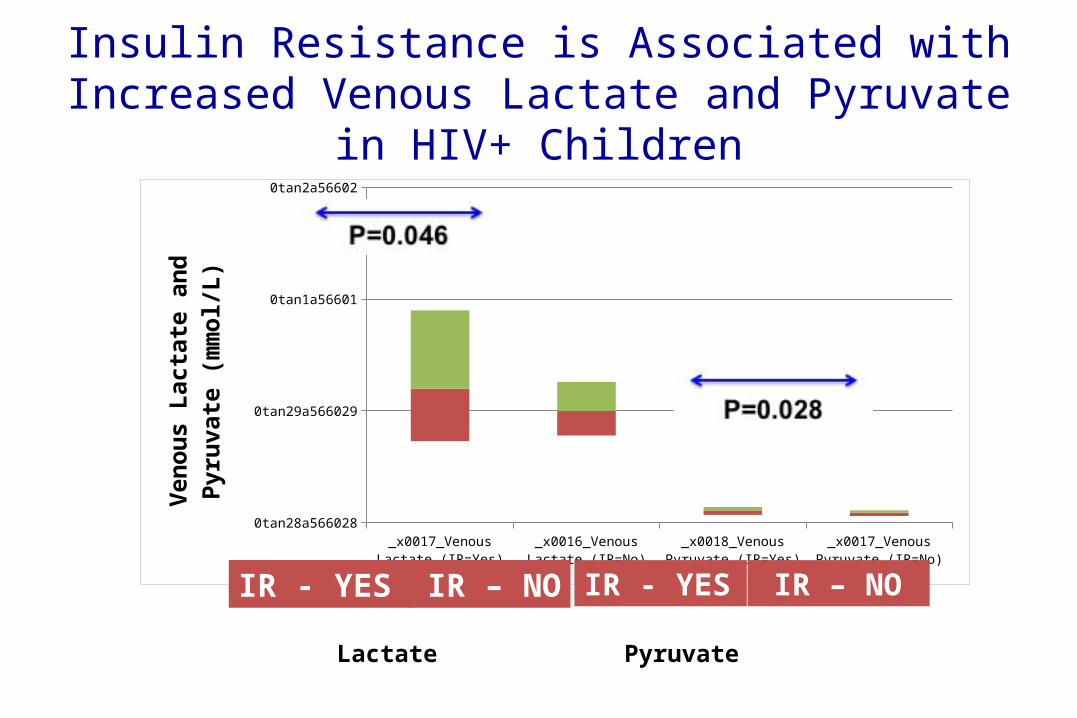
Insulin Resistance is Associated with Increased Venous Lactate and Pyruvate in
HIV+ Children
_x0017_Venous Lactate (IR=Yes)
_x0016_Venous Lactate (IR=No)
_x0018_Venous Pyruvate (IR=Yes)
_x0017_Venous Pyruvate (IR=No)
0tan28a566028
0tan29a566029
0tan1a56601
0tan2a56602Ve
nous
Lac
tate
and
Pyr
uvat
e (m
mol
/L)
IR - YES IR - YESIR – NO IR – NO
Lactate Pyruvate
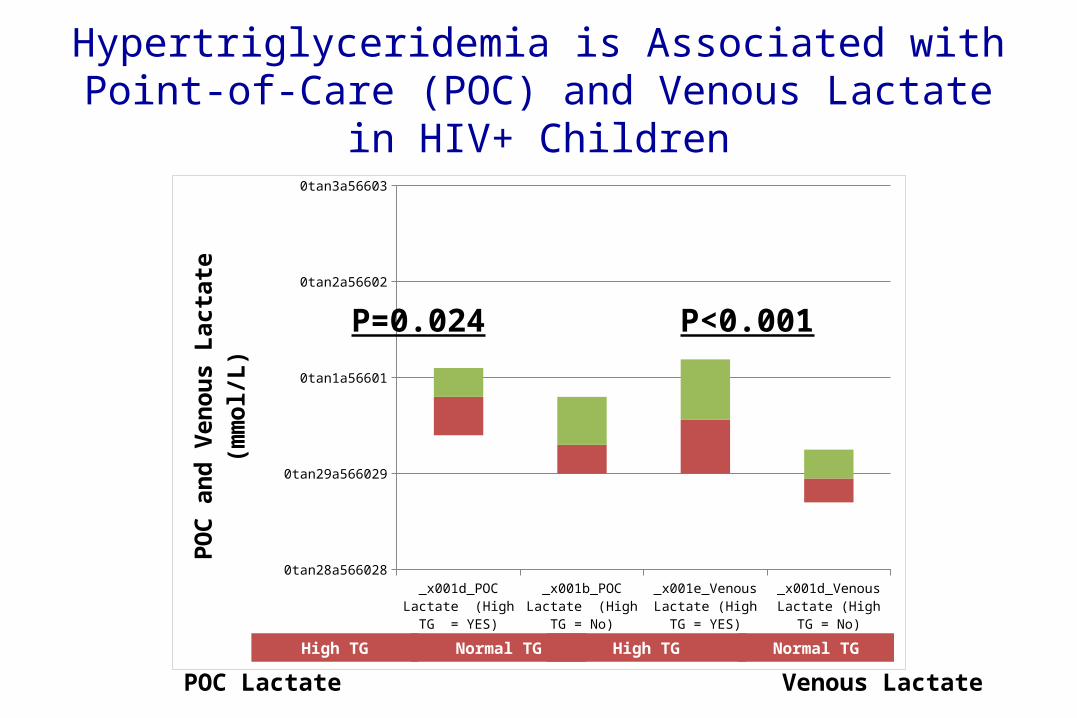
Hypertriglyceridemia is Associated with Point-of-Care (POC) and Venous Lactate in HIV+
Children
_x001d_POC Lactate (High TG = YES)
_x001b_POC Lactate (High TG = No)
_x001e_Venous Lactate (High TG = YES)
_x001d_Venous Lactate (High TG = No)
0tan28a566028
0tan29a566029
0tan1a56601
0tan2a56602
0tan3a56603PO
C an
d Ve
nous
Lac
tate
(mm
ol/L
)
High TG Normal TG High TG Normal TG
POC Lactate Venous Lactate
P=0.024 P<0.001

Low HDL-Cholesterol is Associated with Lower PBMC OXPHOS CI and CIV Enzyme Activities in
HIV+ Children
!CI Activity PBMCs (Low HDL = Yes) CI Activity PBMCs (Low HDL = No) "CIV Activity PBMCs (Low HDL = Yes)
!CIV Activity PBMCs (Low HDL = No)
0tan28a566028
0tan19a566019
0tan9a56609
0tan29a566029
0tan19a566019
0tan10a566010
0tan30a566030
0tan20a566020
CI (O
D/m
in/u
g e-
6) a
nd C
IV (O
D/m
in/u
g e-
5) A
ctiv
-iti
es in
PBM
Cs
Low HDL Normal HDL Low HDL Normal HDL
Complex I Complex IV
P=0.024
P=0.085
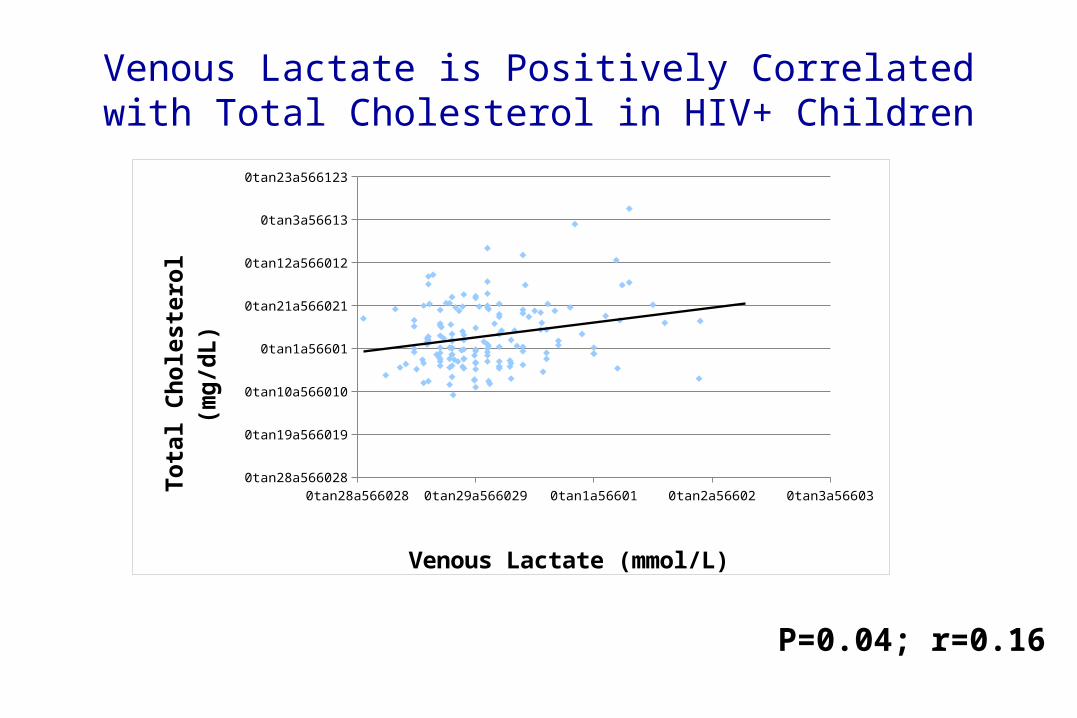
Venous Lactate is Positively Correlated with Total Cholesterol in HIV+ Children
P=0.04; r=0.16
0tan28a566028 0tan29a566029 0tan1a56601 0tan2a56602 0tan3a566030tan28a566028
0tan19a566019
0tan10a566010
0tan1a56601
0tan21a566021
0tan12a566012
0tan3a56613
0tan23a566123
Venous Lactate (mmol/L)
Tota
l Cho
lest
erol
(mg/
dL)

Venous Lactate is Positively Correlated with Triglycerides in HIV+ Children
0tan28a566028 0tan29a566029 0tan1a56601 0tan2a56602 0tan3a566030tan28a566028
0tan19a566019
0tan10a566010
0tan1a56601
0tan21a566021
0tan12a566012
0tan3a56613
0tan23a566123
0tan14a566114
0tan5a56615
Venous Lactate (mmol/L)
Fasti
ng T
rigl
ycer
ide
(mg/
dL)
P<0.0001; r=0.37

Multivariable Model for HDL-Cholesterol in HIV+Children
Effect Estimate SE P-value
Gender (male) 0.42 2.42 0.86
Age (per year) -0.73 0.44 0.10
Viral load (per copy/mL) -0.00009 0.00003 0.010
Venous lactate (mg/dL) -1.75 1.18 0.14
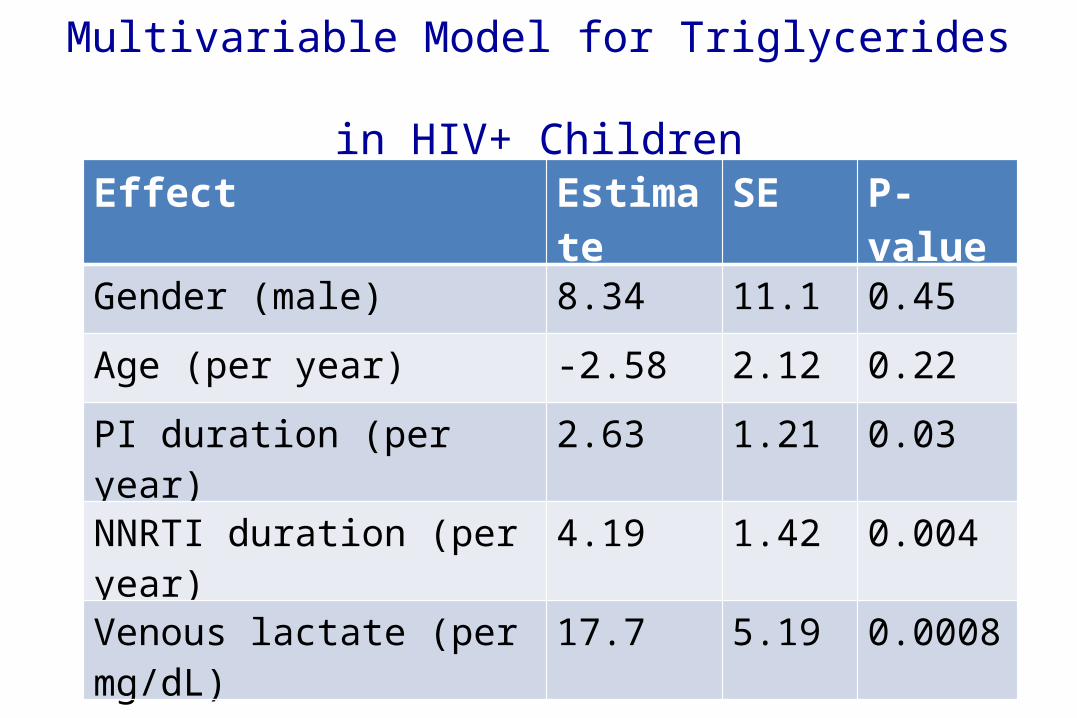
Multivariable Model for Triglycerides in HIV+ Children
Effect Estimate SE P-value
Gender (male) 8.34 11.1 0.45
Age (per year) -2.58 2.12 0.22
PI duration (per year) 2.63 1.21 0.03
NNRTI duration (per year) 4.19 1.42 0.004
Venous lactate (per mg/dL) 17.7 5.19 0.0008

Conclusions in HIV+ Children
• Insulin resistance is associated with higher lactate and pyruvate levels
• Hypertriglyceridemia is associated with higher lactate levels
• Low HDL-cholesterol is associated with lower CI and CIV enzyme activities
• Venous lactate is independently associated with higher triglyceride levels

Overall Conclusions
Mitochondrial dysfunction induced by either HIV or ARV may be responsible for the
observed metabolic changes

Acknowledgments
We thank the study participants, PHACS Community Advisory Board, Frontier Science Inc., and Westat.
PHACS is funded by:
Under cooperative agreements with Harvard School of Public Health (HD052102, 3 U01 HD052102-05S1, 3 U01 HD052102-06S3) and Tulane School of Medicine (HD052104, 3U01HD052104-06S1)

• The following institutions participated in conducting PHACS in 2011:
•Baylor College of Medicine•Bronx Lebanon Hospital Center•Children's Diagnostic & Treatment Center•Children’s Hospital, Boston•Children’s Memorial Hospital•Jacobi Medical Center•New York University School of Medicine•St. Christopher’s Hospital for Children•St. Jude Children's Research Hospital•San Juan Hospital/Department of Pediatrics•SUNY Downstate Medical Center
•Tulane University Health Sciences Center•University of Alabama, Birmingham•University of California, San Diego•University of Colorado Health Sciences Center•University of Florida/Jacksonville•University of Illinois, Chicago•University of Medicine and Dentistry of New Jersey•University of Miami•University of Southern California•University of Puerto Rico Medical Center
Acknowledgments
Funding for this study is from DHHS/NIH/NINR grant R0112885 to M. Gerschensonand T.L. Miller. We also acknowledge the support from the John A. Burns School of
Medicine, University of Hawaii at Manoa.





























