Embed Size (px)
Citation preview

Meta Analysis
Zhezhen Jin
Department of Biostatistics
Mailman School of Public Health
Columbia University
New York, NY 10032

What is meta-analysis?
Combining information
Evidence based medicine
Pulling together evidence
Systematic reviews
A statistical technique for summarizing the results of several
studies into a single estimate.

A little bit history of meta-analysis
Karl Pearson (1904) Averaged correlations for studies of the
effectiveness of inoculation for typhoid fever
R. A. Fisher (1944) When a number of quite independent tests of
significance have been made, it sometimes happens that although
few or none can be claimed individually as significant, yet the
aggregate gives an impression that the probabilities are on the
whole lower than would often have been obtained by chance Source
of the idea of cumulating probability values
W. G. Cochran (1953) Discusses a method of averaging means
across independent studies Laid-out much of the statistical
foundation that modern meta-analysis is built upon (e.g., inverse
variance weighting and homogeneity testing)

Cochrane Collaboration started in 1993 (Evidence based health
care)
Team work: based on protocol and use summary statistical
techniques
“The Cochrane Collaboration is an international network of more
than 28,000 dedicated people from over 100 countries. We work
together to help healthcare practitioners, policy-makers, patients,
their advocates and carers, make well-informed decisions about
health care, by preparing, updating, and promoting the
accessibility of Cochrane Reviews over 5,000 so far, published
online in the Cochrane Database of Systematic Reviews, part of
The Cochrane Library. We also prepare the largest collection of
records of randomised controlled trials in the world, called
CENTRAL, published as part of The Cochrane Library.”

Driven by the evidence-based medicine movement and the
Cochrane collaboration
Advantages:
Reduces bias
Replicable
Resolves controversy between conflicting findings
Provides reliable basis for decision making

How to perform meta-analysis?
1. Formulate research questions
2. Protocol development
3. Search
4. Study selection (inclusion/exclusion criteria)
5. Quality assessment
6. Data abstraction
7. Analysis
8. Summary

Example: Marfan’s syndrome
It is genetic disorder of the connective tissues
Dominant trait: FBN1
Usually tall, with long limb, leg, thin fingers
Major causes of morbidity and mortality: cardiovascular
complication of aortic dissection and rupture
In late 1960s, blood pressure lowing medication improves survival
of general patients with acute dissection of aortic aneurysms.
With the observation: Blood pressure lowering drug used to treat
patients with aortic root dilatation related to Marfan’s syndrome.
Beta blocker therapy: make heart beats more slowly and with less
force, thereby reducing blood pressure, and also help blood vessels
open up to improve blood flow.

Examples of beta blockers include:
Acebutolol (Sectral)
Atenolol (Tenormin)
Bisoprolol (Zebeta)
Metoprolol
Nadolol (Corgard)
Nebivolol (Bystolic)
Propranolol (Inderal LA)

How much effective the treatment?
Several small studies available, using echocardiography to measure
aortic root dilatation
Clinically, beta-blocker therapy is used routinely for Marfan’s
syndrome patients
Problem: No convincing evidence of long-term outcome.
Meta-analysis was performed.
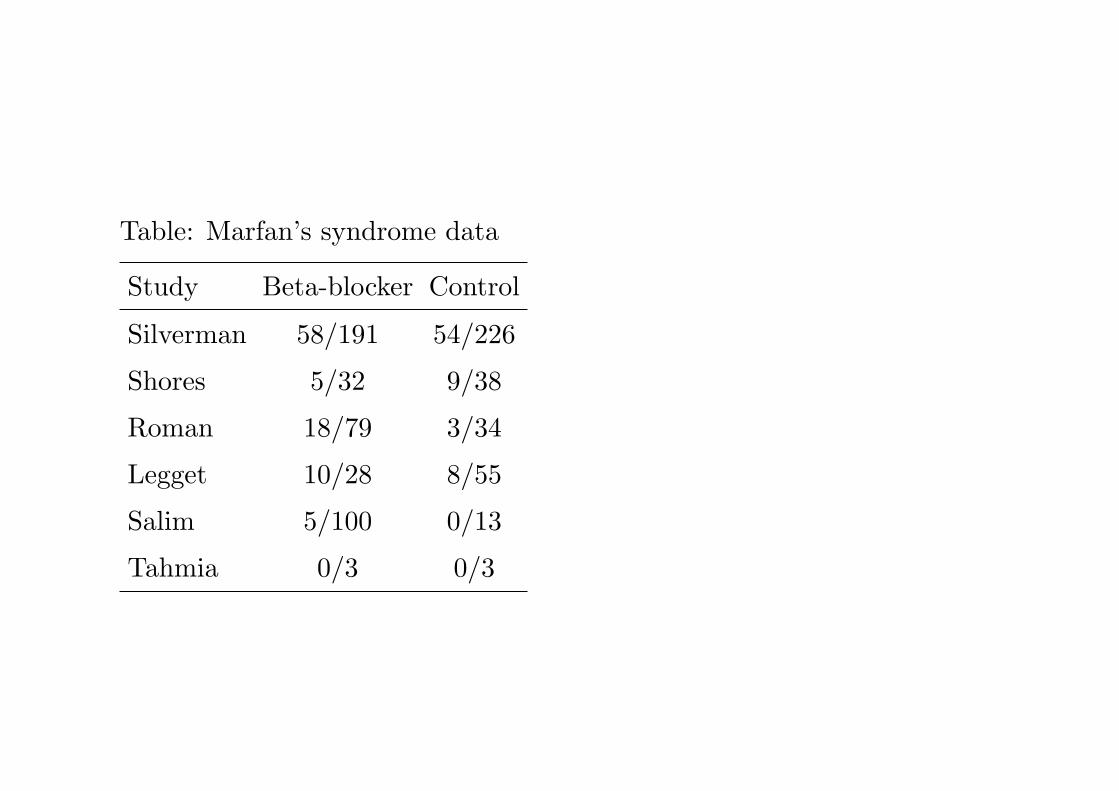
Table: Marfan’s syndrome data
Study Beta-blocker Control
Silverman 58/191 54/226
Shores 5/32 9/38
Roman 18/79 3/34
Legget 10/28 8/55
Salim 5/100 0/13
Tahmia 0/3 0/3

Study types
• Randomized clinical trials
• Observational studies ((e.g. case control, non-randomized
cohorts, cross-sectional prevalence studies, etc.)
• Combination of randomized and observational studies
• Individual patient data studies

Outcome Measures
Create a summary statistic that is comparable across all studies:
1. Binary data: alive/dead, diseased/non-diseased,
Risk difference, relative risk (risk ratio), odds ratio
2. Continuous data: weight loss, blood pressure
Mean difference, standardized mean difference, z-statistic,
p-values
3. Survival data: time to death, time to recurrence, time to
healing
Hazard ratio
4. Ordinal data (ordered categorical data): disease severity,
quality of life
may dichotomize, or treat as continuous

Binary data
Risk difference, relative risk (risk ratio), odds ratio
Table 1. Summary of binary dataRisk difference Relative risk Odds ratio
Parameter D = pT − pC RR = pT /pC OR =pT /(1−pT )pC/(1−pC )
Estimator di = pTi− pCi
ri = pTi/pCi
oi =pTi
/(1−pTi)
pCi/(1−pCi
)
Standard Error sdi=
√pTi
qTinTi
+pCi
qCinCi
slog ri=
√qTi
nTipTi
+qCi
nCipTi
slog oi=
√1a
+ 1b
+ 1c
+ 1d
where qTi = 1− pTi , nTi and nCi de denote the total number of
treated and control patients, and a, b, c, d denote the number of
observations in each cell.
Relative risk and odds ratio both use logarithmic scales

Continuous data
Required for each group: mean, standard deviation, sample size
mean difference, effect size
1. Mean difference: yi = xTi − xCi
Standard error: s2i = s2pi
(1
nTi+ 1
nCi
)where
s2pi=
(nTi − 1)s2Ti+ (nCi − 1)s2Ci
nTi + nCi − 2
2. Effect size (standardized mean difference)
Difference of means divided by the variability of the measures
δ =µT − µC
σ
δ =µT − µC
sp

Survival data
Time to event arise whenever subjects were followed over time until
the event takes place
Problem: not everyone has an event, censoring
Main effect measure: hazard ratio (HR)
HR: ratio of the risk of having an event at any given time in
treatment group over the the risk of an event in the control group.
Analysis with Cox proportional hazards models

Pooling results from different studies
Issues:
Estimates from different studies are different
Two possibilities: sampling error (homogeneous), true variation
exists among studies (heterogeneous)
If homogeneous: fixed effects model
If heterogeneous: random effects model
How to assess heterogeneity?
Cochran’s Chi-square test and I2-test, plots

Test of homogeneity
Suppose there are K studies with summary statistics θi, a
statistical test for the homogeneity
H0 : θ1 = θ2 = · · · = θK = θ
H1 : At least one θi is different
Cochran’s Chi-square test:
Q =K∑i=1
wi(yi − yw)2
where wi = 1/s2i and yw =∑K
i=1 wiyi∑Ki=1 wi
.
Q ∼ χ2K−1, the χ2 distribution with K − 1 degrees of freedom.
Alternatively,
Q =
K∑i=1
wiy2i −
(∑K
i=1 wiyi)2∑K
i=1 wi

Some comments on Cochran’s Q statistic
Power of the test might be very low due to small number of studies
When sample sizes in each study are very large, then H0 may be
rejected even when the individual effect size estimates do not
differ.
The likelihood of design flaws in primary studies and publication
biases makes the interpretation of test complex.

Higgins and Thompson’s I2
I2 = 100(Q− (K − 1))/Q
the proportion of total variability explained by heterogeneity
Values < 25% be thought to be ‘low’

The effect size: has two values, estimate and its standard error
In usual statistics: only one measure is available
Notation: (yi, si), var(yi)=s2i
Idea: yi = θ + ϵi
Fixed effects model and random effects model

Fixed Effects Model
Underlying assumptions:
All studies share common true effect size
Factors that could impact on the true effect size are the same
across studies
Observed effect sizes vary among studies only because a random
sampling error
The random sampling error can be estimated
yi = θ + ϵi
where ϵi ∼ N(0, s2i ) for i = 1, 2, · · · ,K.

The pooled estimate is given by
yw =
∑Ki=1 wiyi∑Ki=1 wi
where wi = 1/s2i .
var(yw) =1∑K
i=1 wi
Approximate 100(1− α)% confidence interval for θ is:
(yw − zα/2√var(yw), yw + zα/2
√var(yw)

Random Effects Model (DerSimonian and Laird model)
Underlying assumptions:
Studies are a random sample of a hypothetical population of
studies.
Two sources of variation: the between and within study variance.
yi = θ + δi + ϵi
where δi ∼ N(0, τ2) and ϵi ∼ N(0, s2i ) for i = 1, 2, · · · ,K. The τ2 is
assumed unknown.
The random effects model will usually generate a confidence
interval as wide or wider than that using the fixed effect model.
Results from a random effects model will usually be more
conservative (there are exceptions).

If τ2 is known, the pooled estimate of θ is given by
θ(τ) =
∑Ki=1 Wi(τ)yi∑Ki=1 Wi(τ)
where Wi(τ) = 1/(s2i + τ2).
var(θ(τ)) =1∑K
i=1 Wi(τ)
Approximate 100(1− α)% confidence interval for θ is:
(θ(τ) − zα/2
√var(θ(τ), θ(τ) + zα/2
√var(θ(τ))

As we said, τ2 is unknown, and need to be estimated.
Under normal error assumptions, maximum likelihood estimate or
restricted maximum likelihood estimate can be used.
Moment based estimate.
τ2 = max
0,Q− (K − 1)∑Ki=1 wi −
∑Ki=1 w2
i∑Ki=1 wi
.

Exploring between study heterogeneity
Random effects models account for heterogeneity between studies,
but fail to explain reasons.
Two approaches can address the issue: subgroup analyses and
meta-regression
Subgroup analyses: focus factors that are possibly different across
studies, such as patient characteristics, study conduct
Meta-regression: include covariates to the fixed and mixed effects
models. Used to estimate the impact/influence of categorical
and/or continuous covariates (moderators) on effect sizes or to
predict effect sizes in studies with specific characteristics. A ratio
of 10:1 (studies to covariates) is recommended

Publication Bias
One major concern of meta-analysis is publication bias:
1. If missing studies are random, failure to include these studies
will result in less information, wider confidence intervals, and
less powerful tests
2. If missing studies are systematically different from available
studies, then results will be biased

Reasons for publication bias:
1. Large studies are likely to be published regardless of statistical
significance
2. Moderately-sized studies are at risk for being lost, only those
with significant results might be published
3. Small studies are at the greatest risk of being lost, studies with
small sample sizes only very large effects are likely to be
significant and those with small and moderate effects are likely
to be unpublished
4. Language bias
How to assess publication bias and how to adjust it?

Funnel plot and linear regression method
Funnel plot: is a scatter plot of sample size or other measure of
precision on the y-axis versus the estimated effect size on the x-axis.
In the absence of publication bias the studies will be distributed
symmetrically about the combined effect size
In the presence of bias, the plot may become skewed, the bottom
of the plot would tend to show a higher concentration of
studies on one side of the mean than the other
This would reflect the fact that smaller studies (which appear
toward the bottom) are more likely to be published if they have
larger than average effects, which makes them more likely to
meet the criterion for statistical significance

Limitations of funnel plot:
It is informal visual method, and a useful funnel plot needs a range
of studies with varying sizes
Different people might interpret the same plot differently
Skewed funnel plot might be caused by factors other than
publication bias

Formal tests
Rank correlation test (Begg and Mazumdar):
y∗i = (yi − yw)/var(yi − yw)
where yw =∑K
i=1 wiyi∑Ki=1 wi
and wi = 1/s2i .
var(yi − yw) = s2i − 1/K∑i=1
wi
Then the rank correlation test is based on statistic
T =K∑i=1
K∑j=1
sign{y∗i − y∗j }
which is U -statistic.
Eggers linear regression method, quantifies the bias captured by
the funnel plot using the actual values of the effect sizes and their
precision
In the Egger test, the standardized effect (effect size divided by
standard error) is regressed on precision (inverse of standard error)
y∗i = yi/si, v = 1/si
Then fit weighted linear regression either with weight 1/si or
unweighted and the equation
y∗i = α+ βv.
The intercept α is used to measure asymmetry.
If it is significantly different from 0, then it is concluded that there
is evidence of publication bias.
A negative α indicates that smaller studies are associated with
bigger effects.

Small studies generally have a precision close to zero, due to their
large standard error In the absence of bias such studies would be
associated with small standardized effects and large studies
associated with large standardized effects
This would create a regression line whose intercept approaches the
origin
If the intercept deviates from this expectation, publication bias
may be the cause
This would occur when small studies are disproportionately
associated with larger effect sizes

If the publication bias is suspected, may model the selection
process into the model for bias correction. One possibility is to
view the problem as a missing data problem and assume that the
studies are missing with probabilities that are a function of their
lack of statistical significance. For example,
pi(z) =
0, if z ≤ 1.96
1, if z > 1.96
Treat pi(z) as missing probability and carry out analysis.

Meta regression
Two types of regression models are possible: fixed effects
meta-regression and random effects mete-regression model
Fixed effects meta-regression:
yi = θ +XTβ + ϵi
where ϵi ∼ N(0, s2i )
Random effects meta-regression:
yi = θ +XTβ + δi + ϵi
where δi ∼ N(0, τ2) and ϵi ∼ N(0, s2i ).

Challenging issues Studies do not report same measures. For
example, the measure for variation might be
Standard errors
Confidence intervals
Reference ranges
Interquartile ranges
Range
Significant test
P-value
‘Not significant’ or ‘P < 0.05’
Number of recurrent events

Number of recurrent events
Individual-patients meta-analysis (recent and still ongoing)

Example: Prevention of fractures after organ transplantation
Organ transplantation: Heart, kidney, lung, liver
Complications: bone loss and fractures
Impact: quality of life
Evidence: 1st year rate 37%
Bone metabolism
Treatment: bisphosphonates, active metabolites of vitamin D

Available studies: small, no definitive clinical trial
To assess differences in bone fracture among treated and untreated
patients.
Data sources and Searches
PUBMED database
MEDLINE database
Cochrane Controlled Clinical Trials Register
Unpublished abstracts for various meetings
Transplant: Kidney, Liver, Heart, Lung
Keywords: transplant, osteoporosis, bone loss, fracture, transplant
and calcitriol, transplant and bisphosphonates, transplant and
osteoporosis, transplant and fracture

Study selection
• Inclusion criteria
Randomized clinical trials, treatment and control groups, fracture
assessment
Age 18 or older
Eligible treatment: oral or IV bisphosphonates (alendronate,
risedronate, pamidronate, ibandronate, zoledronic acid) or active
vitamin D analogs (calcitriol, calcidiol, 1α-hydroxyvitamin D)
No restriction on sample size or specific dose of bisphosphonate or
active vitamin D analog.
• Exclusion criteria
Studies with historical controls were excluded.
Bone marrow transplants were excluded.
Treatments for bone loss prevention: hormone replacement therapy,
calcitonin, or resistence exercise were excluded

Two investigators extracted data on:
Study design, methods, subjects, interventions, fracture, and bone
mineral density (BMD) outcomes.
Primary outcome: vertebral or nonvertebral fracture sustained
within the first year after transplant
Radiographs of the thoracic and lumbar spine (LS) at baseline and
12 months after transplant for fractures
Secondary outcome: BMD measured by dual-energy x-ray
absorptiometry in grams per square centimeter at the LS and
femoral neck (FN)

Quality assessment
Method of randomization, presence/absence of double-blinding,
description of dropouts.
Studies were scored between 0 and 5, with 5 as the highest quality.

685 abstracts: 607 eliminated, 42 duplicate
36 remained, and among them, 28 published
9 were not adequately randomized, 8 were excluded due to delay on
treatment and no response from the authors
Included: 11 studies with 780 participants

Prophylactic use of lidocaine after heart attack
Study Lidocaine Control
1. Chopra 2/39 1/43
2. Mogensen 4/44 4/44
3. Pitt 6/107 4/110
4. Darby 7/103 5/100
5. Bennett 7/110 3/106
6. O’Brian 11/154 4/146
Total 37/557 21/549
Source: Hine, L.K., Laird, N., Hewitt, P. and Chalmers, T.C.
(1989) Meta-analytic evidence against prophylactic use of lidocaine
in Myocardial Infarction, Archives of Internal Medicine, 149,
2694-2698.

RCTs comparing NaF and SMFP
Sodium fuoride (NaF) with sodium monoflouorophosphate (SMFP)
dentrifrices for the purpose of reducing dental decay.
The outcome: decayed, missing or filled teeth score (DMFS)
Study n NaF n SMFP
1 134 5.96 (4.24) 113 6.82 (4.72)
2 175 4.74 (4.64) 151 5.07 (5.38)
3 137 2.04 (2.59) 140 2.51 (3.22)
4 184 2.70 (2.32) 179 3.20 (2.46)
5 174 6.09 (4.86) 169 5.81 (5.14)
6 754 4.72 (5.33) 736 4.76 (5.29)
7 209 10.10 (8.10) 209 10.90 (7.90)
8 1151 2.82 (3.05) 1122 3.01 (3.32)
9 679 3.88 (4.85) 673 4.37 (5.37)

Source: Johnson, M.F. (1993) Comparative efficacy of NaF and
SMFP dentrifrices in caries prevention: a meta-analytic overview,
Caries Res., 27, 328-336.





























