-
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6 JUNE
2008 431
ESTEBAN WALKER, PhDDepartment of Quantitative HealthSciences,
Cleveland Clinic
Meta-analysis:Its strengths and limitations
REVIEW
ABSTRACTNowadays, doctors face an overwhelming amount
ofinformation, even in narrow areas of interest. In
response,reviews designed to summarize the large volumes
ofinformation are frequently published. When a review isdone
systematically, following certain criteria, and theresults are
pooled and analyzed quantitatively, it is calleda meta-analysis. A
well-designed meta-analysis canprovide valuable information for
researchers, policy-makers, and clinicians. However, there are many
criticalcaveats in performing and interpreting them, and thusmany
ways in which meta-analyses can yield misleadinginformation.
KEY POINTSMeta-analysis is an analytical technique designed
tosummarize the results of multiple studies.
By combining studies, a meta-analysis increases thesample size
and thus the power to study effects ofinterest.
There are many caveats in performing a valid meta-analysis, and
in some cases a meta-analysis is notappropriate and the results can
be misleading.
HE AMOUNT OF INFORMATION generatedin medical research is
becoming over-
whelming, even for experienced researchers.New studies are
constantly being published,and clinicians are finding it nearly
impossibleto stay current, even in their own area of
spe-cialty.
To help make sense of the information, weare seeing more and
more review articles thatpool the results of multiple studies. When
cer-tain principles are followed and the data arequantitatively
analyzed, these reviews arecalled meta-analyses. A PubMed search of
theword meta-analysis in the title yielded 1,473articles in the
year 2007.
Combining available information to gen-erate an integrated
result seems reasonableand can save a considerable amount
ofresources. Nowadays, meta-analyses are beingused to design future
research, to provide evi-dence in the regulatory process,1 and even
tomodify clinical practice.
Meta-analysis is powerful but also contro-versialcontroversial
because several condi-tions are critical to a sound meta-analysis,
andsmall violations of those conditions can leadto misleading
results. Summarizing largeamounts of varied information using a
singlenumber is another controversial aspect ofmeta-analysis. Under
scrutiny, some meta-analyses have been inappropriate, and
theirconclusions not fully warranted.2,3
This article introduces the basic conceptsof meta-analysis and
discusses its caveats, withthe aim of helping clinicians assess the
meritsof the results. We will use several recent meta-analyses to
illustrate the issues, including acontroversial one4 with
potentially far-reach-ing consequences.
T
ADRIAN V. HERNANDEZ, MD, PhDDepartment of Quantitative Health
Sciences,Cleveland Clinic
MICHAEL W. KATTAN, PhDDepartment of Quantitative Health
Sciences,Cleveland ClinicCREDIT
CME
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
432 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6
JUNE 2008
OBJECTIVES OF META-ANALYSIS
The main objectives of a meta-analysis are to: Summarize and
integrate results from a
number of individual studies Analyze differences in the results
among
studies Overcome small sample sizes of individual
studies to detect effects of interest, andanalyze end points
that require larger sam-ple sizes
Increase precision in estimating effects Evaluate effects in
subsets of patients Determine if new studies are needed to
further investigate an issue Generate new hypotheses for future
studies.
These lofty objectives can only beachieved when the
meta-analysis satisfactorilyaddresses certain critical issues,
which we willdiscuss next.
CRITICAL ISSUESIN META-ANALYSIS DESIGN
Four critical issues need to be addressed in ameta-analysis:
Identification and selection of studies Heterogeneity of results
Availability of information Analysis of the data.
IDENTIFICATIONAND SELECTION OF STUDIES
The outcome of a meta-analysis depends onthe studies included.
The critical aspect ofselecting studies to be included in a
meta-analysis consists of two phases. The first is
theidentification phase or literature search, inwhich potential
studies are identified. In thesecond phase, further criteria are
used to createa list of studies for inclusion. Three
insidiousproblems plague this aspect of meta-analysis:publication
bias and search bias in the identifi-cation phase, and selection
bias in the selec-tion phase. These biases are discussed below.
Publication bias: Positive studiesare more likely to be
printedSearches of databases such as PubMed orEmbase can yield long
lists of studies. However,these databases include only studies that
have
been published. Such searches are unlikely toyield a
representative sample because studiesthat show a positive result
(usually in favor ofa new treatment or against a
well-establishedone) are more likely to be published than thosethat
do not. This selective publication of stud-ies is called
publication bias.
In a recent article, Turner et al5 analyzedthe publication
status of studies of antidepres-sants. Based on studies registered
with the USFood and Drug Administration (FDA), theyfound that 97%
of the positive studies werepublished vs only 12% of the negative
ones.Furthermore, when the nonpublished studieswere not included in
the analysis, the positiveeffects of individual drugs increased
between11% and 69%.
One reason for publication bias is thatdrug manufacturers are
not generally interest-ed in publishing negative studies.
Anothermay be that editors favor positive studiesbecause these are
the ones that make theheadlines and give the publication
visibility.In some medical areas, the exclusion of studiesconducted
in non-English-speaking countriescan increase publication
bias.6
To ameliorate the effect of publicationbias on the results of a
meta-analysis, a seriouseffort should be made to identify
unpublishedstudies. Identifying unpublished studies is eas-ier now,
thanks to improved communicationbetween researchers worldwide, and
thanks toregistries in which all the studies of a certaindisease or
treatment are reported regardless ofthe result.
The National Institutes of Health main-tains a registry of all
the studies it supports,and the FDA keeps a registry and database
inwhich drug companies must register all trialsthey intend to use
in applying for marketingapproval or a change in labeling. Banks
ofpublished and unpublished trials supported bypharmaceutical
companies are also available(eg, http://ctr.gsk.co.uk/welcome.asp).
TheCochrane collaboration (www.cochrane.org/)keeps records of
systematic reviews and meta-analyses of many diseases and
procedures.
Search bias: Identifying relevant studiesEven in the ideal case
that all relevant studieswere available (ie, no publication bias),
afaulty search can miss some of them. In
META-ANALYSIS WALKER AND COLLEAGUES
Even smallviolations ofthe rules ofmeta-analysiscan lead
tomisleadingresults
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
searching databases, much care should betaken to assure that the
set of key words usedfor searching is as complete as possible.
Thisstep is so critical that most recent meta-analy-ses include the
list of key words used. Thesearch engine (eg, PubMed, Google) is
alsocritical, affecting the type and number of stud-ies that are
found.7 Small differences in searchstrategies can produce large
differences in theset of studies found.8
Selection bias:Choosing the studies to be includedThe
identification phase usually yields a longlist of potential
studies, many of which are notdirectly relevant to the topic of the
meta-analysis. This list is then subject to additionalcriteria to
select the studies to be included.This critical step is also
designed to reduce dif-ferences among studies, eliminate
replicationof data or studies, and improve data quality,and thus
enhance the validity of the results.
To reduce the possibility of selection biasin this phase, it is
crucial for the criteria to beclearly defined and for the studies
to be scoredby more than one researcher, with the finallist chosen
by consensus.9,10 Frequently usedcriteria in this phase are in the
areas of: Objectives Populations studied Study design (eg,
experimental vs obser-
vational) Sample size Treatment (eg, type and dosage) Criteria
for selection of controls Outcomes measured Quality of the data
Analysis and reporting of results Accounting and reporting of
attrition
rates Length of follow-up When the study was conducted.
The objective in this phase is to selectstudies that are as
similar as possible withrespect to these criteria. It is a fact
that evenwith careful selection, differences among stud-ies will
remain. But when the dissimilaritiesare large it becomes hard to
justify pooling theresults to obtain a unified conclusion.
In some cases, it is particularly difficult tofind similar
studies,10,11 and sometimes thediscrepancies and low quality of the
studies
can prevent a reasonable integration ofresults. In a systematic
review of advancedlung cancer, Nicolucci et al12 decided not topool
the results, in view of systematic quali-tative inadequacy of
almost all trials and lackof consistency in the studies and their
meth-ods. Marsoni et al13 came to a similar conclu-sion in
attempting to summarize results inadvanced ovarian cancer.
Stratification is an effective way to dealwith inherent
differences among studies andto improve the quality and usefulness
of theconclusions. An added advantage to stratifica-tion is that
insight can be gained by investi-gating discrepancies among
strata.
There are many ways to create coherentsubgroups of studies. For
example, studies canbe stratified according to their
quality,assigned by certain scoring systems. Commonlyused systems
award points on the basis of howpatients were selected and
randomized, thetype of blinding, the dropout rate, the
outcomemeasurement, and the type of analysis
(eg,intention-to-treat). However, these criteria,and therefore the
scores, are somewhat subjec-tive. Moher et al14 expand on this
issue.
Large differences in sample sizes amongstudies are not uncommon
and can causeproblems in the analysis. Depending on thetype of
model used (see below), meta-analysescombine results based on the
size of eachstudy, but when the studies vary significantlyin size,
the large studies can still have anunduly large influence on the
results.Stratifying by sample size is done sometimes toverify the
stability of the results.4
On the other hand, the presence of dis-similarities among
studies can have advan-tages by increasing the generalizability of
theconclusions. Berlin and Colditz1 point outthat we gain strength
in inference when therange of patient characteristics has
beenbroadened by replicating findings in studieswith populations
that vary in age range, geo-graphic region, severity of underlying
illness,and the like.
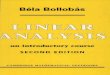
Funnel plot: Detecting biases in theidentification and selection
of studiesThe funnel plot is a technique used to inves-tigate the
possibility of biases in the identifi-cation and selection phases.
In a funnel plot
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6 JUNE
2008 433
Exclusion ofnonpublishedstudiesincreasesselection bias
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
434 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6
JUNE 2008
the size of the effect (defined as a measure ofthe difference
between treatment and control)in each study is plotted on the
horizontal axisagainst standard error15 or sample size9 on
thevertical axis. If there are no biases, the graph
will tend to have a symmetrical funnel shapecentered in the
average effect of the studies.When negative studies are missing,
the graphshows lack of symmetry.
Funnel plots are appealing because theyare simple, but their
objective is to detect acomplex effect, and they can be
misleading.For example, lack of symmetry in a funnel plotcan also
be caused by heterogeneity in thestudies.16 Another problem with
funnel plotsis that they are difficult to interpret when thenumber
of studies is small. In some cases, how-ever, the researcher may
not have any optionbut to perform the analysis and report
thepresence of bias.11
Dentali et al17 conducted a meta-analysisto study the effect of
anticoagulant treatmentto prevent symptomatic venous
thromboem-bolism in hospitalized patients. The conclu-sion was that
the treatment was effective toprevent symptomatic pulmonary
thromboem-bolism, with no significant increase in majorbleeding.
FIGURE 1 shows the funnel plots for thetwo outcomes. Dentali et
al17 concluded thatthe lack of symmetry in the top plot suggests
alack of inclusion of small studies showing anincrease in the risk
of pulmonary thromboem-bolism, and thus, bias. The bottom plot
showsthe symmetry of the funnel plot for majorbleeding, suggesting
absence of bias.
HETEROGENEITY OF RESULTS
In meta-analysis, heterogeneity refers to thedegree of
dissimilarity in the results of individualstudies. In some cases,
the dissimilarities inresults can be traced back to inherent
differ-ences in the individual studies. In other situa-tions,
however, causes for the dissimilaritiesmight not be easy to
elucidate. In any case, asthe level of heterogeneity increases, the
justifi-cation for an integrated result becomes more dif-ficult. A
tool that is very effective to display thelevel of heterogeneity is
the forest plot. In a for-est plot, the estimated effect of each
study alongwith a line representing a confidence interval isdrawn.
When the effects are similar, the confi-dence intervals overlap,
and heterogeneity islow. The forest plot includes a reference line
atthe point of no effect (eg, one for relative risksand odds
ratios). When some effects lie onopposite sides of the reference
line, it means
META-ANALYSIS WALKER AND COLLEAGUES
0.01
0.0
0.4
0.8
1.2
1.6
0.1 1
Stan
dar
d e
rro
rSt
and
ard
err
or
10 100
0.01
0.0
0.4
0.8
1.2
1.6
0.1 1 10 100
Relative risk (fixed)
Relative risk (fixed)
The funnel plot, a way to detectpossible selection bias
FIGURE 1. Top, a funnel plot of studies of anticoagu-lant
prophylaxis that measured the outcome of symp-tomatic pulmonary
embolism. The plot is asymmetri-cal, suggesting that small studies
in which prophylaxiswas associated with an increased risk are
missing.Bottom, a funnel plot of studies with the outcome ofmajor
bleeding is symmetrical, suggesting absence ofselection bias.
DENTALI F, DOUKELIS D, GIANNI M, ET AL. META-ANALYSIS:
ANTICOAGULANT PROPHYLAXIS TOPREVENT SYMPTOMATIC VENOUS
THROMBOEMBOLISM IN HOSPITALIZED MEDICAL PATIENTS.
ANN INTERN MED 2007; 146:278288.
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
that the studies are contradictory and hetero-geneity is high.
In such cases, the conclusions ofa meta-analysis are
compromised.
The previously mentioned study byDentali et al17 presented
several forest plotsthat display the level of heterogeneity of
vari-ous outcomes. FIGURE 2 shows the forest plot forthe outcome of
pulmonary embolism. Exceptfor one, the estimated effects are on the
sameside of the unit line and the confidence inter-vals overlap to
a large extent. This plot showsa low level of heterogeneity. FIGURE
3 shows theforest plot for major bleeding. Here the effectsare on
both sides of the unit line, implying ahigh level of heterogeneity.
Cochrans Q testis a statistical test used in conjunction withthe
forest plot to determine the significance ofheterogeneity among
studies.18
Gebski et al19 performed a meta-analysisof randomized controlled
trials comparing thesurvival of patients with esophageal carcino-ma
who received neoadjuvant chemotherapyvs those who underwent surgery
alone. In onlyone of the eight studies included was neoadju-vant
chemotherapy significantly beneficial.Three of the studies
suggested that it washarmful, although the effects were not
statisti-cally significant. The pooled result was mar-ginally
significant in favor of the treatment (P= .05). This positive
result was due largely tothe fact that the only study with a
significant-ly positive result study also was, by far, thelargest
(with 400 patients in each treatmentgroup, vs an average of 68 per
treatment groupfor the rest). Even though the test for
hetero-geneity was not significant, the marginal Pvalue and the
differences in study size makethe results of this meta-analysis
suspect.
AVAILABILITY OF INFORMATION
Most reports of individual studies includeonly summary results,
such as means, stan-dard deviations, proportions, odds ratios,
andrelative risks. Other than the possibility oferrors in
reporting, the lack of informationcan severely limit the type of
analyses andconclusions that can be reached in a meta-analysis. For
example, lack of informationfrom individual studies can preclude
thecomparison of effects in predetermined sub-groups of
patients.
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6 JUNE
2008 435
Study, Year
Belch et al, 1981
Dahan et al, 1986
Samama et al, 1999
Leizorovic et al, 2004
Cohen et al, 2006
Lederle et al, 2006
Total (95% CI)
Total events
Prophylaxis,n/n
Placebo,n/n
10.10.01
Favors treatment Favors control
0.001 10 100 1000
Mahe et al, 2005
0/50
1/132
0/291
5/1759
0/429
1/140
10/1230
0.20 (0.01 - 4.06)
0.33 (0.03 - 3.14)
0.14 (0.01 - 2.73)
1.24 (0.33 - 4.60)
0.59 (0.27 - 1.29)
0.33 (0.04 - 3.17)
0.43 (0.26 - 0.71)
0.09 (0.00 - 1.60)
2/50
3/131
3/288
Gardlund et al, 1996 3/5776 0.26 (0.07 - 0.91)12/5917
4/1740
5/420
3/140
20 49
17/1244
RR (fixed) (95% Cl)
RR (fixed) (95% Cl)
A low level of heterogeneity:Anticoagulation prevents
pulmonaryembolism
FIGURE 2. A forest plot of studies of anticoagulantprophylaxis
with the outcome of pulmonary embolism.All except one of the
studies show a better outcomewith treatment than with placebo,
indicating a lowlevel of heterogeneity among the studies.
DENTALI F, DOUKELIS D, GIANNI M, ET AL. META-ANALYSIS:
ANTICOAGULANT PROPHYLAXIS TOPREVENT SYMPTOMATIC VENOUS
THROMBOEMBOLISM IN HOSPITALIZED MEDICAL PATIENTS.
ANN INTERN MED 2007; 146:278288.
Study, Year
Dahan et al, 1986
Samama et al, 1999
Fraisse et al, 2000
Leizorovic et al, 2004
Cohen et al, 2006
Lederle et al, 2006
Total (95% CI)
Total events
Prophylaxis,n/n
Placebo,n/n
10.10.01
Favors treatment Favors control
0.001 10 100 1000
Mahe et al, 2005
1/132
6/360
6/108
8/1856
1/425
2/140
1/1230
0.33 (0.03 - 3.14)
1.51 (0.43 - 5.30)
2.09 (0.54 - 8.16)
16.95 (0.98 - 293.36)
0.34 (0.04 - 3.24)
0.40 (0.08 - 2.03)
1.32 (0.73 - 2.37)
0.97 (0.06 - 15.52)
3/131
4/362
3/113
0/1850
1/414
5/140
25 19
3/1244
RR (fixed) (95% Cl)
RR (fixed) (95% Cl)
A high level of heterogeneity:Does anticoagulation increasethe
risk of major bleeding?
FIGURE 3. Risk of major bleeding in studies of anticoagu-lant
prophylaxis. Some of the studies favor the controland others the
treatment. This represents a high level ofheterogeneity
DENTALI F, DOUKELIS D, GIANNI M, ET AL. META-ANALYSIS:
ANTICOAGULANT PROPHYLAXIS TOPREVENT SYMPTOMATIC VENOUS
THROMBOEMBOLISM IN HOSPITALIZED MEDICAL PATIENTS. ANN
INTERN MED 2007; 146:278288.
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
META-ANALYSIS WALKER AND COLLEAGUES
436 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6
JUNE 2008
The best scenario is when data at thepatient level are
available. In such cases, theresearcher has great flexibility in
the analysisof the information. Trivella et al20 performed
ameta-analysis of the value of microvessel den-sity in predicting
survival in non-small-celllung cancer. They obtained information
onindividual patients by contacting researchcenters directly. The
data allowed them tovary the cutoff point to classify
microvesseldensity as high or low and to use statisticalmethods to
ameliorate heterogeneity.
A frequent problem in meta-analysis isthe lack of uniformity in
how outcomes aremeasured. In the study by Trivella et al,20
themicrovessel density was measured by twomethods. The microvessel
density was a signif-icant prognostic factor when measured by oneof
the methods, but not the other.
RANDOMIZED CONTROLLED TRIALSVS OBSERVATIONAL STUDIES
Some researchers believe that meta-analysesshould be conducted
only on randomized con-trolled trials.3,21 Their reasoning is that
meta-analyses should include only reasonably well-conducted studies
to reduce the risk of a mis-leading conclusion. However, many
importantdiseases can only be studied observationally. Ifthese
studies have a certain level of quality,there is no technical
reason not to includethem in a meta-analysis.
Gillum et al22 performed a meta-analysispublished in 2000 on the
risk of ischemicstroke in users of oral contraceptives, based
onobservational studies (since no randomizedtrials were available).
Studies were identifiedand selected by multiple researchers
usingstrict criteria to make sure that only studiesfulfilling
certain standards were included. Of804 potentially relevant studies
identified,only 16 were included in the final analysis. Afunnel
plot showed no evidence of bias andthe level of heterogeneity was
fairly low. Themeta-analysis result confirmed the results
ofindividual studies, but the precision withwhich the effect was
estimated was muchhigher. The overall relative risk of stroke
inwomen taking oral contraceptives was 2.75,with a 95% confidence
interval of 2.24 to3.38.
A more recent meta-analysis23 (publishedin 2004) on the same
issue found no signifi-cant increase in the risk of ischemic
strokewith the use of oral contraceptives. Gillumand Johnston24
suggest that the main reasonfor the discrepancy is the lower amount
ofestrogen in newer oral contraceptives. Theyalso point out
differences in the control groupsand study outcomes as reasons for
the discrep-ancies between the two studies.
Bhutta et al25 performed a meta-analysisof case-control
(observational) studies of theeffect of preterm birth on cognitive
andbehavioral outcomes. Studies were includedonly if the children
were evaluated after theirfifth birthday and the attrition rate was
lessthan 30%. The studies were grouped accord-ing to criteria of
quality devised specifically forcase-control studies. The
high-quality studiestended to show a larger effect than the
low-quality studies, but the difference was not sig-nificant.
Seventeen studies were included, andall of them found that children
born pretermhad lower cognitive scores; the difference
wasstatistically significant in 15 of the studies. Asexpected, the
meta-analysis confirmed thesefindings (95% confidence interval for
the dif-ference 9.212.5). The number of patients(1,556 cases and
1,720 controls) in the meta-analysis allowed the researchers to
concludefurther that the mean cognitive scores weredirectly
proportional to the mean birth weight(R2 = 0.51, P < .001) and
gestational age (R2= 0.49, P < .001).
ANALYSIS OF DATA
There are specific statistical techniques thatare used in
meta-analysis to analyze and inte-grate the information. The data
from the indi-vidual studies can be analyzed using either oftwo
models: fixed effects or random effects.
The fixed-effects model assumes that thetreatment effect is the
same across studies.This common effect is unknown, and the pur-pose
of the analysis is to estimate it with moreprecision than in the
individual studies.
The random-effects model, on the otherhand, assumes that the
treatment effect is notthe same across studies. The goal is to
estimatethe average effect in the studies.
In the fixed-effects model, the results of
Data-mininggreatlyincreases therisk of false-positive
results
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
individual studies are pooled using weightsthat depend on the
sample size of the study,whereas in the random-effects model
eachstudy is weighted equally. Due to the hetero-geneity among
studies, the random-effectsmodel yields wider confidence
intervals.
Both models have pros and cons. In manycases, the assumption
that the treatmenteffect is the same in all the studies is not
ten-able, and the random-effects model is prefer-able. When the
effect of interest is large, theresults of both models tend to
agree, particu-larly when the studies are balanced (ie, theyhave a
similar number of patients in the treat-ment group as in the
control group) and thestudy sizes are similar. But when the effect
issmall or when the level of heterogeneity ofthe studies is high,
the result of the meta-analysis is likely to depend on the model
used.In those cases, the analysis should be doneand presented using
both models.
It is highly desirable for a meta-analysis toinclude a
sensitivity analysis to determine therobustness of the results. Two
common waysto perform sensitivity analysis are to analyzethe data
using various methods and to presentthe results when some studies
are removedfrom the analysis.26 If these actions cause seri-ous
changes in the overall results, the credi-bility of the results is
compromised.
The strength of meta-analysis is that, bypooling many studies,
the effective sample sizeis greatly increased, and consequently
morevariables and outcomes can be examined. Forexample, analysis in
subsets of patients andregression analyses9 that could not be done
inindividual trials can be performed in a meta-analysis.
A word of caution should be given withrespect to larger samples
and the possibility ofmultiple analyses of the data in
meta-analysis.Much care must be exercised when examin-ing the
significance of effects that are notconsidered prior to the
meta-analysis. Thetesting of effects suggested by the data andnot
planned a priori (sometimes called data-mining) increases
considerably the risk offalse-positive results. One common
problemwith large samples is the temptation to per-form many
so-called subgroup analyses inwhich subgroups of patients formed
accordingto multiple baseline characteristics are com-
pared.27 The best way to minimize the possi-bility of
false-positive results is to determinethe effects to be tested
before the data are col-lected and analyzed. Another method is
toadjust the P value according to the number ofanalyses performed.
In general, post hocanalyses should be deemed exploratory, andthe
reader should be made aware of this factin order to judge the
validity of the conclu-sion.
META-ANALYSIS OF RARE EVENTS
Lately, meta-analysis has been used to analyzeoutcomes that are
rare and that individualstudies were not designed to test. In
general,the sample size of individual studies providesinadequate
power to test rare outcomes.Adverse events are prime examples of
impor-tant rare outcomes that are not always formal-ly analyzed
statistically. The problem in theanalysis of adverse events is
their low inci-dence. Paucity of events causes serious prob-lems in
any statistical analysis (see Shuster etal28). The reason is that,
with rare events,small changes in the data can cause
dramaticchanges in the results. This problem can per-sist even
after pooling data from many studies.Instability of results is also
exacerbated by theuse of relative measures (eg, relative risk
andodds ratio) instead of absolute measures of risk(eg, risk
difference).
In a controversial meta-analysis, Nissenand Wolski4 combined 42
studies to examinethe effect of rosiglitazone (Avandia) on therisk
of myocardial infarction and death fromcardiovascular causes. The
overall estimatedincidence of myocardial infarction in thetreatment
groups was 0.006 (86/14,376), or 6in 1,000. Furthermore, 4 studies
did not haveany occurrences in either group, and 2 of the42 studies
accounted for 28.4% of the patientsin the study.
Using a fixed-effect model, the odds ratiowas 1.42, ie, the odds
of myocardial infarctionwas 42% higher in patients using
rosiglita-zone, and the difference was statistically sig-nificant
(95% confidence interval 1.031.98).Given the low frequency of
myocardial infarc-tion, this translates into an increase of
only1.78 myocardial infarctions per 1,000 patients(from 4.22 to 6
per 1,000). Furthermore,
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6 JUNE
2008 437
With rareeffects, evena smalldifferencecan seem large
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
REFERENCES1. Berlin JA, Colditz GA. The role of meta-analysis in
the regulatory process
for food, drugs, and devices. JAMA 1999; 281:830834.2. Bailar
JC. The promise and problems of meta-analysis. N Engl J Med
1997; 337:559561.3. Simon R. Meta-analysis of clinical trials:
opportunities and limitations. In:
Stangl DK, Berry DA, editors. Meta-Analysis in Medicine and
HealthPolicy. New York: Marcel Dekker, 2000.
4. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of
myocardialinfarction and death from cardiovascular causes. N Engl J
Med 2007;356:24572471.
5. Turner EH, Matthews AM, Linardatos E, et al. Selective
publication ofantidepressant trials and its influence on apparent
efficacy. N Engl J Med2008; 358:252260.
6. LeLorier J, Grgoire G, Benhaddad A, Lapierre J, Derderian
F.Discrepancies between meta-analyses and subsequent large
randomized,
438 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6
JUNE 2008
when the data were analyzed using othermethods or if the two
large studies wereremoved, the effect became nonsignificant.29
Nissen and Wolskis study4 is valuable andraises an important
issue. However, the med-ical community would have been better
servedif a sensitivity analysis had been presented tohighlight the
fragility of the conclusions.
META-ANALYSIS VS LARGE RANDOMIZEDCONTROLLED TRIALS
There is debate about how meta-analysescompare with large
randomized controlled tri-als. In situations where a meta-analysis
and asubsequent large randomized controlled trialare available,
discrepancies are not uncom-mon.
LeLorier et al6 compared the results of19 meta-analyses and 12
subsequent largerandomized controlled trials on the sametopics. In
5 (12%) of the 40 outcomes stud-ied, the results of the trials were
significant-ly different than those of the meta-analysis.The
authors mentioned publication bias,study heterogeneity, and
differences in pop-ulations as plausible explanations for
thedisagreements. However, they correctlycommented: this does not
appear to be alarge percentage, since a divergence in 5percent of
cases would be expected on thebasis of chance alone.6
A key reason for discrepancies is thatmeta-analyses are based on
heterogeneous,often small studies. The results of a meta-analysis
can be generalized to a target popula-tion similar to the target
population in each ofthe studies. The patients in the
individualstudies can be substantially different withrespect to
diagnostic criteria, comorbidities,severity of disease, geographic
region, and thetime when the trial was conducted, amongother
factors. On the other hand, even in alarge randomized controlled
trial, the targetpopulation is necessarily more limited. These
differences can explain many of the disagree-ments in the
results.
A large, well-designed, randomized con-trolled trial is
considered the gold standard inthe sense that it provides the most
reliableinformation on the specific target populationfrom which the
sample was drawn. Withinthat population the results of a
randomizedcontrolled trial supersede those of a meta-analysis.
However, a well conducted meta-analysis can provide complementary
informa-tion that is valuable to a researcher, clinician,or
policy-maker.
CONCLUSION
Like many other statistical techniques,meta-analysis is a
powerful tool when usedjudiciously; however, there are manycaveats
in its application. Clearly, meta-analysis has an important role in
medicalresearch, public policy, and clinical prac-tice. Its use and
value will likely increase,given the amount of new knowledge,
thespeed at which it is being created, and theavailability of
specialized software for per-forming it.30
A meta-analysis needs to fulfill several keyrequirements to
ensure the validity of itsresults: Well-defined objectives,
including precise
definitions of clinical variables and out-comes
An appropriate and well-documentedstudy identification and
selection strategy
Evaluation of bias in the identificationand selection of
studies
Description and evaluation of hetero-geneity
Justification of data analytic techniques Use of sensitivity
analysis.
It is imperative that researchers, policy-makers, and clinicians
be able to criticallyassess the value and reliability of the
conclu-sions of meta-analyses.
META-ANALYSIS WALKER AND COLLEAGUES
Randomizedtrials are thegold standard,but
meta-analysesprovidevaluablecomplementaryinformation
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from
-
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 75 NUMBER 6 JUNE
2008 439
controlled trials. N Engl J Med 1997; 337:536542.7. Steinbrook
R. Searching for the right searchreaching the medical liter-
ature. N Engl J Med 2006; 354:47.8. Dickersin K, Scherer R,
Lefebvre C. Systematic reviews: identifying rele-
vant studies for systematic reviews. BMJ 1994; 309:12861291.9.
De Luca G, Suryapranta H, Stone GW, et al. Coronary stenting versus
bal-
loon angioplasty for acute myocardial infarction: a
meta-regressionanalysis of randomized trials. Int J Cardiol
2007;doi:10.1016/j.ijcard.2007.03.112
10. Ng TT, McGory ML, Ko CY, et al. Meta-analysis in surgery.
Arch Surg 2006;141:11251130.
11. Ray CE, Prochazka A. The need for anticoagulation following
inferiorvena cava filter placement: systematic review. Cardiovasc
InterventRadiol 2007; 31:316324.
12. Nicolucci A, Grilli R, Alexanian AA, Apolone G, Torri V,
Liberati A. Qualityevolution and clinical implications of
randomized controlled trials on thetreatment of lung cancer. A lost
opportunity for meta-analysis. JAMA1989; 262:21012107.
13. Marsoni S, Torri V, Taiana A. Critical review of the quality
and develop-ment of randomized clinical trials and their influence
on the treatmentof advanced epithelial ovarian cancer. Ann Oncol
1990; 1:343350.
14. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF.
Improvingthe quality of reports of meta-analyses of randomised
controlled trials:the QUOROM statement. Quality of Reporting of
Meta-analyses. Lancet1999; 354:18961900.
15. Gami AS, Witt BJ, Howard DE, et al. Metabolic syndrome and
risk of inci-dent cardiovascular events and death. J Am Coll
Cardiol 2007; 49:403414.
16. Terrin N, Schmid CH, Lau J, Olkin I. Adjusting for
publication bias in thepresence of heterogeneity. Stat Med 2003;
22:21132126.
17. Dentali F, Doukelis D, Gianni M, et al. Meta-analysis:
anticoagulant pro-phylaxis to prevent symptomatic venous
thromboembolism in hospital-ized medical patients. Ann Intern Med
2007; 146:278288.
18. Whitehead A. Meta-Analysis of Controlled Clinical Trials.
New York:Wiley, 2002.
19. Gebski V, Burmeister B, Smithers BM, et al. Survival
benefits from neoad-juvant chemoradiotherapy or chemotherapy in
oesophageal carcinoma:a meta-analysis. Lancet Oncology 2007;
8:226234.
20. Trivella M, Pezzella F, Pastorino U, et al. Microvessel
density as a prognos-tic factor in non-small-cell lung carcinoma: a
meta-analysis of individualpatient data. Lancet Oncology 2007;
8:488499.
21. Kunz R, Vist G, Oxman AD. Randomisation to protect against
selectionbias in healthcare trials (Cochrane Methodology Review).
In: TheCochrane Library, Issue 1, 2003. Oxford: Update
Software.
22. Gillum LA, Mamidipudi SK, Johnston SC. Ischemic stroke risk
with oralcontraceptives: a meta-analysis. JAMA 2000; 284:7278.
23. Chan WS, Ray J, Wai EK, et al. Risk of stroke in women
exposed to low-dose oral contraceptives. Arch Intern Med 2004;
164:741747.
24. Gillum LA, Johnston SC. Oral contraceptives and stroke risk:
the debatecontinues. Lancet 2004; 3:453454.
25. Bhutta AT, Cleves MA, Casey PH, et al. Cognitive and
behavioral out-comes of schoolaged children who were born preterm.
JAMA 2002;288:728737.
26. De Luca G, Suryapranta H, Stone GW, et al. Adjunctive
mechanicaldevices to prevent distal embolization in patients
undergoing mechani-cal revascularization for acute myocardial
infarction: a meta-analysis ofrandomized trials. Am Heart J 2007;
153:343353.
27. Wang R, Lagakos SW, Ware JH, et al. Statistics in
medicinereporting ofsubgroup analyses in clinical trials. N Engl J
Med 2007; 357:21892194.
28. Shuster JJ, Jones LS, Salmon DA. Fixed vs random effects
meta-analysis inrare events: the rosiglitazone link with myocardial
infarction and cardiacdeath. Stat Med 2007; 26:43754385.
29. Bracken MB. Rosiglitazone and cardiovascular risk. N Engl J
Med 2007;357:937938.
30. Sutton AJ, Lambert PC, Hellmich M, et al. Meta-analysis in
practice: a crit-ical review of available software. In: Stangl DK,
Berry DA, editors. Meta-Analysis in Medicine and Health Policy. New
York: Marcel Dekker, 2000.
ADDRESS: Esteban Walker, PhD, Quantitative Health Sciences,
Wb4,Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195;
[email protected].
WeWelcome
YourLetters
WeWelcome
YourLetters
WE ENCOURAGE YOU TO WRITE, eitherto respond to an article
published in theJournal or to address a clinical issue ofimportance
to you. You may submitletters by mail, fax, or e-mail.
MAILING ADDRESSLetters to the EditorCleveland Clinic Journal of
Medicine9500 Euclid Ave., NA32Cleveland, OH 44195FAX
216.444.9385E-MAIL [email protected]
Please be sure to include your full address,phone number, fax
number, and e-mailaddress. Please write concisely, as space
islimited. Letters may be edited for style andlength. We cannot
return materials sent.Submission of a letter constitutes
permissionfor the Cleveland Clinic Journal of Medicineto publish it
in various editions and forms.
on November 11, 2013. For personal use only. All other uses
require permission.www.ccjm.orgDownloaded from




















![[Management] Risk Analysis_+_found_at_redsamara.com](https://img.dokumen.tips/doc/110x75/5695cf6a1a28ab9b028e0475/management-risk-analysisfoundatredsamaracom.jpg)







