Embed Size (px)
Citation preview
MESSAGE
It gives me immense pleasure to present you this compendium compiled by Power HR Forum containing various statutory forms under important Industrial Laws. These forms cover the manner of applying for registration & licenece, maintaining various registers and records, filling of various returns.
This is the Volume –I covering the all the Forms under the Important Industrial Laws Central Rules plus the Delhi Factory Rules,1950 and Delhi Shops and Establishment Rules, 1954.
The unique part of this compendium is that it provides multiple indexes for easy searching and easy reference. Apart from indexes of Forms under each rules, consolidated indexes have been given separately for all registers and returns.
I am sure this will be of an important reference point for both HR and Line managers to facilitate the compliances under various labor enactments.
July 19, 2010 (R. P. Ojha) Executive Director (HR),POWERGRID &
Honorary Secretary– Power HR Forum

CONTENTS
1. Forms under
Industrial Laws Regulating Working Conditions 1.1. Industrial Employment (Standing orders) Central Rules,1946 Pg. A 1‐91.2. Building and other construction workers ( Regulation of employment and
condition of service ) Central Rules,1998
Pg. B 1‐33
1.3. Contract Labor (Regulation and Abolition) Central Rules,1971 Pg. C 1‐341.4. Inter‐state Migrant Workmen (Regulation of employment and condition of
Service) Central Rules,1980
Pg. D 1‐32
1.5. Mines Rules,1955 Pg. E 1‐311.6. Dangerous Machines (Regulation) Rules,2007 Pg. F 1‐51.7. Environment (Protection) Rules,1986 Pg. G 1‐81.8. Delhi Factory Rules,1950 Pg. H 1‐551.9. Delhi Shops and Establishment Rules,1954 Pg. I 1‐15
Industrial Laws Regulating Social Security 1.10. Employees Provident Funds Scheme,1952 Pg. J 1‐501.11. Employee’s State Insurance (Central) Rules,1950 Pg. K 1‐481.12. Workmen’s Compensation Rules, 1924 Pg. L 1‐22
Industrial Laws Regulating Wages 1.13. Minimum Wages (Central) Rules,1950 Pg. M 1‐161.14. Payment of Wages (Procedure) Rules, Pg. N 1‐91.15. Payment of Gratuity (Central) Rules,1972 Pg. O 1‐261.16. Payment of Bonus Rules,1975 Pg. P 1‐61.17. Equal Remuneration Rules, 1976 Pg. Q 1‐7
Industrial Laws Regulating Employment 1.18. Employment Exchange (Compulsory Notification of vacancies) Rules, 1960 Pg. R 1‐71.19. Apprenticeship Rules,1992 Pg. S 1‐17
Industrial Laws Regulating Employee Relations 1.20. Industrial Disputes (Central) Rules,1957 Pg. T 1‐351.21. Central Trade Union Regulations,1938 Pg. U 1‐10
2. Index of all forms for registration, certification & license Pg. V 1‐5
3. Index of all forms for maintaining registers & records Pg. W 1‐6
4. Index of all forms for filling returns Pg. X 1‐5

Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 1
Forms under
THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946

Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 2
INDEX FORM I Submission of Draft Standing orders
FORM II Certification of Standing Orders
FORM III Register under Section 8
FORM IV Memorandum of Appeal under Rule 7‐ A(1)
FORM IVA Notice of Change in Shift Working
FORM V Service Card
Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 3
FORM I Submission of Draft Standing Orders
[Industrial Employment (Standing Orders) Act, 1946, section 3]
Dated..............20.... To The Certifying Officer Vide Notification No. L.R.11(98), dated 25th July ,1953
(Area) ………….. (Place) Sir, Under the provisions of section 3 of the Industrial Employment (Standing Orders) Act, 1946, I enclose five copies of the draft standing orders proposed by me for adoption in.......................................................................... ……………………………………………………
(Name) .......................................................................................................................................................................... (Place) (Postal address) an industrial establishment owned/controlled by me, with the request that these orders may be certified under the terms of the Act. I also enclose a statement giving the particulars prescribed in rule 5 of the Industrial Employment (Standing Orders) Central Rules, 1946.
I am etc.,
........................................... (Signature)
Employer/Manager

Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 4
FORM II Certification of Standing Orders
[Notice under section 5 of the Industrial Employment (Standing Orders) Act, 1946]
Office of the Certifying Officer for ............................................................area/place...................................................
dated the......................20......... I................... Certifying Officer............., area, forward herewith a copy of the draft Standing Orders proposed by the employer for adoption in the................................ Industrial Establishment and submitted to me for certification under the Industrial Employment (Standing Orders) Act, 1946. Any objections which the workmen may desire to make to the draft Standing Orders should be submitted to me within fifteen days from the receipt of this notice.
...................................................
(Certifying Officer)
Seal
To
The Secretary,
Union.
Representative elected under rule 6 Name
Occupation
Industrial Establishment.

Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 5
FORM III
Industrial Employment (Standing Orders) Act, 1946, Section 8
Register
PART I
INDUSTRIAL ESTABLISHMENT
S. No.
Date of the dispatch of the copy of standing orders authenticated under section 5 for the first time
Date of filing appeal
Date and nature of decision
Amendment made on appeal, if any
Date of the dispatch of the copy of the standing orders as settled on appeal
Any notice subsequently given or received of any amendment
Result
PART II
(Should contain the authenticated copy of the Standing Orders)
Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 6
FORM IV
[See rule 7A (1) ] Memorandum of Appeal
[To be furnished in respect of each clause appealed against, separately]
1. Draft of the Standing Order under appeal as submitted by the employers. 2. Objection made/modification suggested, if any, to the Draft Standing Order under
appeal, by the Trade Union/ Representatives of workmen. 3. Standing Order under appeal, as certified by the Certifying Officer. 4. Grounds of appeal by the employers/ trade union/ workmen’s representatives.]

Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 7
FORM IVA (See Standing Order 7A of Schedule I )
Notice of Change in Shift Working
Notice of discontinuance/ re‐starting of a shift working to be given by an employer
Name of employer.............................................................................................................
Address...............................................................................................................................
Dated the..................................................................... day of............................ 20..........
In accordance with Standing Order No..... of the Standing Orders certified and approved in respect of my/our industrial establishment, I/we hereby give notice to all concerned that it is my/our intention to discontinue/restart the shift working specified in the Annexure with effect from.......
Signature.............................
Designation.........................
Annexure
(Here specify the particulars of change in the shift working proposed to be effected).]
Copy forwarded to— 1. The Secretary of registred Trade Union, if any. 2. The Assistant Labour Commissioner (Central)/Labour Employment Officer (Here enter
office address of the Assistant Labour Commissioner (Central) Labour Employment Officer in the local area concerned).
3. The Regional Labour Commissioner (Central) Zone. 4. The Chief Labour Commissioner (Central), New Delhi.
Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 8
FORM V (See Standing Order 1, Schedule I‐B)
Service Card
Name of Estt./Factory Ticket/Token No. 1. Register Serial No.
2. Name
3. Specimen Signature/Thumb Impression
4. Father’s or Husband’s name
5. Sex
6. Religion
7. Date of Birth
8. Place of Birth
9. Date of Joining
10. Details of Medical Certificate at the time of joining
11. Educational and other qualifications
12. Can Read
13. Can Write
14. Can Speak
15. Height
16. Identification Marks
17. Category of Workman
18. Department
19. Details of family members
20. Permanent Address
21. Local Address
22. Quarter No.
23. Life Insurance Policy No.
24. Provident Fund Account No.
25. Nominee for Gratuity
26. Nominee for Pension, if any

Forms under THE INDUSTRIAL EMPLOYMENT (STANDING ORDERS) CENTRAL RULES, 1946
C o m p i l e d b y P o w e r H R F o r u m P a g e A 9
27. Employees’ State Insurance No.
28. Training courses attended (details)
29. (Eligibility for higher jobs)
30. Proficiency tests passed
31. Employment History Department Token No. Designation Scale of Pay Joined Left (Reason)
1 2 3 4 5 6
32. Absence Periods
From To Reason Medical reports regarding
suitability for continued employment
i. Sick Leave ii. Earned Leave iii. Any other leave
33. Maternity Benefit Workmen’s Compensation
Details of accidents:
34. Details of Disciplinary Action 35. Promotions
i. Details ii. Awards iii. Issue of Certificate of commendation
36. Date of superannuation 37. Any other matter.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1
Forms under
BUILDING AND OTHER CONSTRUCTION WORKERS
(REGULATION OF EMPLOYMENT AND CONDITIONS OF SERVICE) CENTRAL RULES, 1998
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2
INDEX FORM I Application for Registration of Establishments Employing Building Workers
FORM II Certificate of Registration
Form III Register of Establishments
Form IV Notice of Commencement/Completion of Building or Other Construction Work
FORM V
Certificate of Initial and Periodical Test and Examination of Winches, Derricks and Their Accessory Gear
FORM VI
Certificate of Initial and Periodical Test and Examination of Cranes or Hoists and Their Accessory Gear
FORM VII Certificate of Initial and Periodical Test and Examination of Loose Gears
FORM VIII Certificate of Test and Examination of Wirerope Before Being Taken Into Use
FORM IX Certificate of Annealing af Loose Gears
FORM X Certificate of Annual Thorough Examination of Loose Gears Exempted From Annealing
FORM XI Certificate of Medical Examination
FORM XII Health Register
FORM XIII Notice of Poisoning or Occupational Notifiable Diseases
FORM XIV Report of Accidents and Dangerous Occurrences
FORM XV Register of Building Workers Employed by the Employer
FORM XVI Muster‐Roll
FORM XVII Register of Wages
FORM XVIII Form of Register Of Wages‐Cum‐Muster‐Roll
FORM XIX Register of Deductions For Damage Or Loss
FORM XX Register of Fines
FORM XXI Register of Advances
FORM XXII Register of Overtime
FORM XXIII Wage Book
FORM XXIV Service Certificate
FORM XXV Annual Return of Employer to be Sent to the Registering Officer
FORM XXVI
Register of Periodical Test—Examination of Lifting Appliance and Gears Etc
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 3
FORM I [See Rule 23(1)]
Application for Registration of Establishments Employing Building Workers
1. Name and location of the Establishment where building or other construction work is to‐be carried on.
2. Postal address of the Establishment.
3. Full name and permanent address of the Establishment, if any.
4. Full name and address of the Manager or person responsible for the supervision and control of the Establishment.
5. Nature of building or other construction work carried/is to be carried on in the Establishment.
6. Maximum number of building workers to be employed on any day.
7. Estimated date of commencement of building or the other construction work.
8. Estimated date of completion of the building or other construction work.
9. Particulars of demand draft, enclosed (name of the Bank amount, demand draft No. and date).
Declaration by the employer
i. I hereby declare that the particulars given above are true to the best of my knowledge and belief.
ii. I undertake to abide by the provisions of the Building and other Construction Workers (Regulation of Employment and Conditions of Service) Act, 1996 and the Rules made there under.
Principal Employer
Seal and Stamp
Office of the Registering Officer appointed under the Building and Other Construction Workers (Regulation of Employment and Conditions of Service) Act, 1996 and Central Rules made there under.
Date of Receipt of application:
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 4
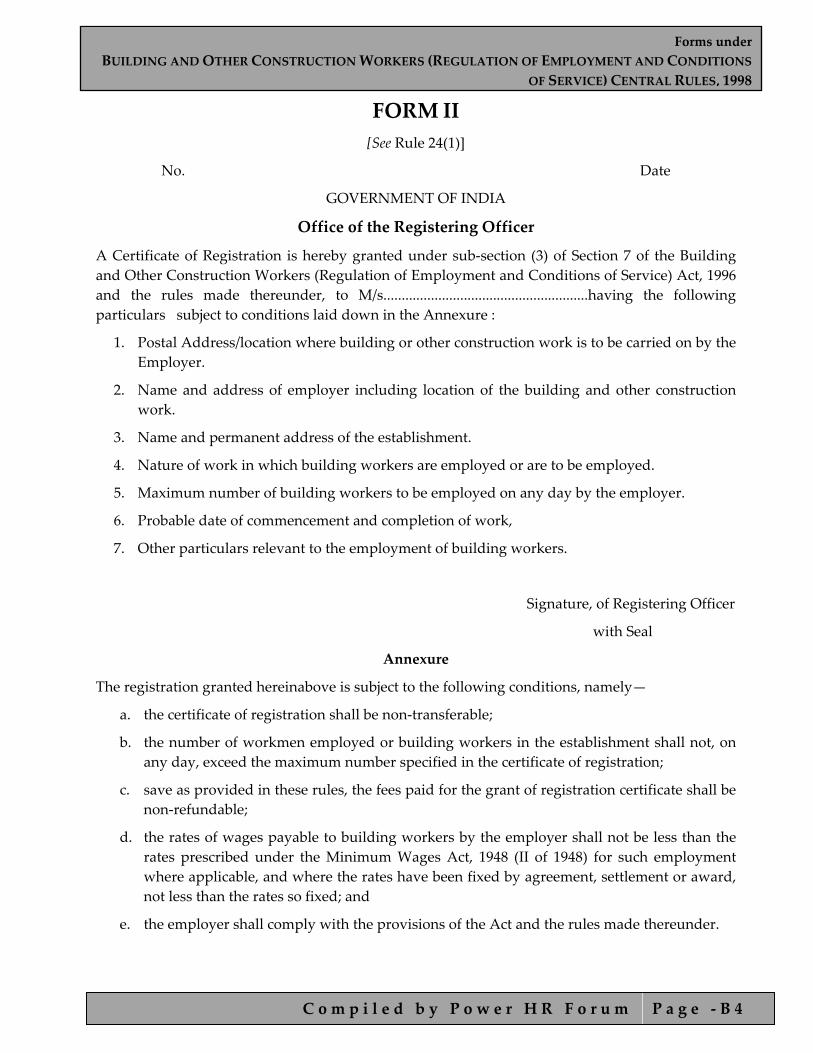
FORM II [See Rule 24(1)]
No. Date
GOVERNMENT OF INDIA
Office of the Registering Officer
A Certificate of Registration is hereby granted under sub‐section (3) of Section 7 of the Building and Other Construction Workers (Regulation of Employment and Conditions of Service) Act, 1996 and the rules made thereunder, to M/s........................................................having the following particulars subject to conditions laid down in the Annexure :
1. Postal Address/location where building or other construction work is to be carried on by the Employer.
2. Name and address of employer including location of the building and other construction work.
3. Name and permanent address of the establishment.
4. Nature of work in which building workers are employed or are to be employed.
5. Maximum number of building workers to be employed on any day by the employer.
6. Probable date of commencement and completion of work,
7. Other particulars relevant to the employment of building workers.
Signature, of Registering Officer
with Seal
Annexure
The registration granted hereinabove is subject to the following conditions, namely—
a. the certificate of registration shall be non‐transferable;
b. the number of workmen employed or building workers in the establishment shall not, on any day, exceed the maximum number specified in the certificate of registration;
c. save as provided in these rules, the fees paid for the grant of registration certificate shall be non‐refundable;
d. the rates of wages payable to building workers by the employer shall not be less than the rates prescribed under the Minimum Wages Act, 1948 (II of 1948) for such employment where applicable, and where the rates have been fixed by agreement, settlement or award, not less than the rates so fixed; and
e. the employer shall comply with the provisions of the Act and the rules made thereunder.

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 5
FORM III [See Rule 25(2)]
Register of Establishments
SI. No.
Registration No. and date
Name and Address location of the establishment registered where a
building or other construction work is to be carried on
Name of the Employer and his address
Nature of building or other construction
work
(1) (2) (3) (4) (5)
Name and permanent address of
Establishment
Probable date of commencement
of work
Maximum No. of building workers to be employed on
any day
Probable duration of building or other
construction work & probable date of completion
Remarks
(6) (7) (8) (9) (10)

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 6
FORM IV [See Rules 26(3) and 239(1)]
Notice of Commencement/Completion of Building or Other Construction Work
1. i. Name and address (Permanent) of the establishment............................................................. ii. Name of the employer and address.........................................................................................
2. Name and situation of place where the building and other construction is proposed to be carried on.
3. No. and date of Certificate of registration..................................................................................... 4. Name and address of the person incharge of the construction work. 5. Address to which the communications relating to building or other construction work may be
sent. 6. Nature of work involved and the facilities including plant or machinery provided. 7. The arrangement storage of explosives, if any, to be used in building or other construction
work. 8. In case the notice is for commencement of work, the approximate duration of work. I/We hereby intimate that the building or other construction work (Name of work) having registration No. ..........................................dated...........................is likely to commence/is likely to be completed with effect from...............................................(date)/on (date).
Signature of the Employer To, The Inspector, …………………….. ……………………..

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 7
FORM V [See Rules 56 and 74(6), Schedule I]
Certificate of Initial and Periodical Test and Examination of Winches, Derricks and Their Accessory Gear
Test Certificate No............................................... (a) In case of construction site, name of the construction site where lifting‐ appliances are
fitted/installed/located:
Situation and Description of lifting appliances and Gear with distinguishing number or marks (if any), which have been tested, thoroughly examined
Angle to the horizontal of derrick boom at which test
load applied
Test load applied
Safe working load at the angle shown in column (2)
(1) (2) (3) (4) (Degrees) (Tonnes) (Tonnes)
Name and address of public service, association, company, or firm or testing
establishment making the test and examination
Name and position of the Competent Person of public service, association, company or firm
or testing establishment
I certify that on the...............................................................day of 19.............the lifting appliance shown in column (1) together with its necessary gear was tested in the manner set forth overleaf in my presence; that a careful examination of the said lifting appliances after the test showed that it had withstood the test load without injury or permanent deformation; and that the safe working load of the said lifting appliance and accessory gear is as shown in column (4). Signature of the Competent Person …………………… Date
Seal Registration/Authority number of the Competent Person
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 8
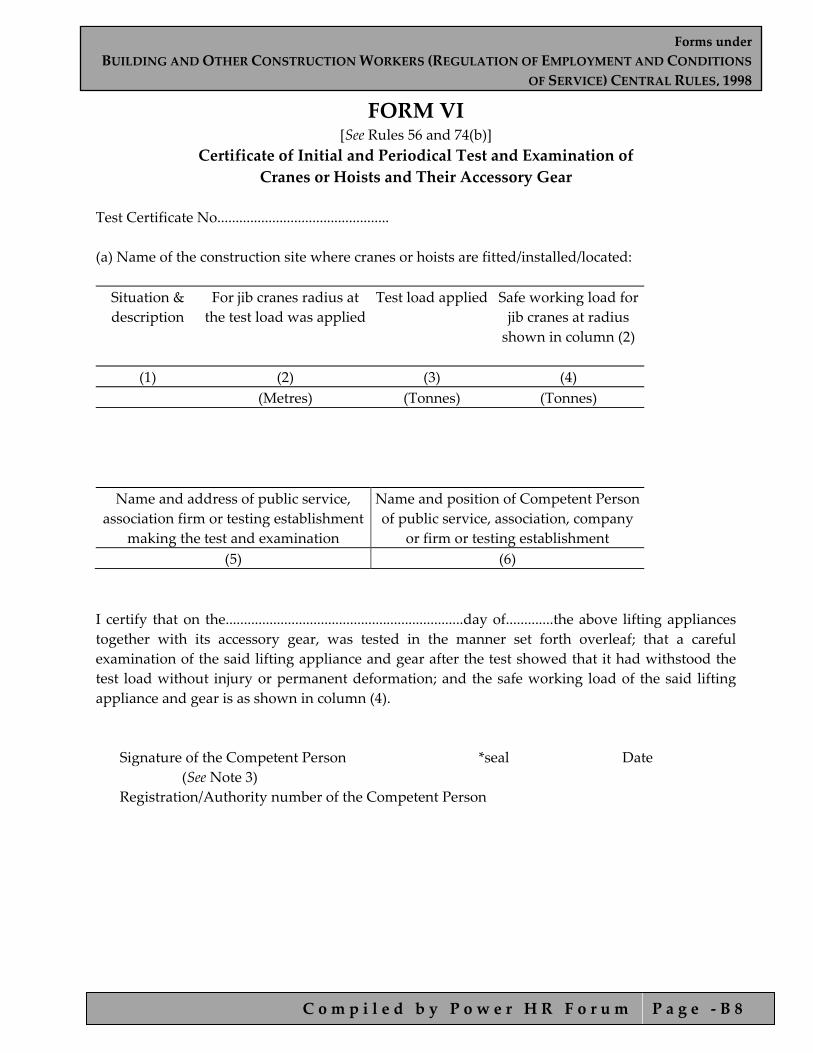
FORM VI [See Rules 56 and 74(b)]
Certificate of Initial and Periodical Test and Examination of Cranes or Hoists and Their Accessory Gear
Test Certificate No............................................... (a) Name of the construction site where cranes or hoists are fitted/installed/located: Situation & description
For jib cranes radius at the test load was applied
Test load applied
Safe working load for jib cranes at radius shown in column (2)
(1) (2) (3) (4) (Metres) (Tonnes) (Tonnes)
Name and address of public service, association firm or testing establishment
making the test and examination
Name and position of Competent Person of public service, association, company
or firm or testing establishment (5) (6)
I certify that on the.................................................................day of.............the above lifting appliances together with its accessory gear, was tested in the manner set forth overleaf; that a careful examination of the said lifting appliance and gear after the test showed that it had withstood the test load without injury or permanent deformation; and the safe working load of the said lifting appliance and gear is as shown in column (4).
Signature of the Competent Person *seal Date (See Note 3) Registration/Authority number of the Competent Person
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 9
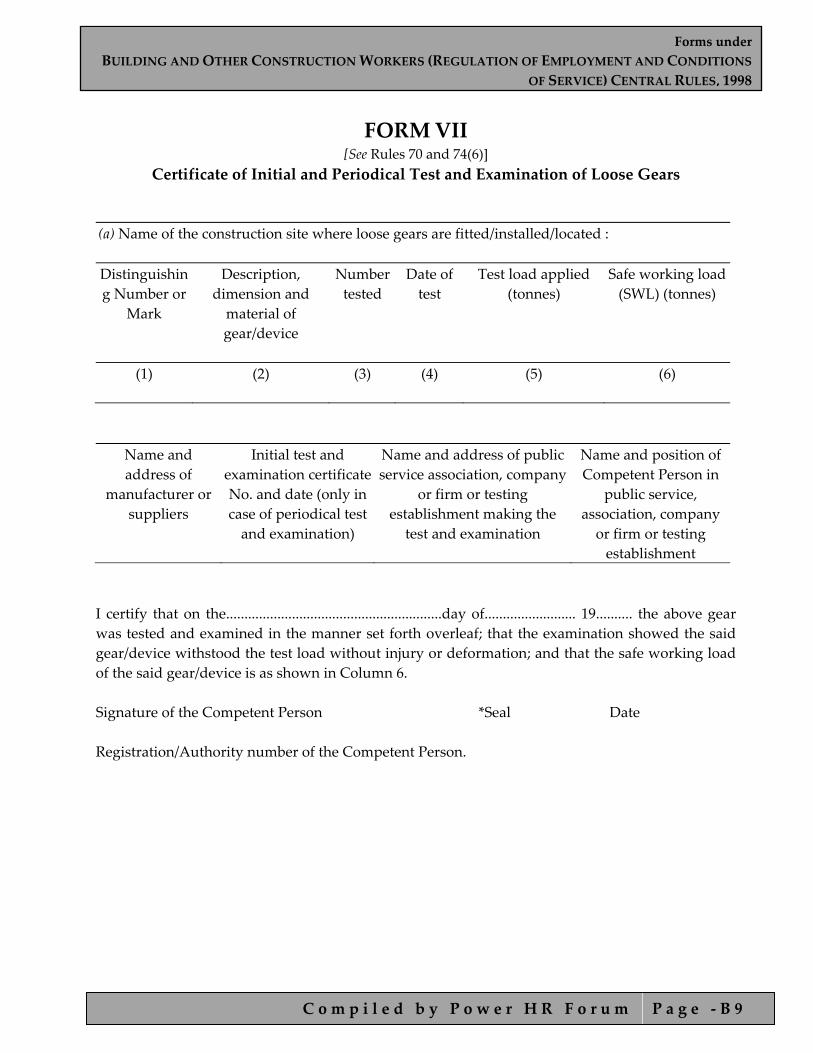
FORM VII [See Rules 70 and 74(6)]
Certificate of Initial and Periodical Test and Examination of Loose Gears
(a) Name of the construction site where loose gears are fitted/installed/located : Distinguishing Number or
Mark
Description, dimension and material of gear/device
Number tested
Date of test
Test load applied (tonnes)
Safe working load (SWL) (tonnes)
(1)
(2)
(3)
(4)
(5)
(6)
Name and address of
manufacturer or suppliers
Initial test and examination certificate No. and date (only in case of periodical test and examination)
Name and address of public service association, company
or firm or testing establishment making the
test and examination
Name and position of Competent Person in
public service, association, company or firm or testing establishment
I certify that on the...........................................................day of......................... 19.......... the above gear was tested and examined in the manner set forth overleaf; that the examination showed the said gear/device withstood the test load without injury or deformation; and that the safe working load of the said gear/device is as shown in Column 6. Signature of the Competent Person *Seal Date Registration/Authority number of the Competent Person.

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 0
FORM VIII [See Rules 62 and 74(b)]
Certificate of Test and Examination of Wirerope before Being Taken Into Use Test Certificate No...............................................
1. Name and address of maker or supplier:
2.
a) Circumference/diameter of rope
b) Number of strand
c) Number of wires per strand
d) Lay
e) Core
3. Quality of wire (e.g. Best Plough steel)
4.
a. Date of test of sample of rope
b. Load at which sample broke (tonnes)
c. Safe working load of rope (tonnes)
d. Intended use
5. Name and address of public service, association, company or firm or testing establishment making the test and examination.
6. Name and position of Competent Person in public service, association, company or firm or testing establishment making the test and examination.
I certify that the above particulars are correct, and that the test and examination were earned out by me and no defect effecting its safe working load (SWL) were found.
Signature of the Competent Person Seal Date
Registration/Authority number of the Competent Person.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 1
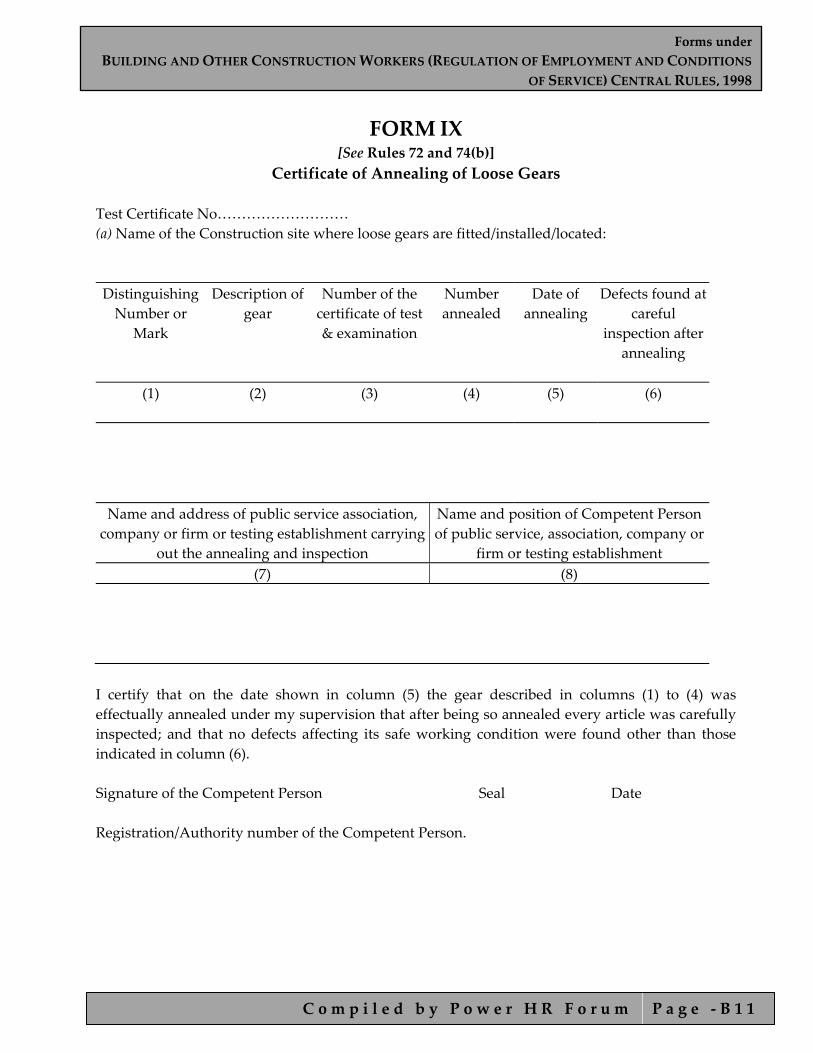
FORM IX [See Rules 72 and 74(b)]
Certificate of Annealing of Loose Gears
Test Certificate No……………………… (a) Name of the Construction site where loose gears are fitted/installed/located: Distinguishing Number or
Mark
Description of gear
Number of the certificate of test & examination
Number annealed
Date of annealing
Defects found at careful
inspection after annealing
(1)
(2)
(3)
(4)
(5)
(6)
Name and address of public service association, company or firm or testing establishment carrying
out the annealing and inspection
Name and position of Competent Person of public service, association, company or
firm or testing establishment (7) (8)
I certify that on the date shown in column (5) the gear described in columns (1) to (4) was effectually annealed under my supervision that after being so annealed every article was carefully inspected; and that no defects affecting its safe working condition were found other than those indicated in column (6). Signature of the Competent Person Seal Date Registration/Authority number of the Competent Person.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 2
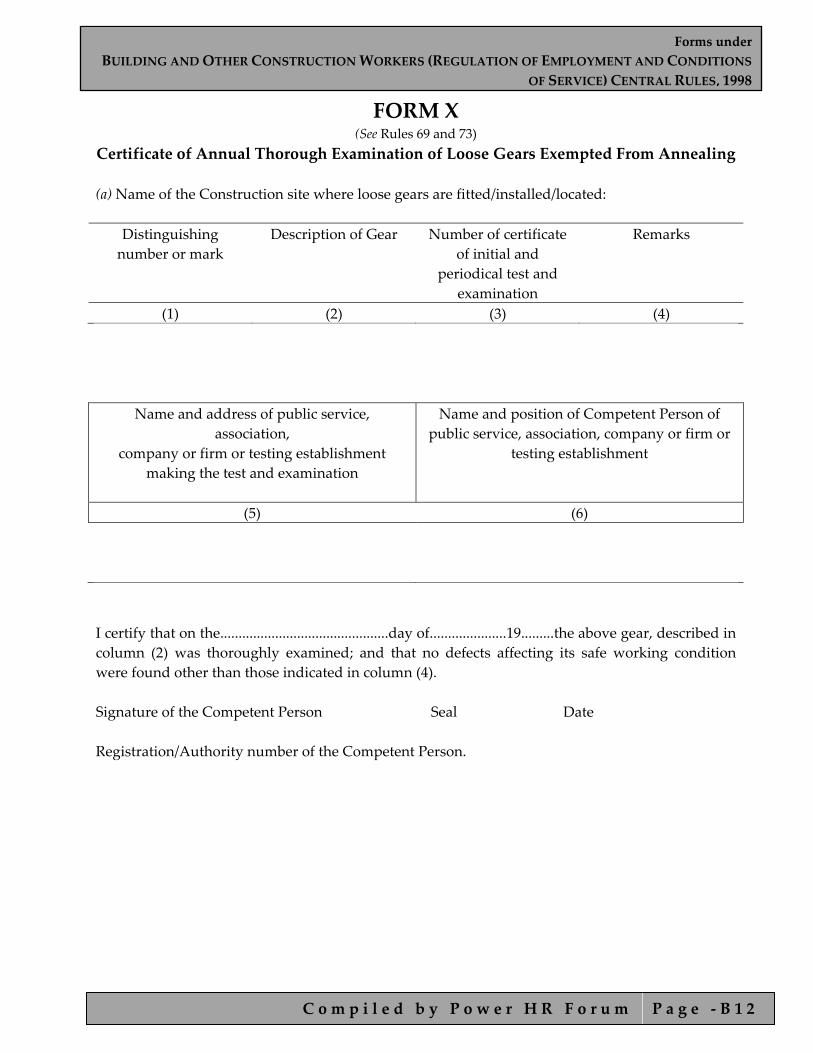
FORM X (See Rules 69 and 73)
Certificate of Annual Thorough Examination of Loose Gears Exempted From Annealing (a) Name of the Construction site where loose gears are fitted/installed/located:
Distinguishing number or mark
Description of Gear Number of certificate of initial and
periodical test and examination
Remarks
(1) (2) (3) (4)
Name and address of public service, association,
company or firm or testing establishment making the test and examination
Name and position of Competent Person of public service, association, company or firm or
testing establishment
(5) (6)
I certify that on the..............................................day of.....................19.........the above gear, described in column (2) was thoroughly examined; and that no defects affecting its safe working condition were found other than those indicated in column (4).
Signature of the Competent Person Seal Date Registration/Authority number of the Competent Person.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 3
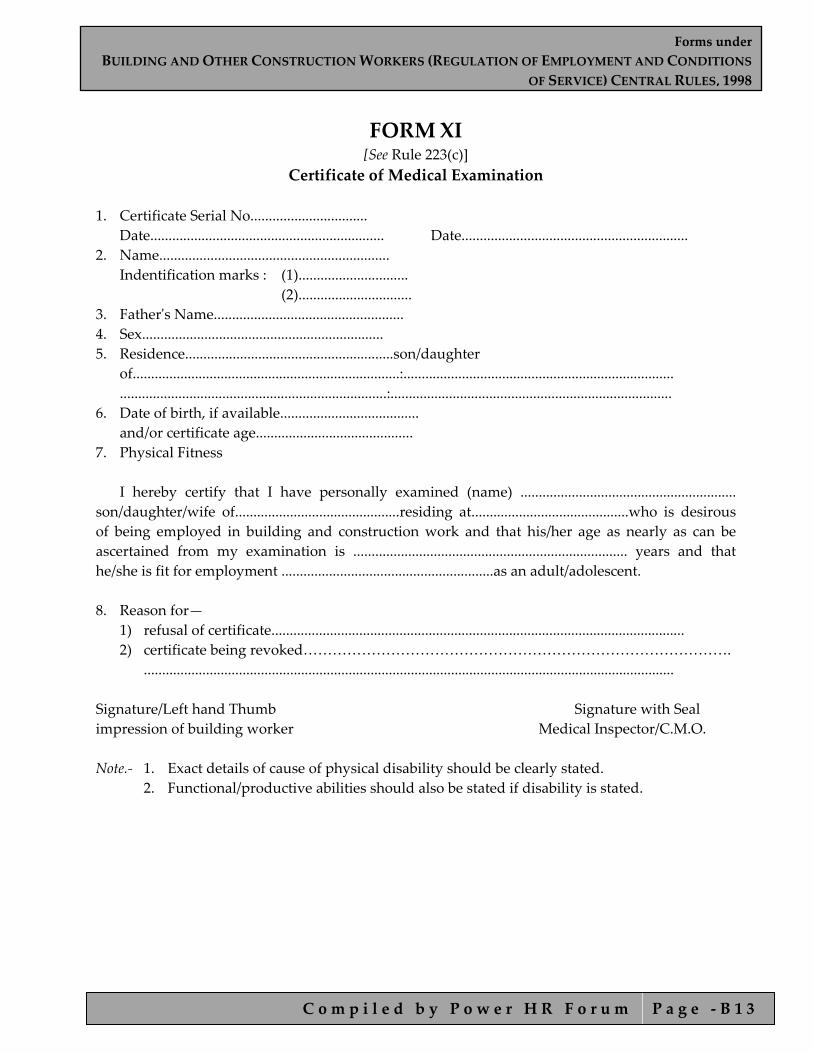
FORM XI [See Rule 223(c)]
Certificate of Medical Examination 1. Certificate Serial No................................ Date................................................................ Date.............................................................. 2. Name............................................................... Indentification marks : (1).............................. (2)............................... 3. Fatherʹs Name.................................................... 4. Sex.................................................................. 5. Residence.........................................................son/daughter of.........................................................................:.......................................................................... .........................................................................:............................................................................. 6. Date of birth, if available...................................... and/or certificate age........................................... 7. Physical Fitness I hereby certify that I have personally examined (name) ........................................................... son/daughter/wife of.............................................residing at...........................................who is desirous of being employed in building and construction work and that his/her age as nearly as can be ascertained from my examination is ........................................................................... years and that he/she is fit for employment ..........................................................as an adult/adolescent. 8. Reason for—
1) refusal of certificate................................................................................................................. 2) certificate being revoked…………………………………………………………………………….
................................................................................................................................................. Signature/Left hand Thumb Signature with Seal impression of building worker Medical Inspector/C.M.O. Note.‐ 1. Exact details of cause of physical disability should be clearly stated. 2. Functional/productive abilities should also be stated if disability is stated.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 4
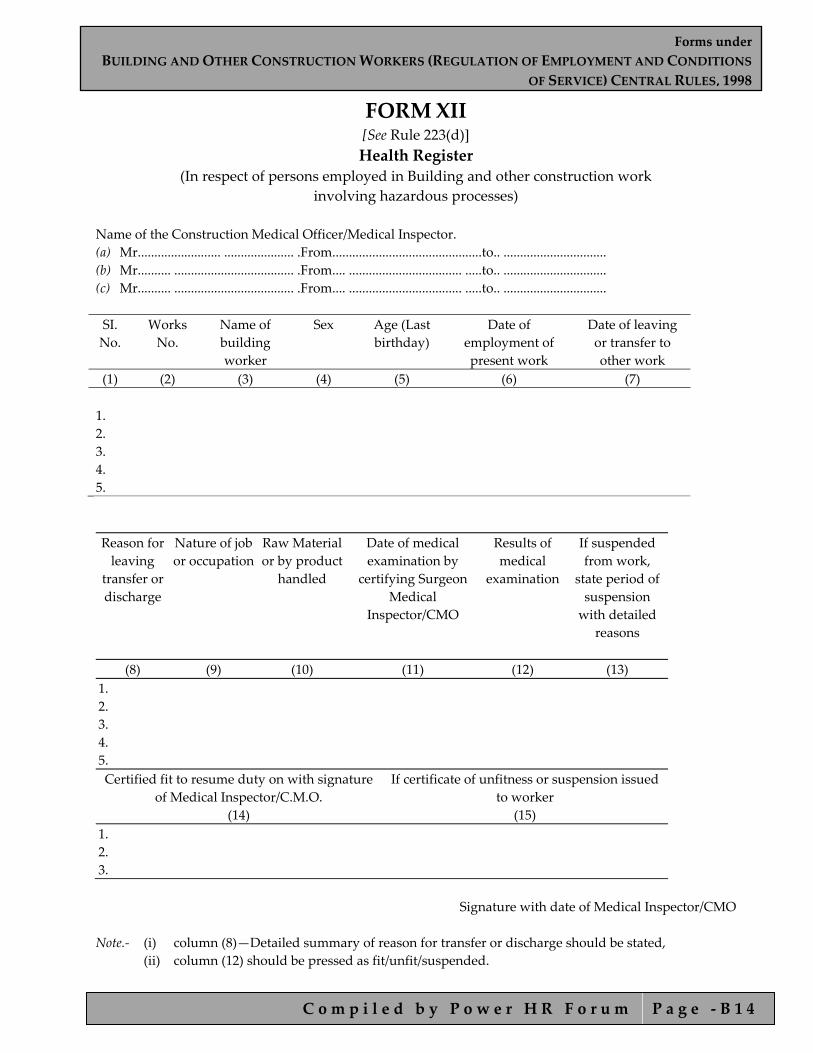
FORM XII [See Rule 223(d)] Health Register
(In respect of persons employed in Building and other construction work involving hazardous processes)
Name of the Construction Medical Officer/Medical Inspector. (a) Mr......................... ..................... .From.............................................to.. ............................... (b) Mr.......... .................................... .From.... .................................. .....to.. ............................... (c) Mr.......... .................................... .From.... .................................. .....to.. ............................... SI. No.
Works No.
Name of building worker
Sex Age (Last birthday)
Date of employment of present work
Date of leaving or transfer to other work
(1) (2) (3) (4) (5) (6) (7) 1. 2. 3. 4. 5. Reason for leaving
transfer or discharge
Nature of job or occupation
Raw Material or by product
handled
Date of medical examination by
certifying Surgeon Medical
Inspector/CMO
Results of medical
examination
If suspended from work,
state period of suspension with detailed
reasons
(8) (9) (10) (11) (12) (13) 1. 2. 3. 4. 5. Certified fit to resume duty on with signature
of Medical Inspector/C.M.O. (14)
If certificate of unfitness or suspension issued to worker
(15) 1. 2. 3.
Signature with date of Medical Inspector/CMO Note.‐ (i) column (8)—Detailed summary of reason for transfer or discharge should be stated, (ii) column (12) should be pressed as fit/unfit/suspended.

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 5
FORM XIII [See Rule 230(a)]
Notice of Poisoning or Occupational Notifiable Diseases
1. Name and address of the employer : 2. Name of the building worker and his work No., if any : 3. Address of the building worker : 4. Sex and Age : 5. Occupation : 6. State exactly what the patient was doing at the time of contracting the disease 7. Nature of poisoning or disease from
which the building worker is suffering from : Date : Signature of the employer/CMO Note.‐ When a building worker contracts any disease specified in Schedule XII, a notice in this form
shall be sent forthwith to the Director General.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 6
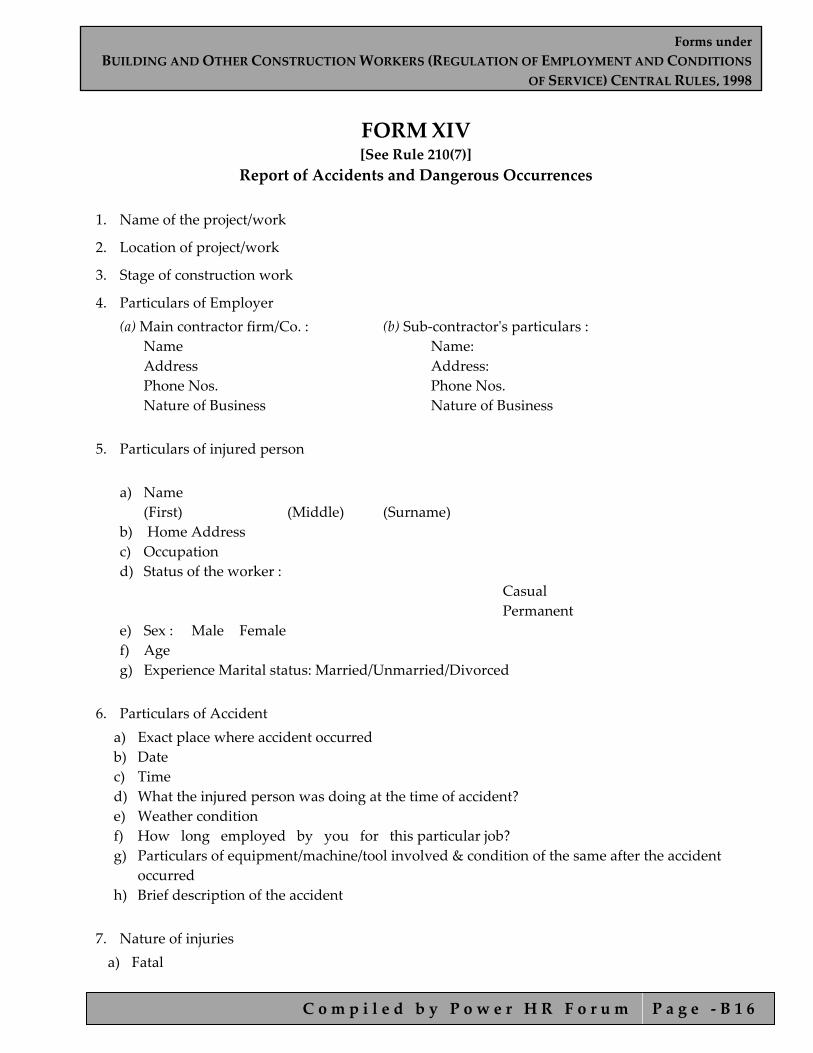
FORM XIV [See Rule 210(7)]
Report of Accidents and Dangerous Occurrences
1. Name of the project/work
2. Location of project/work
3. Stage of construction work
4. Particulars of Employer (a) Main contractor firm/Co. : (b) Sub‐contractorʹs particulars :
Name Name: Address Address: Phone Nos. Phone Nos. Nature of Business Nature of Business
5. Particulars of injured person
a) Name (First) (Middle) (Surname)
b) Home Address c) Occupation d) Status of the worker :
Casual Permanent
e) Sex : Male Female f) Age g) Experience Marital status: Married/Unmarried/Divorced
6. Particulars of Accident
a) Exact place where accident occurred b) Date c) Time d) What the injured person was doing at the time of accident? e) Weather condition f) How long employed by you for this particular job? g) Particulars of equipment/machine/tool involved & condition of the same after the accident
occurred h) Brief description of the accident
7. Nature of injuries a) Fatal

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 7
b) Non fatal c) If non‐fatal, state precisely the nature of injuries (Describe in detail the nature of
injury, for instance fracture of right arm, sprain etc.) d) First‐Aid : Given : Not given : e) If not, give the reasons f) Name & designation of the person by whom
first‐aid was given g) If admitted to hospital,
Name of the hospital: Address of the hospital Phone No. Name of Doctor 8. Mode of transport used Ambulance Truck Tempo Taxi Private Car 9. How much time was taken to shift the injured person?
a. If very late, state the reasons b. How the reporting was made?
Telephone Telegram Special Messenger Letter c. Who visited the accident site first and what action was proposed by him? d. What are the actions taken for the investigation of the accident by the
employer? (Describe about photographs/ Video film/measurements taken etc.) 10. Particulars of the persons given witness: (a) Name Address Occupation 1. 2. 3. 4. (b) Whether Temporary Permanent 11. Particulars in case of fatal: Date Whether registered with Building and other Construction Workersʹ Welfare Board If yes give Reg No. 12. Dangerous Occurrences as covered under the Regulation No. (Give details)
a) collapse or failure of lifting appliances, b) hoist conveyors etc.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 8
c) collapse or subsidence of soil, any wall, d) floor, gallery etc. e) collapse of transmission towers, pipeline, f) bridges etc. g) explosion of receiver, vessel etc. h) fire and explosion i) spillage or leakage of hazardous substances j) collapse, capsizing, toppling or collision of transport equipment. k) leakage or release of harmful toxic gases at the l) construction site. m) failure of lifting appliance, loose gear, hoist n) or building and other construction work machinery, o) transport equipment etc.
13. Certificate from the Employer or authorized signatory. I certify that to the best of my knowledge and belief, the above particulars are cofrect in every respect. Place: Signature Date: Designation c.c forwarded for information and follow‐up action : 1. 2. 3. Note.‐ If more than one person is involved, then for each person, information is to be filled up in separate forms.

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 1 9
FORM XV (See Rule 240)
Register of Building Workers Employed by the Employer Name and address Name and permanent of establishment address of establishment were building and other construction work is to be carried on nature and location of work……………………………
SI. No.
Name and Surname of workman
Age and Sex
Fatherʹs/Husbandʹs name
Nature of Employment/ Designation
Permanent Home address of workman (Village and Taluk and
Distt.)
(1) (2) (3) (4) (5) (6) 1. 2. 3. 4.
Local Address
Date of commencement of
employment
Signature or thumb impression of workman
Date of termination of employment
Reasons for termination
(7)
(8)
(9)
(10)
(11)
1. 2. 3. 4. If the building worker is/was beneficiary, the date of registration as a beneficiary, the registration No. and the name of
Welfare Board
Remarks
1. 2. 3. 4.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 0
FORM XVI [See Rule 241(1 )(a)] Muster‐Roll
Name and permanent address Name and address of establishment where of the establishment building or other construction work is earned
on/is to be carried on Name and address of Employer
Nature of building or other construction work Name and address of Employer For the month of ……………… SI. No.
Name of the building worker
Fatherʹ s/Husbandʹ s
name
Sex
Dates Remarks
(1) (2) (3) (4) (5) (6) 1. 2. 3. 4. 5.
1.
2.
3.
4.
5.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 1
FORM XVII [See Rule 241 (1)(a)] Register of Wages
Name and address of the Name and address of the Establishment Establishment where building or other construction work is ……………………………………….. carried on Nature of building Name and address of the Employer or other construction work ……………………………………….. Wage period: Monthly ……………………………… SI. No.
Name of workman
Serial No. in the register of workman
Designation/nature of work done
No. of days worked
Units of work done
(1) (2) (3) (4) (5) (6)
Daily rate of wages/piece
rate
Amount of wages earned
Basic wages
Dearness allowances
Overtime
Other cash payments (Nature of payment to be
indicated)
Total
(7) (8) (9) (10) (11) (12)
Deductions, if any, (indicate nature)
Net amount paid
Signature/Thumb impression of workman
Initial of employer or his representative
(13)
(14)
(15)
(16)

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 2
FORM XVIII [See Rule 241(1 )(a)]
Form of Register of Wages‐Cum‐Muster‐Roll Name and address of the establishment Name and permanent where building or other construction address of establishment work is carried on/is to be carried on Nature of building or other construction work SI. No. SI. No. in
Register of building workers
Name of employee
Designation/ nature of work
Daily attendance/
units worked
Total attendance/ units of work
done (1) (2) (3) (4) (5) (6)
1. 2. 3. 4. 5.
1. 2. 3. 4. 5.
Daily rate of
wages/piece rate Amount of wages earned
Basic wages Dearness allowances
Overtime Other cash payments (nature of payment to be indicated)
Total
(7) (8) (9) (10) (11) (12)
Deduction if any, (indicate nature)
Net amount paid
Signature/Thumb impression of workman
Initial of employer or his representative
(13) (14) (15) (16)
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 3
FORM XIX [See Rule 241(1) (b)]
Register of Deductions for Damage or Loss Name and Address of establishment where building or other construction work is carried on/is to be carried on
Name and permanent address of building workers
Name and permanent address of employer
Nature of building or other construction work SI. No.
Name of work
Fatherʹs/ Husbandʹs Name
Designation/nature of
employment
Particulars of damage or loss
Date of damage or
loss
Whether building
worker showed cause against deduction
(1) (2) (3) (4) (5) (6) (7)
Name of person in whose presence building workerʹs
explanation was heard
Amount of deduction imposed
No. of installments
Date of recovery First installment
Last installment
(8) (9) (10) (11) (12)

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 4
FORM XX [See Rule 241(1 )(b)] Register of Fines
Name and address of establishment Name and permanent address of where building or other construction establishment work is carried on/is to be carried on Nature of building and other construction work Name and address of employer SI. No.
Name of the building worker
Fatherʹs/Husbandʹs name
Designation/nature of employment
Act/omission for which fine imposed
Date of offence
(1) (2) (3) (4) (5) (6)
Whether building worker
showed cause against fine
Name of person in whose presence building workerʹsexplanation was
heard
Wage periods and wages payable
Amount of the fine imposed
Date on which fine realized
Remarks
(7) (8) (9) (10) (11) (12)

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 5
FORM XXI [See Rule 241(!)(b)]
Register of Advances Name and address of establishment where building or other construction work is carried on/is to be carried on
Name and permanent address of establishment
Nature of building or other construction work
Name and address of the employer
SI. No. Name Fatherʹs/Husbandʹs
name Nature of
employment/ Designation
Wage period and wages payable
Date and amount of
advance given (1) (2) (3) (4) (5) (6)
Purpose(s) for
which advance given
No. of installments by which advance
to be repaid
Date and amount of each installment
repaid
Date on which last installment was
repaid
Remarks
(7)
(8)
(9)
(10)
(11)
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 6
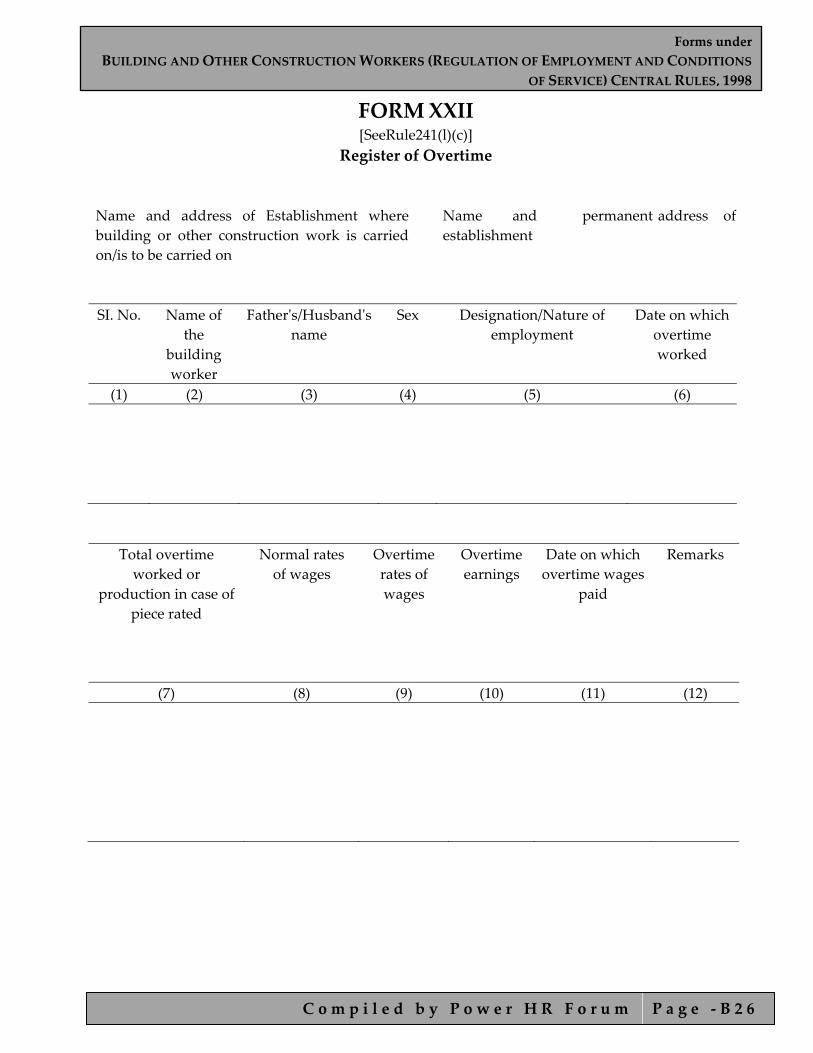
FORM XXII [SeeRule241(l)(c)]
Register of Overtime Name and address of Establishment where building or other construction work is carried on/is to be carried on
Name and permanent address of establishment
SI. No. Name of
the building worker
Fatherʹs/Husbandʹs name
Sex
Designation/Nature of employment
Date on which overtime worked
(1) (2) (3) (4) (5) (6)
Total overtime worked or
production in case of piece rated
Normal rates of wages
Overtime rates of wages
Overtime earnings
Date on which overtime wages
paid
Remarks
(7) (8) (9) (10) (11) (12)

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 7
FORM XXIII [SeeRule241(2)(a)] Wage Book
Name and Address of Employer Name and address of the establishment where building or other construction work is carried on
Name and permanent address of establishment Nature of building or other construction work
For the Week/ Fortnight/ Month ending.............
1. No. of days worked..... ..................................................
2. No. of units worked in case of piece‐rate workers................................
3. Rate of daily/monthly wages/piece‐rate................................................
4. Amount of overtime wages..................................................................
5. Gross wages payable.............................................................................
6. Deductions, if any, on account of the following :
a) fines.
b) damage or loss.
c) loans and advances.
d) subscription towards provident fund.
e) subscription towards the Building Workersʹ Welfare Fund.
f) any other deductions e.g. subscriptions to Cooperative Society or account of loans from Cooperative Society/housing loan, or contribution to any relief fund as per provision of clause (P) of sub‐section (2) of Section 7 of the Payment of Wages Act or for payment of any premium of Life Insurance Corporation.
7. Net amount of wages paid.......................................................................
Initials of the employer
or his Representative

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 8
FORM XXIV [See Rule 241 (2) (b)] Service Certificate
Name and permanent address of the establishment
Name and address/location where the building or other construction work carried on/to be carried on
Nature and location of work : .......................................................................
Name and address of the workman : .......................................................................
Age or Date of Birth : ....................................................................... Identification Marks : .......................................................................
Fatherʹs/Husbandʹs name : ....................................................................... SI. No.
Total period for which employed
From To
Nature of work done
Rate of wages with particulars of unit in case of (piece work)
If the building worker was a beneficiary his
registration No., date and the name of Board
(1) (2) (3) (4) (5) (6)
Reasons/grounds on which the employment terminated Remarks
(7) (8)
Signature
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 2 9
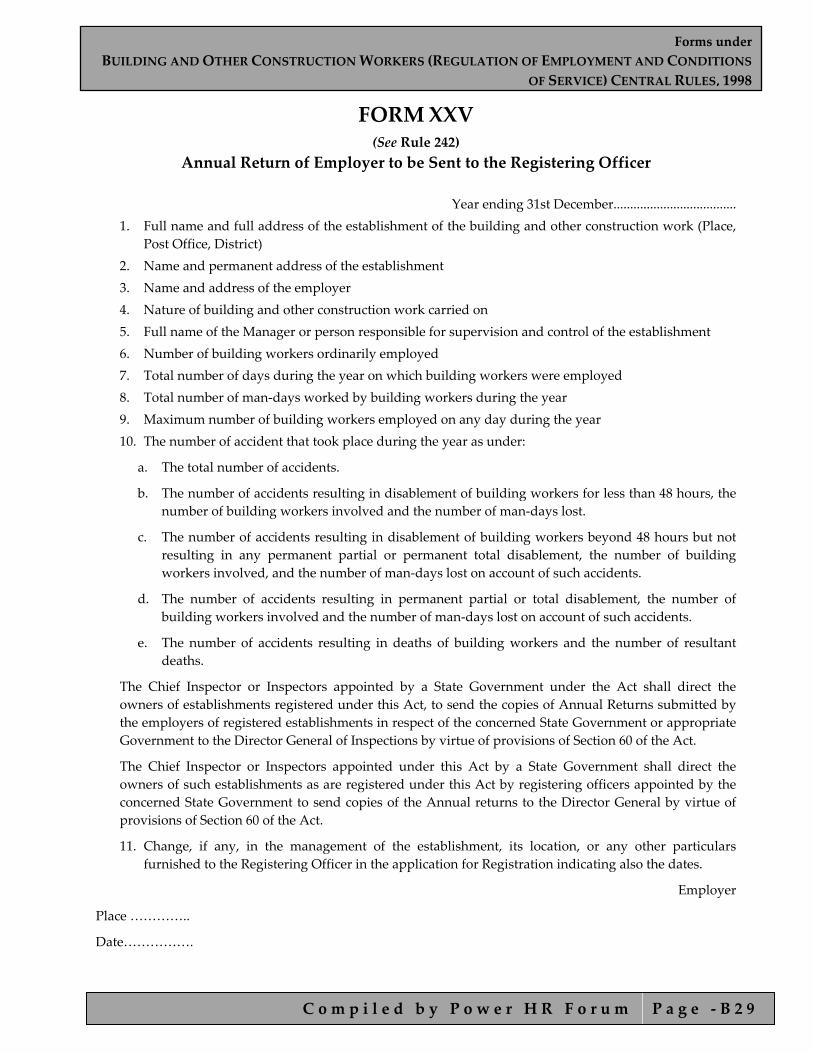
FORM XXV (See Rule 242)
Annual Return of Employer to be Sent to the Registering Officer
Year ending 31st December..................................... 1. Full name and full address of the establishment of the building and other construction work (Place,
Post Office, District) 2. Name and permanent address of the establishment 3. Name and address of the employer 4. Nature of building and other construction work carried on 5. Full name of the Manager or person responsible for supervision and control of the establishment 6. Number of building workers ordinarily employed 7. Total number of days during the year on which building workers were employed 8. Total number of man‐days worked by building workers during the year 9. Maximum number of building workers employed on any day during the year 10. The number of accident that took place during the year as under:
a. The total number of accidents.
b. The number of accidents resulting in disablement of building workers for less than 48 hours, the number of building workers involved and the number of man‐days lost.
c. The number of accidents resulting in disablement of building workers beyond 48 hours but not resulting in any permanent partial or permanent total disablement, the number of building workers involved, and the number of man‐days lost on account of such accidents.
d. The number of accidents resulting in permanent partial or total disablement, the number of building workers involved and the number of man‐days lost on account of such accidents.
e. The number of accidents resulting in deaths of building workers and the number of resultant deaths.
The Chief Inspector or Inspectors appointed by a State Government under the Act shall direct the owners of establishments registered under this Act, to send the copies of Annual Returns submitted by the employers of registered establishments in respect of the concerned State Government or appropriate Government to the Director General of Inspections by virtue of provisions of Section 60 of the Act.
The Chief Inspector or Inspectors appointed under this Act by a State Government shall direct the owners of such establishments as are registered under this Act by registering officers appointed by the concerned State Government to send copies of the Annual returns to the Director General by virtue of provisions of Section 60 of the Act.
11. Change, if any, in the management of the establishment, its location, or any other particulars furnished to the Registering Officer in the application for Registration indicating also the dates.
Employer
Place …………..
Date…………….
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 3 0
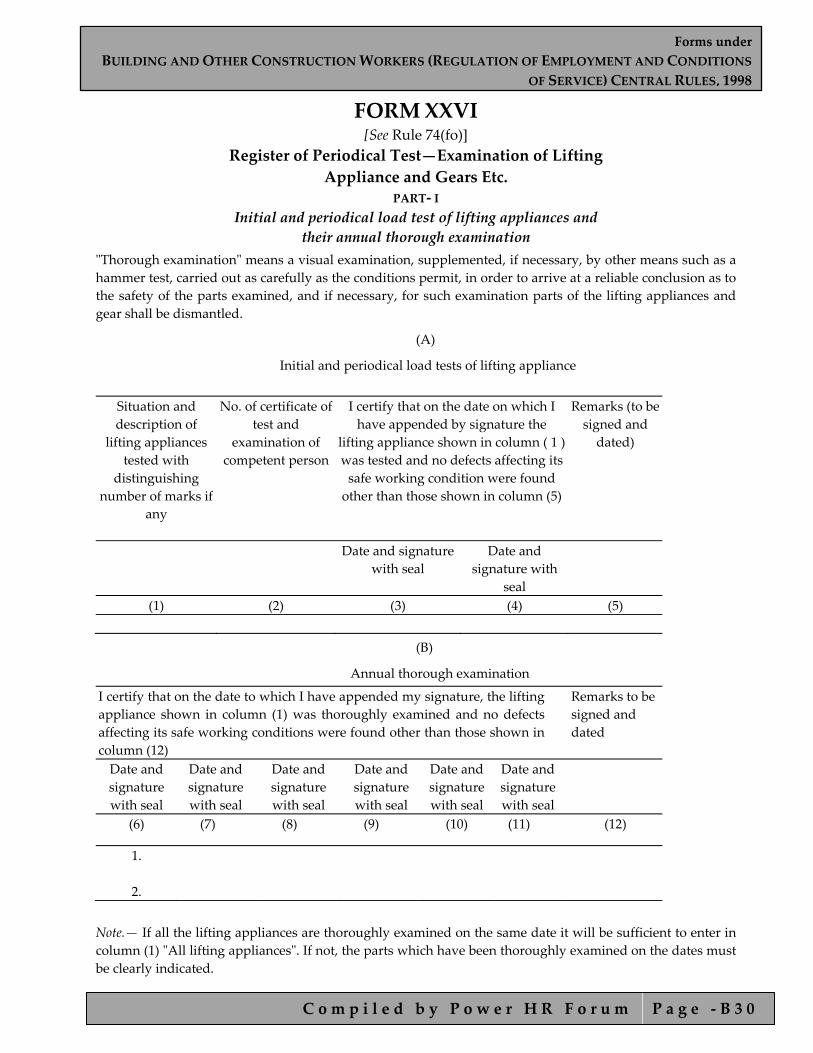
FORM XXVI [See Rule 74(fo)]
Register of Periodical Test—Examination of Lifting Appliance and Gears Etc.
PART‐ I Initial and periodical load test of lifting appliances and
their annual thorough examination ʺThorough examinationʺ means a visual examination, supplemented, if necessary, by other means such as a hammer test, carried out as carefully as the conditions permit, in order to arrive at a reliable conclusion as to the safety of the parts examined, and if necessary, for such examination parts of the lifting appliances and gear shall be dismantled.
(A)
Initial and periodical load tests of lifting appliance
Situation and description of
lifting appliances tested with
distinguishing number of marks if
any
No. of certificate of test and
examination of competent person
I certify that on the date on which I have appended by signature the
lifting appliance shown in column ( 1 ) was tested and no defects affecting its safe working condition were found other than those shown in column (5)
Remarks (to be signed and dated)
Date and signature with seal
Date and signature with
seal
(1) (2) (3) (4) (5)
(B)
Annual thorough examination
I certify that on the date to which I have appended my signature, the lifting appliance shown in column (1) was thoroughly examined and no defects affecting its safe working conditions were found other than those shown in column (12)
Remarks to be signed and dated
Date and signature with seal
Date and signature with seal
Date and signature with seal
Date and signature with seal
Date and signature with seal
Date and signature with seal
(6) (7) (8) (9) (10) (11) (12)
1. 2.
Note.— If all the lifting appliances are thoroughly examined on the same date it will be sufficient to enter in column (1) ʺAll lifting appliancesʺ. If not, the parts which have been thoroughly examined on the dates must be clearly indicated.

Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 3 1
PART II
Initial and periodical load test of loose gears and annual thorough examination
List of loose gear:
The following classes of loose gears namely—
1. Chains made of malleable cast iron;
2. Plate link chains;
3. Chains, rings, hooks, shackles and swivels made of steel;
4. Pitched chains;
5. Rings, hooks, shackles and swivels permanently attached to pitched chains, pulley blocks, container, spreaders, trays, slings, baskets, etc. and any other similar gear.
6. Hooks and swivels having screw‐threaded parts or ball bearings or other case‐heardened parts; and
7. Bordeaux connections.
Distinguishing No. or marks
Description of loose gear tested and
examined
No. of certificates of test and examination of
competent person
I certify that on the date to which I have
appended my signature the loose gears shown in
column (1) and (2) were tested and no defects affecting the
safe working condition were found
other than those shown in column (6)
Date and signature with seal
Date and signature with seal
(1) (2) (3) (4) (5)
1.
2.
3.
4.
5.
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 3 2
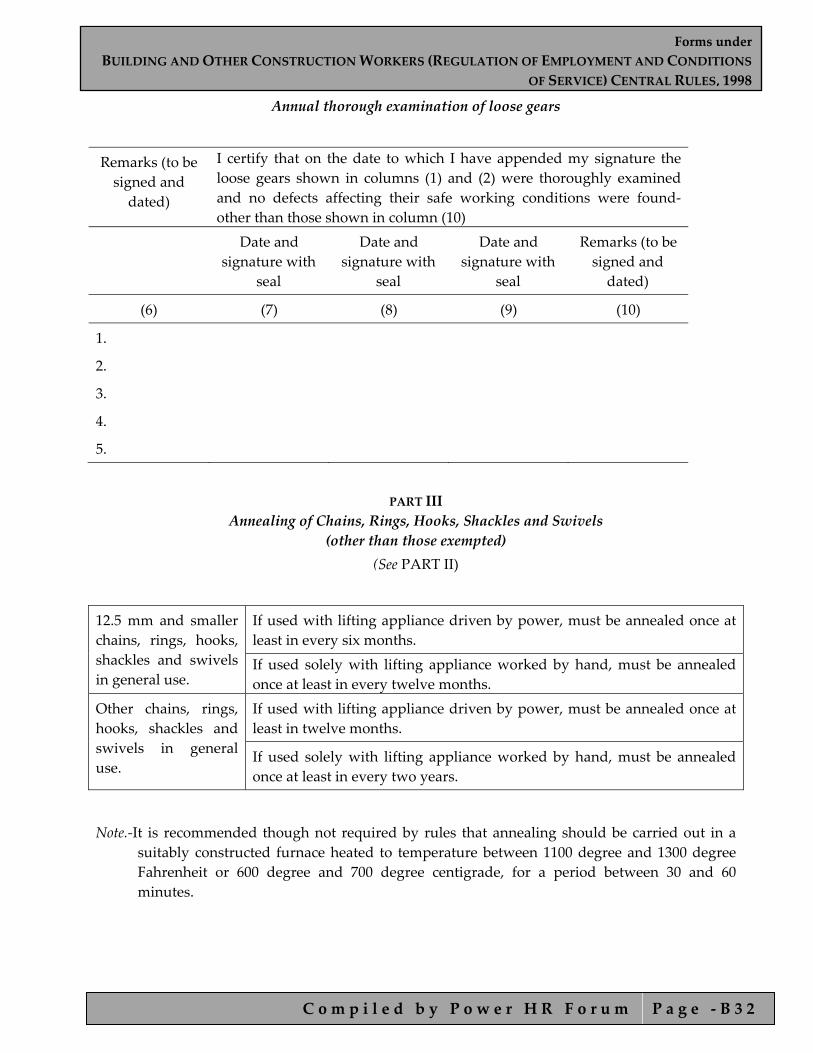
Annual thorough examination of loose gears
Remarks (to be signed and dated)
I certify that on the date to which I have appended my signature the loose gears shown in columns (1) and (2) were thoroughly examined and no defects affecting their safe working conditions were found‐other than those shown in column (10)
Date and signature with
seal
Date and signature with
seal
Date and signature with
seal
Remarks (to be signed and dated)
(6) (7) (8) (9) (10)
1.
2.
3.
4.
5.
PART III
Annealing of Chains, Rings, Hooks, Shackles and Swivels (other than those exempted)
(See PART II)
12.5 mm and smaller chains, rings, hooks, shackles and swivels in general use.
If used with lifting appliance driven by power, must be annealed once at least in every six months. If used solely with lifting appliance worked by hand, must be annealed once at least in every twelve months.
Other chains, rings, hooks, shackles and swivels in general use.
If used with lifting appliance driven by power, must be annealed once at least in twelve months.
If used solely with lifting appliance worked by hand, must be annealed once at least in every two years.
Note.‐It is recommended though not required by rules that annealing should be carried out in a suitably constructed furnace heated to temperature between 1100 degree and 1300 degree Fahrenheit or 600 degree and 700 degree centigrade, for a period between 30 and 60 minutes.
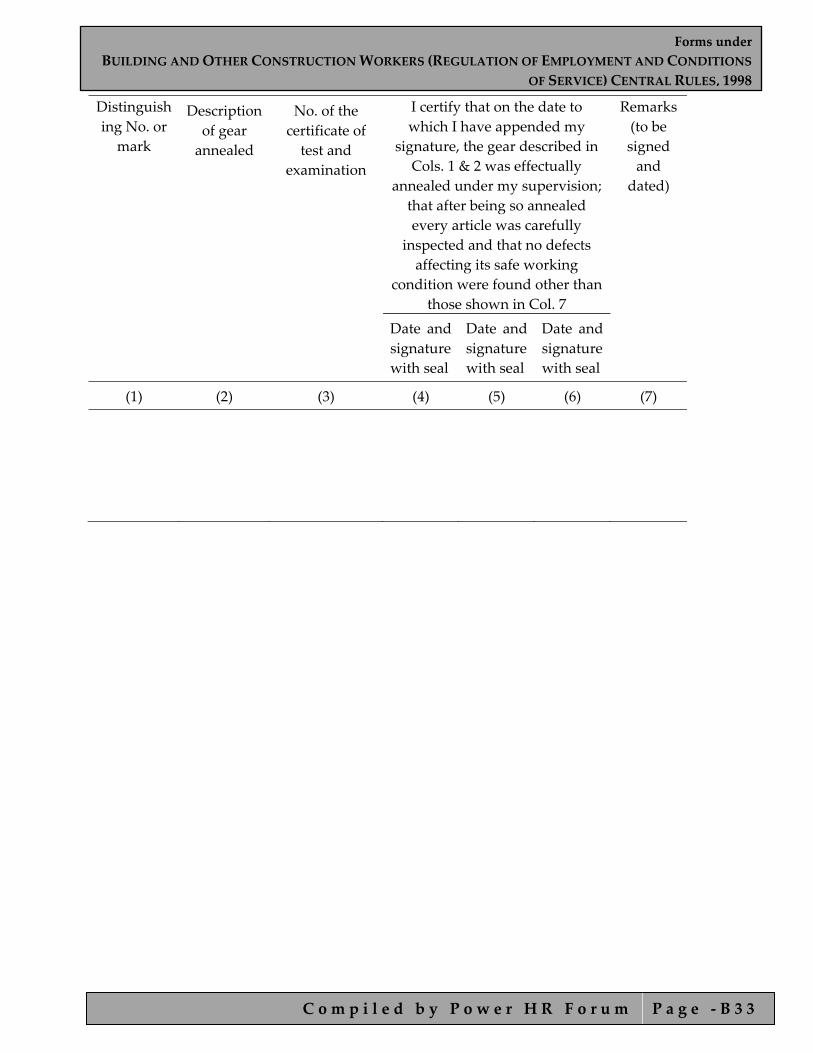
Forms underBUILDING AND OTHER CONSTRUCTION WORKERS (REGULATION OF EMPLOYMENT AND CONDITIONS
OF SERVICE) CENTRAL RULES, 1998
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ B 3 3
Distinguishing No. or
mark
Description of gear annealed
No. of the certificate of test and
examination
I certify that on the date to which I have appended my
signature, the gear described in Cols. 1 & 2 was effectually
annealed under my supervision; that after being so annealed every article was carefully
inspected and that no defects affecting its safe working
condition were found other than those shown in Col. 7
Remarks (to be signed and
dated)
Date and signature with seal
Date and signature with seal
Date and signature with seal
(1) (2) (3) (4) (5) (6) (7)

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1
Forms under
CONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2
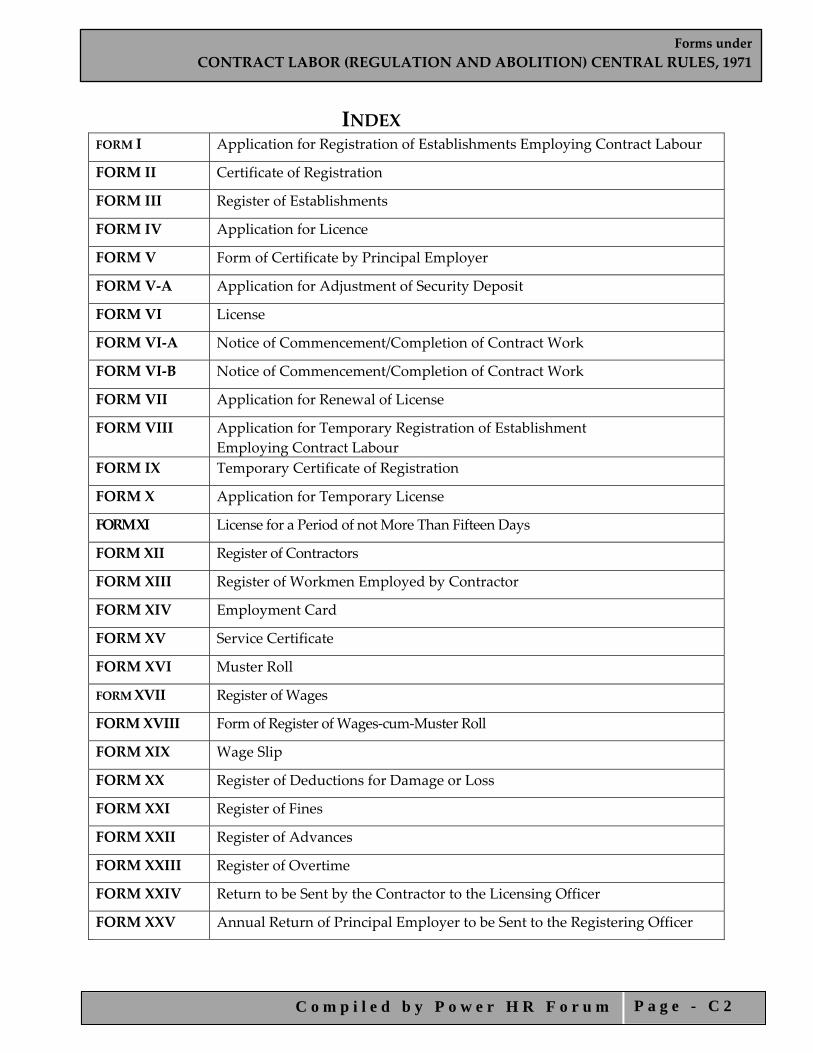
INDEX FORM I Application for Registration of Establishments Employing Contract Labour
FORM II Certificate of Registration
FORM III Register of Establishments
FORM IV Application for Licence
FORM V Form of Certificate by Principal Employer
FORM V‐A Application for Adjustment of Security Deposit
FORM VI License
FORM VI‐A Notice of Commencement/Completion of Contract Work
FORM VI‐B Notice of Commencement/Completion of Contract Work
FORM VII Application for Renewal of License
FORM VIII Application for Temporary Registration of Establishment Employing Contract Labour
FORM IX Temporary Certificate of Registration
FORM X Application for Temporary License
FORM XI License for a Period of not More Than Fifteen Days
FORM XII Register of Contractors
FORM XIII Register of Workmen Employed by Contractor
FORM XIV Employment Card
FORM XV Service Certificate
FORM XVI Muster Roll
FORM XVII Register of Wages
FORM XVIII Form of Register of Wages‐cum‐Muster Roll
FORM XIX Wage Slip
FORM XX Register of Deductions for Damage or Loss
FORM XXI Register of Fines
FORM XXII Register of Advances
FORM XXIII Register of Overtime
FORM XXIV Return to be Sent by the Contractor to the Licensing Officer
FORM XXV Annual Return of Principal Employer to be Sent to the Registering Officer

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 3
FORM I [See Rule 17(1)]
Application for Registration of Establishments Employing Contract Labour
1. Name and location of the Establishment. 2. Postal address of the Establishment. 3. Full name and address of the Principal Employer (furnish fatherʹs name in the
case of individuals). 4. Full name and address of the Manager or person responsible for the supervision
and control of the establishment. 5. Nature of work carried on in the Establishment. 6. Particulars of contractors and Contract Labour:
a. Names and Addresses of Contractors. b. Nature of work in which contract labour is employed or is to be employed. c. Maximum number of contract labour to be employed on any day through
each contractor. (cc)Estimated date of commencement of each contract work under each contractor.]
d. Estimated date of termination of employment of contract labour under each Contractor.
7. Particulars of demand draft enclosed (Name of the Union Bank, amount, demand draft No. and date).]
I hereby declare that the particulars given above are true to the best of my knowledge and belief.
Principal Employer
Seal and Stamp
Office of the Registering Officer.
Date of receipt of application.
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 4
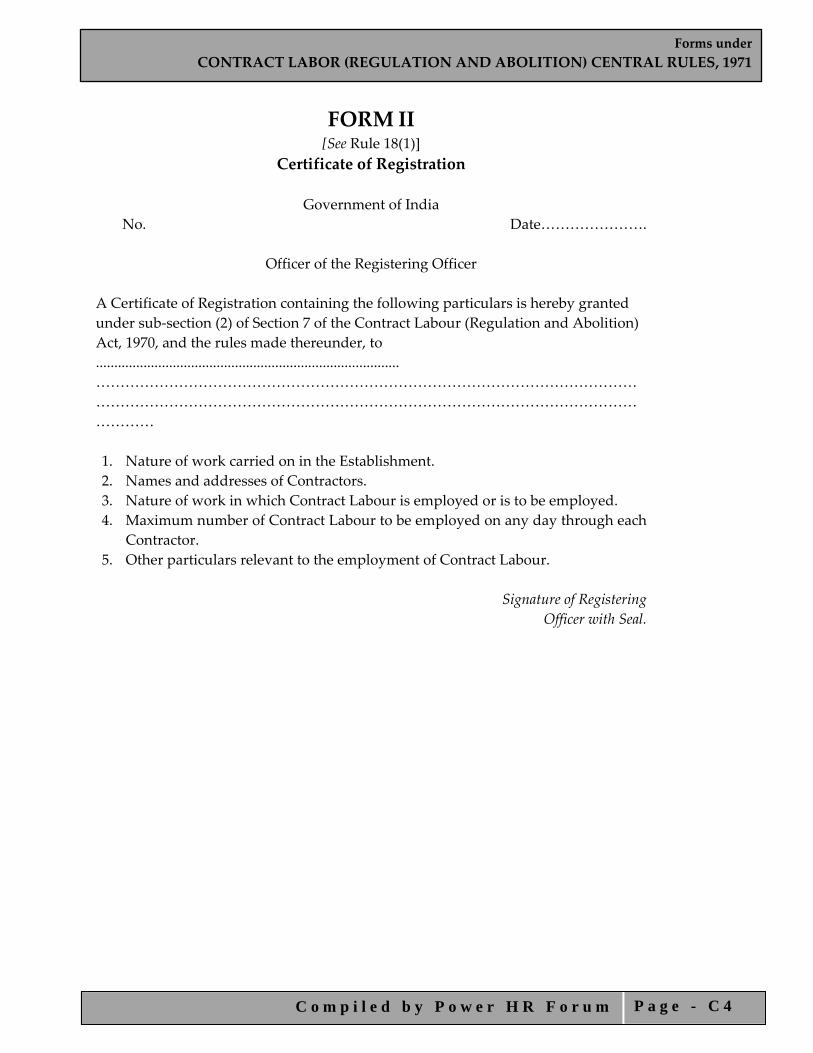
FORM II [See Rule 18(1)]
Certificate of Registration
Government of India No. Date………………….
Officer of the Registering Officer
A Certificate of Registration containing the following particulars is hereby granted under sub‐section (2) of Section 7 of the Contract Labour (Regulation and Abolition) Act, 1970, and the rules made thereunder, to ................................................................................... ……………………………………………………………………………………………………………………………………………………………………………………………………………… 1. Nature of work carried on in the Establishment. 2. Names and addresses of Contractors. 3. Nature of work in which Contract Labour is employed or is to be employed. 4. Maximum number of Contract Labour to be employed on any day through each
Contractor. 5. Other particulars relevant to the employment of Contract Labour.
Signature of Registering Officer with Seal.
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 5
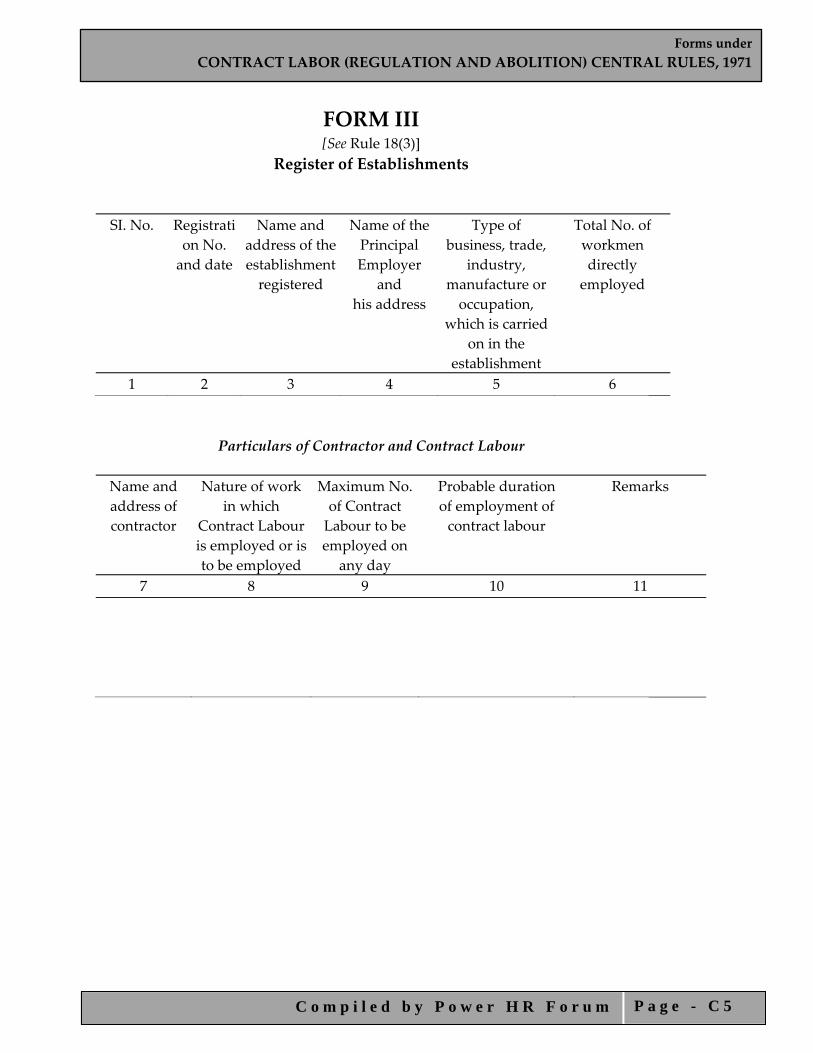
FORM III [See Rule 18(3)]
Register of Establishments
SI. No. Registration No. and date
Name and address of theestablishmentregistered
Name of thePrincipal Employer
and his address
Type of business, trade,
industry, manufacture or occupation,
which is carried on in the
establishment
Total No. of workmen directly employed
1 2 3 4 5 6
Particulars of Contractor and Contract Labour Name and address of contractor
Nature of work in which
Contract Labour is employed or is to be employed
Maximum No. of Contract Labour to be employed on
any day
Probable duration of employment of contract labour
Remarks
7 8 9 10 11
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 6
FORM IV [See Rule 21(1)]
Application for License
1. Name and address of the contractor (including his fatherʹs name in case of individuals). 2. Date of birth and age (in case of individuals). 3. Particulars of Establishment where Contract Labour is to be employed—
(a) Name and address of the Establishment. (b) Type of business, trade, industry, manufacture or occupation, which is carried on in the
Establishment. (c) Number and date of Certificate of Registration of the Establishment under the Act. (d) Name and address of the Principal Employer.
4. Particulars of Contract Labour— 1) Nature of work in which Contract Labour is employed or is to be employed in the
Establishment. 2) Duration of the proposed contract work (give particulars of proposed date of commenc‐
ing and ending). 3) Name and address of the Agent or Manager of Contractor at the worksite. 4) Maximum number of Contract Labour proposed to be employed in the Establishment on
any date. 5. Whether the contractor was convicted of any offence within the preceding five years. If so,
give details. 6. Whether there was any order against the contractor revoking or suspending licence or
forfeiting security deposits in respect of an earlier contract. If so, the date of such order. 7. Whether the contractor has worked in any other establishment within the past five years. If so,
give details of the Principal Employer, Establishments, and nature of work. 8. Whether a certificate by the Principal Employer in Form V is enclosed. 9. Amount of licence fee—name of the Union Bank, demand draft No. and date.] 10. Amount of security deposit—name of the Union Bank, demand draft No. and date. Note.— The application shall be accompanied by demand draft and the challan for the
appropriate amount and a certificate in Form V from the principal employer ……………………. date of the receipt of the application with ʹdemand draftʹ and the challan for fees/security deposit.]
Declaration.— I hereby declare that the details given above are correct to the best of my knowledge and belief.
Signature of the Applicant (Contractor)
Place .............. Date ............... Note.—The application should be accompanied by a Treasury Receipt for the appropriate amount
and a certificate in Form V from the Principal Employer.
(To be filled in the office of the Licensing Officer) Date of receipt of the application with challan for fees/security deposit.
Signature of the Licensing Officer.

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 7
FORM V [See Rule 21(2)]
Form of Certificate by Principal Employer Certified that I have engaged the applicant (name of the contractor) as a contractor in my establishment. I undertake to be bound by all the provisions of the Contract Labour (Regulation and Abolition) Act, 1970, and the Contract Labour (Regulation and Abolition) Central Rules, 1971, insofar as the provisions are applicable to me in respect of the employment of Contract Labour by the applicant in my establishment. Place ................... Signature of Principal Employer Date .................... Name and address Establishment

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 8
FORM V‐A [See Rule 24(1‐A)]
Application for Adjustment of Security Deposit
Name and address of the Contractor
No. and date of licence
Date of expiry of previous licence
Whether the licence of the contractor was suspended or
revoked
(1) (2) (3) (4)
No. and date of the demand draft of the
security deposit in respect of the previous licence
Amount of previous security ‐deposit
No. and date of the demand draft of the balance of security deposit,
if any, required on the fresh contract
(5) (6) (7) No. and date of certificate
of registration of the establishment in relation to which the new licence
is applied for
Name and address of the principal employer
Particulars of fresh contract
Remarks
(8) (9) (10) (11) Place :
Signature of the Applicant. Date :

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 9
FORM VI [See Rule 25(1)]
Government of India
OFFICE OF LICENSING OFFICER Licence No. Dated Fee paid Rs ..................
License
1. Licence is hereby granted to ......................... under Section 12(1) of the Contract Labour (regulation and Abolition) Act, 1970, subject to the conditions specified in Annexure.
2. This licence is for doing the work of (nature of work to be indicated) in the
establishment of________(name of principal employer to be indicated) at______(place of work to be indicated).
3. The licence shall remain in force till__________(date to be indicated). Date……………………….. Signature and Seal of Licensing Officer
RENEWAL
[See Rule 29]
Date of renewal Fee paid for renewal Date of expiry 1. 2. 3.
Date. ........................ Signature and Seal of the Licensing Officer
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 0
ANNEXURE TO FORM VI
The licence is subject to the following conditions— 1. The licence shall be non‐transferable. 2. The number of workmen employed as Contract Labour in the establishment shall
not, on any day, exceed. ........ 3. Except as provided in the rules the fees paid for the grant, or as the case may be,
for renewal of the licence shall be non‐refundable. 4. The rates of wages payable to the workmen by the contractor shall not be less
than the rates prescribed for the Schedule of employment under the Minimum Wages Act, 1948, where applicable, and where the rates have been fixed by agreement, settlement or award, not less than the rates fixed.
5. In cases where the workmen employed by the contractor perform the same or similar kind of work as the workmen directly employed by the principal employer of the establishment, the wage rates, holidays, hours of work and other conditions of service of the workmen of the contractor shall be the same as applicable to the workmen directly employed by the principal employer of the establishment on the same or similar kind of work: provided that in the case of any disagreement with regard to the type of work the same shall be decided by the [Deputy] Chief Labour Commissioner (Central), whose decision shall be final.
6. In other cases the wage rates, holidays, hours of work and conditions of service of the workmen of the contractor shall be such as may be specified in this behalf by the [Deputy] Chief Labour Commissioner (Central).
7. In every establishment where 20 or more women are ordinarily employed as contract labour there shall be provided two rooms of reasonable dimensions for the use of their children under the age of six years. One of such rooms would be used as a play‐room for the children and the other as bedroom for the children. For this purpose the contractor shall supply adequate number of toys and games in the play‐room and sufficient number of cots and beddings in the sleeping‐room. The standard of construction and maintenance of the creches may be such as may be specified in this behalf by the Chief Labour Commissioner (Central).
8. The licensee shall notify any change in the number of workmen or the conditions of work to the Licensing Officer.
9. A copy of the licence shall be displayed prominently at the premises where the contract work is being carried on.]
10. The licensee shall, within fifteen days of the commencement and completion of each contract work submit a return to the Inspector appointed under Section 28 of the Act intimating the actual date of the commencement or, as the case may be, completion of such contract work in Form VI‐A.]

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 1
FORM VI‐A [See Rule 25(2)(vm)]
Notice of Commencement/Completion of Contract Work
I/We, Shri/M/s. (Name and address of the contractor) hereby intimate that the contract work (Name of work). ……... in establishment of the ...................... (Name and address of principal employer). ............... for which licence No ....................... dated ..................has been issued to me/us by the Licensing Officer (name of the headquarters), has been commenced/completed with effect from (date) /on (date). To
Signature of Contractors) The Inspector, …………………….. …………………………

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 2
FORM VI‐B [See Rule 81(3)]
Notice of Commencement/Completion of Contract work
1. Name of the principal employer and address ........... 2. No. and date of certificate of Registration ........... 3. I/We hereby intimate that the contract work (Name of work) given to (name
and address of the contractor) having licence No ..................... dated ............................. has been commenced/completed with effect from (date)/on (date).
Signature of the Principal Employer
To The Inspector, …………………….. …………………………
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 3
FORM VII [See Rule 29(2)]
Application for Renewal of License 1. Name and address of the contractor. 2. Number and date of the licence. 3. Date of expiry of the previous licence. 4. Whether the licence of the contractor was suspended or revoked. 5. Name of the Bank, number and date of the demand draft enclosed. Date of
receipt of the application with demand draft number and date. Place ...................
Date ..................... Signature of the Applicant
(To be filled in the Office of the Licensing Officer)
Date of receipt of the application with Treasury Receipt No. and date.
Signature of the Licensing Officer
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 4
FORM VIII [See Rule 32(2)]
Application for Temporary Registration of Establishment Employing Contract Labour
1. Name and location of the establishment. 2. Postal address of the establishment. 3. Full name and address of the Principal Employer (furnish fatherʹs name in the
case of individuals). 4. Full name and address of the Manager or person responsible for the supervision
and control of the establishment. 5. Nature of work carried on in the establishment. 6. Particulars of contract labour:
A. Nature of work in which contract labour is to be employed and reasons for urgency.
B. Maximum number of contract labour to be employed on any day. C. Estimated date of termination of employment of contract labour.
7. Particulars of demand draft enclosed (name of the Union Bank, demand draft No. and date).
I hereby declare that the particulars given above are true to the best of my knowledge and belief.
Principal Employer Seal and Stamp
Time and date of receipt of application with Treasury Receipt [* *] .
Office of the Registering Officer

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 5
FORM IX [See Rule 32(3)]
Temporary Certificate of Registration
No. Date of Expiry …............. Date
Government of India Office of the Registering Officer
A Temporary Certificate of Registration containing the following particulars is hereby granted under sub‐section (2) of Section 7 of the Contract Labour (Regulation and Abolition) Act, 1970, and the rules made thereunder, to ............................. valid from ................... ..... to ............................
1. Nature of work carried on in the establishment. 2. Nature of work in which Contract Labour is to be employed. 3. Maximum number of Contract Labour to be employed on any day. 4. Other particulars relevant to the employment of Contract Labour.
Signature of Registering Officer with Seal
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 6
FORM X [See Rule 32(2)]
Application for Temporary Licence 1. Name and address of the contractor (including his fatherʹs name in case of
individuals). 2. Date of birth and age (in case of individuals). 3. Particulars of Establishment where Contract Labour is to be employed—
a) Name and address of the Establishment. b) Type of business, trade, industry, manufacture or occupation, which is carried on
in the establishment. c) Name and address of the Principal Employer.
4. Particulars of Contract Labour— a) Nature of work in which Contract Labour is to be employed in the establishment. b) Duration of the proposed contract work (give particulars of proposed date of
commencing and ending). c) Name and address of the Agent or Manager of Contractor at the work‐site. d) Maximum number of Contract Labour proposed to be employed in the
establishment on any day. 5. Whether the contractor was convicted of any offence within the preceding five years.
If so, give details. 6. Whether there was any order against the contractor revoking or suspending licence
or forfeiting security deposits in respect of an earlier contract. If so, the date of such order.
7. Whether the contractor has worked in any other establishment within the past five years. If so, give details of the Principal Employer, Establishments and nature of work.
8. Amount of licence fee paid—name of the Union Bank, demand draft No. and date. 9. Amount of security deposit—name of the Union Bank, demand draft No. and date.
Date of the receipt of the application with demand draft for fees/security deposits. Place…………… Signature of the Applicant Date ……………
(Contractor)
(To be filled in the Office of the Licensing Officer) Date of receipt of the application with challan for fees . . . . . . . . . Security Deposit
Signature of the Licensing Officer

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 7
FORM XI [See Rule 32(3)]
Government of India
OFFICE OF THE LICENSING OFFICER
Licence No. Dated Fee paid Rs … … … … … …
Signature of the Licensing Officer Temporary Licence Expires on . . . . . . . . .
Licence is hereby granted to . . . . . . . . . . . under Section 12(2) of the Contract Labour (Regulation and Abolition) Act, 1970, subject to the conditions specified in Annexure. The Licence shall remain in force till . . . . . . . . . . . . . . . . . . . .
Date . . . . . . . . . . . . . . . . . . . . . . . . . . .
Signature and Seal of the Licensing Officer ANNEXURE
The licence is subject to the following conditions:— 1) The licence shall be non‐transferable. 2) The number of workmen employed as Contract Labour in the establishment
shall not, on any day, exceed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3) Except as provided in the rules the fees paid for the grant of the licence shall
be non‐refundable. 4) The rates of wages payable to the workmen by the contractor shall not be less
than the rates prescribed for the Schedule of employment under the Minimum Wages Act, 1948, where applicable, and where the rates have been fixed by agreement, settlement or award, not less than the rates fixed.
5) In cases where the workmen employed by the contractor perform the same or similar kind of work as the workmen directly employed by the principal employer of the establishment, the wage rates, holidays, hours of work and other conditions of service of the workmen of the contractor shall be the same as applicable to the workmen directly employed by the principal employer of the establishment on the same or similar kind of work: Provided that in the case of any disagreement with regard to the type of work the same shall be decided by the [Deputy] Chief Labour Commissioner (Central), whose decision shall be final.
6) In other cases the wage rates, holidays, hours of work and conditions of service of the workmen of the contractor shall be such as may be specified in this ʹbehalf by the Chief Labour Commissioner (Central).
7) A copy of the licence shall be displayed prominently at the premises where the contract work is being carried on.

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 8
FORM XII [See Rule 74]
Register of Contractors
1 . Name and address of the Principal Employer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. Name and address of the establishment .................................
Sl No. Name and address of contractor
Nature of work on contract
Location of contract work
Period of contract
Maximum No. of
workmen employed by contractor
From To
Place …………………….. Date ………………………
Signature of the Licensing Officer
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 1 9
FORM XIII
[See Rule 75] Register of Workmen Employed by Contractor
Name and address of Contractor .......................................................
Name and address of establishment in/under which............................................ contract is carried on .............. .....
Nature and location of work .................................................................
Name and address of Principal Employer………………………………………………………………………………………………………..
SI. No.
Name and surname of workman
Age and Sex
Fatherʹs/Husbandʹs name
Nature of Employment/ Designation
Permanent Home Address of
workman(Village and Tahsil/Taluk and District)
1 2 3 4 5 6
Local Address
Date of commencement of employment
Signature or thumb‐
impression of workman
Date of termination of employment
Reasons for termination
Remarks
7 8 9 10 11 12
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 0
FORM XIV [See Rule 76]
Employment Card
Name and address of Contractor ………………………………………………
Name and address of Establishment in/under which contract is carried on……….. ……………………...…………………………..……..
Nature of work and location of work ……………………………………………. …………...................................................
Name and address of Principal Employer….. ……………………...…………………………..……..
1. Name of the workman .................................................................................... 2. SI. No. in the register of workmen employed
…………………………………………………….. 3. Nature of employment/Designation ............................................................................ 4. Wage rate (with particulars of unit, in case of piece‐work) ............................... 5. Wage period ...................................................................................... 6. Tenure of employment ...................................................................................... 7. Remarks ........................................................................................................
Signature of Contractor
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 1
FORM XV [See Rule 77]
Service Certificate Name and address of contractor ……………………………
Name and address of establishment in/under which contract is carried on .............................................
Nature and location of work. ……………………………
Name and address of Principal Employer………………………………………….
Name and address of the work‐man………………….……………………………
Age or Date of Birth ……………………………
Identification Marks ……………………………
Fatherʹs/Husbandʹs name ……………………………
SI. No Total period for
which employed Nature of work
done Rate of wages
(with particulars of unit in case of piece‐work)
Remarks
From To
1 2 3 4 5 6
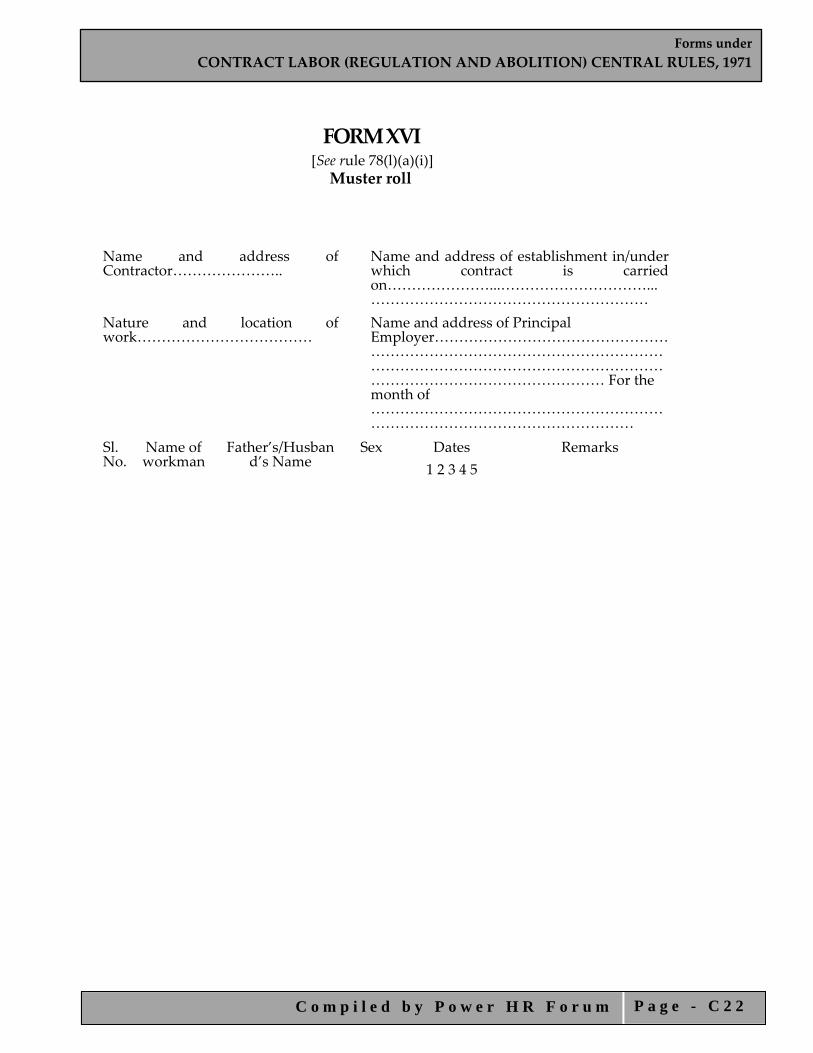
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 2
FORM XVI [See rule 78(l)(a)(i)] Muster roll
Name and address of Contractor…………………..
Name and address of establishment in/under which contract is carried on…………………...…………………………...…………………………………………………
Nature and location of work………………………………
Name and address of Principal Employer……………………………………………………………………………………………………………………………………………………………………………………………… For the month of ……………………………………………………………………………………………………
Sl. No.
Name of workman
Father’s/Husband’s Name
Sex Dates Remarks 1 2 3 4 5
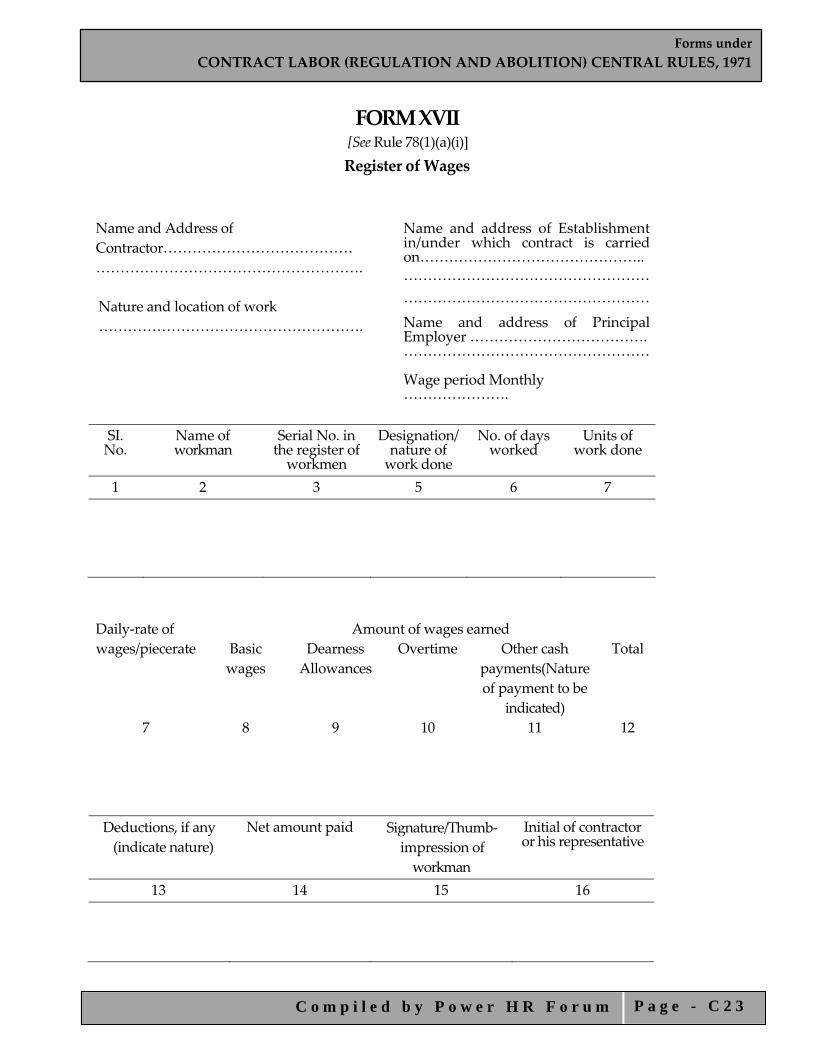
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 3
FORM XVII [See Rule 78(1)(a)(i)] Register of Wages
Name and Address of Contractor………………………………… ……………………………………………….
Name and address of Establishment in/under which contract is carried on……………………………………….. ……………………………………………
Nature and location of work ……………………………………………
………………………………………………. Name and address of Principal Employer ………………………………. …………………………………………… Wage period Monthly ………………….
SI. No.
Name of workman
Serial No. in the register of workmen
Designation/ nature of work done
No. of days worked
Units of work done
1 2 3 5 6 7
Daily‐rate of wages/piecerate
Amount of wages earned Basic wages
Dearness Allowances
Overtime Other cash payments(Nature of payment to be
indicated)
Total
7 8 9 10 11 12
Deductions, if any (indicate nature)
Net amount paid Signature/Thumb‐ impression of workman
Initial of contractor or his representative
13 14 15 16
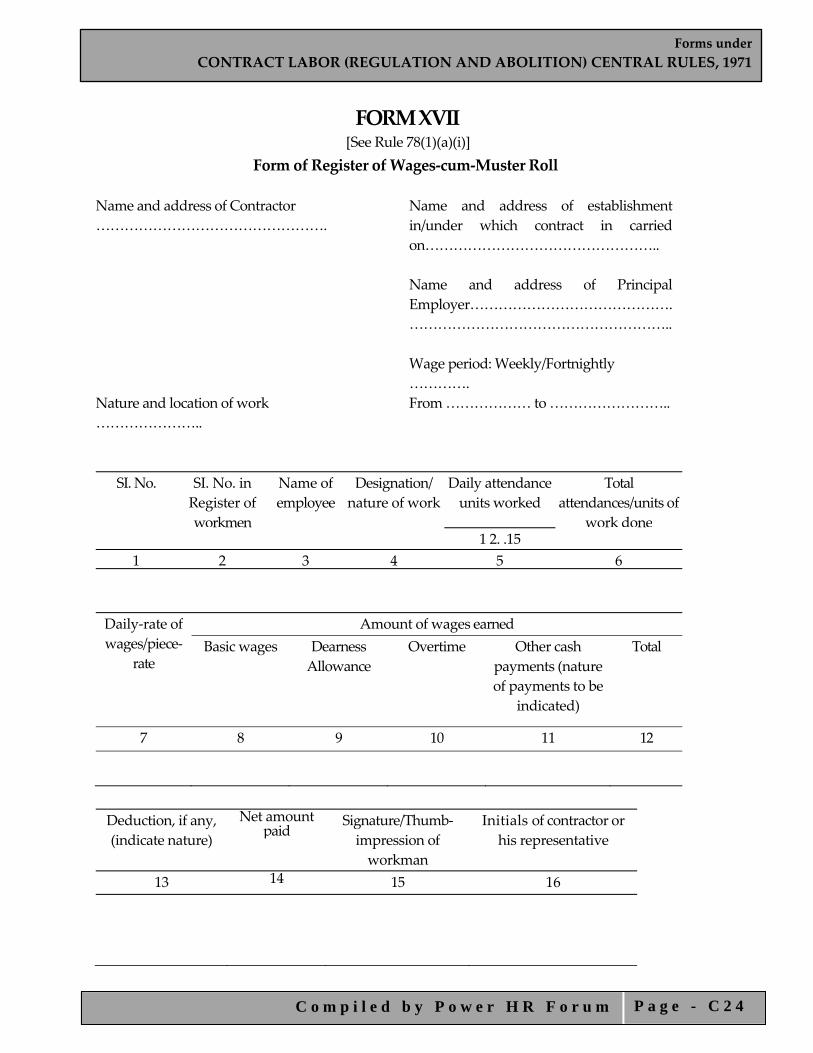
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 4
FORM XVII [See Rule 78(1)(a)(i)]
Form of Register of Wages‐cum‐Muster Roll Name and address of Contractor ………………………………………….
Name and address of establishment in/under which contract in carried on………………………………………….. Name and address of Principal Employer……………………………………. ……………………………………………….. Wage period: Weekly/Fortnightly ………….
Nature and location of work …………………..
From ……………… to ……………………..
SI. No.
SI. No. in Register of workmen
Name of employee
Designation/ nature of work
Daily attendance units worked
Total attendances/units of
work done 1 2. .15
1 2 3 4 5 6 Daily‐rate of wages/piece‐
rate
Amount of wages earned Basic wages
Dearness Allowance
Overtime
Other cash payments (nature of payments to be
indicated)
Total
7 8 9 10 11 12
Deduction, if any, (indicate nature)
Net amount paid
Signature/Thumb‐impression of workman
Initials of contractor or his representative
13 14 15 16
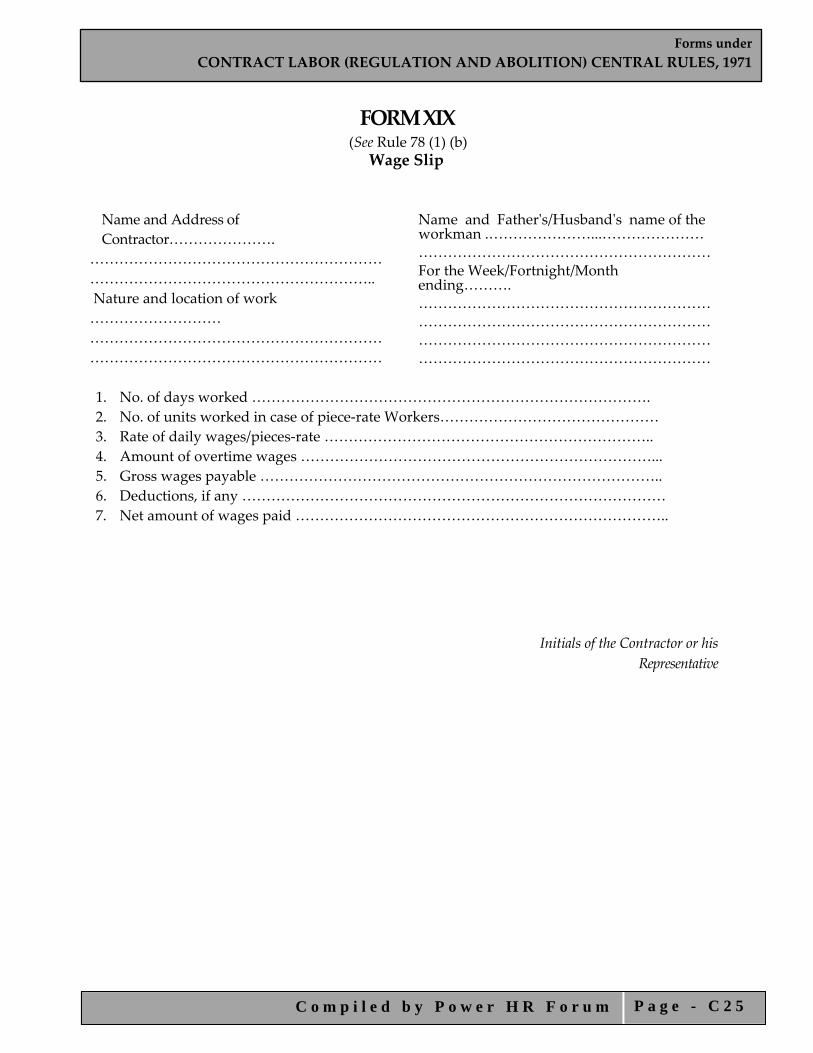
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 5
FORM XIX
(See Rule 78 (1) (b) Wage Slip
Name and Address of Contractor………………….
…………………………………………………… ………………………………………………….. Nature and location of work ……………………… …………………………………………………… ……………………………………………………
Name and Fatherʹs/Husbandʹs name of the workman .…………………...………………… ……………………………………………………For the Week/Fortnight/Month ending………. ……………………………………………………………………………………………………………………………………………………………………………………………………………………
1. No. of days worked ………………………………………………………………………. 2. No. of units worked in case of piece‐rate Workers……………………………………… 3. Rate of daily wages/pieces‐rate ………………………………………………………….. 4. Amount of overtime wages ………………………………………………………………... 5. Gross wages payable ……………………………………………………………………….. 6. Deductions, if any …………………………………………………………………………… 7. Net amount of wages paid …………………………………………………………………..
Initials of the Contractor or his Representative
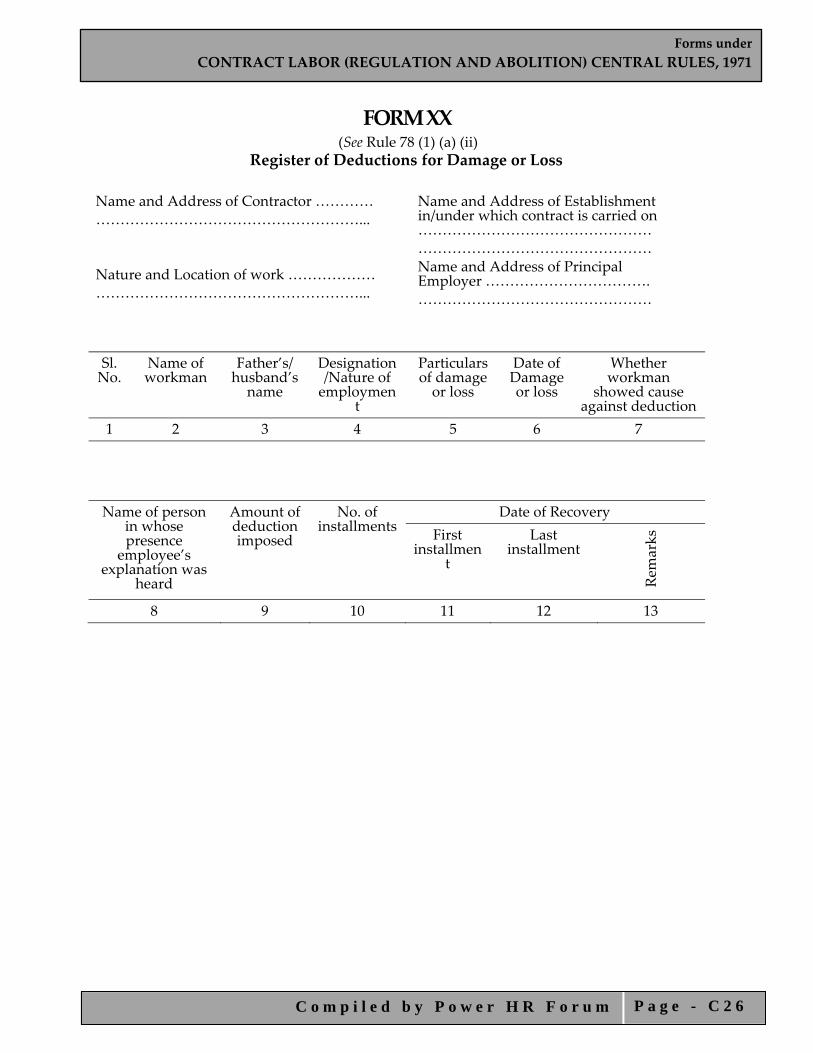
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 6
FORM XX (See Rule 78 (1) (a) (ii)
Register of Deductions for Damage or Loss Name and Address of Contractor ………… ………………………………………………... Nature and Location of work ……………… ………………………………………………...
Name and Address of Establishment in/under which contract is carried on ………………………………………… ………………………………………… Name and Address of Principal Employer ……………………………. …………………………………………
Sl. No.
Name of workman
Father’s/ husband’s name
Designation/Nature of employmen
t
Particulars of damage or loss
Date of Damage or loss
Whether workman
showed cause against deduction
1 2 3 4 5 6 7
Name of person in whose presence
employee’s explanation was
heard
Amount of deduction imposed
No. of installments
Date of Recovery First
installment
Last installment
Remarks
8 9 10 11 12 13

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 7
FORM XXI [See Rule 78(1) (a)(ii)] Register of Fines
Name and Address of Contractor …………………………………………………..
Name and Address of Establishment in/under which contract is carried on ……………………………………….. ………………………………………..
Nature and location work …………………………………………………..
Name and Address of Principal Employer ……………………………... ………………………………………….
Sl. No.
Name of workman
Father’s/ husband’s name
Designation/Nature of employment
Act Omission for which fine imposed
Date of offence
1 2 3 4
5 6
Whether work‐man showed cause against
fine
Name of person in whose presence employeeʹs
explanation was heard
Wage periods and
wages payable
Amount of fine imposed
Date on which fine realized
Remarks
7 8 9 10 11 12

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 8
FORM XXII [See Rule 78(1) (a)(ii)] Register of Advances
Name and Address of Contractor …………………………………………………..
Name and Address of Establishment in/under which contract is carried on ……………………………………….. ………………………………………..
Nature and location work …………………………………………………..
Name and Address of Principal Employer ……………………………... ………………………………………….
Sl. No.
Name Father’s/ husband’s name
Nature of employment/Designation
Wage period and wages payable
Date and amount of
advance given 1 2 3 4 5 6
Purpose(s) for which advance
made
No. of installments by which advance to be repaid
Date and amount of
each installment repaid
Date on which last installment was repaid
Remarks
7 8 9 10 11
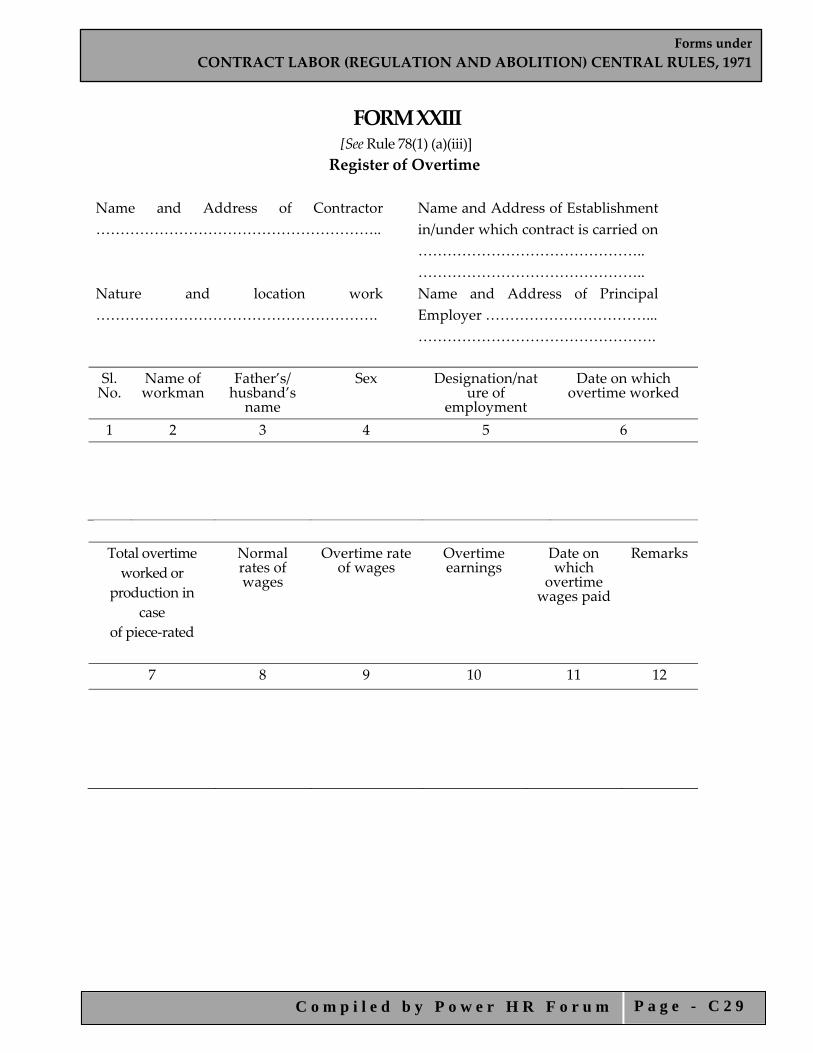
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 2 9
FORM XXIII [See Rule 78(1) (a)(iii)] Register of Overtime
Name and Address of Contractor …………………………………………………..
Name and Address of Establishment in/under which contract is carried on ……………………………………….. ………………………………………..
Nature and location work ………………………………………………….
Name and Address of Principal Employer ……………………………... ………………………………………….
Sl. No.
Name of workman
Father’s/ husband’s name
Sex Designation/nature of
employment
Date on which overtime worked
1 2 3 4 5 6
Total overtime worked or
production in case
of piece‐rated
Normal rates of wages
Overtime rate of wages
Overtime earnings
Date on which
overtime wages paid
Remarks
7 8 9 10 11 12

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 3 0
FORM XXIV [(See Rule 82 (1)]
Return to be Sent by the Contractor to the Licensing Officer
Half‐Year‐Ending .....................
1. Name and address of the Contractor 2. Name and address of the establishment 3. Name and address of the Principal employer 4. Duration of contract: From ................ to ……. 5. No. of days during the half‐year on which—
a. the establishment of the principal employer had worked b. the contractorʹs establishment had worked
6. Maximum number of contract labour employed on any day during the half year: Men Women Children Total 7.
i. Daily hours of work and spread over— ii.
a) whether weekly holiday observed and on what day— b) if so, whether it was paid for—
iii. No. of man‐hours of overtime worked— 8. Number of man‐days worked by— Men Women Children Total 9. Amount of wages paid— Men Women Children Total 10. Amount of deductions from wages, if any— Men Women Children Total 11. Whether the following have been provided—
i. Canteen……………….. ii. Rest‐Rooms ………….. iii. Drinking‐water………… iv. Creches……………….. v. First‐Aid………………..
(If the answer is ʹyesʹ state briefly standards provided) Place Date Signature of Contractor
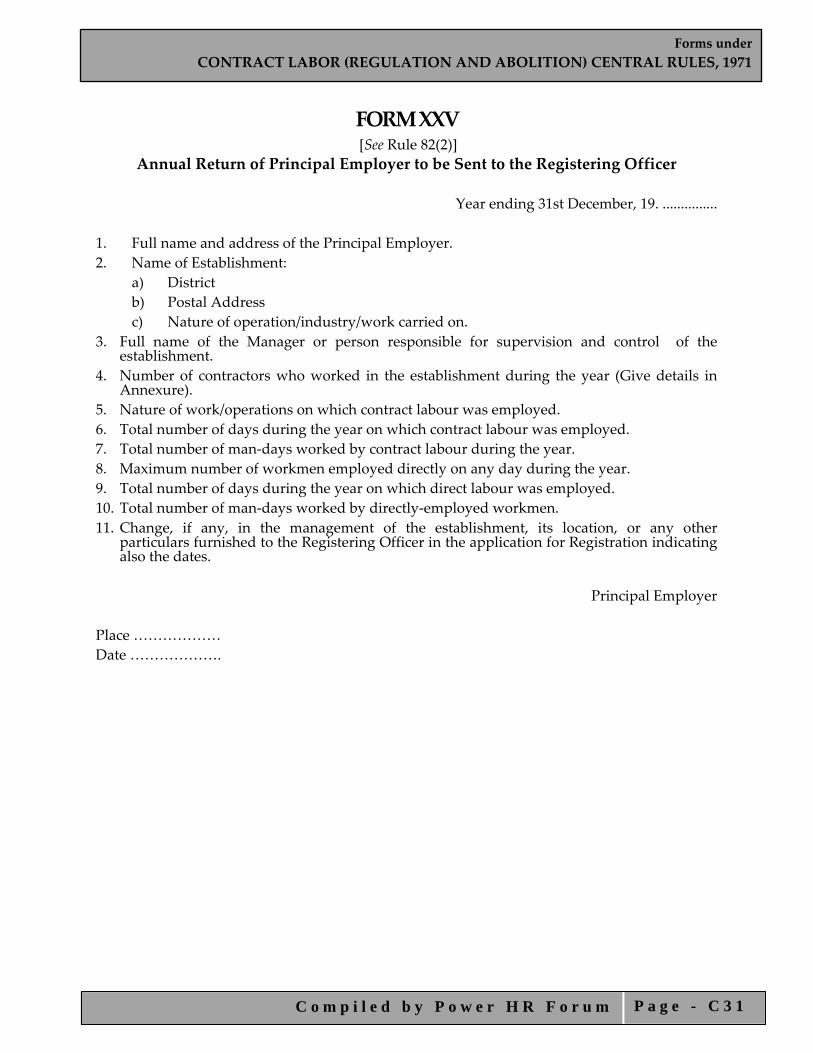
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 3 1
FORM XXV [See Rule 82(2)]
Annual Return of Principal Employer to be Sent to the Registering Officer
Year ending 31st December, 19. ...............
1. Full name and address of the Principal Employer. 2. Name of Establishment:
a) District b) Postal Address c) Nature of operation/industry/work carried on.
3. Full name of the Manager or person responsible for supervision and control of the establishment.
4. Number of contractors who worked in the establishment during the year (Give details in Annexure).
5. Nature of work/operations on which contract labour was employed. 6. Total number of days during the year on which contract labour was employed. 7. Total number of man‐days worked by contract labour during the year. 8. Maximum number of workmen employed directly on any day during the year. 9. Total number of days during the year on which direct labour was employed. 10. Total number of man‐days worked by directly‐employed workmen. 11. Change, if any, in the management of the establishment, its location, or any other
particulars furnished to the Registering Officer in the application for Registration indicating also the dates.
Principal Employer
Place ……………… Date ……………….
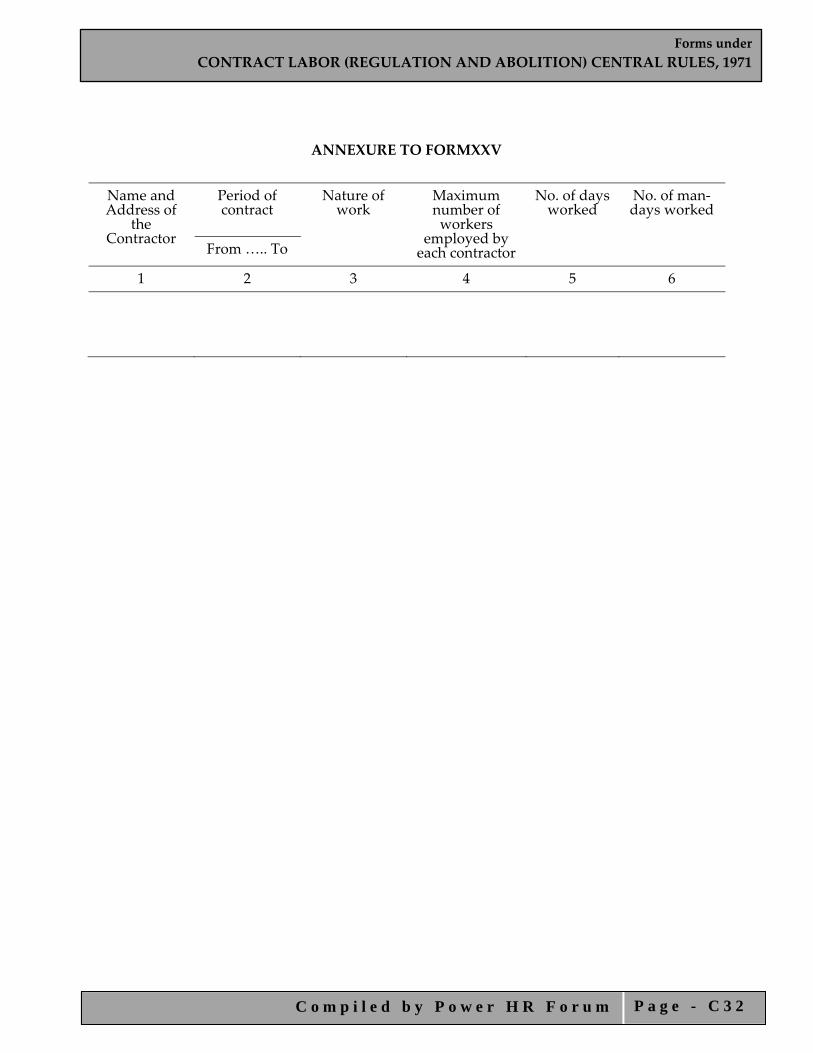
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 3 2
ANNEXURE TO FORMXXV
Name and Address of
the Contractor
Period of contract
Nature of work
Maximum number of workers
employed by each contractor
No. of days worked
No. of man‐days worked
From ….. To
1 2 3 4 5 6

Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 3 3
[ANNEXURE ‘A’] [Rule 38(1)]
Sl. No. Officers Headquarters of the Officers
1 2 3
1 ALC(C) Delhi Delhi
2 ALC(C) Ajmer Ajmer
3 ALC(C) Ajmer Ajmer
4 ALC(C) Adipur Adipur
5 RLC(C) Asansol Asansol
6 ALC(C) Asansol Asansol
7 RLC(C) Bombay Bombay
8 ALC(C) Bombay Bombay
9 ALC(C) Nagpur Nagpur
10 ALC(C) Vasco –Da‐Gama Vasco –Da‐Gama
11 RLC(C) Calcutta Calcutta
12 ALC(C) Calcutta Calcutta
13 RLC(C) Gauhati Gauhati
14 RLC(C) Dhanbad Dhanbad
15 ALC(C) Dhanbad Dhanbad
16 ALC(C) Chaibasa Chaibasa
17 ALC(C) Hazaribagh Hazaribagh
18 RLC(C) Hyderabad Hyderabad
19 ALC(C) Hyderabad Hyderabad
20 ALC(C) Vijaywada Vijaywada
21 ALC(C) Visahakhapatnam Visahakhapatnam
22 RLC(C) Jabalpur Jabalpur
23 ALC(C) Jabalpur Jabalpur
24 ALC(C) Raipur Raipur
25 ALC(C) Shahdol Shahdol
26 RLC(C) Kanpur Kanpur
27 ALC(C) Kanpur Kanpur
28 RLC(C) Chandigarh Chandigarh
Forms underCONTRACT LABOR (REGULATION AND ABOLITION) CENTRAL RULES, 1971
C o m p i l e d b y P o w e r H R F o r u m P a g e - C 3 4
29 RLC(C) Bhubaneswar Bhubaneswar
30 ALC(C) Bhubaneswar Bhubaneswar
31 RLC(C) Madras Madras
32 ALC(C) Madras Madras
33 ALC(C) Ernakulam Ernakulam
34 RLC(C) Bangalore Bangalore
35 ALC(C) Bellary Bellary
36 ALC(C) Dehradun Dehradun
37 ALC(C) Rohtak Rohtak
38 ALC(C) Jagdalpur Jagdalpur
39 ALC(C) Jaipur Jaipur
40 ALC(C) Kplar Gold Fields Kplar Gold Fields
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1
Forms under
INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION OF SERVICE) CENTRAL RULES, 1980

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2
INDEX FORM I Application for Registration of Establishments Employing Migrant
Workmen FORM II Certificate of Registration FORM III Register of Establishments FORM IV Application for Licence for Recruitment FORM V Application for Licence for Employment FORM VI Form of Certificate by Principal Employer FORM VII Form of Certificate by Principal Employer FORM VIII Application for Adjustment of Security Deposit FORM IX Application for Renewal of Licence FORM X Particulars in Respect of Recruitment and Employment of Migrant
Workman/Workmen FORM XI Return to be Sent by the Contractor to the Authorities Specified under
Explanation below Sub‐Section (2) of Section 12 FORM XII Register of Contractors FORM XIII Register of Workmen Employed by Contractor FORM XIV Service Certificate FORM XV Displacement and Outward Journey Allowance Sheet FORM XVI Return Journey Allowance Register FORM XVII Muster Roll FORM XVIII Register of Wages FORM XIX Register of Deduction for Damage or Loss FORM XX Register of Fines FORM XXI Register of Advances FORM XXII Register of Overtime FORM XXIII Return to be Sent by the Contractor to the Licensing Officer FORM XXIV
Annual Return of Principal Employer to be Sent to the Registering Officer

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 3
FORM I [See rule 3(1)]
Application for Registration of Establishments Employing Migrant Workmen
1. Name and location of the establishment.
2. Postal Address of the establishment.
3. Full name and address of the principal employer (furnish father’s/husband’s name in the case of individuals).
4. Names and addresses of the directors/particular partners (in case of companies and firms).
5. Full names and address of the Manager or person responsible for the supervision and control of the establishment.
6. Nature of work carried on in the establishment.
7. Particulars of contractors and migrant workmen.
a. Names and addresses of contractors.
b. Nature of work for which migrant workmen are to be recruited or are employed.
c. Maximum number of migrant workmen to be employed on any day through each contractor.
d. Estimated date and commencement of work under each contractor.
e. Estimated date of termination of employment of migrant workmen under each contractor.
8. Particulars of crossed demand draft ________ (Name of the Bank, Amount, Number and Date)
I hereby declare that the particulars given above are true to the best of my knowledge and belief.
Principal Employer
Seal and Stamp
Office of the Registering Officer
Date of receipt of application:

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 4
FORM II [See rule 4(1)]
Certificate of Registration Date ________________________
GOVERNMENT OF INDIA
Office of the Registering Officer
A certificate of registration containing the following particulars is hereby granted under clause (a) of sub‐section (2) of section 4 of the Inter‐State Migrant Workmen (Regulation of Employment and Conditions of Service) Act, 1979 and the rules made thereunder to......................
1. Nature of work carried on in the establishment.
2. Names and addresses of the contractors.
3. Nature of work for which migrant workmen are to be employed or are employed.
4. Maximum number of migrant workmen to be employed on any day through each contractor.
5. Other particulars relevant to the employment of migrant workmen.
(i)
(ii)
Signature of Registering
Officer with Seal
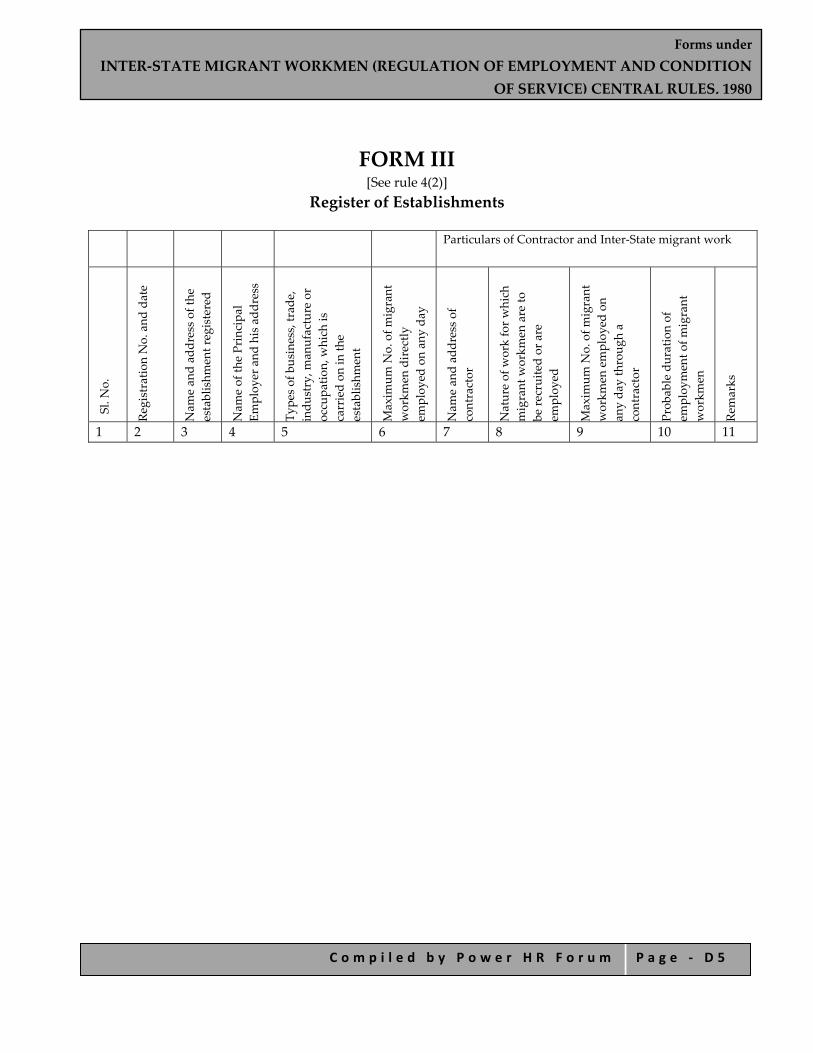
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 5
FORM III [See rule 4(2)]
Register of Establishments
Particulars of Contractor and Inter‐State migrant work
Sl. N
o.
Registratio
n No. and date
Nam
e an
d ad
dress of th
e establishm
ent registered
Nam
e of th
e Principa
l Em
ploy
er and his add
ress
Type
s of business, trad
e,
indu
stry, m
anufacture or
occupa
tion, w
hich is
carried on in th
e establishm
ent
Maxim
um N
o. of m
igrant
workm
en directly
employ
ed on an
y da
y
Nam
e an
d ad
dress of
contractor
Nature of w
ork for w
hich
migrant w
orkm
en are to
be re
cruited or are
employ
ed
Maxim
um N
o. of m
igrant
workm
en employ
ed on
any da
y throug
h a
contractor
Prob
able duration of
employ
ment o
f migrant
workm
en
Remarks
1 2 3 4 5 6 7 8 9 10 11

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 6
FORM IV [See rule 7(1)]
Application for Licence for Recruitment 1. Name and address of the contractor (including his father’s/ husband’s name in case of individuals.) 2. Date of birth and age (in case of individuals). 3. Particulars of establishment where migrant workmen are to be employed.
a. Name and address of the establishment;
b. Type of business, trade, industry manufacture or occupation, which is carried on in the establishment;
c. Number and date of certificate of registration of the establishment under the Act;
d. Name and address of the principal employer. 4. Particulars of migrant workmen:
a. Nature of work in which migrant workmen are employed or are to be employed in the establishment.
b. Duration of the proposed contract work (give particulars of proposed date of commencing and ending).
c. Name and address of the agent or manager of the contractor at the work‐site.
d. Maximum number of migrant workmen proposed to be employed in the establishment on any day.
e. Names and addresses of the directors/partners (in case of companies and firms).
f. Name(s) and address(es) of the person(s) in charge of and responsible to the company/firm, for the conduct of the business of the company/firm, as the case may be.
5. Whether the contractor was convicted of any offence within the preceding five years. If so, give details. 6. Whether there was any order against the contractor revoking or suspending licence or forfeiting
security deposits in respect of an earlier contract. If so, the date of such order. 7. Whether the contractor has worked in any other establishment within the past five years. If so, give
details of the principal employer, establishment, and nature of work. 8. Whether a certificate by the principal employer in Form VI is enclosed. 9. Amount of licence fee paid....................No. of crossed demand draft and date. 10. Amount of security deposit, if any.
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 7
DECLARATION I hereby declare that the details given above are correct to the best of my knowledge and belief.
Place............................ Date............................
Signature of the Applicant (Contractor)
Note.— The application should be accompanied by a crossed demand draft showing the payment of the prescribed licence fee and security deposit, if any and a certificate in Form V from the Principal Employer.
(To be filled in the office of the Licensing Officer)
Date of receipt of the application with crossed demand draft for fees. Signature of the Licensing Officer

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 8
FORM V [See rule 7(2)]
Application for Licence for Employment 1. Name and address of the contractor (including his father’s/ husband’s name in case of individuals.) 2. Date of birth and age (in case of individuals). 3. Particulars of establishment where migrant workmen are to be employed.
a. Name and address of the establishment;
b. Type of business, trade, industry manufacture or occupation, which is carried on in the establishment;
c. Number and date of certificate of registration of the establishment under the Act;
d. Name and address of the principal employer. 4. Particulars of migrant workmen:
a. Nature of work in which migrant workmen are employed or are to be employed in the establishment.
b. Duration of the proposed contract work (give particulars of proposed date of commencing and ending).
c. Name and address of the agent or manager of the contractor at the work‐site.
d. Maximum number of migrant workmen proposed to be employed in the establishment on any day.
e. Names and addresses of the directors/partners (in case of companies and firms).
f. Name(s) and address(es) of the person(s) in charge of and responsible to the company/firm, for the conduct of the business of the company/firm, as the case may be.
5. Whether the contractor was convicted of any offence within the preceding five years. If so, give details. 6. Whether there was any order against the contractor revoking or suspending licence or forfeiting
security deposits in respect of an earlier contract. If so, the date of such order.
7. Whether the contractor has worked in any other establishment within the past five years. If so, give details of the principal employer, establishment, and nature of work.
8. Whether a certificate by the principal employer in Form VI is enclosed.
9. Amount of licence fee paid......................No. of crossed demand draft and date.
10. Amount of security deposit, if any. DECLARATION
I hereby declare that the given are correct to the best of my knowledge and belief. Place......................... Date......................... Signature of the Applicant

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 9
(Contractor) Note.—The application should be accompanied by a crossed demand draft showing the payment of the
prescribed fee and security deposit, if any, and a certificate in Form VI from the principal employer. (To be filled in the office of the Licensing Officer)
Date of receipt of the application with crossed demand draft for fees.
Signature of the Licensing Officer
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 0
FORM VI [See rule 7(3)]
Form of Certificate by Principal Employer Certified that I have engaged the applicant (Name of the contractor) as a contractor in my establishment. I undertake to be bound all the provisions of the Inter‐State Migrant Workman (Regulation of Employment and Conditions of Service) Act, 1979 and the Inter‐State Migrant Workmen (Regulation of Employment and Conditions of Service) Central Rules, 1980 in so far as the provisions are applicable to me in respect of the employment of migrant workmen by the applicant in my establishment.
Place........................... Signature of Principal Employer Date............................. Name and address of establishment

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 1
FORM VII [See rule 10(3)]
Application for Adjustment of Security Deposit
Nam
e an
d ad
dress of th
e Con
tractor
Num
ber a
nd date of app
lication for fresh licence.
Date of exp
iry of previou
s licence
Whether th
e previous licence of th
e contractor
was suspe
nded or revok
ed.
Num
ber a
nd date of th
e crossed de
man
d draft
of security dep
osit in re
spect o
f the previou
s licence.
Amou
nt of p
reviou
s security dep
osit.
Amou
nt of security dep
osit for fresh licence
Num
ber a
nd date of crossed dem
and draft o
f the balance security dep
osit de
posited with
the fresh ap
plication
Num
ber a
nd date of certificate of re
gistratio
n of th
e establishm
ent in relatio
n to w
hich th
e fresh licence is app
lied
Nam
e an
d ad
dress of th
e principa
l employ
er
Particulars of fresh ap
plication
Remarks
1 2 3 4 5 6 7 8 9 10 11 12
Place................... Signature of applicant Date.....................

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 2
FORM VIII [See rule 11(1)]
GOVERNMENT OF INDIA
Office of Licensing Officer
Licence No. Dated Fee paid Rs.
Licence Licence is hereby granted to ............. under section 8(1) of the Inter‐State Migrant Workmen (Regulation of Employment and Conditions of Service) Act, 1979 subject to the conditions specified in the annexure.
2. This licence is for doing the work of (nature of work to be indicated) in the establishment of (name of principal employer to be indicated) at (place of work to be indicated).
3. The licence shall remain in force till (date to be indicated).
Signature and Seal of Licensing Officer.
RENEWAL
[See rule 14)
Date of renewal Fee paid for renewal
Date of expiry.
1
2
3
Date..........................
Signature and Seal of Licensing Officer
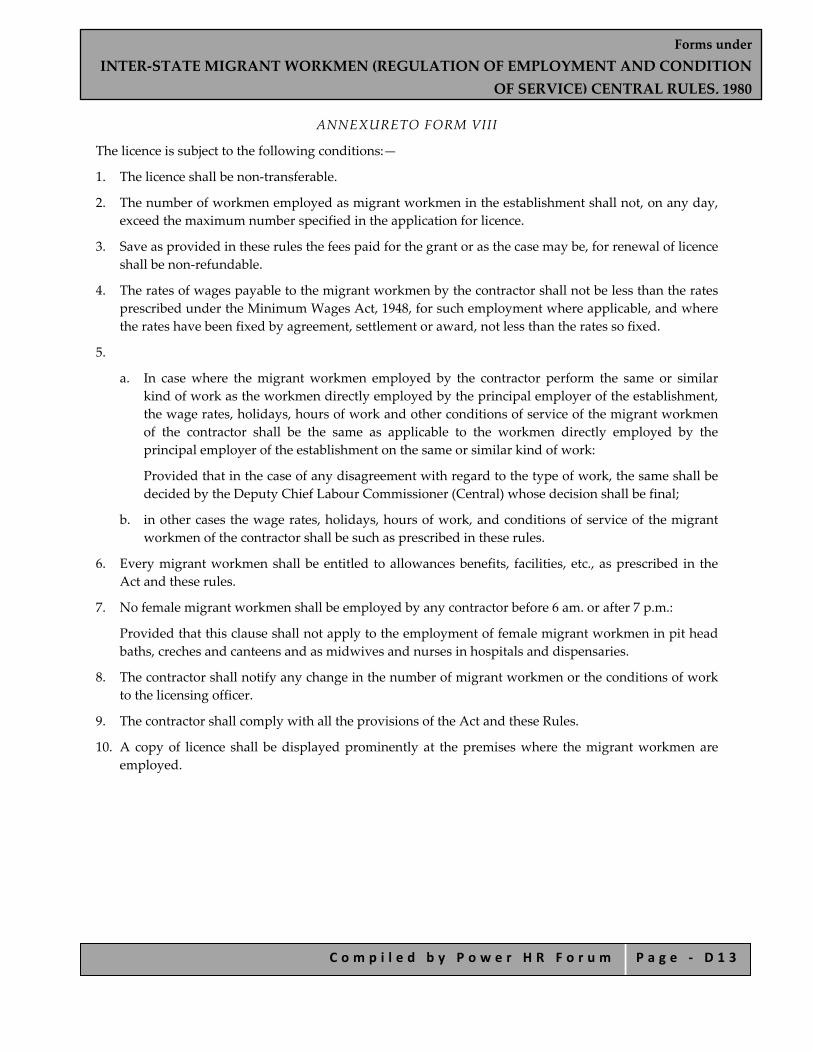
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 3
ANNEXURETO FORM VIII
The licence is subject to the following conditions:—
1. The licence shall be non‐transferable.
2. The number of workmen employed as migrant workmen in the establishment shall not, on any day, exceed the maximum number specified in the application for licence.
3. Save as provided in these rules the fees paid for the grant or as the case may be, for renewal of licence shall be non‐refundable.
4. The rates of wages payable to the migrant workmen by the contractor shall not be less than the rates prescribed under the Minimum Wages Act, 1948, for such employment where applicable, and where the rates have been fixed by agreement, settlement or award, not less than the rates so fixed.
5.
a. In case where the migrant workmen employed by the contractor perform the same or similar kind of work as the workmen directly employed by the principal employer of the establishment, the wage rates, holidays, hours of work and other conditions of service of the migrant workmen of the contractor shall be the same as applicable to the workmen directly employed by the principal employer of the establishment on the same or similar kind of work:
Provided that in the case of any disagreement with regard to the type of work, the same shall be decided by the Deputy Chief Labour Commissioner (Central) whose decision shall be final;
b. in other cases the wage rates, holidays, hours of work, and conditions of service of the migrant workmen of the contractor shall be such as prescribed in these rules.
6. Every migrant workmen shall be entitled to allowances benefits, facilities, etc., as prescribed in the Act and these rules.
7. No female migrant workmen shall be employed by any contractor before 6 am. or after 7 p.m.:
Provided that this clause shall not apply to the employment of female migrant workmen in pit head baths, creches and canteens and as midwives and nurses in hospitals and dispensaries.
8. The contractor shall notify any change in the number of migrant workmen or the conditions of work to the licensing officer.
9. The contractor shall comply with all the provisions of the Act and these Rules.
10. A copy of licence shall be displayed prominently at the premises where the migrant workmen are employed.
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 4
FORM IX [See rule 15(2)]
Application for Renewal of Licence 1. Name and address of the contractor. 2. Number and date of the licence. 3. Date of expiry of the previous licence. 4. Whether the licence of the Contractor was suspended or revoked. 5. Number and date of the crossed demand draft enclosed.
Place......................... Signature of the Applicant Date........................
(To be filled in the Office of the Licensing Officer) Date of receipt of the application with crossed demand draft No. and date.
Signature of the Licensing Officer

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 5
FORM X (See rule 21)
Form in which to furnish particulars in respect of recruitment and employment of migrant workman/workmen as prescribed under sub‐rule (1) of rule 21, to the authorities specified under the Explanation below sub‐section (2) of section 12 of Inter‐State Migrant Workmen (Regulation of
Employment and Conditions of Service) Act, 1979
1. Name and address of the Contractor……………………………………………………………………. 2. Name and address of the sub‐contractor through whom recruitment has been made…………….. 3. Name and address of the establishment…………………………………………………………………. 4. Name and address of the Principal Employer…………………………………………………………… 5. Name of the State in which the place of work is located……………………………………………….. 6. Name of the State in which recruitment was made………………………………………………………
Serial num
ber
Nam
e of m
igrant
workm
an.
Father’s/H
usband
’s
Nam
e Sex.
Age
Perm
anent h
ome
address.
Nam
e an
d ad
dress of
the next of k
in
of th
e migrant
workm
an.
Place an
d ad
dress of
reside
nce in th
e ho
me State.
Amou
nt of d
isplacem
ent
allowan
ce
paid.
1 2 3 4 5 6 7 8 9
Amou
nt of o
utward
journey
allowan
ce paid.
Amou
nt of w
ages fo
r ou
tward
journey pe
riod paid.
Nature of job requ
ired to
be
performed
. Date of re
cruitm
ent
Date of employ
ment
Details of rates of w
ages
and other a
llowan
ces
payable
Period of con
tract o
f em
ploy
ment
Details of o
ther service
cond
ition
s Remarks
10 11 12 13 14 15 16 17 18
Signature of Contractor or his authorised representative

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 6
Date..........................
Submitted to 1. ........................................... .......................................... (Specified authority in the State from which the migrant workman/workmen is/are employed). 2. ........................................... .......................................... (Specified authority in the State in which migrant workman/workmen has/have been recruited.) Copy forwarded to .......................................... (The Principal Employer)
Signature of the Contractor or his authorised representative.
Date.......................... Note.—In case where migrant workmen concerned have been recruited from more than one State, separate returns shall be submitted in respect of each such State.
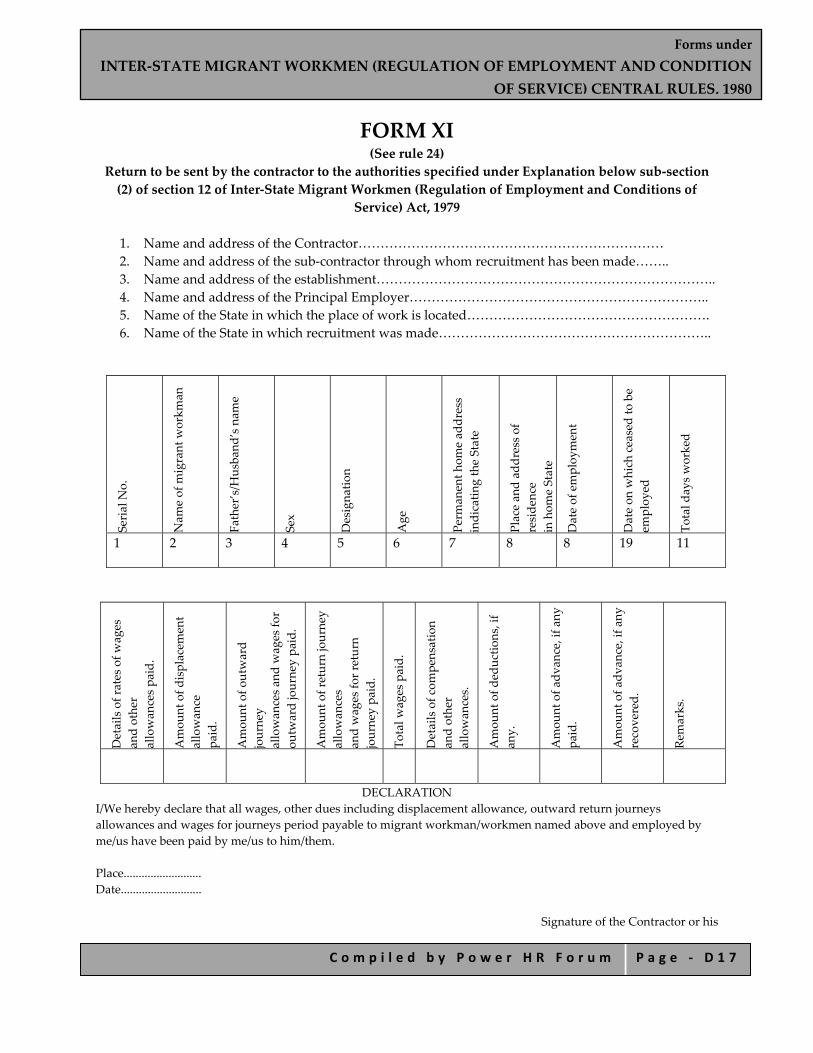
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 7
FORM XI (See rule 24)
Return to be sent by the contractor to the authorities specified under Explanation below sub‐section (2) of section 12 of Inter‐State Migrant Workmen (Regulation of Employment and Conditions of
Service) Act, 1979
1. Name and address of the Contractor…………………………………………………………… 2. Name and address of the sub‐contractor through whom recruitment has been made…….. 3. Name and address of the establishment………………………………………………………………….. 4. Name and address of the Principal Employer………………………………………………………….. 5. Name of the State in which the place of work is located………………………………………………. 6. Name of the State in which recruitment was made……………………………………………………..
Serial N
o.
Nam
e of m
igrant w
orkm
an
Father’s/H
usband
’s nam
e Sex Designa
tion
Age
Perm
anent h
ome ad
dress
indicatin
g the State
Place an
d ad
dress of
reside
nce
in hom
e State
Date of employ
ment
Date on w
hich ceased to be
employ
ed
Total d
ays worked
1 2 3 4 5 6 7 8 8 19 11
Details of rates of w
ages
and other
allowan
ces pa
id.
Amou
nt of d
isplacem
ent
allowan
ce
paid.
Amou
nt of o
utward
journey
allowan
ces an
d wages fo
r ou
tward journey pa
id.
Amou
nt of return journey
allowan
ces
and wages fo
r return
journey pa
id.
Total w
ages paid.
Details of com
pensation
and other
allowan
ces.
Amou
nt of d
eductio
ns, if
any.
Amou
nt of a
dvan
ce, if a
ny
paid.
Amou
nt of a
dvan
ce, if a
ny
recovered.
Remarks.
DECLARATION I/We hereby declare that all wages, other dues including displacement allowance, outward return journeys allowances and wages for journeys period payable to migrant workman/workmen named above and employed by me/us have been paid by me/us to him/them. Place.......................... Date...........................
Signature of the Contractor or his

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 8
authorised representative Submitted to (1) ................................ ................................. (Specified authority in the State in which migrant workman/workmen is/are employed). (2) ................................ ................................ (Specified authority in the State in which migrant workman/workmen has/have been recruited.) Copy forwarded to
........................................ (The Principal Employer)
Signature of the Contractor or his
authorised representative. Date.................... Note.—In case where migrant workmen concerned have been recruited from more than one State, separate returns shall be submitted in respect of each such State.
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 1 9
FORM XII [See Rule 48]
Register of Contractors
1. Name and Address of the principal employer
2. Name and address of the establishment
Name and address of the contractor
Nature of work on contract
Location of contract work
Period of contract`
Maximum number of migrant workmen employed by contractor
From To

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 0
FORM XIII [See Rule 49]
Register of Workmen Employed by Contractor Name and address of contractor …………………………….
Name and address of establishment in/under which migrant workmen are employed……………………………
Name and address of establishment ………………………..
Name and address of Principal Employer………………………………………..
Sl No. Name
and surname of migrant workman
Age and sex
Father’s /Husband’s name
Nature of employment/ designation
Permanent home adderss of migrant workmen, village and Tehsil/Taluk and district
Local address
Date of commencement of employement
1 2 3 4 5 6 7 8
Signature and thumb impression of migrant workmen
Date of termination of employment
Reasons for termination Remarks
9 10 11 12
Signature of contractor or his authorized representative

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 1
FORM XIV (See rule 50)
Service Certificate Name and address of Contractor………..
Name and address of establishment in/under which migrant workmen are
employed………………………
Nature and location of work………… Name and address of Principal Employer………………..
Name and address of the migrant workman……..
Age or date of birth…………………
Identification marks…………………..
Father’s/Husband’s name………………..
Serial No.
Total period for which employed Nature of work done
Rate of wages (with particulars of unit in case of piece work)
Remarks
From To
1 2 3 4 5 6
Signature of the Contractor or his authorised representative.
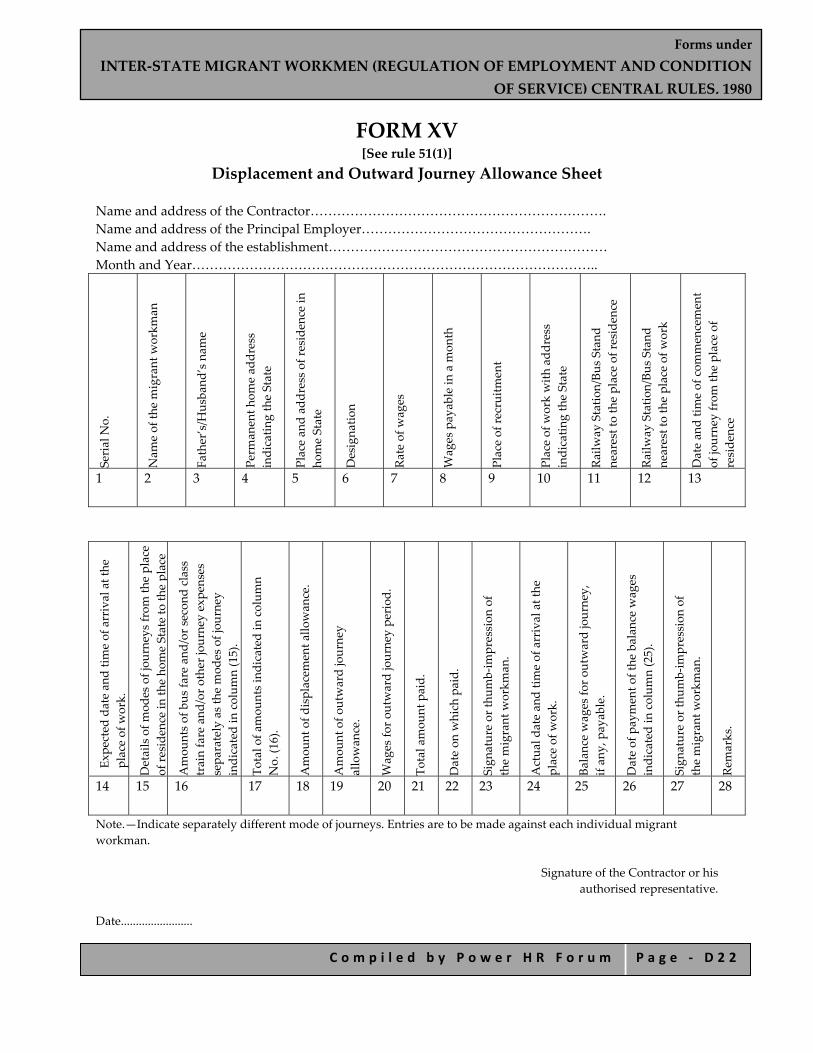
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 2
FORM XV [See rule 51(1)]
Displacement and Outward Journey Allowance Sheet
Name and address of the Contractor…………………………………………………………. Name and address of the Principal Employer……………………………………………. Name and address of the establishment……………………………………………………… Month and Year………………………………………………………………………………..
Serial N
o.
Nam
e of th
e migrant w
orkm
an
Father’s/H
usband
’s nam
e Perm
anent h
ome ad
dress
indicatin
g the State
Place an
d ad
dress of re
side
nce in
home State
Designa
tion
Rate of w
ages
Wages payable in a m
onth
Place of re
cruitm
ent
Place of w
ork with add
ress
indicatin
g the State
Railw
ay Statio
n/Bu
s Stan
d nearest to the place of re
side
nce
Railw
ay Statio
n/Bu
s Stan
d nearest to the place of w
ork
Date an
d tim
e of com
mencement
of journey from th
e place of
reside
nce
1 2 3 4 5 6 7 8 9 10 11 12 13
Expe
cted date an
d tim
e of arrival at the
place of w
ork.
Details of m
odes of jou
rneys from th
e place
of re
side
nce in th
e ho
me State to th
e place
Amou
nts of bus fa
re and
/or secon
d class
train fare and
/or o
ther journey expe
nses
sepa
rately as the mod
es of jou
rney
indicated in colum
n (15).
Total o
f amou
nts indicated in colum
n No. (1
6).
Amou
nt of d
isplacem
ent a
llowan
ce.
Amou
nt of o
utward journey
allowan
ce.
Wages fo
r outward journey pe
riod
.
Total amou
nt paid.
Date on w
hich paid.
Sign
ature or th
umb‐im
pression of
the migrant w
orkm
an.
Actua
l date an
d tim
e of arrival at the
place of w
ork.
Balance wages fo
r outward journey,
if an
y, payable.
Date of payment o
f the balan
ce w
ages
indicated in colum
n (25).
Sign
ature or th
umb‐im
pression of
the migrant w
orkm
an.
Remarks.
14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
Note.—Indicate separately different mode of journeys. Entries are to be made against each individual migrant workman.
Signature of the Contractor or his authorised representative.
Date........................

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 3
FORM XVI [See rule 51(1)]
Return Journey Allowance Register Name and address of the Contractor……………………………………… Name and address of the Principal Employer…………………………….. Name and address of the establishment……………………………………. Month and Year…………………………………………………………………
Serial N
o.
Nam
e of th
e migrant
workm
an
Father’s/H
usband
’s nam
e Perm
anent h
ome ad
dress
indicatin
g the State
Place an
d ad
dress of
reside
nce in hom
e State
Designa
tion
Rate of w
ages
Place of w
ork
Railw
ay Statio
n/Bu
s Stan
d nearest to the place of w
ork
Railw
ay Statio
n/Bu
s Stan
d nearest to the place of
reside
nce in th
e ho
me State
Date an
d tim
e of
commencement o
f jou
rney
from th
e place of w
ork
1 2 3 4 5 6 7 8 9 10 11
Expe
cted date an
d tim
e of arrival
at th
e reside
nce in th
e ho
me State
*Exp
ected of m
odes of jou
rneys
from th
e place of w
ork to place of
reside
nce in th
e ho
me State.
Amou
nt of b
us fa
re and
/or
second class train fare and
/or
other jou
rney exp
enses sepa
rately
as per exp
ected mod
es of jou
rney
indicated in colum
n (13)
Total o
f amou
nts indicated in
column No. (1
4)
Amou
nt of return journey
allowan
ce
Wages fo
r return journey pe
riod
Total amou
nt paid
Date on w
hich paid
Sign
ature or th
umb‐im
pression
of th
e migrant w
orkm
an
Remarks
12 13 14 15 16 17 18 19 20 21
* Indicate separately different modes of journey. Note.—Entries are to be made against each individual inter‐State migrant workman.
Signature of the Contractor or his authorised representative.
Date........................
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 4
FORM XVII [See rule 52(2)(a)] Muster Roll
Name and address of Contractor……………………………………………………………… Nature and location of work……………………………………………………………………. Name and address of establishment in/under which inter‐State migrant workmen are employed……………………............................................... Name and address of Principal Employer…………………………………………………. For the month of ............................................................................................................................
Serial Number Name of migrant workmen
Father’s / Husband’s Name
Sex Date Remarks
1 2 3 4 5
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 5
FORM XVIII [See rule 52(2)(a)]
Register of Wages
Name and address of Contractor……………………………………………………………. Nature and location of work……………………………………………………………….. Name and address of establishment in/under which inter‐State Migrant Workmen are employed……………………………………………….. Name and address of Principal Employer…………………………………….. Wage period………………………………………………………..
Serial N
o.
Nam
e of in
ter‐State migrant
workm
an
Serial N
o. in th
e register of
workm
en
Designa
tion/na
ture of w
ork
Num
ber o
f days worked
Units of w
ork do
ne
Daily ra
te of w
ages/ p
iecerate
Amount of wages earned
Total.
Ded
uctio
ns, if a
ny (ind
icate
nature)
Net amou
nt paid
S i g n a t u r e / T h u m b ‐
impression of Inter‐State
Migrant W
orkm
an
Initials of Con
tractor o
r his
authorised re
presentativ
e
Basic wages
Dearness allowan
ce
Overtim
e
Other cash pa
yments
(nature of payment to be
indicated)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
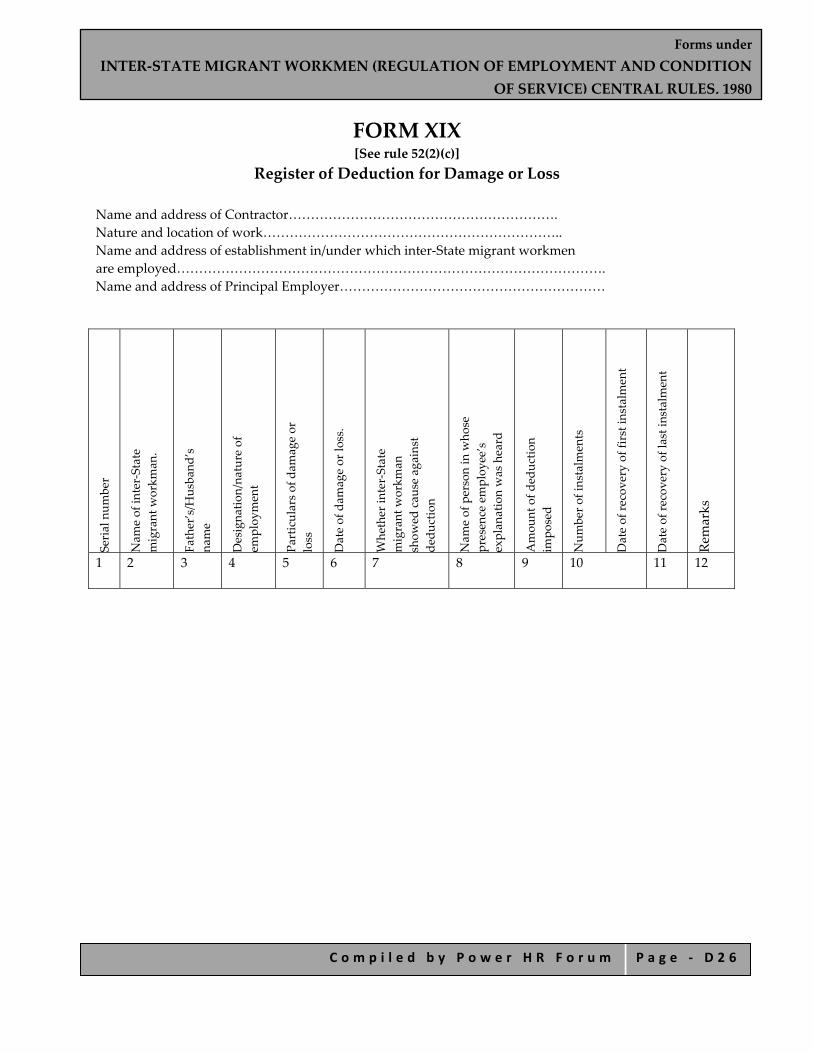
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 6
FORM XIX [See rule 52(2)(c)]
Register of Deduction for Damage or Loss
Name and address of Contractor……………………………………………………. Nature and location of work………………………………………………………….. Name and address of establishment in/under which inter‐State migrant workmen are employed……………………………………………………………………………………. Name and address of Principal Employer……………………………………………………
Serial num
ber
Nam
e of in
ter‐State
migrant w
orkm
an.
Father’s/H
usband
’s
name
Designa
tion/na
ture of
employ
ment
Particulars of dam
age or
loss
Date of dam
age or lo
ss.
Whether in
ter‐State
migrant w
orkm
an
show
ed cau
se against
dedu
ction
Nam
e of person in w
hose
presence employ
ee’s
explan
ation was heard
Amou
nt of d
eductio
n im
posed
Num
ber o
f instalm
ents
Date of re
covery of first in
stalment
Date of re
covery of last instalm
ent
Remarks
1 2 3 4 5 6 7 8 9 10 11 12

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 7
FORM XX [See rule 52(2)(c)] Register of Fines
Name and address of Contractor………………………………………………………………… Nature and location of work……………………………………………… Name and address of establishment in/under which inter‐State migrant workmen are employed…………………………………………………………………………. Name and address of Principal Employer……………………………………….
Serial num
ber
Nam
e of in
ter‐State migrant
workm
an
Father’s/H
usband
’s nam
e Designa
tion/na
ture of
employ
ment
Act/O
mission fo
r which
fine im
posed
Date of offe
nce
Whether in
ter‐State
Migrant W
orkm
an sho
wed
cause against fine
Nam
e of person in w
hose
presence employ
ee’s
explan
ation was heard
Wages periods and w
ages
payable
Amou
nt of fine im
posed
Date on w
hich fine re
alised
Remarks
1 2 3 4 5 6 7 8 9 10 11 12

Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 8
FORM XXI [See rule 52(2)(c)]
Register of Advances
Name and address of Contractor………………………………………………………………. Nature and location of work…………………………………………………………………… Name and address of establishment in/under which inter‐State migrant workmen are employed…………………………………………………………………………………… Name and address of Principal Employer………………………………………………………
Serial num
ber
Nam
e of In
ter‐State
Migrant
Workm
an
Father’s/H
usband
’s nam
e Nature of Employ
ment/
Designa
tion
Wage pe
riod and w
ages
payable
Date an
d am
ount of
advance given
Purpose(s) fo
r which
advance mad
e Num
ber o
f instalm
ents by
which adv
ance to be
repa
id
Date an
d am
ount of each
instalment rep
aid
Date on w
hich last
instalment
was re
paid
Remarks
1 2 3 4 5 6 7 8 9 10 11
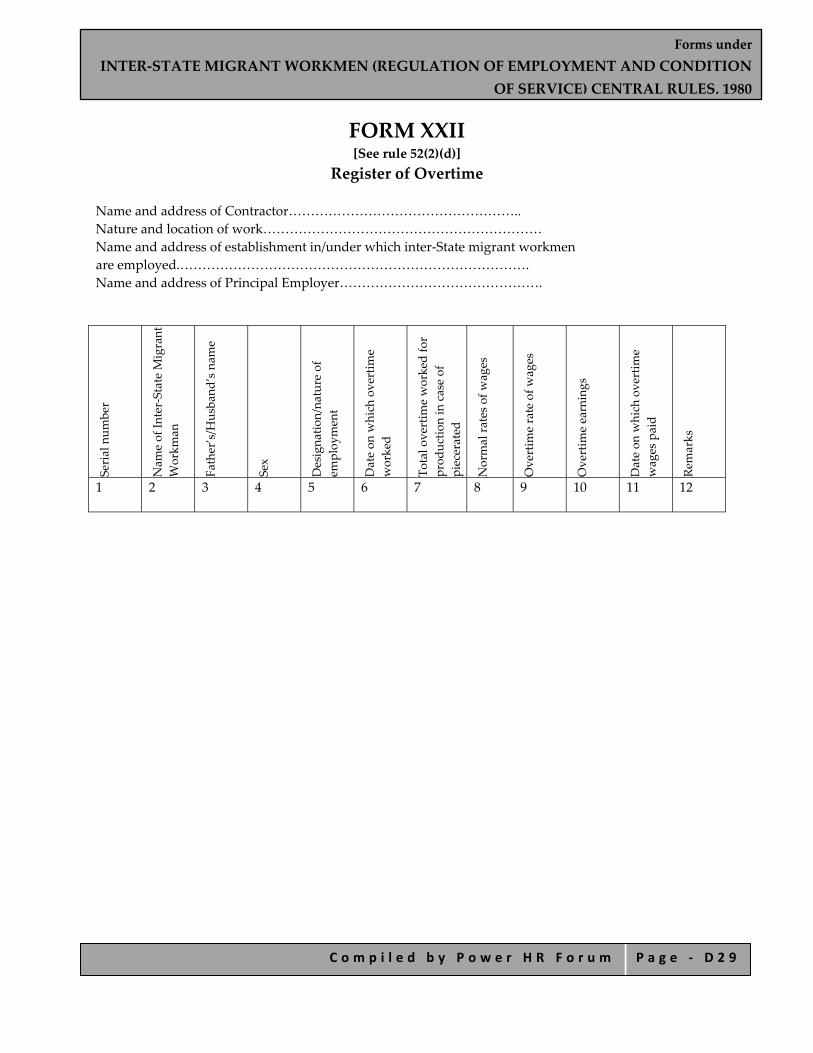
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 2 9
FORM XXII [See rule 52(2)(d)]
Register of Overtime
Name and address of Contractor…………………………………………….. Nature and location of work……………………………………………………… Name and address of establishment in/under which inter‐State migrant workmen are employed.……………………………………………………………………. Name and address of Principal Employer……………………………………….
Serial num
ber
Nam
e of In
ter‐State Migrant
Workm
an
Father’s/H
usband
’s nam
e Sex Designa
tion/na
ture of
employ
ment
Date on w
hich overtim
e worked
Total o
vertim
e worked for
prod
uctio
n in case of
piecerated
Normal ra
tes of w
ages
Overtim
e rate of w
ages
Overtim
e earnings
Date on w
hich overtim
e wages paid
Remarks
1 2 3 4 5 6 7 8 9 10 11 12
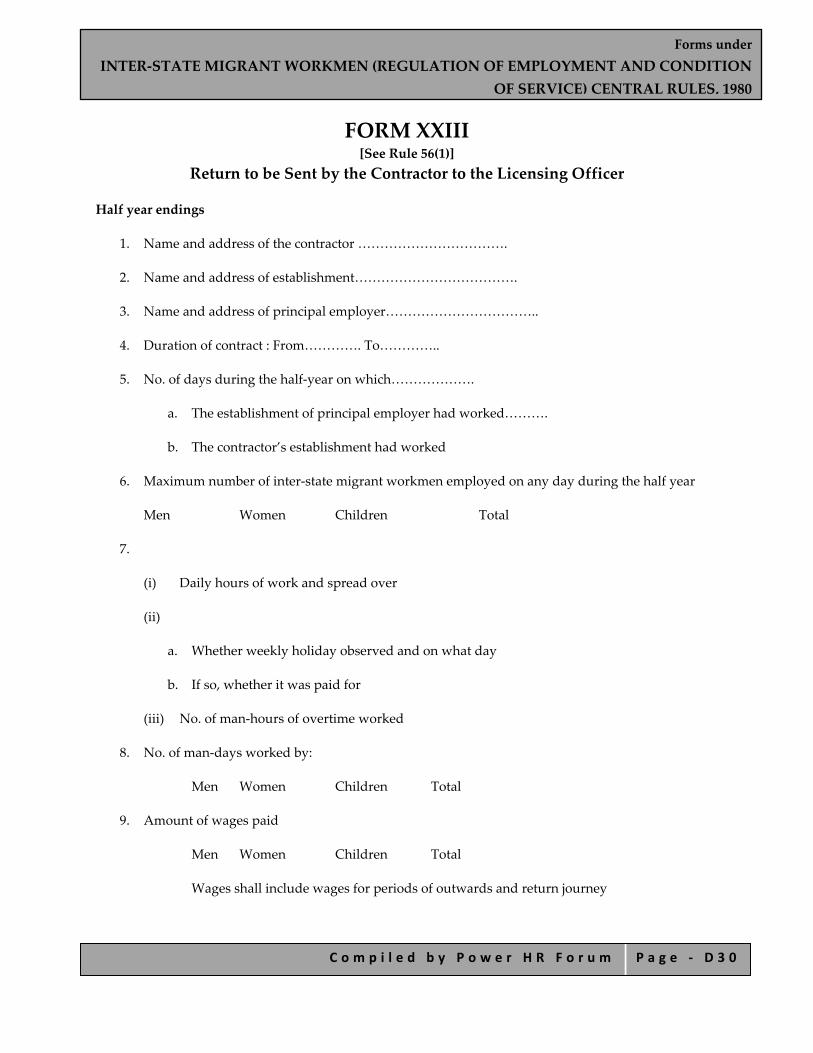
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 3 0
FORM XXIII [See Rule 56(1)]
Return to be Sent by the Contractor to the Licensing Officer
Half year endings
1. Name and address of the contractor …………………………….
2. Name and address of establishment……………………………….
3. Name and address of principal employer……………………………..
4. Duration of contract : From…………. To…………..
5. No. of days during the half‐year on which……………….
a. The establishment of principal employer had worked……….
b. The contractor’s establishment had worked
6. Maximum number of inter‐state migrant workmen employed on any day during the half year
Men Women Children Total
7.
(i) Daily hours of work and spread over
(ii)
a. Whether weekly holiday observed and on what day
b. If so, whether it was paid for
(iii) No. of man‐hours of overtime worked
8. No. of man‐days worked by:
Men Women Children Total
9. Amount of wages paid
Men Women Children Total
Wages shall include wages for periods of outwards and return journey
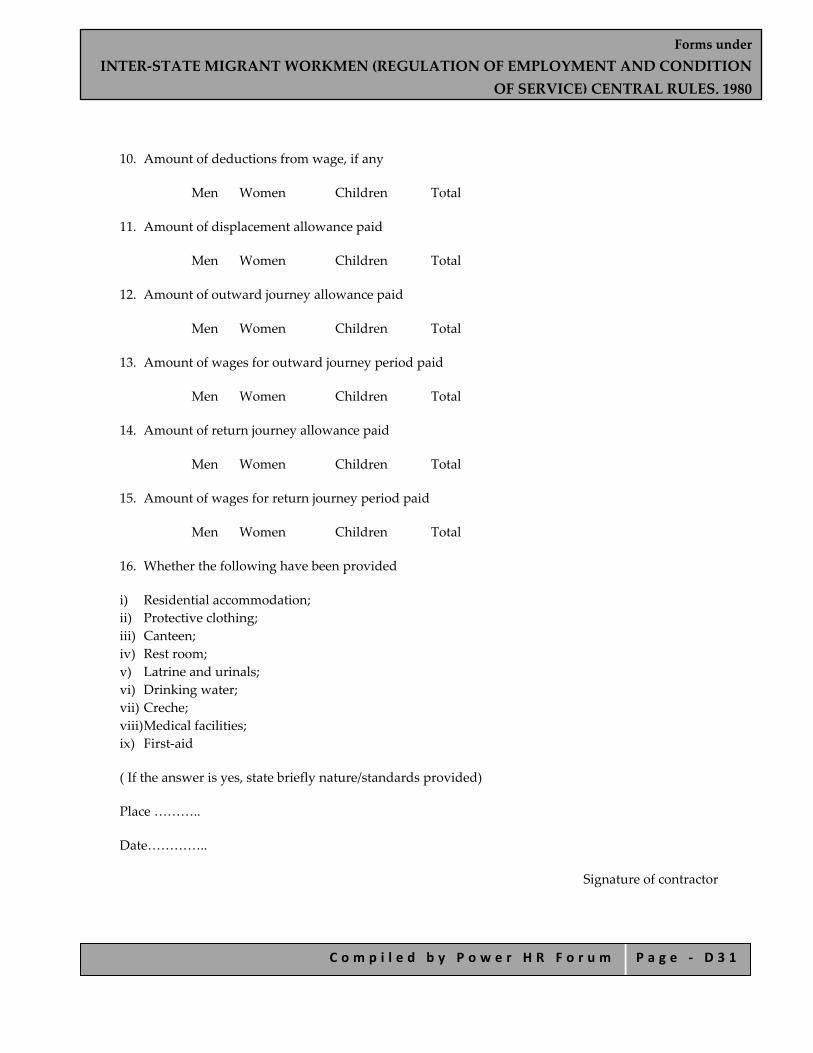
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 3 1
10. Amount of deductions from wage, if any
Men Women Children Total
11. Amount of displacement allowance paid
Men Women Children Total
12. Amount of outward journey allowance paid
Men Women Children Total
13. Amount of wages for outward journey period paid
Men Women Children Total
14. Amount of return journey allowance paid
Men Women Children Total
15. Amount of wages for return journey period paid
Men Women Children Total
16. Whether the following have been provided
i) Residential accommodation; ii) Protective clothing; iii) Canteen; iv) Rest room; v) Latrine and urinals; vi) Drinking water; vii) Creche; viii) Medical facilities; ix) First‐aid
( If the answer is yes, state briefly nature/standards provided)
Place ………..
Date…………..
Signature of contractor
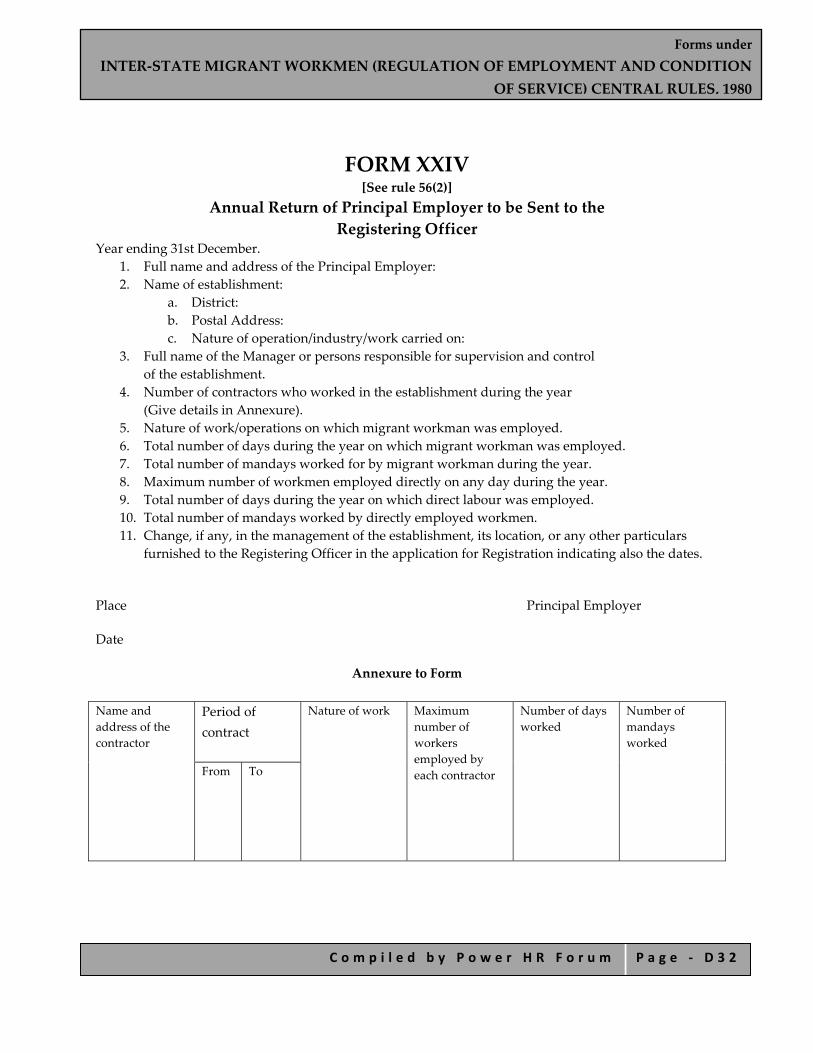
Forms under INTER‐STATE MIGRANT WORKMEN (REGULATION OF EMPLOYMENT AND CONDITION
OF SERVICE) CENTRAL RULES, 1980
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ D 3 2
FORM XXIV [See rule 56(2)]
Annual Return of Principal Employer to be Sent to the Registering Officer
Year ending 31st December. 1. Full name and address of the Principal Employer: 2. Name of establishment:
a. District: b. Postal Address: c. Nature of operation/industry/work carried on:
3. Full name of the Manager or persons responsible for supervision and control of the establishment.
4. Number of contractors who worked in the establishment during the year (Give details in Annexure).
5. Nature of work/operations on which migrant workman was employed. 6. Total number of days during the year on which migrant workman was employed. 7. Total number of mandays worked for by migrant workman during the year. 8. Maximum number of workmen employed directly on any day during the year. 9. Total number of days during the year on which direct labour was employed. 10. Total number of mandays worked by directly employed workmen. 11. Change, if any, in the management of the establishment, its location, or any other particulars
furnished to the Registering Officer in the application for Registration indicating also the dates.
Place Principal Employer
Date
Annexure to Form
Name and address of the contractor
Period of contract
Nature of work
Maximum number of workers employed by each contractor
Number of days worked
Number of mandays worked
From
To

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1
Forms under
MINES RULES, 1955
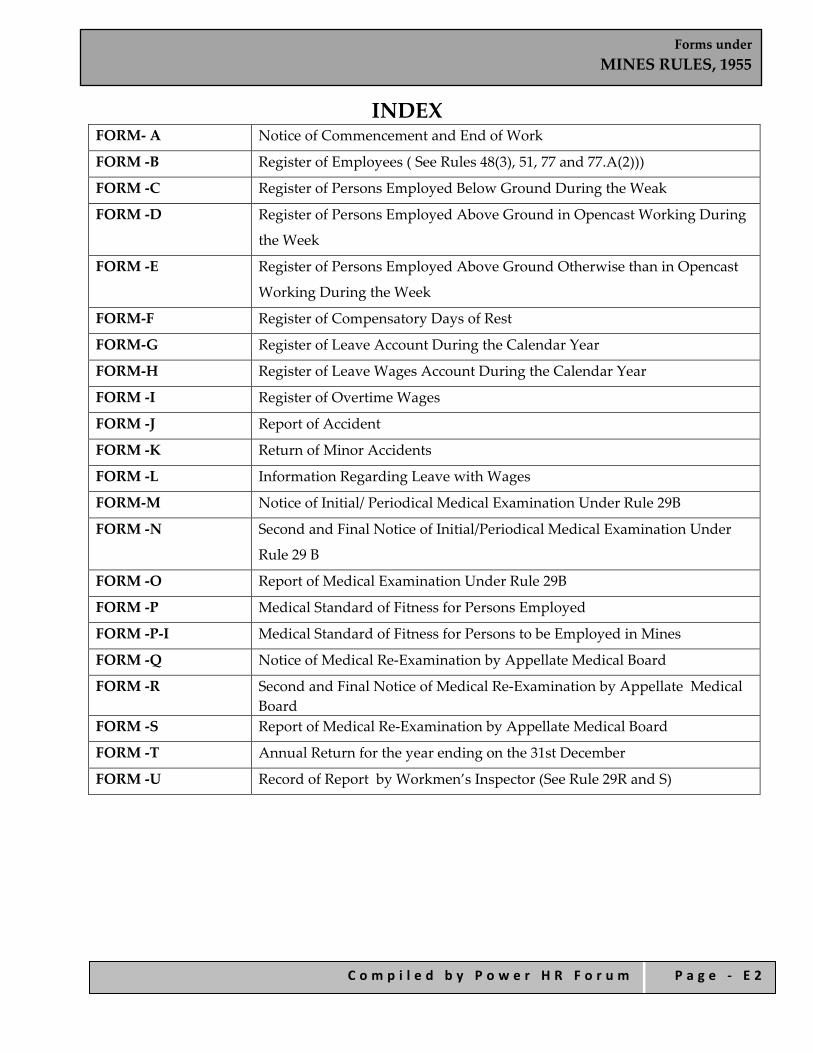
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2
INDEX FORM‐ A Notice of Commencement and End of Work
FORM ‐B Register of Employees ( See Rules 48(3), 51, 77 and 77.A(2)))
FORM ‐C Register of Persons Employed Below Ground During the Weak
FORM ‐D Register of Persons Employed Above Ground in Opencast Working During
the Week
FORM ‐E Register of Persons Employed Above Ground Otherwise than in Opencast
Working During the Week
FORM‐F Register of Compensatory Days of Rest
FORM‐G Register of Leave Account During the Calendar Year
FORM‐H Register of Leave Wages Account During the Calendar Year
FORM ‐I Register of Overtime Wages
FORM ‐J Report of Accident
FORM ‐K Return of Minor Accidents
FORM ‐L Information Regarding Leave with Wages
FORM‐M Notice of Initial/ Periodical Medical Examination Under Rule 29B
FORM ‐N Second and Final Notice of Initial/Periodical Medical Examination Under
Rule 29 B
FORM ‐O Report of Medical Examination Under Rule 29B
FORM ‐P Medical Standard of Fitness for Persons Employed
FORM ‐P‐I Medical Standard of Fitness for Persons to be Employed in Mines
FORM ‐Q Notice of Medical Re‐Examination by Appellate Medical Board
FORM ‐R Second and Final Notice of Medical Re‐Examination by Appellate Medical Board
FORM ‐S Report of Medical Re‐Examination by Appellate Medical Board
FORM ‐T Annual Return for the year ending on the 31st December
FORM ‐U Record of Report by Workmen’s Inspector (See Rule 29R and S)
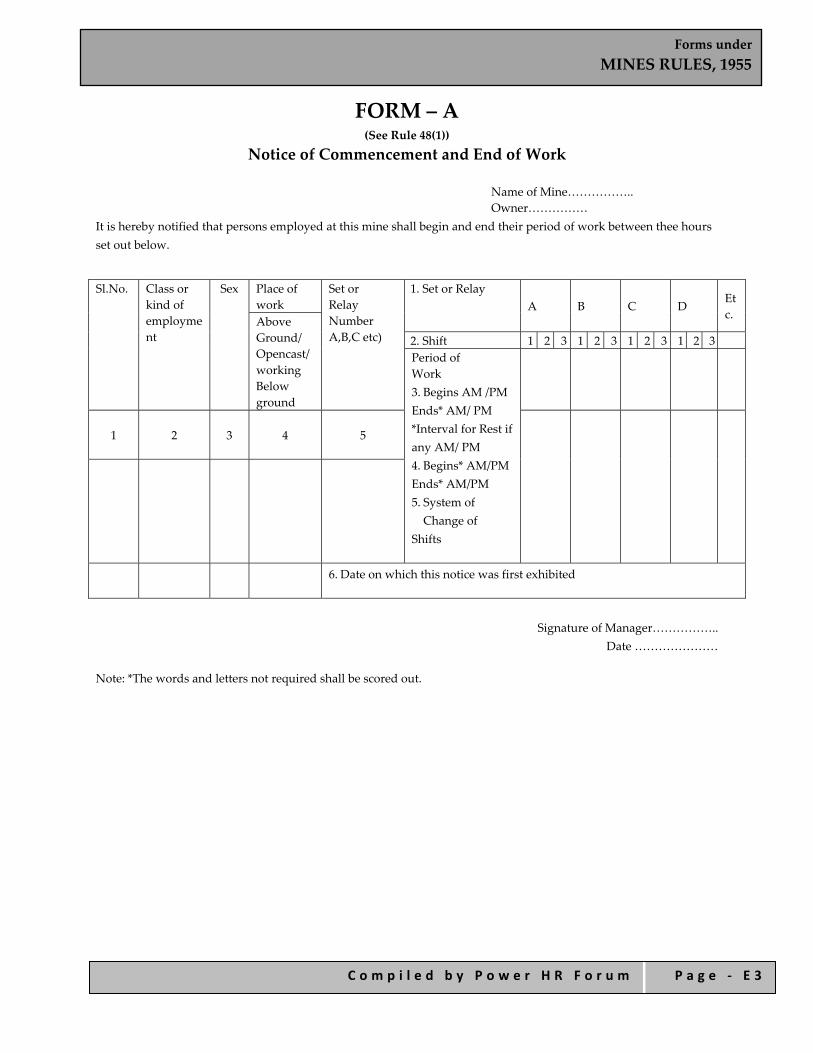
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 3
FORM – A (See Rule 48(1))
Notice of Commencement and End of Work
Name of Mine…………….. Owner……………
It is hereby notified that persons employed at this mine shall begin and end their period of work between thee hours set out below.
Sl.No. Class or kind of employment
Sex Place of work
Set or Relay Number A,B,C etc)
1. Set or Relay A B C D
Etc. Above
Ground/ Opencast/ working Below ground
2. Shift 1 2 3 1 2 3 1 2 3 1 2 3 Period of Work 3. Begins AM /PM Ends* AM/ PM *Interval for Rest if any AM/ PM 4. Begins* AM/PM Ends* AM/PM 5. System of Change of
Shifts
1 2 3 4
5
6. Date on which this notice was first exhibited
Signature of Manager……………..
Date ………………… Note: *The words and letters not required shall be scored out.
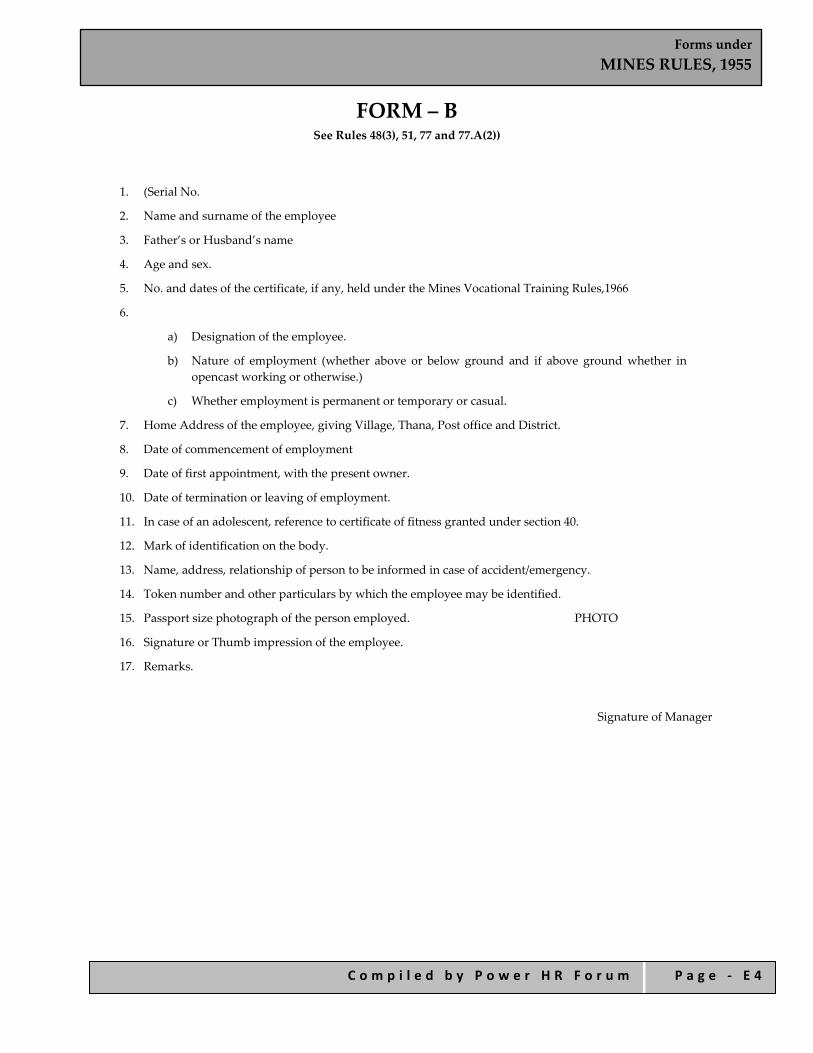
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 4
FORM – B See Rules 48(3), 51, 77 and 77.A(2))
1. (Serial No.
2. Name and surname of the employee
3. Father’s or Husband’s name
4. Age and sex.
5. No. and dates of the certificate, if any, held under the Mines Vocational Training Rules,1966
6.
a) Designation of the employee.
b) Nature of employment (whether above or below ground and if above ground whether in opencast working or otherwise.)
c) Whether employment is permanent or temporary or casual.
7. Home Address of the employee, giving Village, Thana, Post office and District.
8. Date of commencement of employment
9. Date of first appointment, with the present owner.
10. Date of termination or leaving of employment.
11. In case of an adolescent, reference to certificate of fitness granted under section 40.
12. Mark of identification on the body.
13. Name, address, relationship of person to be informed in case of accident/emergency.
14. Token number and other particulars by which the employee may be identified.
15. Passport size photograph of the person employed. PHOTO
16. Signature or Thumb impression of the employee.
17. Remarks.
Signature of Manager
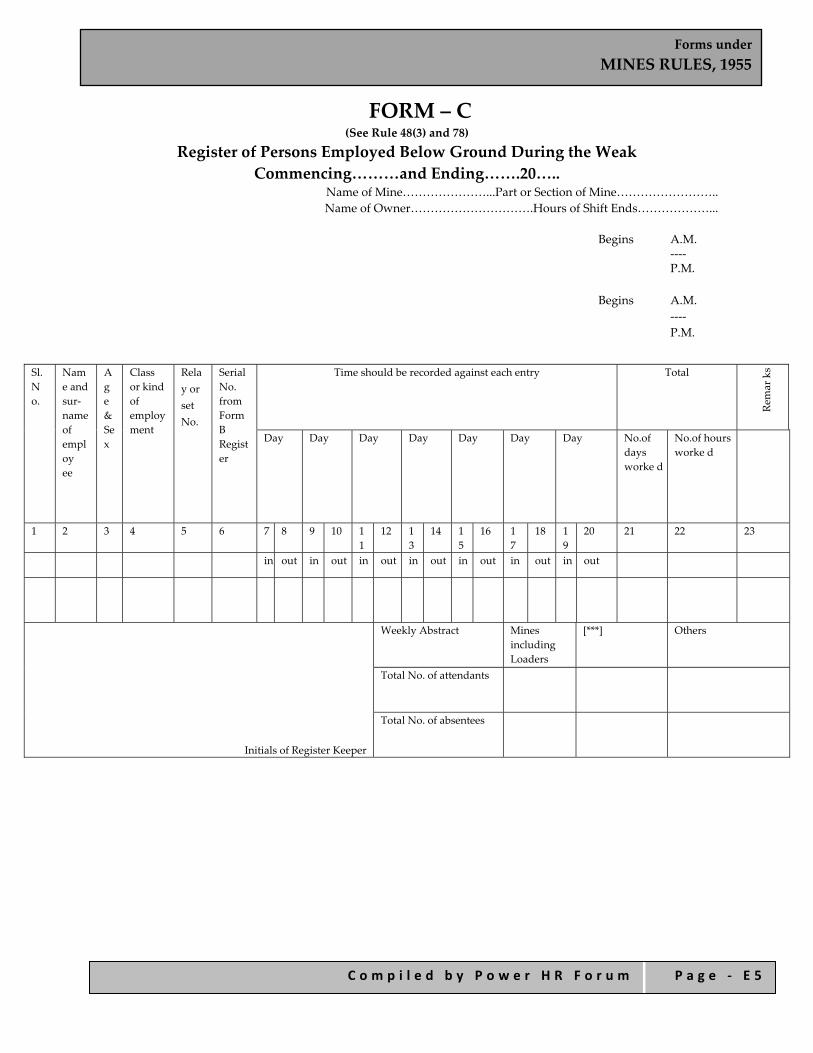
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 5
FORM – C (See Rule 48(3) and 78)
Register of Persons Employed Below Ground During the Weak Commencing………and Ending…….20…..
Name of Mine…………………...Part or Section of Mine…………………….. Name of Owner………………………….Hours of Shift Ends………………...
Begins A.M.
‐‐‐‐ P.M.
Begins A.M.
‐‐‐‐ P.M.
Sl.N o.
Name and sur‐name of employ ee
Ag e & Se x
Class or kind of employ ment
Relay or set No.
Serial No. from Form B Regist er
Time should be recorded against each entry Total
Remar ks
Day Day Day Day Day Day Day No.of days worke d
No.of hours worke d
1 2 3 4 5 6 7 8 9 10 11
12 13
14 15
16 17
18 19
20 21 22 23
in out in out in out in out in out in out in out
Initials of Register Keeper
Weekly Abstract Mines including Loaders
[***] Others
Total No. of attendants
Total No. of absentees
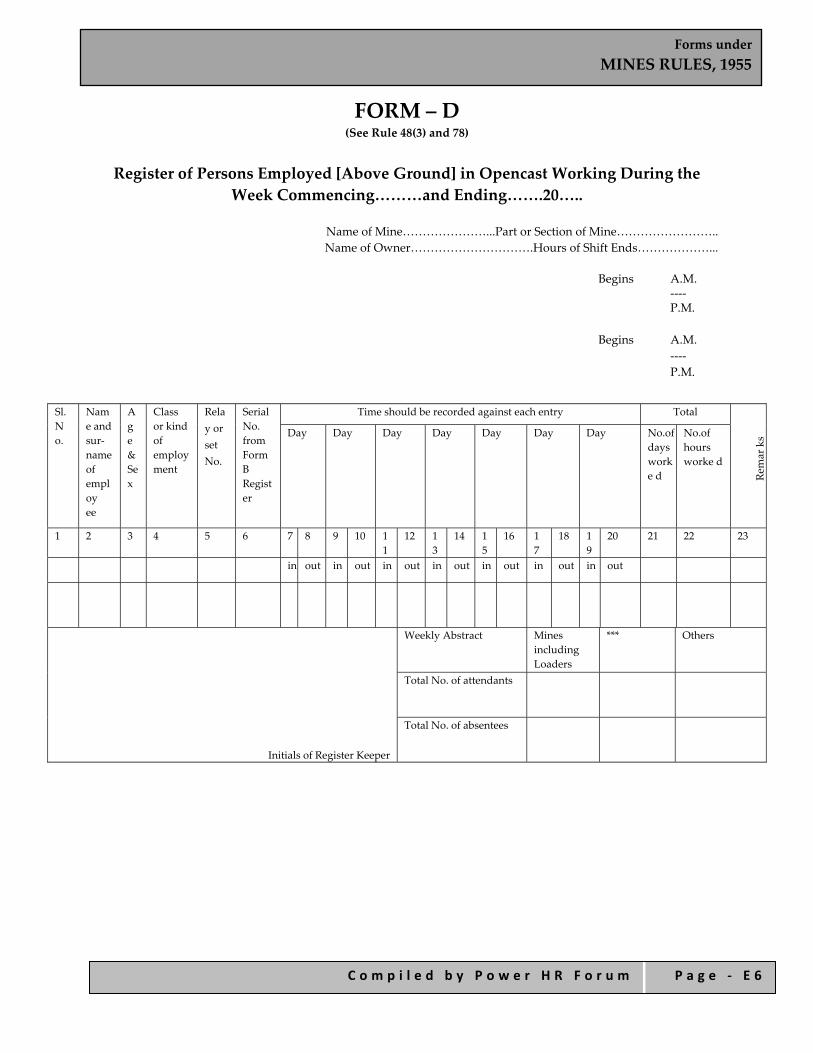
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 6
FORM – D (See Rule 48(3) and 78)
Register of Persons Employed [Above Ground] in Opencast Working During the
Week Commencing………and Ending…….20…..
Name of Mine…………………...Part or Section of Mine…………………….. Name of Owner………………………….Hours of Shift Ends………………...
Begins A.M.
‐‐‐‐ P.M.
Begins A.M.
‐‐‐‐ P.M.
Sl.N o.
Name and sur‐name of employ ee
Ag e & Se x
Class or kind of employment
Relay or set No.
Serial No. from Form B Register
Time should be recorded against each entry Total
Remar ks Day Day Day Day Day Day Day No.of
days worke d
No.of hours worke d
1 2 3 4 5 6 7 8 9 10 11
12 13
14 15
16 17
18 19
20 21 22 23
in out in out in out in out in out in out in out
Initials of Register Keeper
Weekly Abstract Mines including Loaders
*** Others
Total No. of attendants
Total No. of absentees

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 7
FORM – E (See Rule 48(3) and 78)
Register of Persons Employed Above Ground [Otherwise Than in Opencast Working] During the Week Commencing………..and Ending ………………20..
Name of Mine…………………...Part or Section of Mine…………………….. Name of Owner………………………….Hours of Shift Ends………………...
Begins A.M.
‐‐‐‐ P.M.
Begins A.M.
‐‐‐‐ P.M.
Sl.N o.
Name and sur‐name of employ ee
Ag e & Se x
Class or kind of employment
Relay or set No.
Serial No. from Form B Register
Time should be recorded against each entry Total
Remar ks
Day Day Day Day Day Day Day No.of days worke d
No.of hours worke d
1 2 3 4 5 6 7 8 9 10 11
12 13
14 15
16 17
18 19
20 21 22 23
in out in out in out in out in out in out in out
Initials of Register keeper
Weekly Abstract Mines Women [***]
Total No. of attendants
Total No. of absentees
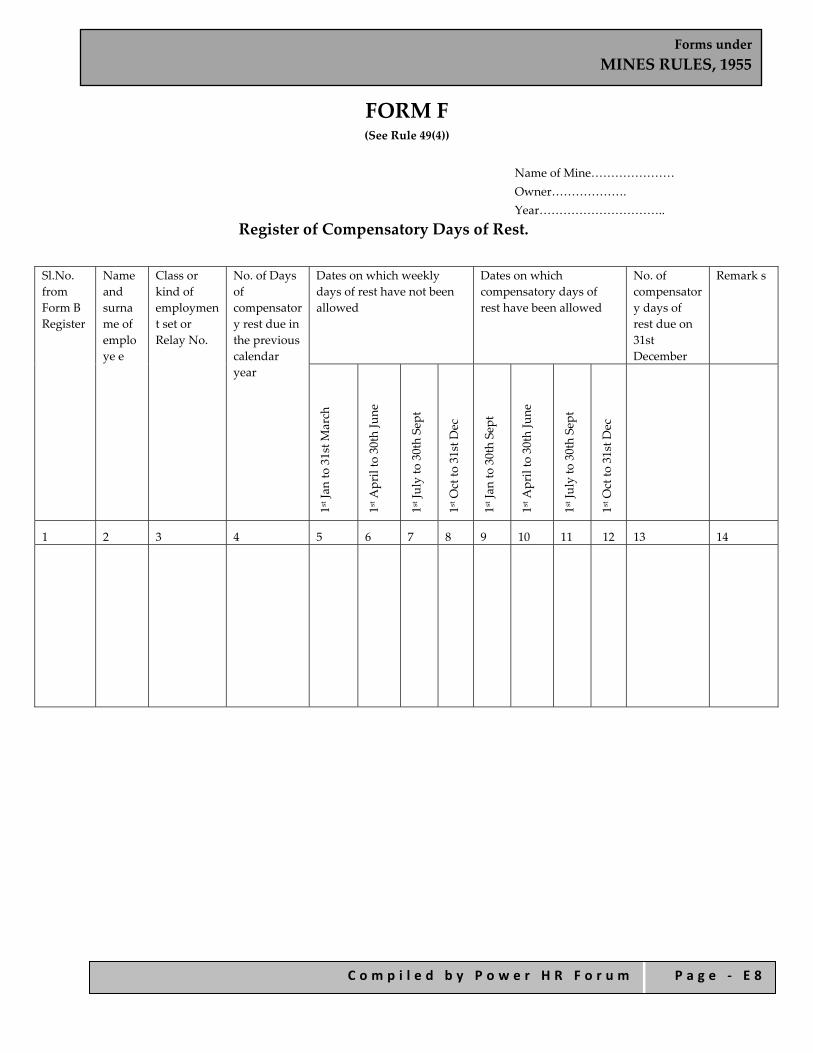
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 8
FORM F (See Rule 49(4))
Name of Mine………………… Owner………………. Year…………………………..
Register of Compensatory Days of Rest.
Sl.No. from Form B Register
Name and surname of employe e
Class or kind of employmen t set or Relay No.
No. of Days of compensator y rest due in the previous calendar year
Dates on which weekly days of rest have not been allowed
Dates on which compensatory days of rest have been allowed
No. of compensator y days of rest due on 31st December
Remark s
1st Jan to 31st M
arch
1st A
pril to 30th June
1st July to 30th Sept
1st O
ct to 31st D
ec
1st Jan to 30th Sept
1st A
pril to 30th June
1st July to 30th Sept
1st O
ct to 31st D
ec
1 2 3 4 5 6 7 8 9 10 11 12 13 14

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 9
FORM – G (See Rules 53)
Name of Mine……………….. Owner…………….
Register of Leave Account During the Calendar Year…………..
Serial N
o. from Form B
Register
Nam
e an
d surnam
e of employ
ee
Nature of employ
ment, mentio
ned
whether abo
ve or b
elow groun
d Category of employ
ment,
mentio
n whether m
onthly, w
eekly,
daily or p
iece‐rated
.
Actual Number of days worked during the year Leave period due in ensuing year
Remarks
Janu
ary
Februa
ry
March
April
May
June
July
Aug
ust
Septem
ber
Octob
er
Nov
ember
Decem
ber
Total
Days of leave
entitled
Arrears from
previous year
Total
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
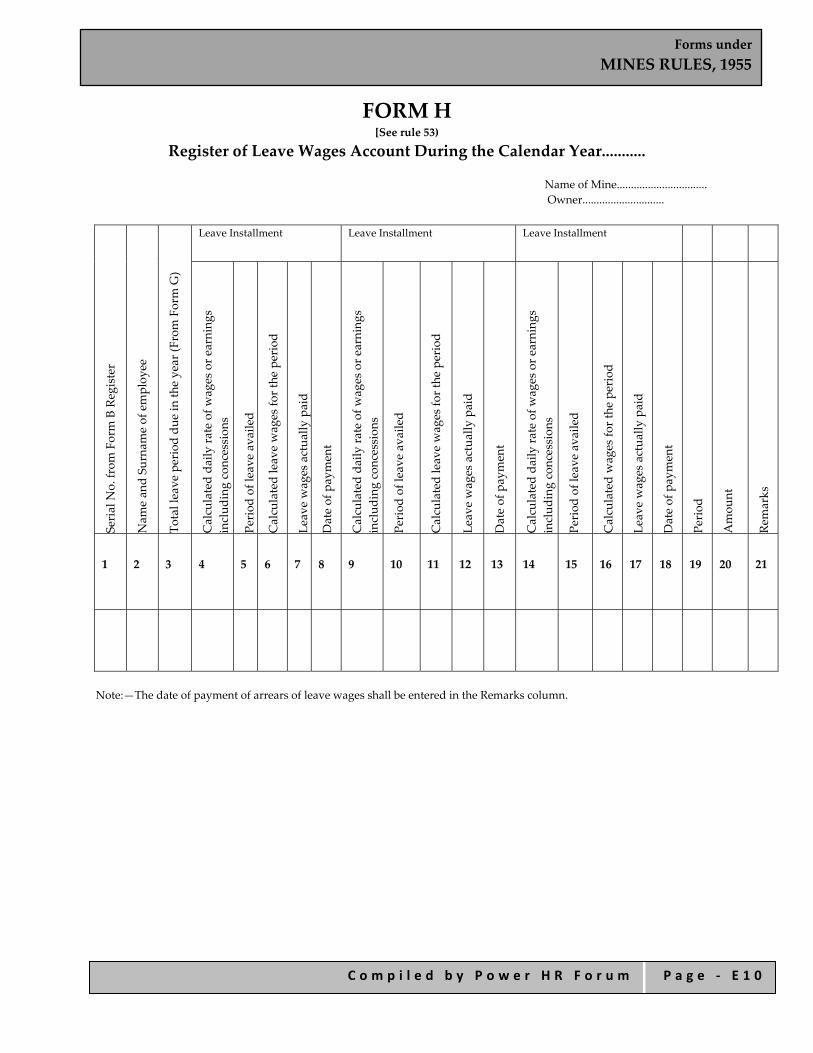
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 0
FORM H [See rule 53)
Register of Leave Wages Account During the Calendar Year...........
Name of Mine................................ Owner.............................
Serial N
o. from Form B Register
Nam
e an
d Su
rnam
e of employ
ee
Total leave period du
e in th
e year (F
rom Form G)
Leave Installment
Leave Installment Leave Installment
Calculated da
ily ra
te of w
ages or e
arning
s includ
ing concession
s
Period of leave availed
Calculated leave wages fo
r the period
Leave wages actua
lly paid
Date of payment
Calculated da
ily ra
te of w
ages or e
arning
s includ
ing concession
s
Period of leave availed
Calculated leave wages fo
r the period
Leave wages actua
lly paid
Date of payment
Calculated da
ily ra
te of w
ages or e
arning
s includ
ing concession
s
Period of leave availed
Calculated wages fo
r the period
Leave wages actua
lly paid
Date of payment
Period
Amou
nt
Remarks
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Note:—The date of payment of arrears of leave wages shall be entered in the Remarks column.

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 1
FORM – I (See Rules 59)
Register of Overtime Wages
Serial N
o. from Form B Register
Nam
e an
d Su
rnam
e of employ
ee
Nature of w
ork abov
e or below
grou
nd
Class or k
ind of employ
ment
Ordinary rate of w
ages
Ovrtim
e rate of w
ages
Week ending Week ending
Date on w
hich overtim
e worked
Num
ber o
f overtim
e ho
urs
worked on th
at date
Num
ber o
f overtim
e ho
urs in
the week
Overtim
e Ea
rning
Date of Payment
Date on w
hich overtim
e worked
Num
ber o
f overtim
e ho
urs
worked on th
at date
Num
ber o
f overtim
e ho
urs in
the week
Overtim
e Ea
rning
Date of Payment
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Week ending Week ending Weekending
Remarks
Date on w
hich overtim
e worked
Num
ber o
f overtim
e ho
urs
worked on th
at date
Num
ber o
f overtim
e ho
urs in
the week
Overtim
e Ea
rning
Date of Payment
Date on w
hich overtim
e worked
Num
ber o
f overtim
e ho
urs
worked on th
at date
Num
ber o
f overtim
e ho
urs in
the week
Overtim
e Ea
rning
Date of Payment
Date on w
hich overtim
e worked
Num
ber o
f overtim
e ho
urs
worked on th
at date
Num
ber o
f overtim
e ho
urs in
the week
Overtim
e Ea
rnings
Date of Payment
17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
Name of Mine…………………… Owner………………… Month …………………..

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 2
FORM – J (See Rules 76)
Report of Accident
Register of reportable accidents
S.No.
Date of entry
Date of accident
Time of accident
Classification
Brief d
escriptio
n of case of
accide
nt
Nam
e of in
jured worker
Sl. N
o. from Register in
Form B.
Nature of employ
ment
Nature of in
jury
Parts o
f bod
y injured
Date of re
turn of injured
person to w
ork
Duration of enforced absence
(in days)
Initials of atte
nding Med
ical
practitioner
Remarks
By place of a
ccident
By Cau
se
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Instructions:— Col. (5): Specify as indicated in Annexure I. Col. (6): Specify as indicated in Annexure II. Col. (7): Give brief description of the circumstances attending the accident. Col. (11): Specify whether simple wound, laceration, abrasion or fracture (only toes, fingers and thumb etc.) Col. (14): Mention the days intervening the days of occurrence and day of rejoining and not including either the date of occurrence or rejoining. Col. (16): In case if an injury proves ‘Serious’ or ‘Fatal’ or when injured person proceeds on leave or leaves his employment, particulars should be entered in this column.
Name of Mine…………………… Owner………………… State ………………….. District………………….. Mineral worked………………….. Quarter ending …………………..
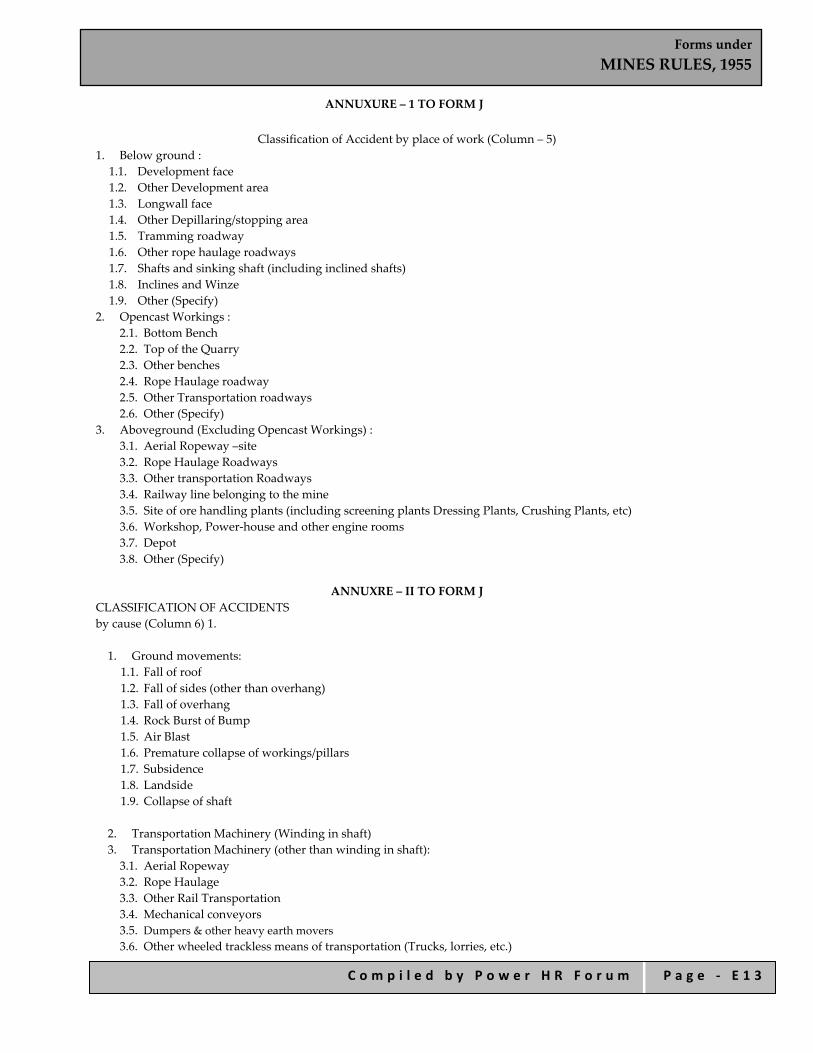
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 3
ANNUXURE – 1 TO FORM J
Classification of Accident by place of work (Column – 5) 1. Below ground :
1.1. Development face 1.2. Other Development area 1.3. Longwall face 1.4. Other Depillaring/stopping area 1.5. Tramming roadway 1.6. Other rope haulage roadways 1.7. Shafts and sinking shaft (including inclined shafts) 1.8. Inclines and Winze 1.9. Other (Specify)
2. Opencast Workings : 2.1. Bottom Bench 2.2. Top of the Quarry 2.3. Other benches 2.4. Rope Haulage roadway 2.5. Other Transportation roadways 2.6. Other (Specify)
3. Aboveground (Excluding Opencast Workings) : 3.1. Aerial Ropeway –site 3.2. Rope Haulage Roadways 3.3. Other transportation Roadways 3.4. Railway line belonging to the mine 3.5. Site of ore handling plants (including screening plants Dressing Plants, Crushing Plants, etc) 3.6. Workshop, Power‐house and other engine rooms 3.7. Depot 3.8. Other (Specify)
ANNUXRE – II TO FORM J
CLASSIFICATION OF ACCIDENTS by cause (Column 6) 1. 1. Ground movements:
1.1. Fall of roof 1.2. Fall of sides (other than overhang) 1.3. Fall of overhang 1.4. Rock Burst of Bump 1.5. Air Blast 1.6. Premature collapse of workings/pillars 1.7. Subsidence 1.8. Landside 1.9. Collapse of shaft
2. Transportation Machinery (Winding in shaft) 3. Transportation Machinery (other than winding in shaft): 3.1. Aerial Ropeway 3.2. Rope Haulage 3.3. Other Rail Transportation 3.4. Mechanical conveyors 3.5. Dumpers & other heavy earth movers 3.6. Other wheeled trackless means of transportation (Trucks, lorries, etc.)

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 4
4. Machinery‐other than Transportation Machinery :
4.1. Drills 4.2. Coal cutting Machinery 4.3. Coal Loading Machinery 4.4. Haulage Engine 4.5. Winding Engine 4.6. Shovels, Draglines, Excavators etc. 4.7. Ore handling Plants (including crushing and screening plants) 4.8. Pumps 4.9. Other (specify)
5. Explosive 6. Electricity 7. Dust Gas and other combustible material : 7.1. Occurrence of gas 7.2. Influx of gas 7.3. Suffocation by gases 7.4. Explosion or ignition of gas/ dust etc. 7.5. Outbreak of fire or spontaneous heating 7.6. Others (Specify)
8. Falls (other than falls of ground) :
8.1. Falls of persons from heights or into depths 8.2. Falls of persons on the same level 8.3. Falls of objects other than falls of ground 8.4. Other falls (Specify)
9. Other Cause : 9.1. Irruption of water 9.2. Flying pieces 9.3. Extremity caught in between objects 9.4. Unclassified (Specify)”}
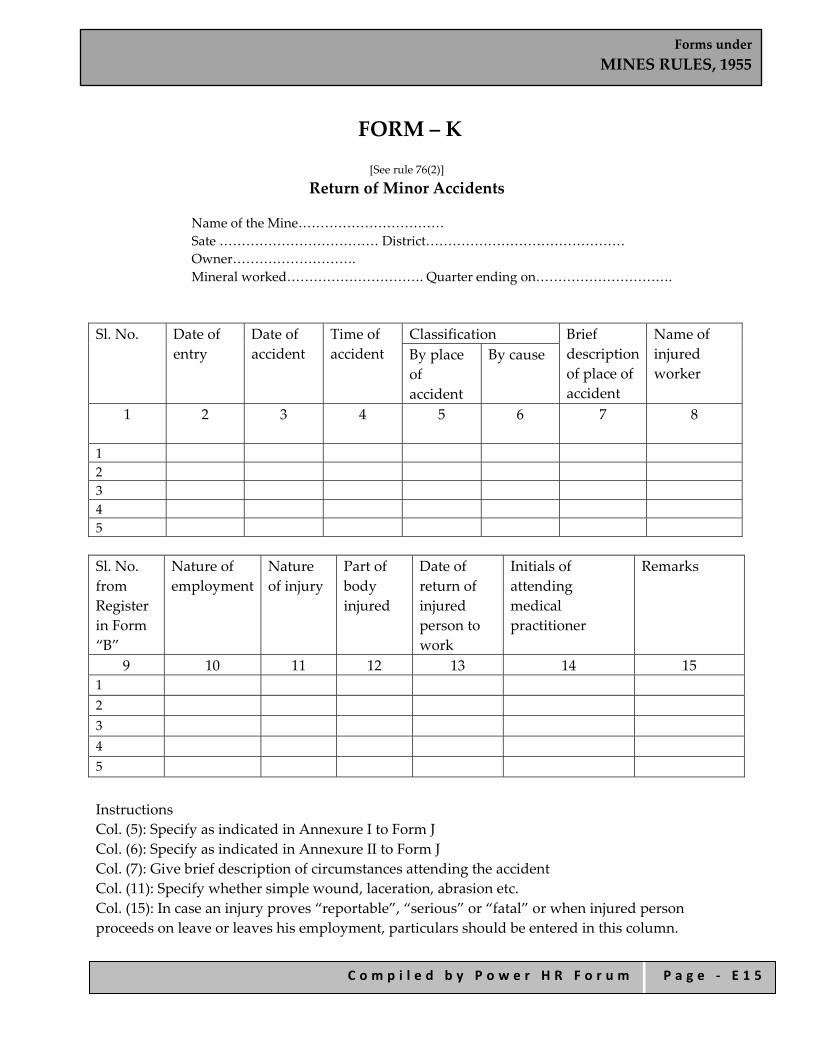
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 5
FORM – K
[See rule 76(2)]
Return of Minor Accidents
Name of the Mine…………………………… Sate ……………………………… District……………………………………… Owner………………………. Mineral worked…………………………. Quarter ending on………………………….
Sl. No. Date of entry
Date of accident
Time of accident
Classification Brief description of place of accident
Name of injured worker
By place of accident
By cause
1 2 3 4 5 6 7 8
1 2 3 4 5 Sl. No. from Register in Form “B”
Nature of employment
Nature of injury
Part of body injured
Date of return of injured person to work
Initials of attending medical practitioner
Remarks
9 10 11 12 13 14 15 1 2 3 4 5 Instructions Col. (5): Specify as indicated in Annexure I to Form J Col. (6): Specify as indicated in Annexure II to Form J Col. (7): Give brief description of circumstances attending the accident Col. (11): Specify whether simple wound, laceration, abrasion etc. Col. (15): In case an injury proves “reportable”, “serious” or “fatal” or when injured person proceeds on leave or leaves his employment, particulars should be entered in this column.
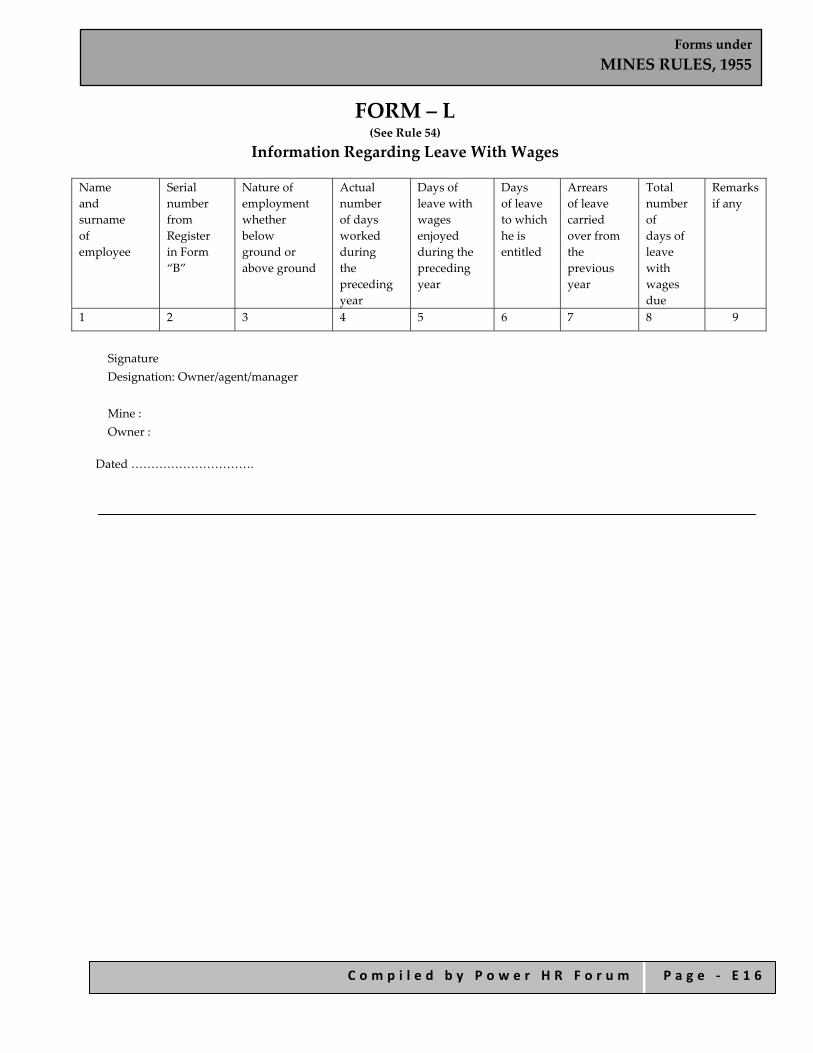
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 6
FORM – L (See Rule 54)
Information Regarding Leave With Wages
Name and surname of employee
Serial number from Register in Form “B”
Nature of employment whether below ground or above ground
Actual number of days worked during the preceding year
Days of leave with wages enjoyed during the preceding year
Days of leave to which he is entitled
Arrears of leave carried over from the previous year
Total number of days of leave with wages due
Remarks if any
1 2 3 4 5 6 7 8 9
Signature Designation: Owner/agent/manager Mine : Owner :
Dated ………………………….
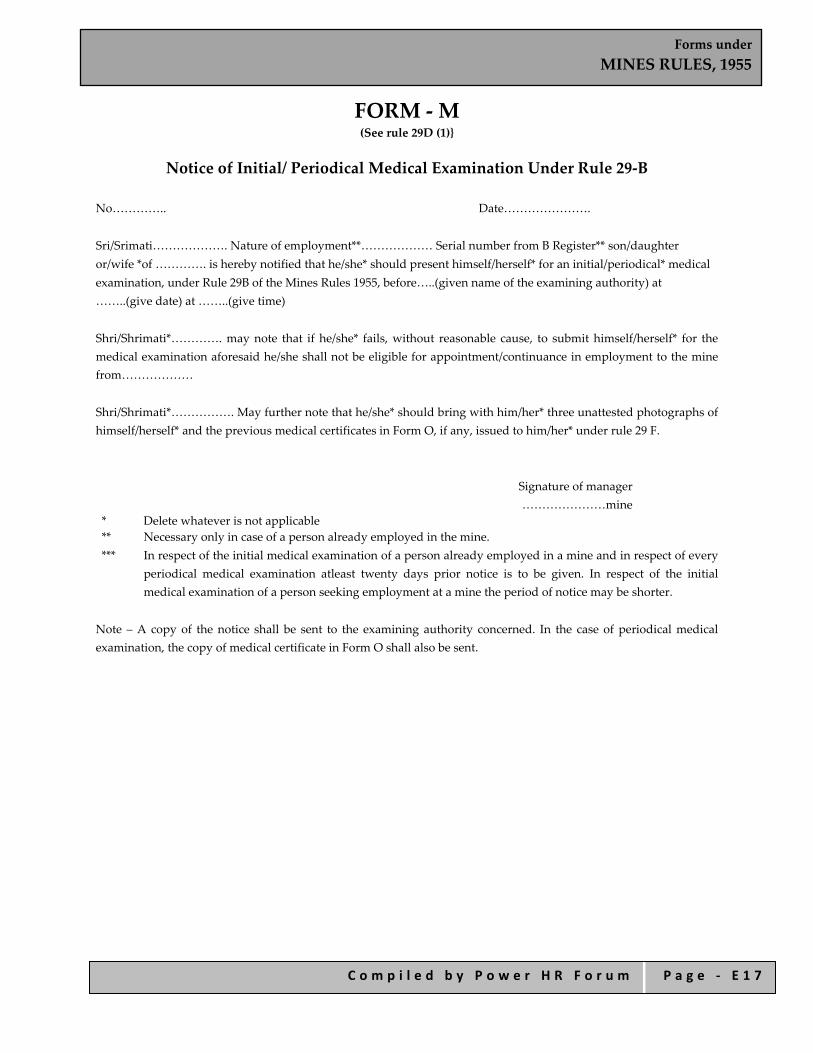
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 7
FORM ‐ M (See rule 29D (1)}
Notice of Initial/ Periodical Medical Examination Under Rule 29‐B
No………….. Date………………….
Sri/Srimati………………. Nature of employment**……………… Serial number from B Register** son/daughter or/wife *of …………. is hereby notified that he/she* should present himself/herself* for an initial/periodical* medical examination, under Rule 29B of the Mines Rules 1955, before…..(given name of the examining authority) at ……..(give date) at ……..(give time)
Shri/Shrimati*…………. may note that if he/she* fails, without reasonable cause, to submit himself/herself* for the medical examination aforesaid he/she shall not be eligible for appointment/continuance in employment to the mine from………………
Shri/Shrimati*……………. May further note that he/she* should bring with him/her* three unattested photographs of himself/herself* and the previous medical certificates in Form O, if any, issued to him/her* under rule 29 F.
Signature of manager …………………mine
* Delete whatever is not applicable ** Necessary only in case of a person already employed in the mine. *** In respect of the initial medical examination of a person already employed in a mine and in respect of every
periodical medical examination atleast twenty days prior notice is to be given. In respect of the initial medical examination of a person seeking employment at a mine the period of notice may be shorter.
Note – A copy of the notice shall be sent to the examining authority concerned. In the case of periodical medical examination, the copy of medical certificate in Form O shall also be sent.

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 8
FORM ‐ N {See rule 29D (S)}
Second and Final Notice of Initial/Periodical Medical Examination Under Rule 29‐B No……… Date………….
Shri/Shrimate*…………… nature of employment………… serial number from Form B Register……… Son/daughter/wife of ………. failed to present himself/herself* for an initial/periodical* medical examination on…… in respect of which he/she/had been given a notice on ………….
He/She* is hereby again notified that he/she* should present himself/herself* for an initial/periodical* medical examination, under rule 29B of the Mines Rules, 1955, before……….(give name of the examining authority) at ……(give date)……..at……….(give time)
Shri/Shrimati*…………, may note that if he/she* fails to submit himself/herself* for the medical examination aforesaid, he/she* shall not be employed/retained in employment in the mine from………
Shri/Shrimati*………….., may further note that he/she* should bring with him/her* three unmounted photographs of himself/herself* and he previous medical certificate in Form O, if any, issued to him/her* under rule 29F.
Signature of Manager
…………………mine * Delete whatever is not applicable ** In respect of the initial medical examination of a person already employed in a mine and in respect of every
periodical medical examination, the second notice is to be given atleast 10 days previously.
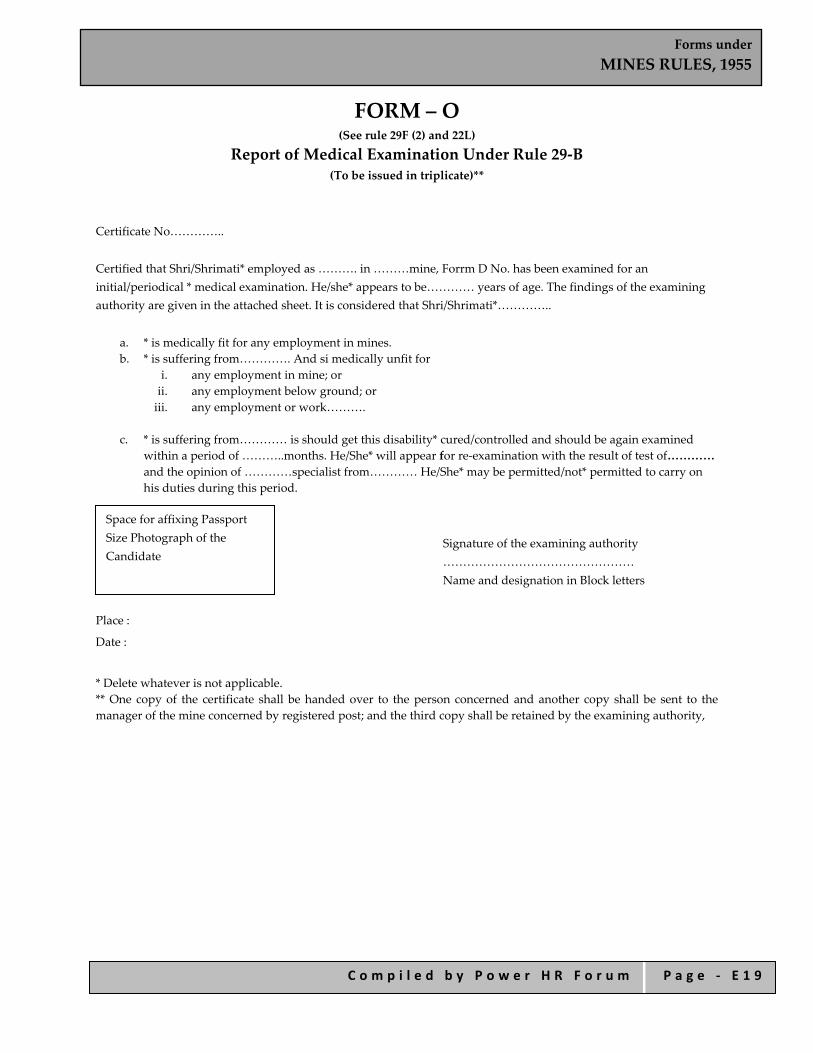
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 1 9
FORM – O (See rule 29F (2) and 22L)
Report of Medical Examination Under Rule 29‐B (To be issued in triplicate)**
Certificate No…………..
Certified that Shri/Shrimati* employed as ………. in ………mine, Forrm D No. has been examined for an initial/periodical * medical examination. He/she* appears to be………… years of age. The findings of the examining authority are given in the attached sheet. It is considered that Shri/Shrimati*…………..
a. * is medically fit for any employment in mines. b. * is suffering from…………. And si medically unfit for
i. any employment in mine; or ii. any employment below ground; or iii. any employment or work……….
c. * is suffering from………… is should get this disability* cured/controlled and should be again examined
within a period of ………..months. He/She* will appear for re‐examination with the result of test of………… and the opinion of …………specialist from………… He/She* may be permitted/not* permitted to carry on his duties during this period.
Signature of the examining authority ………………………………………… Name and designation in Block letters
Place :
Date :
* Delete whatever is not applicable. ** One copy of the certificate shall be handed over to the person concerned and another copy shall be sent to the manager of the mine concerned by registered post; and the third copy shall be retained by the examining authority,
Space for affixing Passport Size Photograph of the Candidate

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 0
FORM O – Cont. Report of the Examining Authority
(to be filled in for every medical examination whether initial or periodical or reexamination or after cure/control of disability). Annexure to Certificate No…………as result of medical examination on ……. Identification Mark……………..
Left thumb impression of the candidate
1. General development‐ Good/Fair/Poor 2. Height…………Cms. 3. Weight…………kg. 4. Eyes :
i. Visual acuity‐Distant vision (with or without glasses).
Right eye……..Left eye………….. ii. any organic disease of eyes iii. night blindness iv. Colour blindness v. Squint
(* to be tested in special cases)
5. Ears : i. Hearing : right ear………….Left ear …………….. ii. Any organic diseases.
6. Respiratory system.
Chest measurement : i. after full inspiration …………cms. ii. After full expiration…………..cms.
7. Circulatory system:
Blood Pressure Pulse
8. Abdomen : Tenderness. Liver. Spleen. Tumour.
9. Nervous system: History of fits or epilepsy Paralysis. Mental helath.
10. Locomotory system 11. Skin. 12. Hyrocele.
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 1
13. Hernia. 14. Any other abnormality 15. Unine :
Reaction. Albumin. Sugar.
16. Skiagram of chest. 17. Any other ‘ c ‘ test considered necessary by the examining authority. 18. Any opinion of specialist considered necessary.
Signature of the examining authority
Place:

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 2
FORM – P (See rule 29F (i) and 29L)
Medical Standard of Fitness for Persons Employed
1. The person should be in good mental and bodily health and free from any physical defect likely to interfere with his efficient employment in a mine.
2. Skeletal nervous system : The limbs should be well formed and developed, and the function of all the limbs should be within normal limits. Any deformity should be recorded. There should be no deformity or paralysis which may interfere with his efficient employment in a mine.
3. Skin :There should be no evidence of extensive and chornic skin disease or ulceration. In case of infective type of skin disease, the candidate could be made fit after he has undergone a treatment. All occupational skin diseases should be noted.
4. Eye vision should be not less than the following standard: 1) Better eye 6/12 2) Worse eye 6/18 b. There should be no night blindness for persons employed below ground and for persons employed
in open cast working in shifts other than in mornings shifts. c. A person having only one eye which functions normally should not be employed below ground,
For employment on surface the vision of such a person in the other eye should be 6/18 with or without glasses.
5. Hearing should be good. Any progressive disease affecting hearing/or occupational deafness should be
recorded. 6. Speech must be without serious impediment. Unless this is also accompanied by generalised partial
paralysis this should not be a reason for declaring unfit. 7. (a) Respiratory system should be sound and free from any chronic bronchial or laryngeal disease. This
however alone should not be reason to make unfit. (b) A full sized postero‐anterior chest radiograph (large enough to include thoracic inlet and both costophrenic angles) obtained by an X‐ray machine of at least 300 mA (A Milli‐Ampere) strength shall be evaluated in the manner specified by the Chief Inspector and Lung function tests (spirometry) to record forced vital capacity (FVC) and forced expiratory volume in one second (EFVI) shall be made. There should not be any evidence of active pulmonary disease. If there are evidences of active pulmonary tuberculosis he may be permitted to work if his sputum is negative on repeated examination and on production of a certificate that he is taking treatment from a qualified medical practitioner/ Hospital.
8. Circulatory system – There should be no evidence of any heart or vascular disease which may interfere with his efficient employment in a mine.
9. In case the candidate has hernia he may be declared fit after he has been successfully operated for the same. 10. Hydrocele if present should not be large enough to impede the normal activities of the candidate. In such
cases he may be declared fit after being successfully operated. 11. The medical examination should include examination of urine and of other system for evidence of disease.
Mere presence of albumen and sugar in the urine without any gross organic disease producing signs and symptoms should not be considered as a disability.
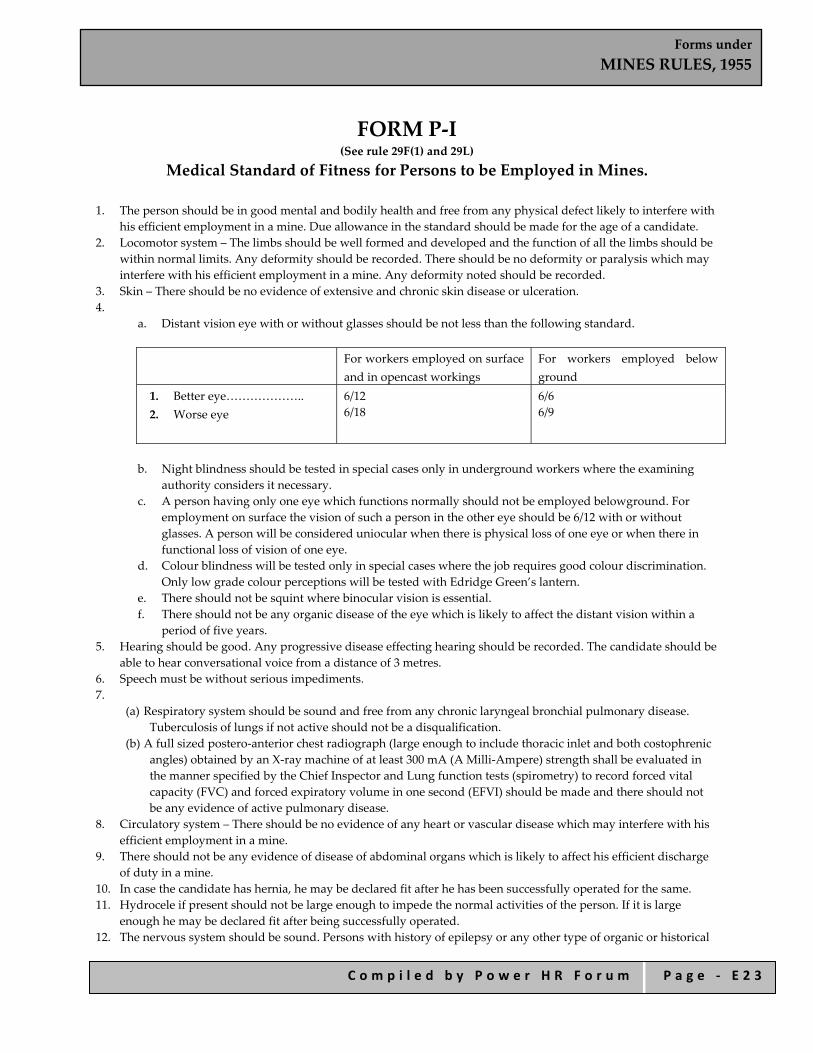
Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 3
FORM P‐I
(See rule 29F(1) and 29L)
Medical Standard of Fitness for Persons to be Employed in Mines. 1. The person should be in good mental and bodily health and free from any physical defect likely to interfere with
his efficient employment in a mine. Due allowance in the standard should be made for the age of a candidate. 2. Locomotor system – The limbs should be well formed and developed and the function of all the limbs should be
within normal limits. Any deformity should be recorded. There should be no deformity or paralysis which may interfere with his efficient employment in a mine. Any deformity noted should be recorded.
3. Skin – There should be no evidence of extensive and chronic skin disease or ulceration. 4.
a. Distant vision eye with or without glasses should be not less than the following standard.
For workers employed on surface and in opencast workings
For workers employed below ground
1. Better eye……………….. 2. Worse eye
6/12 6/18
6/6 6/9
b. Night blindness should be tested in special cases only in underground workers where the examining
authority considers it necessary. c. A person having only one eye which functions normally should not be employed belowground. For
employment on surface the vision of such a person in the other eye should be 6/12 with or without glasses. A person will be considered uniocular when there is physical loss of one eye or when there in functional loss of vision of one eye.
d. Colour blindness will be tested only in special cases where the job requires good colour discrimination. Only low grade colour perceptions will be tested with Edridge Green’s lantern.
e. There should not be squint where binocular vision is essential. f. There should not be any organic disease of the eye which is likely to affect the distant vision within a
period of five years. 5. Hearing should be good. Any progressive disease effecting hearing should be recorded. The candidate should be
able to hear conversational voice from a distance of 3 metres. 6. Speech must be without serious impediments. 7.
(a) Respiratory system should be sound and free from any chronic laryngeal bronchial pulmonary disease. Tuberculosis of lungs if not active should not be a disqualification.
(b) A full sized postero‐anterior chest radiograph (large enough to include thoracic inlet and both costophrenic angles) obtained by an X‐ray machine of at least 300 mA (A Milli‐Ampere) strength shall be evaluated in the manner specified by the Chief Inspector and Lung function tests (spirometry) to record forced vital capacity (FVC) and forced expiratory volume in one second (EFVI) should be made and there should not be any evidence of active pulmonary disease.
8. Circulatory system – There should be no evidence of any heart or vascular disease which may interfere with his efficient employment in a mine.
9. There should not be any evidence of disease of abdominal organs which is likely to affect his efficient discharge of duty in a mine.
10. In case the candidate has hernia, he may be declared fit after he has been successfully operated for the same. 11. Hydrocele if present should not be large enough to impede the normal activities of the person. If it is large
enough he may be declared fit after being successfully operated. 12. The nervous system should be sound. Persons with history of epilepsy or any other type of organic or historical

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 4
fits should not be declared fit for employment in a mine. 13. The medical examination should include examination of urine. Mere presence of albumen and sugar in the
urine without any gross organic disease producing signs and symptoms should not be a disability. 14. Skiagram of the chest should also he obtained. If it is necessary, the medical officer may direct the candidate to
obtain the result of special tests or/and the opinion of a specialist from recognized institution/hospital.

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 5
FORM – Q
(See rule 29J(2) 9 (a))
Notice of Medical Re‐Examination by Appellate Medical Board
No……….. Date………………..
MEMORANDUM
Shri/Shrimati*………..Nature of employment……………serial number from From B Register………… son/daughter/wife* of ………….., who has appealed for a re‐examination against the findings of a medical examination under rule 29B of Mines Rules, 1955 that he/she is unfit for :
a. *Any employment in mines. b. *Any employment below………. Ground. c. *Any employment on work………..(Specify in detail) is hereby notified that he/she * should present
himself/herself* for a medical reexamination by the Appellate Medical Board at ………. (give exact description of place) on**………….(give date) at ……….(Give time).
Shri/Shrimati*…….may note that if he/she* fails without reasonable cause, to submit himself/herself* for the medical re‐examination aforesaid he/she* shall not be retained in employment in the mine.
Signature of manager ……………………mine.
* Delete whatever is not applicable **15 days, prior notice is to be given to a medical re‐examination by the Appellate Medical Board.

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 6
FORM – R (See rule 29J(2) (b) )
Second and Final Notice of Medical Re‐Examination by Appellate Medical Board
No………….. Date……………19
MEMORANDUM
Shri/Shrimati*………..Nature of employment……………serial number from From B Register………… son/daughter/wife* of ………….., failed to present himself/herself* for medical re‐examination on …..in respect of which he/she* had been given a notice on …………
He/She* is hereby again notified that he/she* should present himself/herself* for a medical re‐examination by the Appellate Medical Board at ……..(give exact description of place) on **………….(give date) at …………(give time).
Shri/Shrimati*…..may note that if he/she* fails to submit himself/herself* for the medical re‐examination aforesaid, he/she* shall not be retained in employment in the mine.
Signature of Manager ……………….. mine.
* Delete whatever is not applicable **15 days, prior notice is to be given to a medical re‐xamination by the Appellate Medical Board.

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 7
FORM – S (See rule 29L)
Report of Medical Re‐Examination by Appellate Medical Board
(To be issued in triplicate)**
We do hereby certify that we have examined Shri/Shrimati* ……….. Nature of employment…….., Serial Number from Forrm B Register………….. of ….. mine, who has been declared medically unfit for.
a. *any employment in mine. b. *any employment belowground. c. *any employment in work……………………………………. (Specify in details) as a result of a medical
examination under rule 29B. Our Report is given overleaf. We consider that –
1. He/She* is medically fit for any employment in mine. 2. He/She* is suffering from……….. and is medically unfit for
a. *any employment in mine. b. *any employment belowground. c. * any employment in work………. …………………..(Specify in details)
3. He/She is suffering from…………and should get this disability/cured/controlled* and should be again
examined within a period of ……………months. He will appear for re‐examination within a period of…………months. He will appear for reexamination with the result of test of………* and opinion of ………specialist from…………He may be permitted/not permitted* to carry on his duties during this period.
Signature of members of Appellate Medical Board
Place............. Date..............
1…………………(Convenor) 2………….. 3……………
* Delete whatever is not applicable **One copy of certificate shall be handed over to the person concerned and another copy shall be sent to the manager of the mines concerned by registered post, and the third copy shall be retained by the Convener of the Appellate Medical Board.

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 8
REPORT OF THE APPLELLATE MEDICAL BOARD
Annexure to certificate No………….as a result of Medical examination On…………….
identification mark :
Left thumb impression of the candidate
1. General development. Good/Fair/Poor 2. Height……….cms. 3. Weigth……….kg. 4. Eyes………
i. visual acuity Distant vision(with or without glasses) ii. any organic disease of eyes. iii. *night blindness Right eye………Left eye…………. iv. *Colour blindness……… v. Squint…………………..
(* to be tested in special cases) 5. Ears :
(i) Hearing……… Right Ear………………… Left Ear……………………. (ii) any organic disease
6. Respiratory system :
Chest measurement i. after full inspiration …….cms ii. after full expiration……
7. Circulatory system :
Blood pressure…………. Pulse…………..
8. Abdomen :
Tenderness…….. Liver…….. Spleen………… Tumour………..
9. Nervous system : History of fits or epilepsy….. Paralysis…….. Mental helath………
10. Locomotor system : 11. Skin : 12. Hernia : 13. Hydrocele :
14. Any other abnormality :
Urine: Reaction…….. Albumin………

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 2 9
Sugar……….. 15. Skiagram of chest : 16. Any other test considered necessary by the examining authority. 17. Any opinion of specialist considered necessary. Place : Signature of the Appellate Medical Board

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 3 0
FORM – T (See rule 29‐P(i))
Annual Return for the Year Ending on The 31st December
1. Name of mines……………… 2. Postal address of Mines…………… 3. Date of opening ……………….. 4. Date of closing (if closed)…………. 5. Situation of Mine (District/State)………….. 6. Name of Owner………..
Postal address of owner………… 7. Number of persons required to be medically examined……….
8. Number of persons medically examined…………… 9. Number of persons declared medically unfit………… 10. Categorization of the persons declared unfit…………. Certified that the information given above is correct to the best of my knowledge.
Signature…………….. Designation…………….. Date………………

Forms under MINES RULES, 1955
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ E 3 1
FORM – U (See rule 29‐R and 29‐ S)
Record of Report by Workmen Inspector
Name of Mine………Owner…………
Manager…………….. Place/installation Inspected by ………………on ……………
Accompanied by………………
Observations Remedial Measures Suggested
Action taken for remedial measures
Date on which action taken
Remarks if any
Signature of Workmen’s Inspector with date Signature of Manager with date
Signature of mine official Accompanying the work‐Men’s Signature of Manager with date Inspector Date…….. Designation

Forms under
DANGEROUS MACHINES (REGULATION) RULES, 2007
C o m p i l e d b y P o w e r H R F o r u m P a g e - F 1
Forms under
DANGEROUS MACHINES
(REGULATION) RULES, 2007

Forms under
DANGEROUS MACHINES (REGULATION) RULES, 2007
C o m p i l e d b y P o w e r H R F o r u m P a g e - F 2
Index FORM I
Form of Licence For Manufacture or Commencement of Carrying on Business as a Manufacturer of a Dangerous Machine
FORM II
Form of Licence for Commencement or Carrying on Business as a Dealer of a Dangerous Machine

Forms under
DANGEROUS MACHINES (REGULATION) RULES, 2007
C o m p i l e d b y P o w e r H R F o r u m P a g e - F 3
FORM I [See Rule 3(1) and (3)]
Form of Licence for Manufacture or Commencement of Carrying on Business as a Manufacturer of a Dangerous Machine
Licence No. ..........................
Whereas M/s .............................. .............................. ......................................... .............................. of ........................................................................................................................................................ has/have (give full address) .................... applied for a licence for commencement of/carrying on business as a manufacturer of ..............................................................................
(here specify which dangerous machine)
And whereas the Controller is satisfied that the condition specified in clause (a) of sub section (4) of Section 9 or, as the case may be, sub section (4) of section 9 has been complied with.
Now, therefore, in exercise of the powers, conferred by Section 9 of the Act, licence is granted/renewed to M/s ................................ for a period of five years to commence/carry on business as a manufacturer of the: 1. 2. 3. (give name of machine [ power thresher, power operated chaff cutter, power operated sugarcane crusher ] and trade name with brief description and overall dimensions) This licence is issued subject to the following conditions, namely:— 1. The manufacturer shall ensure that the machine and every part thereof complies with the
standards specified by Rule 4 of the Dangerous Machines (Regulation) (Ammendment) Rules, 2007.
2. Without prejudice to the generality of condition No. (1) above, the manufacturer shall ensure
that the following parts are secured by safeguard of substantial construction :—
(a) The prime mover and every part thereof. (b) The transmission machinery and every part thereof. (c) Every other dangerous part such as rollers, blowers, elevators and the like.
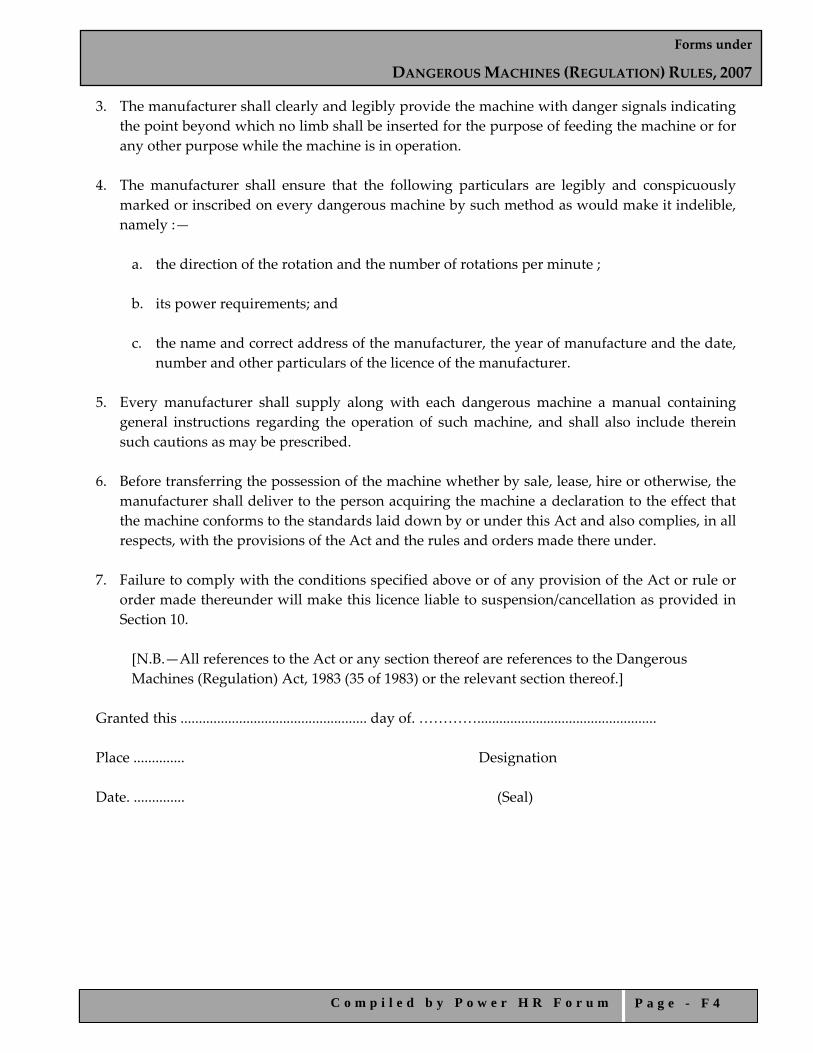
Forms under
DANGEROUS MACHINES (REGULATION) RULES, 2007
C o m p i l e d b y P o w e r H R F o r u m P a g e - F 4
3. The manufacturer shall clearly and legibly provide the machine with danger signals indicating the point beyond which no limb shall be inserted for the purpose of feeding the machine or for any other purpose while the machine is in operation.
4. The manufacturer shall ensure that the following particulars are legibly and conspicuously
marked or inscribed on every dangerous machine by such method as would make it indelible, namely :—
a. the direction of the rotation and the number of rotations per minute ;
b. its power requirements; and
c. the name and correct address of the manufacturer, the year of manufacture and the date,
number and other particulars of the licence of the manufacturer. 5. Every manufacturer shall supply along with each dangerous machine a manual containing
general instructions regarding the operation of such machine, and shall also include therein such cautions as may be prescribed.
6. Before transferring the possession of the machine whether by sale, lease, hire or otherwise, the
manufacturer shall deliver to the person acquiring the machine a declaration to the effect that the machine conforms to the standards laid down by or under this Act and also complies, in all respects, with the provisions of the Act and the rules and orders made there under.
7. Failure to comply with the conditions specified above or of any provision of the Act or rule or
order made thereunder will make this licence liable to suspension/cancellation as provided in Section 10.
[N.B.—All references to the Act or any section thereof are references to the Dangerous Machines (Regulation) Act, 1983 (35 of 1983) or the relevant section thereof.] Granted this ................................................... day of. …………................................................. Place .............. Designation Date. .............. (Seal)
Forms under
DANGEROUS MACHINES (REGULATION) RULES, 2007
C o m p i l e d b y P o w e r H R F o r u m P a g e - F 5
FORM II [See Rule 3(3)]
Form of Licence for Commencement or Carrying on Business as a Dealer of a Dangerous Machine
Licence No ....................... Whereas M/s ........................................................... of .......................................................................
(here give full address) has/have applied for a licence for commencement of/carrying on business as a dealer of ................ ……………………………………………
(here specify which dangerous machine)
And whereas the Controller is satisfied that the applicant proposes to commence/carry on business in ................................................................. which conform to the standards laid down (specify which machine) by or under the Dangerous Machines (Regulation) Act, 1983 (35 of 1983). Now, therefore, in exercise of the powers conferred by sub‐section (4) of Section 9, licence is granted to M/s .................................. for a period of five years to commence/carry on business as a dealer of : Sl. No. Name of the machine Make/model and brief
description HP/KW requirement of
the machine 1. 2. 3.
(specify types of threshers, power operated chaff cutter and power operated sugar cane crusher or other dangerous machine) This licence is issued subject to the following conditions, namely :—
1. The dealer shall deal only in machines of a manufacturer licenced under the Act.
2. Before transferring the possession of any machine whether by sale, lease, hire or otherwise, the dealer shall deliver to the person acquiring the possession of such machine, a declaration to the effect that the machine conforms to the standards laid down by or under this Act and also complies with, in all respects, the provisions of this Act and the rules and orders made there under.
3. Failure to comply with the conditions specified above or any provisions of the Act or rule or oreder made there under will make this licence liable to suspension /cancellation as provided in Section 10.
[N.B.— All references to the Act or any section thereof are references to the Dangerous Machines
(Regulation) Act, 1983 (35 of 1983) or to the relevant section thereof.] Granted this ...................................................... day of ...................................................................... Date ........................ Designation Place ........................ (Seal)
Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 1
Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 2
INDEX
FORM I
Notice of Intention to Have Sample Analyzed
FORM II
Memorandum to Government Analyst
FORM III
Report by Government Analyst
FORM IV Form of Notice
FORM V Environmental Statement for The Financial Year
Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 3
FORM I (See Rule 7)
Notice of Intention to have Sample Analysed To
.......................... ..........................
Take notice that is intended to have analysed the sample of............................................. which has been taken today, the.................................................................. day of......................................20......................................... from*..................................................................................... (Name and designation of the person who takes the sample) ................................................................................................................................................
(SEAL)
DATE...................... *Specify the place from where the sample is taken.

Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 4
FORM II (See Rule 8)
Memorandum to Government Analyst From ........................................ ........................................
To
The Government Analyst
........................................
........................................
The portion of sample described below is sent herewith for analysis (under Rule 6 of the Environment (Protection) Rules, 1986.
The portion of the sample has been marked by me with the following mark:
Details of the portion of samples taken.
Name and designation of person who sends the sample.
(SEAL) Date......................

Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 5
FORM III (See Rule 8)
Report by Government Analyst Report No...................... Date.................................
I hereby certify that I.................................................Government Analyst duly appointed under section 13 of the Environment (Protection) Act, 1986, received on the ................................. day of .................................................................................................................20.........................................................................from......................*...................................................................................................................................................................... a sample of.............................................................for analysis.
The sample was in a condition fit for analysis as reported below.
I further certify that I have analyzed the aforementioned sample on....................... and declare that the result of the analysis to be as follows:
**...........................................................................................................................................................................................................
The condition of seals, fastening of samples on receipt was as follows:
Signed this..................................... day of.......................................20.........................
Address.....................................................................
Signature
(Government Analyst) To
........................................
........................................ ........................................
*Here write the names of the officer/authority from whom the sample was obtained.
** Here write full details of analysis and method of analysis.
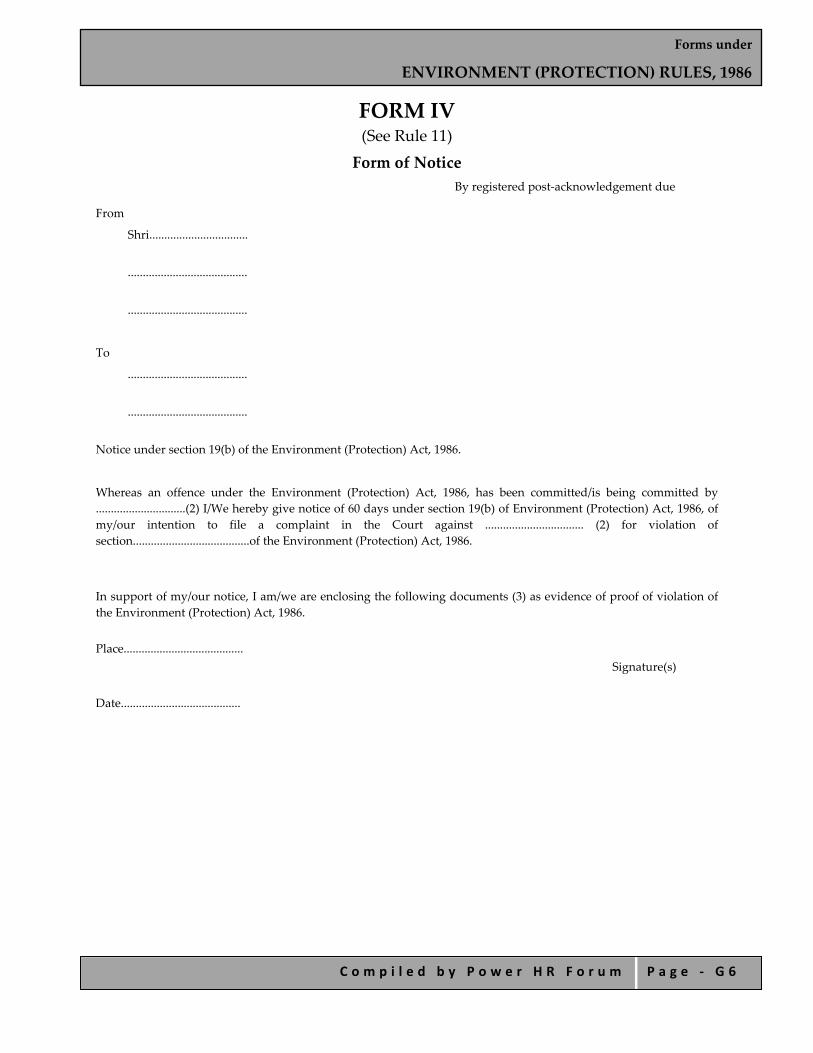
Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 6
FORM IV (See Rule 11) Form of Notice
By registered post‐acknowledgement due
From
Shri.................................
........................................
........................................
To
........................................
........................................
Notice under section 19(b) of the Environment (Protection) Act, 1986.
Whereas an offence under the Environment (Protection) Act, 1986, has been committed/is being committed by ..............................(2) I/We hereby give notice of 60 days under section 19(b) of Environment (Protection) Act, 1986, of my/our intention to file a complaint in the Court against ................................. (2) for violation of section.......................................of the Environment (Protection) Act, 1986.
In support of my/our notice, I am/we are enclosing the following documents (3) as evidence of proof of violation of the Environment (Protection) Act, 1986.
Place........................................ Signature(s)
Date........................................
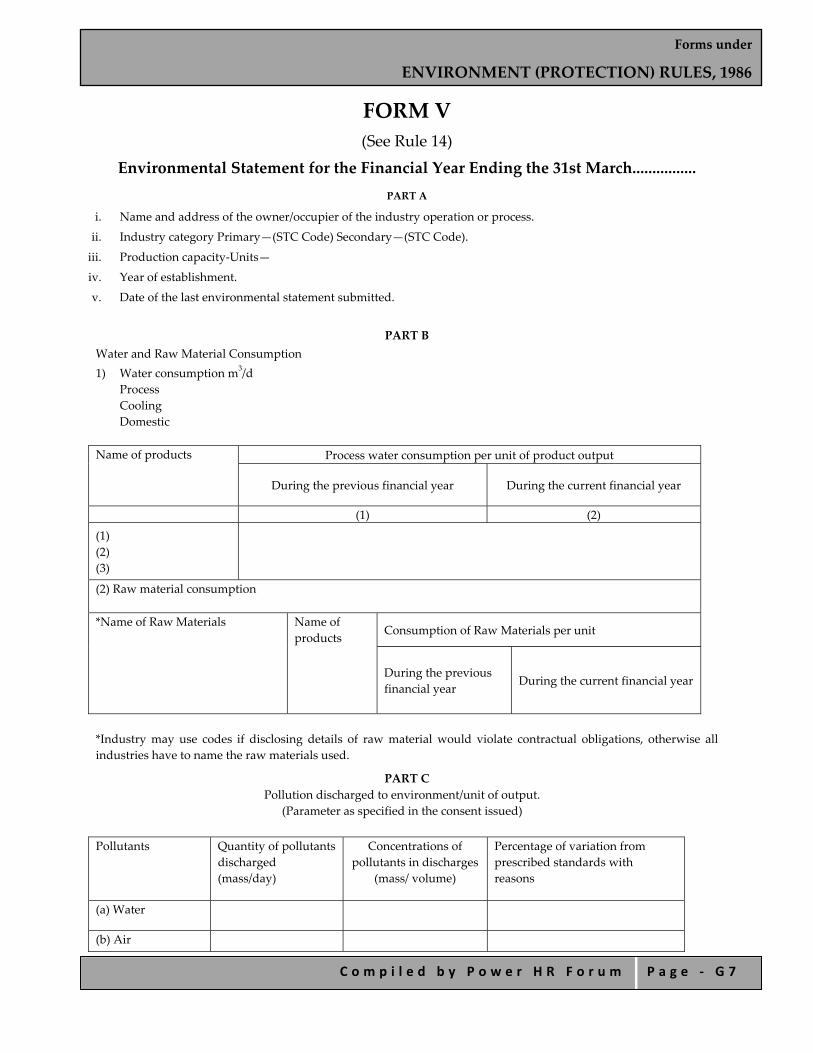
Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 7
FORM V (See Rule 14)
Environmental Statement for the Financial Year Ending the 31st March................ PART A
i. Name and address of the owner/occupier of the industry operation or process.
ii. Industry category Primary—(STC Code) Secondary—(STC Code).
iii. Production capacity‐Units—
iv. Year of establishment.
v. Date of the last environmental statement submitted.
PART B
Water and Raw Material Consumption 1) Water consumption m3/d
Process Cooling Domestic
Name of products Process water consumption per unit of product output
During the previous financial year During the current financial year
(1) (2)
(1) (2) (3)
(2) Raw material consumption *Name of Raw Materials Name of
products Consumption of Raw Materials per unit
During the previous financial year
During the current financial year
*Industry may use codes if disclosing details of raw material would violate contractual obligations, otherwise all industries have to name the raw materials used.
PART C Pollution discharged to environment/unit of output.
(Parameter as specified in the consent issued) Pollutants Quantity of pollutants
discharged (mass/day)
Concentrations of pollutants in discharges
(mass/ volume)
Percentage of variation from prescribed standards with reasons
(a) Water
(b) Air

Forms under
ENVIRONMENT (PROTECTION) RULES, 1986
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ G 8
PART D
Hazardous Wastes
(as specified under Hazardous Wastes (Management and Handling) Rules, 1989)
Hazardous Wastes Total Quantity (Kg)
During the previous financial year
During the current financial year
(a) From process (b) From pollution control facilities
PART E
Solid Wastes
Total Quantity
During the previous financial year
During the current financial year
(a) From process (b) From pollution control facility (c) 1. Quantity recycled or re‐utilized within the unit 2. Sold 3. Disposed
PART F
Please specify the characterization (in terms of composition and quantum) of hazardous as well as solid wastes and indicate disposal practice adopted for both these categories of wastes.
PART G
Impact of the pollution abatement measures taken on conservation of natural resources and on the cost of production.
PART H
Additional measures/investment proposal for environmental protection abatement of pollution, prevention of pollution.
PART I
Any other particulars for improving the quality of the environment.
—————
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1
Forms under the
DELHI FACTORY RULES, 1950

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2
INDEX
FORM 1
Application for Permission to Construct, Extend or take into Use any Building as a Factory
FORM 2 Application for Registration and Grant or Renewal of License for The Year and Notice of Occupation Specified in Sections 6 & 7
FORM 3 Notice of Change of Manager FORM 4
Licence to Work a Factory
FORMS 5 Certificate of Fitness Under Section 107 FORM 6 Humidity Register Under Rule 22 FORM. 7 Record of Lime Washing, Painting etc. Under Rule 16 FORM 7B Report of Examination of Hoist or Lift/ Occupier/ (or Owner) of
Premises Under Rule 55 FORM 8 Report of Examination of Pressure Vessel Under Rule 56 FORM 8A Report of Examination of Water‐Sealed Gasholder Under Rule 56a FORM 9 Register of Compensatory Holidays Under Rule 77 FORM 10 Overtime Muster Roll of Exempted Workers Under Rule 78 FORM 10(A) Overtime Slip for overtime Work Under Rule 78a FORM 11(A) Notice of Periods of Work for Adults Under Rule 79 FORM 11(B) Notice of Periods of Work for Adult Workers Under Rule 76 FORM 12 Register of Adult Workers Under Rule 80 FORM 13 Notice of Periods of Work for Child Workers Under Rule 85 FORM 14 Notice of Periods of Work for Child Workers Under Rule 86 FORM 15 Register of Leave With Wages Under Rule 87 & 88 FORM 16 Leave Book Under Rule 87 & 88 FORM 17 Health Register Under Rule 14 FORM 17A Test Report Of Dust Extraction System Under Rule 56a FORM 18
Notice of Accident or Dangerous Occurrence Resulting in Death or Bodily Injury Under Rule 96
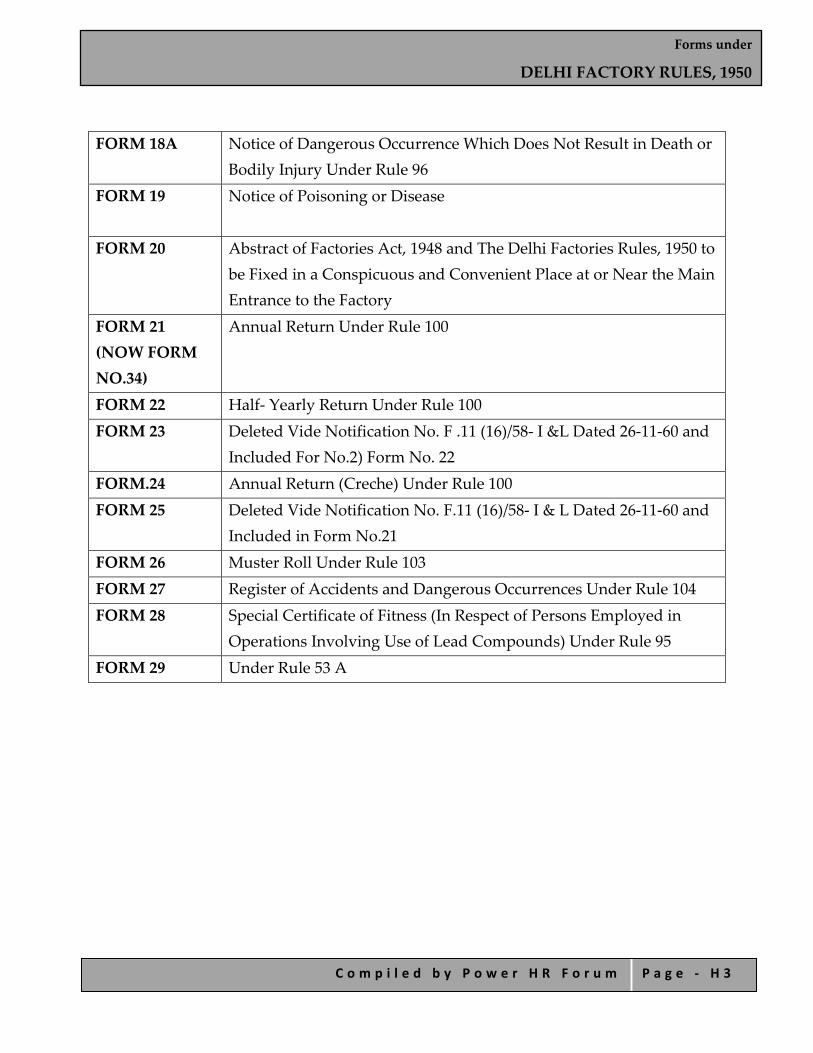
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3
FORM 18A
Notice of Dangerous Occurrence Which Does Not Result in Death or Bodily Injury Under Rule 96
FORM 19
Notice of Poisoning or Disease
FORM 20 Abstract of Factories Act, 1948 and The Delhi Factories Rules, 1950 to be Fixed in a Conspicuous and Convenient Place at or Near the Main Entrance to the Factory
FORM 21 (NOW FORM NO.34)
Annual Return Under Rule 100
FORM 22 Half‐ Yearly Return Under Rule 100 FORM 23 Deleted Vide Notification No. F .11 (16)/58‐ I &L Dated 26‐11‐60 and
Included For No.2) Form No. 22 FORM.24 Annual Return (Creche) Under Rule 100 FORM 25 Deleted Vide Notification No. F.11 (16)/58‐ I & L Dated 26‐11‐60 and
Included in Form No.21 FORM 26 Muster Roll Under Rule 103 FORM 27 Register of Accidents and Dangerous Occurrences Under Rule 104 FORM 28
Special Certificate of Fitness (In Respect of Persons Employed in Operations Involving Use of Lead Compounds) Under Rule 95
FORM 29 Under Rule 53 A
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4
FORM NO. 1 (Prescribed under Rule 3)
Application for Permission to Construct, Extend or Take Into Use any Building as a Factory
1. Applicantʹs Name.....................................................................
Applicantʹs Calling.....................................................................
Applicantʹs Address.....................................................................
2. Full Name & Postal address of factory.....................................................................
3. Situation of the factory‐.....................................................................
Province.....................................................................
District.....................................................................
Town or village.....................................................................
Nearest Police Station.....................................................................
Nearest Railway Station or Steamer Ghat.....................................................................
4. Particulars of plant to be installed.....................................................................
Signature of Applicant
Date.....................................................................
NOTE:‐ This application shall be accompanied by the following documents:
a. A flow chart of the manufacturing process supplemented by a brief description of the process in its various stages;
b. Plans, in duplicate, drawn to scale, showing :‐
i. the site of the factory and immediate surroundings including adjacent buildings and other structures, roads, drains etc. and
ii. the plan elevation and necessary cross‐sections of the various buildings, indicating all relevant details relating to natural lighting, ventilation and means of escape in case of fire. The plans shall also clearly indicate the position of the plant and machinery aisles and passage ways; and
c. Such other particulars as the Chief Inspector may require.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 5
FORM NO. 2 (Prescribed under Rule 4)
Application for Registration and Grant or Renewal of License for the Year and Notice of Occupation
Specified in Sections 6 & 7
1. Full name of the factory with factory licence No. if .......... already registered. 2.
a. Full Postal address and situation of the factory. ............ b. Full address to which communication relating to ................the factory should be sent.
3. Nature of manufacturing process/processes.
a. Carried on in the factory during the Last twelve months………………… (in the case of factories already in existence)
b. to be carried on in the factories during the next twelve months……………… (in the case of all factories)
4. Names and values of principal products manufactured during the last 12 months. 5.
i. Maximum number of workers proposed to be employed on anyone day during the year. ii. Maximum number of workers employed on any one day during the last 12 months. iii. Number of workers to be ordinarily employed in the factory.
6. i. Nature and total amount of power (H.P. installed or proposed to be installed). ii. Maximum amount of power (H.P.) proposed to be used.
7. Full name and residential address of the person who shall be the Manager of the factory for the purposes of the
Act. 8. Full name and residential address of the occupier:
i. The Proprietor of the factory in case of private firm/proprietory concern. ii. Directors in case of a public limited liability company/firm. iii. Where a Managing Agent has been appointed the name of Managing agents and Directors thereof. iv. Shareholders in case of a private company where no Managing Agent has been appointed. v. The Chief Administrative Head in case of a Government or local fund factory.
9. Full name and address of the owner of the premises or building (including the precincts thereof) referred to in
Section 93. 10. In case of factory constructed or extended after the date of the commencement of the Delhi Factories Rules, 1950.
a. Reference number and date of approval of the plans or construction or extension of factory by the Chief Commissioner /Chief Inspector.
b. Reference number and date of approval of the arrangements, if any made for the disposal of trade waste and effluents and the name of the authority granting such approval.
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 6
11. Amount of fee Rs........ (Rupees) ....... paid in ........Treasury on ........vide challan No ........ (enclosed
Signature of Occupier……… Date…………………………
Signature of Manager………..
Date………………………… Notes: 1. This form should be completed in ink in block letters or typed.
2. If power is not used at the time of filling up this form; but is introduced later; the fact should be communicated to the Chief Inspector immediately.
3. If any of the person named against item 8 is minor, the fact should be clearly stated.
4. In the case of a factory, where under the provision of sub‐sections 1 and 2 of Section 100, a person has been nominated as the occupier, information required in item 8 should be supplied only in respect of that person.
5. In the case of a factory where a managing Agent or Agents have been appointed as occupiers under the Indian Companies Act, 1913 VII of 1913), information required in item 8 should be supplied on y in respect of that person or persons.
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 7
FORM NO. 3 (Prescribed under Rule 12A)
Notice of Change of Manager
1. Name of factory with current license number....................................................................
2. Postal address....................................................................
3. Name of outgoing manager....................................................................
4. Name of new manager with postal address of his residence and telephone number, if installed....................................................................
5. Date of appointment of the new manager with parentage....................................................................]
Date Signature of new Manager Signature of Occupier Place

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 8
FORM NO. 4 (Prescribed under Rule 5) Licence to Work a Factory
Licence No............................... Reg. No............................... Date of Reg........................... Licence is hereby granted to..................................................... for premises known as .................................................. situated at.............................................. for use as a factory within the limits stated hereinafter, subject to provisions of the Factoryʹs Act, 1948, and the rules made there under :‐
The.................. 20 Issuing Authority
Valid for
Calendar Year
Maximum number of workers on any day
Maximum installed power capacity in
Fee Date of payment
Excess fee of late payment
Date of payment
signature of the Issuing Authority
Granted under Rule 5
Renewed under Rule 7
…………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………..
…………………………………………………………………………………………………………………………………………………………..
TRANSFERS
To whom transferred Year of transfer Date of payment of transfer fee Signature of the Issuing Authority

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 9
AMENDMENTS
Year When amended
Workers Installed power capacity in H.P
Date of payment of amendment fee
Additional fee Date of fee Signature of the issuing Authority
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 0
FORM NO. 5 Rule prescribed under Section 107
Certificate of Fitness 1. Serial No...............................................................
Date………………………………………………
2. Name ...................................................................
3. Fatherʹs Name .....................................................
4. Sex .......................................................................
5. Residence ............................................................
6. *Date of Birth, if available and / or age Certified
............................................................................
7. Physical Fitness ......................................................
8. Descriptive marks ...............................................
................................................................................
................................................................................
................................................................................
9. Reason for –
1. Refusal of certificate .......................................
…………………………………………………..
2. Certificate being revoked ...............or............
................................................................................
................................................................................
................................................................................
Initials of Certifying Surgeon Certifying Surgeon
Note;‐ Exact details of cause of physical disability should be clearly stated.
* Vide Notification No. F.1(135)/53‐I & L (ii) dated 25 th June, 1957 .
Serial No.........................................................
Date……………………………………………………………
I hereby certify that I have personally examined Name................................................
.........................................................................
.........................................................................
Son/ Daughter ........................................................
.........................................................................
.........................................................................
who is desirous of being employed in a factory, and that his / her age, as nearly as can be as certained from my examination, is .................. years; and that he/ she is fit for employment in factory as an adult / child.
His / her descriptive marks are ...............................
.........................................................................
.........................................................................
Thumb impression Thumb impression
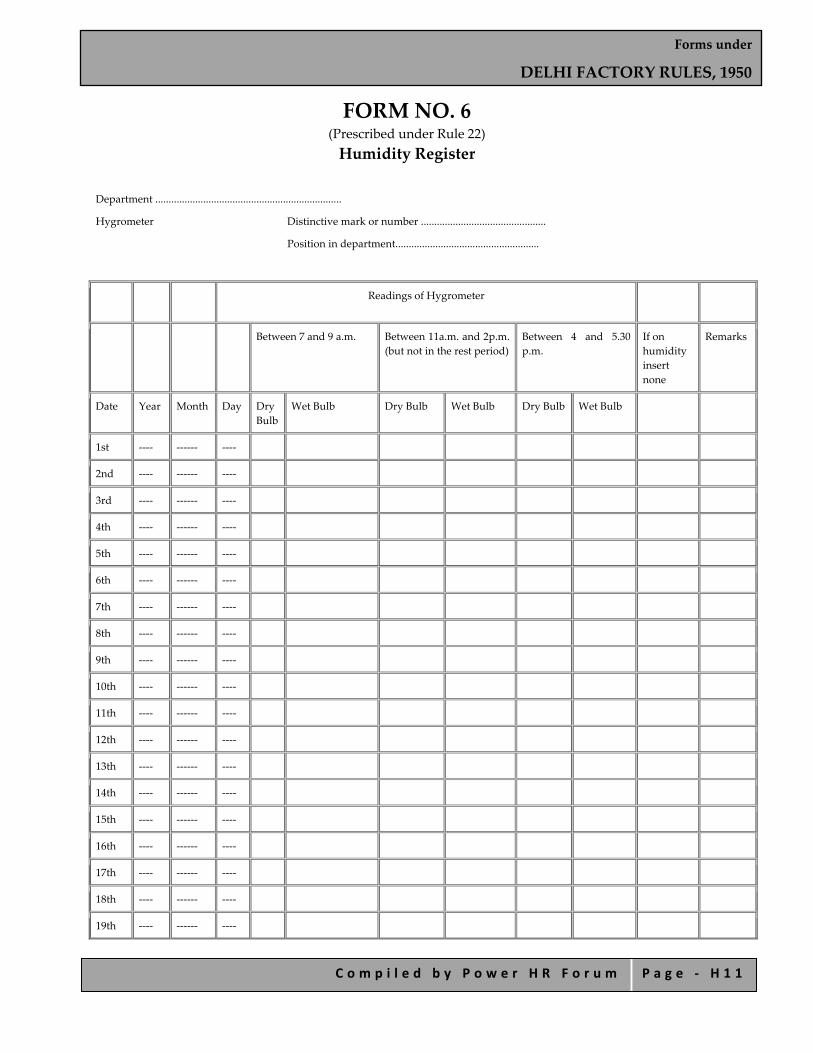
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 1
FORM NO. 6 (Prescribed under Rule 22) Humidity Register
Department ......................................................................
Hygrometer Distinctive mark or number ...............................................
Position in department......................................................
Readings of Hygrometer
Between 7 and 9 a.m. Between 11a.m. and 2p.m. (but not in the rest period)
Between 4 and 5.30 p.m.
If on humidity insert none
Remarks
Date Year Month Day Dry Bulb
Wet Bulb Dry Bulb Wet Bulb Dry Bulb Wet Bulb
1st ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
2nd ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
3rd ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
4th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
5th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
6th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
7th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
8th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
9th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
10th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
11th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
12th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
13th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
14th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
15th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
16th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
17th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
18th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
19th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 2
20th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
21st ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
22nd ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
23rd ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
24th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
25th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
26th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
27th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
28th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
29th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
30th ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
31st ‐‐‐‐ ‐‐‐‐‐‐ ‐‐‐‐
(Signed) .....................................................
Certified that the above entries are correct
(signed) ....................................................

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 3
FORM NO. 7 (Prescribed under Rule 16)
Record of Lime washing, Painting etc.
Part of factory e.g. name of room
Parts lime‐washed, painted, varnished or oiled e.g. walls, ceiling, wood work etc.
Treatment, whether lime‐washed, painted varnished or oiled
Date on which lime‐washing, painting varnishing or oiling was carried out (according to the English calendar)
Remarks
Date Month Year
1 2 3 4 5 6 7

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 4
FORM NO. 7B (Prescribed under Rule 55)
Prescribed for Report of Examination of Hoist or Lift/ Occupier/ (or owner) of Premises
Address:
1.
a. Type of hoist or lift and Identification number or description.
b. Date of construction or re‐construction (if ascertainable).
2. Design and construction.
Are all parts of the hoist or life of good mechanical construction sound material and adequate strength (so as ascertainable).
3. Maintenance.
Are the following parts of the hoist or lift properly maintained and in good working order, If not, state what defects have been found :‐
a. Enclosure of hoistway or liftway. b. Landing gates and cage gate(s). c. Interlocks on the landing gates and cage gate(s). d. Other gates fastenings. e. Cage and platform and fittings guides, buffers, interior of the hoistway or liftway. f. Over‐running devices. g. Suspension ropes or chain and their attachments. h. Safety gear, i.e. arrangements for preventing fall of platform or cage brakes. i. Brakes. j. Worm or super gearing. k. Other electrical equipment. l. Other parts.
4. What parts (if any were) inaccessible.
5. Repairs, renewals or alterations (if any) required and the period with which they should be executed.
6. Maximum safe working load subject to repairs, renewals or alterations (if any) specified in (5).
7. Others.
I/We verify that on .......................I/We thoroughly examined this hoist of life and that above is correct report of the result.
Signature............. Counter signature...........
If employed by a company or association give names and address.
Qualification ........................................................... Address.................................................................. Date ................................
Date .............................
Note:‐Details of any renewal or alterations required should be given in 5 above.
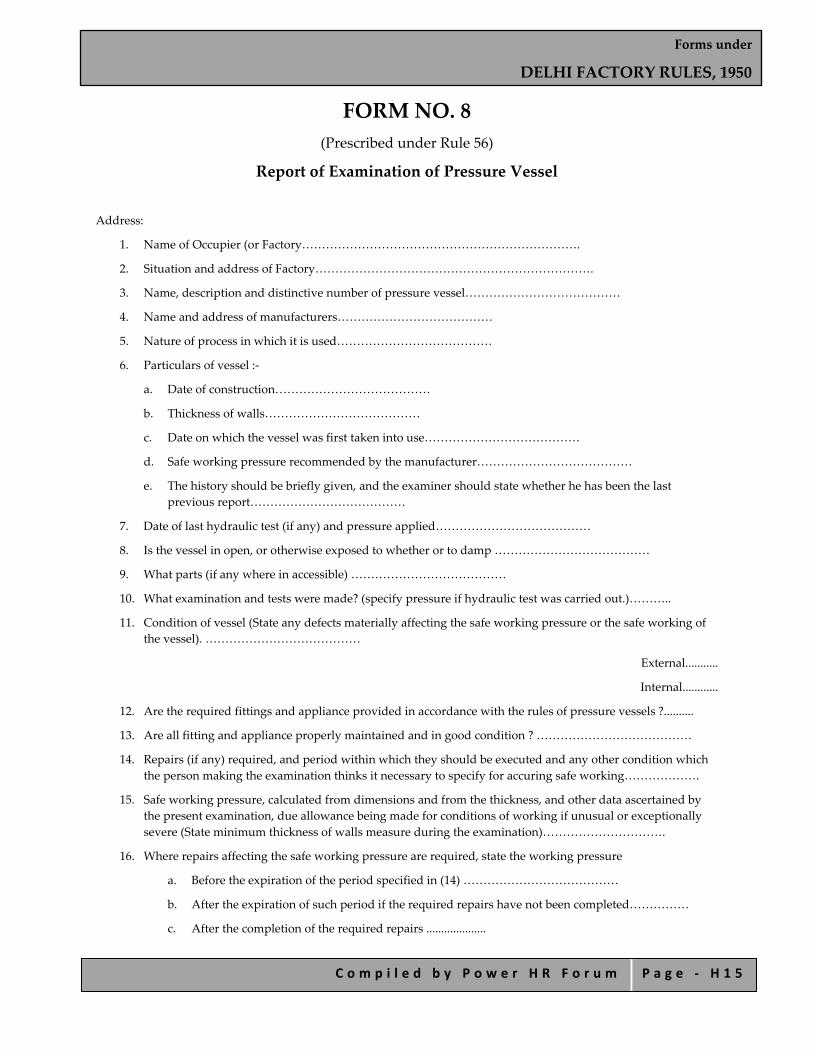
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 5
FORM NO. 8 (Prescribed under Rule 56)
Report of Examination of Pressure Vessel
Address:
1. Name of Occupier (or Factory…………………………………………………………….
2. Situation and address of Factory…………………………………………………………….
3. Name, description and distinctive number of pressure vessel…………………………………
4. Name and address of manufacturers…………………………………
5. Nature of process in which it is used…………………………………
6. Particulars of vessel :‐
a. Date of construction…………………………………
b. Thickness of walls…………………………………
c. Date on which the vessel was first taken into use…………………………………
d. Safe working pressure recommended by the manufacturer…………………………………
e. The history should be briefly given, and the examiner should state whether he has been the last previous report…………………………………
7. Date of last hydraulic test (if any) and pressure applied…………………………………
8. Is the vessel in open, or otherwise exposed to whether or to damp …………………………………
9. What parts (if any where in accessible) …………………………………
10. What examination and tests were made? (specify pressure if hydraulic test was carried out.)………..
11. Condition of vessel (State any defects materially affecting the safe working pressure or the safe working of the vessel). …………………………………
External...........
Internal............
12. Are the required fittings and appliance provided in accordance with the rules of pressure vessels ?..........
13. Are all fitting and appliance properly maintained and in good condition ? …………………………………
14. Repairs (if any) required, and period within which they should be executed and any other condition which the person making the examination thinks it necessary to specify for accuring safe working……………….
15. Safe working pressure, calculated from dimensions and from the thickness, and other data ascertained by the present examination, due allowance being made for conditions of working if unusual or exceptionally severe (State minimum thickness of walls measure during the examination)………………………….
16. Where repairs affecting the safe working pressure are required, state the working pressure
a. Before the expiration of the period specified in (14) …………………………………
b. After the expiration of such period if the required repairs have not been completed……………
c. After the completion of the required repairs ....................

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 6
17. Other observations.............................
I certify that on ...................... the pressure vessel described above was thoroughly cleaned and (so far as its construction permits) made accessible for thorough examination and for such tests as were necessary for thorough examination and that on the said date, I thoroughly examined this pressure vessel including its fittings, and that the above is a true report of my examination.
Signature ....................
Qualification ..................
Address ......................
Date ........................
If employed by a Company or Association................................................ give name and address.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 7
FORM NO. 8A (Prescribed under Rule 56A)
Report of Examination of Water‐Sealed Gasholder 1. Name of Occupier of Factory
2. Situation and address of Factory
3. Name, description, distinguishing number or letter and type of gasholder.
4. Name and address of the manufacturer.
5.
a. No. of lifts.
b. Maximum capacity in cub‐meters (cub. ft.)
c. Pressure thrown by holder when full of gas.
6. Particulars of gas to be stored in the holder.
7. Particulars as to be condition of‐
a. Crown
b. Side sheeting, including grips and cups.
c. Guiding Mechanism (Roller carriages, rollers, pins, guide rails or ropes.).
d. Tank.
e. Other structure, if any (columns, framing and bracing).
8. Particulars as to position of the lifts at the time of examination.
9. Particulars as to whether the tank and lifts were found sufficiently level for safe working and if not, as to the steps taken to remedy the defect.
10. Date of examination and by whom it was carried out.
11. Condition of vessel
1. External
2. Internal
12. Are all fittings, appliances properly maintained and in a good condition, repairs, if any, required and period within which they should be executed and any other condition which the person making the examination thinks it necessary for safe working.
13. Other observations.
I certify that on…………………the gasholder described above was thoroughly examined and such of the tests as were necessary made on the same day and that the above is a true report of my examination.
Signature ....................
Qualification ..................
Address ......................
Date ........................
If employed by a Company or Association................................................ give name and address.
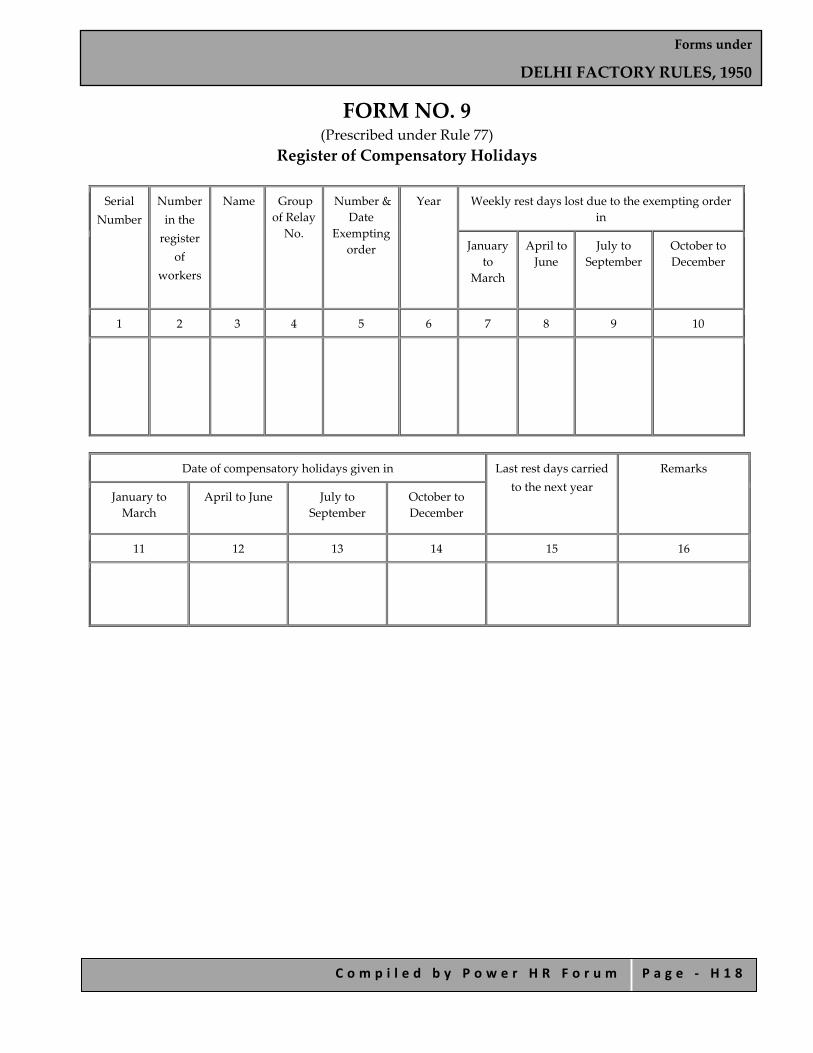
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 8
FORM NO. 9 (Prescribed under Rule 77)
Register of Compensatory Holidays Serial
Number Number in the register
of workers
Name Group of Relay No.
Number & Date
Exempting order
Year Weekly rest days lost due to the exempting order in
January to
March
April to June
July to September
October to December
1 2 3 4 5 6 7 8 9 10
Date of compensatory holidays given in Last rest days carried to the next year
Remarks
January to March
April to June July to September
October to December
11 12 13 14 15 16

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 1 9
FORM NO. 10 (Prescribed under Rule 78)
Overtime Muster Roll Exempted Workers Month ending..........20..
No. in Register Name Department Dates on which overtime has been worked
Extent of overtime on each occasion
Total overtime worked or
production in case of piece workers
Normal Hours
1 2 3 4 5 6 7
Normal rate
of Pay Overtime rate of
pay Normal earning
Overtime earning
* Cash equivalent of advantage accruing
through the concessional sale of food grains and other
articles
Total earning Dates on which overtime
payments made
8 9 10 11 12 13 14

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 0
FORM NO. 10(A) (Prescribed under Rule 78A)
Overtime Slip for Overtime Work
Month ending..................20…
No. in Register Name Department Dates on which overtime work has been done
Extent of C.T. work on each date
Total C.T. work or prdts in case
of piece workers
Normal Hours
1 2 3 4 5 6 7
Normal rate of Pay
Overtime rate of pay Normal earning Overtime earning Total earning Dates on which overtime payments
made
8 9 10 11 12 13
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 1
FORM NO. 11(A) (Prescribed under Rule 79)
Notice of Periods of Work for Adults Name of Factory ...........
Where Situated............
On ordinary working days……….
Hours of starting work..........
Hours of closing work..........
(Signed) ............
Period of rest interval From ...... To ......... Manager
On half working days .........
Hours of starting work........
Hour of closing work.........
Date on which notice first exhibited....
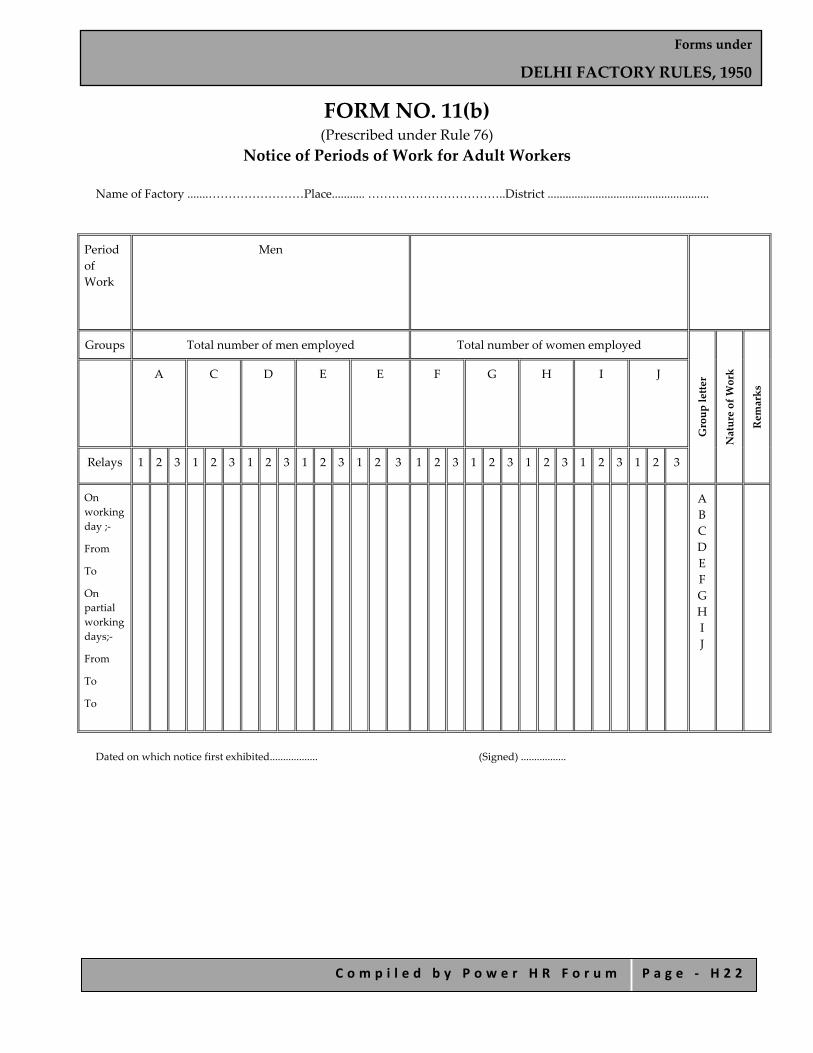
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 2
FORM NO. 11(b) (Prescribed under Rule 76)
Notice of Periods of Work for Adult Workers Name of Factory .......……………………Place........... ……………………………..District ......................................................
Period of Work
Men
Groups Total number of men employed Total number of women employed
Group letter
Nature of Work
Remarks A C D E E F G H I J
Relays 1 2 3 1 2 3 1 2 3 1 2 3 1 2 3 1 2 3 1 2 3 1 2 3 1 2 3 1 2 3
On working day ;‐
From
To
On partial working days;‐
From
To
To
A B C D E F G H I J
Dated on which notice first exhibited.................. (Signed) .................

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 3
FORM NO. 12 (Prescribed under Rule 80) Register of Adult Workers
Serial No.
Name Fatherʹs Name
Residential Address
Nature of Work
Letter of
group as in Form No.
Number of relay, if
working in shifts
Number and date of Certificate, if an adolescent
Number of Certificate and Date
Token Number giving
reference to the
Certificate
Remarks
1 2 3 4 5 6 7 8 9 10

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 4
FORM NO. 13 (Prescribed under Rule 85)
Notice of Periods of Work for Child Workers Name of Factory ..........................................................Place ....................................................District .........................................
Periods of Work
Children
Total number of children employed
Description of groups
Groups A B C
Relays 1 2 1 2 1 2 Group Letter
Nature of Work
Remarks
From .......
To ........
Dated on which this notice is first exhibited ............
Manager (Signed) ..............
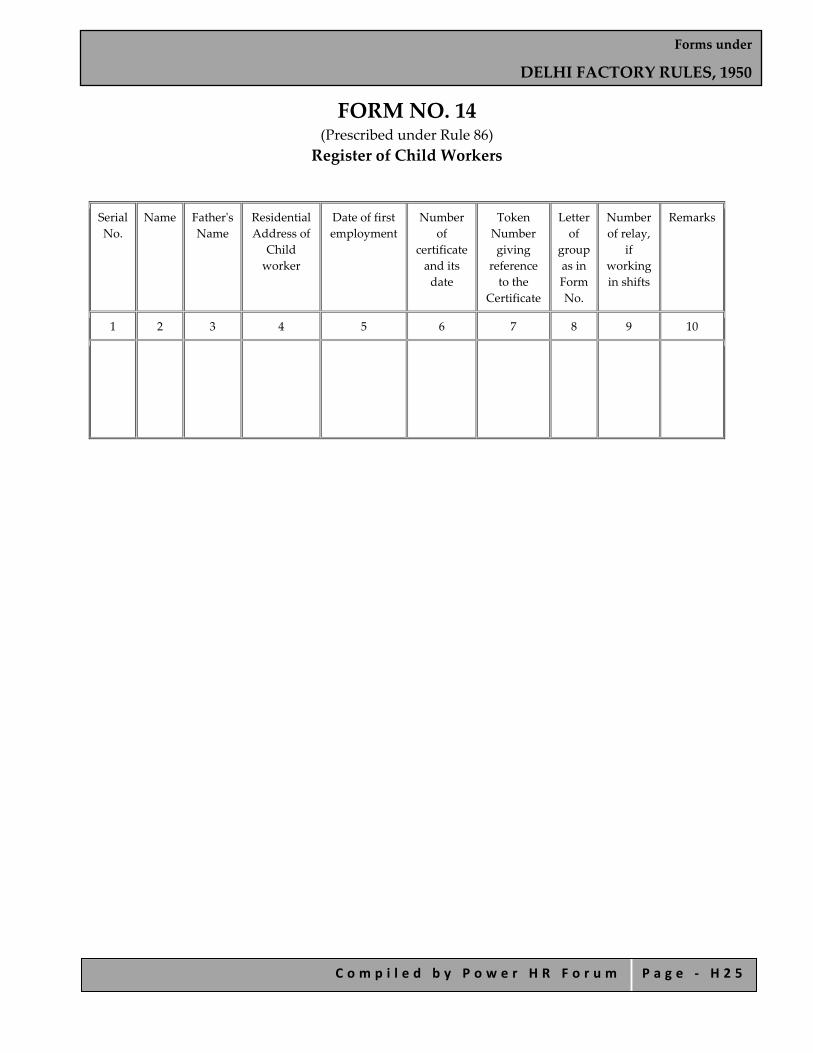
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 5
FORM NO. 14 (Prescribed under Rule 86) Register of Child Workers
Serial No.
Name Fatherʹs Name
Residential Address of
Child worker
Date of first employment
Number of
certificate and its date
Token Number giving
reference to the
Certificate
Letter of
group as in Form No.
Number of relay,
if working in shifts
Remarks
1 2 3 4 5 6 7 8 9 10
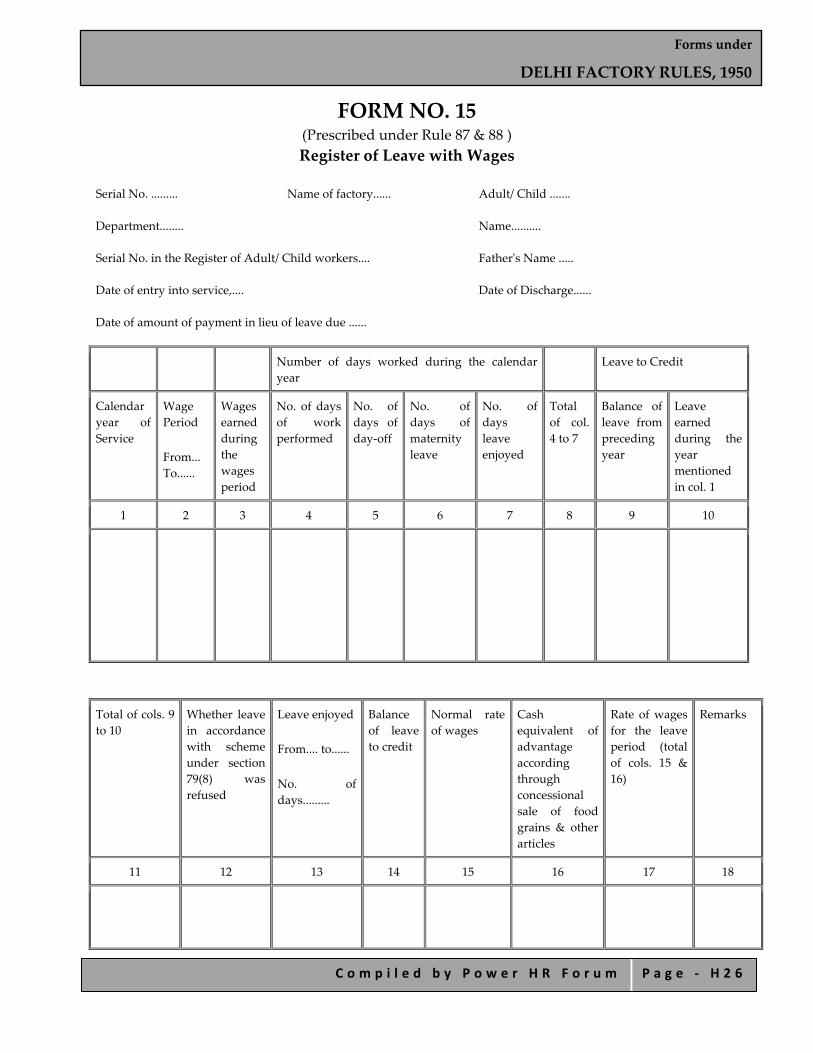
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 6
FORM NO. 15 (Prescribed under Rule 87 & 88 ) Register of Leave with Wages
Serial No. ......... Name of factory...... Adult/ Child .......
Department........ Name..........
Serial No. in the Register of Adult/ Child workers.... Fatherʹs Name .....
Date of entry into service,.... Date of Discharge......
Date of amount of payment in lieu of leave due ......
Number of days worked during the calendar year
Leave to Credit
Calendar year of Service
Wage Period
From... To......
Wages earned during the wages period
No. of days of work performed
No. of days of day‐off
No. of days of maternity leave
No. of days leave enjoyed
Total of col. 4 to 7
Balance of leave from preceding year
Leave earned during the year mentioned in col. 1
1 2 3 4 5 6 7 8 9 10
Total of cols. 9 to 10
Whether leave in accordance with scheme under section 79(8) was refused
Leave enjoyed
From.... to......
No. of days.........
Balance of leave to credit
Normal rate of wages
Cash equivalent of advantage according through concessional sale of food grains & other articles
Rate of wages for the leave period (total of cols. 15 & 16)
Remarks
11 12 13 14 15 16 17 18

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 7
FORM NO. 16 (Prescribed under Rule 87 & 88 )
Leave Book Shall be the same as Register of Leave with Wages (Form No. 15 but shall be made out separately for each worker on a thick bound sheet)

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 8
FORM NO. 17 (Prescribed under Rule 14)
Health Register (In respect of persons employed in occupations declared to be dangerous operations under Section 87) Name of Certifying Surgeon :
a. Shri ............. From ......... To...........
b. Shri ............. From ......... To...........
c. Shri ............. From ......... To...........
Serial No.
Work No.
Name of Worker
Sex Age (last birthday)
Date of employment on present work
Date of leaving or transfer to other work
Reason for leaving transfer or discharge
1 2 3 4 5 6 7 8
Nature of Job or
occupation
Raw material or Byproduct handled
Dates of medical Examination by
Certifying Surgeon
If suspended from work,
state period of suspension with detailed
reasons.
Recertified fit to resume
duty on (with signature of Certifying Surgeon)
If certifying of unfitness or suspension issued t o worker
Signature with date of Certifying Surgeon
Results of medical examination
9 10 11 12 13 14 15
Note :‐
i. Column 8. Detail summery of reasons for transfer or discharge should be stated. ii. Column 11. Should be expressed as fit/ unfit/ suspended.
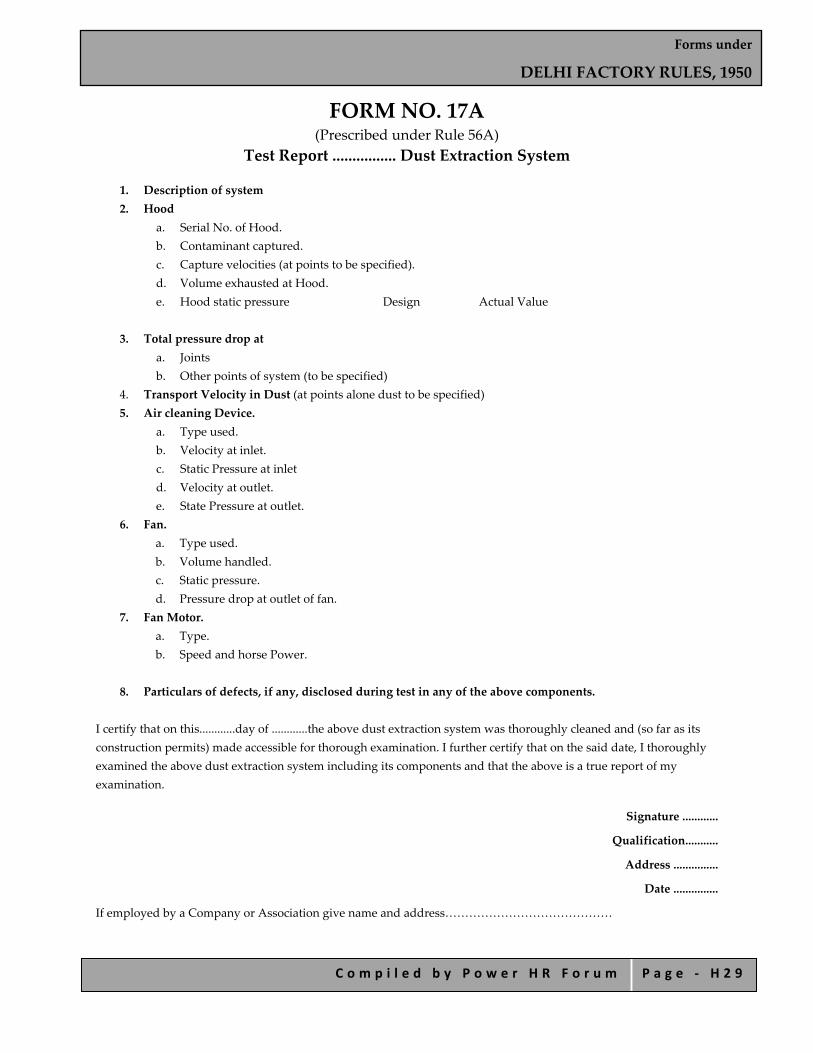
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 2 9
FORM NO. 17A (Prescribed under Rule 56A)
Test Report ................ Dust Extraction System
1. Description of system 2. Hood
a. Serial No. of Hood. b. Contaminant captured. c. Capture velocities (at points to be specified). d. Volume exhausted at Hood. e. Hood static pressure Design Actual Value
3. Total pressure drop at
a. Joints b. Other points of system (to be specified)
4. Transport Velocity in Dust (at points alone dust to be specified) 5. Air cleaning Device.
a. Type used. b. Velocity at inlet. c. Static Pressure at inlet d. Velocity at outlet. e. State Pressure at outlet.
6. Fan. a. Type used. b. Volume handled. c. Static pressure. d. Pressure drop at outlet of fan.
7. Fan Motor. a. Type. b. Speed and horse Power.
8. Particulars of defects, if any, disclosed during test in any of the above components.
I certify that on this............day of ............the above dust extraction system was thoroughly cleaned and (so far as its construction permits) made accessible for thorough examination. I further certify that on the said date, I thoroughly examined the above dust extraction system including its components and that the above is a true report of my examination.
Signature ............
Qualification...........
Address ...............
Date ...............
If employed by a Company or Association give name and address……………………………………
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 0
FORM NO. 18 (Prescribed under Rule 96)
Notice of Accident or Dangerous Occurrence Resulting in Death or Bodily Injury
(To be sent forthwith to the Inspector of Factories) (See Instruction below)
This space to be completed by Inspector of Factories
District……………………………
Date of Receipt……………………………………..
Number of Accident or dangerous Occurrences…………………………….
Industry No………………………………….
Causation No………………………………………………
Sex (M.W.B., or G)…………………………………………..
Other particulars (e.g. fatel, leg injury, arm injury etc.)…………………………………….
Date of Investigation……………………………………………
Result of Investigation……………………………………………
1. Name of Factory
2. Address of Works where accident or dangerous occurrence happened
3. Nature of Industry
4. Branch or Department and exact place where the accident or dangerous, occurrence happened.
5. Injured personʹs name and address
6.
a. Sex
b. Age (last birthday and)
c. Occupation of injured person
7. Date and hour of accident or dangerous occurrence
8. Hour at which he started work on day of accident or dangerous occurrence.
9.
a. Cause or nature of accident or dangerous occurrence (a)
b. If caused by machinery:
i. Give name of the machine and part causing the accident or dangerous occurrence, and (b) (i)
ii. State whether it was moved by mechanical power at the time (b) (ii).
c. State exactly what injured person was doing at the time (e)
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 1
10. Nature and extent of injuries (e.g.) fatel, loss of finger, fracture of leg, scald, scratch followed by ...............................................Sepsis ..................................................
11. If accident or dangerous occurrence is not fatal, state whether injured person was disabled for 48 hour or more ...............................
12. Name of medical officers in attendance or injured person.
I Certify that to the best of my knowledge and belief the above particulars are correct in every respect.
Signature of Occupier or Manage
Date of despatch of report…………..
Note: ‐ To be completed in legible handwriting or preferably typewritten.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 2
EXTRACT FROM THE FACTORIES Act, 1948
Notice Certain Accidents (Section 88)
1. Where in any factory an accident occurs which causes death, or which cause any bodily injury by reason of which the person injured is prevented from working for a period of forty‐eight hours or more immediately following the accident, or which is of such nature as may be prescribed in this behalf, the manager of the factory shall send notice thereof to such authorities, and in such form and within such time, as may be prescribed.
2. Where a notice given under sub‐section (1) relates to an accident causing death, the authority to whom the notice is sent shall make an inquiry into the occurrence within one month of the receipt of the notice or, if such authority is not the Inspector cause the Inspector, to make an inquiry within the said period
3. The State Government may make rules for regulating the procedure at inquiries under this section.
EXTRACT FROM DELHI F ACTORIES, RULES 1950
(Rule 96 prescribed under Sections 38 and 88‐A)
1. When any accident which results in the death of any person or which result in such bodily injury to any person as is likely to cause his death or any dangerous occurrence specified in the Schedule takes place in a factory, the manager of the factory shall forthwith send a notice thereof by telephone, special messenger or telegram to the Inspector and the Chief Inspector.
2. When any accident or any dangerous occurrence specified in the Schedule, which results in the death of any person or which result in such bodily injury to any person as is likely to cause his death, takes place in a factory, notice as mentioned in sub‐rule (i) shall be sent also to :‐
a. the District Magistrate or sub‐Divisional Officer.
b. the officer‐in‐charge of the nearest police station, and
c. the relatives of the injured or deceased person.
3. Any notice given as required under sub‐rules (1) and {2) shall be confirmed by the manager of the factory to the authorities mentioned in these sub‐rules within 12 hours of the accident or the dangerous occurrence by sending the written report in Form No.18 in the case of an accident or dangerous occurrence causing death or bodily injury to any person and in Form 18‐A in the case of dangerous occurrence which has not resulted in any bodily injury to any person.
4. When any accident or dangerous occurrence specified in the Schedule takes place in a factory and it causes such bodily injury to any person as prevents the person injured from working for a period of 48 hours or more immediately following the accident or the dangerous occurrence, as the case may be, the manager of the factory shall send a report thereof to the Inspector in Form No.18 within 24 hours after the expiry of 48 hours from the time of the accident or the dangerous occurrence.
Provided that if in the case of any accident or dangerous occurrence, death occurs of any person injured by such accident or dangerous occurrence after the notices and reports referred to in the foregoing sub‐rules have been sent the manager of the factory shall forthwith send a notice thereof by telephone, special messenger or
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 3
telegram to the authorities and persons mentioned in sub‐rules (1) and (2) and also have this information confirmed in writing within 12 hours of the death.
Provided further, that, if the period of disability from working for 48 hours or more referred to in sub‐rule (4) does not occur immediately following the accident, or the dangerous occurrence, but later on occurs in more than one spell, the report referred to shall be sent to the Inspector in the prescribed form 18 within 24 hours immediately following the hour when the actual total period of disability from working resulting from the accident or the dangerous occurrence becomes 48 hours.
SCHEDULE
The following classes of dangerous occurrence, whether or not they are attended by personal injury disablement:
a. Bursting of a plant used far containing or supplying steam under pressure greater than atn1ospheric pressure.
b. Collapse or failure of a crane, derrick, which hoist or other appliances used in raising or lowering persons or goods, or any part thereof, or the overturning of a crane.
c. Explosion. fire, bursting out, leakage or escape of any molten metal, or hot liquor or gas causing bodily injury to any person or damage to any room or place in which persons are employed, or fire in rooms of cotton pressing factories when a cotton opener is in use.
d. Explosion of a receiver or container used for the storage at a pressure greater than atmospheric pressure of any gas or gases (including air) or any liquid or solid resulting from the compression of gas.
e. Collapse or subsidence of any floor, gallery, roof, bridge, tunnel, chimney, wall, building or any other structure.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 4
FORM NO. 18A (Prescribed under Rule 96)
Vide para 2 of Schedule Under Rule 96) (Notice of Dangerous Occurrence which does not Result in Death or Bodily injury)
1. Name and address of the factory
2. Name of the Occupier
3. Name of the Manager
4. Nature of Industry
5. Branch or Department and exact place where the dangerous occurrence took place
6. Date and Hour of occurrence
(State exactly what happened)
I certify that, to the best of knowledge and belief the above particulars are correct in every respect.
Note:‐ To be completed in legible handwriting or preferably typewritten. (This space to be completed by Inspector of Factories).
District Date of receipt
D.O.No.
Date of Investigation
Causation No.
Result of Investigation

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 5
FORM NO.19 (Prescribed under Rule 97)
Notice of Poisoning or Disease
(See Instruction on reverse)
Factory Particulars
Person Affected
General Particulars
1. Name of Factory
2. Address of factory
3. Address of office or private residence of occupier
4. Nature of industry
5. Name and Works Number of Patient
6. Address of Patient
7. Sex and Age of Patient
8. Precise occupation of Patient
9. Nature of Poisoning or Disease from which patient is suffering
10. Has the case been reported to the Certifying Surgeon
Signature of Factory Manager
Dated
To be filled in by the Chief Inspector, No. of case Remarks

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 6
NOTICE OF POISONING DISEASE
Extract from the Factories Act, 1948
(Section 89)
Where any worker in a factory contracts any disease specified in the Schedule, the manager of the factory shall send notice thereof to such authorities, and in such form and within such time, as may be prescribed.
Extract from Delhi Factory Rules,1950
(Rule 97)
A notice in Form No. 19 should be sent forthwith both to the Chief Inspector and to the Certifying Surgeon, by the Manager of a factory in which there occurs a cast lead, phosphorous, mercury, manganese, arsenic, carbon disulphide or benzene poisoning or poisoning by nitrous fumes, or by halogens or halogen derivatives of the hydrocarbon of aliphatic series, or of chrome ulceration, anthrax silicosis, toxic anaemia, toxic jaundice, primary optheliomatous cancer of the skin or pathological manifestations due to radium or other radio active substance or X‐rays.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 7
FORM NO. 20 (Prescribed under Rule No.99)
Abstract of Factories Act, 1948 and The Delhi
Factories Rules, 1950
(To be fixed in a conspicuous and convenient place at or near the main entrance to the factory)
Interpretation
ʺFactoryʺ means any premises including the precincts thereof‐
i. whereon ten or more workers are working, or were working on any day of the preceding twelve months, and in any part of which a manufacturing process is being carried on with the aid of power, or is ordinarily so carried on, or
ii. whereon twenty or more workers are working or were working on any day of the preceding twelve months, and in any part of which a manufacturing process is being carried on without the aid of power, or is ordinarily so carried on, but does not include a mine subject to the operation of the Indian Mines Act, 1923 (IV of 1923), or a railway running shed.
ʺWorkerʺ means a person employed, directly or through any agency, whether for wages or not in any manufacturing process or in cleaning any part of the machinery or premises used for a manufacturing process in any other kind of work incidental to, or connected with the manufacturing process, or the subject of the manufacturing process.
ʺManufacturing processʺ means any process for making, altering, repairing ornamenting, finishing, packing, oiling, washing, cleaning, breaking up, demolishing, or otherwise treating or adopting any article or substance with a view to its, sale, transport, delivery or disposal, or pumping oil, water or sewage, or generating, transforming power or composing types for printing, printing by letter press, lithography, photogravure or other similar processes or book binding or constructing reconstructing, repairing, refitting, finishing or breaking up ships or vessels.
Working hours, holidays, intervals for rest, etc.
1. Hours of work (Adults). Sections 51 and 54‐ No Adult worker shall be required, or allowed to work in a factory for more than 48 hours in any week and for more than 9 hours in any day, or with the previous approval of the Chief Inspector, the daily maximum specified in Sec. 51 may be exceeded in order to facilitate the change of shifts.
2. Relaxation of hours of Work (Adults). Section 64‐ The ordinary limits on working hours of adults may be relaxed in certain special cases, e.g. workers engaged on urgent repairs; in preparatory or complementary work which must necessarily be carried on outside the limits laid down for the general working of the factory, in work which is necessarily so intermittent that the intervals during which they do not work while on duty ordinarily amount to more than the intervals for rest in work which for technical reasons must be carried on continuously throughout the day; in making or supplying articles of prime necessity which must be made or supplied every day; in a manufacturing process which cannot be carried on except during fixed seasons, or at times dependent on the irregular action of natural forces in engine rooms or boiler houses or in attending to power plant or transmission machinery, or in printing of news paper held upon account of the breakdown of machinery, or the loading or unloading of railway wagons.
Except in the case of urgent repairs, the relaxation shall not exceed the following limits‐
i. the total number of hours of work in any day shall not exceed ten;
ii. the total number of hours of overtime work shall not exceed 50 for anyone quarter;

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 8
iii. the spread over inclusive of intervals for rest shall not exceed 12 hours in anyone day.
In the case of any or all adult workers in any factory, the ordinary limits on working hours of adults may be relaxed, for a period or periods not exceeding in the aggregate 3 months in any year, to enable the factory to deal within exceptional press of work.
3. Payment for Overtime. Section 59‐ Where a women works in a factory for more than 9 hours in any day or for more than 48 hours in any week he shall, in respect of overtime work, be entitled to wages at the rate of twice his ordinary rate wages.
4. Exemption of supervisory Staff. Section 64‐ Chapter VI of the Act‐ Working hours of adults‐does not apply to persons holding position in a factory.
5. Weekly Holiday (Adult). Section 52‐ No adult worker shall be required or allowed to work in a factory on the first day of the week unless he has, or will have, a holiday for a whole day on one of the three days immediately before or after the said day, and the manager of the factory has, before the said day or the substituted day, whichever is earlier, delivered a notice at the office of the Inspector of his intention to require the worker to work on the said day and of the day which is to be substituted, and displayed a notice to that effect in the factory.
Provided that no substitution shall be made which will result in any worker working for more than ten days consecutively without a holiday for a whole day.
Where a worker in a factory, as a result of exemption from the ordinary provision relating to weekly holidays is, deprived of any of the weekly holidays he shall be allowed, within the month in which the holidays were due to him or within the two months immediately following that month compensatory holidays of equal number of the holidays so lost.
6. Intervals for Rest (Adults). Sections 55 and 56‐ The periods of work of adult workers in a factory each day shall be so fixed that no period shall exceed 5 hours before he has had an interval for rest of at least half hour and that inclusive of his intervals for rest they shall not spread over more than 10 hours in any day or, with the permission of the Chief Inspector in writing, 12 hours.
7. Prohibition of Double Employment. Sections 60,71 and 99‐ No child or, except in certain circumstances an adult worker, shall be required or allowed to work in any factory on any day on which he has already been working in any other factory.
If a child works in a factory on any day on which he has already been working in another factory, the parent or guardian of the child or the person having custody of or control over him or obtaining any direct benefit from his wages shall be punishable with fine, which may extend to Rs. 50 unless it appears to the court that the child so worked without the consent or connivance of such parent, guardian or person.
8. Prohibition of Employment of Children under 14 Section 67‐ No child who has not completed his fourteenth year shall be required or allowed to work in any factory.
9. Hours of Work (Children). Section 71‐Nochild shall be employed or permitted to work in any factory for more than 4‐1/2 hours in any day and between the hours of 7 P.M. and 6 A.M. The period of work of all children employed in a factory shall be limited to two shifts which shall not overlap or spread over more than 5 hours each and each child shall be employed in only one of relays

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 3 9
The provision relating to weekly holidays shall also apply to child workers and no exemption from this provision may be granted in respect of any child.
10. Prohibition of Employment of Women. Section 66‐ No Woman shall in any circumstances be employed in any factory more than 9 hours in any day or between the hours of 7 P.M. and 6 A.M. There shall be no change of shifts except after a weekly holiday or any other holiday.
Leave with wages
11. Leave with Wages. Section 79 and 80/83 and Rules‐ Every worker who has worked for a period of 240 days or more in a factory during a calendar year shall be allowed during the subsequent calendar year, leave with wages for a number of days calculated at the rate of‐
i. if an adult, one day for every twenty days of work performed by him during the previous calendar year;
ii. if a child, one day for every 15 days of work performed by him during the previous calendar year;
Any days of layoff, by agreement or contract, or as permissible under the standing orders; in case of a female worker, maternity leave for any number of days not exceeding twelve weeks, and the leave earned in the year prior to that in which the leave is enjoyed shall be deemed to be days on which the worker has worked in a factory for the computation of the period of 240 days or more but he shall not earn leave for these days.
The leave admissible under Sec. 79 shall be exclusive of all holidays, whether, occurring during or at either end of the period of leave.
A worker whose service commences otherwise than on the first day of January, shall be entitled to leave with wages at the rate laid down in Sec. 79 (i) if he has worked for two‐thirds of the total days in the remainder of the calendar year.
If a worker is discharged or dismissed from service during the course of the year he shall be entitled to leave with wages at the rates laid down in Sec. 79 (1) even if he has not worked in the entire calendar year.
Fraction of leave of half a day or more shall be treated as one full dayʹs leave and fraction of less than half a day shall be omitted.
If a worker does not in anyone calendar year take the whole of the leave allowed to him, any leave not taken by him shall be added to the leave to be allowed to him in the succeeding calendar year provided total number of days of leave that may be carried forward to a succeeding year shall not exceed thirty in case of adult and forty in the case of a child. Unavailed leave shall be carried forward without any limit provided a worker who has applied for leave with wages but has not been given such leave in accordance with any scheme laid down under Sec. 79(8), (9).
A worker may at any time apply in writing to the manager of a factory not less than fifteen days before the date on which he wishes leave to being and thirty days before that date if he is employed in a public utility service provided that the number of time in which leave may be taken during any year shall not exceed three. If a worker wants to avail himself of leave with wages due to him to cover a period of illness he shall be granted leave even if application is not made within the time specified above.
An application for leave with wages which does not contravene any scheme lodged under sec. 79 (8), (9) shall not be refused if it is made within the time specified above.
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 0
If the employment of a worker who is entitled to leave under Section 79 terminated by the occupier before he has taken the entire leave to which he is entitled, or if having applied for and having not been granted such leave, the worker quits his employment before he has taken the leave, the occupier of the factory shall pay him the amount payable in respect of the leave not taken and such payment shall be made before the expiry of the second working day on which his employment is terminated.
Unavailed leave of a worker shall not be taken into consideration in computing the period of any notice required to be given before discharge or dismissal.
The manager shall maintain a leave with wages register in the prescribed Form No.14 and shall provide each worker with a book called the ʹLeave Bookʹ in the prescribed Form No.15. The Leave Book shall be the property of the worker and the manager or his agent shall not demand it except to make entries of the dates of holidays or interruptions in service and shall not keep it for more than a week at a time. If a worker loses his Leave Book, the manager shall provide him with another copy on payment of one anna and shall complete it from his record.
Health
12. Cleanliness. Section 11‐ Except in cases specially exempted all inside walls and partition, all ceilings or tops of rooms and all walls, sides arid tops of passages and staircases in a factory shall be kept white‐washed or colour‐washed. The white‐washing or colour‐washing shall be carried out at least once in every period of fourteen months. The floors of every workroom shall be cleaned at least once in every week by washing using disinfectant, where necessary or some other method.
13. Disposal of Wastes & Effluents. Section 12‐ Effective arrangement shall be made in every factory for the disposal of wastes and effluents due to the manufacturing process carried on therein.
14. Ventilation and Temperature. Section 13‐ Effective and suitable provision shall be made in every factory securing and maintaining in every workroom adequate ventilation by the circulation of fresh air and such a temperature as will secure to workers therein reasonable conditions of comfort and prevent injury to health.
15. Overcrowding. Section 16‐ Unless exemption has been granted, there be in every workroom of a factory in existence on 1st April, 1949 at least 350 cubic feet and of a factory built after this date at least 500 cubic feet of space for every worker employed therein and for this purpose no account shall be taken of any space which is more than 14 ft, above the level of the floor of the room,
16. Lighting. Section 17‐ In every part of a factory where workers are working or passing, there shall be provided and maintained sufficient and suitable light, natural or artificial or both.
17. Drinking Water .Section 18‐ In every factory effective arrangements shall be made to provide and maintain in suitable points, conveniently situated for all workers employed therein, a sufficient supply of wholesome drinking water,
In every factory wherein more than 250 workers are ordinarily employed the drinking water shall during the hot weather, be cooled by ice or other effective methods. The cooled drinking water shall be supplied in every canteen. Lunch room and rest room and also at conveniently accessible points throughout the factory,
18. Latrines and Urinals. Section 19 and Rules‐In every factory sufficient latrine and urinal accommodation of the prescribed type (separate enclosed accommodation for male and female workers) shall be provided conveniently situated and accessible to workers at all times while they are at the factory. Every latrine shall be under cover
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 1
and so partitioned off as to secure privacy and shall have a proper door and fastening. Sweepers shall be employed whose primary duty It would be to keep clean latrine, urinals and washing places.
19. Spittoons. Section 20‐ In every factory, there shall be provided a sufficient number of spittoons of the type prescribed in convenient places and, they shall be maintained in a clean and hygienic condition, No person shall spit within the premises of a factory except in the spittoons provided for the purpose. Whoever spits in contravention of this provision shall be punishable with fine not exceeding five rupees.
Safety
20. Fencing of Machinery. Section 21‐In every factory dangerous parts of machines e.g., every moving part of a prime mover and every fly‐wheel connected to a prime mover etc., shall be securely fenced by safeguards of substantial construction which shall be kept in position while the parts of machinery they are fencing are in motion or in use.
21. Work on or near Machinery in motion. Section 22‐ No women or young person shall be allowed to clean, lubricate, or adjust any part of a prime mover or of any transmission machinery while the prime mover or transmission machinery is in motion, or to clean, lubricate or adjust any part of any machine if the cleaning, lubrication or adjustment thereof would expose the woman or young person to risk injury from any moving part either of that machine or of any adjacent machinery.
22. Employment of young Persons on Dangerous Machinery Section 22‐ No young person shall work at any machine declared to be dangerous unless he has been full instructed as to the dangers arising in connection with the machine and the precautions to be observed and has received sufficient training in work at the machine or is under adequate supervision by a person who has a thorough knowledge and experience of the machine.
23. Casing of new Machinery. Section 26‐ In all machinery driven by power and installed in any factory after 1st August, 1950, every set screw, bolt or key on any revolving shaft, spindle, wheel or pinion shall be so sunk, encased or otherwise effectively guarded as to prevent danger; all spur, worm and other toothed or friction gearing which does not require frequent adjustment while in motion shall be completely encased, unless it is so situated as to be as safe as it would be if it were completely encased.
Whoever sells or lets on hire or as agent of a seller or hirer, causes or procures to be sold or let on hire, for use in a factory any machinery driven by power which does not comply with these provisions, shall be punishable with imprisonment for a term which may extend to three months or with fine which may extend to five hundred rupees or with both.
24. Prohibition of employment of Women and Children near Cotton Openers Section 27
No woman or child shall be employed in any part of a factory for pressing cotton in which a cotton opener is at work.
25. Excessive Weights. Section 34‐ No woman or young person shall unaided by another person, lift, carry or move by hand, any material article, tool or appliance exceeding the following limits :‐
Adult female ‐ 65 Ibs. Adolescent male ‐ 65 Ibs. Adolescent female ‐ 45 Ibs. Male child ‐ 35 Ibs. Female child ‐ 30 Ibs.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 2
26. Protection of Eyes. Section 35‐ Effective screens or suitable goggles shall be provided for the protection of persons employed in or in the vicinity of processes which involve risk or injury to the eyes from particles or fragments thrown off in the course of the process or which involve risk of injury to the eyes by reason of exposure to excessive light.
27. Precautions in case of fire. Section 38‐ Every factory shall be provided with adequate means of escape in case of fire for the persons employed therein. The doors affording exit from any room shall, unless they are of the sliding type be constructed to open outwards. Every window, door or other exit in affording a means of escape in a case of fire, other than the means of exit in ordinary use shall be distinctively marked. Effective and clearly audible means of giving warning in a case of fire to every person employed in the factory shall be provided. Effective measures shall be taken to ensure that wherein more than twenty workers are ordinarily employed in any place above the ground floor or wherein explosive or highly inflammable materials are used or stored, all the workers are familiar with the means of escape in ease of fire and have been adequately trained in the routine to be followed in such case.
Welfare
28. Washing Facilities. Section 42‐Ineveryfactory adequate and suitable facilities for washing shall be provided and maintained for the use of the workers therein. Such facilities shall include soap and nail brushes or other suitable means of cleaning and the facilities shall be conveniently accessible and shall be kept in a clean and orderly condition.
If female workers are employed, separate facilities shall be provided and so enclosed or screened that the interiors are not visible from any place where persons of the other sex work or pass.
29. Facilities for storing and Drying Clothing. Section 43 and Rule‐In the case of certain dangerous operations e.g., lead processes, liming and tanning of raw hides and skins etc. Suitable places for keeping clothing not worn during working hours and for the drying of wet clothing shall be provided and maintained.
30. Facilities for Sitting. Section 44‐ In every factory suitable arrangements for sitting shall be provided and maintained for all workers obliged to work in a standing position in order that they may take advantage of any opportunities for rest which may occur in the course of their work.
31. First aid and Ambulance Room. Section 45‐ There shall in every factory be provided and maintained so as to be readily accessible during all working hours first‐aid boxes or cupboards equipped with the prescribed contents. Each first aid box or cupboard shall be kept in the charge of a separate responsible person who is trained in first aid treatment and who shall always be readily available during the working hours of the factory.
In every factory wherein more than 500 workers are employed there shall be provided and maintained an ambulance room of the prescribed size and containing the prescribed equipment. The ambulance room shall be in charge of a qualified medical practitioner assisted by at least a qualified nurse and such other staff as may be prescribed.
32. Canteens. Section 46 and Rules‐ In specified factories wherein more than 250 workers are ordinarily employed a canteen or canteens shall be provided and maintained by the occupier for the use of this workers. Food, drink and other items served in the canteen shall be sold on a non‐profit basis and the prices charged shall be subject to the approval of a Canteen Managing Committee which shall be appointed by the Manager and shall consist of an equal number of persons nominated by the occupier and elected by the workers. The number of elected workers shall be in the proportion of 1 for every 1,000 workers employed in the factory provided that in no case shall
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 3
there be more than 5 or less than 2 workers on the Committee. The Committee shall be consulted from time to time on to the quality and quantity of food‐stuffs to be served in the Canteen, the arrangement of the menus, etc.
33. Shelters, Rest Rooms and Lunch Rooms. Section 47‐ In every factory wherein more than 150 workers are ordinarily, employed, adequate and suitable shelters or rest rooms and a suitable lunch room, with provision for drinking water, where workers can eat meals, brought by them, shall be provided and maintained for the use of the workers.
34. Creches. Section 48 and Rules‐ In every factory wherein more than 50 women workers are ordinarily employed, there shall be provided and maintained a suitable room or rooms for the use of children under the age six years of such women. The Creche shall be adequately furnished and equipped and in particular there shall be one suitable cot or a cradle with the necessary bedding for each child, at least one chair or equivalent seating accommodation for the use of the mother while she is feeding or attending to her child and sufficient supply of suitable toys for older children.
There shall be in or adjoining the Creche a suitable wash‐room for the washing of the children and their clothing. An adequate supply of clean cloths, soap and clean towels shall be made available for each child while it is in the Creche. At least half a pint of clean pure milk shall be available for each child on every day it is accommodated in the Creche and the mother of such a child shall be allowed in the course of her daily work suitable intervals to feed the child. For children above two years of age there shall be provided, in addition, an adequate supply of wholesome refreshments. A suitably fenced and shady open air play‐ground shall also be provided for the older children.
35. Welfare Officers. Section 49‐ In every factory wherein 500 or more workers are ordinarily employed the occupier shall employ in the factory such number of welfare Officers as may be prescribed.
Special Provisions
36. Dangerous Operation. Section 87 and Rules‐ Employment of women, adolescents and children is prohibited or restricted in certain operation declared to be dangerous, e.g. manufacture of aerated water, electroplating, manufacture and repair of electric accumulators, glass manufacture grinding or glazing of metals, manufacture and treatment of lead and certain compounds of lead, generating petrol gas from petrol, sandblasting, liming and tanning of raw hides and skins, and certain lead process in Printing Presses and Type Foundries.
37. Notice of Accidents. Section 88 and Rules‐ Where in any factory an accident occurs which causes death or which causes bodily injury by reason of which the person injured is prevented from working for a period of 48 hours or more immediately following the accident or which, though not attended by personal injury or disablement is of one of the following types :‐
i. Bursting of vessel used for containing steam under pressure greater than atmospheric pressure other than plant which comes within the scope of the Indian Boilers Act;
ii. Collapse or failure of a crane, derrick, hoist or other appliances used in raising or lowering persons or goods, or any part thereof, or the overturning of a crane;
iii. Explosion or fire causing damage to any room or place in which persons are employed or fire in rooms of cotton pressing factories, where a cotton opener is in use;
iv. Explosion of a receiver or container used for the storage at a pressure greater than atmospheric pressure of and gas or gases including air or any liquid or solid resulting from the compression of gas;

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 4
v. Collapse or subsidence of any floor, gallery, roof, bridge, tunnel, chimney, wall or building, forming part of a factory or within the compound or cartilage of factory.
The Manager of the factory shall forthwith send notice thereof to the Chief Inspector, if the accident is fatal or of such a serious nature that it is likely to prove fatal, notice shall also be sent to the District Magistrate or the Sub Divisional Officer and the Officer‐in‐Charge of the nearest Police Station.
38. Notice of Certain Diseases. Section 89 and Rules‐ Where any worker in a factory contracts any of the following diseases the Manager of the factory shall send notice thereof forthwith both to the Chief Inspector and the Certifying Surgeon:
Lead, phosphorus, mercury, manganese, arsenic, carbon bisulphide or benzene poisoning by nitrous fumes, or by halogens or halogen derivatives of the hydrocarbon of the aliphatic series; or of chrome ulceration, anthrax, silicosis, toxic anemia toxic jaundice, primary opitheliomatous cancer of the skin, or pathological manifestations due to radium or other radioactive substances or X‐rays.
39. No Charge for Facilities and Conveniences. Section 114‐ No fee or charge shall be realized from any worker in respect of any arrangements or facilities to be provided or any equipments or appliances to be supplied by the occupier under the provision of the Act.
40. Powers of Inspectors. Sections 9 and 82‐ Inspectors have power to inspect factories any time and may require the production of registers, certificates etc, prescribed under the Act and the Rules.
Any Inspector may institute proceeding on behalf of any workers to recover any sum required to be paid by an employer under the provisions relating to leave with wages, which the employer has not paid.
41. Obligations of Workers. Sections 97 and 111‐Noworker in a factory :‐
i. shall wilfully interfere with or misuse any appliance, convenience or other thing provided in a factory for the purposes of securing the health, safety or welfare of the workers therein.
ii. shall wilfully and without any reasonable cause do any thing likely to endanger himself or others, and
iii. shall wilfully neglect to make use of any appliance or other thing provided in the factory for the purposes of securing the health or safety of the workers therein.
If any worker employed in a factory contravenes any of these provisions or any rule or order made there under he shall be punishable with imprisonment for a term which may extend to three months, or which may extend to Rs. 100 or with both.
If any worker employed in a factory contravenes any provision of the Act or any rules or orders made thereunder imposing any duty or liability on workers he shall be punishable with fine which may extend to Rs. 20.
42. Certificates of Fitness. Sections 68, 70 and 98‐ No child who has completed his fourteenth year or an adolescent shall be required or allowed to work in any factory unless a certificate of fitness granted with reference to him is in the custody of the Manager of the factory and such child or adolescent carries, while he is at work, at token giving a reference to such certificate. Any fee payable for such a certificate shall be paid by the occupier and shall not be recoverable from the young person, his parents or guardian.
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 5
An adolescent who has been granted a certificate of fitness to work in a factory as an adult and who while a work in a factory carries a token giving reference to the certificate shall be deemed to be an adult for all the purposes of the provision of the Act relating to the working hours of adult and the employment of young persons. An adolescent who has not been granted a certificate of fitness to work in a factory as an adult shall, notwithstanding his age, be deemed to be a child for all the purposes of the Act.
Whoever knowingly uses or attempts to use, as a certificate of fitness granted to himself a certificate granted to another adolescent to work in a factory as an adult, or who having procured such certificate knowingly allows it to be used or an attempt to use it to be made, by another person, shall be punishable with imprisonment for a term which may extend to one month or with fine which may extend to Rs. 50 or with both.
43. Registers, Notices and Returns. Sections 61, 63, 72, 74, 79, 80 and 110‐ A Register of adult workers in the prescribed Form No.12 and a register of child workers in the prescribed Form No.14 shall be maintained by the Manager of every factory.
A notice of periods of work for adults and a notice of periods of work of children in the prescribed Form No.11 (a) or 11 (b) and 12 shall be correctly maintained and displayed in every factory. No adult worker or child shall be required or allowed to work in any factory otherwise than in accordance with their respective notice of periods of work displayed in the factory.
The Owners Occupiers or Managers of factories shall submit the prescribed periodical returns to the Inspector regularly.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 6
FORM NO. 21
(NOW FORM NO.34) (Prescribed under sub‐rule (1) of rule 100)
Annual Return
For the Year ending 31st December, 19............
1. Registration number of factory.
2. Name of factory.
3. Name of occupier.
4. Name of the manager.
5. District.
6. Full postal address of factory.
7. Nature of industry.
Number of workers and particulars of employment
8. No. of days worked in year.
9. No. of Man‐days worked during the year.
a. Men.
b. Women.
c. Children.
10. Average number of workers employed daily (See explanatory note).
a. Adults.
i. Men.
ii. Women.
b. Adolescents
i. Male.
ii. Female.
c. Children
i. Male.
ii. Female.
11. Total No. of man‐hours worked including overtime.
a. Men
b. Women
c. Children
12. Average number of hours worked per day work (See explanatory note).
a. Men.
b. Women.
c. Children.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 7
13. Does the factory carry out any process or operation declared as dangerous under Section 87. (See rule 95).
Name of the dangerous Process of operations carried on
Average No. of persons employed daily in each of the processes or operations given in Col. 1
(i)
(ii)
(iii) etc.
Leave with wages
14. Total number of workers employed during the year.
a. Men.
b. Women.
c. Children.
15. Number of workers who were entitled to annual leave with wages during the year.
a. Men.
b. Women.
c. Children.
16. Number of workers who were granted leave during the year.
a. Men.
b. Women.
c. Children.
17.
a. Number of workers who were discharged, or dismissed from the service, or quit employment, or were superannuated, or who died while in service during the year.
b. Number of such workers in respect of whom wages in lieu of leave were paid.
18.
a. Number of Safety Officers required to be appointed as per notification under Section 40‐B.
b. Number of Safety Officers appointed.
AMBULANCE ROOM
19. Is there an ambulance room provided in the factory as required under Section 45?
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 8
CANTEEN
20.
a. Is there a canteen provided in the factory as required under Section 46?
b. Is the canteen provided managed :
i. departmentally, or
ii. through a contractor ?
SHELTERS OR REST ROOMS AND LUNCH ROOMS
21.
a. Are there adequate and suitable shelters or rest rooms provided in the factory as required under Section 47 ?
b. Are there adequate and suitable lunch rooms provided in the factory as required under Section 47 ?
CRECHES
22. Is there a creche provided in the factory as required under Section 48 ?
WELFARE OFFICERS
23.
a. Number of Welfare Officers to be appointed as required under Section 49 ?
b. Number of Welfare Officers appointed. ACCIDENTS
24.
a) Total number of accidents (See explanatory note) :
i. Fatal.
ii. Non‐fatal.
b) Accidents in which workers returned to work during the year to which this return relates.
i. Accidents (workers injured) occurring during the year in which injured workers returned to work during the same year.
(aa) Number of accidents.
(bb) Man‐days lost due to accidents.
ii. Accidents (workers injured) occurring in the previous year in which injured workers returned to work during the year to which this return relates :
(aa) Number of accidents.
(bb) Man‐days lost due to accidents.
c) Accidents (workers injured) occurring during the year in which injured workers did not return to work during the year to which the return relates.
i. Number of accidents.
ii. Man‐days lost due to accidents.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 4 9
SUGGESTION SCHEME
25.
a. Is a suggestion Scheme in operation in the factory
b. If so, the number of suggestions
i. Received during the year
ii. Accepted during the year
c. Amount awarded each prizes during the period
i. Total amount awarded
ii. Value of the maximum cash prize awarded
iii. Value of maximum cash prize awarded
Certified that the information furnished above is to the best of my knowledge and belief, correct.
Signature of the manager
Date.........
Explanatory Notes :
1. The average number of workers employed daily should be calculated by dividing the aggregate number of attendance on working days (that is, men‐days worked) by the number of working days in the year. In reckoning attendance, attendance by temporary as well as permanent employed should be counted, and all employees should be included, whether they are employed directly or under contractors. Attendance on separate shifts (e.g. night and day shifts) should be counted, separately. Days on which the factory was closed for whatever cause, and days on which the manufacturing processes were not carried on should not be treated as working days. Partial attendance for less than half a shift on a working day should be ignored, while attendance for half a shift or more on such day should be treated as full attendance.
2. For seasonal factories, the average number of workers employed during the working season and the off‐season should be given separately. Similarly the number of days worked and average number of man hours worked per week during the working and off‐season should be given separately.
3. The average number of hours worked per week means the total actual hours worked by all workers during the year excluding the rest intervals but including overtime work divided by the product of total number of workers employed in the factory during the year and 52. In case the factory has not worked for the whole year, the number of weeks during which the factory worked should be used in view of the figure 52.
4. Every person killed or injured should be treated as one separate accident. If in one occurrence six persons were injured or killed it should be counted as six accidents.
5. In item 24(a), the number accident which took place during the year should be given in case of non‐fatal accidents only.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 5 0
FORM NO. 22 [Prescribed under sub‐rule (3) of rule 100]
Half‐ Yearly Return Period ending 30th June 20.. / 31st December 20..
Name of Factory
Name of Occupier
Name of Manager
1. District
2. Postal Address
3. Nature of industry
4. Average number of workers employed daily*
Men
Women
Adolescent :
Male
Female
Children :
Male
Female
5. Number of days worked during the half year ending 30th June 20/ 31 st December 20
Signature of Occupier .......... Signature of Manager .......
Date of Dispatch .......... Date of Dispatch ..........................

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 5 1
FORM NO.24 [Prescribed under sub‐rule (5) of Rule 100]
Annual Return ‐ Creche
Year ending 31stDecember 20…
1. Industry
2. Name of factory
3. Number of women workers ordinarily employed
4. Number of children admitted in the creche
5. Average daily attendance of children at the creche
a. 2 years and below
b. Above 2 years.
6. Details of facilities provided with regard to :‐
a. Milk
b. Food
c. Clothes
d. Toys
e. Medical Aid
f. Other
7. Details of staff employed
i. Doctors :‐
a. Males
b. Females
ii. Nurses
iii. Teachers
iv. Ayahs
v. Sweepers
8. General remarks.
Signature of Occupier .......... Signature of Manager .......
Date of Dispatch .......... Date of Dispatch ..........................

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 5 2
FORM NO. 26 (Prescribed under Rule 103)
Muster Roll
Name of Factory..........
Place where situated..........
Working Hours
Monday to Friday Saturday
Time of Commencement of work Rest Period
Time of Completion of work
Serial No.
Name Fatherʹs Name
Nature of Work
For the Period ending ... Remarks
1 2 3 4 5 6
Note:‐ Separate page should be used for workers employed during different period of work.

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 5 3
FORM NO. 27 (Prescribed under Rule 104)
Register of Accidents and Dangerous Occurrences
Name of injured persons (if any)
Date of accident or dangerous occurrence
Date of report (in Form No.18) to Inspector
Nature of accident or dangerous occurrence
Date of return of injured person to work
No. of days injured person was absent from work
1 2 3 4 5 6
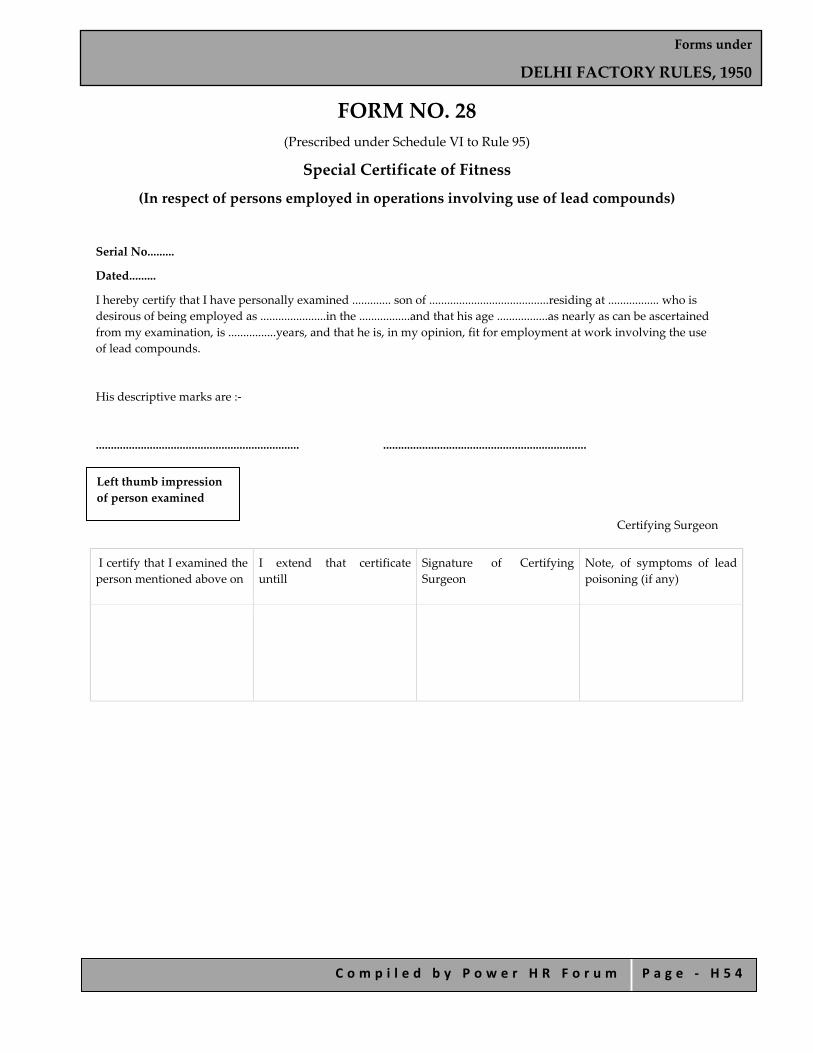
Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 5 4
FORM NO. 28 (Prescribed under Schedule VI to Rule 95)
Special Certificate of Fitness
(In respect of persons employed in operations involving use of lead compounds)
Serial No.........
Dated.........
I hereby certify that I have personally examined ............. son of ........................................residing at ................. who is desirous of being employed as ......................in the .................and that his age .................as nearly as can be ascertained from my examination, is ................years, and that he is, in my opinion, fit for employment at work involving the use of lead compounds.
His descriptive marks are :‐
.................................................................... ....................................................................
Certifying Surgeon
I certify that I examined the person mentioned above on
I extend that certificate untill
Signature of Certifying Surgeon
Note, of symptoms of lead poisoning (if any)
Left thumb impression of person examined

Forms under
DELHI FACTORY RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ H 5 5
FORM NO. 29 [Prescribed under Rule 53 (A)]
PART I
1. Name of the Worker .......................................................................................
2. Serial No. as in the register of workers, under section 62 of the act ...............................................
3. Fatherʹs Name.......................................................................................
4. Age and date of birth.......................................................................................
5. Nature of work ........................................................................................
6. Qualifications, if any, or period of service on similar work ............................................
7. Date when tight fitting clothing were provided.........................................
8. Signature or thumb impression of workers........................................
9. Remarks
Signature of Occupier
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 1
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 2
INDEX
FORM A Statement Under Section 5 (1)
FORM B Register of Establishments
FORM C Registration Certificate of Establishment
FORM D Notice of Change
FORM E Notice of Close Day or a Change in Close Day
FORM G Register of Employment & Remuneration
FORM H Register of Employment and Remuneration of Employees
FORM I Register of Leave
FORM J Notice of Holiday Under Section 17
FORM K Notice Under Section 33 of the Delhi Shops and Establishments Act, 1954, to be Exhibited Conspicuously at the Premises of the Establishment
FORM L Renewal of Registration Certificate

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 3
FORM A Statement under Section 5 (1)
(See rule 3) Part I
1. Name of the establishment, if any.........................................
2. Postal address of the establishment.........................................
3. Full name of the occupier or the employer including his fatherʹs name........................................
4. Full name of the Manager, if any including his fatherʹs name........................................
5. Category of the establishment, i.e., whether a shop, commercial establishment, residential hotel, restaurant, eating house, theatre or other place of public amusement or entertainment.........................................
6. Nature of business.........................................
Part II
7. Names of members of employerʹs family, working in the establishment (state separately the names of young persons, if any). ........................................
8. Names of other persons occupying position of management or employees engaged in confidential capacity. ........................................
9. Total number of employees (state separately the number of men, women and/or young persons, if any).
Men Women Young Person
10. Date on which the establishment commenced its work.........................................
11. I hereby declare that the details given above are correct to the best of my knowledge.
Dated .............................................................
Note: This statement shall be sent to the Chief Inspector with such fees as are prescribed in Schedule I.
Signature of the occupier/employer
..........................................................
Received from ........................................Form A with Challan No........................................Signature
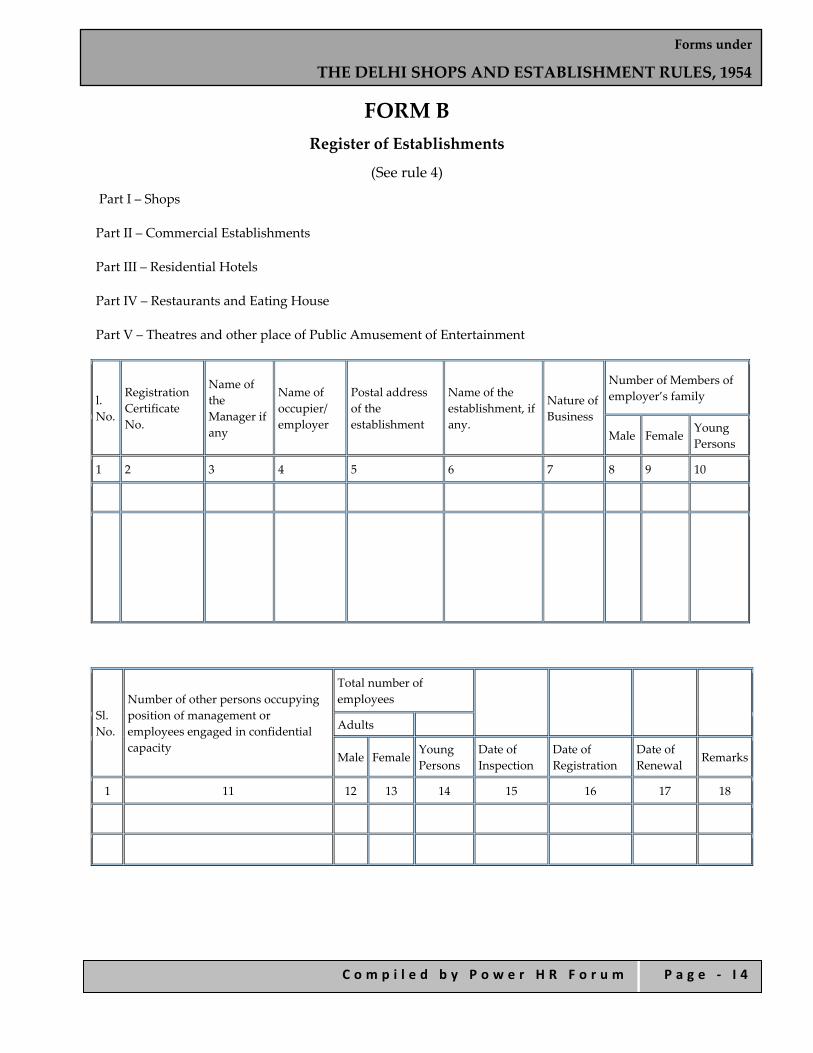
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 4
FORM B Register of Establishments
(See rule 4)
Part I – Shops
Part II – Commercial Establishments
Part III – Residential Hotels
Part IV – Restaurants and Eating House
Part V – Theatres and other place of Public Amusement of Entertainment
l. No.
Registration Certificate No.
Name of the Manager if any
Name of occupier/ employer
Postal address of the establishment
Name of the establishment, if any.
Nature of Business
Number of Members of employer’s family
Male FemaleYoung Persons
1 2 3 4 5 6 7 8 9 10
Sl. No.
Number of other persons occupying position of management or employees engaged in confidential capacity
Total number of employees
Adults
Male FemaleYoung Persons
Date of Inspection
Date of Registration
Date of Renewal
Remarks
1 11 12 13 14 15 16 17 18
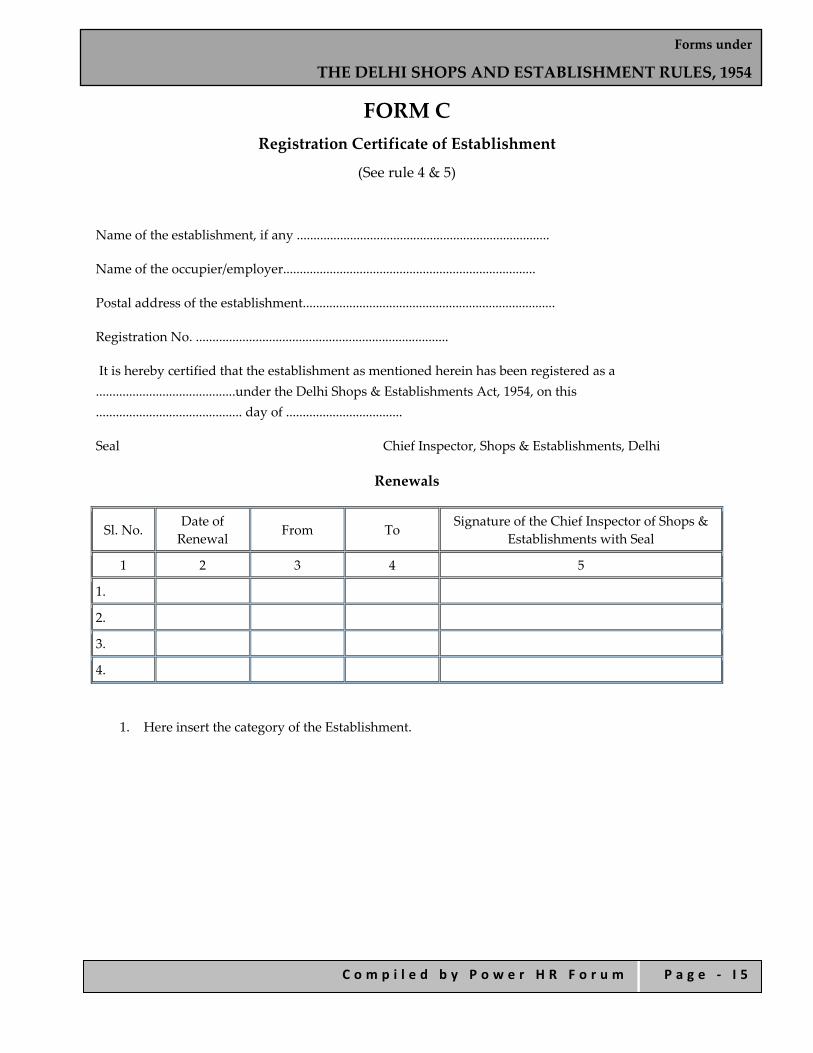
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 5
FORM C Registration Certificate of Establishment
(See rule 4 & 5)
Name of the establishment, if any ............................................................................
Name of the occupier/employer............................................................................
Postal address of the establishment............................................................................
Registration No. ............................................................................
It is hereby certified that the establishment as mentioned herein has been registered as a ..........................................under the Delhi Shops & Establishments Act, 1954, on this ............................................ day of ...................................
Seal Chief Inspector, Shops & Establishments, Delhi
Renewals
Sl. No. Date of Renewal From To Signature of the Chief Inspector of Shops &
Establishments with Seal
1 2 3 4 5
1.
2.
3.
4.
1. Here insert the category of the Establishment.

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 6
FORM D Notice of Change (See rule 4 & 5)
1. Name of the establishment and/or name of occupier/employer................................................................
2. Full Address ................................................................................................................................
3. Registration Certificate No............................. Dated the ..................... Date of ..................20...............
To,
The Chief Inspector under the Delhi Shops & Establishments Act, 1954
Notice is hereby given that the following change has taken place in respect of information relating to Part I of the Form A which please note.
.........................................................
Signature of the occupier/employer
Note – Notice of change in this form shall be sent together with such fees as are prescribed in Schedule II.

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 7
FORM E Notice of Close Day or a Change in Close Day
(See rule 8)
To,
The Chief Inspector
Shops & Establishments
Delhi
Name of Establishment ...................................................................................................
Address ...........................................................................................................................
Registration Certificate No. ..............................................................................................
Notice is hereby given that with effect from........................................... the establishment shall observe ........................................... as the close day.
Date ....................................................... .........................................................
Signature of the occupier/employer

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 8
FORM G Register of Employment & Remuneration
(See rule 14)
Year...........................Month..........................of..................
Wage Period
(Where Different)………………………………………………………….
Name of Establishment ........................................................................................
Name of Employee ...............................................................................................
Nature of Work ....................................................................................................
Wage Period ........................................................................................................
Father’s Name.......................................................................................................
Rate of Wages .....................................................................................................
Date of Employment .............................................................................................
Date
Hours of Work
Interval for Rest & Meals Hours
worked with the employe
r
Overtime Casual or
sickness Leave Availed during the
Month/ Wage Period
Privilege Leave
Signature of Owner or
Occupier
Remarks
From
To
From
To
Hours Worked
Wages
earned
Leave Due
Leave Availabl
e
Balance
1 2 3 4 5 6 7 8 9 10 11 12 13 14
1.
2.
3.
4.
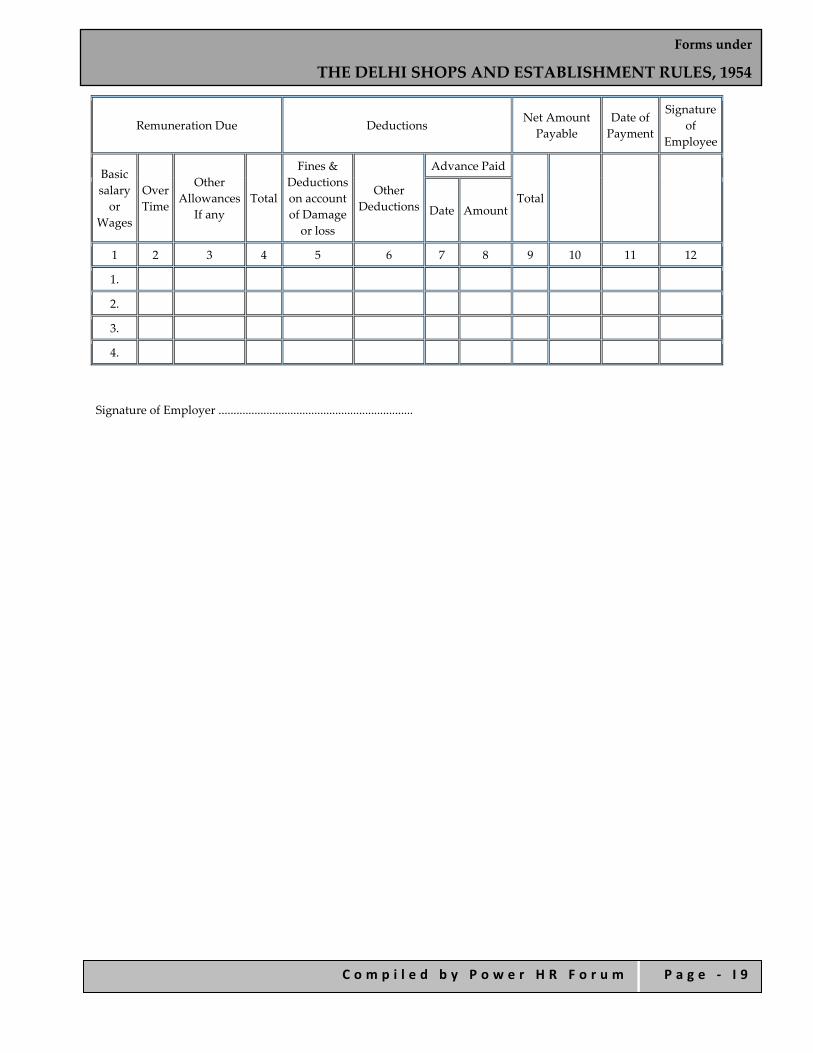
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 9
Remuneration Due Deductions Net Amount Payable
Date of Payment
Signature of
Employee
Basic salary or
Wages
Over Time
Other Allowances
If any Total
Fines & Deductions on account of Damage or loss
Other Deductions
Advance Paid
Total
Date Amount
1 2 3 4 5 6 7 8 9 10 11 12
1.
2.
3.
4.
Signature of Employer .................................................................
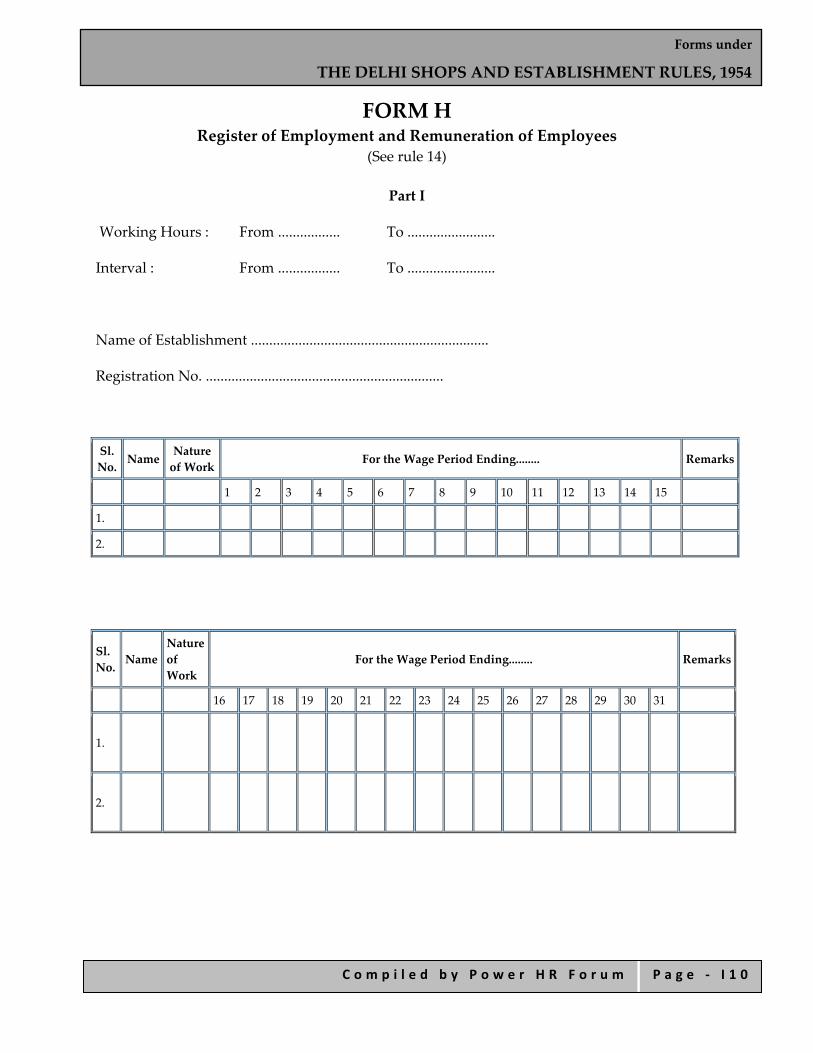
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 1 0
FORM H Register of Employment and Remuneration of Employees
(See rule 14)
Part I
Working Hours : From ................. To ........................
Interval : From ................. To ........................
Name of Establishment .................................................................
Registration No. .................................................................
Sl. No. Name
Nature of Work For the Wage Period Ending........ Remarks
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
1.
2.
Sl. No. Name
Nature of Work
For the Wage Period Ending........ Remarks
16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31
1.
2.
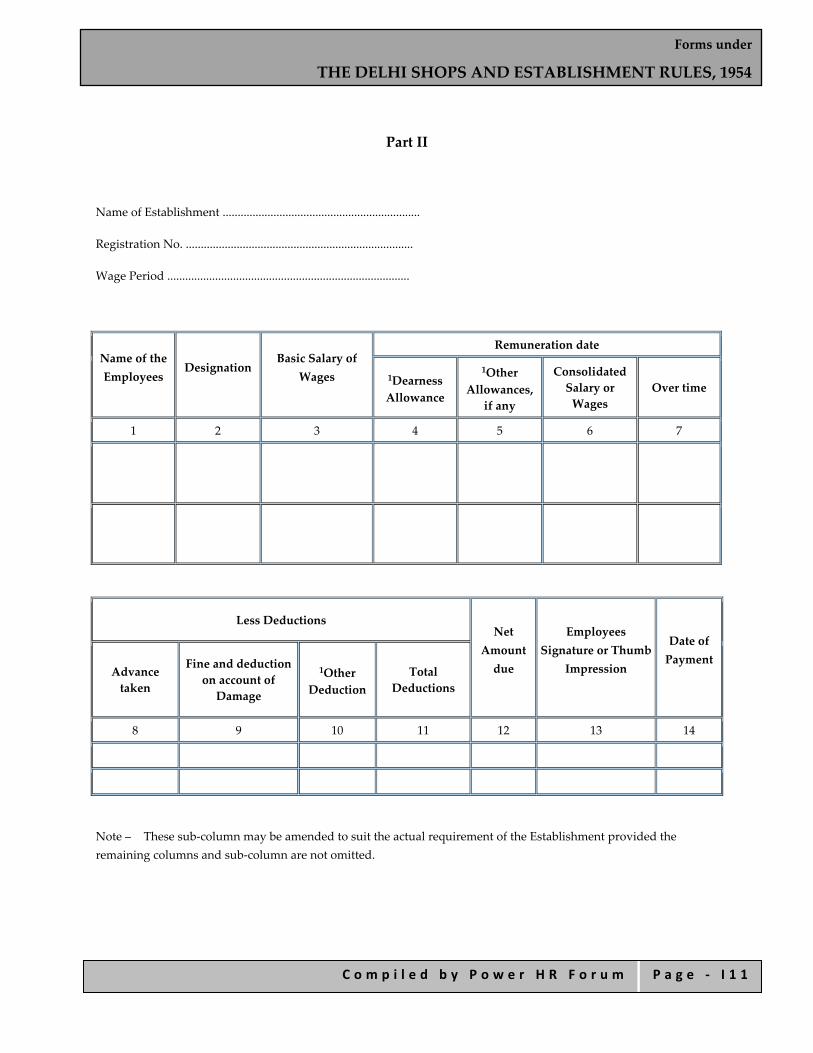
Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 1 1
Part II
Name of Establishment ..................................................................
Registration No. ............................................................................
Wage Period .................................................................................
Name of the Employees
Designation Basic Salary of
Wages
Remuneration date
1Dearness Allowance
1Other Allowances, if any
Consolidated Salary or Wages
Over time
1 2 3 4 5 6 7
Less Deductions Net
Amount due
Employees Signature or Thumb
Impression
Date of Payment
Advance taken
Fine and deduction on account of Damage
1Other Deduction
Total Deductions
8 9 10 11 12 13 14
Note – These sub‐column may be amended to suit the actual requirement of the Establishment provided the remaining columns and sub‐column are not omitted.

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 1 2
FORM I Register of Leave
(See rule 14)
Name of Establishment .................................................................
Name of Employee ...........................................................................
Date of Employment ....................................................................
Casual or sick leave Privilege Privilege Leave
Amount of Leave Requested
Date of Application if any
Leave Availed Total
Leave Availed
Date of Application
Whether Application Granted or Refused Fully or Partly
Leave Availed Total
Leave Availed
Balance at the end of the year From To From To
1 2 3 4 5 6 7 8 9 10 11

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 1 3
FORM J Notice of Holiday under Section 17
[See rule 14(2)]
Name of Establishment .................................................................
Address ........................................................................................
The person employed in the establishment shall be given a holiday on the day mentioned below in the week following the date of this and until further notice :‐
Sl. No. Name of Employee Day on which Holiday is Allowed

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 1 4
FORM K
Notice under Section 33 of the Delhi Shops and Establishments Act, 1954, to be Exhibited
Conspicuously at the Premises of the Establishment
(See rule 14)
Please intimate subsequent change if any in this space
(1) Close Day ...........................................................................................................
Date Effective from ..............................................................................................
(2) Daily Hours of Work Fixed ....................................................................................
(a) On Days other than Saturdays .....................................................................
(b) On Saturdays ................................................................................................
Signature of the Employer or Occupier

Forms under
THE DELHI SHOPS AND ESTABLISHMENT RULES, 1954
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ I 1 5
FORM L (See Rule 5)
Renewal of Registration Certificate
Category of Establishment …………………………………..
Name of Establishment…………………………………………..
Total number of existing employees………………………………
Postal Address ………………………………………………..
To
The Chief Inspector of Shops of Establishments, Delhi
As the period of Registration certificate No. …………………………..originally granted/subsequently renewed is due to expire on……………………….. or has already expired on………………………. I have to request for its renewal.
Dated ……………. Signature of the Occupier/Employer
Note: The application shall be sent along with renewal fee as is prescribed in Schedule I
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
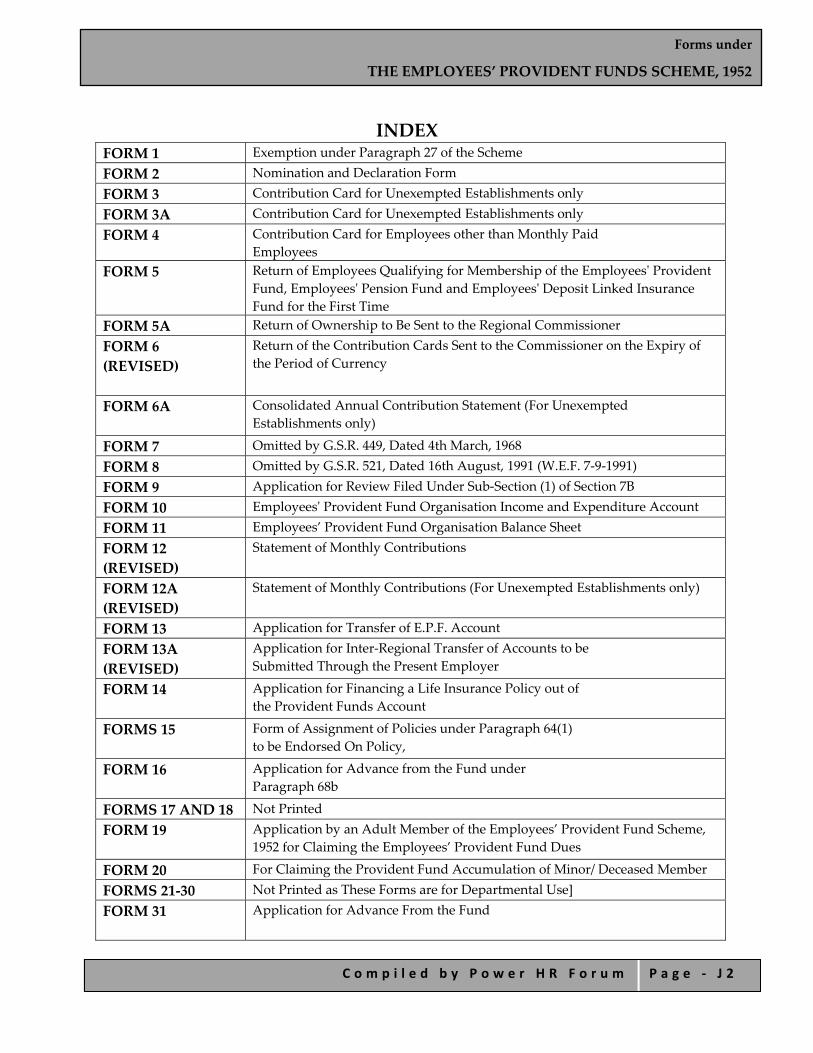
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2
INDEX
FORM 1 Exemption under Paragraph 27 of the Scheme FORM 2 Nomination and Declaration Form FORM 3 Contribution Card for Unexempted Establishments only FORM 3A Contribution Card for Unexempted Establishments only FORM 4 Contribution Card for Employees other than Monthly Paid
Employees FORM 5
Return of Employees Qualifying for Membership of the Employeesʹ Provident Fund, Employeesʹ Pension Fund and Employeesʹ Deposit Linked Insurance Fund for the First Time
FORM 5A Return of Ownership to Be Sent to the Regional Commissioner FORM 6 (REVISED)
Return of the Contribution Cards Sent to the Commissioner on the Expiry of the Period of Currency
FORM 6A
Consolidated Annual Contribution Statement (For Unexempted Establishments only)
FORM 7 Omitted by G.S.R. 449, Dated 4th March, 1968 FORM 8 Omitted by G.S.R. 521, Dated 16th August, 1991 (W.E.F. 7‐9‐1991) FORM 9 Application for Review Filed Under Sub‐Section (1) of Section 7B FORM 10 Employeesʹ Provident Fund Organisation Income and Expenditure Account FORM 11 Employees’ Provident Fund Organisation Balance Sheet FORM 12 (REVISED)
Statement of Monthly Contributions
FORM 12A (REVISED)
Statement of Monthly Contributions (For Unexempted Establishments only)
FORM 13 Application for Transfer of E.P.F. Account FORM 13A (REVISED)
Application for Inter‐Regional Transfer of Accounts to be Submitted Through the Present Employer
FORM 14
Application for Financing a Life Insurance Policy out of the Provident Funds Account
FORMS 15
Form of Assignment of Policies under Paragraph 64(1) to be Endorsed On Policy,
FORM 16
Application for Advance from the Fund under Paragraph 68b
FORMS 17 AND 18 Not Printed FORM 19
Application by an Adult Member of the Employees’ Provident Fund Scheme, 1952 for Claiming the Employees’ Provident Fund Dues
FORM 20 For Claiming the Provident Fund Accumulation of Minor/ Deceased Member FORMS 21‐30 Not Printed as These Forms are for Departmental Use] FORM 31
Application for Advance From the Fund
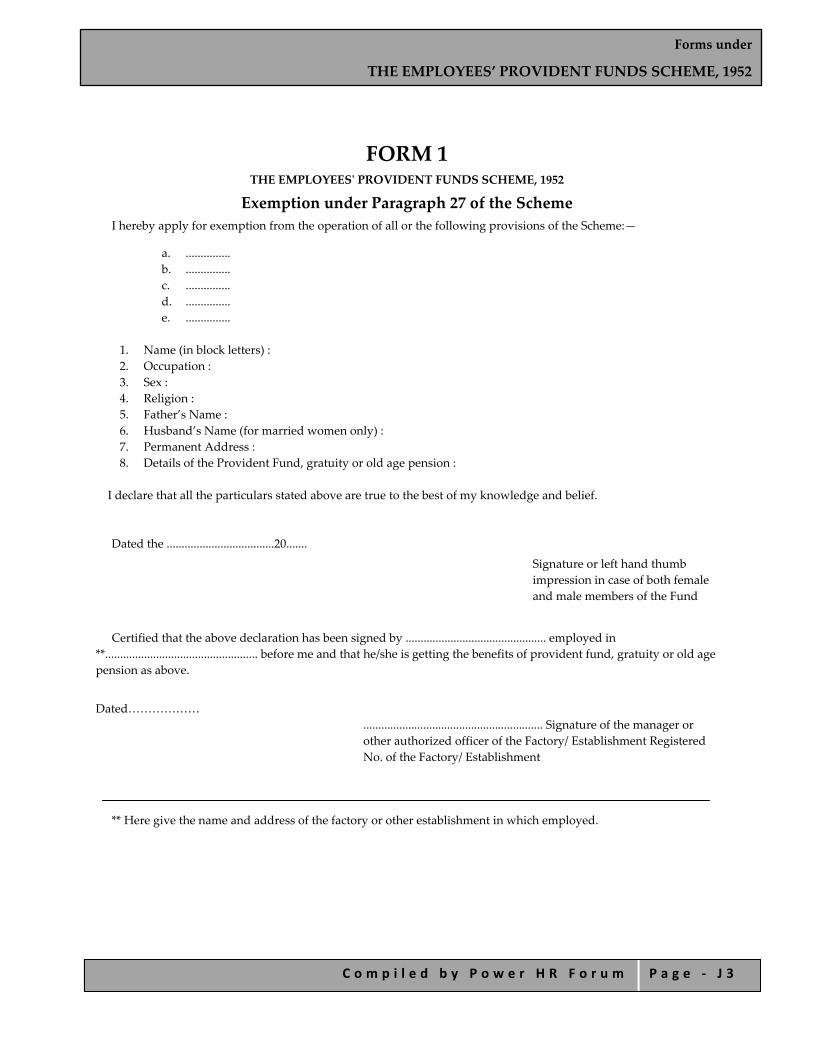
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3
FORM 1 THE EMPLOYEESʹ PROVIDENT FUNDS SCHEME, 1952
Exemption under Paragraph 27 of the Scheme I hereby apply for exemption from the operation of all or the following provisions of the Scheme:—
a. ............... b. ............... c. ............... d. ............... e. ...............
1. Name (in block letters) : 2. Occupation : 3. Sex : 4. Religion : 5. Father’s Name : 6. Husband’s Name (for married women only) : 7. Permanent Address : 8. Details of the Provident Fund, gratuity or old age pension :
I declare that all the particulars stated above are true to the best of my knowledge and belief.
Dated the ....................................20.......
Signature or left hand thumb impression in case of both female and male members of the Fund
Certified that the above declaration has been signed by ............................................... employed in
**................................................... before me and that he/she is getting the benefits of provident fund, gratuity or old age pension as above.
Dated………………
............................................................ Signature of the manager or other authorized officer of the Factory/ Establishment Registered No. of the Factory/ Establishment
** Here give the name and address of the factory or other establishment in which employed.
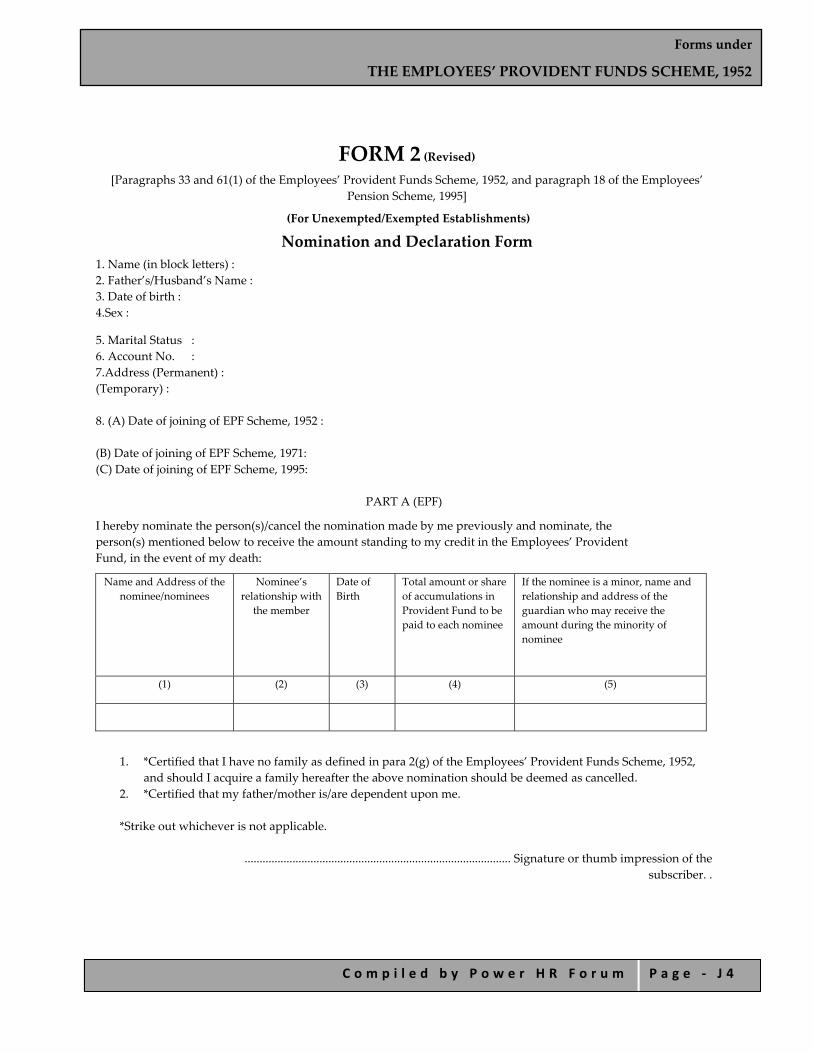
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4
FORM 2 (Revised) [Paragraphs 33 and 61(1) of the Employees’ Provident Funds Scheme, 1952, and paragraph 18 of the Employees’
Pension Scheme, 1995]
(For Unexempted/Exempted Establishments)
Nomination and Declaration Form 1. Name (in block letters) : 2. Father’s/Husband’s Name : 3. Date of birth : 4.Sex :
5. Marital Status : 6. Account No. : 7.Address (Permanent) : (Temporary) : 8. (A) Date of joining of EPF Scheme, 1952 : (B) Date of joining of EPF Scheme, 1971: (C) Date of joining of EPF Scheme, 1995:
PART A (EPF)
I hereby nominate the person(s)/cancel the nomination made by me previously and nominate, the person(s) mentioned below to receive the amount standing to my credit in the Employees’ Provident Fund, in the event of my death:
Name and Address of the nominee/nominees
Nominee’s relationship with
the member
Date of Birth
Total amount or share of accumulations in Provident Fund to be paid to each nominee
If the nominee is a minor, name and relationship and address of the guardian who may receive the amount during the minority of nominee
(1) (2) (3) (4) (5)
1. *Certified that I have no family as defined in para 2(g) of the Employees’ Provident Funds Scheme, 1952,
and should I acquire a family hereafter the above nomination should be deemed as cancelled. 2. *Certified that my father/mother is/are dependent upon me.
*Strike out whichever is not applicable.
......................................................................................... Signature or thumb impression of the subscriber. .

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 5
PART B (EPF)
(Para 18)
I hereby furnish below particulars of the members of my family who would be eligible to receive widow/children pension in the event of my death.
Sl. No. Name and address of the family members
Date of Birth Relationship with the member
(1) (2) (3) (4)
*Certified that I have no family, as defined in para 2(vii) of Employees’ Family Pension Scheme, 1995, and should I acquire a family hereafter I shall furnish particulars thereon in the above form.
I hereby nominate the following person for receiving the monthly widow pension (admissible under para
16(2)(g)(i) & (ii) of employees Pension Scheme, 1995 in the event of my death without leaving any eligible family member for receiving pension.
Name and Address of the Nominee Date of Birth
Relationship with the member
Date........................ ....................................................... Signature or thumb impression of the subscriber.
*Strike out whichever is not applicable.
CERTIFICATE BY EMPLOYER
Certified that the above declaration and nomination has been signed/thumb impressed before me by Shri/Smt./Kumari ................................... employed in my establishment after he/she has read the entries/the entries have been read over to him/her by me and got confirmed by him/her.
................................................................................. Signature of the Employer or other authorised officer of the establishment
Place........................... Designation..................................................
Dated the ...................., 20.....

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 6
Name and address of the Factory/Establishment or rubber stamp thereof
Note.—Whom you can nominate
A. Under the Employees’ Provident Fund Scheme 1) A member of E.P.F. who is married and/or his father/mother is/are dependant upon him can nominate
only one or more persons belonging to his family as defined below:— a. In the case of a male member, his wife, his children, his dependant parents and his deceased
son’s widow and children; b. In the case of a female member, her husband, her children, her dependant parents, her
husband’s dependent parents, her deceased son’s widow and children.
2) If the member has got no family, or is bachelor, nomination may be in favour of any person or persons, whether related to him or not or even to an institution. If the member subsequently acquires a family such nomination shall forthwith become invalid and the member should make a fresh nomination in favour of one or more persons belonging to his family.
B. Under the Family Pension Scheme 1. On the death of a member of the Family Pension Scheme, his family will be entitled to the benefits
under the Family Pension Scheme. The family is defined as under: i. wife in the case of a male member; ii. husband in the case of a female member; and iii. minor sons and unmarried daughters.
Explanation.—The expression “sons” and “daughters” shall include children adopted legally before death in service.
2. If the member has got no family, the monthly family pension, on the death of the member, will not be paid. However, Life Assurance Benefit will be paid to the person or persons entitled to receive his provident fund accumulations.
Note.— A fresh nomination shall be made by the member on his marriage and any nomination made before such
marriage shall be deemed to be invalid.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 7
FORM 3 (For Unexempted Establishments only)
(Paragraphs 35 and 42 of The Employeesʹ Provident Funds Scheme, 1952)
Contribution Card for the Currency Period From.......... To............
1. Account No. ................................................................................................................ 2. Name......................................................... Surname............................................ (In Block Capitals) 3. Father’s/Husband’s Name.......................................................................................... 4. Name and address of establishment......................................................................... 5. Statutory rate of contribution..................................................................................... 6. Voluntary, higher rate of employee’s contribution, if any.................................. 7. Age as on....................................................................................................................... 8. Occupation/Job............................................................................................................ 9. Income per month ...................................................................................................... 10. Permanent/Temporary/Contractual .....................................................................
MONTHS CONTRIBUTIONS
Refund of
advances
Break in membership/ reckonable service
Remarks
MEMBER’S SHARE EMPLOYER’S SHARE
E.P.F. F.P.F. @ 1‐ 1/6%
TOTAL E.P.F. F.P.F. @ 1‐ 1/6%
TOTAL
April May June July August September October November December January February March TOTAL
Dated the............................20.......
Signature of the Employer (Office Seal)]
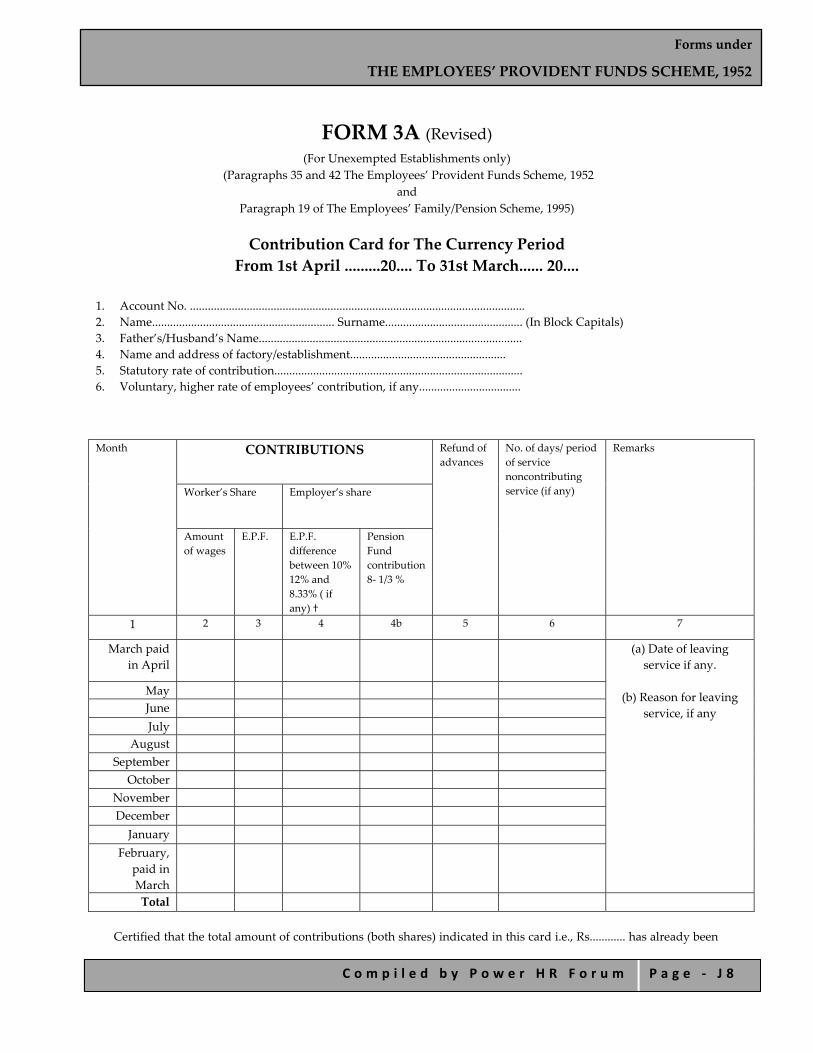
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 8
FORM 3A (Revised) (For Unexempted Establishments only)
(Paragraphs 35 and 42 The Employees’ Provident Funds Scheme, 1952 and
Paragraph 19 of The Employees’ Family/Pension Scheme, 1995)
Contribution Card for The Currency Period From 1st April .........20.... To 31st March...... 20....
1. Account No. ................................................................................................................ 2. Name............................................................. Surname.............................................. (In Block Capitals) 3. Father’s/Husband’s Name........................................................................................ 4. Name and address of factory/establishment.................................................... 5. Statutory rate of contribution................................................................................... 6. Voluntary, higher rate of employees’ contribution, if any..................................
Month CONTRIBUTIONS Refund of advances
No. of days/ period of service noncontributing service (if any)
Remarks
Worker’s Share Employer’s share
Amount of wages
E.P.F. E.P.F. difference between 10% 12% and 8.33% ( if any) †
Pension Fund contribution 8‐ 1/3 %
1 2 3 4 4b 5 6 7
March paid in April
(a) Date of leaving service if any.
(b) Reason for leaving
service, if any
May
June
July
August
September
October
November
December
January
February, paid in March
Total
Certified that the total amount of contributions (both shares) indicated in this card i.e., Rs............ has already been

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 9
remitted in full in EPF A/c. No. 1 (PF. A/c.) and A/ c. No. 10............ vide Note below. Certified that the difference between the total of the contributions shown under columns (3) and (4)(a) and (4)(b) of the above table and that arrived at on the total wages shown in column (2) at the prescribed rate is solely due to the rounding off of contributions to the nearest rupee under the rules. Dated the...........................20...... Signature of Employer
With Office Seal
† Rates now enhanced by EPF (Amendment) Act, 1998
Note.—
1. In respect of the Form (3A) sent to the Regional Office during the course of the currency period for the purpose of final settlement of the accounts of the members who has left service details of date and reasons for leaving service, should be furnished under column 7(a) & (b).
2. In respect of those who are not members of the Pension Fund, the employer’s share of contribution to
the EPF will be 12%,10% or 8.33% as the case may be and is to be shown under column 4(a).]

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 0
FORM 4 (Paragraphs 35 and 42 The Employees’ Provident Funds Scheme, 1952 )
Contribution Card for Employees other than Monthly Paid Employees for the Period From......................... To..............................
1. Account No. .............................................................................................................. 2. Name (in block capitals) ............................................... Surname ......................... 3. Caste .......................................................................................................................... 4. Sex ............................................................................................................................. 5. Date of birth as given in Form 2 ............................................................................ 6. Occupation.............................................................................................................. 7. Father’s Name....................................................................................................... 8. Husband’s name........................................................................................................ (for married woman only) 9. Marital status .............................................................................................................
(whether bachelor, spinster, married, widow or widower) 10. Permanent Address ..................................................................................................
Village ............................., Thana .................... Taluk/Sub‐Division ..................... District................................, State.............................................. Signature or left hand thumb impression of member .........................................
11. Signature of person preparing the card ................................................................ 12. Signature of the Manager of the factory or other establishment .................. 13. Registered Number of the factory or other establishment .............................
....................................................................................................................................... 14. Name and address of the factory or other establishment ..............................
.......................................................................................................................................
Particulars of Employment
Registered number of [factory or other establishment]
Duration of employment Remarks Initials of the employer’s authorized clerk
From To
The employer’s and members contribution should be shown separately for each week
Employer’s / member’s total amount refunded
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6
Week 7 Week 8 Week 9 Week 10 Week 11 Week 12 Week 13 Week 14 Week 15
Week 16 Week 17 Week 18 Week 19 Week 20 Week 21 Week 22 Week 23 Week 24
Week 25 Week 26 Week 27 Week 28 Week 29 Week 30 Week 31 Week 32 Week 33
Week 34 Week 35 Week 36 Week 37 Week 38 Week 39 Week 40 Week 41 Week 42
Week 43 Week 44 Week 45 Week 46 Week 47 Week 48 Week 49 Week 50 Week 51
Week 52 Total contribution of the employer Rs P. Signature of the employer’s Head
Clerk or any Authorised Clerk Total contribution by the member Checked and found correct Grand Total Amount refunded Authorized official of the Office of
the Commissioner

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 1
FORM 5 (Paragraph 36(2)(a) of The Employeesʹ Provident Funds Scheme, 1952 and
Paragraph 20(4) of the The Employeesʹ Pension Scheme, 1995)
Return of Employees Qualifying for Membership of the Employeesʹ Provident Fund, Employeesʹ Pension Fund and Employeesʹ Deposit Linked Insurance Fund for the
First Time During the Month of............................ (To be Sent to The Commissioner with Form No. 2) (EPF and EPS)
Name and address of factory/establishment:......................................................
Code No. of factory/establishment...................................................
Sl. No.
Account No. Name of the employee (in block capitals)
Fatherʹs Name or Husbandʹs Name (in case of married
woman)
Date of Birth
Sex Date of joining the Fund
Total period of previous
service as on the date of joining the
Fund (Enclose Scheme
Certificate if applicable)
Remarks
1 2 3 4 5 6 7 8 9
Date.......................... Signature of the Employer or other authorised Officer
of the Establishment
Stamp of the Factory/Establishment
1. This Form should be accompanied by declaration and nomination in Form 2 (EPF). 2. All particulars to be filled in CAPITAL LETTERS.
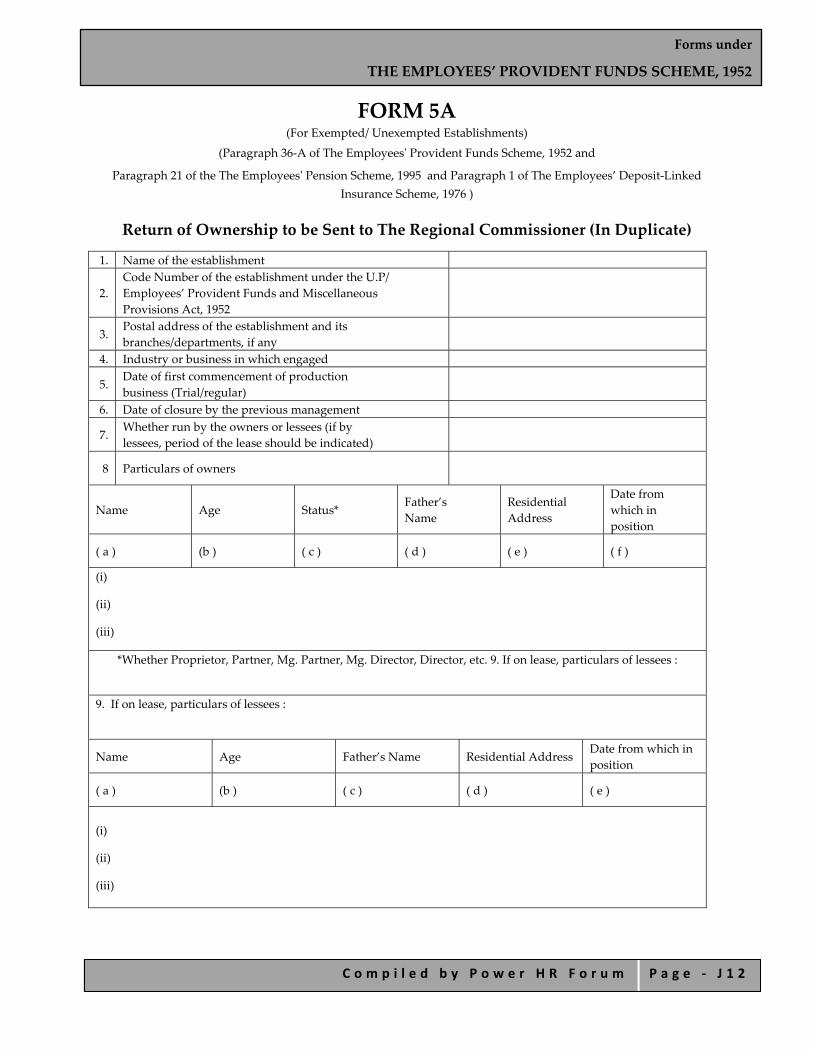
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 2
FORM 5A (For Exempted/ Unexempted Establishments)
(Paragraph 36‐A of The Employeesʹ Provident Funds Scheme, 1952 and
Paragraph 21 of the The Employeesʹ Pension Scheme, 1995 and Paragraph 1 of The Employees’ Deposit‐Linked Insurance Scheme, 1976 )
Return of Ownership to be Sent to The Regional Commissioner (In Duplicate)
1. Name of the establishment
2. Code Number of the establishment under the U.P/ Employees’ Provident Funds and Miscellaneous Provisions Act, 1952
3. Postal address of the establishment and its branches/departments, if any
4. Industry or business in which engaged
5. Date of first commencement of production business (Trial/regular)
6. Date of closure by the previous management
7. Whether run by the owners or lessees (if by lessees, period of the lease should be indicated)
8 Particulars of owners
Name Age Status* Father’s Name
Residential Address
Date from which in position
( a ) (b ) ( c ) ( d ) ( e ) ( f )
(i)
(ii)
(iii)
*Whether Proprietor, Partner, Mg. Partner, Mg. Director, Director, etc. 9. If on lease, particulars of lessees :
9. If on lease, particulars of lessees :
Name Age Father’s Name Residential Address Date from which in position
( a ) (b ) ( c ) ( d ) ( e )
(i)
(ii)
(iii)
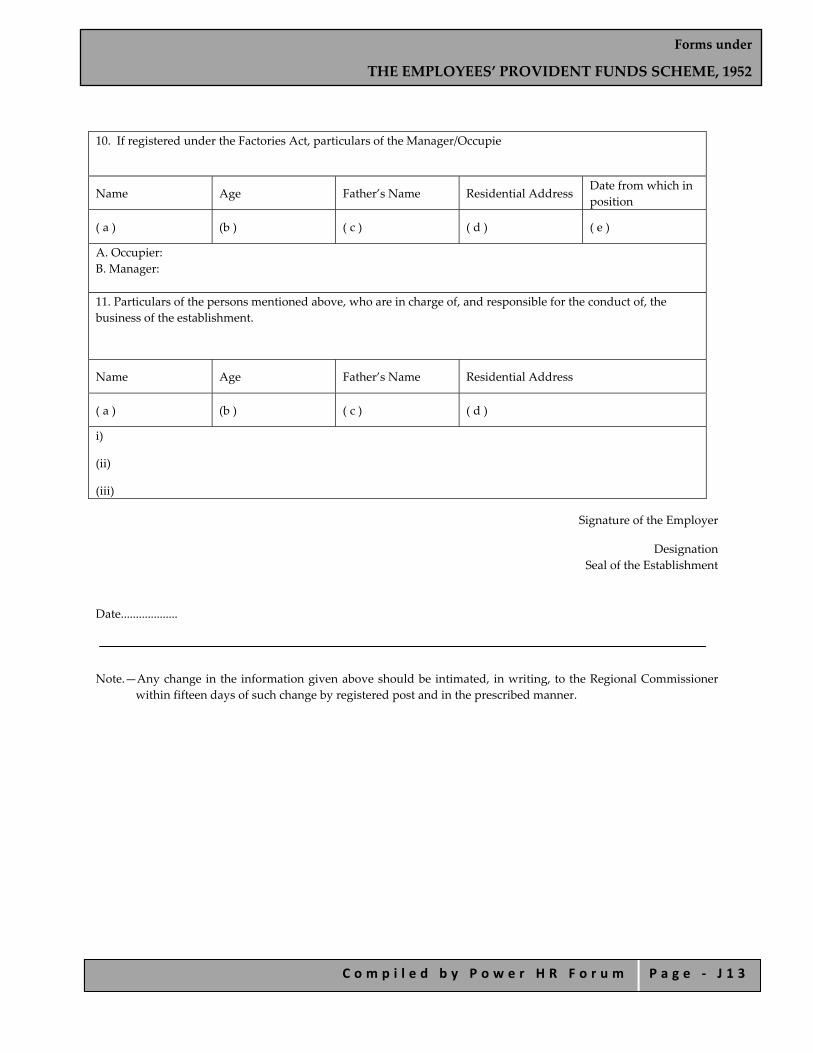
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 3
10. If registered under the Factories Act, particulars of the Manager/Occupie
Name Age Father’s Name Residential Address Date from which in position
( a ) (b ) ( c ) ( d ) ( e )
A. Occupier: B. Manager: 11. Particulars of the persons mentioned above, who are in charge of, and responsible for the conduct of, the business of the establishment.
Name Age Father’s Name Residential Address
( a ) (b ) ( c ) ( d )
i)
(ii)
(iii)
Signature of the Employer
Designation Seal of the Establishment
Date...................
Note.—Any change in the information given above should be intimated, in writing, to the Regional Commissioner within fifteen days of such change by registered post and in the prescribed manner.
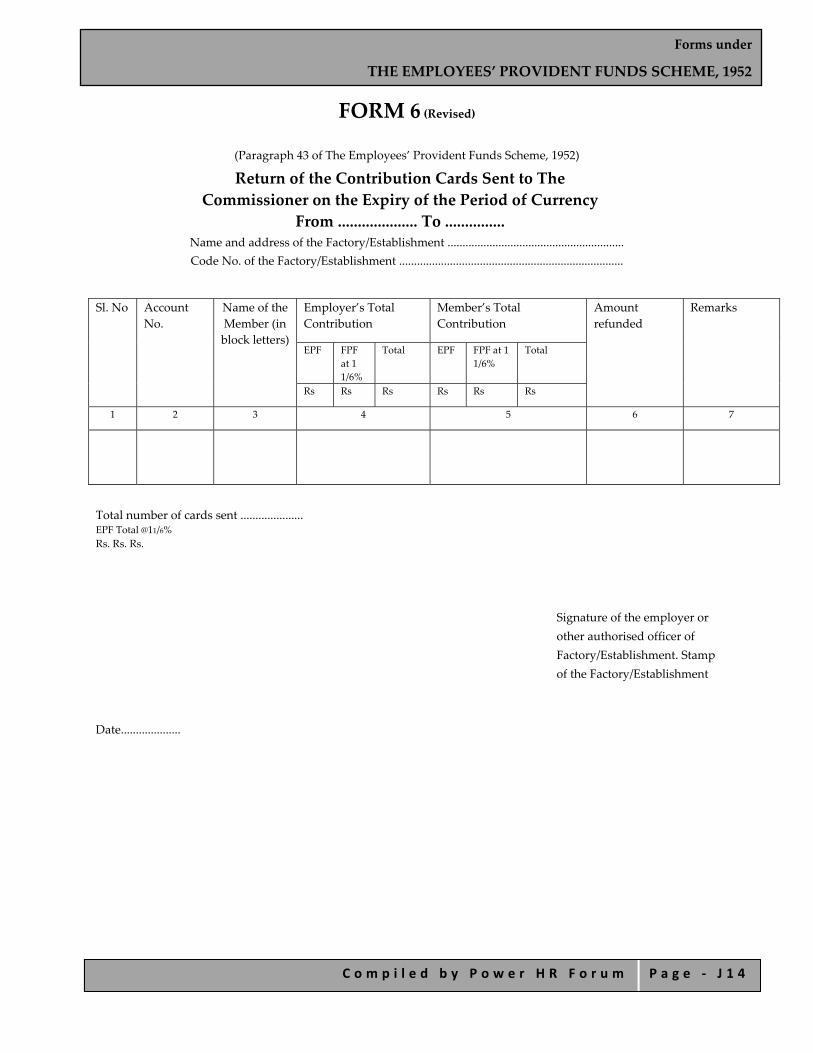
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 4
FORM 6 (Revised)
(Paragraph 43 of The Employees’ Provident Funds Scheme, 1952)
Return of the Contribution Cards Sent to The Commissioner on the Expiry of the Period of Currency
From .................... To ............... Name and address of the Factory/Establishment ........................................................... Code No. of the Factory/Establishment ...........................................................................
Sl. No Account No.
Name of the Member (in block letters)
Employer’s Total Contribution
Member’s Total Contribution
Amount refunded
Remarks
EPF FPF at 1 1/6%
Total EPF FPF at 1 1/6%
Total
Rs Rs Rs Rs Rs Rs
1 2 3 4 5 6 7
Total number of cards sent ..................... EPF Total @11/6% Rs. Rs. Rs.
Signature of the employer or other authorised officer of Factory/Establishment. Stamp of the Factory/Establishment
Date....................
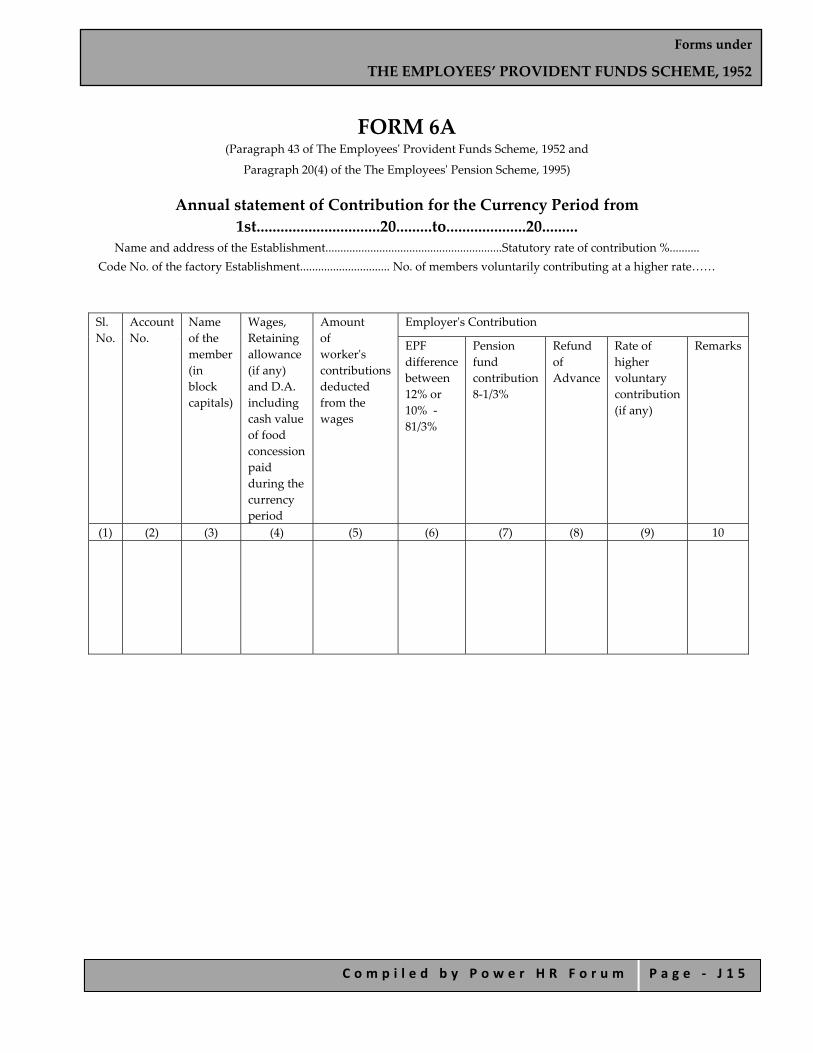
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 5
FORM 6A (Paragraph 43 of The Employeesʹ Provident Funds Scheme, 1952 and
Paragraph 20(4) of the The Employeesʹ Pension Scheme, 1995)
Annual statement of Contribution for the Currency Period from 1st...............................20.........to....................20.........
Name and address of the Establishment...........................................................Statutory rate of contribution %.......... Code No. of the factory Establishment.............................. No. of members voluntarily contributing at a higher rate……
Sl. No.
Account No.
Name of the member (in block capitals)
Wages, Retaining allowance (if any) and D.A. including cash value of food concession paid during the currency period
Amount of workerʹs contributions deducted from the wages
Employerʹs Contribution
EPF difference between 12% or 10% ‐ 81/3%
Pension fund contribution 8‐1/3%
Refund of Advance
Rate of higher voluntary contribution (if any)
Remarks
(1) (2) (3) (4) (5) (6) (7) (8) (9) 10
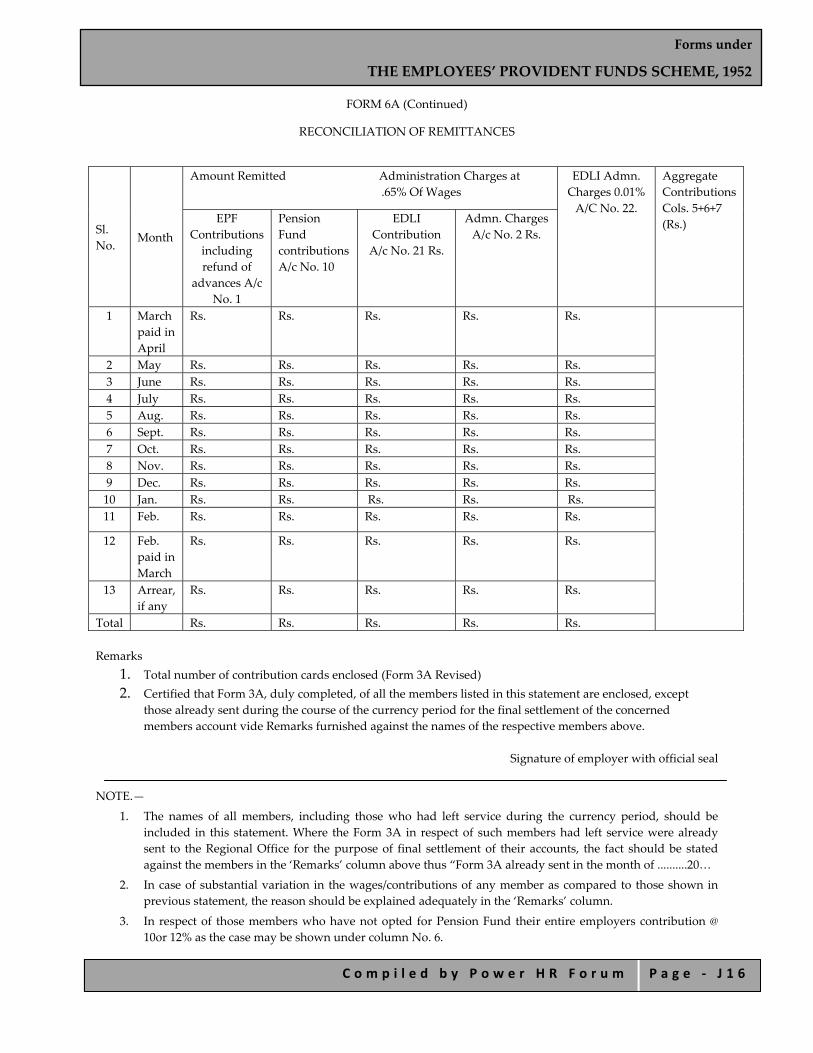
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 6
FORM 6A (Continued)
RECONCILIATION OF REMITTANCES
Sl. No.
Month
Amount Remitted Administration Charges at .65% Of Wages
EDLI Admn. Charges 0.01% A/C No. 22.
Aggregate Contributions Cols. 5+6+7 (Rs.)
EPF Contributions including refund of
advances A/c No. 1
Pension Fund contributions A/c No. 10
EDLI Contribution A/c No. 21 Rs.
Admn. Charges A/c No. 2 Rs.
1 March paid in April
Rs. Rs. Rs. Rs. Rs.
2 May Rs. Rs. Rs. Rs. Rs. 3 June Rs. Rs. Rs. Rs. Rs. 4 July Rs. Rs. Rs. Rs. Rs. 5 Aug. Rs. Rs. Rs. Rs. Rs. 6 Sept. Rs. Rs. Rs. Rs. Rs. 7 Oct. Rs. Rs. Rs. Rs. Rs. 8 Nov. Rs. Rs. Rs. Rs. Rs. 9 Dec. Rs. Rs. Rs. Rs. Rs. 10 Jan. Rs. Rs. Rs. Rs. Rs. 11 Feb. Rs. Rs. Rs. Rs. Rs.
12 Feb. paid in March
Rs. Rs. Rs. Rs. Rs.
13 Arrear, if any
Rs. Rs. Rs. Rs. Rs.
Total Rs. Rs. Rs. Rs. Rs. Remarks
1. Total number of contribution cards enclosed (Form 3A Revised) 2. Certified that Form 3A, duly completed, of all the members listed in this statement are enclosed, except
those already sent during the course of the currency period for the final settlement of the concerned members account vide Remarks furnished against the names of the respective members above.
Signature of employer with official seal
NOTE.—
1. The names of all members, including those who had left service during the currency period, should be included in this statement. Where the Form 3A in respect of such members had left service were already sent to the Regional Office for the purpose of final settlement of their accounts, the fact should be stated against the members in the ‘Remarks’ column above thus “Form 3A already sent in the month of ..........20…
2. In case of substantial variation in the wages/contributions of any member as compared to those shown in previous statement, the reason should be explained adequately in the ‘Remarks’ column.
3. In respect of those members who have not opted for Pension Fund their entire employers contribution @ 10or 12% as the case may be shown under column No. 6.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 7
FORM 9 Application for Review Filed under Sub‐Section (1) of Section 7B
of the Employees’ Provident Funds and Miscellaneous Provisions Act, 1952
(Paragraph 79A)
For use in Commissioner’s Office
Date of filing or
Date of receipt by post
Registration No.
Signature for Commissioner
1. Name of the Applicant ………………………………………………….
2. Designation of the applicant or his relationship with the factory/establishment (whether owner/partner/
director/manager, etc., to be indicated)………………...........................................................................
3. Name and complete address of the factory/establishment ……………………………………………………
4. Address of the employer for service of notice/summons. …………………………………………………….
5. Particulars of the order against which the review application is filed — ……………………………………
i. Order No. ………………………………
ii. Date of order ……………………………
iii. Passed by ………………………………..
iv. Subject in brief ………………………………
6. Main ground(s) on which the application for review has been made and the relief(s) sought. (If necessary, attach a duly signed statement with copies of the documents relied upon marked as A1, A2, A3 and so on…………………………………………………………………………
VERIFICATION
I................... (name of the applicant) s/o, d/o, w/o................... age .............. working as ................. resident of .................... do hereby verify that the contents of particulars given at Sl. Nos. 1 to 6 above are true to the best of my knowledge and belief and I have not suppressed any material fact. I further declare that—
i. I am filing the application within 45 days from the date of the original order.
ii. I have not preferred any appeal against the original order under the Employees’ Provident Funds and Miscellaneous Provisions Act, 1952.
iii. I am filing with this application, the original document authorizing me to represent the aggrieved person (applicable only in cases where the application is filed by agent, advocate or other representative).
Place........................ Signature. Date........................

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 8
FORM 10 (Paragraph 36 92)(b) of the Employees’ Provident Funds Scheme, 1952 )
Return of Members Leaving Service during the Month of Name and address of factory /Estt.. ……………………………………… Code No. Sl. No. Account No. Name of
Member (in block letters)
Father’s name (or husband’s name in case of married women)
Date of leaving service
* Reasons of leaving service
Remarks
1 2 3 4 5 6 7
Signature of employer or other authorized officer
Date Stamp of the Factory/ Establishment * Please state whether the member is (a) retiring according to para 69(1)(a) or (b) of the scheme (b) leaving India for permanent settlement abroad (c) retrenchment, (cc) part or ltotal disablement due to employment injury (d) ordinarily dismissed for serious or willful misconduct (e) discharged (f) resigning from or leaving service (g) taking up employment elsewhere. (The name and address of the employee should be stated), (h) death (i) attainment of the age of 58 years. A request for deduction for the account of a member dismissed for serious and willful misconduct should be reported by the following certificate. “Certified that the member mentioned at Serial No…………………. Shri……………………….. was dismissed for serios and willful misconduct. I recommend that the employer’s contribution for…………. should be forfeited from the account in the fund. A copy of the order of dismissal is enclosed.” “Certified that the member mentioned at serial No. ………………… Shri……………………. was paid/not paid retrenchment compensation of rupees ………………………. under the Industrial Disputes Act, 1947. “
Signature of the employer (Also filled in Form No. 5)

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 1 9
FORM 11 ( For enexempted establishments only)
(Paragraph 34 of The Employeesʹ Provident Funds Scheme, 1952 and
Paragraph 19 of the The Employeesʹ Family Pension Scheme, 1971)
Declaration by a Person Taking up Employment in an Establishment in Which the Employees’ Provident Fund and Family Pension Scheme are in Force:
I …………………………… ** son/wife/daughter of ………………………… ……………………………………………… (Name) Hereby solemnly declare that ‐ (a) I was last employed in……………………………………………………………………
( Name and full address of the establishment) And left service on ……………………………… (prior to that I was employee……………………….. from ………………date………………….to…………………….date (b) ** I was a member of ……………………………… Provident fund ** and also /** but not __________ of the Family Pension Fund from ………………….. to………………….. and my account number(s) was/were …………………………… /……………………………. / ………………………./ (c) ** I have / have not withdrawn the amount of any Provident Fund / Family Pension Scheme. (d) ** I have /have not drawn any superannuation benefits in respect of my past service from any employer. (e) I have never been a member of any Provident Fund and/or Family Pension Scheme. (f) I am drawing/ not drawing pension under EPS 95. (g) I am a holder / not holder of scheme certificate. (h) Scheme certificate surrendered/ not surrendered Date ………………………
Signature or ** right/left thumb impression of the employee
(To be filled in by the employer only when the person employed had not already been a member of the Employee’s Provident Fund ) Shri……………….. …………………………….is appointed as ……………………………………………… (Name of employee) (Designation) In …………………………………………………………………………………………………………………………..
( Name of factory/establishment) With effect from ……………………………………………………
(date of appointment)

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 0
Date of completion of 120 actual working days in a period of 6 months or less or six months* continuous service or date of confirmation whichever is earliest. Date of admission as member of Employee’s Provident Fund…………………. Account No………………..
Signature of the Manager or other Authorized officer Date * (1) Strike whichever is not applicable N.B.‐ The principal employer should have filled it up also in respect of employees to be employed by or through a contractor.
(For unexempted establishments only)
Contract Rest Total Total No. of employees …………………………………
Total No. of subscribers ………………………
From……………..to……….No. of days worked
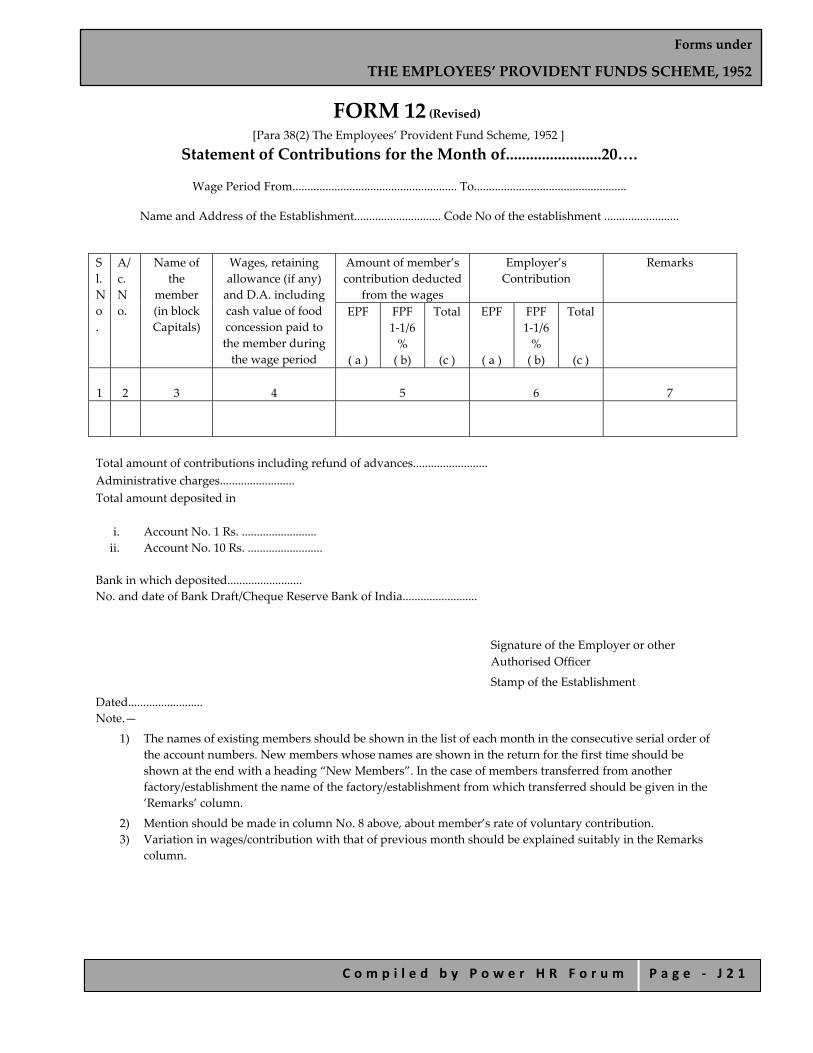
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 1
FORM 12 (Revised) [Para 38(2) The Employees’ Provident Fund Scheme, 1952 ]
Statement of Contributions for the Month of........................20….
Wage Period From....................................................... To...................................................
Name and Address of the Establishment............................. Code No of the establishment .........................
Sl. No.
A/c. No.
Name of the
member (in block Capitals)
Wages, retaining allowance (if any) and D.A. including cash value of food concession paid to the member during the wage period
Amount of member’s contribution deducted
from the wages
Employer’s Contribution
Remarks
EPF
( a )
FPF 1‐1/6 % ( b)
Total
(c )
EPF
( a )
FPF 1‐1/6 % ( b)
Total
(c )
1 2 3 4 5
6
7
Total amount of contributions including refund of advances......................... Administrative charges......................... Total amount deposited in
i. Account No. 1 Rs. ......................... ii. Account No. 10 Rs. .........................
Bank in which deposited......................... No. and date of Bank Draft/Cheque Reserve Bank of India.........................
Signature of the Employer or other Authorised Officer
Stamp of the Establishment
Dated......................... Note.—
1) The names of existing members should be shown in the list of each month in the consecutive serial order of the account numbers. New members whose names are shown in the return for the first time should be shown at the end with a heading “New Members”. In the case of members transferred from another factory/establishment the name of the factory/establishment from which transferred should be given in the ’Remarks’ column.
2) Mention should be made in column No. 8 above, about member’s rate of voluntary contribution. 3) Variation in wages/contribution with that of previous month should be explained suitably in the Remarks
column.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 2
FORM 12A (Revised)
(For Unexempted Establishments only) [Proviso to paragraph 38(2) of The Employees’ Provident Funds Scheme, 1952]
Statement of Contribution for the Month of...............
Name and address of the establishment........................................................................... Code No. of the Establishment..........................................................................................
Total number of subscribers
Wages on which contributions are recovered
Amount of contributions due as per recoveries made in the wages/ acquaintance register Worker’s Share
Employer’s Share
EPF
( a )
FPF 1‐1/6 % ( b)
Total
(c )
EPF
( a )
FPF 1‐1/6 % ( b)
Total
(c )
1
2
3
4
Amount of contributions remitted in Account No. 1 and 10
Total number of subscribers
Worker’s Share
Employer’s Share
Total
EPF
( a )
FPF 1‐1/6 %
( b)
Total
(c )
EPF
( a )
FPF 1‐1/6 %
( b)
Total
(c )
5
6
7
8
1. Total amount remitted in Account No. 1 Rs................................................................
Date of remittance........................................................................
2. Total amount remitted in Account No. 10 Rs................................................. Date of remittance................................................

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 3
Amount of Adm. Charges due 0.37% of the amount of wages shown in column 2
Amount of Admn. Charges remitted in A/c No. 2
Date of remittance
9
10
11
Name and location of the bank in which remitted or No. and date of the cheque/draft sent to Regional Officer
Whether the triplicate challan receipt is enclosed, if not, state
reason
Remarks
12
13
14
Account No. 1................................................ ………………….................................... Account No. 10.............................................. ………………….................................... Account No. 2................................................ …………………....................................
No. as per last month’s return
(+) No. of New Subscribers—vide Form 5
(–) No. of Subscribers left service—vide Form 10
*Net Total
This should tally with the figure given at the top right hand corner of this Form
Total No. of Employees.............................. Contract ..............Rest ..............Total......... Total No. of Subscribers.............................
Currency period form 1st April, 20..... to 31st March, 20...... Statutory Rate of Contribution...................................... No. of members voluntarily contributing at higher than the statutory rate...............
Signature of the Employer (with official seal)
Date...........................
Notes.—
1) If there is any substantial variation between the wages and amount of contribution shown above and those shown in the last month’s return suitable explanation should be given in the ‘Remarks’ column.
2) If any arrears of contributions or damages are included in the figures under Columns 6 to 8,, suitable details indicating the circumstances, amount, No. of subscribers and the period involved should be furnished in the ‘Remarks’ column or on the reverse.
3) Remittance shall invariably be made by deposits in the State Bank of India or its subsidiaries.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 4
FORM 13 Revised For office use only
Date Seal/Reg No…………………….. [Para 57 of The Employee Provident Fund Scheme, 1952]
Application for Transfer of E.P.F. Account
Note.— i. To be submitted by the member to the present employer for onward transmission to the
Commissioner, EPF by whom the transfer is to be effected. ii. In case the P.F. transfer is due from the P.F. Trust of an exempted establishment, the application should be
sent directly by the employer to the P.F. Trust of the exempted establishment, with a copy to the RPFC concerned for details of the Family Pension membership.
To, To, The Commissioner, M/s. ........................................... Employees’ Provident Fund
..................................................... .................................................. .....................................................
[To be filled in, if Note (ii) above is applicable]
Sir,
I request that my Provident Fund balance along with the membership details in Family Pension Fund may please be transferred to my present account under intimation to me.
Necessary particulars are furnished below: 1. Name ...................................................
2. Fathers/husband’s name in case of female..................................................
3. Name and address of previous employer ...................................................
4. EPF account number allotted by previous employer ...................................................
5. With whom the PF account of the previous employer is maintained
With Regional PF commissioner With provident fund trust
.................................................. …………………………………..
6. Previous account number allotted by the employer (if allotted separately) ...................................................
7. Date of leaving service with previous employer ...................................................
8. Date of joining the present employer ....................................................
Date......................... Signature/left hand thumb impression of the member
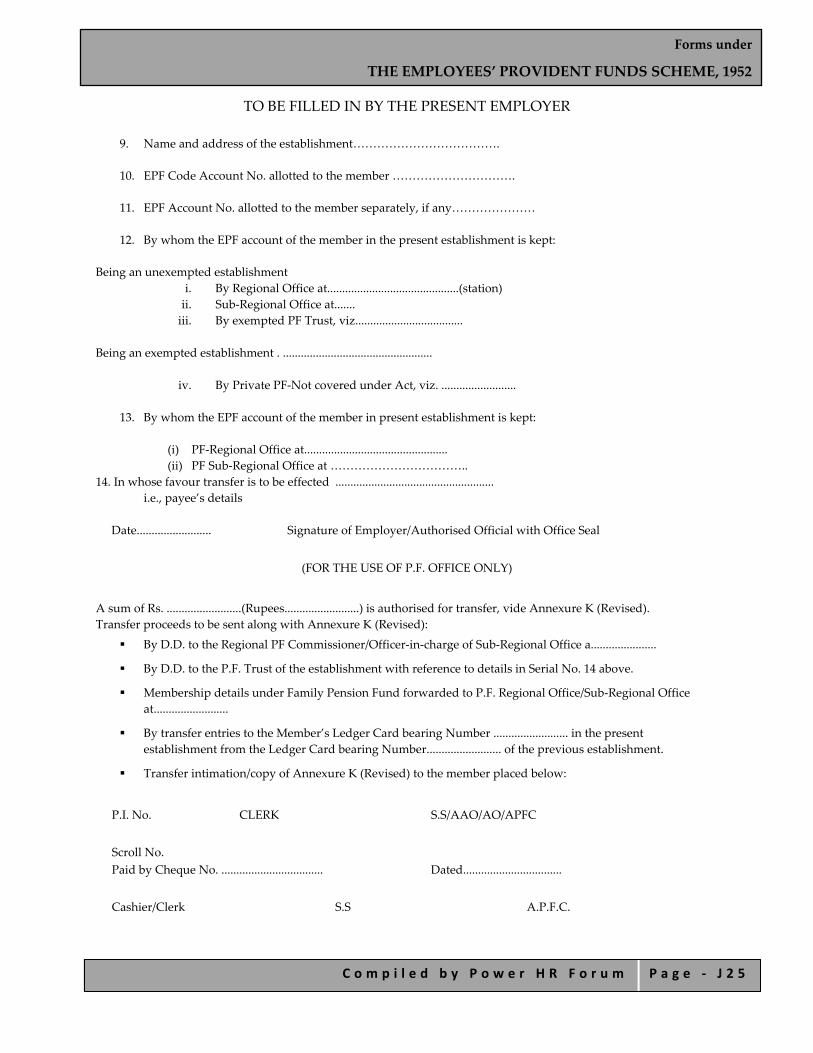
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 5
TO BE FILLED IN BY THE PRESENT EMPLOYER
9. Name and address of the establishment……………………………….
10. EPF Code Account No. allotted to the member ………………………….
11. EPF Account No. allotted to the member separately, if any…………………
12. By whom the EPF account of the member in the present establishment is kept:
Being an unexempted establishment i. By Regional Office at............................................(station) ii. Sub‐Regional Office at....... iii. By exempted PF Trust, viz....................................
Being an exempted establishment . ..................................................
iv. By Private PF‐Not covered under Act, viz. .........................
13. By whom the EPF account of the member in present establishment is kept:
(i) PF‐Regional Office at................................................ (ii) PF Sub‐Regional Office at ……………………………..
14. In whose favour transfer is to be effected ..................................................... i.e., payee’s details
Date......................... Signature of Employer/Authorised Official with Office Seal
(FOR THE USE OF P.F. OFFICE ONLY)
A sum of Rs. .........................(Rupees.........................) is authorised for transfer, vide Annexure K (Revised). Transfer proceeds to be sent along with Annexure K (Revised):
By D.D. to the Regional PF Commissioner/Officer‐in‐charge of Sub‐Regional Office a......................
By D.D. to the P.F. Trust of the establishment with reference to details in Serial No. 14 above.
Membership details under Family Pension Fund forwarded to P.F. Regional Office/Sub‐Regional Office at.........................
By transfer entries to the Member’s Ledger Card bearing Number ......................... in the present establishment from the Ledger Card bearing Number......................... of the previous establishment.
Transfer intimation/copy of Annexure K (Revised) to the member placed below:
P.I. No. CLERK S.S/AAO/AO/APFC
Scroll No. Paid by Cheque No. .................................. Dated.................................
Cashier/Clerk S.S A.P.F.C.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 6
FORM 13A (Revised) THE EMPLOYEES PROVIDENT FUND SCHEME, 1952
[Para 57]
Application for Inter‐Regional Transfer of Accounts to be Submitted through the Present Employer
To,
The Commissioner, Employees’ Provident Fund ................................................
Sir, I request that the Provident Fund and Family Pension Account may please be transferred to my present account under intimation to me. Necessary particulars regarding Provident Fund and Family Pension Fund are furnished below:
1. Name.............................................................................................................................. 2. Father’s name (or husband’s name in case of married woman)......................... 3. Name and address of previous employer, whether
unexempted/exempted/uncovered........................................................................... 4.
a) Previous Provident Fund Account No. ............................................................. b) Previous Family Pension Fund Account No. ...................................................
5. Date of leaving service with previous employer.................................................... 6. Name and address of the employer......................................................................... 7. Whether unexempted/exempted/uncovered.......................................................... 8.
a) Present Provident Fund Account No. ................................................................. b) Present Family Pension Fund Account No. (if any).........................................
9. Date of joining with present employer.........................
*Signature or left/right‐hand thumb impression of the member
Endorsement to be completed by the forwarding authority
Forwarded with the particulars furnished above duly verified. **(The rules of our private provident fund permit such transfer and hence the transfer may be made. The cheque may be drawn in favour of......................... including/excluding bank collection charges.)
Signature of employer or other authorised officer of the
factory/establishment with official seal
* Left‐hand thumb‐impression in the case of illiterate male member and right‐hand thumb impression in the case of illiterate female member.
** Will apply in case of transfer to uncovered establishment. Note.—In case of transfer to provident fund accumulation to uncovered establishment, the benefit under Family Pension Fund Scheme should be paid to the member.
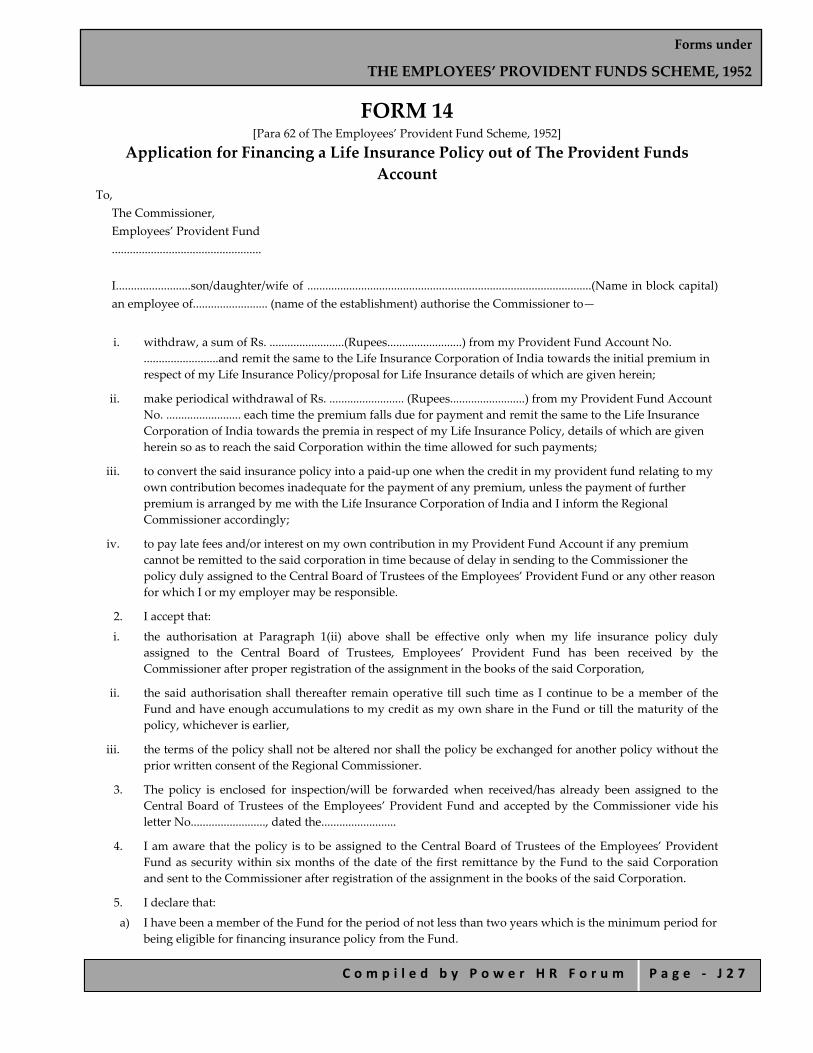
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 7
FORM 14 [Para 62 of The Employees’ Provident Fund Scheme, 1952]
Application for Financing a Life Insurance Policy out of The Provident Funds Account
To, The Commissioner, Employees’ Provident Fund .................................................. I.........................son/daughter/wife of ...............................................................................................(Name in block capital) an employee of......................... (name of the establishment) authorise the Commissioner to—
i. withdraw, a sum of Rs. .........................(Rupees.........................) from my Provident Fund Account No. .........................and remit the same to the Life Insurance Corporation of India towards the initial premium in respect of my Life Insurance Policy/proposal for Life Insurance details of which are given herein;
ii. make periodical withdrawal of Rs. ......................... (Rupees.........................) from my Provident Fund Account No. ......................... each time the premium falls due for payment and remit the same to the Life Insurance Corporation of India towards the premia in respect of my Life Insurance Policy, details of which are given herein so as to reach the said Corporation within the time allowed for such payments;
iii. to convert the said insurance policy into a paid‐up one when the credit in my provident fund relating to my own contribution becomes inadequate for the payment of any premium, unless the payment of further premium is arranged by me with the Life Insurance Corporation of India and I inform the Regional Commissioner accordingly;
iv. to pay late fees and/or interest on my own contribution in my Provident Fund Account if any premium cannot be remitted to the said corporation in time because of delay in sending to the Commissioner the policy duly assigned to the Central Board of Trustees of the Employees’ Provident Fund or any other reason for which I or my employer may be responsible.
2. I accept that:
i. the authorisation at Paragraph 1(ii) above shall be effective only when my life insurance policy duly assigned to the Central Board of Trustees, Employees’ Provident Fund has been received by the Commissioner after proper registration of the assignment in the books of the said Corporation,
ii. the said authorisation shall thereafter remain operative till such time as I continue to be a member of the Fund and have enough accumulations to my credit as my own share in the Fund or till the maturity of the policy, whichever is earlier,
iii. the terms of the policy shall not be altered nor shall the policy be exchanged for another policy without the prior written consent of the Regional Commissioner.
3. The policy is enclosed for inspection/will be forwarded when received/has already been assigned to the Central Board of Trustees of the Employees’ Provident Fund and accepted by the Commissioner vide his letter No........................., dated the.........................
4. I am aware that the policy is to be assigned to the Central Board of Trustees of the Employees’ Provident Fund as security within six months of the date of the first remittance by the Fund to the said Corporation and sent to the Commissioner after registration of the assignment in the books of the said Corporation.
5. I declare that:
a) I have been a member of the Fund for the period of not less than two years which is the minimum period for being eligible for financing insurance policy from the Fund.
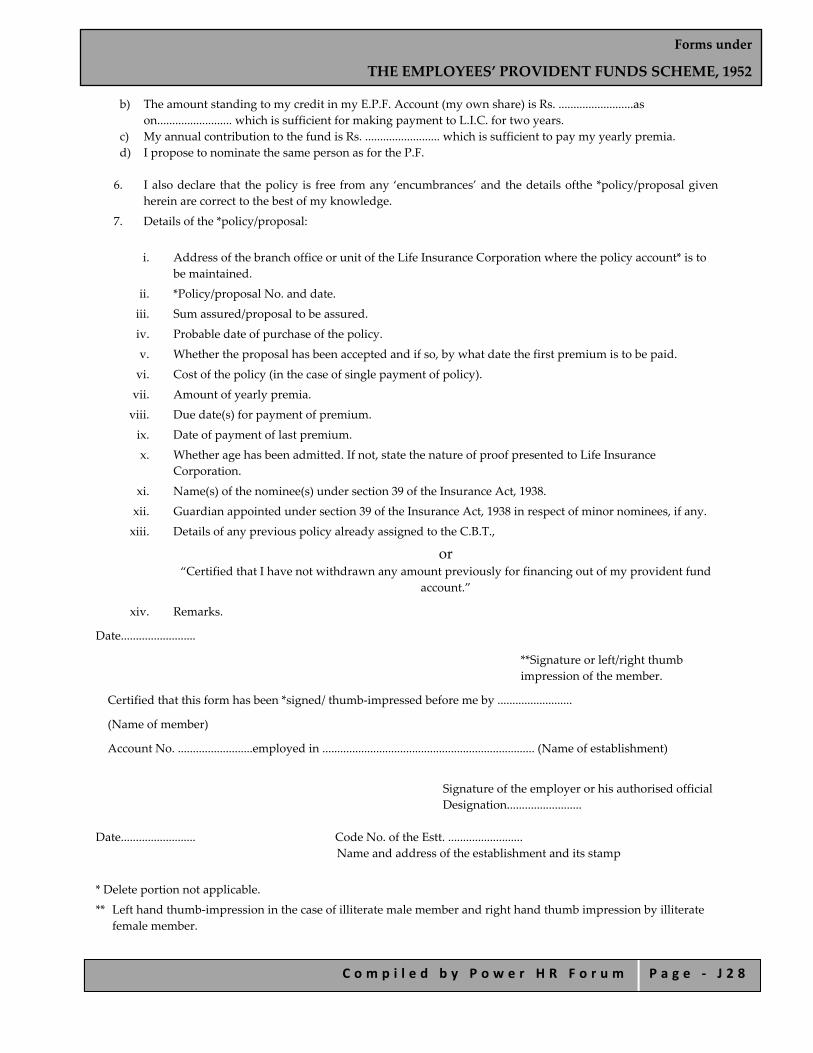
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 8
b) The amount standing to my credit in my E.P.F. Account (my own share) is Rs. .........................as on......................... which is sufficient for making payment to L.I.C. for two years.
c) My annual contribution to the fund is Rs. ......................... which is sufficient to pay my yearly premia. d) I propose to nominate the same person as for the P.F.
6. I also declare that the policy is free from any ‘encumbrances’ and the details ofthe *policy/proposal given
herein are correct to the best of my knowledge.
7. Details of the *policy/proposal:
i. Address of the branch office or unit of the Life Insurance Corporation where the policy account* is to
be maintained.
ii. *Policy/proposal No. and date.
iii. Sum assured/proposal to be assured.
iv. Probable date of purchase of the policy.
v. Whether the proposal has been accepted and if so, by what date the first premium is to be paid.
vi. Cost of the policy (in the case of single payment of policy).
vii. Amount of yearly premia.
viii. Due date(s) for payment of premium.
ix. Date of payment of last premium.
x. Whether age has been admitted. If not, state the nature of proof presented to Life Insurance Corporation.
xi. Name(s) of the nominee(s) under section 39 of the Insurance Act, 1938.
xii. Guardian appointed under section 39 of the Insurance Act, 1938 in respect of minor nominees, if any.
xiii. Details of any previous policy already assigned to the C.B.T.,
or “Certified that I have not withdrawn any amount previously for financing out of my provident fund
account.”
xiv. Remarks.
Date.........................
**Signature or left/right thumb impression of the member.
Certified that this form has been *signed/ thumb‐impressed before me by .........................
(Name of member)
Account No. .........................employed in ....................................................................... (Name of establishment)
Signature of the employer or his authorised official Designation.........................
Date......................... Code No. of the Estt. ......................... Name and address of the establishment and its stamp
* Delete portion not applicable.
** Left hand thumb‐impression in the case of illiterate male member and right hand thumb impression by illiterate female member.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 2 9
For use in Regional Commissioner’s Office
(ACCOUNTS SECTION)
Please furnish the following information in respect of the subscriber:
Average of yearly Contribution (employee’s share only) on the basis of recent 12 months Form No. 12
Total contribution (Employee’s share only) as on
Whether any other L.I.P. advance has been granted before. If so, mention the date of withdrawal
Whether the subscriber has contributed for two years
The above case has been examined vide Paragraphs 62 to 64 of the Employees’ Provident Funds Scheme, 1952. A sum of Rs. ......................... (Rupees.........................) may be paid.
Clerk Head Clerk Accounts Officer R.P.F.C.
INSURANCE SECTION D.P. Sheet prepared and put up for signature
Clerk (Ins.) H.C. (Ins.) Accounts Officer R.P.F.C.
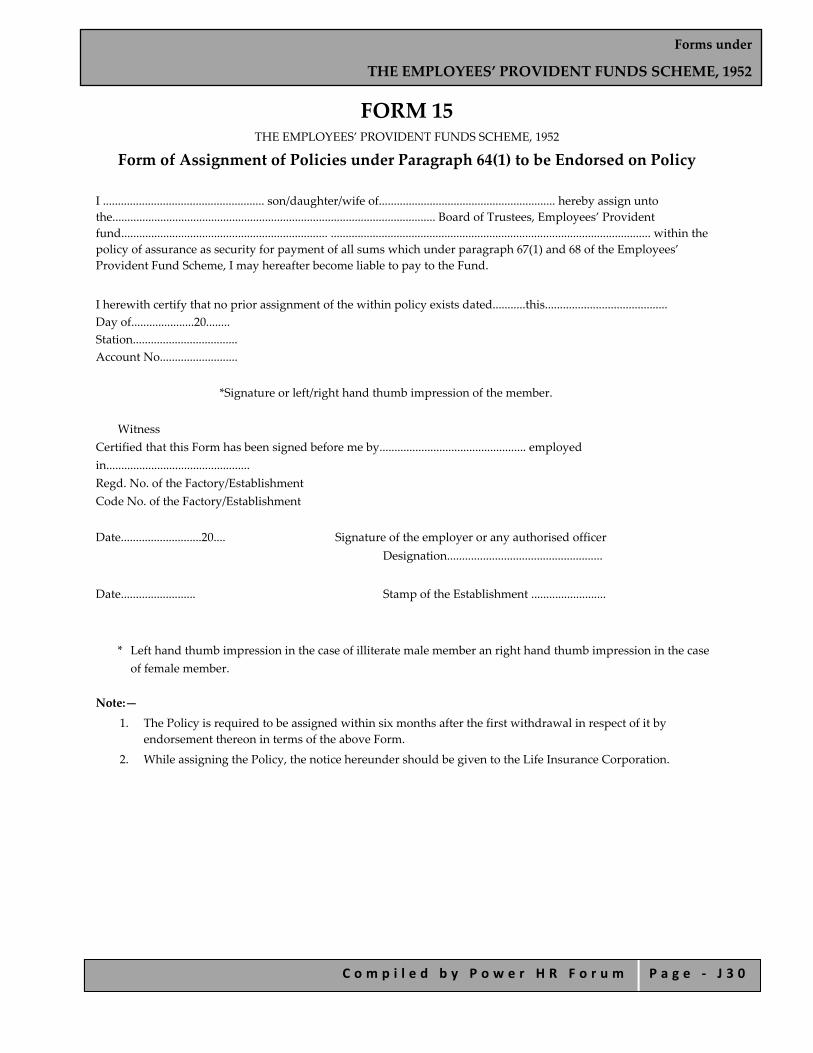
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 0
FORM 15 THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
Form of Assignment of Policies under Paragraph 64(1) to be Endorsed on Policy I ...................................................... son/daughter/wife of........................................................... hereby assign unto the............................................................................................................ Board of Trustees, Employees’ Provident fund..................................................................... ........................................................................................................... within the policy of assurance as security for payment of all sums which under paragraph 67(1) and 68 of the Employees’ Provident Fund Scheme, I may hereafter become liable to pay to the Fund.
I herewith certify that no prior assignment of the within policy exists dated...........this......................................... Day of.....................20........ Station................................... Account No..........................
*Signature or left/right hand thumb impression of the member.
Witness Certified that this Form has been signed before me by................................................. employed in................................................ Regd. No. of the Factory/Establishment Code No. of the Factory/Establishment Date...........................20.... Signature of the employer or any authorised officer
Designation....................................................
Date......................... Stamp of the Establishment .........................
* Left hand thumb impression in the case of illiterate male member an right hand thumb impression in the case of female member.
Note:—
1. The Policy is required to be assigned within six months after the first withdrawal in respect of it by endorsement thereon in terms of the above Form.
2. While assigning the Policy, the notice hereunder should be given to the Life Insurance Corporation.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 1
NOTICE
To The Divisional Manager, The Life Insurance Corporation of India. Unit........................................... Subject: Assignment of Policy No........................
Notice is hereby given that policy No............................... for Rs. ................................. on the life of Shri/Shrimati............................................................................................ as on this........................................... day of...................................20.... been assigned in favour of Central Board of Trustees, Employees’ Provident Fund by Shri/Shrimati...........................................
2. The said policy is enclosed. Please have the assignment registered in books and return the policy to the Regional Provident Fund Commissioner.................................... State.
(give complete address)
Yours faithfully, Signature of the Assignee
Full Address
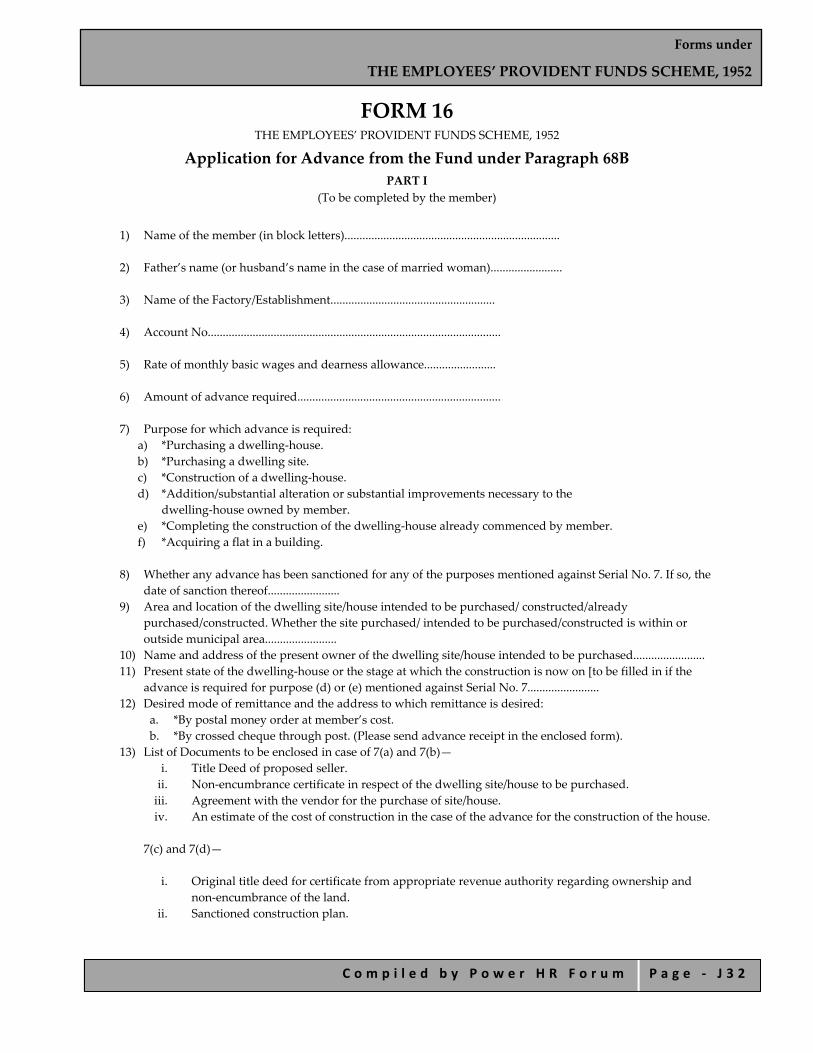
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 2
FORM 16 THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
Application for Advance from the Fund under Paragraph 68B PART I
(To be completed by the member)
1) Name of the member (in block letters)........................................................................
2) Father’s name (or husband’s name in the case of married woman)........................
3) Name of the Factory/Establishment.......................................................
4) Account No..................................................................................................
5) Rate of monthly basic wages and dearness allowance........................
6) Amount of advance required....................................................................
7) Purpose for which advance is required:
a) *Purchasing a dwelling‐house. b) *Purchasing a dwelling site. c) *Construction of a dwelling‐house. d) *Addition/substantial alteration or substantial improvements necessary to the
dwelling‐house owned by member. e) *Completing the construction of the dwelling‐house already commenced by member. f) *Acquiring a flat in a building.
8) Whether any advance has been sanctioned for any of the purposes mentioned against Serial No. 7. If so, the
date of sanction thereof........................ 9) Area and location of the dwelling site/house intended to be purchased/ constructed/already
purchased/constructed. Whether the site purchased/ intended to be purchased/constructed is within or outside municipal area........................
10) Name and address of the present owner of the dwelling site/house intended to be purchased........................ 11) Present state of the dwelling‐house or the stage at which the construction is now on [to be filled in if the
advance is required for purpose (d) or (e) mentioned against Serial No. 7........................ 12) Desired mode of remittance and the address to which remittance is desired:
a. *By postal money order at member’s cost. b. *By crossed cheque through post. (Please send advance receipt in the enclosed form).
13) List of Documents to be enclosed in case of 7(a) and 7(b)— i. Title Deed of proposed seller. ii. Non‐encumbrance certificate in respect of the dwelling site/house to be purchased. iii. Agreement with the vendor for the purchase of site/house. iv. An estimate of the cost of construction in the case of the advance for the construction of the house.
7(c) and 7(d)—
i. Original title deed for certificate from appropriate revenue authority regarding ownership and
non‐encumbrance of the land. ii. Sanctioned construction plan.
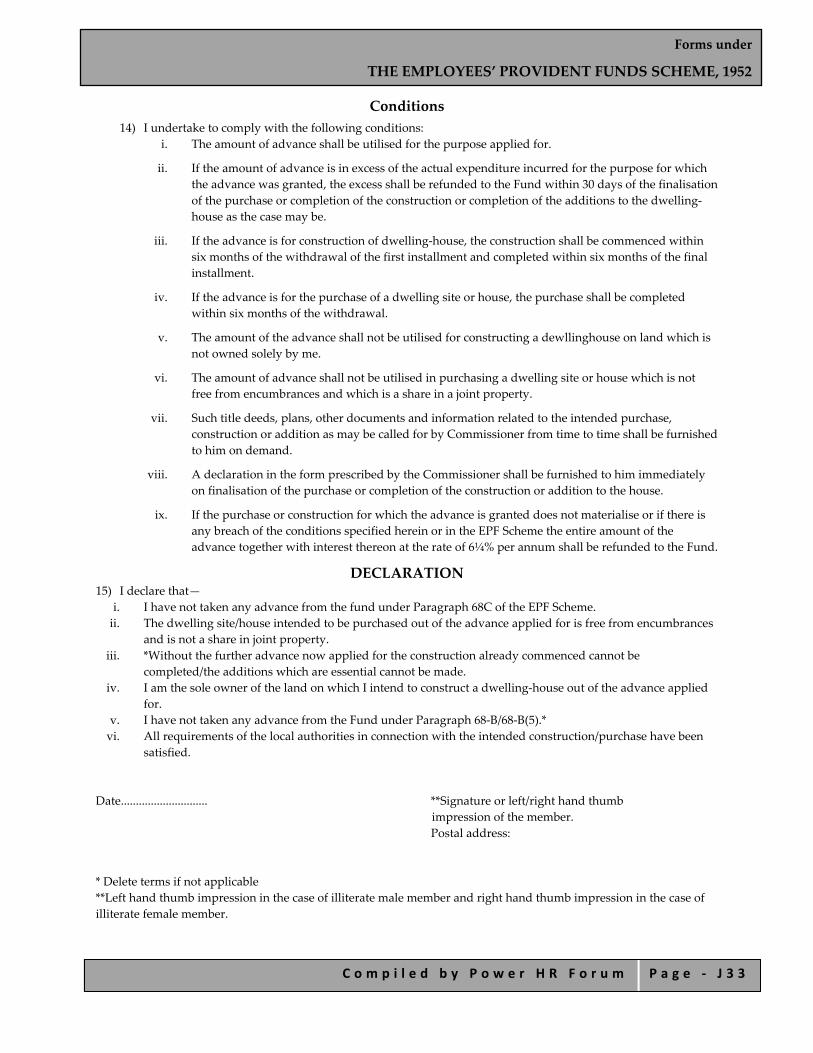
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 3
Conditions 14) I undertake to comply with the following conditions:
i. The amount of advance shall be utilised for the purpose applied for.
ii. If the amount of advance is in excess of the actual expenditure incurred for the purpose for which the advance was granted, the excess shall be refunded to the Fund within 30 days of the finalisation of the purchase or completion of the construction or completion of the additions to the dwelling‐house as the case may be.
iii. If the advance is for construction of dwelling‐house, the construction shall be commenced within six months of the withdrawal of the first installment and completed within six months of the final installment.
iv. If the advance is for the purchase of a dwelling site or house, the purchase shall be completed within six months of the withdrawal.
v. The amount of the advance shall not be utilised for constructing a dewllinghouse on land which is not owned solely by me.
vi. The amount of advance shall not be utilised in purchasing a dwelling site or house which is not free from encumbrances and which is a share in a joint property.
vii. Such title deeds, plans, other documents and information related to the intended purchase, construction or addition as may be called for by Commissioner from time to time shall be furnished to him on demand.
viii. A declaration in the form prescribed by the Commissioner shall be furnished to him immediately on finalisation of the purchase or completion of the construction or addition to the house.
ix. If the purchase or construction for which the advance is granted does not materialise or if there is any breach of the conditions specified herein or in the EPF Scheme the entire amount of the advance together with interest thereon at the rate of 6¼% per annum shall be refunded to the Fund.
DECLARATION 15) I declare that—
i. I have not taken any advance from the fund under Paragraph 68C of the EPF Scheme. ii. The dwelling site/house intended to be purchased out of the advance applied for is free from encumbrances
and is not a share in joint property. iii. *Without the further advance now applied for the construction already commenced cannot be
completed/the additions which are essential cannot be made. iv. I am the sole owner of the land on which I intend to construct a dwelling‐house out of the advance applied
for. v. I have not taken any advance from the Fund under Paragraph 68‐B/68‐B(5).* vi. All requirements of the local authorities in connection with the intended construction/purchase have been
satisfied.
Date............................. **Signature or left/right hand thumb
impression of the member. Postal address:
* Delete terms if not applicable **Left hand thumb impression in the case of illiterate male member and right hand thumb impression in the case of illiterate female member.
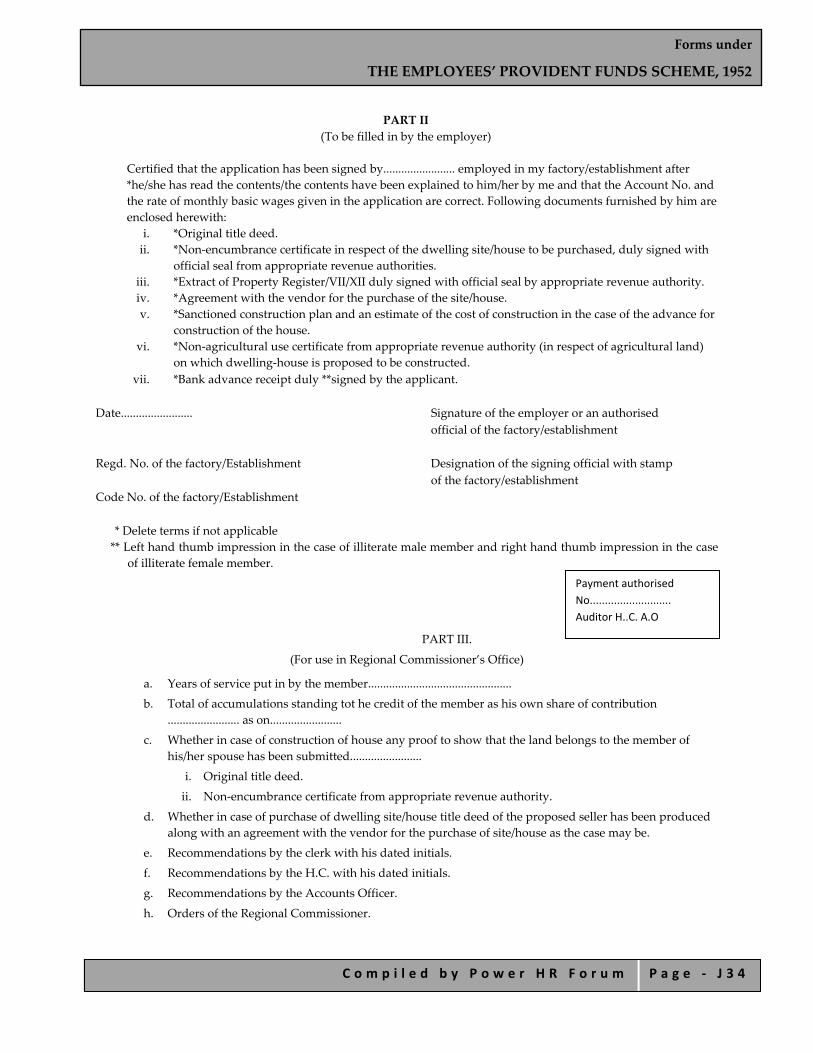
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 4
PART II
(To be filled in by the employer)
Certified that the application has been signed by........................ employed in my factory/establishment after *he/she has read the contents/the contents have been explained to him/her by me and that the Account No. and the rate of monthly basic wages given in the application are correct. Following documents furnished by him are enclosed herewith:
i. *Original title deed. ii. *Non‐encumbrance certificate in respect of the dwelling site/house to be purchased, duly signed with
official seal from appropriate revenue authorities. iii. *Extract of Property Register/VII/XII duly signed with official seal by appropriate revenue authority. iv. *Agreement with the vendor for the purchase of the site/house. v. *Sanctioned construction plan and an estimate of the cost of construction in the case of the advance for
construction of the house. vi. *Non‐agricultural use certificate from appropriate revenue authority (in respect of agricultural land)
on which dwelling‐house is proposed to be constructed. vii. *Bank advance receipt duly **signed by the applicant.
Date........................ Signature of the employer or an authorised official of the factory/establishment Regd. No. of the factory/Establishment Designation of the signing official with stamp of the factory/establishment Code No. of the factory/Establishment
* Delete terms if not applicable ** Left hand thumb impression in the case of illiterate male member and right hand thumb impression in the case
of illiterate female member.
PART III.
(For use in Regional Commissioner’s Office)
a. Years of service put in by the member................................................
b. Total of accumulations standing tot he credit of the member as his own share of contribution ........................ as on........................
c. Whether in case of construction of house any proof to show that the land belongs to the member of his/her spouse has been submitted........................
i. Original title deed.
ii. Non‐encumbrance certificate from appropriate revenue authority.
d. Whether in case of purchase of dwelling site/house title deed of the proposed seller has been produced along with an agreement with the vendor for the purchase of site/house as the case may be.
e. Recommendations by the clerk with his dated initials.
f. Recommendations by the H.C. with his dated initials.
g. Recommendations by the Accounts Officer.
h. Orders of the Regional Commissioner.
Payment authorised No........................... Auditor H..C. A.O

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 5
FORM 19 THE EMPLOYEES PROVIDENT FUND SCHEME, 1952 [Para 72(5)]
Form to be used by a Major Member of Employees’ Provident Fund Scheme, 1952 for Claiming The Employees’ Provident Fund Dues
(Refer instructions) 1. Name of the member (in block letters)........................................................................ 2. Father’s name (or husband’s name in the case of married woman)......................... 3. Name and address of the factory/establishment in which the member was last employed............................... 4. Account No. ................................................. 5. Date of leaving service................................ 6. Reason of leaving service............................ 7. Full postal address (in block letters) Sh./Smt./Kumari.........................
S/o./W/o./D/o............................ .........................Pin
8. Mode of remittance [Put a ‘tick’ in the box against the one opted]
a. By postal money order at my cost To the address given against item No. 7 b. By account payee cheque sent
direct for credit to my S.B. A/c. (Scheduled Bank/PO) under intimation to me.
(Advance stamped receipt furnished below)
Certified that the particulars are true to the best of my knowledge. Date of joining the establishment......................... Date of leaving service.........................
CONTRIBUTION FOR THE CURRENT FINANCIAL YEAR
Month Wages Contribution Period of break, if any
Month Wages Contribution Period of break, if any
Employee Employer Total Employee Employer Total EPF FP EPF FP EPF FP EPF FP EPF FP EPF FP
(Information to be furnished by the employer if the claim form is attested by the employer) Certified that the above contributions have been included in the regular monthly remittances. The applicant has signed/thumb‐impressed before me.
Signature of the employer or Signature or left/right hand thumb authorised official impression of the member Designation and seal Date......................... Encl.........................
S.B. Account No. (in figures).............(in words).............................................. Name of the Bank................................. Branch.................................................... Full address of the branch..................
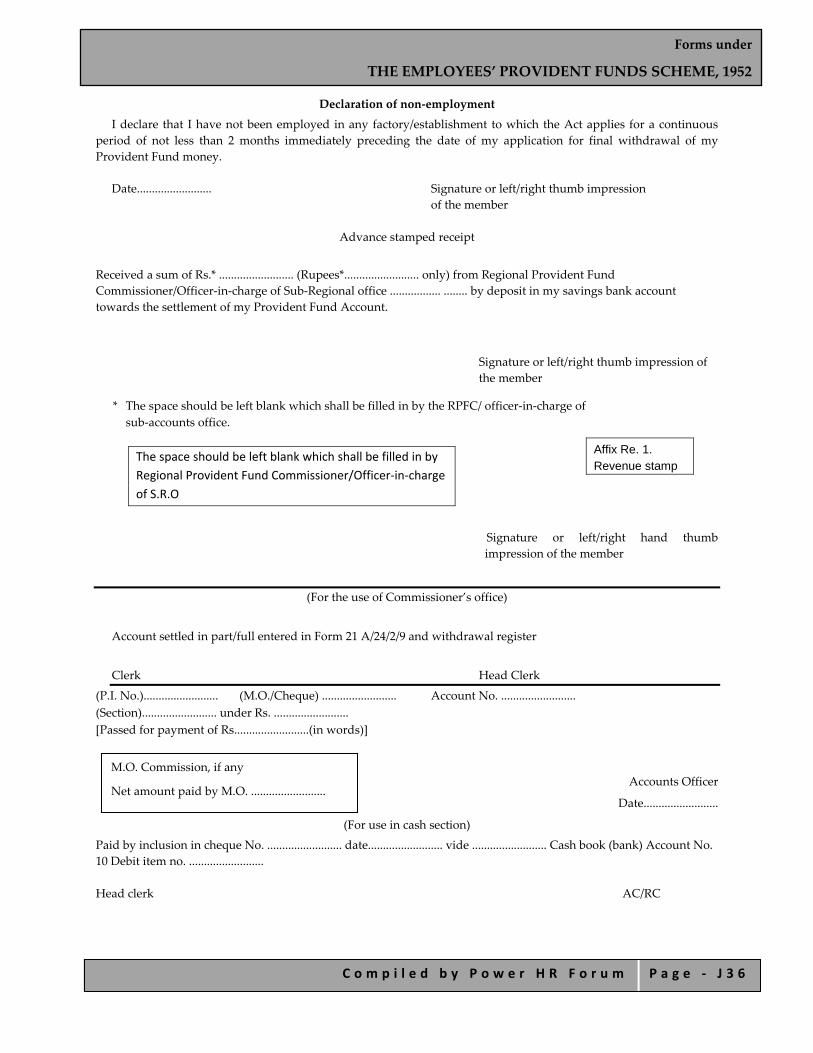
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 6
Declaration of non‐employment
I declare that I have not been employed in any factory/establishment to which the Act applies for a continuous period of not less than 2 months immediately preceding the date of my application for final withdrawal of my Provident Fund money.
Date......................... Signature or left/right thumb impression of the member
Advance stamped receipt
Received a sum of Rs.* ......................... (Rupees*......................... only) from Regional Provident Fund Commissioner/Officer‐in‐charge of Sub‐Regional office ................. ........ by deposit in my savings bank account towards the settlement of my Provident Fund Account.
Signature or left/right thumb impression of the member
* The space should be left blank which shall be filled in by the RPFC/ officer‐in‐charge of sub‐accounts office.
Signature or left/right hand thumb impression of the member
(For the use of Commissioner’s office)
Account settled in part/full entered in Form 21 A/24/2/9 and withdrawal register
Clerk Head Clerk
(P.I. No.)......................... (M.O./Cheque) ......................... Account No. ......................... (Section)......................... under Rs. ......................... [Passed for payment of Rs.........................(in words)]
Accounts Officer
Date.........................
(For use in cash section)
Paid by inclusion in cheque No. ......................... date......................... vide ......................... Cash book (bank) Account No. 10 Debit item no. ......................... Head clerk AC/RC
Affix Re. 1. Revenue stamp
The space should be left blank which shall be filled in by Regional Provident Fund Commissioner/Officer‐in‐charge of S.R.O
M.O. Commission, if any
Net amount paid by M.O. .........................
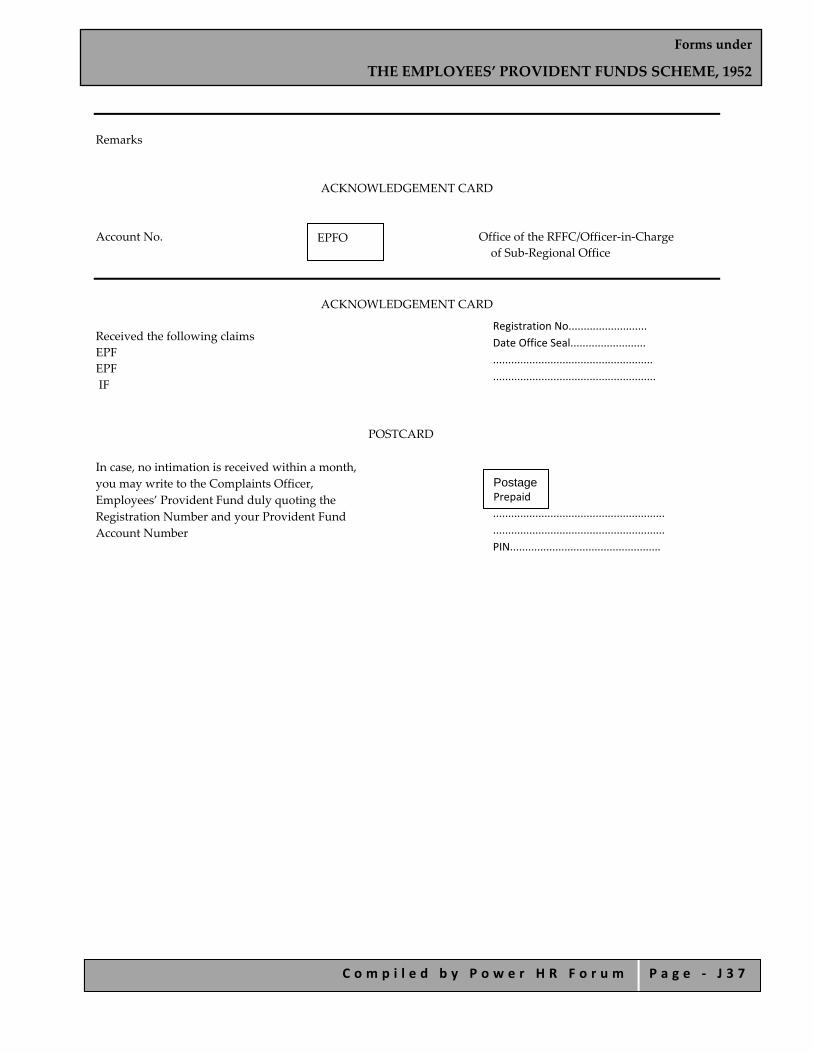
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 7
Remarks
ACKNOWLEDGEMENT CARD
Account No. Office of the RFFC/Officer‐in‐Charge of Sub‐Regional Office
ACKNOWLEDGEMENT CARD
Received the following claims EPF EPF IF
POSTCARD In case, no intimation is received within a month, you may write to the Complaints Officer, Employees’ Provident Fund duly quoting the Registration Number and your Provident Fund Account Number
Registration No.......................... Date Office Seal......................... ..................................................... ......................................................
......................................................... ......................................................... PIN..................................................
EPFO
Postage Prepaid
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 8
EMPLOYEES’ PROVIDENT FUND ORGANISATION Office of the Regional Provident Fund
Commissioner/S.R.O. .........................(Full Address)......................................................................
Instructions for filling up the applications (Form 19 & 10B) (For the guidance of applicant only. Not to be sent along with the claims)
1. All the columns in the form should be filled in completely in ink, without any overwriting. 2. Against the column reason for leaving service, indicate the one applicable:
a. Retired from service after attaining the age of 55 years/attained the age of 55 years. b. Retired on account of permanent and total incapacity for work due to Bodily/ Mental infirmity. c. Retired under voluntary retirement scheme. d. Migrating from India for permanent settlement abroad. e. Leaving India at least for a year. f. Retrenched from service. g. Discharged from service on receiving compensation under the Industrial Disputes Act, 1947. h. Resigned, not employed in any factory to which the Employee’s Provident Fund Scheme applies.
3. “Full postal address”, should be given clearly in Block Letters. Since the M.O. & Payment intimation is to be
sent to this address the name of the member and Father’s (Husband’s) should also be furnished in this column. Correct postal address including pin code will enable the Commissioner to make prompt payment to the correct payees.
4. It was advisable to have the payment by cheque. For this purpose the account payee cheque will be sent direct
to the Scheduled Bank in which the S.B. A/c. is maintained under intimation to the member. This will expedite the settlement of the correct payee.
5. The literate member should sign the application form, illiterate male member should affix his left hand thumb
impression and illiterate female member should affix her right hand thumb impression and the fact should be clearly recorded below thumb impression.
6. If the claim is required to be submitted after completing the prescribed period (i.e. in case falling under items
2(g) and (h) above only, the declaration of non‐employment in the application should be completed duly dated.
7. The claim application should be attested and forwarded by the employer under whom the member was last employed.
If the member is unable to send the application through the employer or duly attested by him for and reason whatsoever he may forward the claims duly signed in the presence of any one of the following authorised and got attested over his official seal. (i) Magistrate; (ii) A Gazetted Officer; (iii) Post/Sub‐Postmaster; (iv) President of the Village Union; (v) President of the Village Panchayat where if no Union Board; (vi) Chairman/Secretary/Member of the Municipal /District Local Board (vii) Member of Parliament/Legislative Assembly; (viii) Member of Central Board of Trustee/Regional Committees Employee’s Provident Fund; (ix) Manager of the Bank in which the Saving Bank Account is maintained; (x) Head of any recognised education institution; (xi) any authorised person as may be approved by the Commissioner.
8. The following documents should be enclosed in support of the claim:
If the member retired on account of permanent and total incapacity due to bodily or mental infirmity a medical certificate from the ESI or if the employee is covered under the ESI Scheme, from, the Medical Officer

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 3 9
designated by the Establishment should be attached. In case of migration from India for permanent settlement abroad, Visa, Passport, Journey ticket, etc., should be sent for perusal and return.
9. The member should also furnish the address in the acknowledgement card attached to the claim(s).
10. Instructions to the employer before forwarding the claims.
Details of contribution in of the member for the current financial year should be furnished in the certificate portion, in case, the contribution is not already paid it should be remitted by separate challan and receipted triplicate challan should be enclosed to the claim.
11. In support of claim under Employee’s Family Pension Scheme, 1971 the period of break in reckonable service
(i.e. period for which EPF contribution is not payable) should be furnished if not already intimated through contribution card.
Note: If in Form 10‐B (EPF) along proffered S. Nos 2,6 & 8 are not applicable
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 0
FORM 20 THE EMPLOYEES’ PROVIDENT FUND SCHEME, 1952
(For Claiming the Provident Fund Accumulation if Minor/ Deceased Member)
Regn. No. ......................... (For office use only) Form to be used
1) by the guardian of minor/lunatic member, or 2) by a nominee or legal heir of the deceased member, or 3) by the guardian of the minor/lunatic nominee or heir for claiming the Provident Funds accumulation of
minor/deceased member. Note.—Read the instructions carefully before completing this form.
Particulars of member 1.
a) Name of the member (in Block Letters).........................
b) Father’s name (or husband’s name in case of married woman).........................
c) Name and address of the factory/establishment in which the member was last employed.........................................
d) Account No. ..........................................
e) Date of leaving service.........................
f) Reason of leaving service (in case of deceased member).........................
g) Date of death of the member....................................................................
h) Marital status of the member on the day of death...............................
Particulars of the claimant
2. (To be filled in by a major nominee/legal heir/member of the family of the deceased member) a) Name of the Claimant (in Block Letters).........................
b) Father’s/husband’s name.........................
c) Sex.........................
d) Age (as on the date of death of the member).........................
e) Marital status (as on the date of death of the member).........................
(whether unmarried, married, widow or widower)
f) Relationship with the deceased member.........................
3. (To be filled in by the Guardian/Manager of minor/lunatic member or lunatic minor *[Nominee(s) /legal
heir(s)]/Family member(s) of the deceased member)
a) Name of the claimant (i.e. guardian) .........................
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 1
b) Father’s/Husband’s name.........................
c) Relationship with the member/deceased member.........................
3A. Particulars of the minor/ lunatic nominee(s) /legal heir(s) /family member(s)* on whose behalf the provident fund
amount is claimed.
Sl. No.
Name Sex Age Religion Relationship
With the deceased member With the guardian
4. Claimant’s full postal address Shri/Smt......................... (in block letters) S/o/ W/o/ H/o.......................................
Pin.........................
5. Mode of remittance:
(a) By postal money order at my cost *to the address given in item No. 4
or (b) By account payee cheque sent directfor
credit to my S.B. A/c. (Sch. Bank/Post Office) under intimation Branch......................... to me (Advance stamped receipt Full address of the bank............ furnished below)
Certificate
⎯ To the best of my knowledge no posthumous child will be born to the deceased member. ⎯ I certify that the particulars given above are true to the best of my knowledge. ⎯ I certify that the minor(s) /lunatic Sri/Smt......................... is living with me and is being supported and looked
after by myself and the Provident Fund money claimed on behalf of minor/lunatic will be spent in his/her best interests and benefits.
⎯ I certify that the minor member has not been employed in any factory/ establishment to which the Act applies for a continuous period of not less than 6 months immediately preceding the date of this application.
Enclosures:
Date......................... Signatures or left/right hand thumb
impression of the claimant
* Delete, if not applicable.
Advance Stamped Receipt
SB Account No.
Bank
Branch
Full address of the bank
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 2
[To be furnished only in case of 5(b) above]
Received a sum of Rs.*......................... (Rupees*.........................) from Regional Provident Fund Commissioner/Officer‐in‐charge of sub‐regional office ......................... by deposit in my Saving Bank account towards the settlement of Provident Fund account of Sri/Smt.........................
Signature or left/right hand thumb impression of the claimant
* The space should be left blank which shall be filled in by RPFC/ Officer‐in‐charge of SRO.
Certificate by the attesting authority
CONTRIBUTION FOR THE CURRENT PERIOD
⎯ Certified that the above contributions have been included in the regular monthly remittances. ⎯ Certified that the facts stated above are correct. ⎯ Certified that the claimant Sri/Smt./Kumari......................... is known to me and signed/thumb impressed
before me.
Signature of the employer or any authorized officer designation and office seal.........................
For the use of Commissioner’s office
Account settled in part/full. Entered in Form 21A/24/2/9 (Revised)
Clerk Head clerk P.I. No......................... M.O./Cheque......................... Account No. ........................ Section......................... Passed for payment for Rs......................... (in words) M.O. Commission (if any)......................... Net amount to be paid by M.O. .........................
Accounts officer Date.........................
For use in cash section Paid by inclusion in cheque No. ......................... dated ......................... vide Cash book (Bank) Account No. 3 Debit Item No. ......................... Head Clerk Assistant Commissioner/Regional Commissioner Remarks..................................................................................................................................
......................................................................................................................................................
Affix Re. 1 Revenue stamp

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 3
ACKNOWLEDGEMENT CARD Account No. .........................EPFO Office of the FPFC/Officer‐in‐Charge of Sub‐Regional Office
ACKNOWLEDGEMENT Received the following claims Registration No. ......................... EPF......................... Date......................... FPF......................... Office Seal IF.........................
POST CARD
In case, no intimation is received within a month, you may write to the Complaints Officer Employees’ Provident Fund duly ................................. quoting the Registration Number and your ................................. Provident Fund Account Number.
EMPLOYEES PROVIDENT FUND ORGANISATION
Office of the Regional Provident Fund Commissioner/S.R.O. ......................... Full Address.........................
Instructions
(For the Guidance of applicant only, not to be sent along with the claim)
1. Employees’ Provident Fund Scheme, 1952: Form 20: Claim for the withdrawalof Provident Fund
Accumulation of minor/deceased member. By whom the claim application should be preferred ? 2. If the member is a minor by the guardian.
OR
On death of the member:— a) If nomination subsists: by the nominee(s) if the nominee(s) is/are minor by the guardian of minor(s). b) If no nomination subsists: by the family member’s (family) includes posthumous child if any, except major
sons, and married daughters whose husbands are alive, of the deceased member duly supported by the list of surviving family members (as on the date of the death of the member) furnished by the last employer or mamlatdar/Tehsildar or Executive Magistrate indicating complete particulars such as name, relationship with deceased member (in the case of parents whether dependant or not) age, marital status. If any family member is a minor by the guardian of minor. If both (a) & (b) above are not applicable: by legal heir(s) duly supported by a legal heirship certificate (from the appropriate State normally Revenue authorities).
…………………………………………
………………………………………….
…………………………PIN
Postage Prepaid
Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 4
3. Documents to be enclosed: a) if the application is preferred by a guardian other than the natural guardian or minor
member/nominee/family member/legal heir a guardianship certificate issued by competent court of law should be enclosed.
b) Death certificate. c) If the amount receivable exceeds Rs. 5000 but less than 25,000 an affidavit‐cum‐idemnity bond (Form may
be obtained from the ex‐employer of Regional Provident Fund Commissioner or Officer‐in‐Charge of Sub‐Regional Office......................) or Estate Duty Clearance Certificate.
d) If the amount receivable exceeds Rs. 25,000 on Estate Duty Clearance Certificate.
Form 11 (FPF): Claim for benefits as admissible under the Employee’s Pension Scheme, 1971. By whom claim application should be preferred?
i. If the member is minor by his guardian,]
OR
(2) On death of the member: i. If the deceased had ‘family’ on the day of death the claim should be preferred by.
a. the widow or widower. b. failing (a) above, by the guardian or eldest surviving minor son. c. failing (a) and (b) above by the guardian or eldest surviving minor, unmarried daughter.
ii. If the deceased member had no family on the day of death, the Family Pension Fund benefit should be claimed by the person(s) eligible to receive the Provident Fund accumulation of the deceased member and if such member is a minor by the guardian. *(If the claimant being other than the natural guardian a guardianship certificate issued by the court of law should be enclosed.
Important Note:—In case the member died while in service after contributing to the Family Pension Fund for a period of not less than two years, an application in Form 10A should also be preferred for claiming monthly Family Pension.
iii. Form 5(F) ‘Benefit under Employees’ Deposit‐Linked Insurance Scheme, 1976. The benefit under Employees’ Deposit‐Linked Insurance Scheme, 1976 is admissible to the person(s) entitled to
receive the Provident Fund Accumulation of the deceased member only under the following conditions:
1. The death should have occurred while in service and, 2. The average balance in the accounts of the deceased employee should not be below the sum of Rs. 1000
during the preceding three years or during the period of his membership, whichever is less. An affidavit‐cum‐indemnity bond in the prescribed form should be furnished wherever the payment under Employees’ Deposit‐Linked Insurance exceeds Rs. 5000 (if amount receivable under Employees’ Provident Fund and Employees’ Deposit‐Linked Insurance does not exceed Rs. 25,000 one affidavit‐cum‐indemnity bond is sufficient).
GENERAL:
1) All the columns in the form should be filled in, in ink, without any overwriting. 2) Correct postal address, including Pin Code will enable to make prompt payment to the correct payee. 3) The claimant should also furnish the address in the acknowledgment attached to the claims. 4) The literate claimant should sign the application form. In case of illiterate:—Left hand thumb impression by
illiterate male claimant and right hand thumb impression by illiterate female should be affixed in the claim form.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 5
5) Attestation of claim application:—The application should be submitted through the employer under whom the member was last employed if for any reason, the claimant is unable to submit through the employer, the claim may be got attested with official seal by any one of the following officials: (i) Magistrate; (ii) A Gazetted Officer; (iii) Post/Sub‐Postmaster; (iv) President of Village Union; (v) President of the Village Panchayat where there is no Union Board; (vi) Chairman/Secretary/Member of the Municipal/District/Local Board; (vii) Member of Parliament/Legislative Assembly; (viii) Member of C.B.T. Regional Committee of the E.P.F.; (ix) Manager of the Bank where claimant has account; (x) Head of any recognised educational institution or; (xi) Any other official asmay be approved by the Commissioner.
6) Instruction to employers.—While forwarding the claims the employer should ensure that all the information required in the claim furnished correctly and requisites documents are enclosed in support of claim under Employees’ Family Pension Scheme, 1971 the period of break in reckonable service (i.e. period for EPF contribution is not payable should be furnished, if not already intimated through contribution card.
Signature
For Office use only
Dated........................
Official Seal and Registration No. ....................

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 6
FORM 31 Application for Advance From the Fund
[Refer: Instructions] (For office use only)
Dated......................... Official Seal and Registration No. ......................... Amount of advance required (in words)................
Purpose of which advance is required......................... ...................................................................................... Name in full (in block letters).........................
1. Father’s/Husband’s name.................................
2. Name of the factory/establishment in which employed and address ...................................................................
3. Provident Fund Account No. ..........................
4. Monthly basic wages, DA : Basic + DA Total.........................
5. Full postal address of the member to which payment/intimation to be sent..........................................................
6. Mode of remittance
a) In case of advance for purchase of site/house/flat or construction through an ‘agency’ or repayment of
housing loan, indicate i. in whose favour of the cheque is to be drawn and ii. full address.........................
In other cases put a tick against any one of the following:
b) By account payee cheque, through the employer (to the address given against Sl. No. 3) c) By deposit in Bank A/c. No. ......................... located at......................... (Full postal address) d) By money order at my cost to the address given against SI. No. 6.
*I declare that the advance is required to meet the expenses in connection, with my marriage/marriage of my
son/daughter/brother/sister, Shri/Kumari ......................... aged......................... to be celebrated on......................... (Date) at ............. ............ (Address)
I declare that the above particulars are true to the best of my knowledge and I will abide by the conditions
governing the grant of advance under the Scheme, Certificate(s)/document(s) in support of my application is/are furnished /enclosed. Station......................... Signature/left or right hand thumb
Date......................... impression of the member ————— *Delete if the advance applied for is not for marriage.

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 7
Advance stamped receipt
[To be furnished with reference to 7(a) or (b) or (c) above only]
Received a sum of *Rs. ......................... (Rupees.........................) from the Regional Provident Fund
Commissioner/Officer in‐charge of Sub‐regional Office, Employees’ Provident Fund towards the grant of advance from my Employees’ Provident Fund Account maintained by him.
Signature of member
*To be filled by the Employees’ Provident Fund Office
To be furnished by the employer
(During the closure/lock‐out of the factory/establishment by any Gazette Officer or the Chief Executive/Head of a
local authority or MP or MLA or a Member of CBT/Regional Committee, EPF)
Certified that the application has been signed by the member in my presence after he/she had read the
contents/the contents had been explained to him/her by me and that the information given in the application is correct. Required certificate(s) is/ are enclosed.
Date......................... Designation of the signing official with
stamp of the factory /establishment Encls.......................... Signature of employer or an authorized
official of the factory/establishment
For use in Provident Fund Commissioner’s Office
Section......................... Account No. .........................
Authority for payment of advance only Para 68 Passed for payment for Rs. ......................... (Rupees......................... only) Mode of remittance: Refer Sl. No. 7 M.O. Commission, if any Net amount to be paid by MO......................... Clerk Head Clerk Accounts Officer P.I. No. .........................vide payment scroll P.C. to A .O.
For use in cash section Paid by inclusion in Cheque No. .........................dated......................... vide Cash Book (Bank) Account No. 3 ...............debit item No. ......................... Clerk Head Clerk Assistant Commissioner
REMARKS .............................................................................................................................
Instructions

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 8
A member of the Fund may avail the following non‐refundable advances:The documents to be furnished in support of the application are given in brackets: 1. Purchase of a dwelling site
(From an ’agency’)—Original allotment order. (From an individual)—Original title deed non‐encumbrance certificate. (for verification and return agreement with the seller)
2. Purchase of a dwelling‐house/flat (From an ’agency’)—Original Allotment order. (From an individual)—Original title deed (for verification and return agreement with the seller, non‐encumbrance certificate from an appropriate authority that the house/flat is a new and unveiled one furnishing the number and date of approval of plan, commencement and completion of the house/flat tax bills and receipts.
3. Construction of house (Original title deed) (for verification and return), non‐ encumbrance certificate, estimated cost for construction. Approved plan. Note.—While claiming the second and subsequent instalments the declaration/ certificate as requried by the Commissioner in his letter sanctioning the advance should be submitted along with the application. ‘Agency’ referred to in 1 to 3 above would mean Central/State Government, a Co‐operative Society, an institution, a trust, a local body or a housing finance corporation. In case of transactions through an agency the payment will be made only by Account Payee Cheque, direct to the ‘agency’ concerned].
4. Additions, alteration or improvement to the house owned by member or by spouse (Approval of the
appropriate authority, estimate of the work, original title deed of the house (for verification), non‐encumbrance certificate, a certificate from the appropriate authority specifying the date of completion of the house.)
5. Repayment of (Housing) loan to the State Government Housing Board, Municipal Corporation or a body
similar to Delhi Development Authority A certificate from the lending authority furnishing the details of loan and outstanding amount. 6. Closure/lock‐out of the factory/establishment, for reasons other than strike
(Furnish the certificate ‘A’ given later)
7. Non‐receipt of wages for 2 months (Furnish the certificate ‘B’ given later)
8. Illness of member/family member (Furnish the certificate ‘C’ given later)
9. Marriage of self/son/daughter/sister/brother.
10. Post‐matriculation education of son/daughter (Certificate from the Institution regarding the course of study and anticipated expenditure)
11. Damage to the property due to natural calamity (Flood/riot/earthquake) (Furnish the certificate ‘D’ given
later)
12. Affected by cut in electricity (Furnish the certificate ‘E’ given later)
13. Purchase of equipment for physically handicapped members (Furnish the certificate ’F’ given later) Note.—

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 4 9
1. Such other document, certificate, etc. as may be required by the sanctioning authority are also required to be furnished through the establishment.
2. In case no intimation is received within a month please write to the RPFC/Officer‐in‐charge of sub‐regional office, through the establishment.
Certificate—A (Refer instruction Sl. No. 6)
Certified that no compensation was paid to the member Sri/Smt. ......................... for the period of lock‐out/closure.
Signature of employer /authorised official with date and seal
Certificate—B (Refer instruction Sl. No. 7) Certified that member Sri/Smt. ......................... has/had been granted leave for a period of......................... from......................... to.........................
i. The ESI facilities/cash benefits are not actually available to the member/themember has ceased to be eligible for cash benefits under ES1‐‐Certificate from ESI enclosed.
Signature of the employer/authorised officer with date and seal
Certificate—C (Refer instruction Sl. No. 8) Certified that—
i. The memebr Sri/Smt. ....................................has/had been granted leave for a period of....................... from............................ to......................
ii. The ESI facilities/cash benefits are not actually available to the member/the member has ceased to be eligible for cash benefits under ESI certificate from ESI enclosed.
(Signature of the employer/authorised officer with date and seal)
Medical certificate to be issued: (i) in case of major surgical operation or where the hospitalisation for one month or more had or has become necessary—By a doctor of the Government/ESI /private hospital; (ii) in case of treatment of TB, leprosy, paralysis or cancer‐ by a doctor of Government /private hospital/ESI or by a registered medical practitioner; (iii) in case of treatment of heart ailment or mental derangement—By a specialist doctor.
(ii) Certified that Sri /Smt./Kumari......................... S/o., W/o., D/o. ........................
i. is suffering from TB/leprosy/paralysis/cancer/mental derangement/heart ailment. ii. is suffering from......................... (disease) for which a major surgical
operation/and hospitalisation for a period of......................... days from......................... to......................... had or has become necessary.
iii. is suffering from......................... and hospitalisation for a period of days from......................... to......................... had or has become necessary. Signature of the Doctor with date and seal —————

Forms under
THE EMPLOYEES’ PROVIDENT FUNDS SCHEME, 1952
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ J 5 0
* Delete whichever is not applicable.
Certificate—D (Refer instruction Sl. No. 11)
Certified that the movable/immovable property of Sri/Smt. ......................... viz..........................situated at......................... has been damaged due to......................... on (date)......................... The estimated loss of property due to......................... calamity is valued at Rs. ......................... The State Government has declared that the calamity has effected the general public in the area in which the property of the member is/ was located vide Notification/Press release No. ................ and date.
Signature of employer/ revenue official/ Gazetted officer/MLA/MP/
Member of CBT/Regional Committee with seal and date
Certificate—E (Refer instructions SI. No. 12)
Certified that the fall in wages amounting to 25% more than 25% of the wages in respect of Sri/Smt. ......................... due to power cut.
Signature of the employer/ authorised official with date and seal
Certificate—F (Refer instructions Sl. No. 13)
Medical certificate from a competent medical practitioner
Certified that Sri/Smt./Kum. ......................... S/o/ W/o/ D/o ......................... is physically handicapped, viz. ......................... (Nature of handicap) and requires the equipment, viz. ......................... costing about Rs. ......................... to minimise the hardship on account of handicap.
Signature of the doctor with date and seal
—————
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2
INDEX FORM 01 Employer’s Registration Form
FORM 01(A) Form of Annual Information of Factory/Establishment Covered under ESI Act
FORM 1 Declaration Form
FORM IA Family Declaration Form
FORM 2 Addition/Deletion in Family Declaration Form
FORM 3 Return of Declaration Form
FORM 4 Identity Card
FORM 4A Family Identity Card
FORM 5 Return of Contributions
FORM 5A Statement of Advance Contributions Made for the Contribution Period
FORM 6 Register of Employees
FORM 7 First/Intermediate/Final Certificate
FORM 8 Special Intermediate Certificate
FORM 9 Claim for Sickness/T.D.B./Maternity Benefit for Sickness
FORM 10 Abstention Verification in Respect of Sickness Benefit/Temporary Disablement Benefit/Maternity Benefit
FORM 11 Accident Book
FORM 12 Accident Report From Employer
FORM 13 Death Certificate
FORM 14 Claim for Permanent Disablement Benefit
FORM 15 Claim Form for Dependants’ Benefit
FORM 16 Claim for Periodical Payments of Dependant’s Benefit
FORM 17 Certificate/Notice of Pregnancy
FORM 18 Certificate of Expected Confinement/ Confinement/Miscarriage/Maternity Benefit

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3
FORM 19 Claim for Maternity Benefit and Notice of Work
FORM 20 Claim for Maternity Benefit After the Death
of an Insured Woman Leaving Behind the Child
FORM 21 Death Certificate in Case of Confinement of Claiming Maternity Benefit
FORM 22 Funeral Expenses Claim Form
FORM 23 Life Certificate for Permanent Disablement Benefit
FORM 24 Declaration and Certificate for Dependants’ Benefit

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4
FORM 01 Employer’s Registration Form
[Regulation 10‐B ]
*Employer’s Code No.
1. Name of the Factory/Establishment
……………………………………………….
2. Complete Postal address of the Factory/Establishment
………………………………………………. …………………PIN……………………….
3. a) Telephone No., if any b) Fax No., if any c) E‐mail address, if any
………………………………………………. ………………………………………………. ……………………………………………….
4. Location of Factory/Establishment a. State b. District c. Municipality/Ward d. Name of Town/Revenue village e. Police station f. Revenue Demarcation/Hudbast No.
………………………………………………. ………………………………………………. ………………………………………………. ………………………………………………. ………………………………………………. ……………………………………………….
5. a. Whether the building/premises of Factory/Estt.
is owned or hired.
b. If hired or there is a change in the name of Unit/ownership, please indicate— i. ESI code number, if covered earlier ii. Date from which earlier Factory/ Estt.
closed down. iii. Terms and conditions under which
property acquired/taken on lease (enclose copy of agreement/relevant deed)
…………………………………………….. ………………………………………………. ………………………………………………. ……………………………………………….
6. Details of Bank A/c.: a) Account No................................ b) Account No................................ c) Account No................................
(b) Name of Bank and Branch: (i) ................................................................. (ii) ................................................................ (iii) ...............................................................
7. (a) Income Tax PAN/GIR No. (b) (b) Income Tax Ward/Circle/Area
………………………………………………. ……………………………………………….
8. Exact nature of work/business carried on
……………………………………………….
9. Date of commencement of Factory/ Establishment
……………………………………………….

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 5
10. a. Whether registered under Factories/Shop & Estt./
Other Act (Please Specify) : b. Factory licence No./Trade licence No./Catering
Estt. licence No./Shop, Estt. Registration No./Licence No. under Cinematography Act etc.
c. Please give whichever is applicable i. Commercial Tax No. ii. State Sales Tax No. iii. Central Sales Tax No.
iv. Any other Tax No. d. Maximum no. of persons that can be employed
on any one day, as per Licence :
………………………………………………. License No. Date Licensing Authority No. Date Issung Authority
i. ii. iii. iv.
…………………………………………………………………...
11. a) Whether power is used for manufacturing
process as per section 2(K) of the Factories Act. If so, since when :
b) In case of factory whether Licence issued underSection 2(m)(i) or 2(m)(ii) of the Factories Act, 1948
c) Power connection No.
……………………………………………………………….. ………………………………………………………………. …………………………………………………………………. No. Sanctioned Power Load Issuing Authority
12. a. Whether it is Public or Private Ltd.
Company/Partnership/Proprietor‐ship/Co‐operative Society/Owner‐ship (attach copy of Memorandum & Articles of Association/ Partnership Deed/Resolution). :
b. Give name, present and permanent : residential address of present Pro‐ prietor/Managing Directors, Dire‐ ctor/Managing Partners, Partners/ Secretary of the Co‐operative Society.
………………………………………………………………. Name Designation Address
i. ii. iii. iv. v. vi. vii.
13. Address(es) of the Registered Office/ Head Office/Branch Office/Sales office /Administrative Office/other offices if any, with no. of employees attached with each such office and person responsible for the office.
Address as on date
No. of employee
Phone No. / Fax No.
Function Person responsible for day ‐to ‐day‐ functioning of office
14. a. (a)Whether any work/business carried out
throught contractor/immediate employer : b. If yes, give nature of such work/ business
(Give details on separate sheet , if required) ……………………………………………………………………. ……………………………………………………………………..
15. EPF Code No. (If covered under EPF Act) No. Issuing Authority
16. Total number of employees employed for wages directly and through immediate employers on the date of application. (whether manual/clerical/supervisor, connected with the administration or purchase of raw
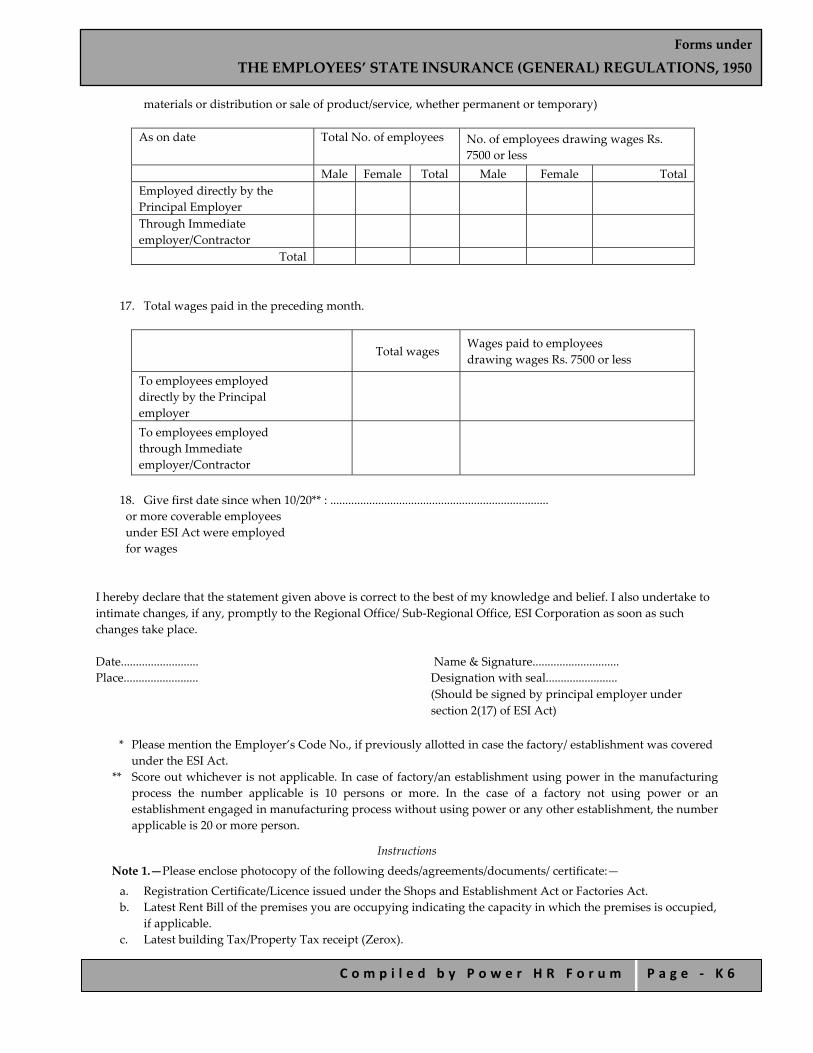
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 6
materials or distribution or sale of product/service, whether permanent or temporary)
As on date Total No. of employees No. of employees drawing wages Rs. 7500 or less
Male Female Total Male Female Total Employed directly by the Principal Employer
Through Immediate employer/Contractor
Total
17. Total wages paid in the preceding month.
Total wages
Wages paid to employees drawing wages Rs. 7500 or less
To employees employed directly by the Principal employer
To employees employed through Immediate employer/Contractor
18. Give first date since when 10/20** : ......................................................................... or more coverable employees under ESI Act were employed for wages
I hereby declare that the statement given above is correct to the best of my knowledge and belief. I also undertake to intimate changes, if any, promptly to the Regional Office/ Sub‐Regional Office, ESI Corporation as soon as such changes take place. Date.......................... Name & Signature............................. Place......................... Designation with seal........................
(Should be signed by principal employer under section 2(17) of ESI Act)
* Please mention the Employer’s Code No., if previously allotted in case the factory/ establishment was covered under the ESI Act.
** Score out whichever is not applicable. In case of factory/an establishment using power in the manufacturing process the number applicable is 10 persons or more. In the case of a factory not using power or an establishment engaged in manufacturing process without using power or any other establishment, the number applicable is 20 or more person.
Instructions
Note 1.—Please enclose photocopy of the following deeds/agreements/documents/ certificate:—
a. Registration Certificate/Licence issued under the Shops and Establishment Act or Factories Act. b. Latest Rent Bill of the premises you are occupying indicating the capacity in which the premises is occupied,
if applicable. c. Latest building Tax/Property Tax receipt (Zerox).

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 7
d. Memorandum and Articles of Association/Partnership Deed/Trust Deed. e. Zerox Copy of certificate of commencement of production and/or Registration No. of CST/ST. Note 2.—“Power” shall have the meaning assigned to it in the Factories Act, 1948 which is as under: “power” means electrical energy, or any other form of energy which is mechanically transmitted and is not generated by human or animal agency.
Note 3.—Manufacturing process as defined in section 2(k) in Factories Act is as under: “Manufacturing process” means any process for—
i. making, altering, repairing, ornamenting, finishing, packing, oiling, washing, cleaning, breaking up, demolishing, or otherwise treating or adapting any article or substance with a view to its use, sale, transport, delivery or disposal;
ii. pumping oil, water, sewage or any other substance; iii. generating, transforming or transmitting power;
iv. composing types for printing, printing by letter press, lithography photogravure or other similar process or book binding;
v. constructing, reconstructing, repairing, refitting, finishing or breaking up ships or vessels; vi. preserving or storing any article in cold storage.
Note 4.—“Immediate employer” in relation to employees employed by or through him, means a person who has undertaken the execution, on the premises of the factory or an establishment to which this Act applies or under the supervision of the principal employer or his agent, of the whole or any part of any work which is ordinarily part of the work of the factory or establishment of the principal employer or is preliminary to the work carried on in, or incidental to the purpose of, any such factory or establishment and includes a person by whom the services of an employee who has entered into a contract of service with him are temporarily lent or let on hire to the principal employer and includes a contractors. Note 5.—“Principal Employer” means—
a. in a factory, the owner or occupier of the factory and includes the managing agent of such owner or occupier, the legal representative of a deceased owner or occupier and where a person has been named as the manager of the factory under the Factories Act, 1948, the person so named;
b. in any establishment under the control of any department of any Government, in India the authority appointed by such Government in this behalf or where no authority is so appointed, the head of the Departments;
c. in any other establishment, any person responsible for the supervision and control of the establishment. Note 6.—“Occupier” of a factory/establishment means the person who has ultimate control over the affairs of the
factory/establishment and when the said affairs are entrusted to a managing agent shall be the Occupier of the factory/establishment. Note 7.—“Employees” means any person employed for wages in or in connection with the work of a factory or an
establishment to which this Act applies and—
i. who is directly employed by the principal employer on any work of, or incidental or preliminary to or connected with the work of, the factory or establishment whether such work is done by the employee in the factory or elsewhere; or
ii. who is employed by or through an immediate employer on the premises of the factory or establishment or under the supervision of the principal employer or his agent on work which is ordinarily part of the work of the factory or establishment or which is preliminary to be carried on in or incidental to the purpose of the factory or establishment; or
iii. whose services are temporarily lent or let on hire to the principal employer by the person with whom the person whose services are so lent or let on hire has entered into a contact of service,

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 8
and includes any person employed for wages on any work connected with the administration of the factory or establishment or any part, department or branch thereof with the purchase of raw materials for, or the distribution or sale of the products of, the factory or establishment; (or any person engaged as an apprentice, not being an apprentice engaged under the Apprentices Act, 1961 (52 of 1961), or under the standing orders of the establishment; but does not include)—
a. Any member of the Indian Naval, Military or Air Force; or b. Any person so employed whose wages excluding remuneration for overtime work exceeds such wages as
may be prescribed by the Central Government, a month:
Provided that an employee whose wages excluding remuneration for over time work exceeds such wages as may be prescribed by the Central Government, a month at any time after and not before the beginning of the contribution period, shall continue to be an employee until the end of that period.
Note 8.—“Wages” means all remuneration paid or payable in cash to an employee, if the terms of the contract of
employment, express or implied, were fulfilled and includes any payment to an employee in respect of any period of authorised leave, lock‐out, strike which is not illegal or lay off and other additional remuneration, if any, paid at intervals not exceeding two months, but does not include—
a. any contribution paid by the employer to any pension fund or provident fund, or under this Act; b. any travelling allowance or the value of any travelling concession; c. any sum paid to the person employed to defray special expenses entailed on him by the nature of his
employment; or d. any gratuity payable on discharge.]
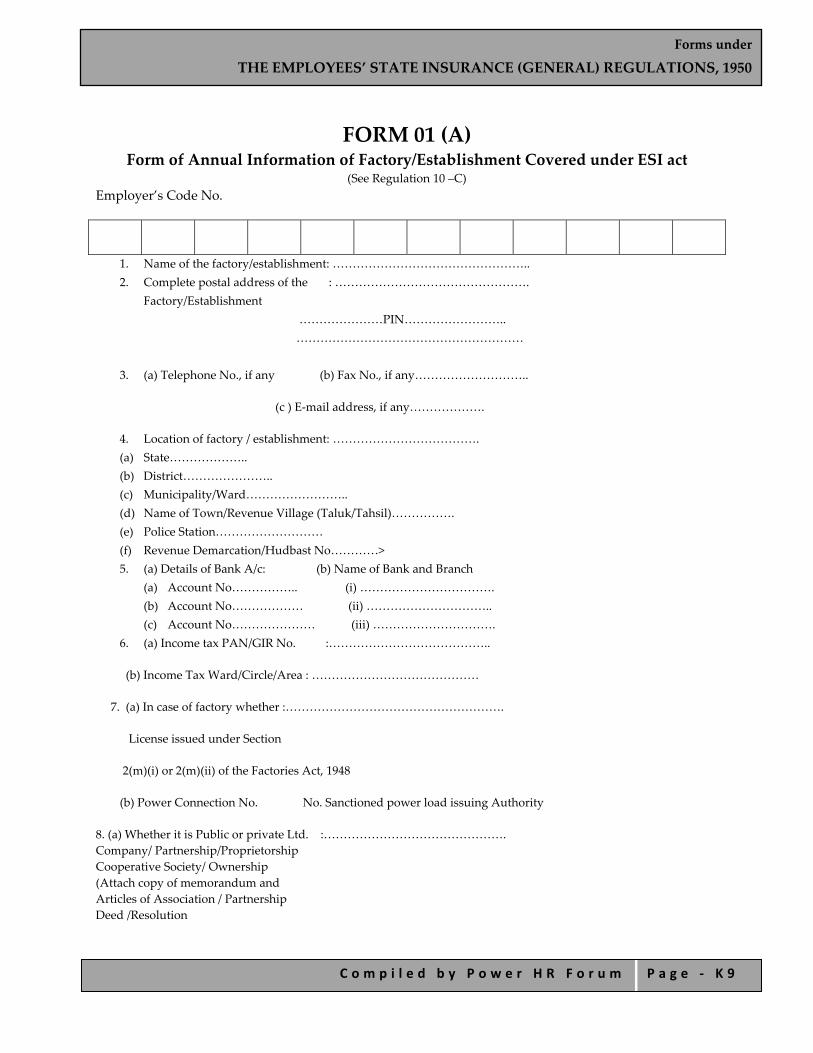
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 9
FORM 01 (A) Form of Annual Information of Factory/Establishment Covered under ESI act
(See Regulation 10 –C) Employer’s Code No.
1. Name of the factory/establishment: ………………………………………….. 2. Complete postal address of the : ………………………………………….
Factory/Establishment …………………PIN…………………….. …………………………………………………
3. (a) Telephone No., if any (b) Fax No., if any………………………..
(c ) E‐mail address, if any……………….
4. Location of factory / establishment: ………………………………. (a) State……………….. (b) District………………….. (c) Municipality/Ward…………………….. (d) Name of Town/Revenue Village (Taluk/Tahsil)……………. (e) Police Station……………………… (f) Revenue Demarcation/Hudbast No…………> 5. (a) Details of Bank A/c: (b) Name of Bank and Branch
(a) Account No…………….. (i) ……………………………. (b) Account No……………… (ii) ………………………….. (c) Account No………………… (iii) ………………………….
6. (a) Income tax PAN/GIR No. :…………………………………..
(b) Income Tax Ward/Circle/Area : ……………………………………
7. (a) In case of factory whether :……………………………………………….
License issued under Section
2(m)(i) or 2(m)(ii) of the Factories Act, 1948
(b) Power Connection No. No. Sanctioned power load issuing Authority
8. (a) Whether it is Public or private Ltd. :………………………………………. Company/ Partnership/Proprietorship Cooperative Society/ Ownership (Attach copy of memorandum and Articles of Association / Partnership Deed /Resolution
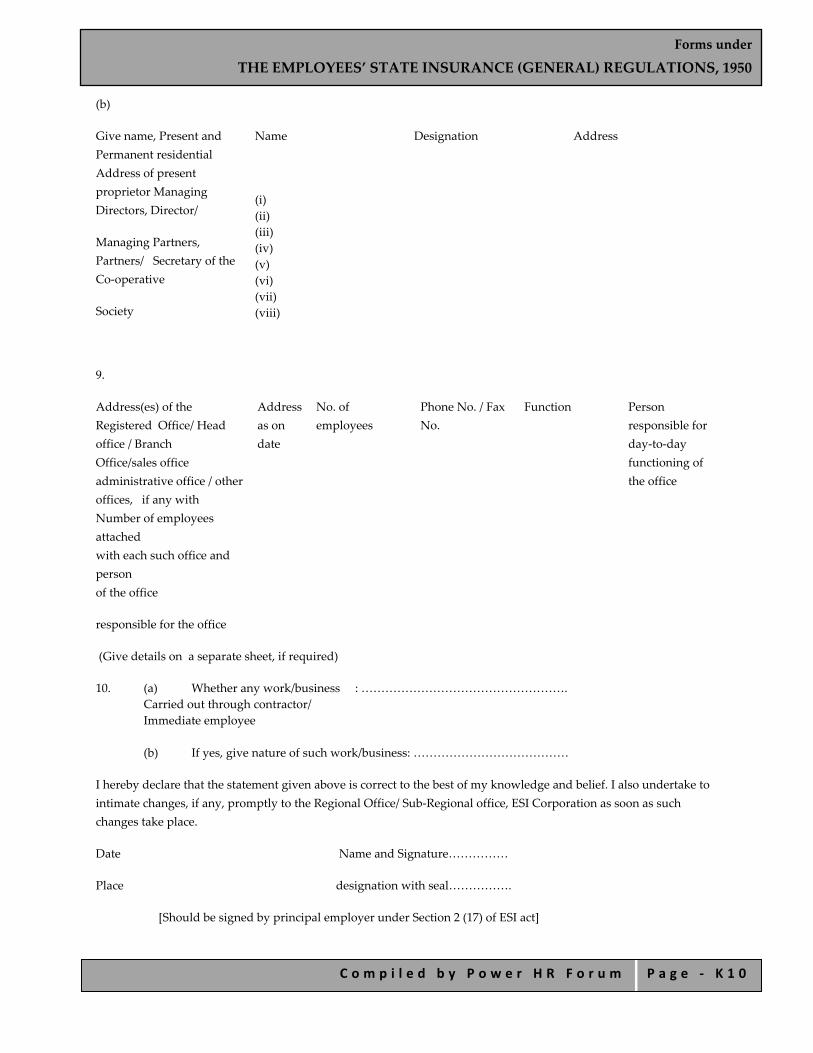
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 0
(b)
Give name, Present and Permanent residential Address of present proprietor Managing Directors, Director/
Managing Partners, Partners/ Secretary of the Co‐operative
Society
Name
(i) (ii) (iii) (iv) (v) (vi) (vii) (viii)
Designation Address
9.
Address(es) of the Registered Office/ Head office / Branch Office/sales office administrative office / other offices, if any with Number of employees attached with each such office and person of the office
responsible for the office
Address as on date
No. of employees
Phone No. / Fax No.
Function Person responsible for day‐to‐day functioning of the office
(Give details on a separate sheet, if required)
10. (a) Whether any work/business : ……………………………………………. Carried out through contractor/ Immediate employee
(b) If yes, give nature of such work/business: …………………………………
I hereby declare that the statement given above is correct to the best of my knowledge and belief. I also undertake to intimate changes, if any, promptly to the Regional Office/ Sub‐Regional office, ESI Corporation as soon as such changes take place.
Date Name and Signature……………
Place designation with seal…………….
[Should be signed by principal employer under Section 2 (17) of ESI act]

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 1
FORM 1 Declaration Form (Regulations 11 and 12)
To be filled in by the employee after reading instructions overleaf. Two Postcard Size photographs are to be attached with this from.
This from is free of cost.
(A) INSURED PERSONʹS PARTICULARS
1. Insurance No.
2. Name (In block letters)
3. Fatherʹs/Husbandʹs Name
4. Date of Birth
D M Y 5. Marital Status M/U/W
6. Sex M/F
7. Present Address ..................................................... ..................................................... ..................................................... ..................................................... Pin Code e‐mail address
8. Permanent Address............................................................................. .................................................................................................................. …………………………………………………………………………… ........................................................................................................ Pin Code e‐mail address
Branch Office Dispensary
(B) EMPLOYERʹS PARTICULARS
9. Employerʹs Code No.
10. Date of Appointment Day Month Year
11. Name & Address of the Employer .................................................................................................... .................................................................................................... ....................................................................................................
12. In case of any previous employment please fill up the details as under:
(a) Previous Ins. No.

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 2
(b) Employerʹs Code No.
(c) Name & address of the Employer Telephone No./ e‐mail address
(c) Details of Nominee u/s 71 of the ESI Act, 1948/Rule 56(2) of the ESI (Central) Rules, 1950 for payment of cash benefit in the event of death.
Name Relationship Address
I hereby declare that the particulars given by me are correct to the best of my knowledge and belief. I undertake to intimate the Corporation any changes in the membership of my family within 15 days of such change.
Counter‐signature by the employer Signature/T.I. of IP Signature with seal (D) FAMILY PARTICULARS OF INSURED PERSON Sl. No.
Name Date of Birth/ Age as on date of filling from
Relationship with the Employee
Whether residing with him/her?
If ʹNoʹ, state place of Residence
1. Yes No Town State
2.
3.
4.
5.
6.
7.
8.
..................................................................................................................................................................

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 3
ESI Corporation Temporary Identity Card (Valid for 3 months from the date of appointment) Name
Ins. No. Date of appointment
Branch Office
Dispensary
Employerʹs Code No. & Address
Validity. Dated Signature/T.I of I.P Signature of B.M. with seal
INSTRUCTIONS
1. Submission of Form 1 is governed by regulations 11 and 12 of the ESI (General) Regulations, 1950. 2. ʺFamilyʺ means all or any of the following relatives of an Insured Person namely:—
(i) a spouse; (ii) a minor legitimate or adopted child dependent upon the I.P.; (iii) a child who is wholly dependent on the earnings of the I.P. and who is (a) receiving education, till he or she attains the age of 21 years (b) an unmarried daughter; (iv) a child who is infirm by reason of any physical or mental abnormality or injury and is wholly dependant on the earnings of the I.P. so long as the infirmity continues: (v) dependant parents [Please see section 2, clause (11) of the ESI Act, 1948 for details].
3. Identity Card is Non‐transferable. 4. Loss of Identity Card be reported to Employer/Branch Manager immediately. 5. Submission of false information attracts penal action under section 84 of the ESI Act, 1948. 6. This form duly filled in must reach the concerned Branch Officer within 10 days of appointment of an
employee. Delay attracts penal action under section 85 of the Act, against employer. 7. As an Insured Person you and your dependent family members are entitled to full medical care. The other
benefits in cash include (1) Sickness Benefit (2) Temporary Disablement Benefit (3) Permanent Disablement Benefit (4) Dependents Benefit and (5) Maternity Benefit (in case of women employees) subject to fulfillment of contributory conditions.
8. For more details please visit website of ESIC at WWW.esic.org.in or contact Regional Office or Branch Office.
Space for photograph
For Branch Office use only
1. Date of Allotment of Ins. No. …………………………………………..
2. Date of Issue of TIC …………………………………………………..
3. Name/No. of Disp. …………………………………………………….
4. Whether reciprocal Medical arrangements involved? If yes, please indicate:………………………………………
Signature of Branch Manager
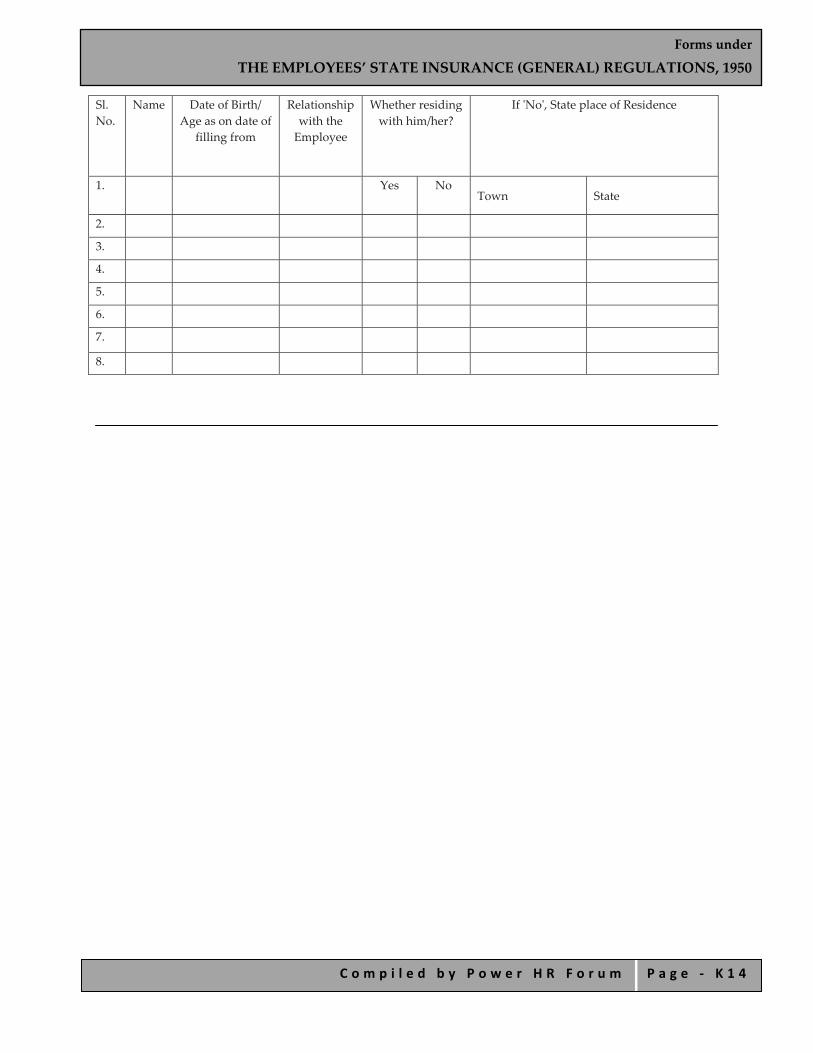
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 4
Sl. No.
Name Date of Birth/ Age as on date of
filling from
Relationship with the Employee
Whether residing with him/her?
If ʹNoʹ, State place of Residence
1. Yes No Town State
2.
3.
4.
5.
6.
7.
8.

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 5
FORM I –A Family Declaration Form
(Regulation 15‐A)
Name of the insured person………………………………………………………
Insurance Number…………………………………………………………………..
Serial No. Name Date of Birth Relationship with insured persons
Whether residing with him/her or not
I hereby declare that the particulars above have been given by me and are true to the best of my knowledge and belief. I also undertake to intimate to the Corporation any changes in the membership of my family within 15 days of such changes having occurred.
Date …………………….. Signature or thumb impression
of the insured person
Countersigned……………
Date…………………………
Designation………………………….
Name, address and
Code No. of Employer………………………………………………………………………………………….
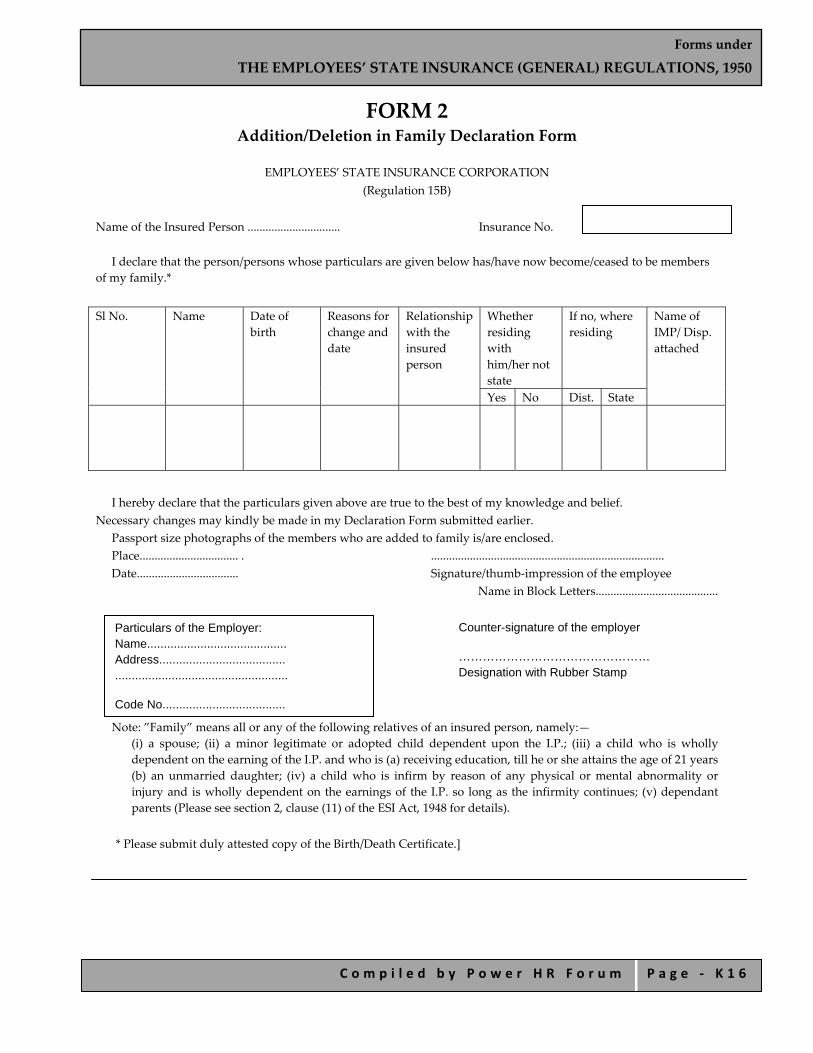
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 6
FORM 2 Addition/Deletion in Family Declaration Form
EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 15B)
Name of the Insured Person ............................... Insurance No.
I declare that the person/persons whose particulars are given below has/have now become/ceased to be members of my family.*
Sl No. Name Date of
birth Reasons for change and date
Relationship with the insured person
Whether residing with him/her not state
If no, where residing
Name of IMP/ Disp. attached
Yes No Dist. State
I hereby declare that the particulars given above are true to the best of my knowledge and belief.
Necessary changes may kindly be made in my Declaration Form submitted earlier. Passport size photographs of the members who are added to family is/are enclosed. Place................................. . .............................................................................. Date.................................. Signature/thumb‐impression of the employee
Name in Block Letters.........................................
Note: ”Family” means all or any of the following relatives of an insured person, namely:— (i) a spouse; (ii) a minor legitimate or adopted child dependent upon the I.P.; (iii) a child who is wholly dependent on the earning of the I.P. and who is (a) receiving education, till he or she attains the age of 21 years (b) an unmarried daughter; (iv) a child who is infirm by reason of any physical or mental abnormality or injury and is wholly dependent on the earnings of the I.P. so long as the infirmity continues; (v) dependant parents (Please see section 2, clause (11) of the ESI Act, 1948 for details).
* Please submit duly attested copy of the Birth/Death Certificate.]
Particulars of the Employer: Name.......................................... Address...................................... ....................................................
Code No.....................................
Counter-signature of the employer
………………………………………… Designation with Rubber Stamp
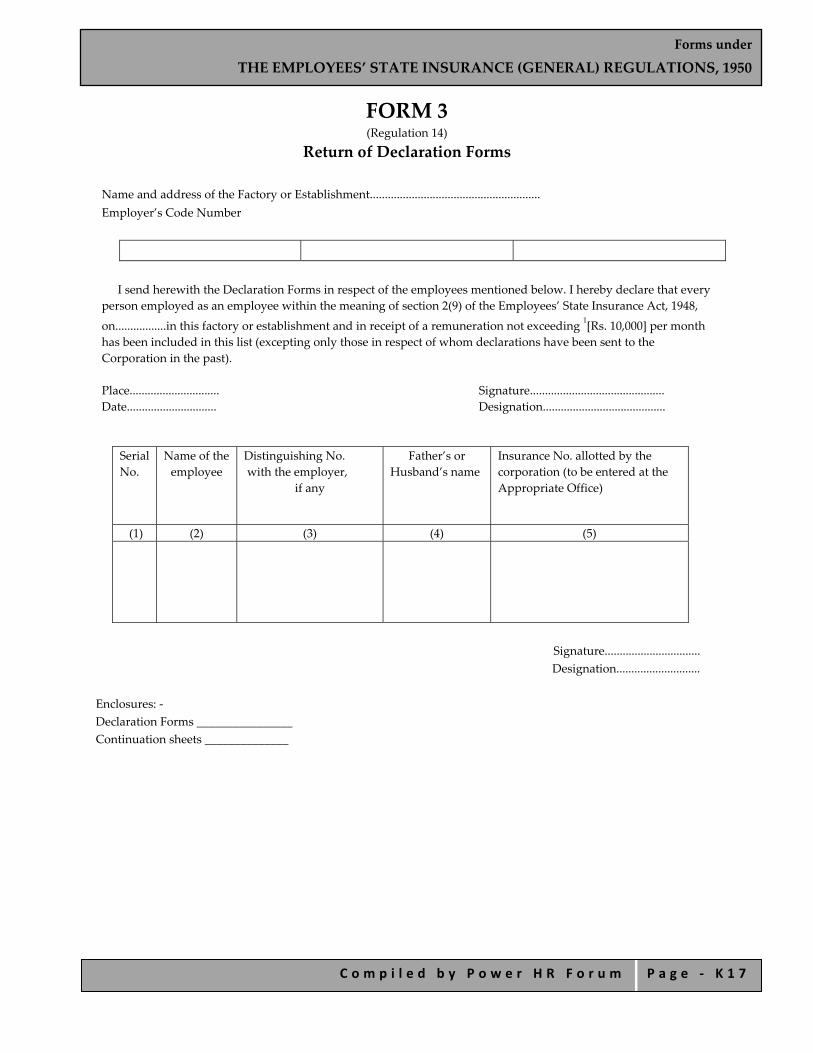
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 7
FORM 3 (Regulation 14)
Return of Declaration Forms
Name and address of the Factory or Establishment......................................................... Employer’s Code Number
I send herewith the Declaration Forms in respect of the employees mentioned below. I hereby declare that every
person employed as an employee within the meaning of section 2(9) of the Employees’ State Insurance Act, 1948,
on.................in this factory or establishment and in receipt of a remuneration not exceeding 1[Rs. 10,000] per month has been included in this list (excepting only those in respect of whom declarations have been sent to the Corporation in the past).
Place.............................. Signature............................................. Date.............................. Designation.........................................
Serial No.
Name of the employee
Distinguishing No. with the employer,
if any
Father’s or Husband’s name
Insurance No. allotted by the corporation (to be entered at the Appropriate Office)
(1) (2) (3) (4) (5)
Signature................................ Designation............................
Enclosures: ‐ Declaration Forms ________________ Continuation sheets ______________

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 8
FORM 4 (Regulations 17)
Identity Card Insurance No.
Name ............................. Sex......................... Son of/daughter of/wife of ........................ Year of birth ................................................... Address .......................................................... ......................................................................... Dispensary ..................................................... Local Office ....................................................
Identification marks
Photograph of the insured person
Employment changes Date Code No. Date Code No
Prepared by ................................................... Signature or thumb‐impression of the employee
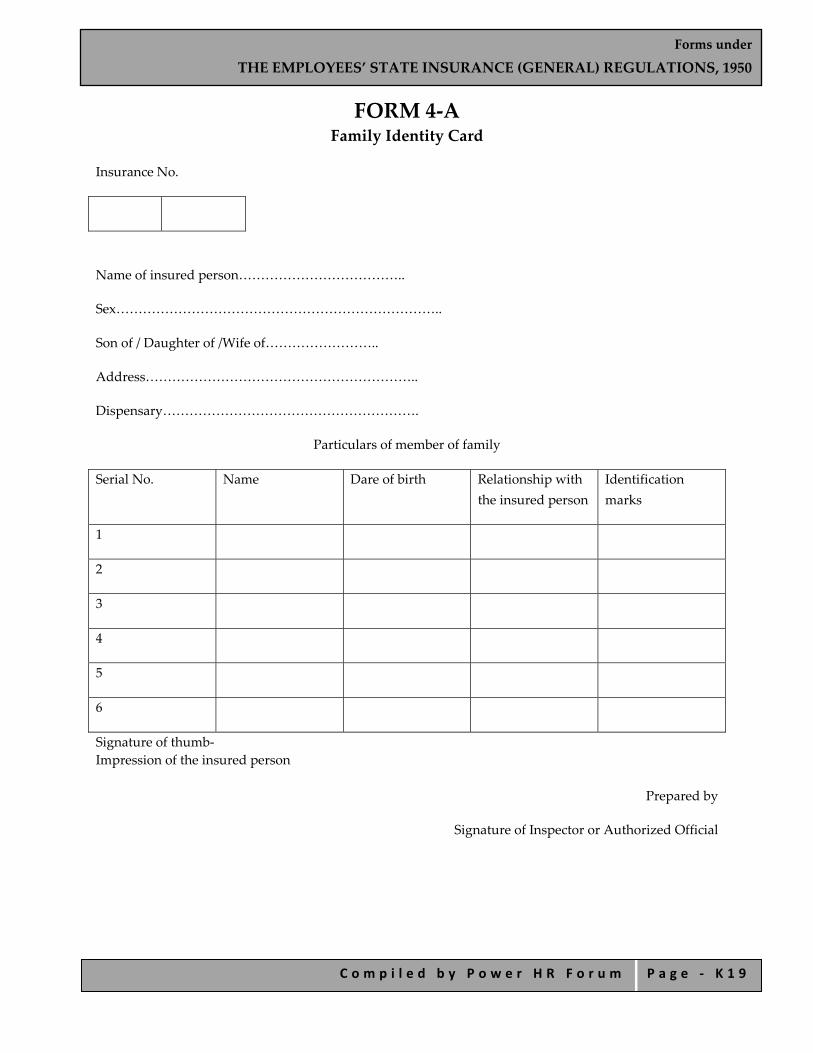
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 1 9
FORM 4‐A Family Identity Card
Insurance No.
Name of insured person………………………………..
Sex………………………………………………………………..
Son of / Daughter of /Wife of……………………..
Address……………………………………………………..
Dispensary………………………………………………….
Particulars of member of family
Serial No. Name Dare of birth Relationship with the insured person
Identification marks
1
2
3
4
5
6
Signature of thumb‐ Impression of the insured person
Prepared by
Signature of Inspector or Authorized Official

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 0
FORM 5 (Regulation 26)
Due date for submission— Name of Branch Office...................... Employer’s Code No. ....................
Return of Contributions EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 26) Name and address of the factory or establishment:.................................................................. Particulars of the principal employer(s):
a) Name:.................................................................................................................................. b) Designation:........................................................................................................................ c) Residential address:...........................................................................................................
Contribution Period from.......................................... to......................................... I furnish below the details of the Employer’s and Employee’s share of contributions in respect of the under mentioned insured persons. I hereby declare that the return includes each and every employee, employed directly or through an immediate employer or in connection with the work of the factory/establishment or any work connected with the administration of the factory/ establishment or purchase of raw materials, sale or distribution of finished products, etc., to whom the ESI Act, 1948 applies, in the contribution period to which this return relates and that the contributions in respect of employer’s and employee’s share have been correctly paid in accordance with the provisions of the Act and Regulations.
Employee’s Share........................................ Employer’s Share......................................... Total contribution........................................
Details of Challans:
Sl. No. Month Date of Challan Amount Name of the Bank and Branch
1. 2. 3. 4. 5. 6.
Total amount paid: Rs....................................
I declare that
(w). All the Records and Registers have been maintained as per provisions contained in ESI Act, rules and regulations framed therein.
(x). During the period of return…. No. of Declaration forms have been submitted.
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 1
(y). During the above period …No. of TICs have been received.
(z) During the above period…..No. of PICs have been received.
(aa) During the above period….No. of PICs have been distributed amongst the eligible IPs.
(bb) During the above period………. accidents have been reported to the concerned branch Office.
(cc) During the period…No of employees directly employed by us been covered and a total wages of Rs………….have been paid to such employees.
(dd) During the period…………No. of employees directly employed by us have not been covered and a total wages of Rs…………. have been paid to such employees.
(ee) During the period ……………No of employees employed through immediate employer have been covered and a total wages of Rs…….. have been paid to such employees.
(ff) During the period…………………….No. of employees employed through immediate employer have not been covered and at total wages of Rs……………have been paid to such employees.
(gg) Following components of wages have been taken into consideration for the purpose of payment of contribution—
1.
2.
3.
4.
5.
(i) Following components of wages not been taken into consideration for the purpose of payment of contribution‐
1.
2.
3.
4.
5.
The abovementioned information is based on records and any information if found incorrect will render me liable for prosecutions under provisions of ESI Act and action for recovery of contribution due along with interest and damages as per provisions of the ESI Act.
Place…………. Signature and Designation of the Employer
Date….. (with Rubber Stamp)

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 2
CERTICATE BY CHARTERED ACCOUNTANT
(To be submitted in case of employers employing 40 or more employees)
Certified that I have verified the above return from the Records and Registers of M.s………..and found it to be correct.
Signature and seal of the Charted
Accounted with Membership No.
Important Instructions: Information to be given in “Remarks Column (No. 9)” i. If any I.P. is appointed for the first time and/or leaves during the contribution period, indicate
“A.............................. (date)” and/or “L................................. (date)”. ii. Please indicate Insurance Nos. in ascending order. iii. Figures in columns 4, 5 and 6 shall be in respect of wage periods ended during the contribution period. iv. Invariably strike totals of columns 4, 5 and 6 of the return. v. No over‐writing shall be made. Any corrections, if made, should be signed by the employer. vi. Every page of this Return should bear full signature and rubber stamp of the employer. vii. Daily wages in column 7 of the Return shall be calculated by dividing figures in column 5 by figures in
column 4 to two decimal places.
For *CP ending 31st March, due date is 12th May For CP ending 30th September, due date is 11th November
EMPLOYEES’ STATE INSURANCE CORPORATION
Employer’s Name and Address.....................................................................................................
Employer’s Code No................................................ Period From................to...............
Sl. No.
Insurance Number
Name of insured person
No. of days for which wages paid
Total amount of wages paid (Rs.)
Employee’s contribution deducted
(Rs.)
Average Daily wages (Rs.)
Whether still continues working
Remarks*
(1) (2) (3) (4) (5) (6) (7) (8) (9) Total
* Date of appointment and leaving the job may be given in remarks column.
Signature of the Employer
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 3
(FOR OFFICAL USE) 1. Entitlement position marked. 2. Total of Col. 5 of Return checked and found correct/correct amount is indicated. 3. Checked the amount of Employer’s/Employee’s contribution paid which is in order/ observation memo.
enclosed.
Counter‐signature...........................
U.D.C. Head Clerk Branch Officer]
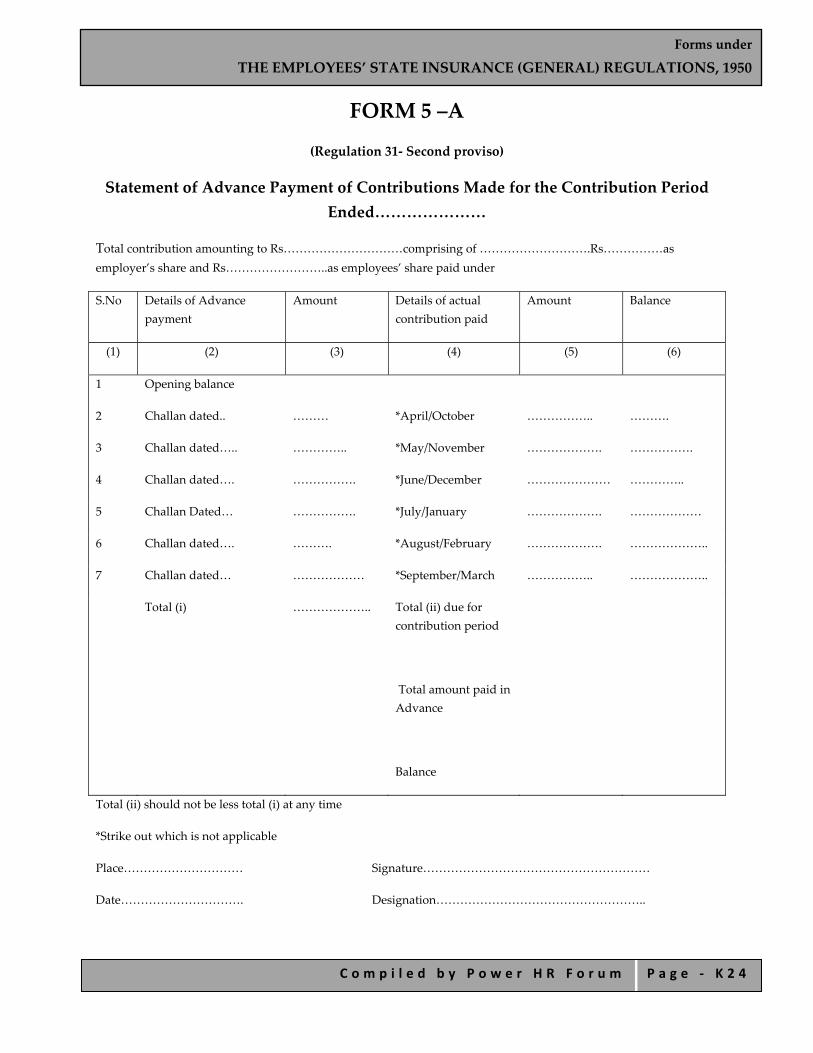
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 4
FORM 5 –A
(Regulation 31‐ Second proviso)
Statement of Advance Payment of Contributions Made for the Contribution Period Ended…………………
Total contribution amounting to Rs…………………………comprising of ……………………….Rs……………as employer’s share and Rs……………………..as employees’ share paid under
S.No Details of Advance payment
Amount Details of actual contribution paid
Amount Balance
(1) (2) (3) (4) (5) (6)
1 Opening balance
2 Challan dated.. ……… *April/October …………….. ……….
3 Challan dated….. ………….. *May/November ………………. …………….
4 Challan dated…. ……………. *June/December ………………… …………..
5 Challan Dated… ……………. *July/January ………………. ………………
6 Challan dated…. ………. *August/February ………………. ………………..
7 Challan dated… ……………… *September/March …………….. ………………..
Total (i) ……………….. Total (ii) due for contribution period
Total amount paid in Advance
Balance
Total (ii) should not be less total (i) at any time
*Strike out which is not applicable
Place………………………… Signature…………………………………………………
Date…………………………. Designation……………………………………………..

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 5
FORM 6 Register of Employees
EMPLOYEES’ STATE INSURANCE CORPORATION [Regulation 32]
Contribution period: From........................................... to................................ Month…………………..
Sl No.
Insurance No.
Name of the insured person
Name of dispensary to which attached
Occupation
Deptt. And shift if any
If appointed or left service during the contribution period, date of appointment/ leaving service
No. of days for which wages paid or payable
Total amount of wages paid or payable
Employee’s share of contribution
1 2 3 3(a) 4 5 6 7 8 9
Total………………………….. Employer’s share……………………….. Grand Total…………………………… Paid on……………………………….
Month Month
No. of days for which wages paid/ payable
Total amount of wages paid/ payable (Rs)
Employee’s share of contribution (Rs)
No. of days for which wages paid/ payable
Total amount of wages paid/ payable (Rs)
Employee’s share of contribution (Rs)
10 11 12 13 14 15
Total………………………….. Employer’s share……………………….. Grand Total…………………………… Paid on……………………………….
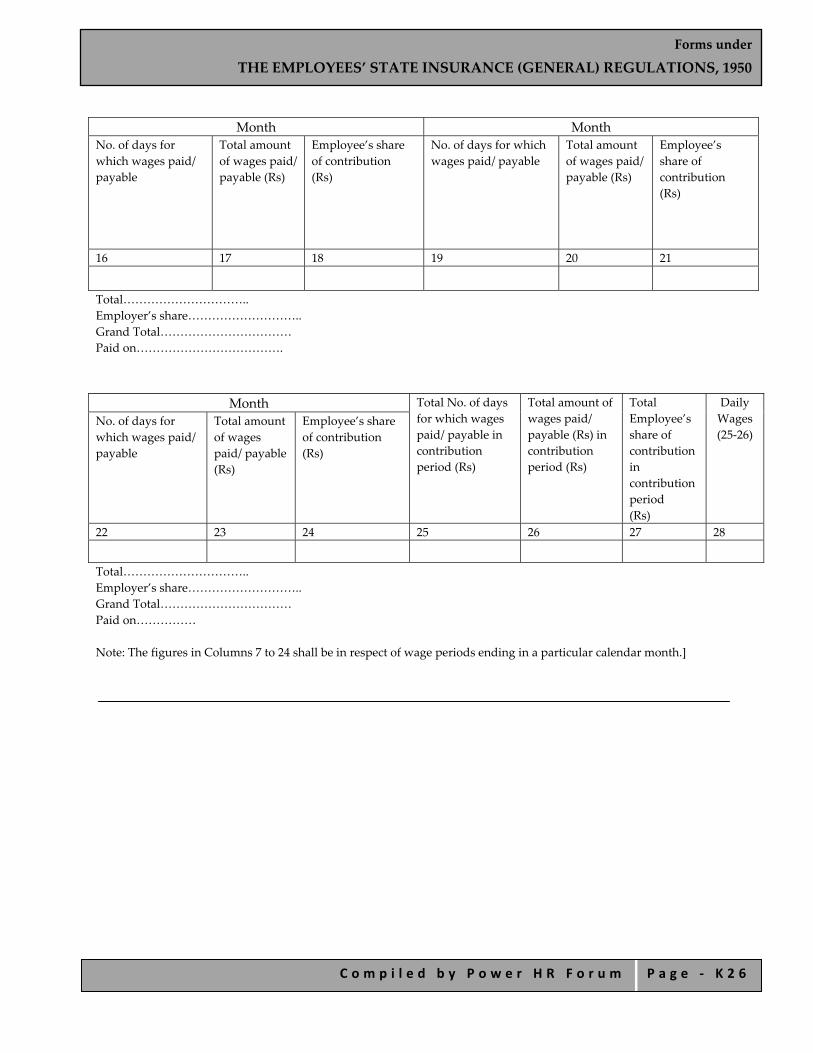
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 6
Month Month
No. of days for which wages paid/ payable
Total amount of wages paid/ payable (Rs)
Employee’s share of contribution (Rs)
No. of days for which wages paid/ payable
Total amount of wages paid/ payable (Rs)
Employee’s share of contribution (Rs)
16 17 18 19 20 21
Total………………………….. Employer’s share……………………….. Grand Total…………………………… Paid on……………………………….
Month Total No. of days
for which wages paid/ payable in contribution period (Rs)
Total amount of wages paid/ payable (Rs) in contribution period (Rs)
Total Employee’s share of contribution in contribution period (Rs)
Daily Wages (25‐26)
No. of days for which wages paid/ payable
Total amount of wages paid/ payable (Rs)
Employee’s share of contribution (Rs)
22 23 24 25 26 27 28
Total………………………….. Employer’s share……………………….. Grand Total…………………………… Paid on…………… Note: The figures in Columns 7 to 24 shall be in respect of wage periods ending in a particular calendar month.]

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 7
FORM 7 (Deposit this certificate within 3 days with the appropriate Branch office
to avoid possible loss of benefit under regulation 64)
First/Intermediate/Final Certificate (Regulations 57, 58, 59 and 89B)
EMPLOYEES’ STATE INSURANCE CORPORATION
Book No.............. ..................................................................
Serial No............. Stamp of Dispensary Signature or thumb‐impression of I.P. Date of First Certificate of spell of Employer’s Code No............................. Sickness or Disablement.................................... Branch Office.........................................
Name.......................................s/w/d/of..............................Insurance No................................... Certified that I have examined you today and that in my opinion:— Any other remarks by the
Medical Officer
............................................................
............................................................
............................................................
Attestation by Med. Officer
i. *You now need medical treatment, attendance and abstention from work on medical grounds by reason of (diagnosis)............................................
ii. *You have continued to need medical treatment, attendance and abstention from work on medical grounds upto and including this day by reason of (diagnosis)..................................................
iii. *In my opinion you will be fit to resume work tomorrow/on.............................................................
Note: The date of fitness must in no case bet later than the third day after the date of the examination in case of First and Final Certificate. Date..................... Signature..........................
Insurance Medical Officer Rubber stamp
Name in Block Letters.........................................
* Strike out whichever is not applicable IMPORTANT:
1. Any person who makes false statement or representation for the purpose of obtaining benefit whether for himself/some other person shall be punishable with imprisonment up to 6 months or fine up to Rs. 2000 or both.
2. This form should be completed and submitted without delay to the appropriate Branch Office to escape penal deduction of benefit under regulation 64 read with regulation 99 of ESI General Regulation, 1950.
3. Insured person must sign, with date, the claim form to avoid delay and inconvenience]
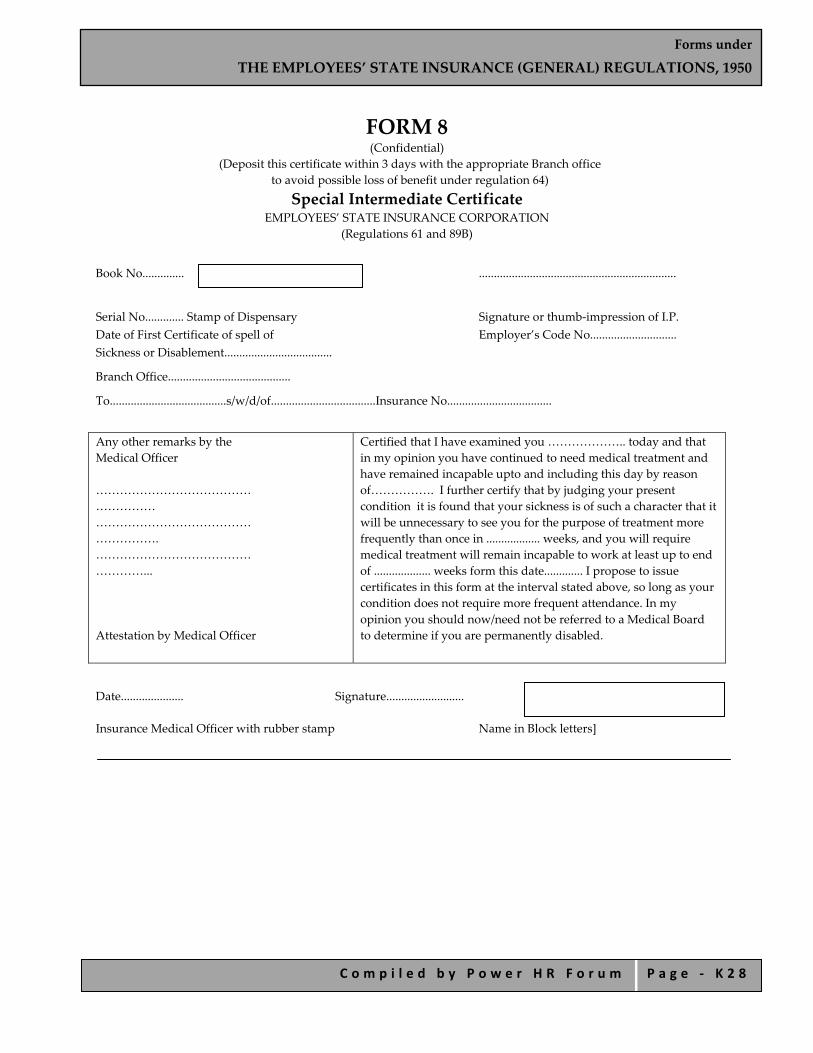
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 8
FORM 8 (Confidential)
(Deposit this certificate within 3 days with the appropriate Branch office to avoid possible loss of benefit under regulation 64)
Special Intermediate Certificate EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulations 61 and 89B)
Book No.............. ..................................................................
Serial No............. Stamp of Dispensary Signature or thumb‐impression of I.P. Date of First Certificate of spell of Employer’s Code No............................. Sickness or Disablement....................................
Branch Office.........................................
To.......................................s/w/d/of...................................Insurance No...................................
Any other remarks by the Medical Officer ……………………………………………… ………………………………………………. ……………………………………………... Attestation by Medical Officer
Certified that I have examined you ……………….. today and that in my opinion you have continued to need medical treatment and have remained incapable upto and including this day by reason of……………. I further certify that by judging your present condition it is found that your sickness is of such a character that it will be unnecessary to see you for the purpose of treatment more frequently than once in .................. weeks, and you will require medical treatment will remain incapable to work at least up to end of ................... weeks form this date............. I propose to issue certificates in this form at the interval stated above, so long as your condition does not require more frequent attendance. In my opinion you should now/need not be referred to a Medical Board to determine if you are permanently disabled.
Date..................... Signature.......................... Insurance Medical Officer with rubber stamp Name in Block letters]

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 2 9
FORM 9 Claim for Sickness/T.D.B./Maternity Benefit for Sickness
(EMPLOYEES’ STATE INSURANCE CORPORATION
Regulations 63 and 89B)
I……………….. s/w/d of………………………………. Insurance No. hereby claim cash benefit for period overleaf and state.
i. *That because of sickness/temporary disablement/sickness due to pregnancy/confinement/premature birth of child/miscarriage, I have not been at work since ............................
ii. *I no longer claim to be sick/temporary disabled/sick due to pregnancy/confinement/premature birth of child/miscarriage from ................ and I shall/did not take up any work for remuneration before that date.
iii. *I have not been in receipt of any wages for the days of leave/holiday(s).
iv. *I was not on strike during the period of certified abstention on account of sickness/temporary disablement i.e. from .......................... to .......................... for which the benefit is claimed.
I desire payment in *cash at Branch Office/By Money Order.
Signature or T.I. of claimant
Name in Block Letters.....................................
Address..........................................................
.......................................................................
Notes.—
1. Any person who makes a false statement or representation for the purpose of obtaining benefit whether for himself/some other person shall be punishable with imprisonment up to 6 months or fine up to Rs. 2000 or both.
2. This form should be completed and submitted without delay to the appropriate Branch Office.
3. A final certificate must be obtained before resuming work
* Strike out if not applicable]
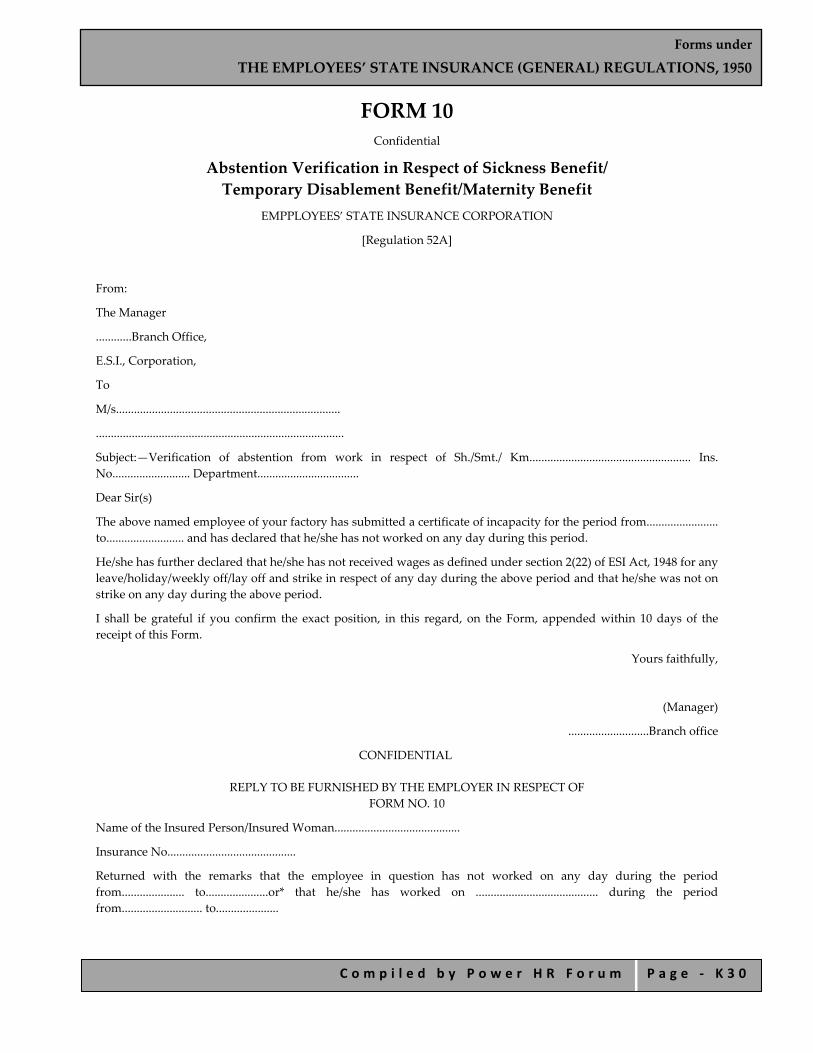
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 0
FORM 10 Confidential
Abstention Verification in Respect of Sickness Benefit/ Temporary Disablement Benefit/Maternity Benefit
EMPPLOYEES’ STATE INSURANCE CORPORATION
[Regulation 52A]
From:
The Manager
............Branch Office,
E.S.I., Corporation,
To
M/s...........................................................................
...................................................................................
Subject:—Verification of abstention from work in respect of Sh./Smt./ Km...................................................... Ins. No.......................... Department..................................
Dear Sir(s)
The above named employee of your factory has submitted a certificate of incapacity for the period from........................ to.......................... and has declared that he/she has not worked on any day during this period.
He/she has further declared that he/she has not received wages as defined under section 2(22) of ESI Act, 1948 for any leave/holiday/weekly off/lay off and strike in respect of any day during the above period and that he/she was not on strike on any day during the above period.
I shall be grateful if you confirm the exact position, in this regard, on the Form, appended within 10 days of the receipt of this Form.
Yours faithfully,
(Manager)
...........................Branch office
CONFIDENTIAL
REPLY TO BE FURNISHED BY THE EMPLOYER IN RESPECT OF FORM NO. 10
Name of the Insured Person/Insured Woman..........................................
Insurance No...........................................
Returned with the remarks that the employee in question has not worked on any day during the period from..................... to.....................or* that he/she has worked on ......................................... during the period from........................... to.....................

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 1
1. It is further confirmed that—
a. He/she remained on leave with wages for the period from........................ to.....................
b. He/she remained on holidays with wages from............... to.....................
c. He/she was on weekly off with wages from.......................................to……………….
d. He/she was on lay‐off with wages from............... to.....................
e. He/she was on strike from............... to.....................
2. In case, the IP/IW is paid any wages for any of the days falling during the above‐ mentioned period subsequently, the same will be notified to you in due course.
3. The day proceeding the first day of absence was*/was not a holiday for the Insured Person/Insured Woman.
Date................... Signature...........................................
Name in block letters and Designation........................... ................................................................... Code No.....................................................
* Strike out which is not applicable]

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 2
FORM 11 Accident Book
EMPLOYEES’ STATE INSURANCE CORPORATION (Regulation 66)
S. No.
Date of notice
Time of notice
Name and address of
Sex Age Insurance No.
Shift, Department and occupation
Details of injury
injured person
of the employee Cause Nature Date Time place
1 2 3 4 5 6 7 8 9 10 11 12 13
What exactly was the injured person doing at the time of accident.
Name, Occupation, address & signature or the thumb‐impression of the person(s) giving
notice.
Signature and designation of the person who makes the entry in the Accident Book.
Name, address and occupation of two witnesses.
Remarks, if any
14 15 16 17 18
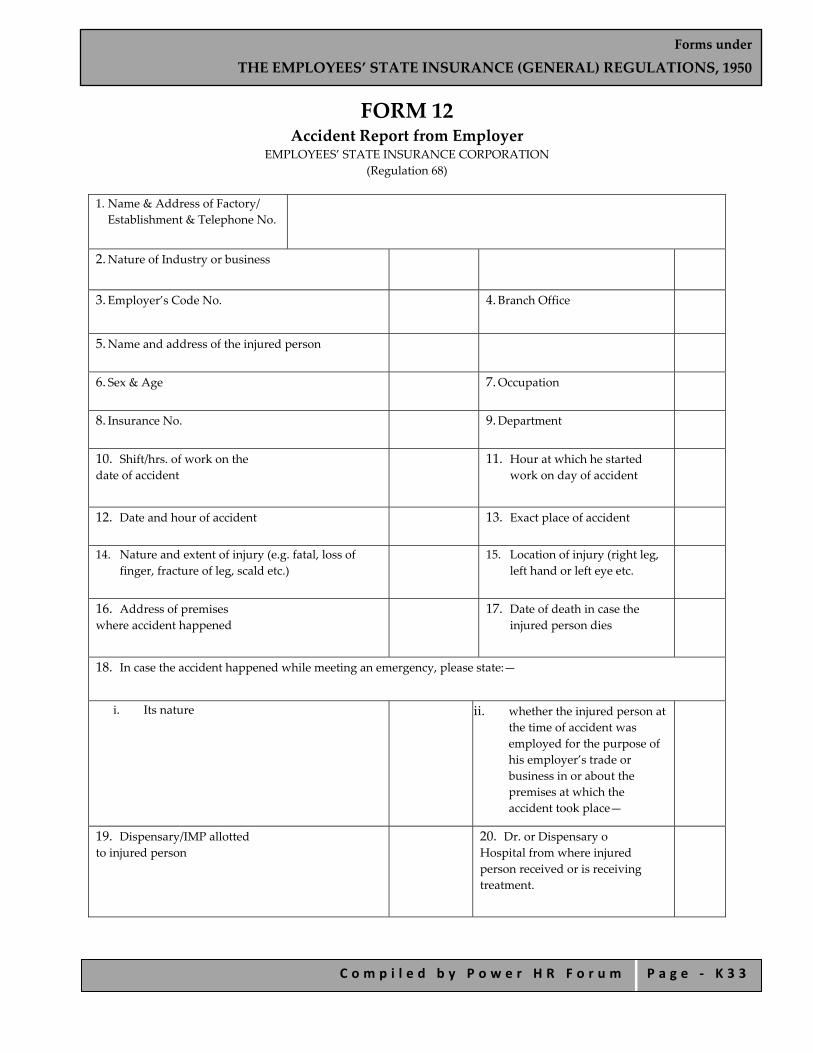
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 3
FORM 12 Accident Report from Employer
EMPLOYEES’ STATE INSURANCE CORPORATION (Regulation 68)
1. Name & Address of Factory/ Establishment & Telephone No.
2. Nature of Industry or business
3. Employer’s Code No.
4. Branch Office
5. Name and address of the injured person
6. Sex & Age
7. Occupation
8. Insurance No.
9. Department
10. Shift/hrs. of work on the date of accident
11. Hour at which he started work on day of accident
12. Date and hour of accident
13. Exact place of accident
14. Nature and extent of injury (e.g. fatal, loss of finger, fracture of leg, scald etc.)
15. Location of injury (right leg, left hand or left eye etc.
16. Address of premises where accident happened
17. Date of death in case the injured person dies
18. In case the accident happened while meeting an emergency, please state:—
i. Its nature ii. whether the injured person at the time of accident was employed for the purpose of his employer’s trade or business in or about the premises at which the accident took place—
19. Dispensary/IMP allotted to injured person
20. Dr. or Dispensary o Hospital from where injured person received or is receiving treatment.
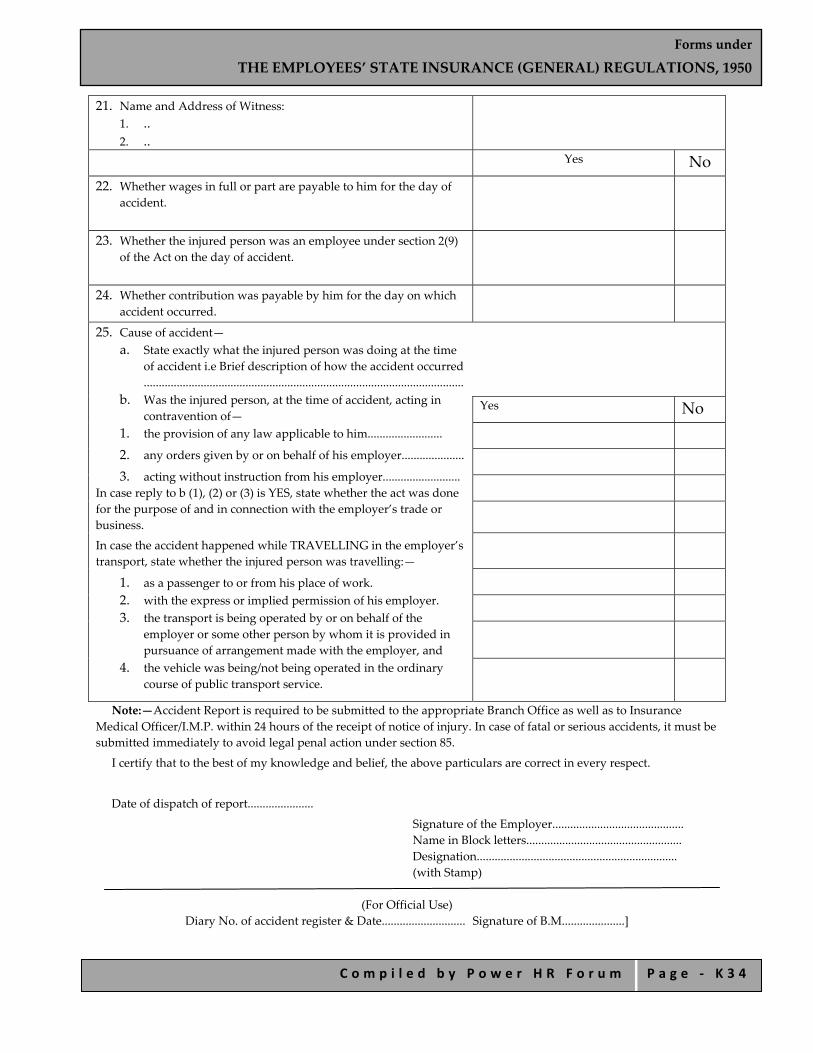
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 4
21. Name and Address of Witness: 1. .. 2. ..
Yes No 22. Whether wages in full or part are payable to him for the day of
accident.
23. Whether the injured person was an employee under section 2(9) of the Act on the day of accident.
24. Whether contribution was payable by him for the day on which accident occurred.
25. Cause of accident— a. State exactly what the injured person was doing at the time
of accident i.e Brief description of how the accident occurred ...........................................................................................................
b. Was the injured person, at the time of accident, acting in contravention of—
1. the provision of any law applicable to him......................... 2. any orders given by or on behalf of his employer..................... 3. acting without instruction from his employer..........................
In case reply to b (1), (2) or (3) is YES, state whether the act was done for the purpose of and in connection with the employer’s trade or business. In case the accident happened while TRAVELLING in the employer’s transport, state whether the injured person was travelling:—
1. as a passenger to or from his place of work. 2. with the express or implied permission of his employer. 3. the transport is being operated by or on behalf of the
employer or some other person by whom it is provided in pursuance of arrangement made with the employer, and
4. the vehicle was being/not being operated in the ordinary course of public transport service.
Yes No
Note:—Accident Report is required to be submitted to the appropriate Branch Office as well as to Insurance Medical Officer/I.M.P. within 24 hours of the receipt of notice of injury. In case of fatal or serious accidents, it must be submitted immediately to avoid legal penal action under section 85.
I certify that to the best of my knowledge and belief, the above particulars are correct in every respect.
Date of dispatch of report......................
Signature of the Employer............................................ Name in Block letters.................................................... Designation................................................................... (with Stamp)
(For Official Use) Diary No. of accident register & Date............................ Signature of B.M.....................]

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 5
FORM 13 (In Duplicate)*
Death Certificate (For Dependent’s Benefit or Funeral Expenses)
EMPLOYEES’ STATE INSURANCE CORPORATION (Regulations 79 and 95C)
Book No.............. Stamp of Dispensary Serial No............................. Name of the deceased Insured person........................................................................s/w/d of.................... Insurance No........................ I certify that in my opinion the above‐named deceased Insured Person died on the ..................... day of..................... 20.......... as a result of an injury/due to*................................ I **had been attending him/her for providing medical benefit before his/her death and I attended him/her for the last time on the ..................... day of.................... 20.......
Signature............................
Insurance Medical Officer/I.M.P. Name in block letters and rubber stamp
Any other remarks by the Medical Officer
Dated.....................
* Please indicate the name of the disease. ** May be suitably amended if the Insurance Medical Officer/I.M.P. has not attended the deceased person before
his/her death.]

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 6
FORM 14 Claim for Permanent Disablement Benefit EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 76A)
I…………………………………………………….. s/d/w of……………………………………………………………………. Insurance No. …………………….having been declared as permanently disabled by the Medical Board/ Medical Appeal Tribunal/ Employees’ Insurance Court, claim Permanent Disablement Benefit accordingly for the period from............... to...............
The amount due may be paid to me by money order/in cash at Branch Office
...................................................... Signature or thumb‐impression of the Claimant
Name in block letters........................... address..................................................
.................................................. Dated..................... Important: Any person who makes a false statement or representation for the purpose of obtaining benefit,
whether for himself or for some other person, commits an offence punishable with imprisonment for a term which may extend to six months or with a fine up to Rs. 2,000, or with both.]

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 7
FORM 15 Claim Form for Dependants’ Benefit
EMPLOYEES’ STATE INSURANCE CORPORATION (Regulation 80)
Name of the deceased Insured Person ...................................... Ins. No. ...........................S/w/d of ................................................................. Date of Death .............................. Last employed as ........................................................ by...............................................................
I/We the following, being dependants of the above named deceased Insured Person, hereby claim and accordingly apply for dependant’s benefit on account of his/her death:
Name of the dependant
Sex Age or year of birth
Marital status
Relationship with the deceased
Present Address
Name of guardian in case of a minor.
1. 2. 3. 4. 5. 6. 7
I/We declare that the particulars given above are true to the best of my/our knowledge and belief.
I/We also declare that to the best of my/our knowledge and belief, there is no other dependant entitled to claim Dependant’s Benefit in r/o the death of the above‐noted deceased I.P., save and except those mentioned above.
1. ........................... 2. ........................... 3. ........................... 4. ...........................
ATTESTATION** Certified that the declarations, made above are true to the best of my knowledge and belief. * All major dependants should sign individually and the guardian to sign in case of a minor dependant. ** This certificate is to be given by (i) an officer of the Revenue, Judicial or Magisterial Departments of Government,
or (ii) a Municipal Commissioner, or (iii) a Workmen’s Compensation Commissioner, or (iv) the Head of the Gram‐Panchayat under the official seal of the Panchayat, or (v) M.L.A./M.P., (vi) Gazetted Officer, or (vii) a member of Local Committee/Regional Board of the ESI Corporation, or (viii) any other authority considered appropriate by the Branch Manager. IMPORTANT: Any person who makes a false statement or representation for the purpose of obtaining benefit, whether for himself or for some other person, commits an offence punishable with imprisonment for a term which may extend up to six months, or with a fine up to Rs. 2000 or with both.]
Signatures*
Name in Block letters and Rubber stamp or seal of the attesting authority
Signature............................. Designation.........................
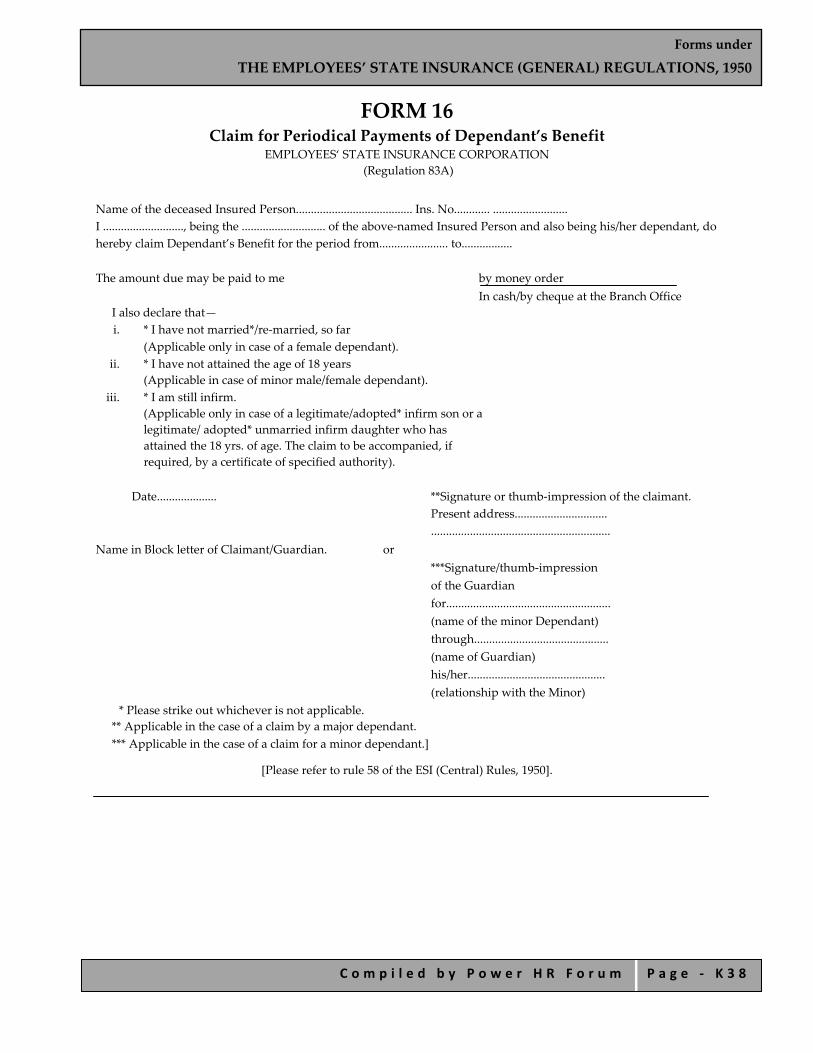
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 8
FORM 16 Claim for Periodical Payments of Dependant’s Benefit
EMPLOYEES‘ STATE INSURANCE CORPORATION (Regulation 83A)
Name of the deceased Insured Person....................................... Ins. No............ ......................... I ..........................., being the ............................ of the above‐named Insured Person and also being his/her dependant, do hereby claim Dependant’s Benefit for the period from....................... to................. The amount due may be paid to me by money order
In cash/by cheque at the Branch Office I also declare that— i. * I have not married*/re‐married, so far
(Applicable only in case of a female dependant). ii. * I have not attained the age of 18 years
(Applicable in case of minor male/female dependant). iii. * I am still infirm.
(Applicable only in case of a legitimate/adopted* infirm son or a legitimate/ adopted* unmarried infirm daughter who has attained the 18 yrs. of age. The claim to be accompanied, if required, by a certificate of specified authority).
Date.................... **Signature or thumb‐impression of the claimant.
Present address............................... ............................................................
Name in Block letter of Claimant/Guardian. or ***Signature/thumb‐impression of the Guardian for....................................................... (name of the minor Dependant) through............................................. (name of Guardian) his/her.............................................. (relationship with the Minor)
* Please strike out whichever is not applicable. ** Applicable in the case of a claim by a major dependant. *** Applicable in the case of a claim for a minor dependant.]
[Please refer to rule 58 of the ESI (Central) Rules, 1950].
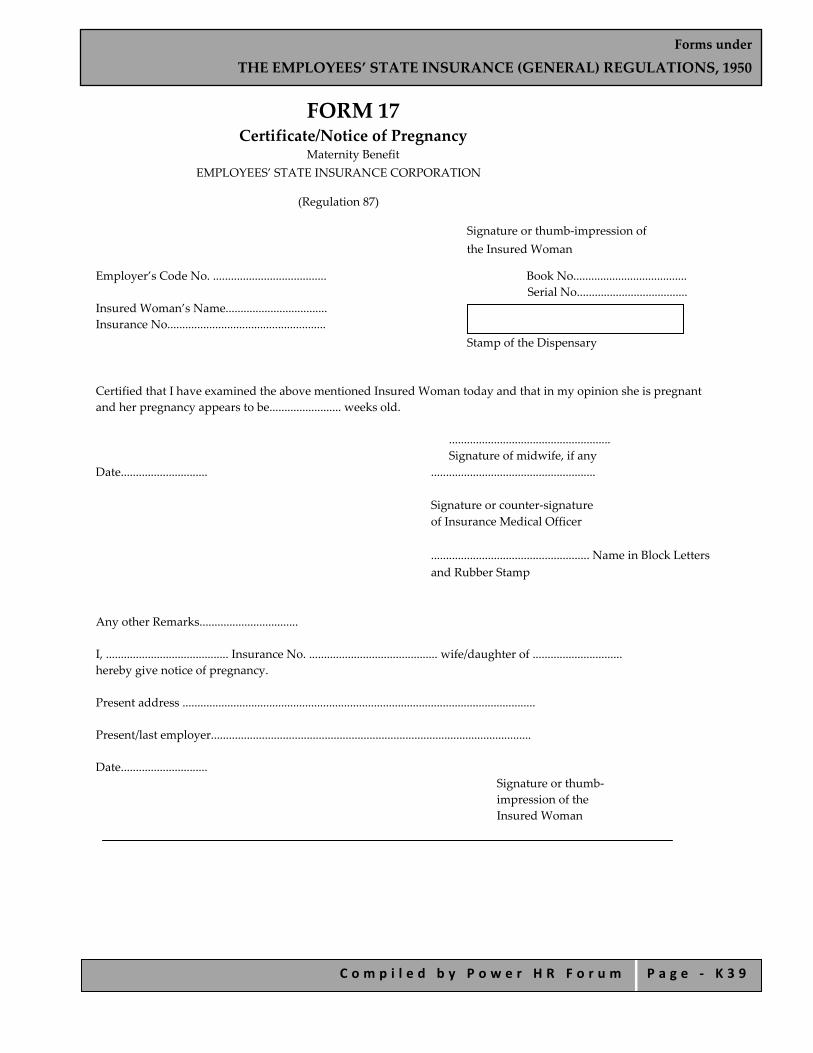
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 3 9
FORM 17 Certificate/Notice of Pregnancy
Maternity Benefit EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 87)
Signature or thumb‐impression of the Insured Woman
Employer’s Code No. ...................................... Book No...................................... Serial No.....................................
Insured Woman’s Name.................................. Insurance No.....................................................
Stamp of the Dispensary
Certified that I have examined the above mentioned Insured Woman today and that in my opinion she is pregnant and her pregnancy appears to be........................ weeks old.
...................................................... Signature of midwife, if any
Date............................. .......................................................
Signature or counter‐signature of Insurance Medical Officer ..................................................... Name in Block Letters and Rubber Stamp
Any other Remarks................................. I, ......................................... Insurance No. ........................................... wife/daughter of .............................. hereby give notice of pregnancy. Present address ...................................................................................................................... Present/last employer........................................................................................................... Date.............................
Signature or thumb‐impression of the Insured Woman
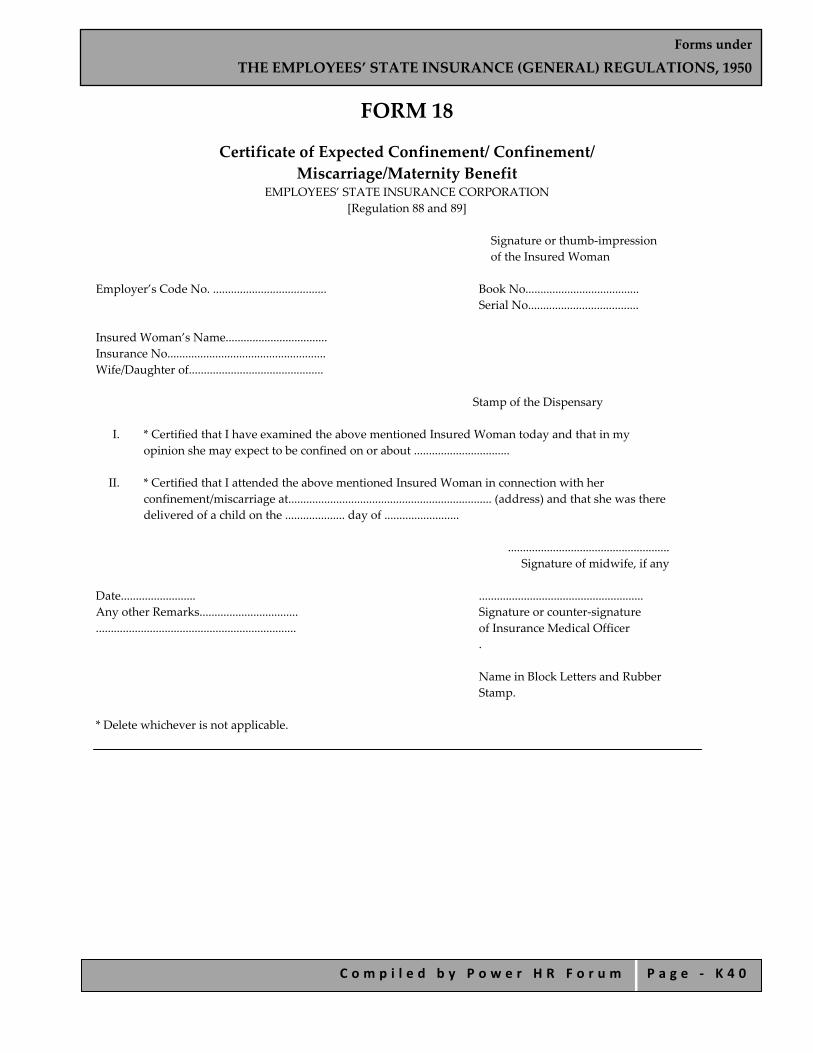
Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 0
FORM 18
Certificate of Expected Confinement/ Confinement/ Miscarriage/Maternity Benefit
EMPLOYEES’ STATE INSURANCE CORPORATION [Regulation 88 and 89]
Signature or thumb‐impression of the Insured Woman
Employer’s Code No. ...................................... Book No......................................
Serial No..................................... Insured Woman’s Name.................................. Insurance No..................................................... Wife/Daughter of.............................................
Stamp of the Dispensary
I. * Certified that I have examined the above mentioned Insured Woman today and that in my opinion she may expect to be confined on or about ................................
II. * Certified that I attended the above mentioned Insured Woman in connection with her
confinement/miscarriage at.................................................................... (address) and that she was there delivered of a child on the .................... day of .........................
......................................................
Signature of midwife, if any Date......................... ....................................................... Any other Remarks................................. Signature or counter‐signature ................................................................... of Insurance Medical Officer
.
Name in Block Letters and Rubber Stamp.
* Delete whichever is not applicable.

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 1
FORM 19 Claim for Maternity Benefit
and Notice of Work EMPLOYEES’ STATE INSURANCE CORPORATION
[Regulations 88 (ii), 89 and 91]
Signature or thumb‐impression of the Insured Woman
Employer’s Code No. ...................................... Book No......................................
Serial No.....................................
Insured Woman’s Name.................................. Insurance No. ................................................... Wife/Daughter of.............................................
Stamp of the Dispensary I, the above mentioned Insured Woman hereby claim Maternity Benefit for expected confinement/confinement*/miscarriage with effect from ............................. I, further declare that I have ceased*/shall cease to work for remuneration with effect from the aforesaid date. *I, do hereby give notice that I have taken up/shall take up work for remuneration with effect from the................ I have drawn maternity benefit only upto .......................... Present/last employer**................................................... Department, shift and occupation................................... Present address.................................................................. Signature or thumb‐impression ............................................................................................. of the Insured Woman Date................. Name of the Branch Office.........
* Please delete whichever not applicable. ** If not in employment, mention the particulars of last employer. IMPORTANT:
1. No work for remuneration should be taken up during the period for which Maternity Benefit is being claimed or is to be claimed.
2. Notice of resumption of work must be sent before any work is taken up. 3. Any person who makes a false statement or representation for the purpose of obtaining benefit, whether for
herself or for some other person commits an offence punishable with imprisonment for a term which may extend up to six months, or with a fine up to Rs. 2000, or with both.

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 2
FORM 20 Claim for Maternity Benefit after the Death
of an Insured Woman Leaving Behind the Child EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 89A)
Claim arising from the death on......................... of Ms........................................................ wife of/daughter of.........................................., having Insurance No.........................................and last employed by M/s.............................................................................................................. I .........................................., *being related to the above‐named deceased Insured Person as her.................................................. and being her nominee/being her legal representative (applicable if the I.W. dies leaving no nominee), hereby claim Maternity Benefit for the period from ................... to .................. . I also declare that—
1. **the deceased Insured Women died on ....................... leaving behind the child who is still alive; or 2. **the deceased Insured Women died on ....................... leaving behind the child who also died on...............
The amount due may be paid to me by money order/or in cash at Branch Office. I further declare that the particulars, as given here‐in‐above, are true to the best of my knowledge and belief.
Date.................
.................................................... Signature/Thumb‐Impression
of the Claimant Name in Block Letter and................................................. Address of claimant............................................................
............................................................
ATTESTATION ***Certified that the declarations, as made here‐in‐above, are true to the best of my knowledge and belief.
* Strike out this line if not applicable. ** Delete either (i) or (ii), as may not be applicable in the case. *** This certificate is to be given by (i) an officer of the Revenue, Judicial or Magisterial Department; or (ii) a
Municipal Commissioner; or (iii) a Workmen’s Compensation Commissioner; or (iv) the Head of the Gram‐Panchayat under the official seal of the Panchayat; or M.L.A./M.P.; or (v) A Gazetted Officer of the Central/State Govt./Member of the Local Committee/Regional Board, or (vi) any other authority considered as appropriate by the Branch Manager concerned.
IMPORTANT:
1. This claim form duly filled up, is required to be submitted to the appropriate Branch Office, together with a death certificate in Form 24B, within 30 days of the death of the Insured Woman.
2. Any person who makes a false statement or representation for the purpose of obtaining benefit, whether for himself or for some other person, commits an offence punishable with imprisonment for a term which may extend up to six months or with a fine up to Rs. 2000 or with both.
Name in Block letters and Rubber stamp or seal of the attesting authority
Signature Designation

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 3
FORM 21 Death Certificate in Case of Confinement
of Claiming Maternity Benefit EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 89A)
Book No................. Name of the deceased insured woman.................................................... Serial No................ w/d of ..................................................
Insurance No.........................................
I certify that in my opinion—
i. the above‐named deceased Insured Woman died on ............................., as a result of ............................................, during her confinement/*during a period of ......................, weeks
(cause of death)
immediately following her confinement, leaving behind the child.
ii. *the said child also died on .............................. as a result of ............................................
Also certified that I had been attending her*/and also her child for providing medical benefit before *her said child’s death and I attended her for the last time on.............................. and her said child for the last time on..............................
Any other remarks ................................................. ................................................. Date......................... ................................................................
Signature of Insurance Medical Officer/ Insurance Medical Practitioner
Note.—
1. *Delete whichever is not applicable. 2. The language may be suitably amended if the Insurance Medical Officer/Insurance Medical Practitioner had
not attended the deceased person before her/his child’s death.
Stamp of the Dispensary
Rubber Stamp and name in Block Letters

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 4
FORM 22
Funeral Expenses Claim Form EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 95E)
Claim arising from the death on ........................... of .......................................................... s/w/d of.................................................................. aged............... years, having Insurance No........................................................ and last employed as ............................................................by M/s. ................................................................. Code No. ......................................................... I ........................................................................ s/w/d of ................................................. aged .......................... years declare:—
i. *that I am the eldest surviving member of the family of the deceased Insured Person, whose particulars are furnished here‐in‐above, and that I actually incurred an expenditure of Rs. ................................ (Rupees ............................................... only) necessary for the funeral of the said deceased person.
or ii. *that the deceased Insured Person, whose particulars are furnished there‐in‐above, did not have a
family/was not living with his family at the time of his/her death and that I actually incurred an expenditure of Rs. ................................ (Rupees ............................................... only) necessary for the funeral of the said deceased insured person.
Accordingly, I do hereby claim funeral expenses for the amount of Rs. ................................ (Rupees ............................................... only).
Date....................... Name in Block ........................................................ Letters........................ Signature/thumb‐impression of the claimant
ATTESTATION
**Certified that the declarations, as made here‐in‐above, are true to the best of my knowledge and belief.
* Delete either (i) or (ii), which may not be applicable in the case.
** This certificate is to be given by (i) an officer of the Revenue, Judicial or Magisterial Department; or (ii) a Municipal Commissioner; or (iii) a Workmen’s Compensation Commissioner; or (iv) the Head of the Gram‐Panchayat under the official seal of the Panchayat; or M.L.A./M.P.; or (v) a Gazetted Officer of the Central/State Government, Local Committee/Regional Board; or (vi) any other authority considered as appropriate by the Branch Manager concerned.
Important.—Any person who makes a false statement or representation for the purpose of obtaining benefit, whether for himself or for some other person, commits an offence punishable with imprisonment for a term which may extend up to six months or with a fine up to Rs. 2000, or with both. Note.—In case of a minor, the guardian should sign the claim form on behalf of the minor and then add the
Name in Block letters and Rubber stamp or seal of the attesting authority
Signature Designation Date

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 5
following below his/her signature. ................................................
(Name of the minor) through …………………………..
(Name of the Guardian) his/her ......................................................
(Relationship with the Minor)

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 6
FORM 23 (To be submitted along with claim of June & December)
Life Certificate for Permanent Disablement Benefit EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 107)
Insurance No. of permanently disabled person
*Certified that Sh./Smt. ................................................... w/s/d of ....................................... is alive this day of ................... 20 ......... Name in Block letter of Signature............................................. Signing Claimant. Date................. .............................................................
Designation with Rubber stamp/ seal of the attesting authority
IMPORTANT.—Any person who makes a false statement or misrepresentation for the purpose of obtaining benefit, whether for himself or for some other person, commits an offence punishable with imprisonment for a term which may extend up to six moths or with a fine up to Rs. 2,000, or with both. *This certificate is to be given by (i) an officer of the Revenue, Judicial or Magisterial Department; or (ii) a Municipal Commissioner; or (iii) a Workmen’s Compensation Commissioner; or (iv) the Head of the Gram‐Panchayat under the official seal of the Panchayat; or (v) an M.L.A./M.P.; or (vi) a Gazetted Officer of the Central/ State Government; or (vii) a member of Local Committee/Regional Board of the ESIC; or (viii) any other authority considered as appropriate by the Branch Manager concerned.

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 7
FORM 24 (To be submitted along with claim of June & December)
Declaration and Certificate for Dependants’ Benefit EMPLOYEES’ STATE INSURANCE CORPORATION
(Regulation 107A)
Name of the deceased Insured person......................... Ins. No.
I ...................................................., being the ......................................... of the above‐named deceased Insured Person and also being his dependant, do hereby solemnly declare:—
i. *that I am not married/re‐married so far.
(to be given only by a female dependant)
ii. *that I have not yet attained the age of eighteen years
(to be given only in respect of a minor male or female dependant).
iii. *that I have attained the age of eighteen years but continue to be infirm.
(to be given by a legitimate/adopted infirm son or by a legitimate/adotped infirm daughter.
Certificate as specified, to be attached, if required)
Present Address:.........................................................................................................................
Date.................... .............................................................
Signature or thumb‐impression of the dependant or
Name in Block letters ............................................................. of signing claimant Signature or thumb‐impression of the Guadian in case of a minor dependant
Name of the Minor........................ Through..........................................
(name of the Guardian) his/her............................................ (relationship with the minor)
CERTIFICATE
**Certified that Sh./Smt./Kumari ................................................... w/s/d of ....................................... is alive this day, the ...................... day of ................... 20 ......... and that the declarations made above are true to the best of my knowledge and belief.
Name in Block letters and Rubber stamp or seal of the attesting authority
Signature …………………… Designation ……………………..
Date ………………………..

Forms under
THE EMPLOYEES’ STATE INSURANCE (GENERAL) REGULATIONS, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ K 4 8
* Strike out whichever is not applicable.
** This certificate is to be given by (i) an officer of the Revenue, Judicial or Magisterial Department; or (ii) a Municipal Commissioner; or (iii) a Workmen’s Compensation Commissioner; or (iv) the Head of Gram‐Panchayat under the official seal of the Panchayat; or (v) M.L.A./M.P.; or (vi) a Gazetted Officer of the Central/State Government; (vii) a member of the Local Committee/Regional Board of the ESIC; or (viii) any other authority considered as appropriate by the Branch Manager concerned.
IMPORTANT.— Any person who makes a false statement or misrepresentation for the purpose of obtaining benefit, whether for himself or for some other person, commits an offence punishable with imprisonment for a term which may extend up to six months or with a fine up to Rs. 2,000, or with both.
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1
Forms under the
THE WORKMEN’S COMPENSATION RULES, 1924

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 2
INDEX FORM AA Deposit of Compensation for Non‐Fatal Accident to
a Woman or Person under Legal Disability
FORM A Deposit of Compensation for Fatal Accident
FORM B Receipt for Compensation
FORM C Statement of Disbursements
FORM D Deposit of Compensation for Non‐Fatal Accidents, other than to a Woman or Person Under Legal Disability
FORM EE Report of Fatal Accidents
FORM E Receipt for Compensation
FORM F Application for Compensation by Workman
FORM G Application for Order to Deposit Compensation
FORM H Application for Commutation
FORM JJ Notice to Appear to Contest the Claim for Compensation
FORM J Notice to Appear to Contest the Claim for Compensation
FORM K Memorandum of Agreement
FORM L Memorandum on Agreement
FORM M Memorandum of Agreement
FORM N Notice to Receive any Objections under an Agreement
FORM O Notice Intimating the Reasons for Which an Agreement Has Been Refused
FORM P Notice Giving Opportunity to Show Cause on Why The Agreement Should be Registered
FORM Q Notice Giving Opportunity to Show Cause on Why The Agreement Should be Registered
FORM R Register of Agreements

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 3
FORM A [See rule 6 (1)]
Deposit of Compensation for Fatal Accident [Section 8 (1) of the Workmen ʹs Compensation Act, 1923]
1. Compensation amounting to Rs. ..............is hereby presented for deposit in respect of injuries
resulting in the death of the workman, whose particulars are given below, which occurred on ........................ Name ........................ Father’s Name ........................ (Husband’s name in case of married woman and widow.) Caste........................ Local address .................................. Permanent address .................................. His/Her monthly wages are estimated at Rs.................. He/ She was over/ under the age of 15 years at the time of his/her death.
2. The said workman had, prior to the date of his/her death, received the following payments, namely:— Rs. ................ on ........................ Rs. ................ on ........................ Rs. ................ on ....................... Rs. ................ on ........................ Rs. ................ on ........................ Rs. ................ on ....................... amounting in all to Rs.................
3. An advance of Rs .............. has been made on account of compensation to .................. being his/her dependant.
4. *I do not desire to be made a party to the proceedings for distribution of the aforesaid compensation. Dated .................... 20.....
Employer. *An employer desiring to be made a party to the proceedings should strike out the words “do not”.
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 4
FORM AA [See rule 6 (1)]
Deposit of Compensation for Non‐Fatal Accident to a Woman or Person under Legal Disability
[Section 8 (1) of the Workmen ʹs Compensation Act, 1923] 1. Compensation amounting to Rs ................ is hereby presented for deposit in respect of injuries
sustained by ......................... residing at ................................... on ............... 20..... resulting in the loss of/temporary disablement. His/Her monthly wages are estimated at Rs. ............... He/She was over/under the age of 15 years at the time of the accident.
2. The said injured workman has prior to the date of the deposit received the following half‐ monthly payments, namely:— Rs. .............. on ........................ Rs. .............. on ........................ Rs. .............. on ........................ Rs. .............. on ........................ Rs. .............. on ........................ Rs. .............. on ........................
Dated..............20..... Employer
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 5
FORM B (See rule 6)
Receipt for Compensation [Deposited under section 8 (1) of the Workmen’s Compensation Act, 1923]
Book No. .................................. Receipt No............... Register No. .............. Depositor .............................
Deceased or injured workman ............................. Date of deposit ............ 20..... Sum deposited Rs ...............
Commissioner.

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 6
FORM C (See rule 6)
Statement of Disbursements [Section 8 (4) of the Workmen’s Compensation Act, 1923]
Serial No. ............. Depositor ....................................... Date .....................20.......... Amount deposited....................... Amount deducted and repaid to the employer under the proviso to section 8 (1) ........ Funeral expenses paid ............ Compensation paid to the following dependants :
Name Relationship
Total —
Dated .................. 20..... Commissioner

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 7
FORM D [See rule 9]
Deposit of Compensation for Non‐Fatal Accidents, other than to a Woman or Person under Legal Disability
[Section 8 (2) of the Workmen’s Compensation Act, 1923] Compensation amounting to Rs. .............. is hereby presented for deposit in respect of
permanent/temporary injuries sustained by .................. residing at ....................... which occcurred on........... 20.....
Dated .............. 20.....
Employer

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 8
FORM E (See rule 9)
Receipt for Compensation [Deposited under section 8 (2) of the Workmen’s Compensation Act, 1923]
Book No. .............. Receipt No. .............. Register No. .............. Depositor ............................ In favour of ............................ Date of deposit .............. 20..... Sum deposited Rs. ..............
Commissioner

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 9
FORM EE [See rule 11]
Report of Fatal Accidents To
...................
................... Sir,
I have the honour to submit the following report of an accident which occurred on................... (date) at ................... (here enter details of premises) and which resulted in the death of the workman/workmen of whom particulars are given in the statement annexed.
2. The circumstances attending the death of the workman/workmen were as under : (a) Time of the accident (b) Place where the accident occurred (c) Manner in which deceased was/were employed at the time (d) Cause of the accident (e) Any other relevant particulars
I have etc. (Signature and designation of person making the report.)
STATEMENT
Name Sex Age Nature of Employment
Full Postal Address
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 0
FORM F (See rule 20)
Application for Compensation by Workman To
The Commissioner for Workmen’s Compensation, ............................................................................. .................... residing at..........................applicant, Versus ..................residing at................................opposite party. It is hereby submitted that—
1. The applicant, a workman employed by (a contractor with) the opposite party on the .............. day of .............. 20....., received personal injury by accident arising out of and in the course of his employment. The cause of the injury was (here insert briefly in ordinary language the cause of the injury)..................................................................................................................................................
2. The applicant sustained the following injuries, namely:— ............................................................................................................................................................. 3. The monthly wages of the applicant amounts to Rs .............. The applicant is over/under the age of 15 years.
4. *
a) Notice of the accident was served on the .............. day of ........................ b) Notice was served as soon as practicable. c) Notice of the accident was not served (in due time) by reason of .......................
5. The applicant is accordingly entitled to receive — a) half‐monthly payment of Rs.......from the............ day of 20..... to .................. b) a lump sum payment of Rs ..........
6. The applicant has taken the following steps to secure a settlement by agreement, namely .................................but it has proved impossible to settle the questions in dispute because................................................................................................................................... * You are therefore requested to determine the following questions in dispute, namely:— a) whether the applicant is a workman within the meaning of the Act ; b) whether the accident arose out of or in the course of the applicant’s employment; c) whether the amount of compensation claimed is due, or any part of that amount; d) whether the opposition party is liable to pay such compensation as is due ; e) etc. (as required) .
Dated ........................ 20.... Applicant.
*Strike out the clauses which are not applicable.
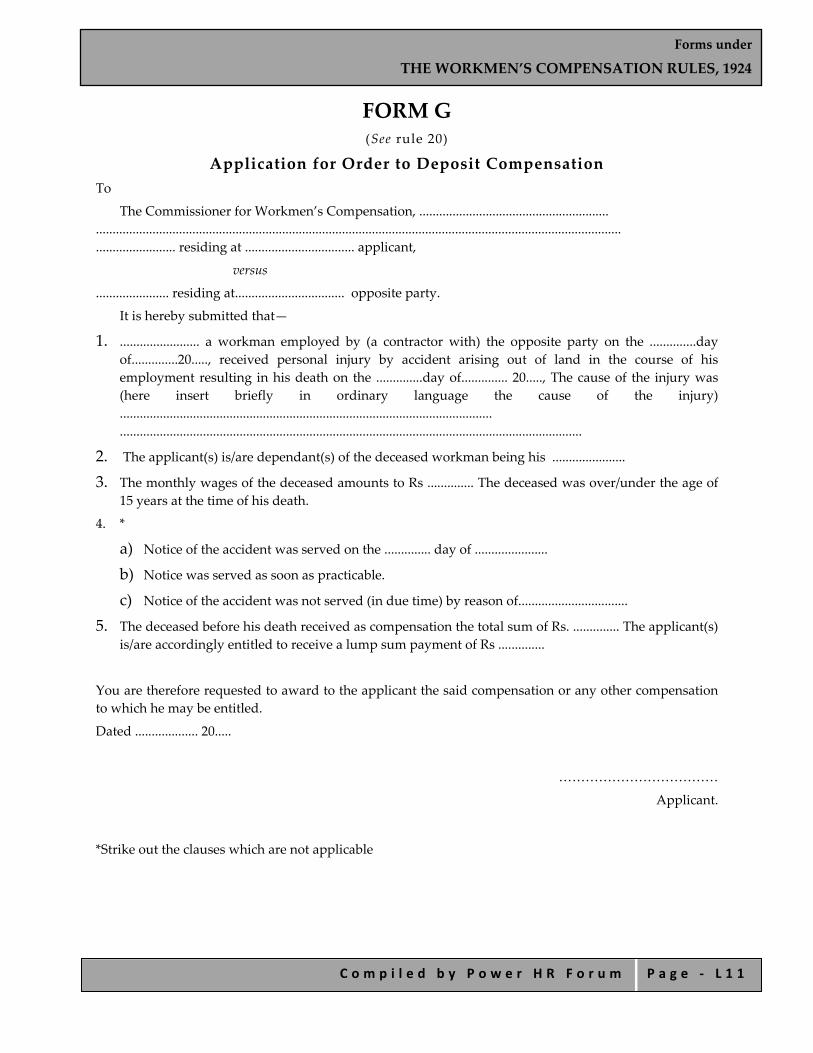
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 1
FORM G (See rule 20)
Application for Order to Deposit Compensation To
The Commissioner for Workmen’s Compensation, ......................................................... .............................................................................................................................................................. ........................ residing at ................................. applicant,
versus ...................... residing at................................. opposite party.
It is hereby submitted that— 1. ........................ a workman employed by (a contractor with) the opposite party on the ..............day
of..............20....., received personal injury by accident arising out of land in the course of his employment resulting in his death on the ..............day of.............. 20....., The cause of the injury was (here insert briefly in ordinary language the cause of the injury) ................................................................................................................ ...........................................................................................................................................
2. The applicant(s) is/are dependant(s) of the deceased workman being his ...................... 3. The monthly wages of the deceased amounts to Rs .............. The deceased was over/under the age of
15 years at the time of his death. 4. *
a) Notice of the accident was served on the .............. day of ...................... b) Notice was served as soon as practicable. c) Notice of the accident was not served (in due time) by reason of.................................
5. The deceased before his death received as compensation the total sum of Rs. .............. The applicant(s) is/are accordingly entitled to receive a lump sum payment of Rs ..............
You are therefore requested to award to the applicant the said compensation or any other compensation to which he may be entitled. Dated ................... 20.....
……………………………… Applicant.
*Strike out the clauses which are not applicable
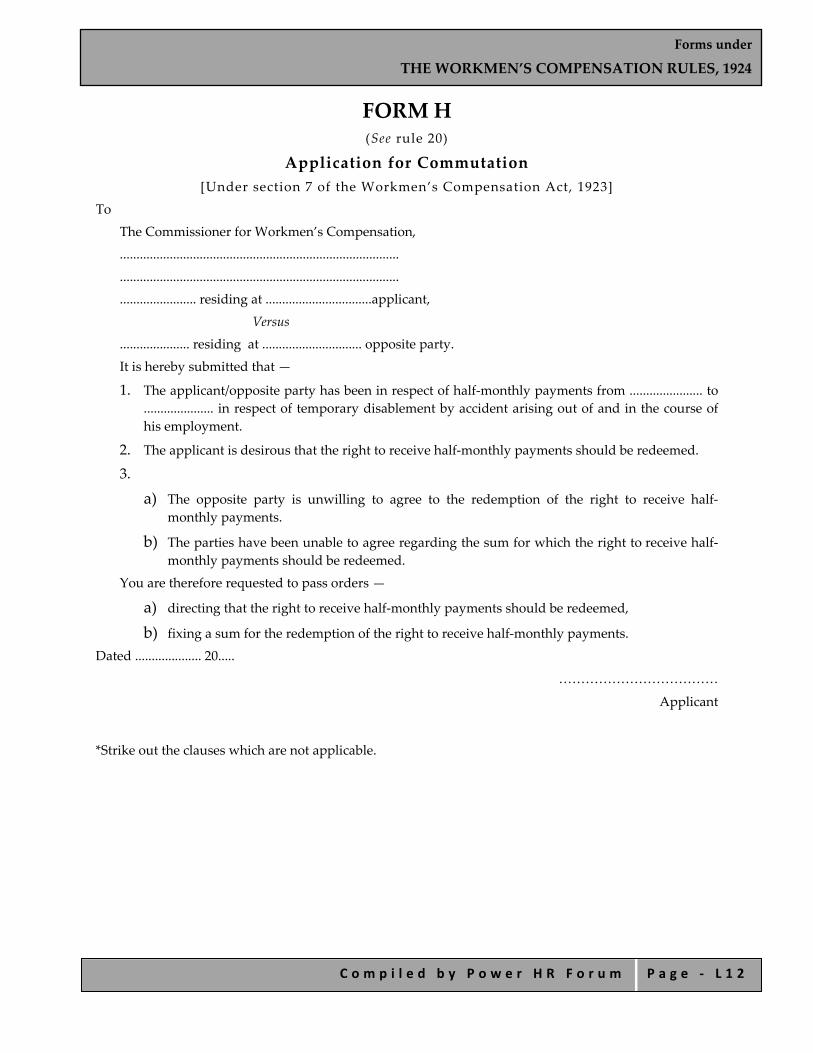
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 2
FORM H (See rule 20)
Application for Commutation [Under section 7 of the Workmen’s Compensation Act, 1923]
To The Commissioner for Workmen’s Compensation, .................................................................................... .................................................................................... ....................... residing at ................................applicant, Versus ..................... residing at .............................. opposite party. It is hereby submitted that — 1. The applicant/opposite party has been in respect of half‐monthly payments from ...................... to
..................... in respect of temporary disablement by accident arising out of and in the course of his employment.
2. The applicant is desirous that the right to receive half‐monthly payments should be redeemed. 3.
a) The opposite party is unwilling to agree to the redemption of the right to receive half‐monthly payments.
b) The parties have been unable to agree regarding the sum for which the right to receive half‐monthly payments should be redeemed.
You are therefore requested to pass orders — a) directing that the right to receive half‐monthly payments should be redeemed, b) fixing a sum for the redemption of the right to receive half‐monthly payments.
Dated .................... 20.....
……………………………… Applicant
*Strike out the clauses which are not applicable.
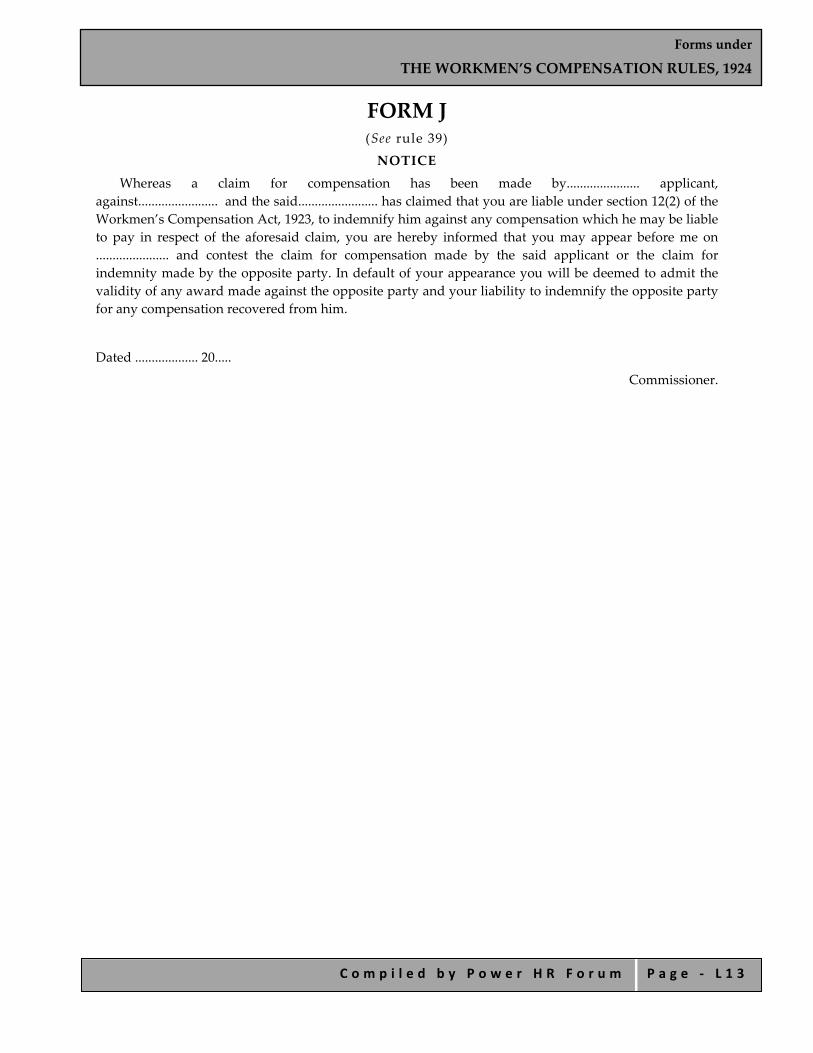
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 3
FORM J (See rule 39) NOTICE
Whereas a claim for compensation has been made by...................... applicant, against........................ and the said........................ has claimed that you are liable under section 12(2) of the Workmen’s Compensation Act, 1923, to indemnify him against any compensation which he may be liable to pay in respect of the aforesaid claim, you are hereby informed that you may appear before me on ...................... and contest the claim for compensation made by the said applicant or the claim for indemnity made by the opposite party. In default of your appearance you will be deemed to admit the validity of any award made against the opposite party and your liability to indemnify the opposite party for any compensation recovered from him.
Dated ................... 20.....
Commissioner.
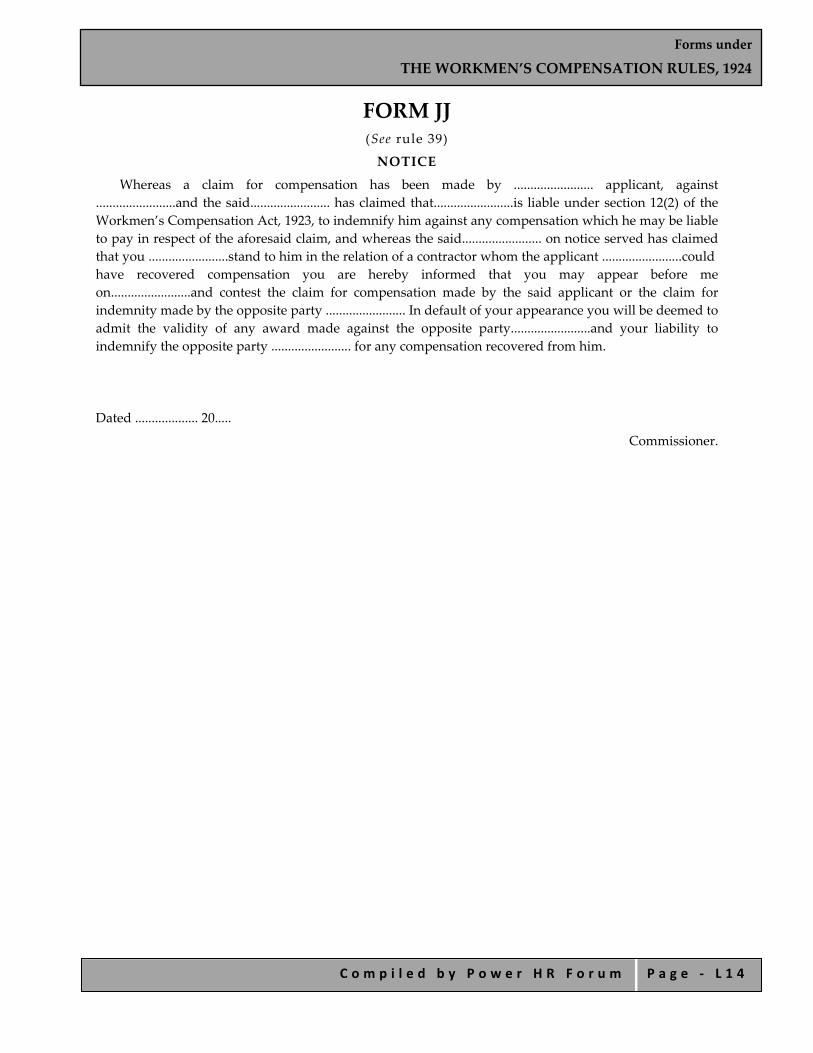
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 4
FORM JJ (See rule 39) NOTICE
Whereas a claim for compensation has been made by ........................ applicant, against ........................and the said........................ has claimed that........................is liable under section 12(2) of the Workmen’s Compensation Act, 1923, to indemnify him against any compensation which he may be liable to pay in respect of the aforesaid claim, and whereas the said........................ on notice served has claimed that you ........................stand to him in the relation of a contractor whom the applicant ........................could have recovered compensation you are hereby informed that you may appear before me on........................and contest the claim for compensation made by the said applicant or the claim for indemnity made by the opposite party ........................ In default of your appearance you will be deemed to admit the validity of any award made against the opposite party........................and your liability to indemnify the opposite party ........................ for any compensation recovered from him.
Dated ................... 20..... Commissioner.

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 5
FORM K (See rule 48)
Memorandum of Agreement It is hereby submitted that on the ........... day of .............. 20..... personal injury was caused
to........................residing at................................ by accident arising out of and in the course of employment in ........................ The said injury has resulted in temporary disablement to the said workman whereby it is estimated that he will be prevented from earning more than of his previous/any wage for a period of........... months. The said workman has been in receipt of half‐monthly payments which have continued from the ........... day of...........20 ..... until the ........... day of...........20..... amounting to Rs . ........... in all. The said workmen’s monthly wages are estimated at Rs........... The workman is over the age of 15 years/will reach the age of 15 years on ....................
It is further submitted that .................... the employer of said workman has agreed to pay, and the said workman has agreed to accept, the sum of Rs ........... in full settlement of all and every claim under the Workmen’s Compensation Act, 1923, in respect of all disablement of a temporary nature arising out of the said accident, whether now or hereafter to become manifest. It is, therefore, requested that this memorandum be duly recorded.
Dated.................20....... Signature of employer....................................... Witness........................ Signature of workman........................ Witness........................ Note.—An application to register an agreement can be presented under the signature of one party,
provided that the other party has agreed to the terms. But both signatures should be appended, whenever possible.
Receipt to be filled in when the money has actually been paid In accordance with the above agreement, I have this day received the sum of
Rs. ...............
........................Workman. Dated ................... 20.....
The money has been paid and this receipt signed in my presence. ........................Witness. Note.—This form may be varied to suit special cases, e.g., injury by occupational diseases, agreement
when workman is under legal disability, etc.
Revenue Stamp
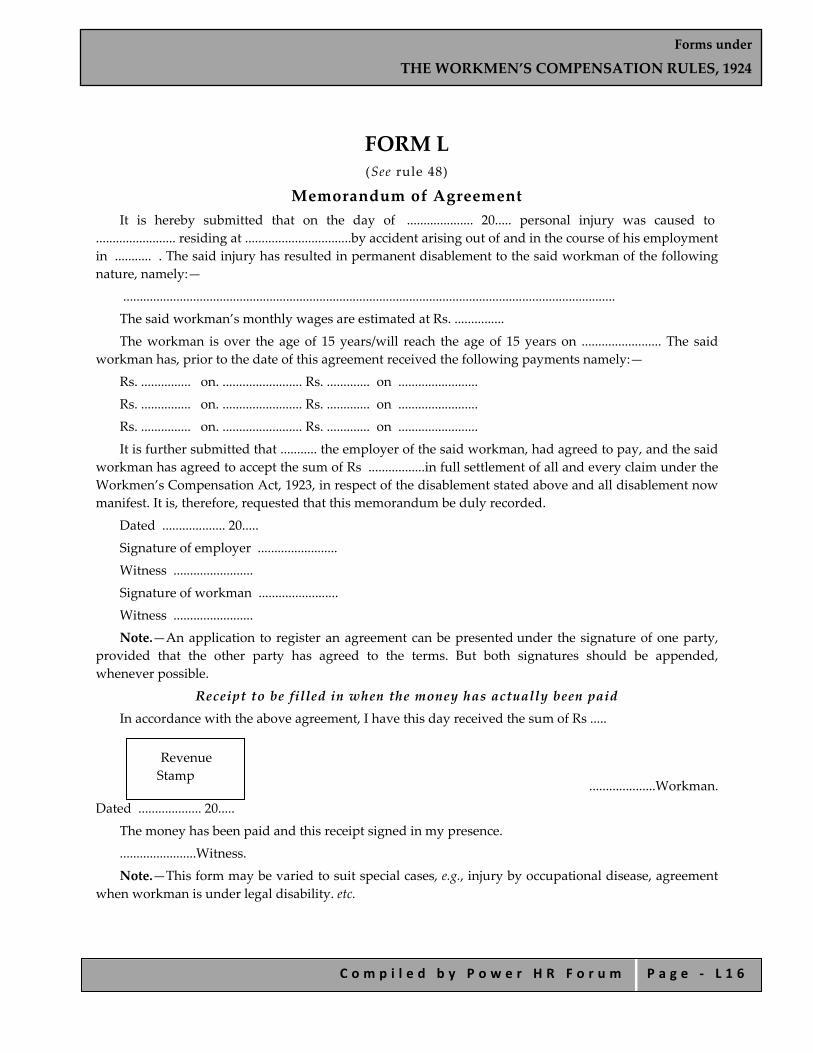
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 6
FORM L (See rule 48)
Memorandum of Agreement It is hereby submitted that on the day of .................... 20..... personal injury was caused to
........................ residing at ................................by accident arising out of and in the course of his employment in ........... . The said injury has resulted in permanent disablement to the said workman of the following nature, namely:—
.................................................................................................................................................... The said workman’s monthly wages are estimated at Rs. ............... The workman is over the age of 15 years/will reach the age of 15 years on ........................ The said
workman has, prior to the date of this agreement received the following payments namely:— Rs. ............... on. ........................ Rs. ............. on ........................ Rs. ............... on. ........................ Rs. ............. on ........................ Rs. ............... on. ........................ Rs. ............. on ........................ It is further submitted that ........... the employer of the said workman, had agreed to pay, and the said
workman has agreed to accept the sum of Rs .................in full settlement of all and every claim under the Workmen’s Compensation Act, 1923, in respect of the disablement stated above and all disablement now manifest. It is, therefore, requested that this memorandum be duly recorded.
Dated ................... 20..... Signature of employer ........................ Witness ........................ Signature of workman ........................ Witness ........................ Note.—An application to register an agreement can be presented under the signature of one party,
provided that the other party has agreed to the terms. But both signatures should be appended, whenever possible.
Receipt to be filled in when the money has actually been paid In accordance with the above agreement, I have this day received the sum of Rs .....
....................Workman. Dated ................... 20.....
The money has been paid and this receipt signed in my presence. .......................Witness. Note.—This form may be varied to suit special cases, e.g., injury by occupational disease, agreement
when workman is under legal disability. etc.
Revenue Stamp

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 7
FORM M (See rule 48)
Memorandum of Agreement It is hereby submitted that on the ............... day of ................20..... personal injury was caused to
........................ residing at ................................ by accident arising out of and in the course of employment in
....................... The said injury has resulted in temporary disablement to the said workman, who is at present in receipt of wages amounting to Rs. ........................ per month/ no wages . The said workman’s monthly wages prior to the accident are estimated at Rs ............ The workman is subject to a legal disability by reason of........................................................................................................................................... .....................................................................................................................
It is further submitted that ........................., the employer of the workman has agreed to pay and ........................ on behalf of the said workman has agreed to accept half‐monthly payments at the rate of Rs. .............. for the period of the said temporary disablement. This agreement is subject to the condition that the amount of the half‐monthly payments may be varied in accordance with the provisions of the said Act, on account of an alteration in the earnings of the said workman during disablement. It is further stipulated that all rights of commutation under section 7 of the said Act are unaffected by this agreements. It is, therefore, requested that this memorandum be duly recorded.
Dated .................. 20...... Signature of employer. Witness ........................ Signature of workman ........................ Witness ........................ Note.—An application to register an agreement can be presented under the signature of one party,
provided that the other party has agreed to the terms. But both signatures should be appended, whenever possible.
Receipt to be filled in when the money has actually been paid In accordance with the above agreement, I have this day received the sum of Rs.......
.....................Workman.
Dated ................... 20.... The money has been paid and this receipt signed in my presence. ...................................Witness. Note.—This form may be varied to suit special cases, e.g., injury by occupational disease, etc.
Revenue Stamp

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 8
FORM N (See rule 49)
Whereas an agreement to pay compensation is said to have been reached between ........................ and ........................and whereas ........................has/have applied for registration of the agreement under section 28 of the Workmen’s Compensation Act, 1923, notice is hereby given that the said agreement will be taken into consideration on .................... 20...., and that any objections to the registration of the said agreement should be made on that date. In the absence of valid objections it is my intention to proceed to the registration of the agreement.
Dated ................... 20..... Commissioner
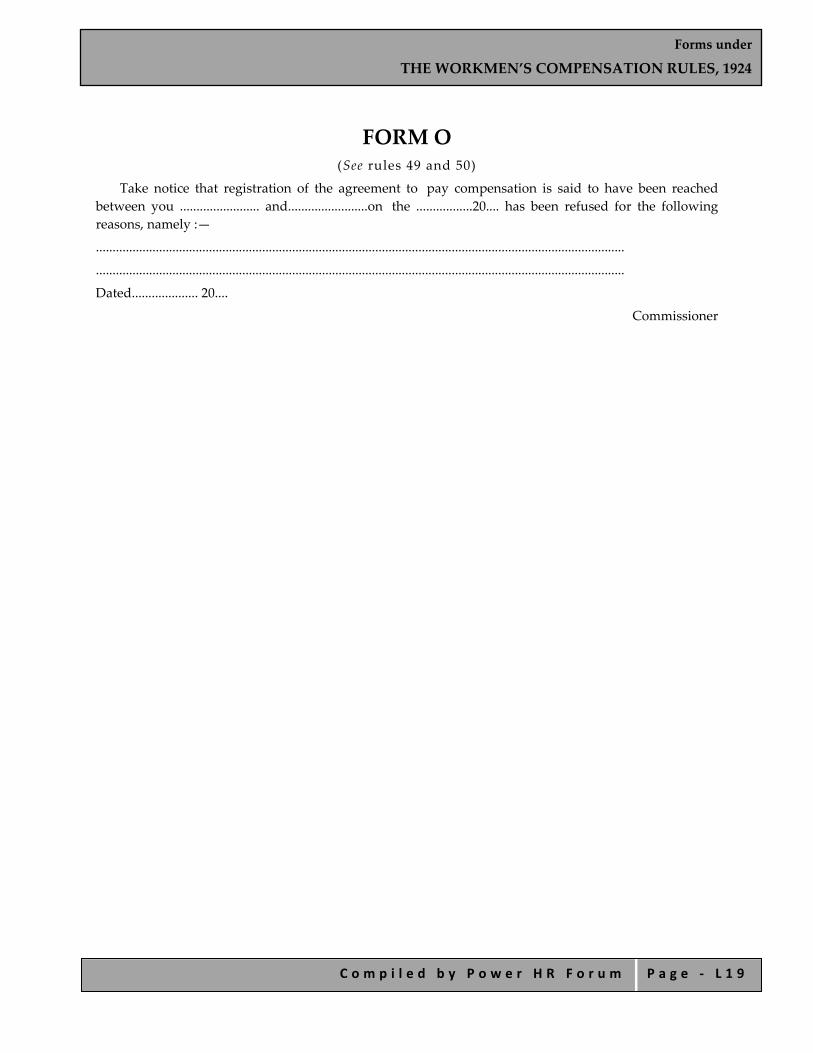
Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 1 9
FORM O (See rules 49 and 50)
Take notice that registration of the agreement to pay compensation is said to have been reached between you ........................ and........................on the .................20.... has been refused for the following reasons, namely :— ............................................................................................................................................................... ............................................................................................................................................................... Dated.................... 20....
Commissioner

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 2 0
FORM P (See rule 50)
Whereas an agreement to pay compensation is said to have been reached between ........................ and ........................ and whereas ........................has /have applied for registration of the agreement under section 28 of the Workmen’s Compensation Act, 1923, and whereas it appears to me that the said agreement ought not to be registered for the following reasons, namely:— ..................................................................................................................................................................... an opportunity will be afforded to your showing of cause on ..................19...../20....., why the said agreement should be registered. If no adequate cause is shown on that date registration of the agreement will be refused. Dated..................
Commissioner

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 2 1
FORM Q (See rule 50)
Whereas an agreement to pay compensation is said to have been reached between ........................ and........................and whereas ........................ has/have applied for registration of the agreement under section 28 of the Workman’s Compensation Act, 1923, and whereas it appears to me that the said agreement ought not to be registered for the following reasons, namely:— ........................................................................................................................................................... ........................................................................................................................................................................... an opportunity will be afforded to the said ........................of showing cause on ....................20..... why the said agreement should be registered. Any representation which you have to make with regard to the said agreement should be made on that date. If adequate cause is then shown, the agreement may be registered. Dated ...................20.....
Commissioner

Forms under
THE WORKMEN’S COMPENSATION RULES, 1924
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ L 2 2
FORM R (See rule 52)
REGISTER OF AGREEMENTS FOR THE YEAR 20....... ......
Serial
Number Date of
Agreement Date of
RegistrationEmployer Workman
Initials of Commissioner
Reference to orders rectifying the register

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1
Forms under the THE MINIMUM WAGES (CENTRAL) RULES, 1950
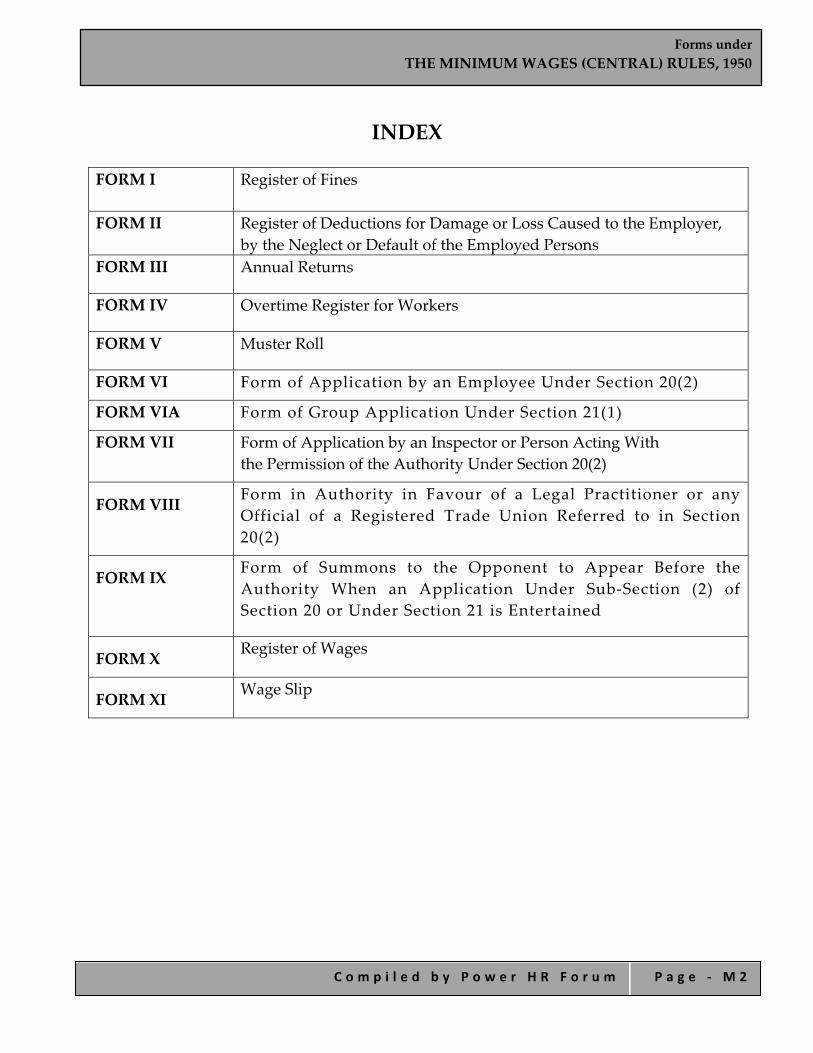
Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 2
INDEX FORM I
Register of Fines
FORM II Register of Deductions for Damage or Loss Caused to the Employer, by the Neglect or Default of the Employed Persons
FORM III Annual Returns
FORM IV Overtime Register for Workers
FORM V Muster Roll
FORM VI Form of Application by an Employee Under Section 20(2)
FORM VIA Form of Group Application Under Section 21(1)
FORM VII Form of Application by an Inspector or Person Acting With the Permission of the Authority Under Section 20(2)
FORM VIII
Form in Authority in Favour of a Legal Practitioner or any Official of a Registered Trade Union Referred to in Section 20(2)
FORM IX
Form of Summons to the Opponent to Appear Before the Authority When an Application Under Sub‐Section (2) of Section 20 or Under Section 21 is Entertained
FORM X Register of Wages
FORM XI Wage Slip

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 3
FORM I Register of Fines
[Rule 21(4)]
..............................................Employer……………………………………..
Serial No.
Name Fatherʹs/ Husbandʹs Name
Sex Department Nature and date of the offence for
which fine
imposed
Whether workman showed cause
against fine or not, if so enter date
Rate of wages
Date and amount of fine imposed
Date on which fine
realized
Remarks
1 2 3 4 5 6 7 8 9 10 11
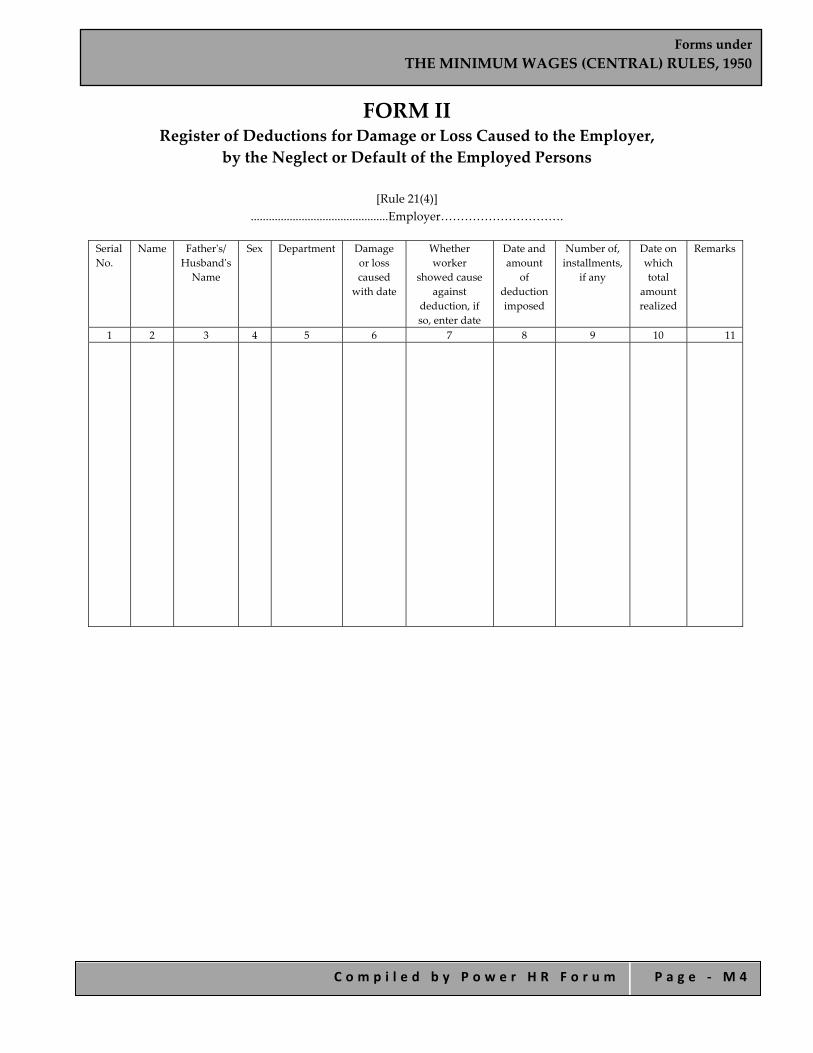
Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 4
FORM II Register of Deductions for Damage or Loss Caused to the Employer,
by the Neglect or Default of the Employed Persons
[Rule 21(4)] ..............................................Employer………………………….
Serial No.
Name Fatherʹs/ Husbandʹs Name
Sex Department Damage or loss caused
with date
Whether worker
showed cause against
deduction, if so, enter date
Date and amount
of deduction imposed
Number of, installments,
if any
Date on which total
amount realized
Remarks
1 2 3 4 5 6 7 8 9 10 11
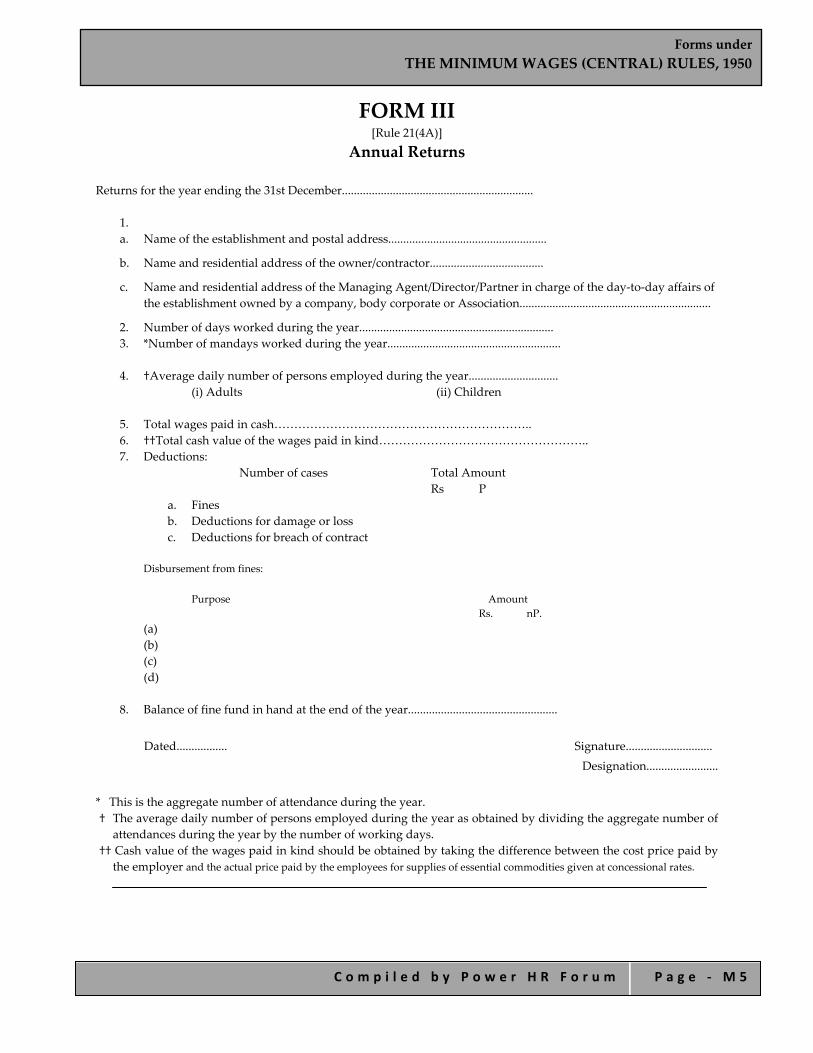
Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 5
FORM III [Rule 21(4A)]
Annual Returns Returns for the year ending the 31st December................................................................
1. a. Name of the establishment and postal address.....................................................
b. Name and residential address of the owner/contractor......................................
c. Name and residential address of the Managing Agent/Director/Partner in charge of the day‐to‐day affairs of the establishment owned by a company, body corporate or Association................................................................
2. Number of days worked during the year................................................................. 3. *Number of mandays worked during the year..........................................................
4. †Average daily number of persons employed during the year..............................
(i) Adults (ii) Children
5. Total wages paid in cash……………………………………………………….. 6. ††Total cash value of the wages paid in kind…………………………………………….. 7. Deductions:
Number of cases Total Amount Rs P
a. Fines b. Deductions for damage or loss c. Deductions for breach of contract
Disbursement from fines:
Purpose Amount Rs. nP.
(a) (b) (c) (d)
8. Balance of fine fund in hand at the end of the year..................................................
Dated................. Signature.............................
Designation........................
* This is the aggregate number of attendance during the year. † The average daily number of persons employed during the year as obtained by dividing the aggregate number of
attendances during the year by the number of working days. †† Cash value of the wages paid in kind should be obtained by taking the difference between the cost price paid by
the employer and the actual price paid by the employees for supplies of essential commodities given at concessional rates.
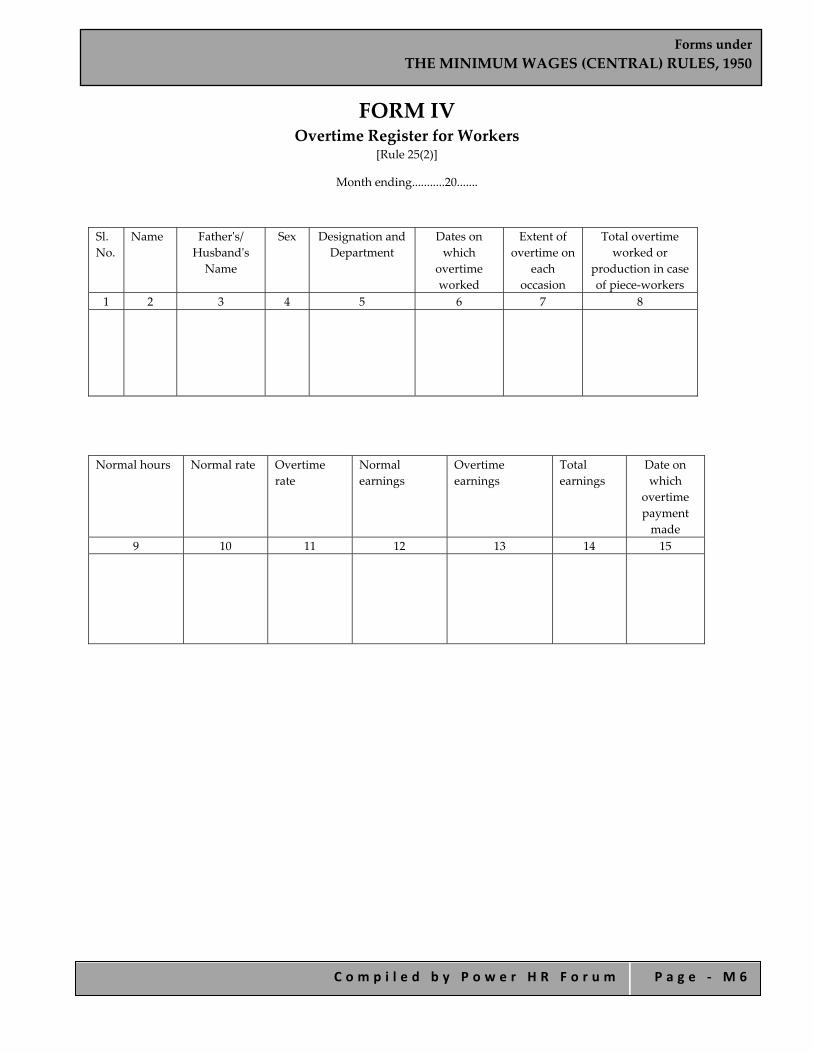
Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 6
FORM IV Overtime Register for Workers
[Rule 25(2)]
Month ending...........20.......
Sl. No.
Name Fatherʹs/ Husbandʹs Name
Sex Designation and Department
Dates on which
overtime worked
Extent of overtime on
each occasion
Total overtime worked or
production in case of piece‐workers
1 2 3 4 5 6 7 8
Normal hours Normal rate Overtime rate
Normal earnings
Overtime earnings
Total earnings
Date on which
overtime payment made
9 10 11 12 13 14 15

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 7
FORM V Muster Roll
[Rule 26(5)]
Name of Establishment................................................... Place.......................................................
S.No. Name Fatherʹs/
Husbandʹs Name
Sex Nature of
work
For the period ending…….. [Total attendance] Remarks.....................
1 2 3 4 5

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 8
FORM VI Form of Application by an Employee under Section 20(2)
In the Court of the Authority appointed under the Minimum Wages Act, 1948, for.. . . . . . . . . . . . . . . . . . . . . . . . . . .area.
Application No........................... of 20......... (1).......................................................................Applicant (through........................ a legal practitioner/an official of
................... which is a registered Trade Union), Address................................................
Versus (1)................................................ (2)................................................ (3)................................................ Opponent(s) Address................................................ The applicant above named states as follows:—
1) The applicant was/has been employed from.............to..........as..........(Category) in........................(establishment) of Shri/Messrs...............engaged in............... (nature of work) which is a scheduled employment within the meaning of section 2(g) of the Minimum Wages Act.
2) The opponent(s) is/are the employer(s) within the meaning of section 2(e) of the Minimum Wages Act.
3)
a. * The applicant has been paid wages at less than the minimum rate of wages fixed for his category of employment under the Act by Rs.........per day for the period from.........to...........;
b. * The applicant has not been paid wages at Rs.....................per day for weekly days of rest from........to..........;
c. * The applicant has not been paid wages at the over time rate for the period from................to............
4) The applicant estimates the value of relief sought by him on each account as under:
a. Rs..............................
b. Rs..............................
c. Rs.............................. Total Rs..............................
5) The applicant, therefore, prays that a direction may be issued under section 20(3) of the Act for:
a. * payment of the difference between the wages payable under the Minimum Wages Act and the wages actually paid.
b. * payment of remuneration for the days of rest. c. * payment of wages at the overtime rates. d. compensation amounting to Rs........
Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 9
6) The applicant begs leave to amend or add to or make alterations in the application, if and when necessary, with the permission of the Authority.
7) The applicant does solemnly declare that the facts stated in this application are true to the best of his knowledge, belief and information.
Date..........................
Signature or thumb impression of the employed person, or legal practitioner or official of a Registered Trade Union duly authorized.
*Delete the portions not required.

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1 0
FORM VIA Form of Group Application under Section 21(1)
In the Court of the Authority appointed under the Minimum Wages Act, 1948 for.......................... area Application No.........................of 20................ Between A.B.C. and (state the number)............................others: Applicants (through a legal practitioner/an official of ......................... which is a registered trade Union), Address..........................
and x.y.z ...........................................................opposite party Address..........................
The applicants state as follows:— 1) The applicants whose names appear in the attached schedule were/have been employed from..............
to................ as............... (Categories).................... in................ (Establishment) of Shri/Messrs............. engaged in .................... (nature of work) which is/are scheduled employment(s) within the meaning of section 2(g) of the Minimum Wages Act.
2) The opponent(s) is/are the employer(s) within the meaning of section 2(e) of the Minimum Wages Act. 3)
a. *the applicants have been paid wages at less than the minimum rates of wages fixed for their category (categories) of employment(s) under the Act by Rs................ per day for the period (s) from...............to.......;
b. *The applicants have not been paid wages at Rs............. per day for the weekly days of rest from..............to..................;
c. *The applicants have not been paid wages at the overtime rates(s) for the period from............ to........................;
4) The applicants estimate the value of relief sought by them on each account as under:
a. Rs........................
b. Rs........................
c. Rs........................ Total Rs.....................
5) The applicants, therefore, pray that a direction may be issued under section 20(3) of the Act for:
a. *payment of the difference between the wages payable under the Minimum Wages Act and the wages actually paid;
b. *payment of remuneration for the days of rest;
c. *payment of wages at the overtime rate(s);
d. compensation amounting to Rs........

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1 1
6) The applicants beg leave to amend or add to or make alterations in the application, if and when necessary, with the permission of the Authority.
7) The applicants do solemnly declare that the facts stated in this application are true to the best of their knowledge, belief and information.
Date........................
Signature or thumb impression of the employed persons or legal practitioner, or official of a Registered Trade Union duly authorized.
*Delete the portions not required.

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1 2
FORM VII Form of Application by an Inspector or Person Acting with
the Permission of the Authority under Section 20(2)
In the Court of the Authority appointed under the Minimum Wages Act, 1948, for.................................area.
Application No.............................. of 20................ (1) ........................................................................Applicant Address................................................................................
Versus
(1) ....................................................................Opponent(s) Address................................................................................ The applicant above named states as follows:— 1. The opponent(s) has/have—
a. *paid wages at less than the minimum rates of wages fixed for their cateogry (categories) of employment(s) under the Act by Rs...................... per day for the period(s) from........................to........................;
b. *not paid wages at Rs.............................per day for the weekly days of rest from...........................to.....................; c. *not paid wages at overtime rate(s) for the period from.................. to...........to the following employees;
2. The applicant estimates the value of relief sought for the employees on each account as under:
a. Rs........................
b. Rs........................
c. Rs........................ Total Rs........................
3. The applicant, therefore, prays that a direction may be issued under section 20(3) of the Act for:
a. *payment of the difference between the wages payable under the Minimum Wages Act and the wages actually paid;
b. *payment of remuneration for the days of rest; c. *payment of wages at the overtime rate(s); d. compensation amounting to Rs............
4. The applicant begs leave to amend or add to or make alternations in the application, if and when necessary, with the permission of the Authority.
5. The applicant does solemnly declare that the facts stated in this application are true to the best of his knowledge, belief and information. Date....................... Signature……………………… *Delete the portion not required.

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1 3
FORM VIII Form in Authority in Favour of a Legal Practitioner or any Official
of a Registered Trade Union Referred to in Section 20(2) In the Court of the Authority appointed under the Minimum Wages Act, 1948
for.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .area. Application No.....................of 20.......... (1).......................................................................................................................... (2).......................................................................................................Applicant(s)† (3) .......................................................................................................................
Versus (1) ................................................................................................................................... (2) .......................................................................................................Opponent(s) (3) ...................................................................................................................... I hereby authorize Mr. ..........................a legal practitioner/an official of the registered trade union of
.......................... to appear and act on my behalf in the above described proceedings and to do all things incidental to such appearing and acting.
Date.......................
Signature or thumb impression of the employee.
† When the application is by a group of employees, the thumb impression or signatures of two of the applicants need be put to the application and a full list of applicants should be attached to the application.

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1 4
FORM IX Form of Summons to the Opponent to Appear Before the Authority
When an Application under Sub‐Section (2) of Section 20 or under Section 21 is Entertained
(Title of the application) To...................................................(Name, description and place of residence) Whereas........................has made the above said application to me under the Minimum Wages Act, 1948, you are
hereby summoned to appear before me in person or by a duly authorised agent, and able to answer all material questions relating to the application, or who shall be accompanied by some person able to answer all such questions on the.........day of ........20............. at................ Oʹclock in the................. noon, to answer the claim; and as the day fixed for the appearance is appointed for the final disposal of the application, you must be prepared to produce on that day all the witnesses upon whose evidence and all the documents upon which you intend to rely in support of your defence.
Take notice that in default of your appearance on the day before mentioned, the application will be heard and determined in your absence.
Date..................... Signature.
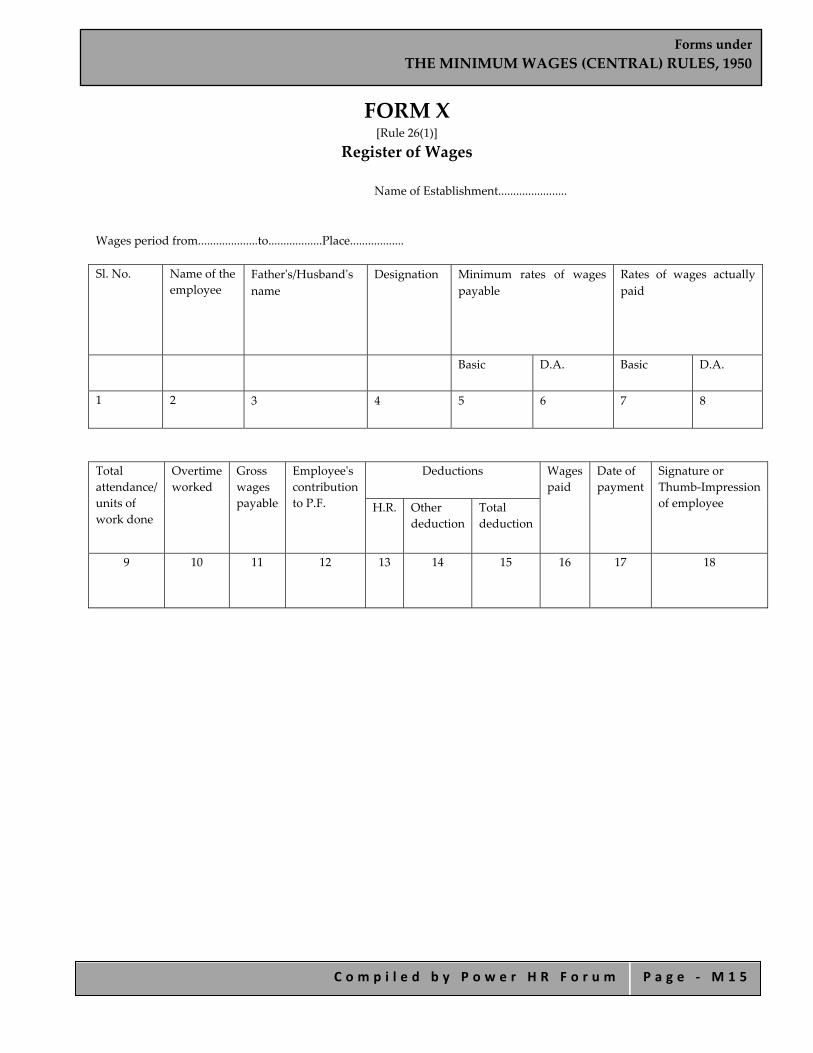
Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1 5
FORM X [Rule 26(1)]
Register of Wages
Name of Establishment.......................
Wages period from....................to..................Place..................
Sl. No.
Name of the employee
Fatherʹs/Husbandʹs name
Designation Minimum rates of wages payable
Rates of wages actually paid
Basic D.A. Basic D.A.
1 2 3 4 5 6 7 8
Total attendance/ units of work done
Overtime worked
Gross wages payable
Employeeʹs contribution to P.F.
Deductions
Wages paid
Date of payment
Signature or Thumb‐Impression of employee H.R.
Other deduction
Total deduction
9 10 11 12 13 14 15 16 17 18

Forms under THE MINIMUM WAGES (CENTRAL) RULES, 1950
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ M 1 6
FORM XI [Rule 26(2)]
Wage Slip Name of the establishment....................................
Place.............................................. 1. Name of employee with fatherʹs/husbandʹs name.......................................... 2. Designation 3. Wages Period. 4. Rate of wages payable:
(a) Basic (b) D.A.
5. Total attendance/units of work done 6. Overtime wages. 7. Gross wages payable 8. Total deductions 9. Net wages paid
Pay‐in‐charge Employeeʹs signature/thumb impression].

Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 1
Forms under
PAYMENT OF WAGES (PROCEDURE) RULES, 1937
Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 2
INDEX
FORM A
Form of Individual Application
FORM B
Form of Group Application
FORM C
Form of Application by an Inspector or Person Permitted by the Authority or Authorised to Act
FORM D
Certificate of Authorisation
FORM E
Notice for the Disposal of Application
FORM F
Record of Order or Direction
FORM G
Notice to Respondent of the Day Fixed for The Hearing of the Appeal under Section 17 of The Payment of Wages Act, 1936
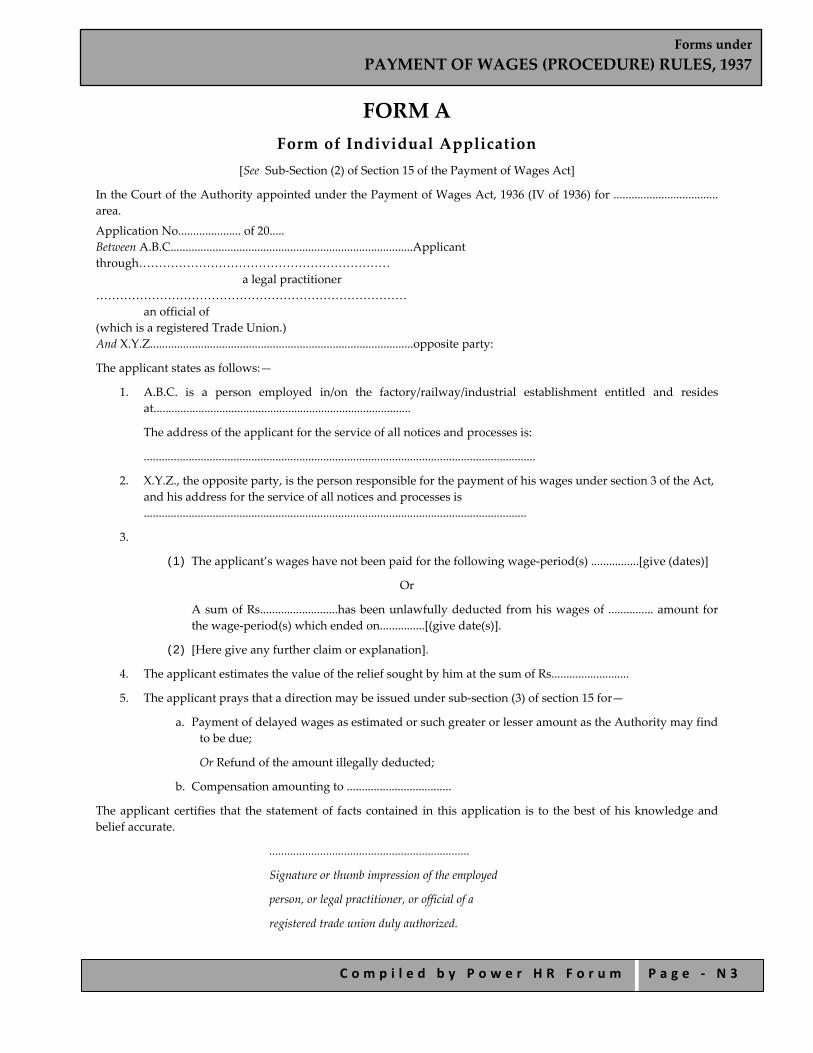
Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 3
FORM A Form of Individual Application
[See Sub‐Section (2) of Section 15 of the Payment of Wages Act]
In the Court of the Authority appointed under the Payment of Wages Act, 1936 (IV of 1936) for ................................... area.
Application No..................... of 20..... Between A.B.C.................................................................................Applicant through………………………………………………………
a legal practitioner ……………………………………………………………………
an official of (which is a registered Trade Union.) And X.Y.Z........................................................................................opposite party:
The applicant states as follows:—
1. A.B.C. is a person employed in/on the factory/railway/industrial establishment entitled and resides at......................................................................................
The address of the applicant for the service of all notices and processes is:
...................................................................................................................................
2. X.Y.Z., the opposite party, is the person responsible for the payment of his wages under section 3 of the Act, and his address for the service of all notices and processes is ................................................................................................................................
3.
(1) The applicant’s wages have not been paid for the following wage‐period(s) ................[give (dates)]
Or
A sum of Rs..........................has been unlawfully deducted from his wages of ............... amount for the wage‐period(s) which ended on...............[(give date(s)].
(2) [Here give any further claim or explanation].
4. The applicant estimates the value of the relief sought by him at the sum of Rs..........................
5. The applicant prays that a direction may be issued under sub‐section (3) of section 15 for—
a. Payment of delayed wages as estimated or such greater or lesser amount as the Authority may find to be due;
Or Refund of the amount illegally deducted;
b. Compensation amounting to ...................................
The applicant certifies that the statement of facts contained in this application is to the best of his knowledge and belief accurate.
...................................................................
Signature or thumb impression of the employed
person, or legal practitioner, or official of a
registered trade union duly authorized.
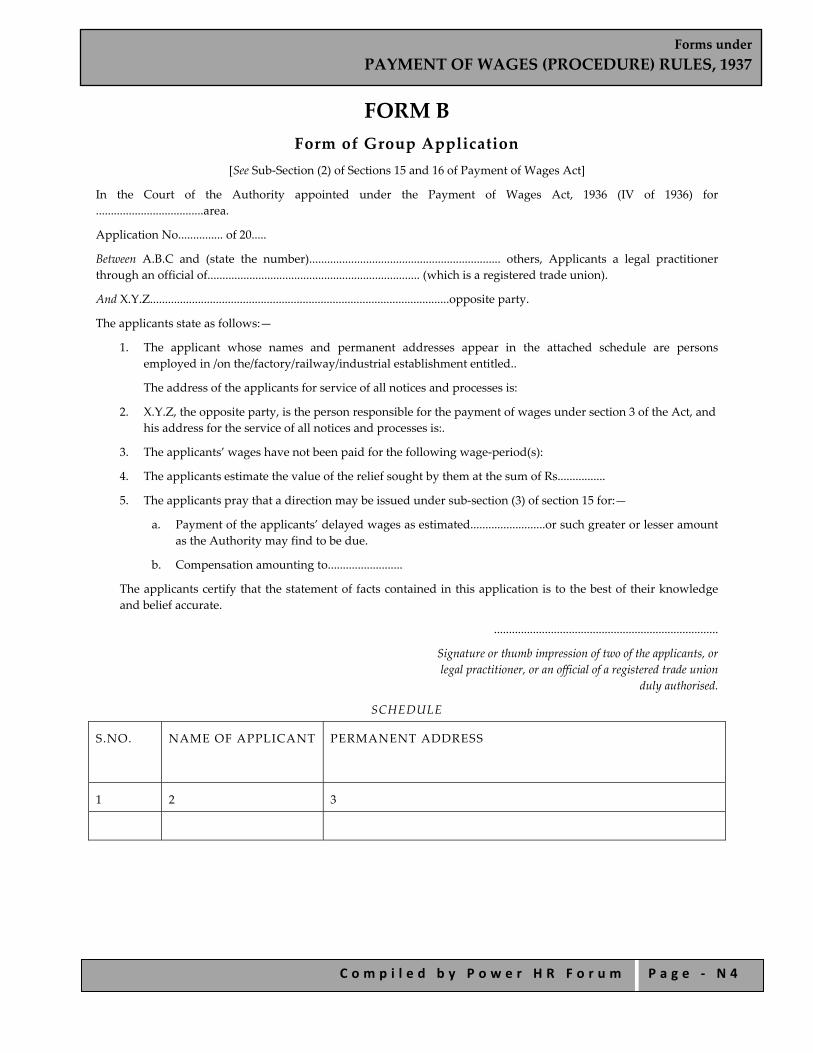
Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 4
FORM B Form of Group Application
[See Sub‐Section (2) of Sections 15 and 16 of Payment of Wages Act]
In the Court of the Authority appointed under the Payment of Wages Act, 1936 (IV of 1936) for ....................................area.
Application No............... of 20.....
Between A.B.C and (state the number)................................................................ others, Applicants a legal practitioner through an official of....................................................................... (which is a registered trade union).
And X.Y.Z....................................................................................................opposite party.
The applicants state as follows:—
1. The applicant whose names and permanent addresses appear in the attached schedule are persons employed in /on the/factory/railway/industrial establishment entitled..
The address of the applicants for service of all notices and processes is:
2. X.Y.Z, the opposite party, is the person responsible for the payment of wages under section 3 of the Act, and his address for the service of all notices and processes is:.
3. The applicants’ wages have not been paid for the following wage‐period(s):
4. The applicants estimate the value of the relief sought by them at the sum of Rs................
5. The applicants pray that a direction may be issued under sub‐section (3) of section 15 for:—
a. Payment of the applicants’ delayed wages as estimated.........................or such greater or lesser amount as the Authority may find to be due.
b. Compensation amounting to.........................
The applicants certify that the statement of facts contained in this application is to the best of their knowledge and belief accurate.
...........................................................................
Signature or thumb impression of two of the applicants, or legal practitioner, or an official of a registered trade union
duly authorised.
SCHEDULE
S.NO.
NAME OF APPLICANT PERMANENT ADDRESS
1 2 3
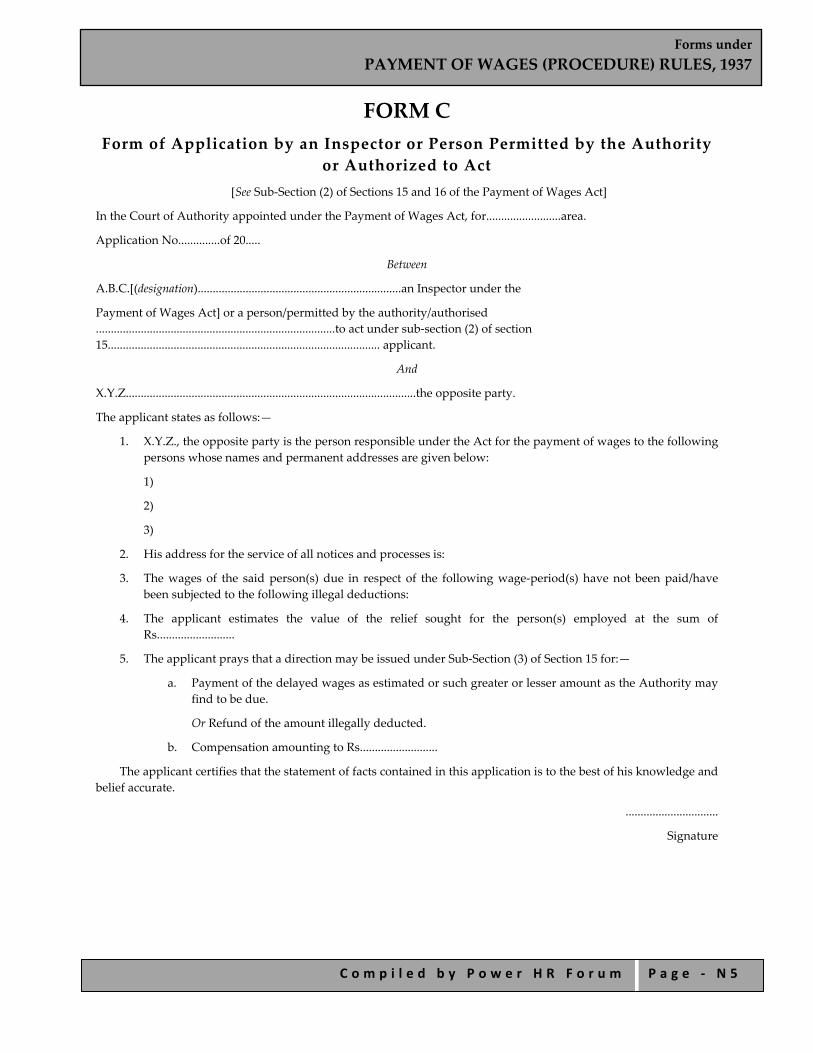
Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 5
FORM C Form of Application by an Inspector or Person Permitted by the Authority
or Authorized to Act [See Sub‐Section (2) of Sections 15 and 16 of the Payment of Wages Act]
In the Court of Authority appointed under the Payment of Wages Act, for.........................area.
Application No..............of 20.....
Between
A.B.C.[(designation)....................................................................an Inspector under the
Payment of Wages Act] or a person/permitted by the authority/authorised ................................................................................to act under sub‐section (2) of section 15........................................................................................... applicant.
And
X.Y.Z.................................................................................................the opposite party.
The applicant states as follows:—
1. X.Y.Z., the opposite party is the person responsible under the Act for the payment of wages to the following persons whose names and permanent addresses are given below:
1)
2)
3)
2. His address for the service of all notices and processes is:
3. The wages of the said person(s) due in respect of the following wage‐period(s) have not been paid/have been subjected to the following illegal deductions:
4. The applicant estimates the value of the relief sought for the person(s) employed at the sum of Rs..........................
5. The applicant prays that a direction may be issued under Sub‐Section (3) of Section 15 for:—
a. Payment of the delayed wages as estimated or such greater or lesser amount as the Authority may find to be due.
Or Refund of the amount illegally deducted.
b. Compensation amounting to Rs..........................
The applicant certifies that the statement of facts contained in this application is to the best of his knowledge and belief accurate.
...............................
Signature

Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 6
FORM D Certificate of Authorization
I/We employed person(s) hereby authorise a legal practitioner/an official of................................ which is a registered trade union to act on my/our behalf under section 15 and section 17 of the Payment of Wages Act, 1936 (IV of 1936), in respect of the claim against.........................on account of the delay in payment/illegal deduction from my/our wages for.........................
Witnesses Signatures
(1) (1)
(2) (2)
(3) (3)
(4) (4)
I accept the authorisation.
.............................................
Signature
Legal practitioner/ Official of a registered trade union
Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 7
FORM E Notice for the Disposal of Application
To
Whereas under the Payment of Wages Act, 1936 (IV of 1936) a claim against you has been presented to me in the application of which a copy is enclosed, you are hereby called upon to appear before me either in person or by any person duly instructed, and able to answer all material questions relating to the application, or who shall be accompanied by some person able to answer all material questions relating to the application, or who shall be accompanied by some person able to answer all such questions, on the ........................day of.........................20.........at............o’clock in the forenoon/afternoon to answer the claim; and as the day fixed for your appearance is appointed for the final disposal of the application, you must be prepared to produce on that day all the witnesses upon whose evidence, and the documents upon which you intend to rely in support of your defence.
Take notice that, in default of your appearance on the day before mentioned, the application will be heard and determined in your absence.
Given under my hand and seal, this day of..............20......
.........................
Authority
SEAL
Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 8
FORM F Record of Order or Direction
1) Serial number.........................
2) Date of the application.........................
3) Name or names, parentage, address or addresses of the applicants, or some, or all of the applicants belonging to the same unpaid group……………………………………………..
4) Name and address of the employer……………………………….
5) Amount claimed…………………..
a. as delayed wages: Rs ..........................
b. as deducted from wages: Rs.........................
6) Plea of the employer and his examination (if any):
7) Finding, and a brief statement of the reasons therefor…………………….
8) Amounts awarded……………
a. Delayed wages ........................
b. Deducted wages.........................
9) Compensation awarded.........................
10) Penalty imposed.........................
11) Costs awarded to:
a. Court‐fee charges.........................
b. Pleader’s fee.........................
c. Witnesses’ expenses.........................
12) Date by which the amounts awarded shall be paid.
Signed.........................
Dated..........................
Note:—In case where an appeal lies, attach on a separate sheet the substance of the evidence.

Forms under PAYMENT OF WAGES (PROCEDURE) RULES, 1937
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ N 9
FORM G Notice to Respondent of the Day Fixed for the Hearing of the Appeal under
Section 17 of the Payment of Wages Act, 1936
Appeal from the decision of the Authority for the................................... area dated the..............day of..................20......
To
Respondent
Take notice that an appeal of which a copy is enclosed, from the decision of the Authority for...................................area has been presented by X.Y.Z. (and others), and registered in this Court, and that the ..............day of..............20....., has been fixed by this Court for the hearing of the appeal.
If no appearance is made on your behalf by yourself, or by some one by law authorised to act for you in this appeal, it will be heard and decided in your absence.
Given under my hand and the seal of the Court, this...............day of...............20......
.........................
Judge
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1
Forms under
PAYMENT OF GRATUITY (CENTRAL) RULES, 1972

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2
INDEX FORM A Notice of Opening
FORM B Notice of Change
FORM C Notice of Closure
FORM D Notice for Excluding Husband from Family
FORM E Notice of Withdrawal of Notice for Excluding Husband from Family
FORM F Nomination
FORM G Fresh Nomination
FORM H Modification of Nomination
FORM I Application of Gratuity by an Employee
FORM J Application for Gratuity by a Nominee
FORM K Application for Gratuity by a Legal Heir
FORM L Notice for Payment of Gratuity
FORM M Notice Rejecting Claim for Payment of Gratuity
FORM N Application for Direction
FORM O Notice for Appearance Before the Controlling Authority
FORM P Summons
FORM Q Particulars of Application under Section 7
FORM R Notice for Payment of Gratuity
FORM S
Notice for Payment of Gratuity as Determined by Appellate Authority
FORM T Application for Recovery of Gratuity
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 3
FORM ‐A [See Sub‐Rule (1) of Rule 3]
Notice of Opening
1. Name and address of the Establishment. 2. Name and designation of the Employer 3. Number of persons employed. 4. Maximum number of persons employed on any day during the preceding twelve months with date. 5. Number of employees covered by the Act. 6. Nature of industry. 7. Whether seasonal. 8. Date of opening. 9. Details of Head Office/Branches.
a) Name and address of the head office. Number of employees. b) Names and addresses of other branches in India.
1. 2. 3.
I verify that the information furnished above is true to the best of my knowledge and belief. Place............................. Signature of the employer Date............................. with name and designation To The Controlling Authority ........................................ .......................................
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 4
FORM ‐B [See Sub‐Rule (2) of Rule 3]
Notice of Change Name and address of the Establishment,
Take notice that following changes have taken place with effect from ....................... in the particulars furnished by me in notice dated ........................... on Form ‘A’.
Name. Address. Name of the employer. Nature of business Place............................. Signature of the employer Date............................. with name and designation To The Controlling Authority ........................................ ........................................

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 5
FORM ‐C [See Sub‐Rule (3) of Rule 3]
Notice of Closure Take notice that it is intended to close down the establishment with effect from .................. The other details are
furnished below:
1. Name and address of the establishment. 2. Name and address of the Head Office, if any. 3. Name and designation of the employer. 4. Number of persons in employment. 5. Number of employees entitled to Gratuity. 6. Amount of Gratuity involved.
Place............................. Signature of the employer Date............................. with name and designation To The Controlling Authority ........................................ ......................................

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 6
FORM‐D [See Sub‐Rule (1) of Rule 5]
Notice for Excluding Husband from Family From ............................................................................. 1. Name of the female employee. 2. Name or description of establishment where employed. 3. Post held with Ticket or Serial No., if any. 4. Department/Branch/Section where employed. 5. Permanent address.
Take notice that I, Shrimati ..................... desire to exclude my husband Shri .....................from my family for the purposes of the Payment of Gratuity Act, 1972. Place............................. Signature/Thumb impression Date............................. of the employee.
Declaration by witnesses
The above notice was signed/thumb impressed before me. Name in full and full Signature of witnesses. address of witnesses. 1. 1. 2. 2. Place............................ Date............................. To The Controlling Authority. (Through the employer) [Name and address of the employer here]
For use by the employer Received and recorded in this establishment.
Date............................. Reference No. Signature of the employer or an officer authorised in this behalf by the employer
To 1. ............................... (Employee) 2. The Controlling Authority. Note : strike out the words not applicable

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 7
FORM ‐ E [See Sub‐Rule (2) of Rule 5]
Notice of Withdrawal of Notice for Excluding Husband from Family 1. Name of the female employee. 2. Name or description of establishment where employed. 3. Post held with Ticket or Serial No., if any. 4. Department/Branch/Section where employed. 5. Permanent address.
Take notice that I, Shrimati .................... hereby withdraw the notice dated .................... whereby I exclude my husband Shri ................... from my family for the purposes of the Payment of Gratuity Act, 1972. The earlier notice was recorded under your reference No. ............dated ......................... Place............................. Signature/Thumb impression Date............................. of the employee.
Declaration by witnesses The above notice of withdrawal was signed/thumb impressed before me. Name in full and full Signature of witnesses. address of witnesses. 1. 1. 2. 2. Place............................ Date............................. To The Controlling Authority.(Through the employer) [Name and address of the employer]
For use by the employer Received and recorded in this establishment.
Reference No. Date.............................
To 1. ........................... (Employee) 2. The Controlling Authority.
Note : strike out the words not applicable
Signature of the employer or officer authorized or Seal or rubber stamp of the establishment.
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 8
FORM ‐ F [See Sub‐Rule (1) of Rule 6]
Nomination To ...............................................................................................................................................
[Give here name or description of the establishment with full address]
I, Shri/Shrimati/Kumari .........................................…………………………..
[Name in full here]
whose particulars are given in the statement below, hereby nominate the person(s) mentioned below to receive the gratuity payable after my death as also the gratuity standing to my credit in the event of my death before that amount has become payable, or having become payable has not been paid and direct that the said amount of gratuity shall be paid in proportion indicated against the name(s) of the nominee(s).
2. I hereby certify that the person(s) mentioned is a/are member(s) of my family within the meaning of clause (h) of section (2) of the Payment of Gratuity Act, 1972.
3. I hereby declare that I have no family within the meaning of clause (h) of section (2) of the said Act. 4.
a. My father/mother/parents is/are not dependant on me.
b. My husband’s father/mother/parents is/are not dependant on my husband.
5. I have excluded my husband from my family by a notice dated the ................ to the Controlling Authority in terms of the proviso to clause (h) of section 2 of the said Act.
6. Nomination made herein invalidates my previous nomination.
Nominee(s)
Name in full with full address of nominee(s)
Relationship with the employee
Age of nominee
Proportion by which the gratuity will be shared
1. 2. 3. so on.
Statement
1. Name of employee in full. 2. Sex. 3. Religion. 4. Whether unmarried/married/widow/widower. 5. Department/Branch/Section where employed. 6. Post held with Ticket or Serial No., if any. 7. Date of appointment. 8. Permanent address. Village ................... Thana ................... Sub‐division ................... Post Office ................... District ................... State ................... Place............................ Signature/Thumb impression Date............................. of the employee
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 9
Declaration by witnesses
Nomination signed/thumb impressed before me.
Name in full and full Signature of witnesses. address of witnesses.
1. 1. 2. 2.
Place............................
Date.............................
Certificate by the employer
Certified that the particulars of the above nomination have been verified and recorded in this establishment.
Employer’s Reference No., if any.
Signature of the employer/ officer authorised
Designation
Date............................. Name and address of the establishment or rubber stamp thereof.
Acknowledgement by the employee
Received the duplicate copy of nomination in Form ‘F’ filed by me and duly certified by the employer.
Date............................. Signature of the employee
Note : strike out the words not applicable
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 0
FORM ‐ G
[See Sub‐Rule (3) of Rule 6]
Fresh Nomination To
[Give here name or description of the establishment with full Address]
I, Shri/Shrimati ..............................................................................................................
[Name in full here]
whose particulars are given in the statement below, have acquired a family within the meaning of clause (h) of section (2) of the Payment of Gratuity Act, 1972 with effect from the ...................... [date here] in the manner indicated below and therefore nominate afresh the person(s) mentioned below to receive the gratuity payable after my death as also the gratuity standing to my credit in the event of my death before that amount has become payable, or having become payable has not been paid direct that the said amount of gratuity shall be paid in proportion indicated against the name(s) of the nominee(s).
2. I hereby certify the person(s) nominated is a/are member(s) of my family within the meaning of clause (h) of section 2 of the said Act.
3. a. My father/mother/parents is/are not dependant on me. b. My husband’s father/mother/parents is/are not dependant on my husband.
4. I have excluded my husband from my family by a notice dated the ..................... to the controlling authority in
terms of the proviso to clause (h) of section 2 of the said Act.
Nominee(s)
Name in full with full address of nominee(s)
Relationship with the employee
Age of nominee
Proportion by which the gratuity will be shared
1. 2. 3. 4. so on.
Manner of acquiring a “family”
[Here give details as to how a family was acquired, i.e., whether by marriage or parents being rendered dependant or through other process like adoption].
Statement 1. Name of the employee in full. 2. Sex. 3. Religion. 4. Whether unmarried/married/widow/widower. 5. Department/Branch/Section where employed.
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 1
6. Post held with Ticket No. or Serial No., if any. 7. Date of appointment. 8. Permanent address. Village .................. Thana .................. Sub‐division .................. Post Office .................. District .................. State .................. Place............................ Signature/Thumb impression Date............................. of the employee.
Declaration by witnesses Fresh nomination signed/thumb impressed before me. Name in full and full Signature of witnesses. addresses of witnesses. 1. 1. 2. 2.
Place............................. Date.............................
Certificate by the employer
Certified that the particulars of the above nomination have been verified and recorded in this establishment.
Employer’s reference No., if any. Signature of the employer/ officer authorised Designation
Date............................. Name and address of the establishment or rubber stamp thereof.
Acknowledgement by the employee
Received the duplicate copy of the nomination in Form .................. filed by me on.................. duly certified by the employer.
Date............................. Signature of the employer
Note : strike out the words not applicable
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 2
FORM‐H [See Sub‐Rule (4) of Rule 6]
Modification of Nomination To [Give here name or description of the establishment with full address]
I, Shri/Shrimati/Kumari .........................................................................................
[Name in full here]
whose particulars are given in the statement below, hereby give notice that the nomination filed by me on …………..[date] and recorded under your reference No. .......... dated .................. shall stand modified in the following manner:
[Here give details of the modifications intended]
Statement 1. Name of the employee in full. 2. Sex. 3. Religion. 4. Whether unmarried/married/widow/widower. 5. Department/Branch/Section where employed. 6. Post held with Ticket No. or Serial No., if any. 7. Date of appointment. 8. Address in full.
Place............................. Signature/Thumb impression Date............................. of the employee.
Declaration by witnesses Modification of nomination signed/thumb impressed before me. Name in full and full Signature of witnesses. address of witnesses. 1. 1. 2. 2. Place............................. Date.............................
Certificate by the employer Certified that the above modification have been recorded. Employer’s reference No., if any.
Signature of the employer/officer authorised Designation

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 3
Name and address of the establishment or rubber stamp thereof.
Acknowledgement by the employee Received the duplicate copy of the notice for modification in Form ‘H’ filed by me on ................. duly certified by
the employer. Date............................. Signature of the employee
Note: Strike out the words not applicable.
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 4
FORM ‐I [See Sub‐Rule (1) of Rule 7]
Application of Gratuity by an Employee To
[Give here name or description of the establishment with full address] Sir/Gentlemen,
I beg to apply for payment of gratuity to which I am entitled under sub‐section (1) of section 4 of the Payment of Gratuity Act, 1972 on account of my superannuation/retirement/resignation after completion of not less than five years of continuous service/ total disablement due to accident/total disablement due to disease with effect from the .................. Necessary particulars relating to my appointment in the establishment are given in the statement below:
Statement 1. Name in full. 2. Address in full. 3. Department/Branch/Section where last employed. 4. Post held with Ticket No. or Serial No., if any. 5. Date of appointment. 6. Date and cause of termination of service. 7. Total period of service. 8. Amount of wages last drawn. 9. Amount of gratuity claimed. I was rendered totally disabled as a result of
[Here give the details of the nature of disease or accident] The evidences/witnesses in support of my total disablement are as follows:
[Here give details] Payment may please be made in cash/open or crossed bank cheque.
As the amount of gratuity payable is less than rupees one thousand, I shall request you to arrange for payment of the sum due to me by Postal Money Order at the address mentioned above after deducting postal money order commission there from.
Yours faithfully,
Signature/Thumb impression of the applicant employee.
Place............................ Date.............................
Note.—1. Strike out the words not applicable. 2. Strike out paragraph or paragraphs not applicable.
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 5
FORM ‐J [See Sub‐Rule (2) of Rule 7]
Application for Gratuity by a Nominee To
[Give here the name or description of the establishment with full address] Sir/Gentlemen,
I beg to apply for payment of gratuity to which I am entitled under sub‐section (1) of section 4 of the Payment of Gratuity Act, 1972 as a nominee of late.....................................................................................
[name of the employee]
who was an employee of your …………….establishment and died on the .................. The gratuity is payable on account of the death of the aforesaid employee while in service/superannuation of the aforesaid employee on .................. retirement of/resignation of the aforesaid employee on .................. after completion of .................. years of service/total disablement of the aforesaid employee due to accident or disease while in service with effect from the .................. Necessary particulars relating to my claim given in the statement below:
Statement 1. Name of applicant nominee. 2. Address in full of the applicant nominee. 3. Marital status of the applicant nominee
(unmarried/married/widow/widower) 4. Name in full of the employee. 5. Marital status of employee. 6. Relationship of the nominee with employee. 7. Total period of service of the employee. 8. Date of appointment of the employee. 9. Date and cause of termination of service of the employee. 10. Department/Branch/Section where the employee last worked. 11. Post last held by the employee with Ticket or Serial No., if any. 12. Total wages last drawn by the employee. 13. Date of death and evidence/witness as proof of death of the employee. 14. Reference No. of recorded nomination, if available. 15. Total gratuity payable to the employee. 16. Share of gratuity claimed.
2. I declare that the particulars mentioned in the above statement are true and correct to the best of my knowledge and belief.
3. Payment may please be made in cash/crossed or open bank cheque. 4. As the amount payable is less than rupees one thousand, I shall request you to arrange for payment of the sum
due to me by Postal Money Order at the address mentioned above after deducting Postal Money Order commission there from.
Yours faithfully,
Signature/Thumb impression of the applicant employee.
Place............................

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 6
Date.............................
Note.—1. Strike out the words not applicable.
FORM ‐ K [See Sub‐Rule (3) of Rule 7]
Application for Gratuity by a Legal Heir To [Give here the name or description of the establishment with full address] Sir/Gentlemen, I beg to apply for payment of gratuity to which I am entitled under sub‐section (1) of section 4 of the Payment of
Gratuity Act, 1972 as a legal heir of late .......................................................................................................
[name of the employee]
who was an employee of your …………………….establishment and died on the ....... without making any nomination. The gratuity is payable on account of the death of the aforesaid employee while in service/ superannuation of the aforesaid employee on the .................. retirement or resignation of the aforesaid employee on the .................. after completion of .................. years of service/total disablement of the aforesaid employee due to accident or disease while in service with effect from the .................. Necessary particulars relating to my claim are given in the statement below:
Statement 1. Name of applicant legal heir. 2. Address in full of applicant legal heir. 3. Marital status of the applicant legal heir (unmarried/married/widow/widower) 4. Name in full of the employee. 5. Relationship of the applicant with the employee. 6. Religion of both the applicant and the employee. 7. Date of appointment and total period of service of the employee. 8. Department/Branch/Section where the employee worked last. 9. Post last held by the employee with Ticket or Serial No., if any. 10. Total wages last drawn by the employee. 11. Date and cause of termination of service of the employee (death or otherwise). 12. Date of death of the employee and evidence/witness in support thereof. 13. Total gratuity payable to the employee. 14. Percentage of the gratuity claimed. 15. Basis of the claim and evidence/witness in support thereof.
2. I declare that the particulars mentioned in the above statement are true and correct to the best of my knowledge and belief.
3. Payment may please be made in cash/open or crossed bank cheque. 4. As the amount payable is less than rupees one thousand, I shall request you to arrange for payment of the sum
due to me by Postal Money Order at the address mentioned above, after deducting Postal Money Order commission there from.
Yours faithfully, Signature/Thumb impression of applicant legal heir.
Place............................
Date.............................
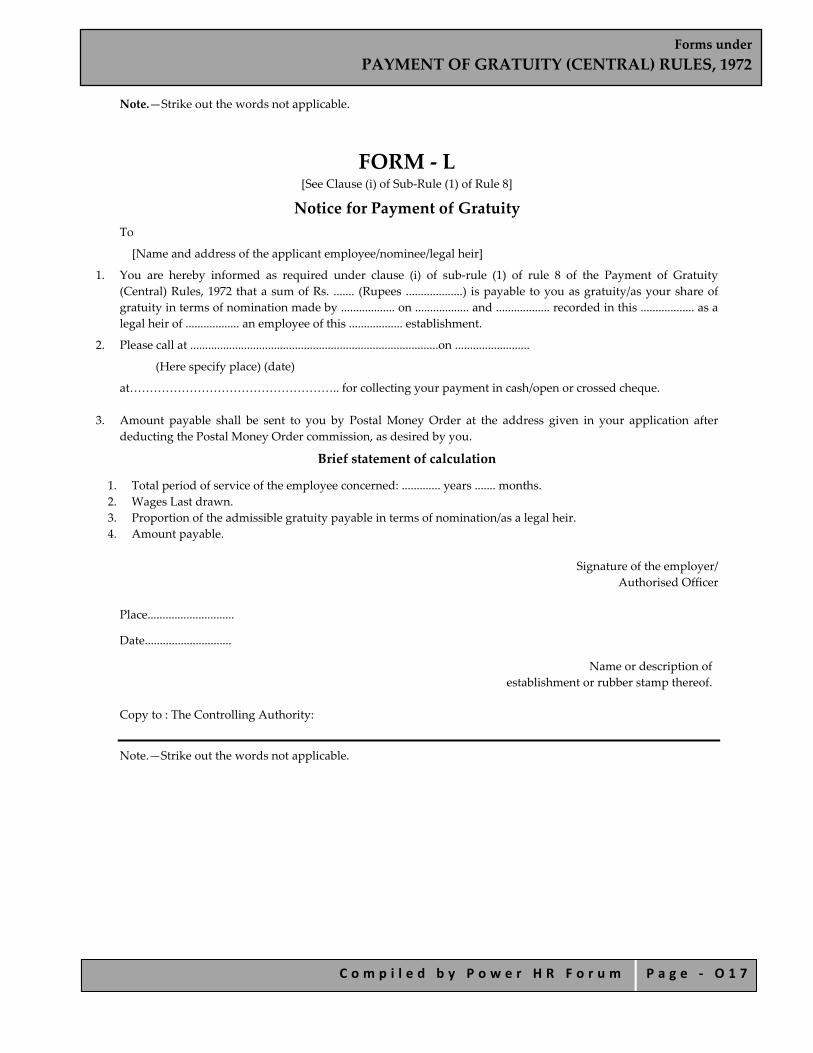
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 7
Note.—Strike out the words not applicable.
FORM ‐ L [See Clause (i) of Sub‐Rule (1) of Rule 8]
Notice for Payment of Gratuity To
[Name and address of the applicant employee/nominee/legal heir]
1. You are hereby informed as required under clause (i) of sub‐rule (1) of rule 8 of the Payment of Gratuity (Central) Rules, 1972 that a sum of Rs. ....... (Rupees ...................) is payable to you as gratuity/as your share of gratuity in terms of nomination made by .................. on .................. and .................. recorded in this .................. as a legal heir of .................. an employee of this .................. establishment.
2. Please call at ...................................................................................on .........................
(Here specify place) (date)
at…………………………………………….. for collecting your payment in cash/open or crossed cheque.
3. Amount payable shall be sent to you by Postal Money Order at the address given in your application after deducting the Postal Money Order commission, as desired by you.
Brief statement of calculation
1. Total period of service of the employee concerned: ............. years ....... months. 2. Wages Last drawn. 3. Proportion of the admissible gratuity payable in terms of nomination/as a legal heir. 4. Amount payable.
Signature of the employer/
Authorised Officer
Place.............................
Date.............................
Name or description of establishment or rubber stamp thereof.
Copy to : The Controlling Authority:
Note.—Strike out the words not applicable.

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 8
FORM ‐ M [See Clause (ii) of Sub‐Rule (1) of Rule 8]
Notice Rejecting Claim for Payment of Gratuity To
[Name and address of the applicant employee/nominee/legal heir] You are hereby informed as required under Clause (ii) of Sub‐Rule (i) of Rule 8 of the Payment of Gratuity
(Central) Rules, 1972 that your claim for payment of gratuity as indicated on your application in Form ........ under the said rules is not admissible for the reasons stated below:
Reasons [Here specify the reasons]
Signature of the employer/ Authorised Officer.
Place............................ Date.............................
Name or description of establishment or rubber stamp thereof.
Copy to : The Controlling Authority.
Note: Strike out the words not applicable.

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 1 9
FORM ‐N [See Sub‐Rule (i) of Rule 10]
Application for Direction
Before the controlling authority under the Payment of Gratuity Act, 1972.
Application No…………………………. Date……………………………………….
BETWEEN
[Name in full of the applicant with full address]
AND
[Name in full of the employer concerned with full address]
1. The applicant is an employee of the above‐mentioned employer/a nominee of late ..................... an employee of the above mentioned employer/a legal heir of late ..................... an employee of the above‐mentioned employer, and is entitled to payment of gratuity under section 4 of the Payment of Gratuity Act, 1972, on account of his own/ aforesaid employee’s superannuation on ............................... [date] /his own retirement/aforesaid employee’s resignation on .......................... [date] after completion of ..................... years of continuous service/his own/aforesaid employee’s total disablement with effect from .............[date] due to accident/disease/death of the aforesaid employee on .....................
2. The applicant submitted an application under Rule ..................... of the Payment ofGratuity Act, 1972 on the ..................... but the above‐mentioned employer refused to entertain it/issued a notice dated the ..................... under clause .......of sub‐rule of rule ................ offering an amount of gratuity which is less than my due/issued a notice dated the..................... under Clause .................... of Sub‐Rule ........ of Rule ........ rejecting my eligibility to payment of gratuity. The duplicate copy of the said notice is enclosed.
3. The applicant submits that there is a dispute on the matter. [Specify the dispute]
4. The applicant furnishes the necessary particulars in the annexure hereto and prays that the Controlling Authority may be pleased to determine the amount of gratuity payable to the petitioner and direct the above mentioned employer to pay the same to the petitioner.
5. The applicant declares that the particulars furnished in the annexure hereto are true and correct to the best of his knowledge and belief.
Date Signature of the applicant/
Thumb impression of the applicant.
ANNEXURE
1. Name in full of applicant with full address. 2. Basis of claim : [Death/Superannuation/Retirement/Resignation/
Disablement of employee]. 3. Name and address in full of the employee. 4. Marital status of the employee
(unmarried/married/widow/widower) 5. Name and address in full of the employer. 6. Department/Branch/Section where the employee was employed [if known]. 7. Post held by the employee with Ticket or Serial No., if any [if known].

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2 0
8. Date of appointment of the employee [if known]. 9. Date and cause of termination of service of the employee. [superannuation/
retirement/resignation/disablement/death] 10. Total period of service by the employee. 11. Wages last drawn by the employee. 12. If the employee is dead, date and cause thereof. 13. Evidence/witness in support of death of the employee. 14. If a nominee, No. and date of recording of nomination with the employer. 15. Evidence/witness in support of being a legal heir, if a legal heir. 16. Total gratuity payable to the employee [if known]. 17. Percentage of gratuity payable to the applicant as a nominee/legal heir. 18. Amount of gratuity claimed by the applicant.
Place............................ Signature/Thumb impression of the applicant.
Date.............................
Note: Strike out the words not applicable.
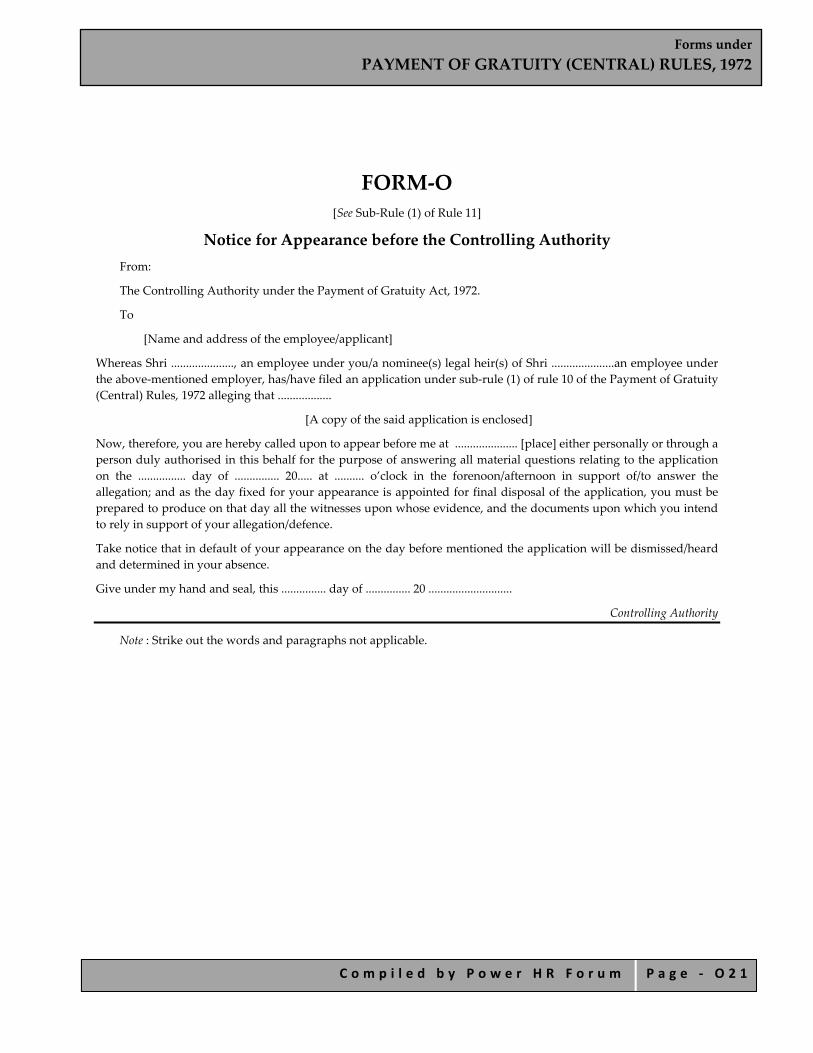
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2 1
FORM‐O [See Sub‐Rule (1) of Rule 11]
Notice for Appearance before the Controlling Authority From: The Controlling Authority under the Payment of Gratuity Act, 1972. To [Name and address of the employee/applicant]
Whereas Shri ....................., an employee under you/a nominee(s) legal heir(s) of Shri .....................an employee under the above‐mentioned employer, has/have filed an application under sub‐rule (1) of rule 10 of the Payment of Gratuity (Central) Rules, 1972 alleging that ..................
[A copy of the said application is enclosed] Now, therefore, you are hereby called upon to appear before me at ..................... [place] either personally or through a person duly authorised in this behalf for the purpose of answering all material questions relating to the application on the ................ day of ............... 20..... at .......... o’clock in the forenoon/afternoon in support of/to answer the allegation; and as the day fixed for your appearance is appointed for final disposal of the application, you must be prepared to produce on that day all the witnesses upon whose evidence, and the documents upon which you intend to rely in support of your allegation/defence. Take notice that in default of your appearance on the day before mentioned the application will be dismissed/heard and determined in your absence. Give under my hand and seal, this ............... day of ............... 20 ............................
Controlling Authority
Note : Strike out the words and paragraphs not applicable.
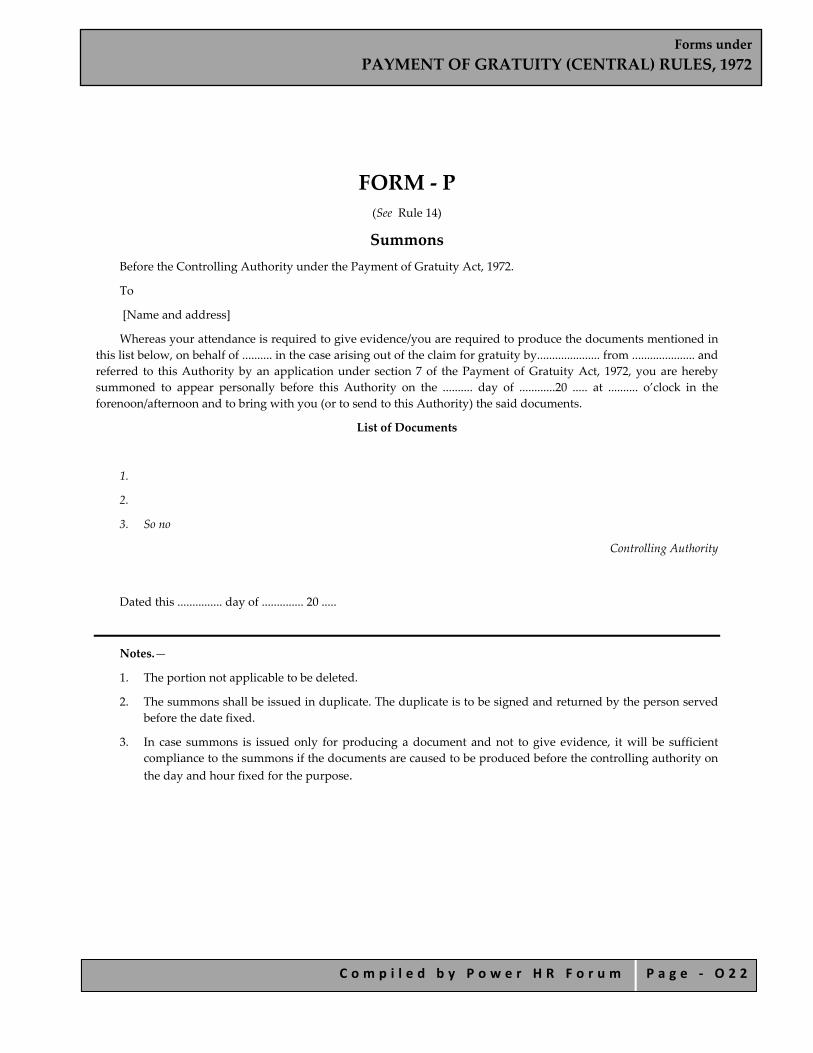
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2 2
FORM ‐ P (See Rule 14)
Summons Before the Controlling Authority under the Payment of Gratuity Act, 1972. To [Name and address] Whereas your attendance is required to give evidence/you are required to produce the documents mentioned in
this list below, on behalf of .......... in the case arising out of the claim for gratuity by..................... from ..................... and referred to this Authority by an application under section 7 of the Payment of Gratuity Act, 1972, you are hereby summoned to appear personally before this Authority on the .......... day of ............20 ..... at .......... o’clock in the forenoon/afternoon and to bring with you (or to send to this Authority) the said documents.
List of Documents
1.
2.
3. So no
Controlling Authority
Dated this ............... day of .............. 20 .....
Notes.—
1. The portion not applicable to be deleted. 2. The summons shall be issued in duplicate. The duplicate is to be signed and returned by the person served
before the date fixed. 3. In case summons is issued only for producing a document and not to give evidence, it will be sufficient
compliance to the summons if the documents are caused to be produced before the controlling authority on the day and hour fixed for the purpose.

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2 3
FORM ‐ Q [See Sub‐Rule (1) of Rule 19]
Particulars of Application under Section 7 1. Serial No. 2. Date of the Application. 3. Name and address of the applicant. 4. Name and address of the employer. 5. Amount of gratuity claimed. 6. Dates of hearing. 7. Findings with date. 8. Amount awarded. 9. Cost, if any, awarded. 10. Date of notice issued for payment of gratuity. 11. Date of appeal, if any. 12. Decision of the appellate authority. 13. Date of issue of Final Notice for payment of gratuity. 14. Date of payment of gratuity by Employer with mode of payment. 15. Date of Receipt of application for recovery of Gratuity. 16. Date of Issue of Recovery Certificate. 17. Date of Recovery. 18. Other remarks. 19. Signed. 20. Date.
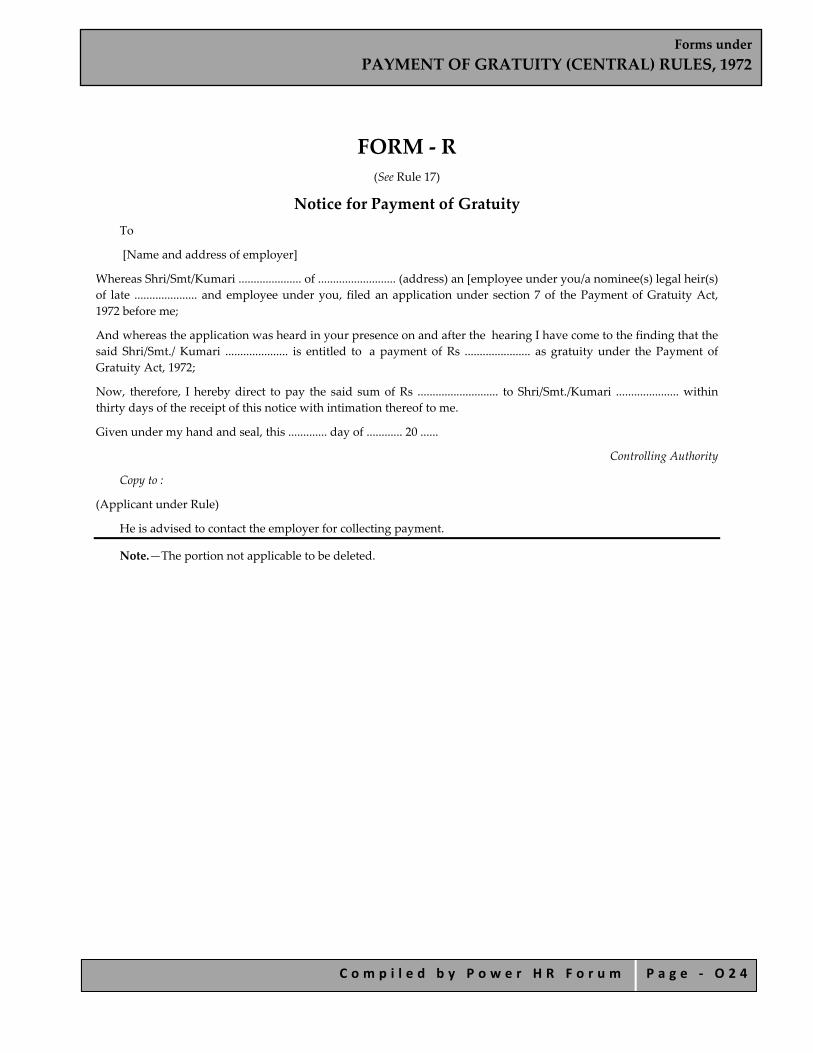
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2 4
FORM ‐ R (See Rule 17)
Notice for Payment of Gratuity To
[Name and address of employer] Whereas Shri/Smt/Kumari ..................... of .......................... (address) an [employee under you/a nominee(s) legal heir(s) of late ..................... and employee under you, filed an application under section 7 of the Payment of Gratuity Act, 1972 before me; And whereas the application was heard in your presence on and after the hearing I have come to the finding that the said Shri/Smt./ Kumari ..................... is entitled to a payment of Rs ...................... as gratuity under the Payment of Gratuity Act, 1972; Now, therefore, I hereby direct to pay the said sum of Rs ........................... to Shri/Smt./Kumari ..................... within thirty days of the receipt of this notice with intimation thereof to me. Given under my hand and seal, this ............. day of ............ 20 ......
Controlling Authority Copy to :
(Applicant under Rule) He is advised to contact the employer for collecting payment.
Note.—The portion not applicable to be deleted.
Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2 5
FORM ‐S [See Sub‐Rule (5) of Rule 18]
Notice for Payment of Gratuity as Determined by Appellate Authority
To [Name and address of employer]
Whereas a notice was given to you on ...................... Form ‘R’ requiring you to make a payment of Rs ................. to Shri/Smt./Kumari .................... as gratuity under the Payment of Gratuity Act, 1972; Whereas you/the applicant went in appeal before the appellate authority, who has decided that an amount of Rs ................ is due to be paid to Shri/Smt./Kumari ..................... as gratuity due under the Payment of Gratuity Act, 1972; Now, therefore, I hereby direct you to pay the said sum of Rs ............... to Shri/Smt./Kumari ..................... within 30 days of the receipt of this notice with an intimation thereof to me. Given under my hand and seal, this ........... day of ........... 20.....
Controlling Authority. Copy to:
1. The Applicant. He is advised to contact the employer for collecting payment.
2. The Appellate Authority.
Note.— The portion not applicable to be deleted.

Forms under PAYMENT OF GRATUITY (CENTRAL) RULES, 1972
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ O 2 6
FORM ‐T (See Rule 19)
Application for Recovery of Gratuity Before the Controlling Authority under the Payment of Gratuity Act, 1972. Application No............... Date .......................
BETWEEN
[Name in full of the applicant with address] AND
[Name in full of the employer with full address] 1. The applicant is an employee of the above‐mentioned employer/a nominee of late................. an employee of the
above mentioned employer/a legal heir of late............., an employee of the above mentioned employer, and you were pleased to direct the said employer in your notice dated the ................. under Rule ................ of the Payment of Gratuity (Central) Rules, 1972 for payment of a sum of Rs ............. as gratuity payable under the Payment of Gratuity Act, 1972.
2. The applicant submits that the said employer failed to pay the said amount of gratuity to me as directed by you although I approached him for payment.
3. The applicant therefore prays that a certificate may be issued under section ............. of the said Act for the recovery of the said sum of Rs.................. due to me as gratuity in terms of your direction.
Signature/Thumb impression of the applicant
Place............................
Date.............................
Note : Strike out the words and paragraphs not applicable.

Forms under PAYMENT OF BONUS RULES,1975
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ P 1
Forms under
PAYMENT OF BONUS RULES,1975

Forms under PAYMENT OF BONUS RULES,1975
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ P 2
INDEX FORM A
Computation of the Allocable Surplus under Section 2(4)
FORM B
Set‐on and Set‐off of Allocable Surplus under Section 15
FORM C Bonus Paid to Employees for the Accounting Year
FORM D
Annual Return—Bonus Paid to Employees for The Accounting Year

Forms under PAYMENT OF BONUS RULES,1975
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ P 3
FORM A [See Rule 4(1)]
Computation of the Allocable Surplus under Section 2(4)
Name of the establishment................................... Accounting year ending on the................................................
Sums deducted from gross profit Direct taxes section 6(c)
Further sums as are specified under the Third Schedule to the Act Gross profit for the
Accounting year Rs.
Depreciation under section 6(a)
Development rebate or Development allowance
section 6(b)
1 2 3 4 5
Total of sums deducted under
Column 2,3,4, and 5 Available surplus for the accounting year
(Column 1 minus Column 6) Amount of allocable surplus
† 67% (*60% of Column 7)
6 7 8
† Section 2 (4)(a) * Section 2 (4) (b)

Forms under PAYMENT OF BONUS RULES,1975
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ P 4
FORM B [See Rule 4(b)]
Set‐on and Set‐off of Allocable Surplus under Section 15
Accounting year Amount allocable as bonus (in Rs.)
Amount payable as bonus (in Rs.)
Amount of set‐on or set‐off (in Rs.)
Total set‐on or set‐off carried forward
(in Rs.)
1 2 3 4 5

Forms under PAYMENT OF BONUS RULES,1975
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ P 5
FORM C [See Rule 4(c)]
Bonus Paid to Employees for the Accounting Year Ending on the...................... Name of the establishment...........................................
No. of working days in the year................................
Sl. No.
Name of the
employee
Father’s name
Whether he has completed 15 years
of age at the beginning of the accounting year
Designation No. of days worked in the year
Total salary or wage in respect of the accounting
year
Amount of bonus payable under section 10 or section 11 as the case may be
1 2 3 4 5 6 7 8
Deductions Total sum deducted under Columns, 9 10,10A and 11
Net amount payable (Column 8 minus Column 12)
Amount actually paid
Date on which paid
Signature/ Thumb impression of the employee
Puja bonus or other customary bonus during the accounting year
Interim bonus or bonus paid advance
Amount of Income‐tax deducted
Deduction on account of financial loss, if any, caused by misconduct of the employee
9 10 1[10A] 11 12 13 14 15 16

Forms under PAYMENT OF BONUS RULES,1975
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ P 6
FORM D [See Rule 5]
Annual Return—Bonus Paid to Employees for the Accounting Year Ending on the......................
1. Name of the establishment and its complete postal address: 2. Name of industry: 3. Name of the employer: 4. Total number of employees: 5. Number of employees benefited by bonus payments:
Total amount payable as bonus under section 10 or 11 of the Payment of Bonus Act, 1965 as the case may be
Settlement, if any, reached under section 18(1) of 12(3)
of the Industrial Disputes Act, 1947 with date
Percentage of bonus declared to be paid
(1) (2) (3)
Total amount of bonus actually paid
Date on which payment made
Whether bonus has been paid to all the employees, if not, reasons for non‐payment
Remark
(4) (5) (6) (7)
Signature of the employer of his agent
Forms under EQUAL REMUNERATION RULES, 1976
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ Q 1
Forms under the
EQUAL REMUNERATION RULES, 1976

Forms under EQUAL REMUNERATION RULES, 1976
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ Q 2
INDEX
Form A Complaint under Clause (a) of Sub Section (I) of Section 7 of the Equal
Remuneration Act ,1976 ( 25 of 1976)
Form B Claim under Clause (b) of Section (I) of Section 7 of the Equal Remuneration Act, 1976 (25 of 1976)
Form C Form of Authority in Favor of Legal Practitioner or any Official of a Registered Trade Union
Form D Register to be Maintained by the Employer under Rule (6) of the Equal Remuneration Rules, 1976
Forms under EQUAL REMUNERATION RULES, 1976
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ Q 3
FORM A (To be submitted in Triplicate)
[See Rule 3(1)] Complaint under Clause (a) of Sub Section (I) of Section
7 of the Equal Remuneration Act ,1976 ( 25 of 1976) To The Authority appointed under sub‐section I of section 7 …………………………………………………………………………………. (Address) A…………………………………………………………………Complainant(s)
Full address Versus
B. ……………………………………………………………………Opposite Party
Full address The complainant(s) begs/beg to complain that the opposite party has been guilty of contraventions of the provisions of Equal Remuneration Act, 1976 (25 of 1976) as show below: ‐ (Here set out briefly the particulars showing the manner in which the alleged contravention(s) has/have taken place and the grounds supporting the complaint.) The complainant(s) accordingly prays/ pray that the Authority ___________________________may be pleased to decide the complaint set out above and pass such order or orders thereon as it may deem fit and proper. The number of copies of the complaint (along with annexure) as required under sub‐rule (I) of Rule 3 of the Equal Remuneration Rules, 1976 are submitted herewith. The complainant(s) does/ do solemnly declare that the facts stated in this complaint are true to the best of his/her/their knowledge, belief and information. Signature(s)/ Thumb impressions of the complainant(s). * I have been duly authorized in writing by ____________________ [ here insert the name of the worker(s), to appear and act on his/her/their behalf.
Signature of the legal practitioner / official of a registered Trade Union duly authorized
Station Date * Strike out this portion if applicable
Forms under EQUAL REMUNERATION RULES, 1976
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ Q 4
FORM B (To be submitted in Triplicate)
[See Rule 4(1)] Claim under Clause (b) of Section (I) of Section 7 of the Equal Remuneration Act, 1976 (25 of 1976)
To The Authority appointed under sub‐section I of section 7 …………………………………………………………………………………. (Address) A…………………………………………………………………Petitioner(s)
Full address Versus
B. ……………………………………………………………………Opposite Party Full address
The petitioner(s) above named states/ state as follows:‐
1) The petitioner was/were/ is/ are employed from ______________ to______________ as ___________________ (category) in_____________________ (name of the establishment) of Shri / Messrs__________________ ( name of the employer and address).
2) The opposite party is the employer within the meaning of clause (c) of Section 2 of the Equal Remuneration Act, 1976 ( 25 of 1976).
3) The petitioner(s) was/were/has/have not been paid wages at rates equal to those of workers of the opposite sex for the same work or work of a similar nature for the period from___________________ to____________________
4) The petitioner(s) was/were/has/have been paid wages at the rate of ______________ weheras workers of the opposite sex for the same work or work of a similar nature were paid/ have been paid at the rate of ____________________ during the said period.
5) The petitioner(s) estimates/ estimate the value of relief sought by him/them at Rs________________ [ Rupees________________________________( in words)
6) The petitioner(s), therefore, prays/pray that the Authority may be pleased to decide the claim set out above and pass such order or orders thereon as it may deem fit and proper.
7) The petitioner(s) begs/beg leave to amend or add to or make alternations in the petition, if and when necessary, with permission of Authority.
The petitioner(s) does/do solemnly declare that the facts stated in this petition are true to the best of his/her/their knowledge, belief and information.
Signature / thumb impression(s) of the petitioner(s)
Forms under EQUAL REMUNERATION RULES, 1976
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ Q 5
* I have been duly authorized in writing by ________________________ [ here insert the name of worker(s) ] to appear and act on his/her/their behalf.
Signature of the legal practitioner / official of a registered Trade Union duly authorized
Station Date * Strike out this portion if inapplicable

Forms under EQUAL REMUNERATION RULES, 1976
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ Q 6
FORM C [See Rule 5]
Form of Authority in favor of Legal Practitioner or any
Official of a Registered Trade Union I/we hereby authorize Shri/ Shrimati/ Kumari* ___________________ a legal practitioner/ an official of___________________________which is a registered Trade Union to appear and act on my/our behalf, under * sub‐rule (3) of Rule 3/ sub rule (3) of Rule 4 in respect of the * complaint / claim against________________________ ( mention name of employer) on account of _____________________ ( mention violation of the Act).
Signature / thumb impression(s) of the worker(s)
Station Date Witness (1)……… (2)……… (3)………. I accept the authorization.
* Legal Practitioner/ Official of a registered Trade Union
Station Date * Strike out this portion if inapplicable
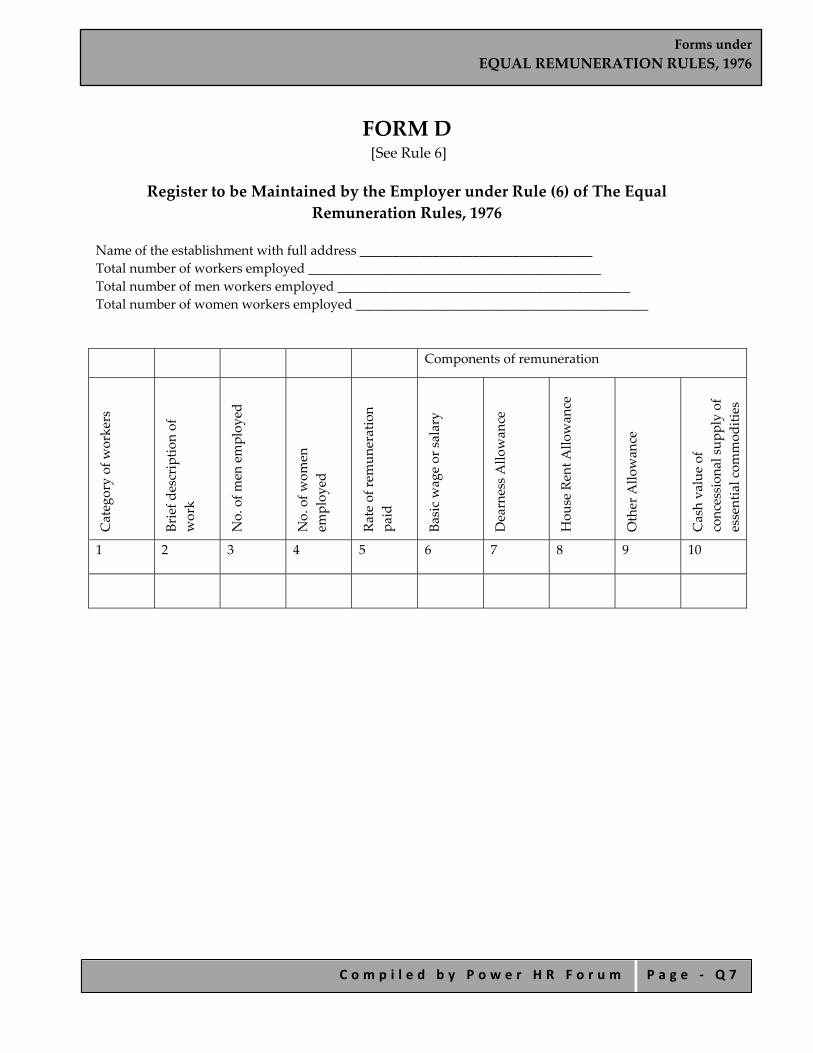
Forms under EQUAL REMUNERATION RULES, 1976
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ Q 7
FORM D [See Rule 6]
Register to be Maintained by the Employer under Rule (6) of The Equal
Remuneration Rules, 1976 Name of the establishment with full address ___________________________________ Total number of workers employed ____________________________________________ Total number of men workers employed ____________________________________________ Total number of women workers employed ____________________________________________
Components of remuneration
Category of w
orkers
Brief d
escriptio
n of
work
No. of m
en employ
ed
No. of w
omen
employ
ed
Rate of rem
uneration
paid
Basic wage or salary
Dearness A
llowan
ce
Hou
se Rent A
llowan
ce
Other Allo
wan
ce
Cash value of
concession
al su
pply of
essential com
mod
ities
1 2 3 4 5 6 7 8 9 10

Forms under EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
C o m p i l e d b y P o w e r H R F o r u m P a g e - R 1
Forms under
EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
Forms under EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
C o m p i l e d b y P o w e r H R F o r u m P a g e - R 2
INDEX FORM AND MANNER OF NOTIFICATION OF VACANCIES
Requisition Form to be Used When Calling for Applicants from Employment Exchanges.
FORM ER‐I Quarterly Return to be Submitted to the Local Employment Exchange
FORM ER‐II
Occupational Return to be Submitted to the Local Employment Exchanges Once in Two Years
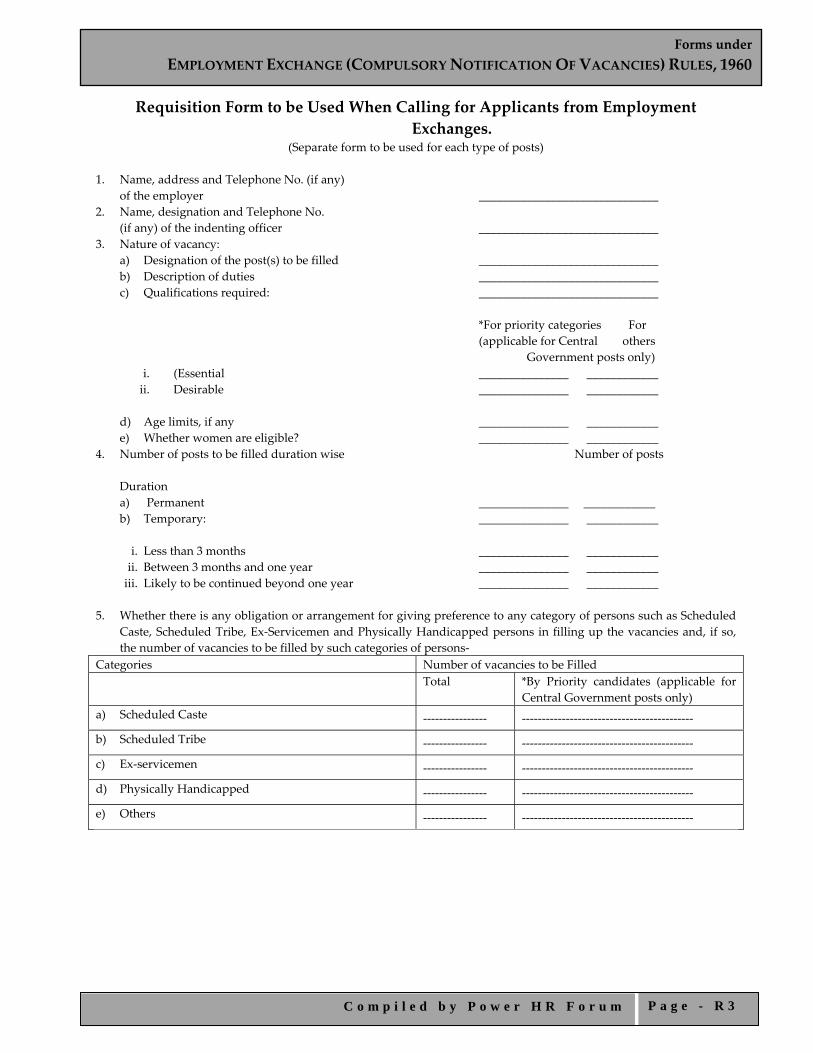
Forms under EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
C o m p i l e d b y P o w e r H R F o r u m P a g e - R 3
Requisition Form to be Used When Calling for Applicants from Employment Exchanges.
(Separate form to be used for each type of posts) 1. Name, address and Telephone No. (if any)
of the employer ______________________________ 2. Name, designation and Telephone No. (if any) of the indenting officer ______________________________ 3. Nature of vacancy:
a) Designation of the post(s) to be filled ______________________________ b) Description of duties ______________________________ c) Qualifications required: ______________________________
*For priority categories For (applicable for Central others
Government posts only) i. (Essential _______________ ____________ ii. Desirable _______________ ____________
d) Age limits, if any _______________ ____________ e) Whether women are eligible? _______________ ____________
4. Number of posts to be filled duration wise Number of posts Duration
a) Permanent _______________ ____________ b) Temporary: _______________ ____________
i. Less than 3 months _______________ ____________ ii. Between 3 months and one year _______________ ____________ iii. Likely to be continued beyond one year _______________ ____________
5. Whether there is any obligation or arrangement for giving preference to any category of persons such as Scheduled
Caste, Scheduled Tribe, Ex‐Servicemen and Physically Handicapped persons in filling up the vacancies and, if so, the number of vacancies to be filled by such categories of persons‐
Categories Number of vacancies to be Filled Total *By Priority candidates (applicable for
Central Government posts only) a) Scheduled Caste ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
b) Scheduled Tribe ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
c) Ex‐servicemen ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
d) Physically Handicapped ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
e) Others ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐

Forms under EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
C o m p i l e d b y P o w e r H R F o r u m P a g e - R 4
6. Pay and allowances _______________ ____________ 7. Place of work (Name of the town/
village and district in which it is situated) _______________ ____________ 8. Probable date by which the vacancy will be filled _______________ ____________ 9. Particulars regarding interview/test of applicants:
a) Date of interview/test: _______________ ____________ b) Time of interview/test: _______________ ____________ c) Place of interview/test: _______________ ____________ d) Name, designation, address and telephone
number, (if any) of the Officer to whom applicants should report _______________ ____________ 10. Any other relevant information _______________ ____________ *Certified that while placing this demand, the instructions connected with the orders on communal representation
in the services have been strictly followed with due regard to the roster maintained in accordance with these orders (to be given only by all the Central Government Offices/Establishments/Undertakings etc. on whom reservation orders are applicable).
Signature of the Head of Office:
Date:— *Delete if not applicable];
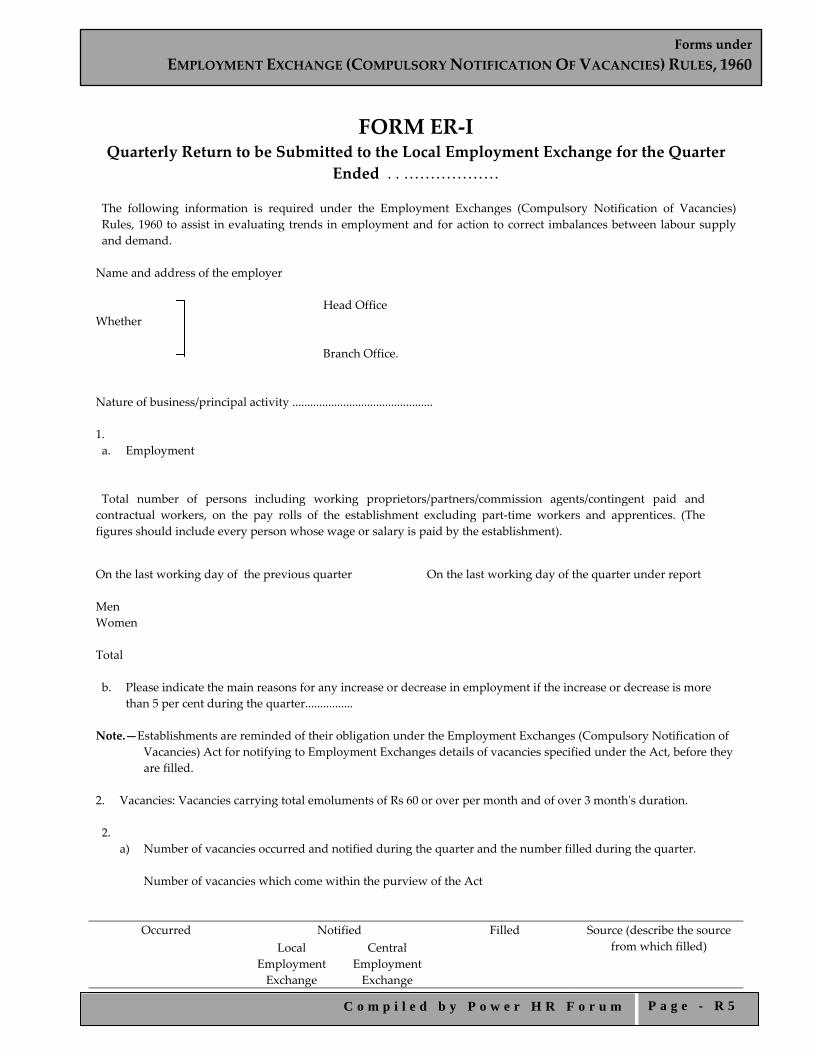
Forms under EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
C o m p i l e d b y P o w e r H R F o r u m P a g e - R 5
FORM ER‐I Quarterly Return to be Submitted to the Local Employment Exchange for the Quarter
Ended . . ……………… The following information is required under the Employment Exchanges (Compulsory Notification of Vacancies) Rules, 1960 to assist in evaluating trends in employment and for action to correct imbalances between labour supply and demand. Name and address of the employer Head Office Whether Branch Office. Nature of business/principal activity ............................................... 1. a. Employment Total number of persons including working proprietors/partners/commission agents/contingent paid and contractual workers, on the pay rolls of the establishment excluding part‐time workers and apprentices. (The figures should include every person whose wage or salary is paid by the establishment).
On the last working day of the previous quarter On the last working day of the quarter under report
Men Women
Total b. Please indicate the main reasons for any increase or decrease in employment if the increase or decrease is more
than 5 per cent during the quarter................ Note.—Establishments are reminded of their obligation under the Employment Exchanges (Compulsory Notification of
Vacancies) Act for notifying to Employment Exchanges details of vacancies specified under the Act, before they are filled.
2. Vacancies: Vacancies carrying total emoluments of Rs 60 or over per month and of over 3 monthʹs duration. 2.
a) Number of vacancies occurred and notified during the quarter and the number filled during the quarter. Number of vacancies which come within the purview of the Act
Occurred Notified Filled Source (describe the source from which filled) Local
Employment Exchange
Central Employment Exchange

Forms under EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
C o m p i l e d b y P o w e r H R F o r u m P a g e - R 6
(1) (2) (3) (4) (5)
b) Reasons for not notifying all vacancies occurred during the quarter under report vide 2(a) above. 3. Manpower shortages
Vacancies/posts unfilled because of shortage of suitable applicants. Name of the occupation or designation of the posts
Number of unfilled vacancies/posts
essential qualifications prescribed
Essential experience
experience not necessary
(1) (2) (3) (4)
Please list any other occupations for which this establishment had recently any difficulty in obtaining suitable applicants.
Signature of employer Employment Exchange, ……………………………….. ……………………………….. Note.—This return shall relate to quarters ending 31st March/30th June/30th September and 31st December and shall be
rendered to the local Employment Exchange within 30 days after the end of the quarter concerned.

Forms under EMPLOYMENT EXCHANGE (COMPULSORY NOTIFICATION OF VACANCIES) RULES, 1960
C o m p i l e d b y P o w e r H R F o r u m P a g e - R 7
FORM ER‐II
Occupational Return to be Submitted to the Local Employment Exchanges Once in Two Years (On a Date to be Specified by Notification in the Official Gazette)
[Vide the Employment Exchanges (Compulsory Notification of Vacancies) Rules, 1960]
Name and address of the employer. Nature of business. (Please describe what the establishment makes or does as its principal activity) 1. Total number of persons on the pay rolls of the establishment on (specified date). ......... (This figure should include every person whose wage or salary is paid by the establishment.) 2. Occupational classification of all employees as given in Item 1 above. (Please give below the number of employees
in each occupation separately.)
Occupation Number of employees (1) (2) (3) (4) (5)
Use exact terms such as engineer (Mechanical); teacher (domestic/science); officer on special duty (actuary); assistant director (metallurgist); scientific assistant (chemist); research officer (economist); instructor (carpenter); supervisor (tailor); fitter (internal combustion engine); inspector (sanitary); superintendent (office); apprentice (electrician).
Men Women Total Please give as far as possible approximate number of vacancies in each occupation you are likely to fill during the next calendar year due to retirement, expansion or reorganization
…………………………………….. ………….
…………… ………
……………………..
…………………………………….. …………. …………… ……… …………………….. Total Dated: Signature of employer. To, The Employment Exchange, (Please fill in here the address of your Local Employment Exchange) Note.—Total of Column (4) under Item 2 should correspond to the figure given against Item 2.
Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1
Forms under
APPRENTICESHIP RULES, 1992
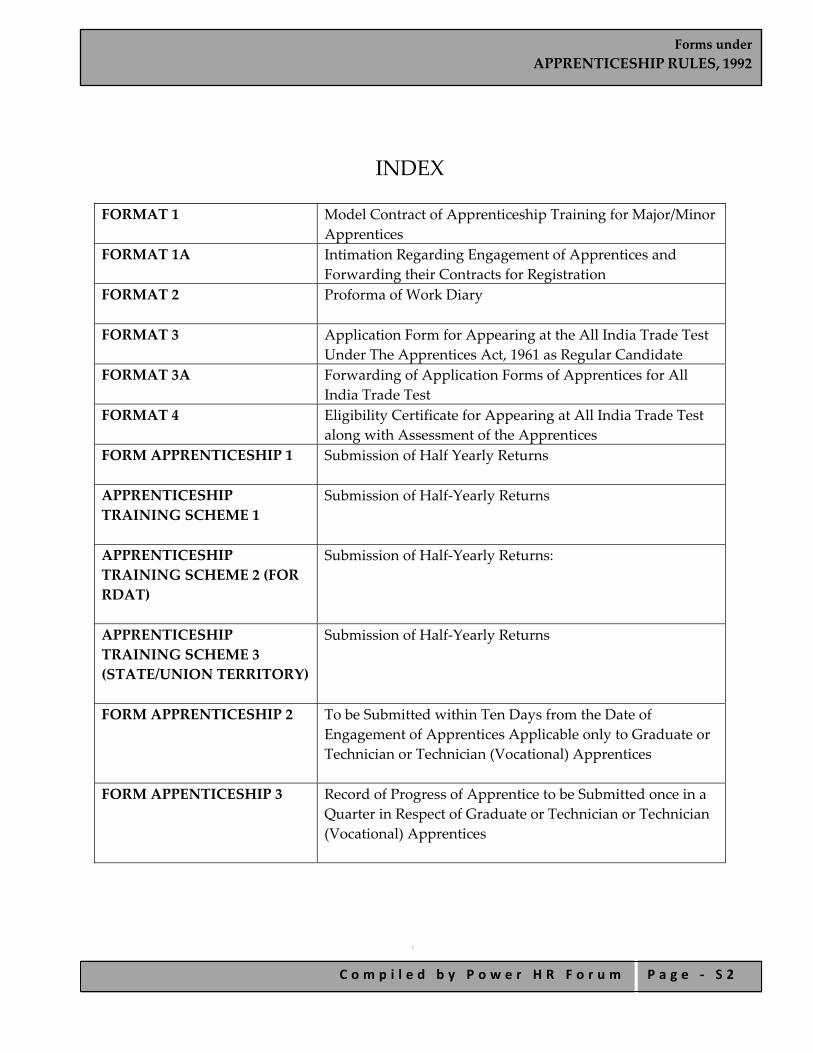
Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 2
INDEX FORMAT 1
Model Contract of Apprenticeship Training for Major/Minor Apprentices
FORMAT 1A
Intimation Regarding Engagement of Apprentices and Forwarding their Contracts for Registration
FORMAT 2
Proforma of Work Diary
FORMAT 3
Application Form for Appearing at the All India Trade Test Under The Apprentices Act, 1961 as Regular Candidate
FORMAT 3A
Forwarding of Application Forms of Apprentices for All India Trade Test
FORMAT 4
Eligibility Certificate for Appearing at All India Trade Test along with Assessment of the Apprentices
FORM APPRENTICESHIP 1
Submission of Half Yearly Returns
APPRENTICESHIP TRAINING SCHEME 1
Submission of Half‐Yearly Returns
APPRENTICESHIP TRAINING SCHEME 2 (FOR RDAT)
Submission of Half‐Yearly Returns:
APPRENTICESHIP TRAINING SCHEME 3 (STATE/UNION TERRITORY)
Submission of Half‐Yearly Returns
FORM APPRENTICESHIP 2
To be Submitted within Ten Days from the Date of Engagement of Apprentices Applicable only to Graduate or Technician or Technician (Vocational) Apprentices
FORM APPENTICESHIP 3
Record of Progress of Apprentice to be Submitted once in a Quarter in Respect of Graduate or Technician or Technician (Vocational) Apprentices
\

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 3
FORMAT 1 (See rule 14)
Model Contract of Apprenticeship Training
for Major/Minor Apprentices (To be prepared in Triplicate)
1. Name and address of the Establishment................................
Telephone No........................ Fax No............................ Telegram................................ E‐Mail Address..............
2. (a) Name of Apprentice (Block Letters)................................... (b) Father’s/Mother’s/Husband’s Name.................................
3. Correspondence Address............................................................
4. Date of birth...................................................................................
5. (a) Date of execution of contract:.............................................. (b) Age on the date of execution of contract.........................
6. Whether belongs to Scheduled Caste/Scheduled Tribe Physically Handicapped/Other Backward Class or Minority Community. If so, please mention the category.................... .................................................................
7. Present Qualification:— a. General Education:................................................................. b. Technical:..................................................................................
Name of the Trade/Course:............................................. Duration of Training:......................................................... From...........to....... Name of the Institute:........................................................ Name of the Board/Council:............................................
8. Name of the Apprenticeship Trade:..........................................
9. a. Duration of Apprenticeship Training:............................... b. Period of Apprenticeship:..............................................................years......months
Photograph of Apprentice

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 4
10. Rates of Stipend From.........to.......... First Year Rs.......p.m Second Year Rs.......p.m Third Year Rs......p.m Fourth Year Rs.......p.m
11. a. Name and Address of Guardian*:...................................... b. Relationship with the Apprentice:......................................
12. Name and Address of the Surety:............................................
13. We, the Employer, Apprentice/Guardian* and the Surety solemnly declare that we have read the Apprentices Act, 1961 and the Apprenticeship Rules, 1992 regarding the contract of Apprenticeship Training including obligations and agree to abide by all the provisions made thereunder. In case of default by either the apprentice or the employer, we agree to compensate the other party as per the provisions of the Apprenticeship Rules, 1992 (Main provisions of the rules may be seen in the Enclosure)
Signature of the Employer with seal
Signature of Apprentice
Signature of Guardian* Signature of Surety
14. Witnesses and their Addresses
1. ............................................. 2. .............................................
15. To be filled in by the Office of the Apprenticeship Adviser:—
i. Registration No..................................................... ii. Date......................................................................... iii. Place.........................................................................
Signature and Seal of the Regional Central ApprenticeshipAdviser/ State Apprenticeship Adviser
*Guardian, in case of minor apprentices
Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 5
ENCLOSURE TO CONTRACT OF APPRENTICESHIP TRAINNING
Main provisions of the Apprenticeship Rules relating to the contract of Apprenticeship Training
1.
a) The employer shall pay stipend to the trade apprentices at the minimum rates of [As per the provision of rule 11(1) of Apprenticeship Rules, 1992]
Rs. 820 per month during first year.
Rs. 940 per month during second year.
Rs. 1090 per month during third year.
Rs. 1230 per month during fourth year.
Rates are liable to change.
b) The stipend for a particular month shall be paid by the tenth day of the following month. No deduction shall be made from the stipend for the period during which an apprentice remains on casual or medical leave as per provision of the rule. Stipend shall, however, not be paid for the period for which the apprentice remains on extraordinary leave.
2. Where the Contract of Apprenticeship is terminated through failure on the part of the employer in carrying out the terms and conditions of the contract (As notified under the Apprenticeship Rules, 1992), he shall pay to the apprentice compensation as prescribed.
3.
a. In the event of premature termination of Contract of Apprenticeship for failure on the part of apprentice to carry out the terms and conditions of the contract (As notified under the Apprenticeship Rules, 1992), the surety at the request of apprentice hereby guarantees to employer the payment of such amount as determined by the Apprenticeship Adviser as and towards the cost of training.
b. The liability of the surety is limited to Rs. 2,500 (Rupees Two thousand five hundred five hundred only) with interest at twelve per cent. per annum.
4. It shall not be obligatory on the part of employer to offer any employment to the passed out trade apprentice on completion of the period of Apprenticeship Training in his establishment, nor shall it be obligatory on the part of the Apprentice to accept an employment under the employer.

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 6
FORMAT 1A Last Date for Forwarding the Contracts for Registration
For the apprentices engaged from 16th January to 15th April : 30th April For the apprentices engaged from 16th April to 15th July : 31st July For the apprentices engaged from 16th July to 15th October : 31st October For the apprentices engaged from 16th October to 15th January : 31st January
Name and Address of Establishment........................................................ Telephone No....................... Telex/Fax No............................. Telegram................................ E‐Mail Address.......................... To The State/Union Territory Apprenticeship Adviser/ The Regional Director of Apprenticeship Training Subject:—Intimation regarding engagement of apprentices and forwarding their contracts for registration Sir/Madam,
Following apprentices have been engaged in our establishment.
Their contracts are forwarded for registration.
Serial Number Name Father’s/Mother’s/Husband’s Name
Trade
We have satisfied ourselves that they fulfill the eligibility criteria as per the provisions of Apprentices Act, 1961 and rules made thereunder. Copies of attested certificates are also enclosed.
Yours Faithfully,
Encl.: As stated above Signature of Employer with
Designation and Seal.

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 7
FORMAT 2 Proforma of Work Diary
Name and Address of Establishment...................................... Name of Apprentice.................................................................... Trade............................................................................................... Registration Number................................................................... Serial Number Date (Week) Job/Work done during the week Signature of Supervisor From To
Note.—The work diary should be maintained by the Apprentice and countersigned by his supervisor once a week.

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 8
FORMAT 3 Last date for forwarding the application
For the All India Trade Test to be held in April/May : 31st December of previous year
For the All India Trade Test to be held in October/November: 30th June
Application Form for Apprearing at the All India Trade Test to be Held in...........(Month).............(Year) under the Apprentices Act, 1961 as Regular Candidate
1. Name (In block letters)................................................... 2. Father’s/Mother’s/Husband’s Name........................... 3. Mailing Address................................................................ 4. Name and Address of establishment where undergoing Apprenticeship
Training.................................................. 5. Name of the Designated Trade.................................... 6. Contract Registration Number..................................... 7. Period of Apprenticeship Training............................... From .............to............ 8. Whether passed in the subject of Social Studies? If so, please give following details:—
a. All‐India Trade Test for Craftsmen held in......................(Month).................(Year) b. Marks obtained in the subject of Social Studies................. (Please enclose attested copies of certificate) Signature of Employer with seal Signature of Apprentice with Date (For office use in RDAT/SAA)
May be allowed subject to fulfillment of eligibility criteria. If not allowed reason therefore...........................................
Name and Signature of Regional Director/SAA.
Photo of apprentice

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 9
FORMAT 3A Last date for forwarding of application For the All India Trade Test to be held in April/May: 31st December of previous year For the All India Trade Test to be held in October/November: 30th June Name and Address of Establishment.......................................... Telephone No................... Telex/Fax No.............. Telegram............................ E‐Mail Address............ To The State/Union Territory Apprenticeship Adviser/ The Regional Director of Apprenticeship Training Subject.—Forwarding of Application Forms of Apprentices for All India Trade Test to be held in .....................(Month)...............(Year) Sir/Madam, The application forms in respect of the following apprentices are forwarded for appearing in All India Trade Test to be held in.....................(Month)...............(Year) Serial Number
Designated Trade Name of the Apprentice
Contract Number Registration
A Demand Draft drawn in favour of ................................is also forwarded towards examination fee of above apprentices @ Rs...................................................
Certified that the progress and attendance of above apprentices are satisfactory.
Date.................... Signature of the Employer with
Designations and Seal.
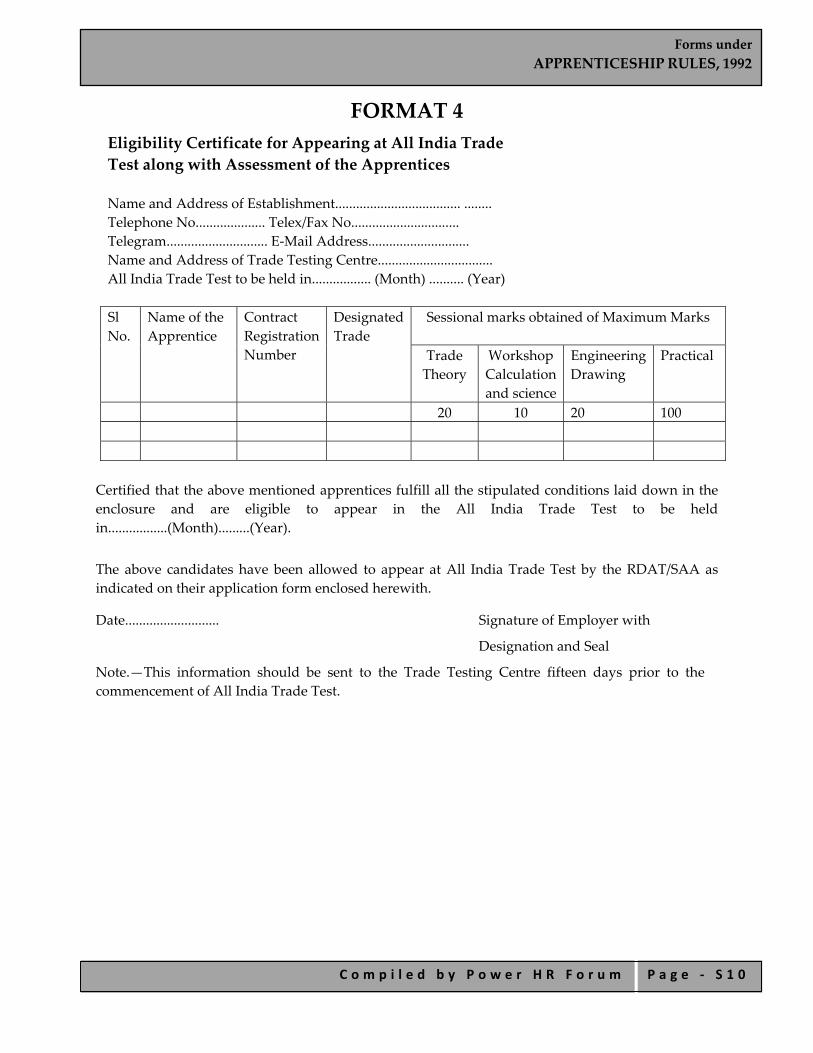
Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 0
FORMAT 4 Eligibility Certificate for Appearing at All India Trade Test along with Assessment of the Apprentices
Name and Address of Establishment.................................... ........ Telephone No.................... Telex/Fax No............................... Telegram............................. E‐Mail Address............................. Name and Address of Trade Testing Centre................................. All India Trade Test to be held in................. (Month) .......... (Year) Sl No.
Name of the Apprentice
Contract Registration Number
DesignatedTrade
Sessional marks obtained of Maximum Marks
Trade Theory
Workshop Calculation and science
Engineering Drawing
Practical
20 10 20 100
Certified that the above mentioned apprentices fulfill all the stipulated conditions laid down in the enclosure and are eligible to appear in the All India Trade Test to be held in.................(Month).........(Year). The above candidates have been allowed to appear at All India Trade Test by the RDAT/SAA as indicated on their application form enclosed herewith.
Date........................... Signature of Employer with
Designation and Seal
Note.—This information should be sent to the Trade Testing Centre fifteen days prior to the commencement of All India Trade Test.

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 1
ENCLOSURE TO ELIGIBILITY CERTIFICATE
Instructions and Guidance to determine eligibility of a candidate for appearing at All India Test under the Apprentices Act, 1961
For determining the eligibility of a candidate to appear at All India Trade Test (AITT), the following points are to be taken into account:— 1. Only those apprentices whose contracts have been registered are eligible for appearing at
AITT. 2. The apprentices who will complete contractual period of training on or before 15th April or
15th October of the calendar year would be eligible for appearing at AITT to be held in April/May or October/November respectively.
3. A candidate who has completed/will be completing Apprenticeship Training on or before the dates as stated at Sl. No. 2 above and has put in the minimum attendance i.e., 200 days per year of apprenticeship training which includes 33 days attendance in Related Instruction Classes or establishments working for five days in a week and 240 days of attendance per year of apprenticeship training which includes 40 days of attendance in R.I. Classes for establishments working for 6 days in a week is eligible for appearing at AITT.
4. A candidate who has completed/will be completing apprenticeship training as stated above but failed/will be failing to acquire minimum attendance for circumstances beyond his control and the employer is satisfied with the grounds for shortfall in attendance and certifies that the apprentice has otherwise completed the full apprenticeship course, he shall be considered as having completed the full period of training and shall be eligible for appearing at AITT.
5. A candidate who has completed/will be completing Apprenticeship Training on or before the dates as stated above but failed/will be failing to put in the minimum period of attendance has not completed the full apprenticeship course, he shall not be considered as having completed the full period of training and the employer shall under sub‐rule (2) of rule 7 of Apprenticeship Rules, 1992 extend his period of training until he completes the full apprenticeship course, and the next test is held if so required by the Apprenticeship Adviser. Similar extension of the period of training may also be allowed in case of those apprentices who having completed but failed in the AITT. An apprentice who fails in the second test shall not be allowed for any extension of the period of training.
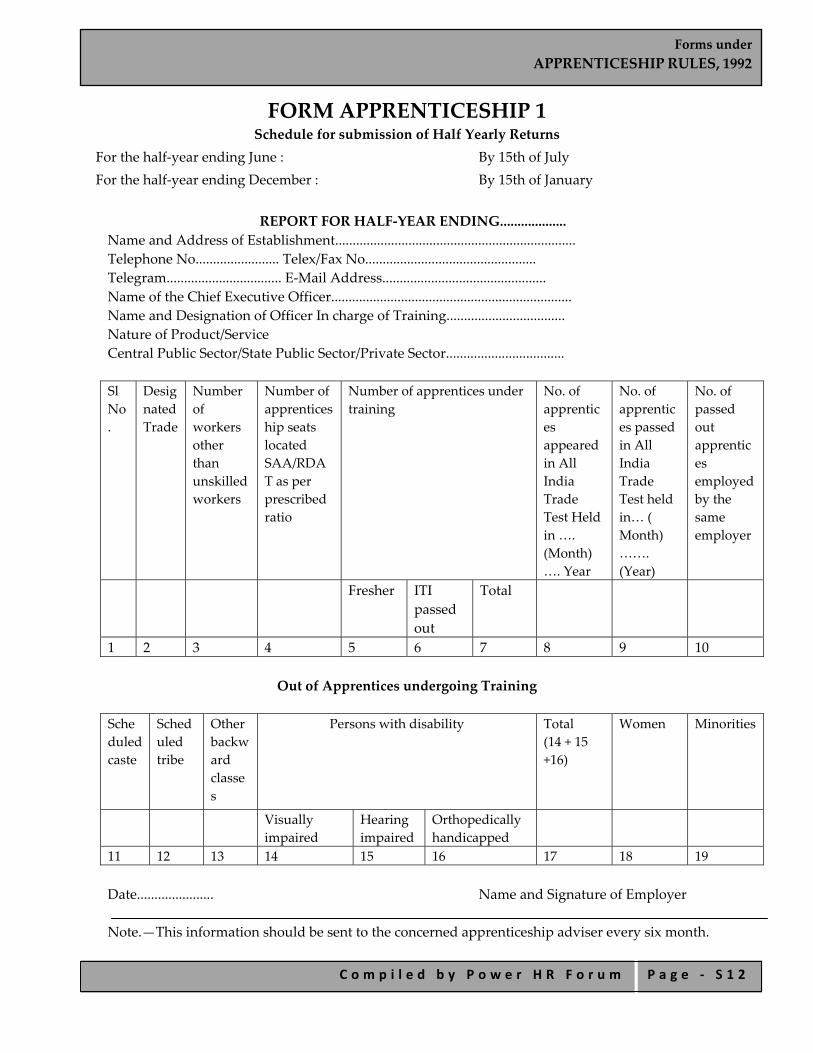
Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 2
FORM APPRENTICESHIP 1 Schedule for submission of Half Yearly Returns
For the half‐year ending June : By 15th of July For the half‐year ending December : By 15th of January
REPORT FOR HALF‐YEAR ENDING................... Name and Address of Establishment..................................................................... Telephone No........................ Telex/Fax No................................................. Telegram................................. E‐Mail Address............................................... Name of the Chief Executive Officer..................................................................... Name and Designation of Officer In charge of Training.................................. Nature of Product/Service Central Public Sector/State Public Sector/Private Sector..................................
Sl No.
Designated Trade
Number of workers other than unskilled workers
Number of apprenticeship seats located SAA/RDAT as per prescribed ratio
Number of apprentices under training
No. of apprentices appeared in All India Trade Test Held in …. (Month)…. Year
No. of apprentices passed in All India Trade Test held in… ( Month) ……. (Year)
No. of passed out apprentices employed by the same employer
Fresher ITI passed out
Total
1 2 3 4 5 6 7 8 9 10
Out of Apprentices undergoing Training Scheduled caste
Scheduled tribe
Other backward classes
Persons with disability Total (14 + 15 +16)
Women Minorities
Visually impaired
Hearing impaired
Orthopedically handicapped
11 12 13 14 15 16 17 18 19 Date...................... Name and Signature of Employer Note.—This information should be sent to the concerned apprenticeship adviser every six month.

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 3
APPRENTICESHIP TRAINING SCHEME 1 Schedule for Submission of Half‐Yearly Returns
For the half‐year ending June : By 31st July For the half‐year ending December : By 31st January
REPORT FOR THE HALF‐YEARLY ENDING.................... Name and Adress of Regional Director of Apprenticeship......................... Training/State/UT/Apprenticeship Adviser.................................................... Telephone No........................ Telex/Fax No....................................... Telegram................................ E‐Mail Address..................................... Sl. No.
Designated Trade
Number of workers other than unskilled workers
Number of apprenticeship seats located by SAA/ RDAT as prescribed ratio
Number of apprentices under Training
Number of apprentices appeared in All India Trade Test held in....... (Month) .......(Year
)
Number of apprentices passed in All India
Trade Test held in..... (Month)
.......(Ysear)
Number of passed out apprentices employed
by the same employer
Fresher ITI passed out
Total
1 2 3 4 5 6 7 8 9 10 Scheduled caste
Scheduled tribe
Other backward classes
Persons with disability Total (14 + 15 +16)
Women Minorities
Visually impaired
Hearing impaired
Orthopedically handicapped
11 12 13 14 15 16 17 18 19 Date...................... Name and Signature of Apprenticeship Adviser
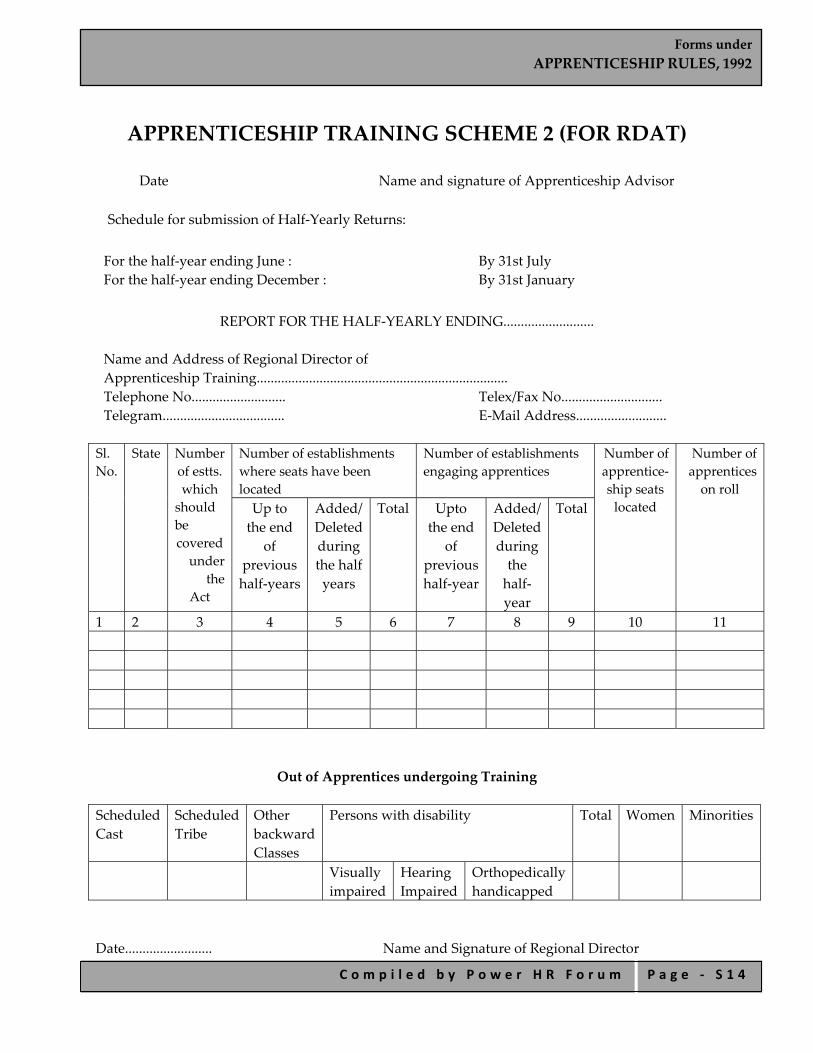
Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 4
APPRENTICESHIP TRAINING SCHEME 2 (FOR RDAT)
Date Name and signature of Apprenticeship Advisor Schedule for submission of Half‐Yearly Returns: For the half‐year ending June : By 31st July For the half‐year ending December : By 31st January
REPORT FOR THE HALF‐YEARLY ENDING..........................
Name and Address of Regional Director of Apprenticeship Training........................................................................ Telephone No........................... Telex/Fax No............................. Telegram................................... E‐Mail Address..........................
Sl. No.
State Number of estts. which should be covered under
the Act
Number of establishments where seats have been located
Number of establishments engaging apprentices
Number of apprentice‐ship seats located
Number of apprentices on roll
Up to the end
of previous half‐years
Added/ Deleted during the half years
Total Upto the end
of previous half‐year
Added/ Deleted during the half‐ year
Total
1 2 3 4 5 6 7 8 9 10 11
Out of Apprentices undergoing Training Scheduled Cast
Scheduled Tribe
Other backward Classes
Persons with disability Total Women Minorities
Visually impaired
Hearing Impaired
Orthopedically handicapped
Date......................... Name and Signature of Regional Director
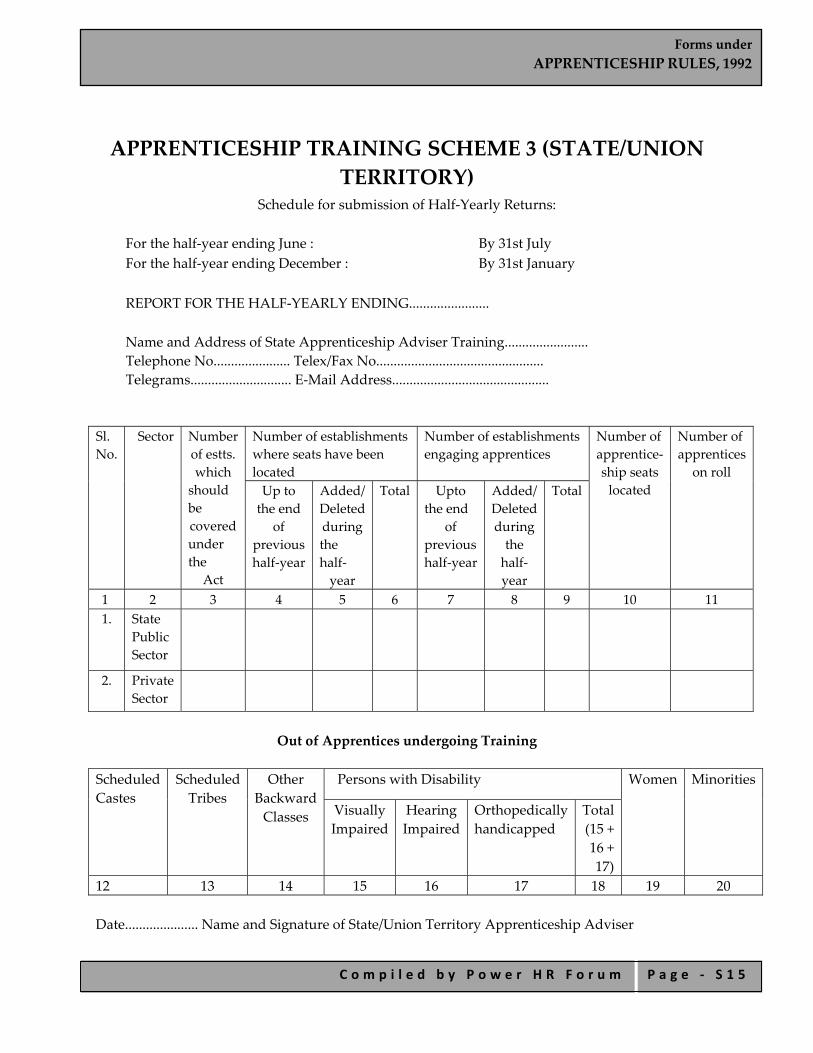
Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 5
APPRENTICESHIP TRAINING SCHEME 3 (STATE/UNION TERRITORY)
Schedule for submission of Half‐Yearly Returns:
For the half‐year ending June : By 31st July For the half‐year ending December : By 31st January REPORT FOR THE HALF‐YEARLY ENDING....................... Name and Address of State Apprenticeship Adviser Training........................ Telephone No...................... Telex/Fax No................................................ Telegrams............................. E‐Mail Address.............................................
Sl. No.
Sector Number of estts. which should be covered under the
Act
Number of establishments where seats have been located
Number of establishments engaging apprentices
Number of apprentice‐ship seats located
Number of apprentices
on roll Up to the end
of previous half‐year
Added/ Deleted during the half‐ year
Total Upto the end
of previous half‐year
Added/ Deleted during the half‐ year
Total
1 2 3 4 5 6 7 8 9 10 11 1. State
Public Sector
2. Private Sector
Out of Apprentices undergoing Training
Scheduled Castes
Scheduled Tribes
Other Backward Classes
Persons with Disability Women Minorities
Visually Impaired
Hearing Impaired
Orthopedically handicapped
Total (15 + 16 + 17)
12 13 14 15 16 17 18 19 20 Date..................... Name and Signature of State/Union Territory Apprenticeship Adviser

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 6
FORM APPRENTICESHIP 2 [To be Submitted within Ten Days from the Date of Engagement of Apprentices Applicable only to Graduate or Technician or
Technician (Vocational) Apprentices]
Please state whether the apprentice is a student of Sandwich course: Yes/No
Personal Details
Name and address of establishment
Nature of industry and standard industrial classification Code No.
Registration No. and date of contract of apprenticeship
Subject field in Engineering/ Technology/ Vocational courses
Date of commencement to training
Name and address of apprentice
Name and address of father/guardian
1 2 3 4 5 6 7
Educational qualification at entry
Date, month and year of birth
Examination passed
Name of Institution
Date of passing Emarks
_____________________________________________________________________________ Period of training................................................. Date of completion of Training........................ Rate of Stipend to...............................................
Passport size photo of apprentice

Forms under APPRENTICESHIP RULES, 1992
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ S 1 7
FORM APPENTICESHIP 3 Record of Progress of Apprentice [To be Submitted once in a Quarter in Respect of Graduate or Technician or Technician (Vocational) Apprentices]
1. Name of Apprentice............................................................
2. Registration Number..........................................................
3. Subject field in Engineering or Technology or Vocational Course......................
4. Under training at...........................................................................................................
5. Date of commencement of training............................................................................
6. Area of training during the quarter.............................................................................
7. Progress report for quarter....................................to...................................................
i. Aptitude for training................................................................................................ ii. Performance during the quarter............................................................................ iii. Shortcomings, if any................................................................................................. iv. Reaction of trainee to corrective action at (iii) above....................................... v. Assessment:
Excellent/Above Average/Average/Below Average (Strike out those not applicable)
Signature of Officer/Executive in‐charge of Training
“Remarks.............................................................................. Signature of Manager of the Industry/Establishment.”]
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1
Forms under
THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2
INDEX
FORM A Form of Application for the Reference of an Industrial Dispute to a Board of Conciliation/Court of Enquiry/Labour Court/Tribunal/National Tribunal under Section 10(2) of The Industrial Disputes Act, 1947
FORM B Notice o Parties to Nominate Representatives FORM C Agreement FORM D Summons FORM E Notice of Change of Service Condition Proposed by an Employer FORM F Nomination of Representative FORM G Form of Nomination Paper Form G Progress Report on Constitution and Functioning of Works Committee for the
Half‐Year Ending the 30th June/31st December FORM H Form for Memorandum of Settlement FORM I Complaints under Section 33‐A of The Industrial Disputes Act,1847 FORM J
Application for Permission under Sub Section (1) or Sub –Section (3) of Section 33 of The Industrial Disputes Act, 1947
FORM K
Application under Sub‐Section (2) of Section 33 of The Industrial Disputes Act, 1947
FORM K 1 Application under Sub‐Section (1) of Section 33c of The Industrial Disputes Act, 1947
FORM K 2
Application by a Person Authorised by a Workman or by the Assignee or Heir of a Deceased Workman under Sub‐Section (1) of Section 33‐C of The Industrial Disputes Act, 1947
FORM K 3 Application Under Sub‐Section (2) Of Section 33‐C of The Industrial Disputes Act, 1947
FORM K 4
Application by a Person Who is an Assignee or Heir of a Deceased Workman Under Sub‐Section (2) of Section 33‐C of The Industrial Disputes Act, 1947 (14 of 1947)
FORM L Form of Notice of Strike to be Given by Union/Workmen in Public Utility Service FORM M
Form of Notice of Lock‐Out to be Given by an Employer Carrying on a Public Utility Service
FORM N Form of Report of Strike or Lock‐Out in a Public Utility Service FORM O Register of Settlements
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 3
FORM O 1 Notice of Lay off FORM O 2 Notice of End of Lay off FORM O 3
Form of Application for Permission to Lay‐off, to Continue the Lay‐off of Workmen in Industrial Establishments to Which Provisions of Chapter VB of The Industrial Disputes Act, 1947 (14 Of 1947) Apply
FORM P
Form of Notice of Retrenchment to be Given by an Employer Under Clause (C) of Section 25F of Industrial Disputes Act, 1947
FORM PA
Form of Notice for Permission for Retrenchment of Workmen to be Given by an Employer under Clause (D) of Sub‐Section (1) of Section 25N of The Industrial Disputes Act, 1947 (14 Of 1947)
FORM Q
Form of Notice of Closure to be Given by an Employer Under Section 25FFA of The Industrial Disputes Act, 1947 (14 Of 1947)
FORM QA
Form of Notice For Permission of Closure to be Given by an Employer under Sub‐Section (1) of Section 25‐O of The Industrial Disputes Act, 1947 (14 Of 1947)
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 4
FORM A
(See rule 3)
Form of Application for the Reference of an Industrial Dispute to a Board of Conciliation/Court of Enquiry/Labour Court/ Tribunal/National Tribunal Under Section 10(2) of The
Industrial Disputes Act, 1947
Whereas an industrial dispute **is apprehended/exists between....................................and..............................and it is expedient that **the matters specified in the enclosed statement which are connected with or relevant to the dispute he should be referred for **enquiry/adjudication by a Board of conciliation/a court of Enquiry/a Labour Court/a Tribunal/a National Tribunal for investigation and settlement, an application is hereby made under sub‐section (2) of section 10 of the Industrial Disputes Act, 1947, that the **said matters/said dispute should be referred to **a Board of conciliation/a Court of Enquiry/a Labour Court/a Tribunal/a National Tribunal. This application is made by the undersigned who have/has been duly authorised to do so by virtue of a resolution (copy enclosed) adopted by a majority of the members present at a meeting of the ...................................held on the................................. 20.... A statement giving the particulars required under rule 3 of the Industrial Disputes(Central) Rules, 1957, is attached. Dated the.................. Signature of employer **..........................................................
or agent............................................................................. or manager....................................................................... or principal officer of the Corporation.....................................................................
Signature of the President of the trade union **..................................... Secretary of the trade union.........................................
Or **Signature of five representatives
duly authorized (vide resolution enclosed)..........................................................................
Or **Signature of the workman...........................
Or **Signature of the workman in the same establishment duly authorised (vide authorisation

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 5
enclosed)...................................................................................] To The Secretary to the Government of India, Ministry of Labour. Statement required under rule 3 of the Industrial Disputes (Central) Rules, 1957, to accompany the form of application prescribed under sub‐section (2) of section 10 of the Industrial Disputes Act, 1947:
a. Parties to the dispute including the name and address of the establishment or undertaking involved;
b. Specific matters in dispute; c. Total number of workmen employed in the undertaking affected; d. Estimated number of workmen affected or likely to be affected by the dispute; e. Efforts made by the parties themselves to adjust the dispute.
Copy to—
i. The Assistant Labour Commissioner (Central) .......................................................; [here enter office address of the Assistant Labour Commissioner (Central) in the local area concerned];
ii. The Regional Labour Commissioner (Central); iii. The Chief Labour Commissioner (Central), New Delhi.
**Delete whichever is not applicable.

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 6
FORM B (See rule 6)
Notice to Parties to Nominate Representatives
Whereas an industrial dispute has arisen/is apprehended between ........................... and..........................and it is expedient to refer the said dispute under section 10 of the Industrial Disputes Act, 1947, to a Board of Conciliation for the purpose of investigating the same and for promoting a settlement thereof, you are hereby required to intimate to the undersigned not later than the .................... the name(s) and address (es) of one /two person(s) whom you wish to recommend for appointment as your representative(s) on the said Board. If you fail to make the recommendation by the date specified above, the Central Government will select and appoint such person(s) as it thinks fit to represent you.
Secretary to the Government of India, Ministry of Labour.
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 7
FORM C (See rule 7)
Agreement [Under section 10A of the Industrial Disputes Act, 1947]
Name of the Parties:
Representing employers: Representing workmen/workman:
It is hereby agreed between the parties to refer the following dispute to the arbitration of ............................................. [here specify the name(s) and address(es) of the arbitrator(s)].
i. Specific matters in disputes; ii. Details of the parties to the dispute including the name and address of the
establishment or undertaking involved; iii. Name of the workman in case he himself is involved in the dispute or the name
of the Union, if any, representing the workmen or workman in question; iv. Total number of workmen employed in the undertaking affected; v. Estimated number of workmen affected or likely to be affected by the dispute.
*We further agree that the majority decisions of the arbitrator(s) be binding on us/ in case the arbitrators are equally divided in their opinion, that they shall appoint another person as umpire whose award shall be binding on us. The arbitrator(s) shall make his (their) award within a period of ....................... (here specify the period agreed upon by the parties) [from the date of publication of tthis agreement in the official Gazzette by the appropriate Government] or within such further time as is extended by mutual agreement between us in writing. In case the award is not made within the period aforementioned, the reference to arbitration shall stand automatically cancelled and we shall be free to negotiate for fresh arbitration.
Signature of the parties Representing employer
**Workman/Representing workman/workmen Witnesses: (1) (2) Copy to:
i. The Assistant Labour Commissioner (Central), (here enter office address of the Conciliation Officer in local area concerned);
ii. The Regional Labour Commissioner (Central)............; iii. The Chief Labour Commissioner (Central), New Delhi; iv. The Secretary to the Government of India, Ministry of Labour, Employment
and Rehabilitation (Department of Labour and Employment), New Delhi.
*Where applicable. **Delete whichever is not applicable.]

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 8
FORM D (See rule 17)
Summons
Whereas an industrial dispute between .......................... and ...................................... has been referred to this Board of Conciliation for investigation and settlement, Court of Enquiry for investigation/Labour Court/Tribunal/National Tribunal for adjudication, under section 10 of the Industrial Disputes Act, 1947, you are hereby summoned to appear before the Board/Court/Labour Court/Tribunal/National Tribunal in person on the .............. day of ........... at .......... o’clock in the ............................. noon to answer all material questions relating to the said dispute and you are directed to produce on that day all the books, papers and other documents and things in your possession or under control in any way relating to the matter under investigation by this Board/Court/Labour Court/Tribunal/National Tribunal. Date ............................
Board of Conciliation. Chairman/Secretary,———————————
Court of Enquiry.
Labour Court. ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
Tribunal Presiding Officer/Secretary, —————————————
National Tribunal
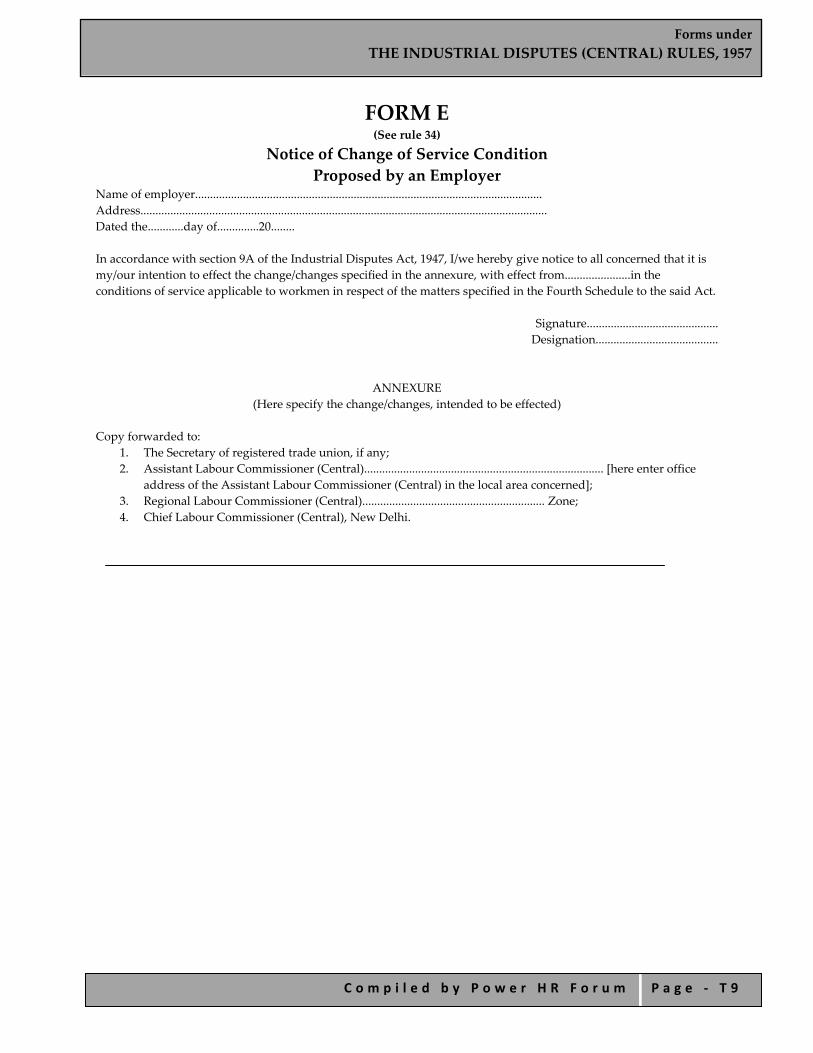
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 9
FORM E (See rule 34)
Notice of Change of Service Condition Proposed by an Employer
Name of employer.................................................................................................................... Address........................................................................................................................................ Dated the............day of..............20........ In accordance with section 9A of the Industrial Disputes Act, 1947, I/we hereby give notice to all concerned that it is my/our intention to effect the change/changes specified in the annexure, with effect from......................in the conditions of service applicable to workmen in respect of the matters specified in the Fourth Schedule to the said Act.
Signature............................................ Designation.........................................
ANNEXURE (Here specify the change/changes, intended to be effected)
Copy forwarded to:
1. The Secretary of registered trade union, if any; 2. Assistant Labour Commissioner (Central)................................................................................ [here enter office
address of the Assistant Labour Commissioner (Central) in the local area concerned]; 3. Regional Labour Commissioner (Central)............................................................. Zone; 4. Chief Labour Commissioner (Central), New Delhi.

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 0
FORM F Nomination of Representative
(See rule 36)
Before (Here mention the authority concerned)
Reference No.........................................of....................................................................................................................workmen
Versus ......................................................................................................................................Employer In the matter of …………………………………..I/we hereby authorise Shri/Sarvashree........................ to represent me/us in the above matter. Dated this..............day of............20......
Signature of person(s) nominating the representative(s) Address
Accepted. Signature of representative(s). Address.
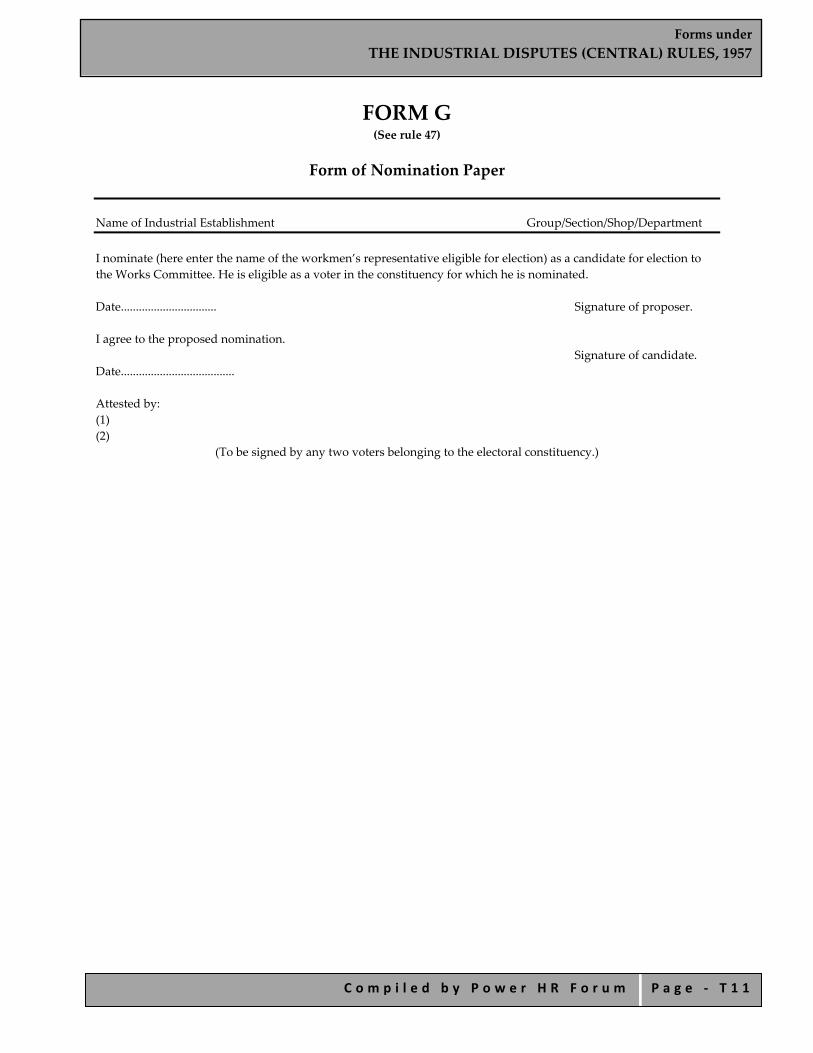
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 1
FORM G (See rule 47)
Form of Nomination Paper
Name of Industrial Establishment Group/Section/Shop/Department I nominate (here enter the name of the workmen’s representative eligible for election) as a candidate for election to the Works Committee. He is eligible as a voter in the constituency for which he is nominated. Date................................ Signature of proposer. I agree to the proposed nomination.
Signature of candidate. Date...................................... Attested by: (1) (2)
(To be signed by any two voters belonging to the electoral constituency.)
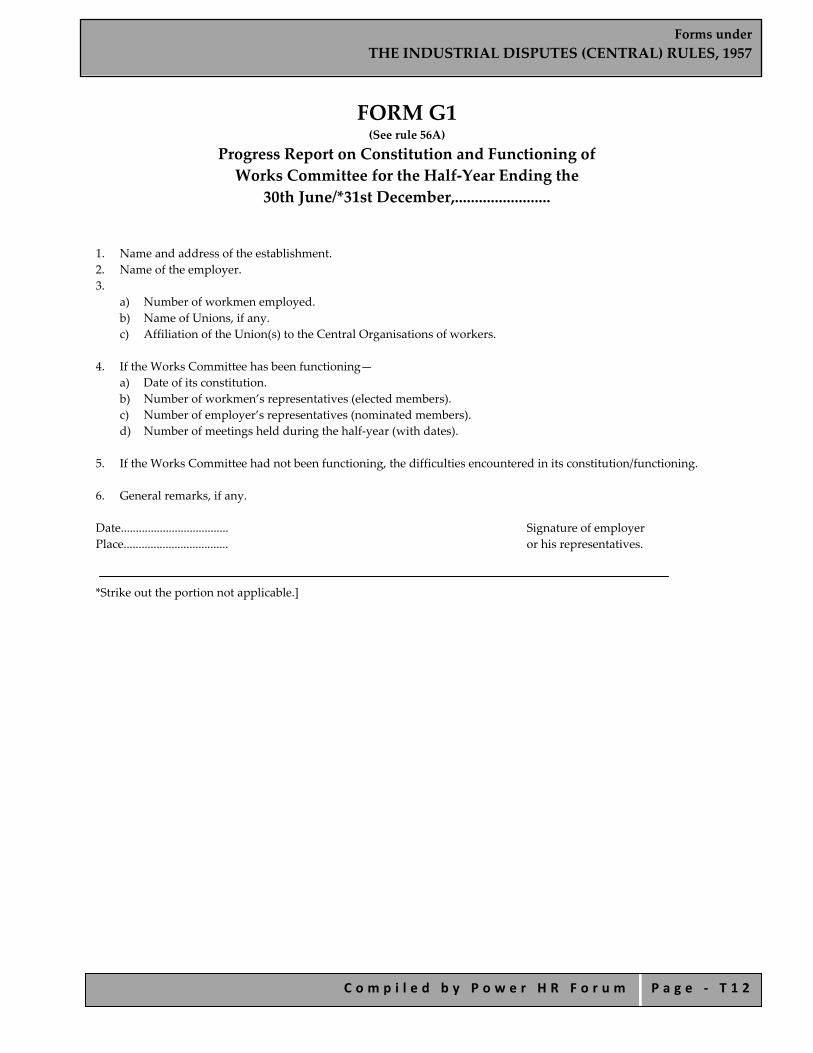
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 2
FORM G1 (See rule 56A)
Progress Report on Constitution and Functioning of Works Committee for the Half‐Year Ending the
30th June/*31st December,........................
1. Name and address of the establishment. 2. Name of the employer. 3.
a) Number of workmen employed. b) Name of Unions, if any. c) Affiliation of the Union(s) to the Central Organisations of workers.
4. If the Works Committee has been functioning—
a) Date of its constitution. b) Number of workmen’s representatives (elected members). c) Number of employer’s representatives (nominated members). d) Number of meetings held during the half‐year (with dates).
5. If the Works Committee had not been functioning, the difficulties encountered in its constitution/functioning. 6. General remarks, if any. Date.................................... Signature of employer Place................................... or his representatives. *Strike out the portion not applicable.]
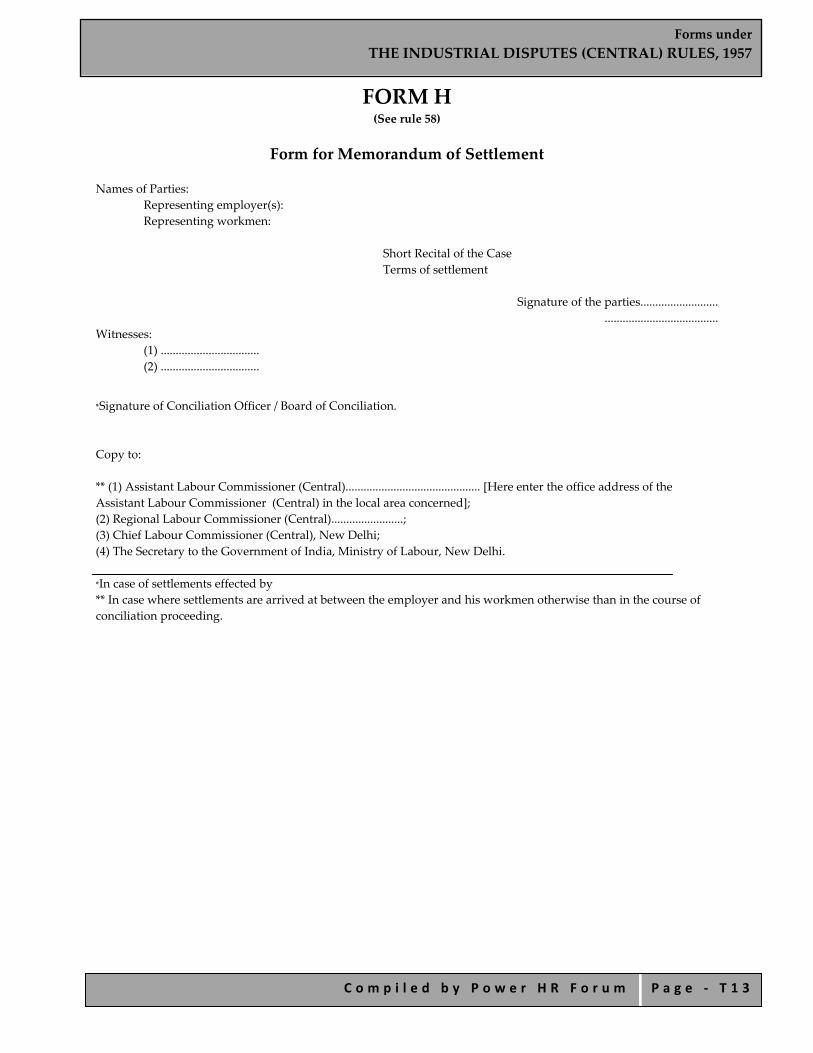
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 3
FORM H (See rule 58)
Form for Memorandum of Settlement
Names of Parties: Representing employer(s): Representing workmen:
Short Recital of the Case Terms of settlement
Signature of the parties..........................
...................................... Witnesses:
(1) ................................. (2) .................................
*Signature of Conciliation Officer / Board of Conciliation.
Copy to: ** (1) Assistant Labour Commissioner (Central)............................................. [Here enter the office address of the Assistant Labour Commissioner (Central) in the local area concerned]; (2) Regional Labour Commissioner (Central)........................; (3) Chief Labour Commissioner (Central), New Delhi; (4) The Secretary to the Government of India, Ministry of Labour, New Delhi. *In case of settlements effected by ** In case where settlements are arrived at between the employer and his workmen otherwise than in the course of conciliation proceeding.

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 4
FORM I (See rule 59)
Before the Labour Court/ Tribunal / National Tribunal
Complaint under Section 33A of the Industrial Disputes Act, 1947
A............................................ Complainant(s);
Versus
B....................................... Opposite Party(ies). Address: In the matter of : Reference No. ................................... The petitioner(s) begs/beg to complain that the Opposite Party(ies) has/have been guilty of a contravention of the provisions of section 33 of the Industrial Disputes Act, 1947 (14 of 1947), as shown below: (Here set out briefly the particulars showing the manner in which the alleged contravention has taken place and the grounds on which the order or act of the Management is challenged.) The complainant(s) accordingly prays/pray that the Labour Court/ Tribunal/ National Tribunal may be pleased to decide the complaint set out above and pass such order or orders thereon as it may deem fit and proper. The number of copies of the complaint and its annexures required under rule 59 of the Industrial Dispute (Central) Rules, 1957, are submitted herewith.
Signature of the Complainant(s)
Dated this............day of............20..... Verification
I do solemnly declare that what is stated in paragraph.............................. above is true to my knowledge and that what is stated in paragraphs....................................... above is stated upon information received and believed by me to be true. * This verification is signed by me at.................... on ............day of.....................20......
Signature or Thumb impression of the person verifying
* Delete, if not applicable
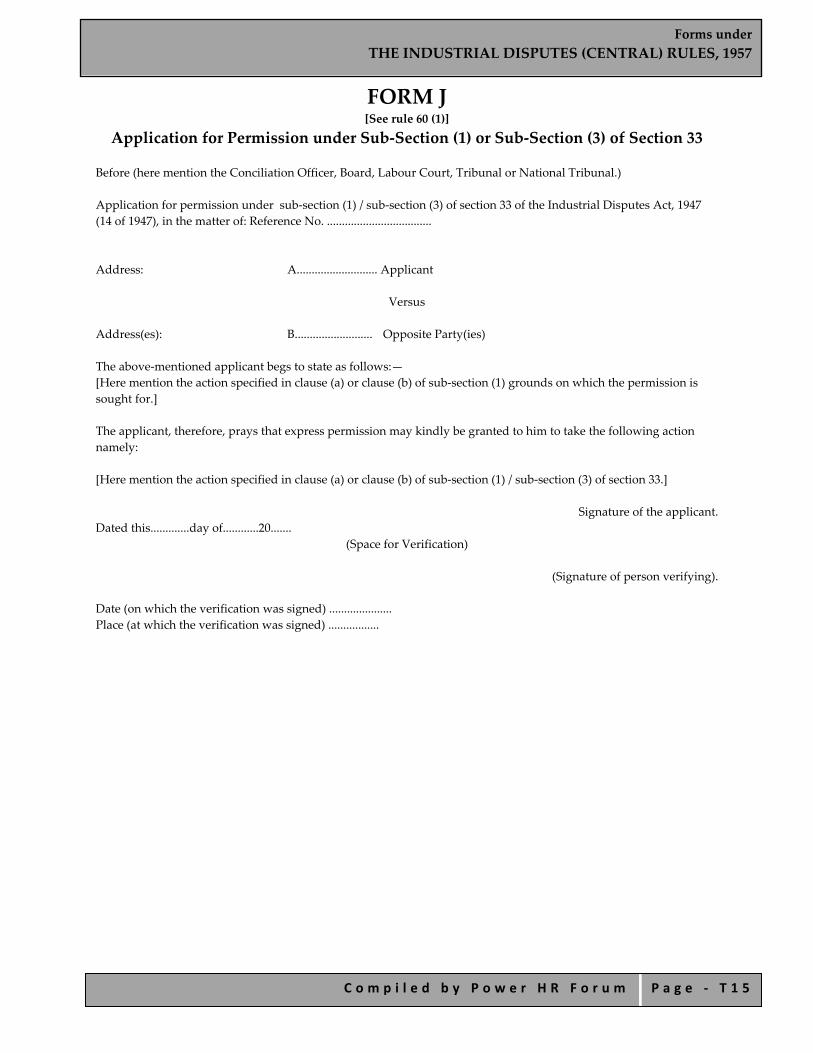
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 5
FORM J [See rule 60 (1)]
Application for Permission under Sub‐Section (1) or Sub‐Section (3) of Section 33
Before (here mention the Conciliation Officer, Board, Labour Court, Tribunal or National Tribunal.) Application for permission under sub‐section (1) / sub‐section (3) of section 33 of the Industrial Disputes Act, 1947 (14 of 1947), in the matter of: Reference No. ................................... Address: A........................... Applicant
Versus
Address(es): B.......................... Opposite Party(ies) The above‐mentioned applicant begs to state as follows:— [Here mention the action specified in clause (a) or clause (b) of sub‐section (1) grounds on which the permission is sought for.] The applicant, therefore, prays that express permission may kindly be granted to him to take the following action namely: [Here mention the action specified in clause (a) or clause (b) of sub‐section (1) / sub‐section (3) of section 33.]
Signature of the applicant.
Dated this.............day of............20....... (Space for Verification)
(Signature of person verifying).
Date (on which the verification was signed) ..................... Place (at which the verification was signed) .................
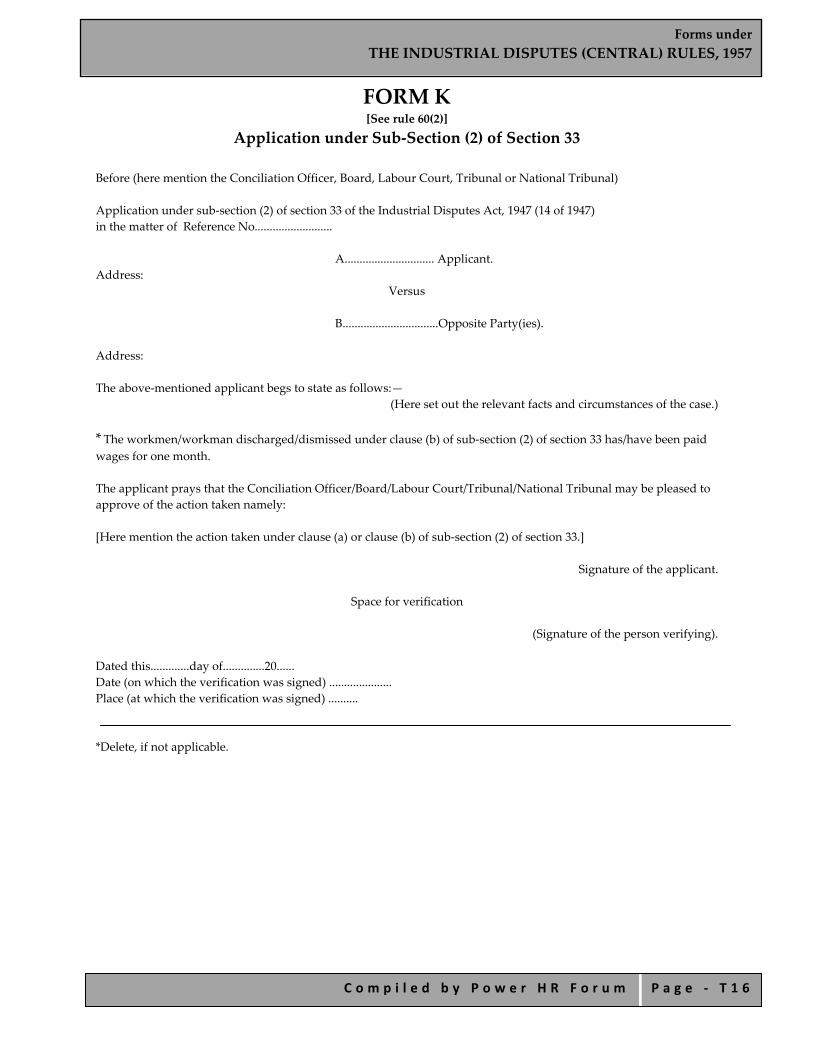
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 6
FORM K [See rule 60(2)]
Application under Sub‐Section (2) of Section 33
Before (here mention the Conciliation Officer, Board, Labour Court, Tribunal or National Tribunal)
Application under sub‐section (2) of section 33 of the Industrial Disputes Act, 1947 (14 of 1947) in the matter of Reference No..........................
A.............................. Applicant. Address:
Versus
B................................Opposite Party(ies).
Address: The above‐mentioned applicant begs to state as follows:—
(Here set out the relevant facts and circumstances of the case.)
* The workmen/workman discharged/dismissed under clause (b) of sub‐section (2) of section 33 has/have been paid wages for one month. The applicant prays that the Conciliation Officer/Board/Labour Court/Tribunal/National Tribunal may be pleased to approve of the action taken namely: [Here mention the action taken under clause (a) or clause (b) of sub‐section (2) of section 33.]
Signature of the applicant.
Space for verification
(Signature of the person verifying).
Dated this.............day of..............20...... Date (on which the verification was signed) ..................... Place (at which the verification was signed) .......... *Delete, if not applicable.

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 7
FORM K‐1 [See rule 62(1)]
Application under Sub‐Section (1) of Section 33c of The Industrial Disputes Act, 1947
To 1) The Secretary to the Government of India, Ministry of Labour and Employment, New Delhi. 2) The Regional Labour Commissioner (Central),....................... (here insert the name of the region).
Sir, I/We have to state that I am/we are entitled to receive from M/s...........................a sum of Rs. ............. on account of ................ under the provisions of Chapter VA/Chapter VB of the Industrial Disputes Act, 1947/in terms of the award dated the..................... given by...................../in terms of the settlement dated the .....................arrived at between the said M/s ......................... and their workmen through........................... the duly elected representatives. I/We further state that I/we served the management with a demand notice by registered post on ..................... for the said amount which the management has neither paid nor offered to pay to me/us even though a fortnight has since elapsed. The details of the amount have been mentioned in the statement hereto annexed. I/We request that the said sum may kindly be recovered for the management under sub‐section (1) of section 33C of the Industrial Disputes Act, 1947, and paid to me/us as early as possible. Signature of the applicant(s) Address(es) 1. 2. 3 4.
Station:……………………………………………….. Date: ………………………………………………..
ANNEXURE (Here indicate the details of the amount(s) claimed.)]
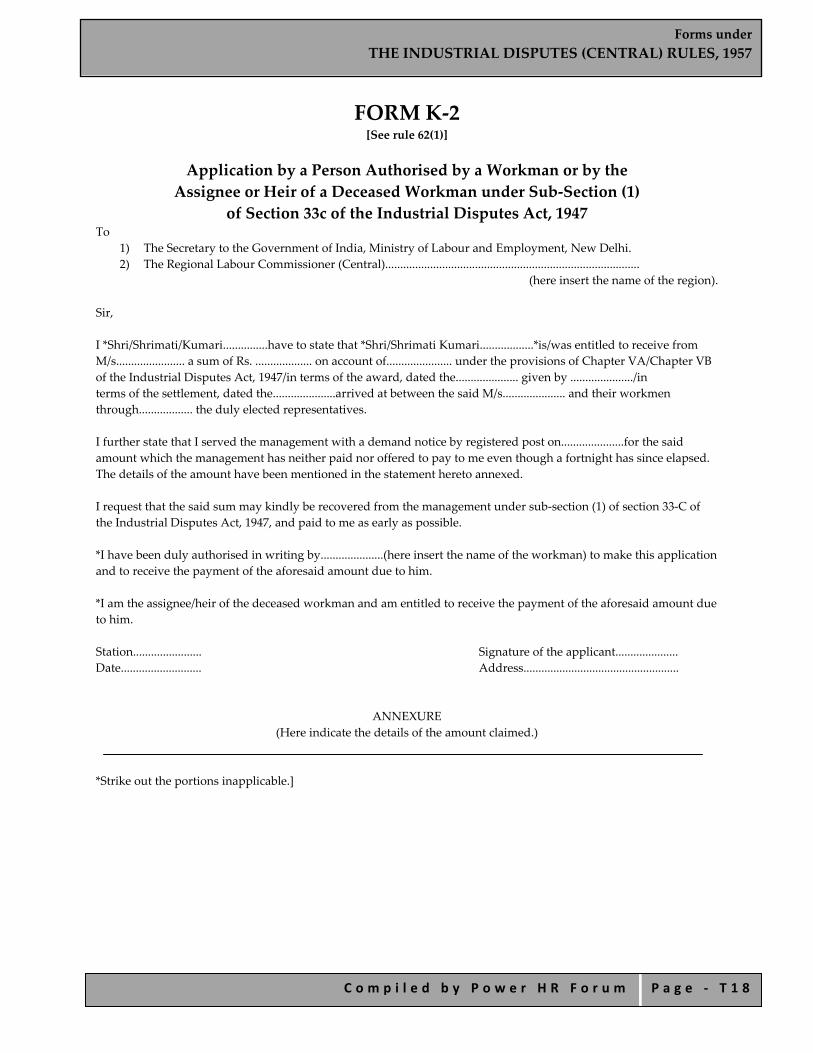
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 8
FORM K‐2 [See rule 62(1)]
Application by a Person Authorised by a Workman or by the Assignee or Heir of a Deceased Workman under Sub‐Section (1)
of Section 33c of the Industrial Disputes Act, 1947 To
1) The Secretary to the Government of India, Ministry of Labour and Employment, New Delhi. 2) The Regional Labour Commissioner (Central).....................................................................................
(here insert the name of the region).
Sir, I *Shri/Shrimati/Kumari...............have to state that *Shri/Shrimati Kumari..................*is/was entitled to receive from M/s....................... a sum of Rs. ................... on account of...................... under the provisions of Chapter VA/Chapter VB of the Industrial Disputes Act, 1947/in terms of the award, dated the..................... given by ...................../in terms of the settlement, dated the.....................arrived at between the said M/s..................... and their workmen through.................. the duly elected representatives. I further state that I served the management with a demand notice by registered post on.....................for the said amount which the management has neither paid nor offered to pay to me even though a fortnight has since elapsed. The details of the amount have been mentioned in the statement hereto annexed. I request that the said sum may kindly be recovered from the management under sub‐section (1) of section 33‐C of the Industrial Disputes Act, 1947, and paid to me as early as possible. *I have been duly authorised in writing by.....................(here insert the name of the workman) to make this application and to receive the payment of the aforesaid amount due to him. *I am the assignee/heir of the deceased workman and am entitled to receive the payment of the aforesaid amount due to him. Station....................... Signature of the applicant..................... Date........................... Address....................................................
ANNEXURE
(Here indicate the details of the amount claimed.) *Strike out the portions inapplicable.]
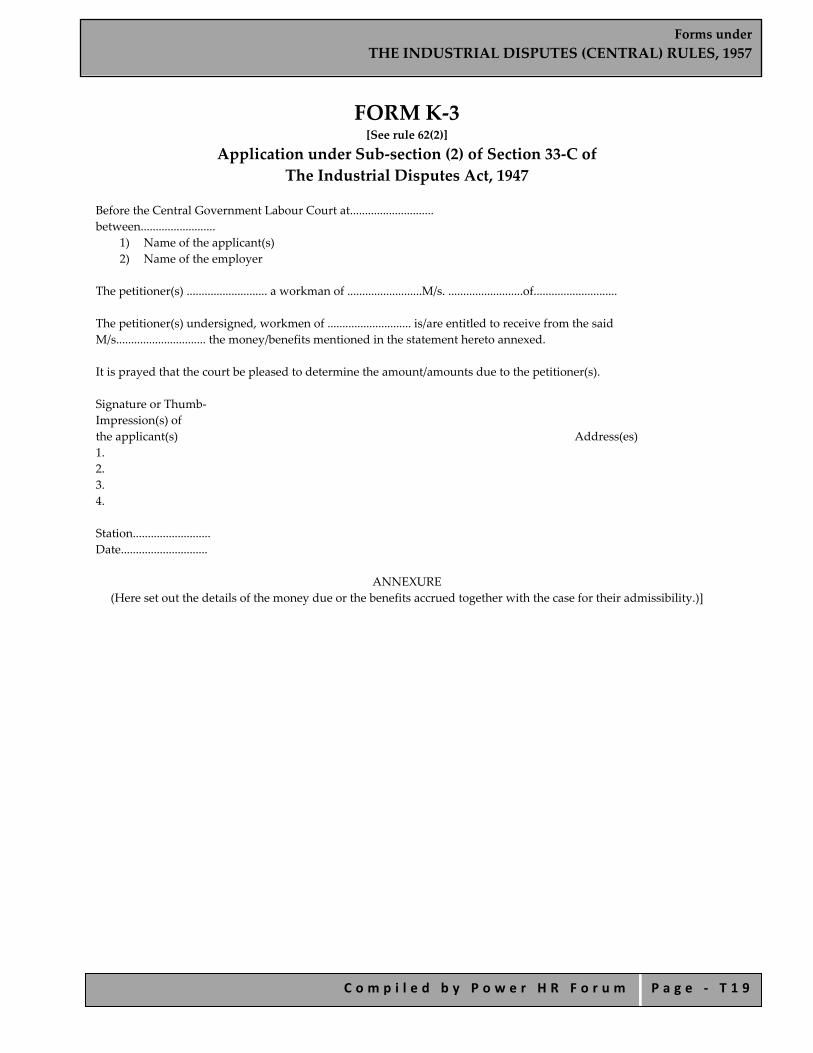
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 1 9
FORM K‐3 [See rule 62(2)]
Application under Sub‐section (2) of Section 33‐C of The Industrial Disputes Act, 1947
Before the Central Government Labour Court at............................ between.........................
1) Name of the applicant(s) 2) Name of the employer
The petitioner(s) ........................... a workman of .........................M/s. .........................of............................ The petitioner(s) undersigned, workmen of ............................ is/are entitled to receive from the said M/s.............................. the money/benefits mentioned in the statement hereto annexed. It is prayed that the court be pleased to determine the amount/amounts due to the petitioner(s). Signature or Thumb‐ Impression(s) of the applicant(s) Address(es) 1. 2. 3. 4. Station.......................... Date.............................
ANNEXURE (Here set out the details of the money due or the benefits accrued together with the case for their admissibility.)]
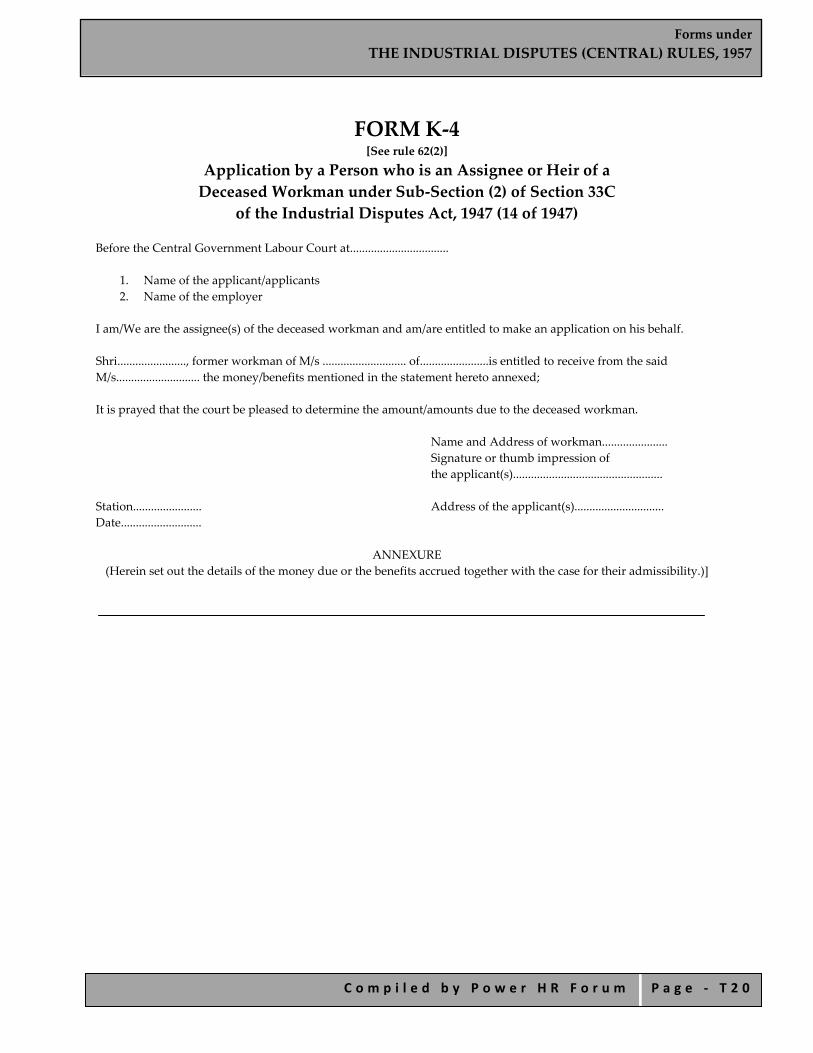
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 0
FORM K‐4 [See rule 62(2)]
Application by a Person who is an Assignee or Heir of a Deceased Workman under Sub‐Section (2) of Section 33C
of the Industrial Disputes Act, 1947 (14 of 1947)
Before the Central Government Labour Court at.................................
1. Name of the applicant/applicants 2. Name of the employer
I am/We are the assignee(s) of the deceased workman and am/are entitled to make an application on his behalf. Shri......................., former workman of M/s ............................ of.......................is entitled to receive from the said M/s............................ the money/benefits mentioned in the statement hereto annexed; It is prayed that the court be pleased to determine the amount/amounts due to the deceased workman.
Name and Address of workman...................... Signature or thumb impression of the applicant(s)..................................................
Station....................... Address of the applicant(s).............................. Date...........................
ANNEXURE (Herein set out the details of the money due or the benefits accrued together with the case for their admissibility.)]

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 1
FORM L (See rule 71)
Form of Notice of Strike to be given by [Union/Workmen] in Public Utility Service
(Name of Union)
[Names of five elected representatives of workmen.] Dated the......day of......20......
(The name of the employer). Dear Sir/Sirs, In accordance with the provisions contained in sub‐section (1) of section 22 of the Industrial Disputes Act, 1947 —— I/We——————————————— hereby give you notice that ————————————— on.................20....., for the reasons explained in the annexure. Yours faithfully, Secretary of the Union [Five representatives of the workmen duly elected at a meeting held on........................................... (date), vide resolution attached.]
ANNEXURE Statement of the Case. Copy to:
1. Assistant Labour Commissioner (Central)................................................................ (Here enter office address of the Assistant Labour Commissioner (Central) in the local area concerned.)
2. Regional Labour Commissioner (Central).............Zone. 3. Chief Labour Commissioner (Central), New Delhi.
I propose to call a strike
We propose to go on strike
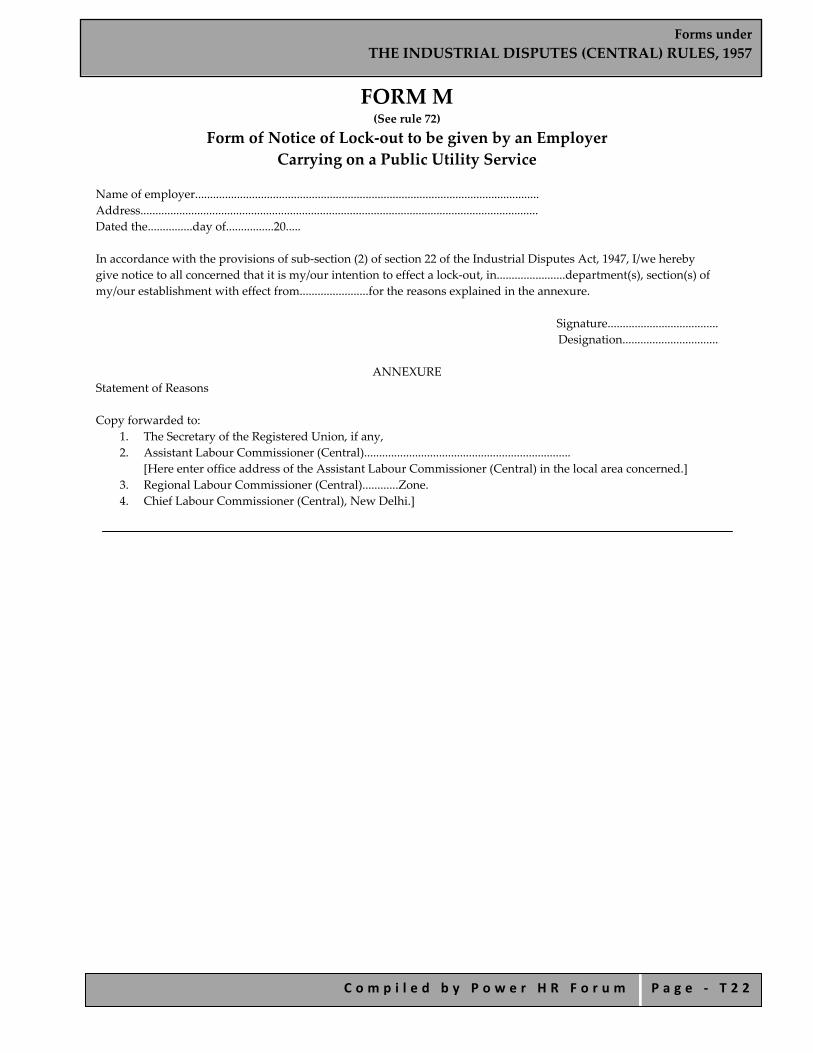
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 2
FORM M (See rule 72)
Form of Notice of Lock‐out to be given by an Employer Carrying on a Public Utility Service
Name of employer................................................................................................................... Address..................................................................................................................................... Dated the...............day of................20..... In accordance with the provisions of sub‐section (2) of section 22 of the Industrial Disputes Act, 1947, I/we hereby give notice to all concerned that it is my/our intention to effect a lock‐out, in.......................department(s), section(s) of my/our establishment with effect from.......................for the reasons explained in the annexure.
Signature..................................... Designation................................
ANNEXURE
Statement of Reasons
Copy forwarded to: 1. The Secretary of the Registered Union, if any, 2. Assistant Labour Commissioner (Central).....................................................................
[Here enter office address of the Assistant Labour Commissioner (Central) in the local area concerned.] 3. Regional Labour Commissioner (Central)............Zone. 4. Chief Labour Commissioner (Central), New Delhi.]

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 3
FORM N (See rule 73)
Form of Report of Strike or Lock‐out in a Public Utility Service Information to be supplied in this form immediately on the occurrence of a strike or lock‐out in a public utility service to the
Assistant Labour Commissioner (Central) for the local area concerned
Name of Undertaking
Station and District
Normal Working Strength
Number of workers involved
Strike or lockout
Date of commencement of strike or lockout
Cause Was notice of strike or lockout given? If so, on what date for what period?
Is there any permanent agency or agreement in the undertaking for the settlement of disputes between the employer and the workmen? If any exists, particular thereof
Any other information
Directly Indirectly
1 2 3 4 5 6 7 8 9 10 11
Notes.— Column (3) Give the average number of workmen employed during the month previous to the day on which the strike or lock‐out occurred. While reckoning the average, omit the days on which the attendance was not normal for reasons other than individual reasons of particular workmen. Thus days on which strike or lock‐out occurs or communal holiday is enjoyed by a large section of workers should be omitted. Column (4) If, say, 200 workers in a factory strike work and in consequence the whole factory employing 1,000 workers has to be closed than, 200 should be shown under “directly” and the remaining under “indirectly”. If the strike of 200 workers does not affect the working of the other departments of the factory, the number of workers involved would only be 200, which figure should appear under “directly” and column “indirectly” would be blank. Column (8) Give the main causes of the dispute as well as the immediate cause that led to the strike or lock‐out.

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 4
FORM O (See rule 75)
Register of Settlements Register ‐ PART I
Serial No. Industry Parties to the
Settlement Date of settlement Remarks*
*Whether the settlement was effected at the intervention of the conciliation machinery, or by mutual negotiations between the parties, may be indicated here.
PART II Should contain one copy each of the settlements in the serial order indicated in Part I.
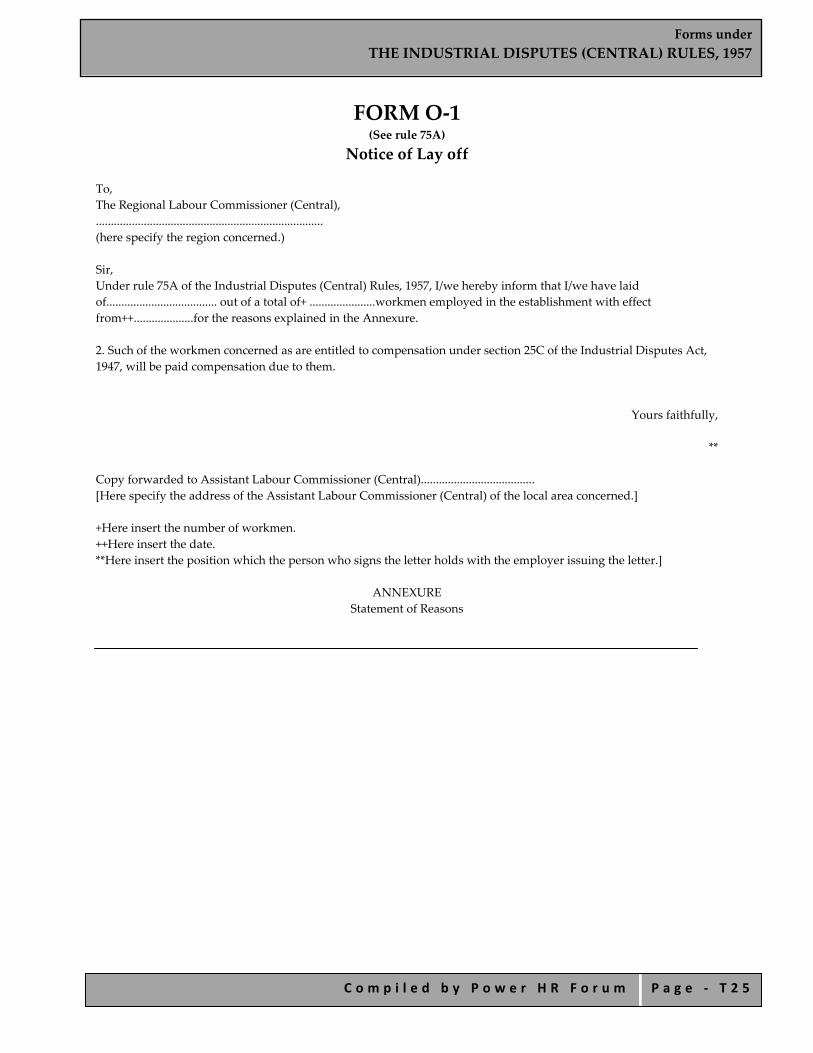
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 5
FORM O‐1 (See rule 75A)
Notice of Lay off To, The Regional Labour Commissioner (Central), ............................................................................ (here specify the region concerned.) Sir, Under rule 75A of the Industrial Disputes (Central) Rules, 1957, I/we hereby inform that I/we have laid of..................................... out of a total of+ ......................workmen employed in the establishment with effect from++....................for the reasons explained in the Annexure. 2. Such of the workmen concerned as are entitled to compensation under section 25C of the Industrial Disputes Act, 1947, will be paid compensation due to them.
Yours faithfully,
** Copy forwarded to Assistant Labour Commissioner (Central)...................................... [Here specify the address of the Assistant Labour Commissioner (Central) of the local area concerned.] +Here insert the number of workmen. ++Here insert the date. **Here insert the position which the person who signs the letter holds with the employer issuing the letter.]
ANNEXURE Statement of Reasons
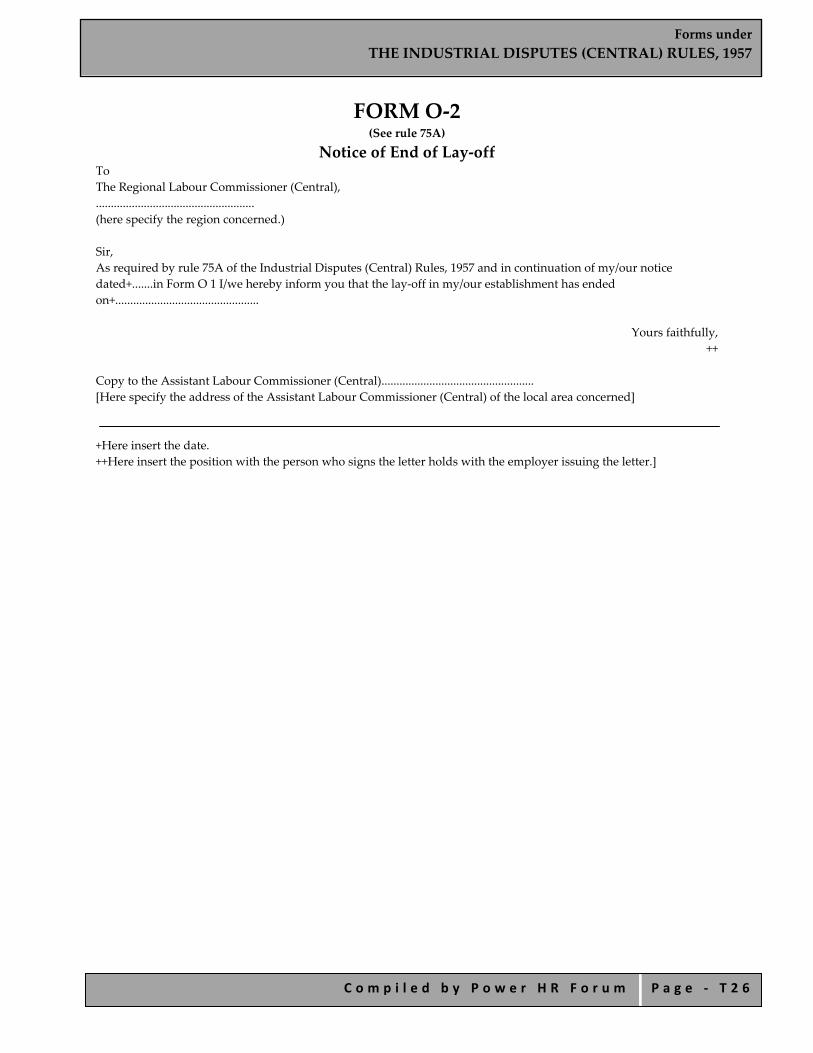
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 6
FORM O‐2 (See rule 75A)
Notice of End of Lay‐off To The Regional Labour Commissioner (Central), ..................................................... (here specify the region concerned.) Sir, As required by rule 75A of the Industrial Disputes (Central) Rules, 1957 and in continuation of my/our notice dated+.......in Form O 1 I/we hereby inform you that the lay‐off in my/our establishment has ended on+................................................
Yours faithfully, ++
Copy to the Assistant Labour Commissioner (Central)................................................... [Here specify the address of the Assistant Labour Commissioner (Central) of the local area concerned]
+Here insert the date. ++Here insert the position with the person who signs the letter holds with the employer issuing the letter.]
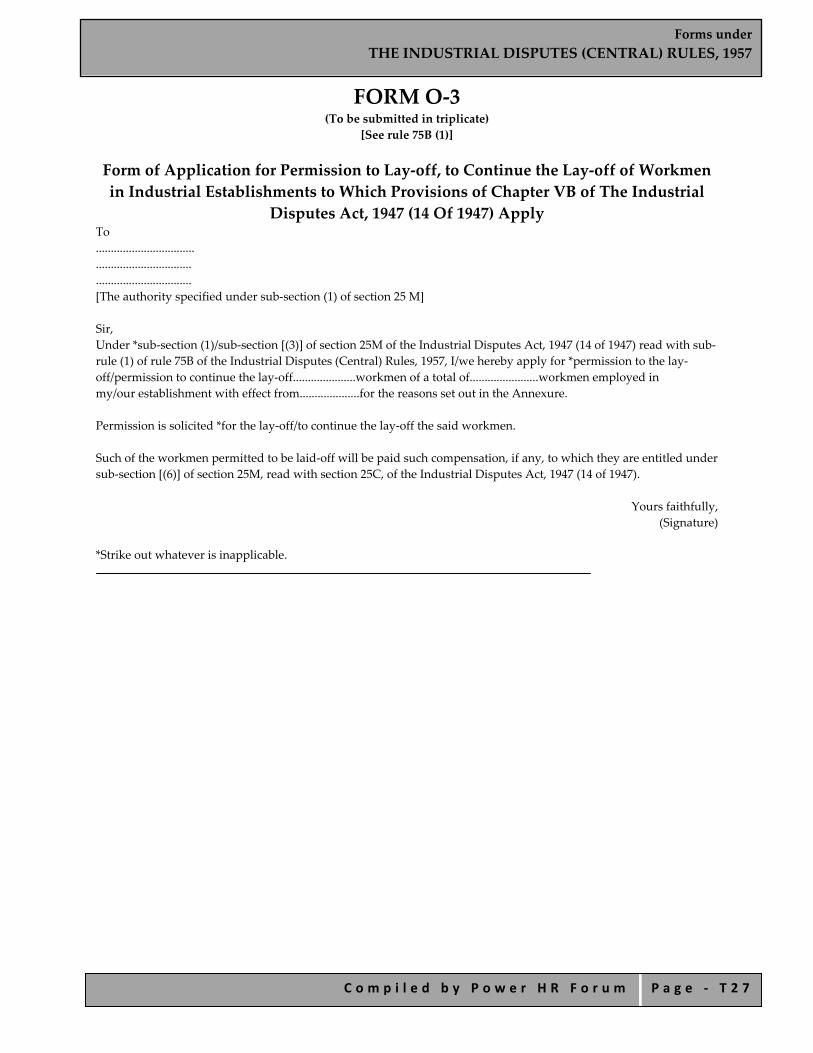
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 7
FORM O‐3 (To be submitted in triplicate)
[See rule 75B (1)]
Form of Application for Permission to Lay‐off, to Continue the Lay‐off of Workmen in Industrial Establishments to Which Provisions of Chapter VB of The Industrial
Disputes Act, 1947 (14 Of 1947) Apply To ................................. ................................ ................................ [The authority specified under sub‐section (1) of section 25 M] Sir, Under *sub‐section (1)/sub‐section [(3)] of section 25M of the Industrial Disputes Act, 1947 (14 of 1947) read with sub‐rule (1) of rule 75B of the Industrial Disputes (Central) Rules, 1957, I/we hereby apply for *permission to the lay‐off/permission to continue the lay‐off.....................workmen of a total of.......................workmen employed in my/our establishment with effect from....................for the reasons set out in the Annexure. Permission is solicited *for the lay‐off/to continue the lay‐off the said workmen. Such of the workmen permitted to be laid‐off will be paid such compensation, if any, to which they are entitled under sub‐section [(6)] of section 25M, read with section 25C, of the Industrial Disputes Act, 1947 (14 of 1947).
Yours faithfully, (Signature)
*Strike out whatever is inapplicable.
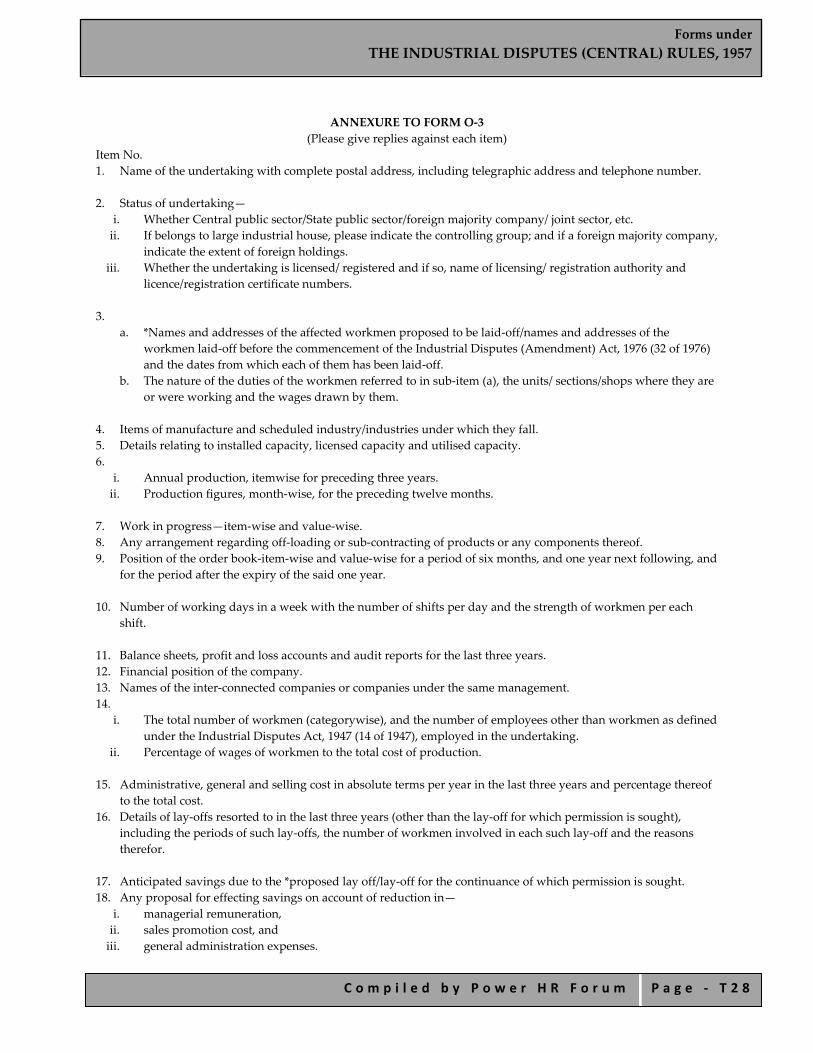
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 8
ANNEXURE TO FORM O‐3 (Please give replies against each item)
Item No. 1. Name of the undertaking with complete postal address, including telegraphic address and telephone number. 2. Status of undertaking—
i. Whether Central public sector/State public sector/foreign majority company/ joint sector, etc. ii. If belongs to large industrial house, please indicate the controlling group; and if a foreign majority company,
indicate the extent of foreign holdings. iii. Whether the undertaking is licensed/ registered and if so, name of licensing/ registration authority and
licence/registration certificate numbers. 3.
a. *Names and addresses of the affected workmen proposed to be laid‐off/names and addresses of the workmen laid‐off before the commencement of the Industrial Disputes (Amendment) Act, 1976 (32 of 1976) and the dates from which each of them has been laid‐off.
b. The nature of the duties of the workmen referred to in sub‐item (a), the units/ sections/shops where they are or were working and the wages drawn by them.
4. Items of manufacture and scheduled industry/industries under which they fall. 5. Details relating to installed capacity, licensed capacity and utilised capacity. 6.
i. Annual production, itemwise for preceding three years. ii. Production figures, month‐wise, for the preceding twelve months.
7. Work in progress—item‐wise and value‐wise. 8. Any arrangement regarding off‐loading or sub‐contracting of products or any components thereof. 9. Position of the order book‐item‐wise and value‐wise for a period of six months, and one year next following, and
for the period after the expiry of the said one year.
10. Number of working days in a week with the number of shifts per day and the strength of workmen per each shift.
11. Balance sheets, profit and loss accounts and audit reports for the last three years. 12. Financial position of the company. 13. Names of the inter‐connected companies or companies under the same management. 14.
i. The total number of workmen (categorywise), and the number of employees other than workmen as defined under the Industrial Disputes Act, 1947 (14 of 1947), employed in the undertaking.
ii. Percentage of wages of workmen to the total cost of production. 15. Administrative, general and selling cost in absolute terms per year in the last three years and percentage thereof
to the total cost. 16. Details of lay‐offs resorted to in the last three years (other than the lay‐off for which permission is sought),
including the periods of such lay‐offs, the number of workmen involved in each such lay‐off and the reasons therefor.
17. Anticipated savings due to the *proposed lay off/lay‐off for the continuance of which permission is sought. 18. Any proposal for effecting savings on account of reduction in—
i. managerial remuneration, ii. sales promotion cost, and iii. general administration expenses.

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 2 9
19. Position of stocks on last day of each of the months in the preceding twelve months. 20. Annual sales figures for the last three years and month‐wise sales figures for the preceding twelve months both
item‐wise and value‐wise. 21. Reasons for the *proposed lay‐off/lay‐off for the continuance of which permission is sought. 22. Any specific attempts made so far to avoid the *proposed lay‐off/lay‐off for the continuance of which permission
is sought. 23. Any other relevant factors with details thereof. *Strike out whatever is inapplicable.]

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 3 0
FORM P (See rule 76)
Form of Notice of Retrenchment to be given by an Employer under Clause (C) of Section 25f of
Industrial Disputes Act, 1947 Name of employer............................... Address.................................................... Dated .............. day of..............20........ To, The Secretary to the Government of India, Ministry of Labour, New Delhi Sir, Under clause (c) of section 25F of the Industrial Disputes Act, 1947 (14 of 1947), I/we hereby inform you that I/we have decided to retrench*...................... workmen with effect from**........................ for the reasons explained in the Annexure. 2. +The workmen concerned were given on the.**........ 20......one month’s notice in writing as required under clause (a) of section 25F of the Act. Retrenchment is being effected in pursuance of an agreement, a copy of which is enclosed. The workmen were given on the ** ................... 20 ...... one monthʹs pay in lieu of notice as required under clause (a) of section 25‐F of that Act. 3. The total number of workmen employed in the industrial establishment is*** ......... and the total number of those who will be affected by the retrenchment is given below: Category and designation of workmen to be retrenched
Number of workmen Employed To be retrenched
1 2 3 4. I/We hereby declare that the workman/workmen concerned has/have been/will be paid compensation due to them under section 25F of the Act on **........................./the expiry of the notice period.
Yours faithfully,
++ *Here insert the number of workmen. **Here insert the date. +Delete the portion which is not applicable. ***Here insert the total number of workmen employed in the industrial establishment. ++Here insert the position which the person who signs this letter holds with the employer issuing the letter.
ANNEXURE Statement of Reasons
Copy to : 1. Assistant Labour Commissioner (Central). ............................................................
[Here enter office address of the Assistant Labour Commissioner (Central) in local area concerned.] 2. Regional Labour Commissioner (Central)……………………………….Zone 3. Employment Officer, Employment Exchange........................................................... (Enter the full address of the
Employment Exchange concerned.)]
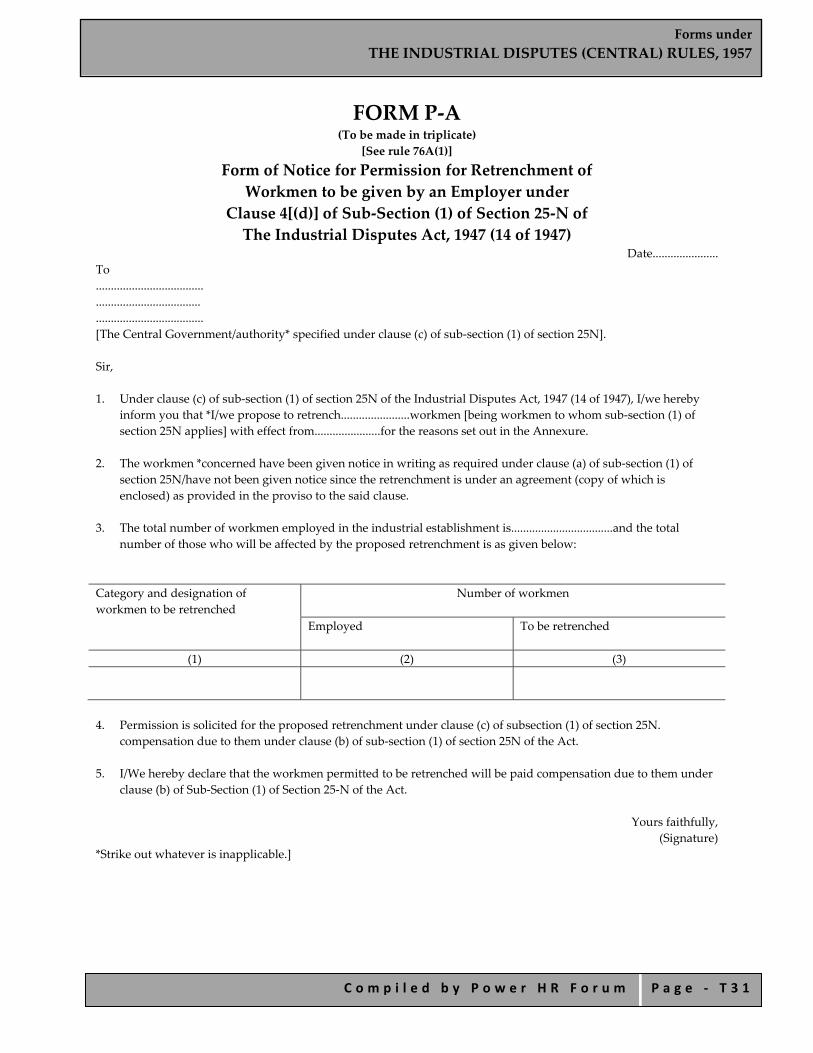
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 3 1
FORM P‐A (To be made in triplicate)
[See rule 76A(1)]
Form of Notice for Permission for Retrenchment of Workmen to be given by an Employer under
Clause 4[(d)] of Sub‐Section (1) of Section 25‐N of The Industrial Disputes Act, 1947 (14 of 1947)
Date...................... To .................................... ................................... .................................... [The Central Government/authority* specified under clause (c) of sub‐section (1) of section 25N]. Sir, 1. Under clause (c) of sub‐section (1) of section 25N of the Industrial Disputes Act, 1947 (14 of 1947), I/we hereby
inform you that *I/we propose to retrench.......................workmen [being workmen to whom sub‐section (1) of section 25N applies] with effect from......................for the reasons set out in the Annexure.
2. The workmen *concerned have been given notice in writing as required under clause (a) of sub‐section (1) of
section 25N/have not been given notice since the retrenchment is under an agreement (copy of which is enclosed) as provided in the proviso to the said clause.
3. The total number of workmen employed in the industrial establishment is..................................and the total
number of those who will be affected by the proposed retrenchment is as given below: Category and designation of workmen to be retrenched
Number of workmen Employed To be retrenched
(1) (2) (3)
4. Permission is solicited for the proposed retrenchment under clause (c) of subsection (1) of section 25N.
compensation due to them under clause (b) of sub‐section (1) of section 25N of the Act. 5. I/We hereby declare that the workmen permitted to be retrenched will be paid compensation due to them under
clause (b) of Sub‐Section (1) of Section 25‐N of the Act.
Yours faithfully, (Signature)
*Strike out whatever is inapplicable.]

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 3 2
ANNEXURE TO FPRM P‐A (Please give replies against each item)
Item No. 1. Name of the undertaking with complete postal address, including telegraphic addresses and telephone number. 2. Status of undertaking—
i. Whether Central public sector/State public sector / foreign majority company/joint sector, etc. ii. If belongs to large industrial house, please indicate the controlling group; and if a foreign majority company,
indicate the extent of foreign holdings. iii. Whether the undertaking is licensed/ registered and if so, name of licensing/registration authority and
licence registration certificate numbers. 3. Names and addresses of the workmen proposed to be retrenched and the nature of the duties, the
units/sections/shops where they are working and the wages drawn by them. 4. Items of manufacture and scheduled industry/industries under which they fall. 5. Details relating to installed capacity licensed capacity and the utilised capacity. 6.
i. Annual production, item‐wise for preceding three years. ii. Production figures month‐wise for preceding twelve months.
7. Work in progress—item‐wise and valuewise. 8. Any arrangement regarding off‐loading or sub‐contracting of products or any components thereof. 9. Position of the order book—item‐wise and value‐wise for a period of six months and one year next following,
and for the period after the expiry of the said one year. 10. Number of working days in a week with number of shifts per day and strength of workmen per each shift. 11. Balance sheet; profit and loss account and audit reports for the last three years. 12. Financial position of the company. 13. Names of the inter‐connected companies or companies under the same management. 14.
i. The total number of workmen (category‐wise), and the number of employees other than workmen as defined in the Industrial Disputes Act, 1947 (14 of 1947), employed in the undertaking.
ii. Percentage of wages of workmen to the total cost of production. 15. Administrative, general and selling cost in absolute terms per year for the last three years and percentage thereof
to the total costs. 16. Details of retrenchment resorted to in the last three years, including dates of retrenchment, the number of
workmen involved in each case, and the reasons therefor. 17. Has any of the retrenched workmen been given re‐employment and if so, when? Give details. 18. Are seniority lists maintained in respect of the categories of workmen proposed to be retrenched and if so, the
details and the position of the workmen affected indicating their length of service including broken periods of service?
19. Anticipated savings due to the proposed retrenchment. 20. Any proposal for effecting savings on account of reduction in—
i. managerial remuneration, ii. sales promotion cost, and iii. general administration expenses.
21. Position of stocks on the last day of each of the month in the preceding twelve months. 22. Annual sales figures for the last three years and month‐wise sales figures—for the preceding twelve months both
item‐wise and value‐wise. 23. Reasons for the proposed retrenchment. 24. Any specific attempt made so far to avoid the proposed retrenchment. 25. Any other relevant factors with details thereof.

Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 3 3
FORM Q (See rule 76A)
Form of Notice of Closure to be given by an Employer Under Section 25ffa of the Industrial Disputes
Act, 1947 (14 of 1947)
Name of employer......................................... Address........................................................ Dated the....... day of......20..... To
The Secretary to the Government of India, Department of Labour and Employment, New Delhi.
Sir, Under section 25FFA of the Industrial Disputes Act, 1947 (14 of 1947), I/we* hereby inform you that I/we have decided to close down.........................(name of the undertaking) with effect from.....................for the reasons explained in the annexure. The number of workmen whose services would be terminated on account of the closure of the undertaking is................. (number of workmen).
Yours faithfully,
*(Here insert the position which the person who signs this letter holds with the employer issuing this letter.)
ANNEXURE Statement of reasons
Copy to:
1) The Regional Labour Commissioner (Central)*......................................................... 2) The Assistant Labour Commissioner (Central)*........................................................ 3) The Employment Exchange*.........................................................................................
*(Here enter the office address of the Regional Labour Commissioner (Central)/ Assistant Labour Commissioner (Central) and the Employment Exchange in the local area concerned).]
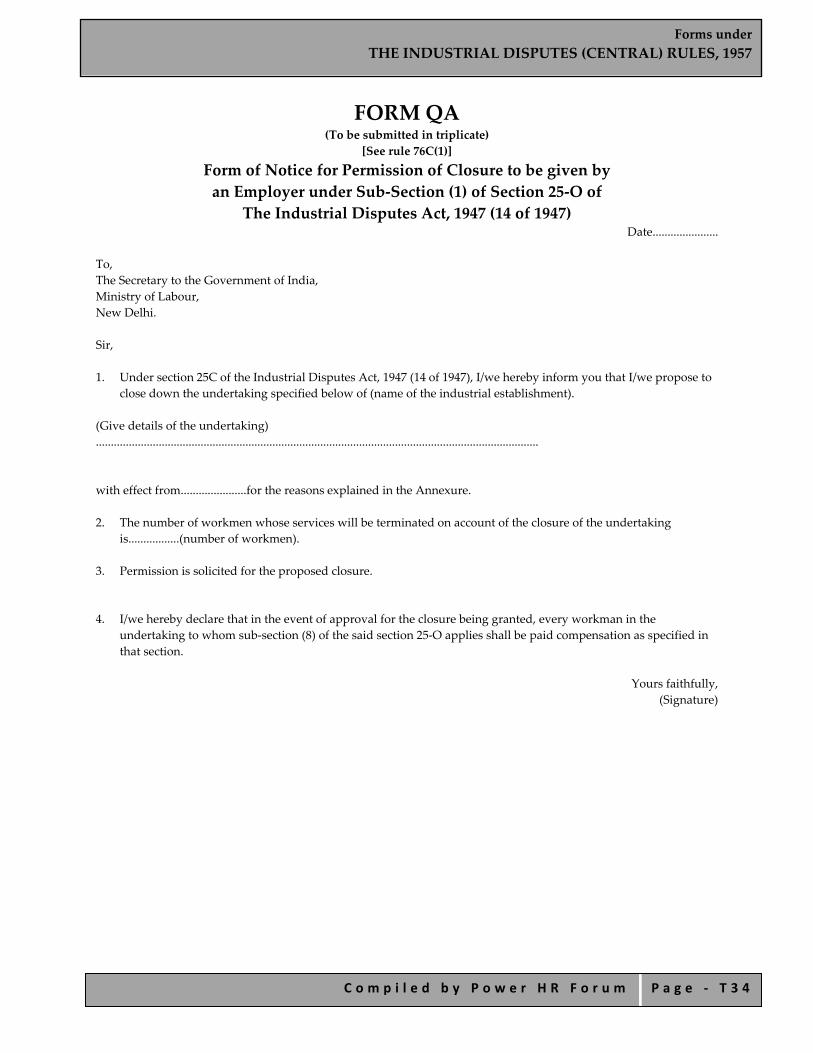
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 3 4
FORM QA (To be submitted in triplicate)
[See rule 76C(1)]
Form of Notice for Permission of Closure to be given by an Employer under Sub‐Section (1) of Section 25‐O of
The Industrial Disputes Act, 1947 (14 of 1947) Date......................
To, The Secretary to the Government of India, Ministry of Labour, New Delhi. Sir, 1. Under section 25C of the Industrial Disputes Act, 1947 (14 of 1947), I/we hereby inform you that I/we propose to
close down the undertaking specified below of (name of the industrial establishment). (Give details of the undertaking) .................................................................................................................................................... with effect from......................for the reasons explained in the Annexure. 2. The number of workmen whose services will be terminated on account of the closure of the undertaking
is.................(number of workmen). 3. Permission is solicited for the proposed closure.
4. I/we hereby declare that in the event of approval for the closure being granted, every workman in the undertaking to whom sub‐section (8) of the said section 25‐O applies shall be paid compensation as specified in that section.
Yours faithfully,
(Signature)
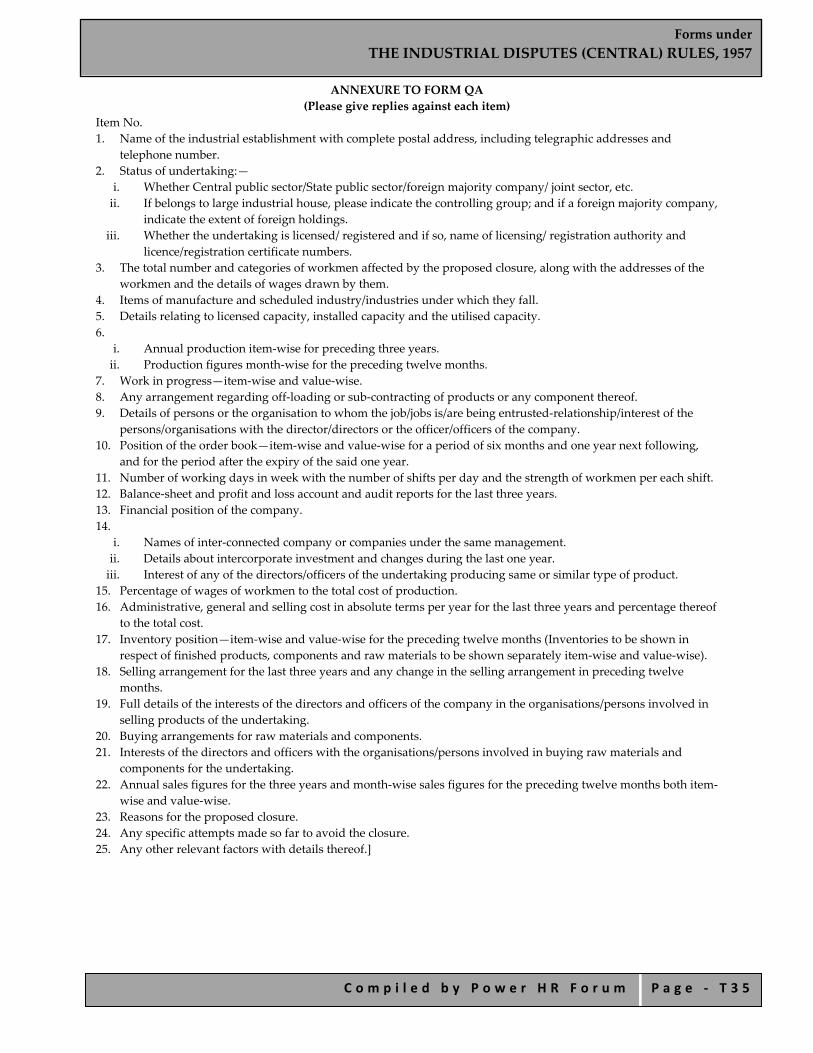
Forms under THE INDUSTRIAL DISPUTES (CENTRAL) RULES, 1957
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ T 3 5
ANNEXURE TO FORM QA (Please give replies against each item)
Item No. 1. Name of the industrial establishment with complete postal address, including telegraphic addresses and
telephone number. 2. Status of undertaking:—
i. Whether Central public sector/State public sector/foreign majority company/ joint sector, etc. ii. If belongs to large industrial house, please indicate the controlling group; and if a foreign majority company,
indicate the extent of foreign holdings. iii. Whether the undertaking is licensed/ registered and if so, name of licensing/ registration authority and
licence/registration certificate numbers. 3. The total number and categories of workmen affected by the proposed closure, along with the addresses of the
workmen and the details of wages drawn by them. 4. Items of manufacture and scheduled industry/industries under which they fall. 5. Details relating to licensed capacity, installed capacity and the utilised capacity. 6.
i. Annual production item‐wise for preceding three years. ii. Production figures month‐wise for the preceding twelve months.
7. Work in progress—item‐wise and value‐wise. 8. Any arrangement regarding off‐loading or sub‐contracting of products or any component thereof. 9. Details of persons or the organisation to whom the job/jobs is/are being entrusted‐relationship/interest of the
persons/organisations with the director/directors or the officer/officers of the company. 10. Position of the order book—item‐wise and value‐wise for a period of six months and one year next following,
and for the period after the expiry of the said one year. 11. Number of working days in week with the number of shifts per day and the strength of workmen per each shift. 12. Balance‐sheet and profit and loss account and audit reports for the last three years. 13. Financial position of the company. 14.
i. Names of inter‐connected company or companies under the same management. ii. Details about intercorporate investment and changes during the last one year. iii. Interest of any of the directors/officers of the undertaking producing same or similar type of product.
15. Percentage of wages of workmen to the total cost of production. 16. Administrative, general and selling cost in absolute terms per year for the last three years and percentage thereof
to the total cost. 17. Inventory position—item‐wise and value‐wise for the preceding twelve months (Inventories to be shown in
respect of finished products, components and raw materials to be shown separately item‐wise and value‐wise). 18. Selling arrangement for the last three years and any change in the selling arrangement in preceding twelve
months. 19. Full details of the interests of the directors and officers of the company in the organisations/persons involved in
selling products of the undertaking. 20. Buying arrangements for raw materials and components. 21. Interests of the directors and officers with the organisations/persons involved in buying raw materials and
components for the undertaking. 22. Annual sales figures for the three years and month‐wise sales figures for the preceding twelve months both item‐
wise and value‐wise. 23. Reasons for the proposed closure. 24. Any specific attempts made so far to avoid the closure. 25. Any other relevant factors with details thereof.]

Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 1
Forms under
CENTRAL TRADE UNION REGULATIONS, 1938

Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 2
INDEX
FORM A Application for Registration of Trade Union
FORM B Register of Trade Unions
FORM C
Certificate of Registration of Trade Union
FORM D
Annual Return Prescribed under Section 28 of The Indian Trade Unions Act, 1926,
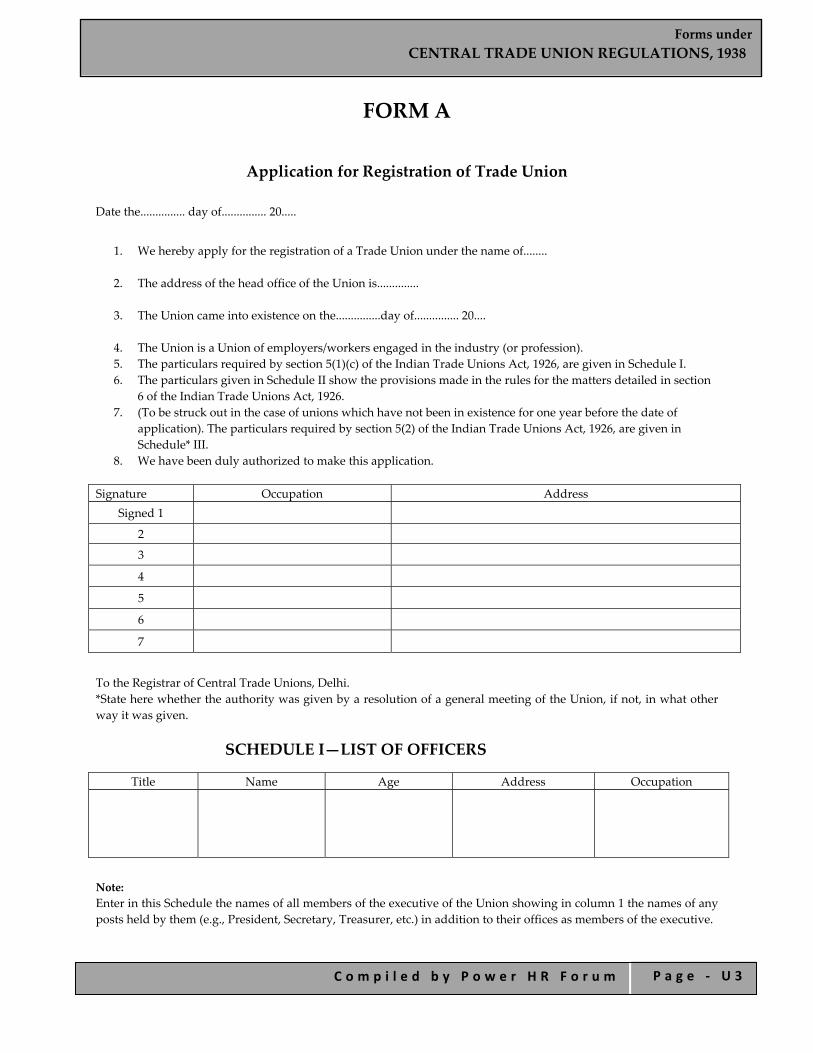
Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 3
FORM A
Application for Registration of Trade Union Date the............... day of............... 20.....
1. We hereby apply for the registration of a Trade Union under the name of........
2. The address of the head office of the Union is..............
3. The Union came into existence on the...............day of............... 20....
4. The Union is a Union of employers/workers engaged in the industry (or profession). 5. The particulars required by section 5(1)(c) of the Indian Trade Unions Act, 1926, are given in Schedule I. 6. The particulars given in Schedule II show the provisions made in the rules for the matters detailed in section
6 of the Indian Trade Unions Act, 1926. 7. (To be struck out in the case of unions which have not been in existence for one year before the date of
application). The particulars required by section 5(2) of the Indian Trade Unions Act, 1926, are given in Schedule* III.
8. We have been duly authorized to make this application. Signature Occupation Address
Signed 1
2
3
4
5
6
7
To the Registrar of Central Trade Unions, Delhi. *State here whether the authority was given by a resolution of a general meeting of the Union, if not, in what other way it was given.
SCHEDULE I—LIST OF OFFICERS
Title Name Age Address Occupation
Note: Enter in this Schedule the names of all members of the executive of the Union showing in column 1 the names of any posts held by them (e.g., President, Secretary, Treasurer, etc.) in addition to their offices as members of the executive.

Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 4
SCHEDULE II—REFERENCE TO RULES
The numbers of the rules‐making provision for the several matters detailed in column 1 are given in column 2 below:
Matter Number of rules Name of union
The whole of the objects for which the union has been established.
The whole of the purposes for which the general funds of the union shall be applicable.
The maintenance of a list of members.
The facilities provided for the inspection of the list of members by officers and members.
The admission of ordinary members.
The admission of honorary or temporary members.
The conditions under which members are entitled to benefit assured by the rules.
The conditions under which fines or forfeitures can be imposed or varied.
The manner in which the rule shall be amended, varied or rescinded.
The manner in which the members of the executive and the other officers of the union shall be appointed and removed.
The safe custody of the funds.
The annual audit of the accounts.
The facilities for the inspection of the account books by officers and members.
The manner in which the union may be dissolved.
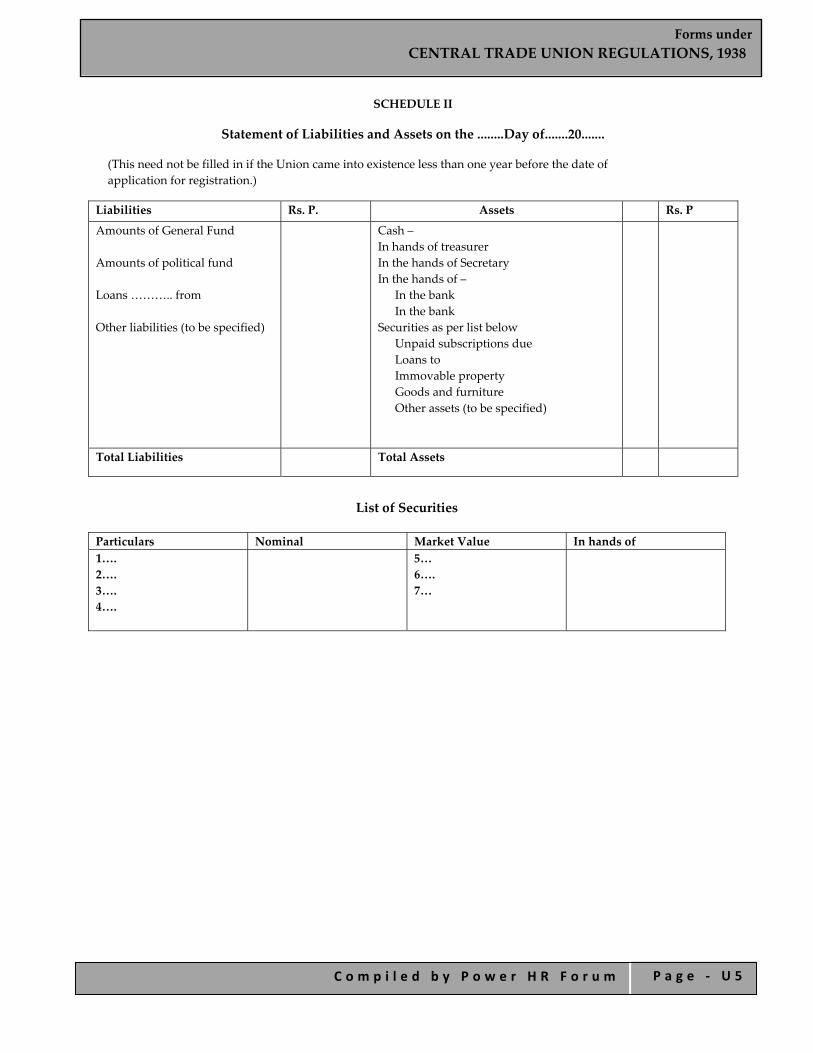
Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 5
SCHEDULE II
Statement of Liabilities and Assets on the ........Day of.......20.......
(This need not be filled in if the Union came into existence less than one year before the date of application for registration.)
Liabilities Rs. P. Assets Rs. P
Amounts of General Fund Amounts of political fund Loans ……….. from Other liabilities (to be specified)
Cash – In hands of treasurer In the hands of Secretary In the hands of –
In the bank In the bank
Securities as per list below Unpaid subscriptions due Loans to Immovable property Goods and furniture Other assets (to be specified)
Total Liabilities Total Assets
List of Securities
Particulars Nominal Market Value In hands of 1…. 2…. 3…. 4….
5…6…. 7…

Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 6
FORM B Register of Trade Unions
Serial No. Officers Name of Union
Address of Head Office
Date of Registration
Year of entering in office
Nam
e
Age of entry
Add
ress
Occup
ation
Year of relinqu
ishing
offic
e
Other offices held in
additio
n to m
embership
of executiv
e with date
Number of applications from List of members applying for registration
1. 2. 3. 4. 5. 6.

Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 7
FORM C Certificate of Registration of Trade Union
No.
It is hereby certified that the ............................. has been registered under the Indian Trade Unions Act, 1926, this............day of.............20.....
Seal
Registrar of Central Trade Unions
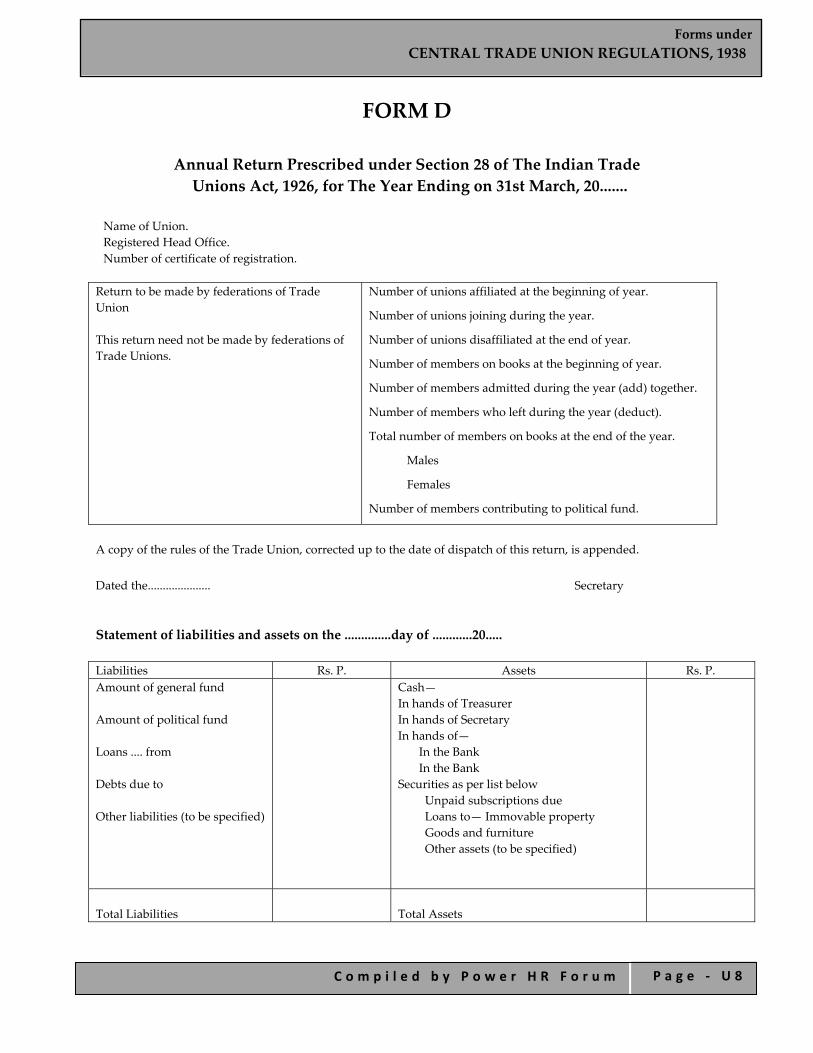
Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 8
FORM D
Annual Return Prescribed under Section 28 of The Indian Trade Unions Act, 1926, for The Year Ending on 31st March, 20.......
Name of Union. Registered Head Office. Number of certificate of registration.
Return to be made by federations of Trade Union This return need not be made by federations of Trade Unions.
Number of unions affiliated at the beginning of year.
Number of unions joining during the year.
Number of unions disaffiliated at the end of year.
Number of members on books at the beginning of year.
Number of members admitted during the year (add) together.
Number of members who left during the year (deduct).
Total number of members on books at the end of the year.
Males
Females
Number of members contributing to political fund.
A copy of the rules of the Trade Union, corrected up to the date of dispatch of this return, is appended. Dated the..................... Secretary Statement of liabilities and assets on the ..............day of ............20..... Liabilities Rs. P. Assets Rs. P. Amount of general fund Amount of political fund Loans .... from Debts due to Other liabilities (to be specified)
Cash— In hands of Treasurer In hands of Secretary In hands of—
In the Bank In the Bank
Securities as per list below Unpaid subscriptions due Loans to— Immovable property Goods and furniture Other assets (to be specified)
Total Liabilities
Total Assets
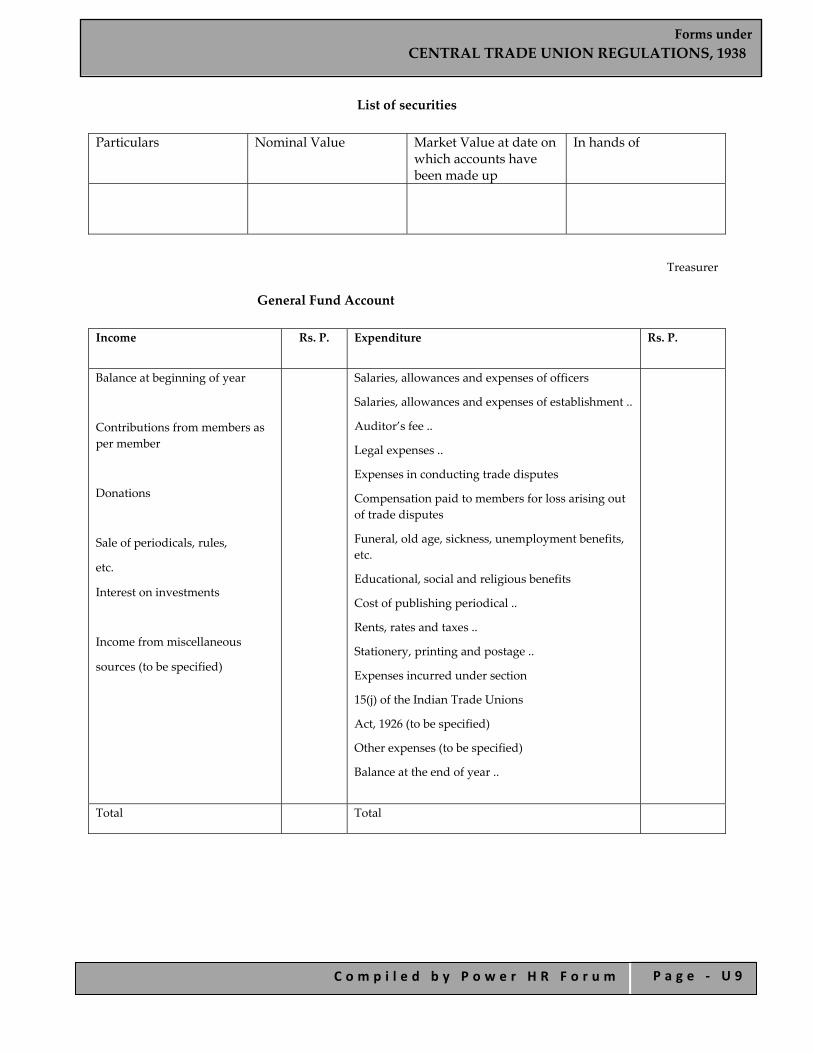
Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 9
List of securities Particulars Nominal Value Market Value at date on
which accounts have been made up
In hands of
Treasurer
General Fund Account Income Rs. P. Expenditure
Rs. P.
Balance at beginning of year
Contributions from members as per member
Donations
Sale of periodicals, rules,
etc.
Interest on investments
Income from miscellaneous
sources (to be specified)
Salaries, allowances and expenses of officers
Salaries, allowances and expenses of establishment ..
Auditor’s fee ..
Legal expenses ..
Expenses in conducting trade disputes
Compensation paid to members for loss arising out of trade disputes
Funeral, old age, sickness, unemployment benefits, etc.
Educational, social and religious benefits
Cost of publishing periodical ..
Rents, rates and taxes ..
Stationery, printing and postage ..
Expenses incurred under section
15(j) of the Indian Trade Unions
Act, 1926 (to be specified)
Other expenses (to be specified)
Balance at the end of year ..
Total Total

Forms under CENTRAL TRADE UNION REGULATIONS, 1938
C o m p i l e d b y P o w e r H R F o r u m P a g e ‐ U 1 0
Political Fund Account Income Rs. P. Expenditure
Rs. P.
Balance at beginning of year
Contribution from members as per member..
Total
Payments made on objects specified in section 16(2) of the Indian Trade Unions Act, 1926 (to be specified) ..
Expenses of managements (to be specified).
Balance at the end of year
Total
Auditor’s Declaration
The undersigned, having had access to all the books and accounts to the Trade Union and having examined the foregoing Statements and verified the same as found to be correct, duly vouched and in accordance with the law, subject to the remarks, if any, appended hereto.
Auditor.
The following changes of officers have been made during the year—
Officers Relinquishing Office Name Office Date of Relinquishing
Officers Appointed
Name Age Office Address Occupation Date of
appointment
Secretary

INDEX OF FORMS FOR REGISTRATION, CERTIFICATION & LICENSE
C o m p i l e d b y P o w e r H R F o r u m P a g e V 1
INDEX OF FORMS FOR REGISTRATION, CERTIFICATION & LICENSE
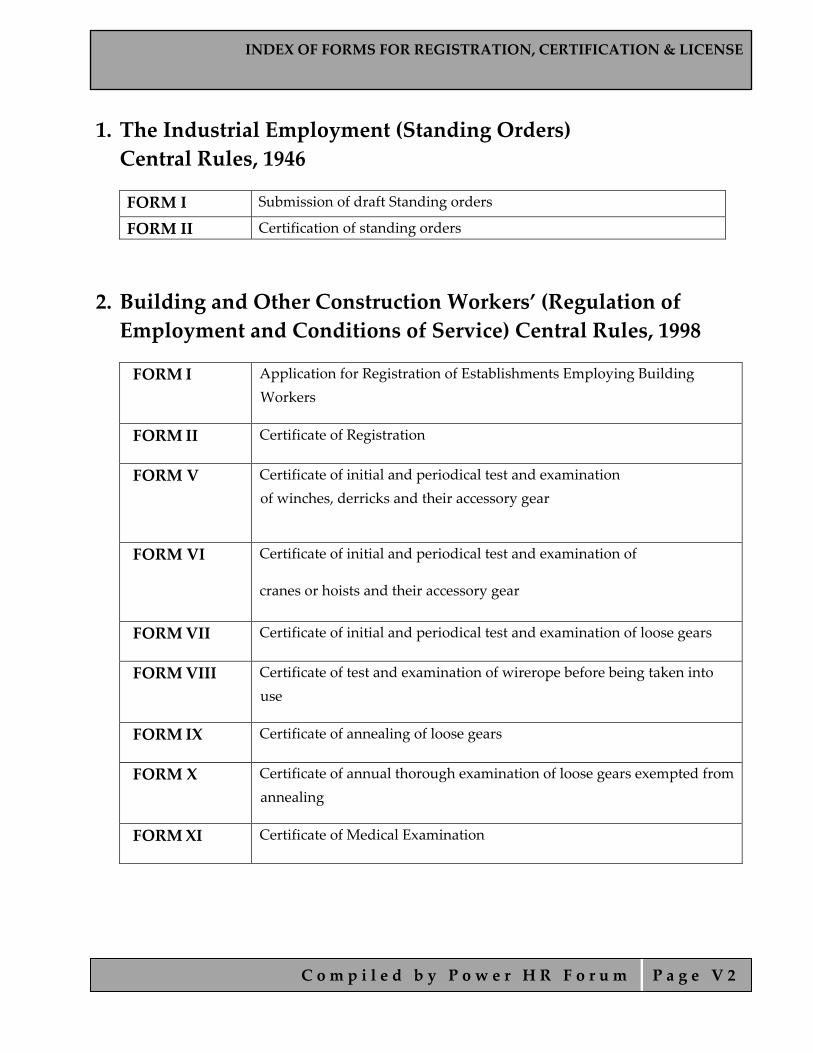
INDEX OF FORMS FOR REGISTRATION, CERTIFICATION & LICENSE
C o m p i l e d b y P o w e r H R F o r u m P a g e V 2
1. The Industrial Employment (Standing Orders) Central Rules, 1946
FORM I Submission of draft Standing orders
FORM II Certification of standing orders
2. Building and Other Construction Workers’ (Regulation of Employment and Conditions of Service) Central Rules, 1998
FORM I Application for Registration of Establishments Employing Building Workers
FORM II Certificate of Registration
FORM V
Certificate of initial and periodical test and examination of winches, derricks and their accessory gear
FORM VI
Certificate of initial and periodical test and examination of
cranes or hoists and their accessory gear
FORM VII Certificate of initial and periodical test and examination of loose gears
FORM VIII Certificate of test and examination of wirerope before being taken into use
FORM IX Certificate of annealing of loose gears
FORM X Certificate of annual thorough examination of loose gears exempted from annealing
FORM XI Certificate of Medical Examination

INDEX OF FORMS FOR REGISTRATION, CERTIFICATION & LICENSE
C o m p i l e d b y P o w e r H R F o r u m P a g e V 3
3. Contract Labor (Regulation and Abolition) Central Rules, 1971
FORM I Application for Registration of Establishments Employing Contract Labour
FORM II Certificate of Registration
FORM IV Application for Licence
FORM V Form of Certificate by Principal Employer
FORM VI License
FORM VII Application for Renewal of License
FORM VIII
Application for Temporary Registration of Establishment
Employing Contract Labour
FORM IX Temporary Certificate of Registration
FORM X Application for Temporary License
FORM XI License for a period of not more than fifteen days
4. Inter‐State Migrant Workmen (Regulation of Employment and Condition of Service) Central Rules, 1980
FORM I Application for registration of establishments employing migrant workmen
FORM II Certificate of registration
FORM IV Application for licence for recruitment
FORM V Application for licence for employment
FORM VI Form of certificate by principal employer
FORM VII Form of certificate by principal employer
FORM IX Application for renewal of licence
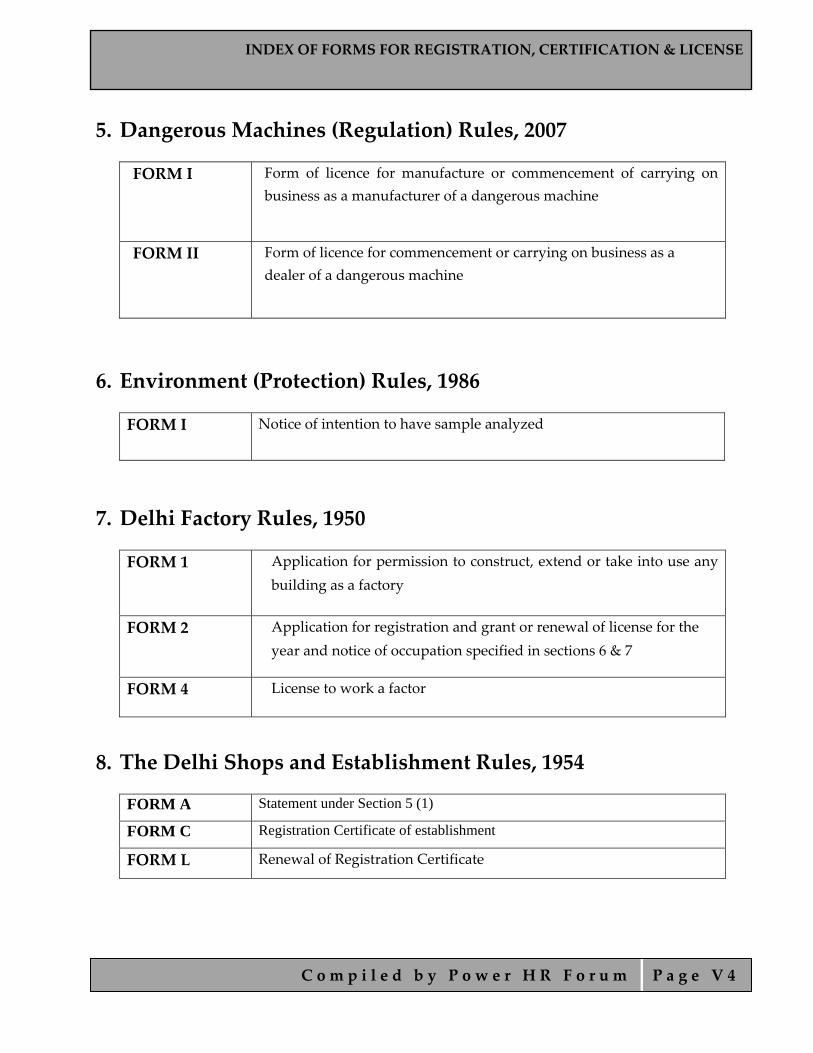
INDEX OF FORMS FOR REGISTRATION, CERTIFICATION & LICENSE
C o m p i l e d b y P o w e r H R F o r u m P a g e V 4
5. Dangerous Machines (Regulation) Rules, 2007
FORM I
Form of licence for manufacture or commencement of carrying on business as a manufacturer of a dangerous machine
FORM II
Form of licence for commencement or carrying on business as a dealer of a dangerous machine
6. Environment (Protection) Rules, 1986
FORM I
Notice of intention to have sample analyzed
7. Delhi Factory Rules, 1950
FORM 1
Application for permission to construct, extend or take into use any building as a factory
FORM 2 Application for registration and grant or renewal of license for the year and notice of occupation specified in sections 6 & 7
FORM 4 License to work a factor
8. The Delhi Shops and Establishment Rules, 1954
FORM A Statement under Section 5 (1)
FORM C Registration Certificate of establishment
FORM L Renewal of Registration Certificate
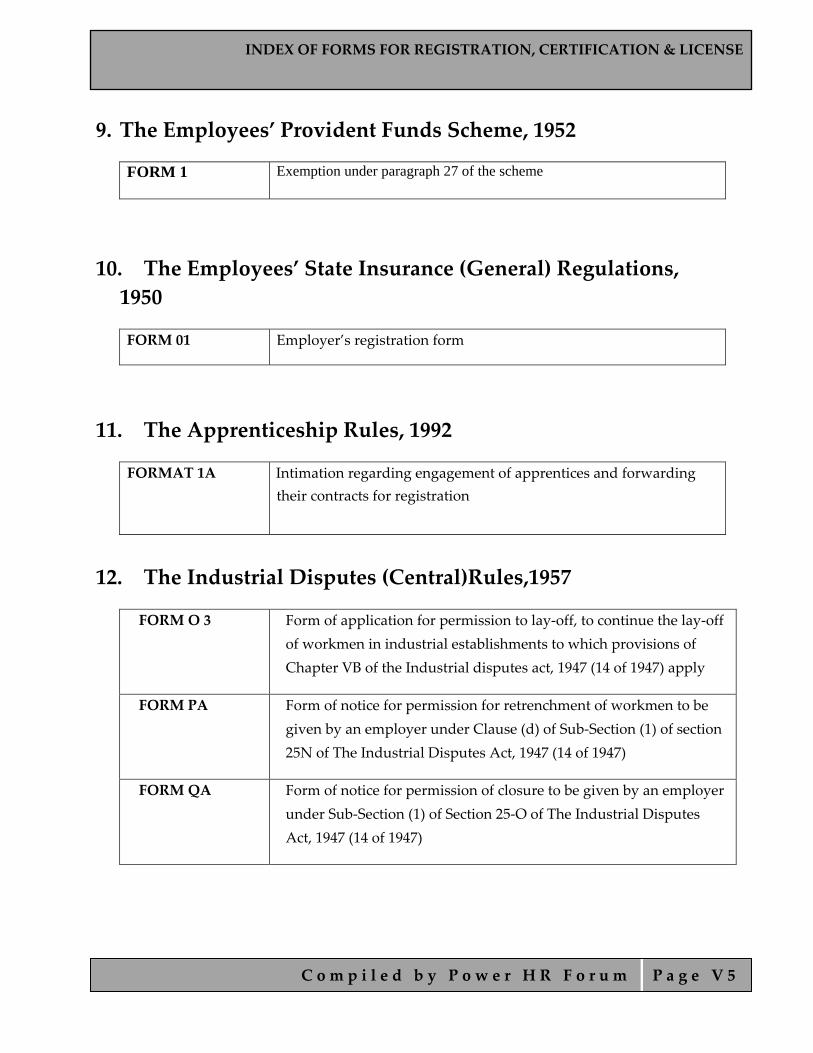
INDEX OF FORMS FOR REGISTRATION, CERTIFICATION & LICENSE
C o m p i l e d b y P o w e r H R F o r u m P a g e V 5
9. The Employees’ Provident Funds Scheme, 1952
FORM 1 Exemption under paragraph 27 of the scheme
10. The Employees’ State Insurance (General) Regulations, 1950
FORM 01 Employer’s registration form
11. The Apprenticeship Rules, 1992
FORMAT 1A
Intimation regarding engagement of apprentices and forwarding their contracts for registration
12. The Industrial Disputes (Central)Rules,1957
FORM O 3
Form of application for permission to lay‐off, to continue the lay‐off of workmen in industrial establishments to which provisions of Chapter VB of the Industrial disputes act, 1947 (14 of 1947) apply
FORM PA
Form of notice for permission for retrenchment of workmen to be given by an employer under Clause (d) of Sub‐Section (1) of section 25N of The Industrial Disputes Act, 1947 (14 of 1947)
FORM QA
Form of notice for permission of closure to be given by an employer under Sub‐Section (1) of Section 25‐O of The Industrial Disputes Act, 1947 (14 of 1947)

INDEX OF FORMS FOR MAINTAINING RESGISTERS AND RECORDS
C o m p i l e d b y P o w e r H R F o r u m P a g e W 1
INDEX OF FORMS FOR MAINTAINING REGISTERS AND RECORDS

INDEX OF FORMS FOR MAINTAINING RESGISTERS AND RECORDS
C o m p i l e d b y P o w e r H R F o r u m P a g e W 2
1. The Industrial Employment (Standing Orders) Central Rules, 1946
Form III Register under Section 8
2. Building and Other Construction Workers’ (Regulation of Employment and Conditions of Service) Central Rules, 1998
FORM III Register of Establishments
FORM XII Health Register
FORM XV Register of Building Workers Employed by the Employer
FORM XVI Muster‐Roll
FORM XVII Register of Wages
FORM XVIII Form of Register of Wages‐Cum‐Muster‐Roll
FORM XIX Register of deductions for damage or loss
FORM XX Register of fines
FORM XXI Register of Advances
FORM XXII Register of Overtime
FORM XXVI
Register of Periodical Test—Examination of Lifting
Appliance and Gears etc

INDEX OF FORMS FOR MAINTAINING RESGISTERS AND RECORDS
C o m p i l e d b y P o w e r H R F o r u m P a g e W 3
3. Contract Labor (Regulation and Abolition) Central Rules, 1971
FORM III Register of Establishments
FORM XII Register of Contractors
FORM XIII Register of Workmen Employed by Contractor
FORM XVI Muster roll
FORM XVII Register of Wages
FORM XVIII Form of Register of Wages‐cum‐Muster Roll
FORM XX Register of Deductions for Damage or Loss
FORM XXI Register of Fines
FORM XXII Register of Advances
FORM XXIII Register of Overtime
4. Inter‐State Migrant Workmen (Regulation of Employment and Condition of Service) Central Rules, 1980 FORM III Register of establishments
FORM XII Register of Contractors
FORM XIII Register of workmen employed by contractor
FORM XVII Muster roll
FORM XVIII Register of wages
FORM XIX Register of deduction for damage or loss
FORM XX Register of fines
FORM XXI Register of advances
FORM XXII Register of overtime
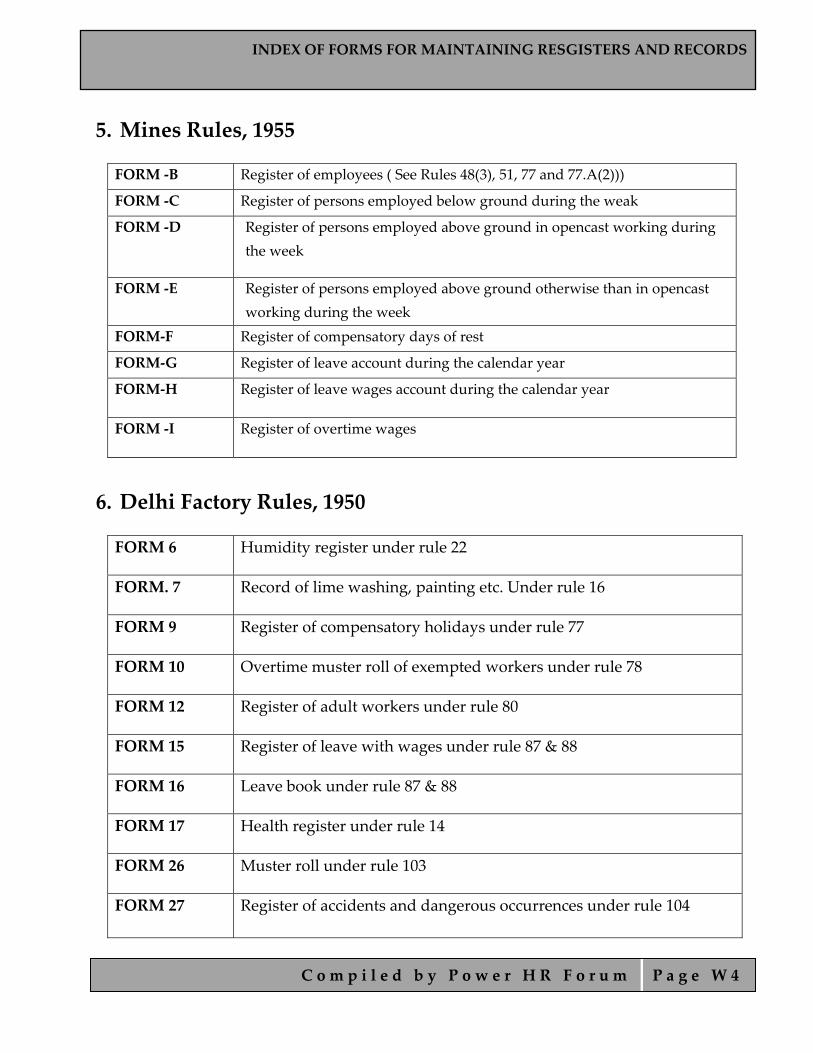
INDEX OF FORMS FOR MAINTAINING RESGISTERS AND RECORDS
C o m p i l e d b y P o w e r H R F o r u m P a g e W 4
5. Mines Rules, 1955 FORM ‐B Register of employees ( See Rules 48(3), 51, 77 and 77.A(2)))
FORM ‐C Register of persons employed below ground during the weak
FORM ‐D Register of persons employed above ground in opencast working during the week
FORM ‐E Register of persons employed above ground otherwise than in opencast working during the week
FORM‐F Register of compensatory days of rest
FORM‐G Register of leave account during the calendar year
FORM‐H Register of leave wages account during the calendar year
FORM ‐I Register of overtime wages
6. Delhi Factory Rules, 1950 FORM 6 Humidity register under rule 22
FORM. 7 Record of lime washing, painting etc. Under rule 16
FORM 9 Register of compensatory holidays under rule 77
FORM 10 Overtime muster roll of exempted workers under rule 78
FORM 12 Register of adult workers under rule 80
FORM 15 Register of leave with wages under rule 87 & 88
FORM 16 Leave book under rule 87 & 88
FORM 17 Health register under rule 14
FORM 26 Muster roll under rule 103
FORM 27 Register of accidents and dangerous occurrences under rule 104

INDEX OF FORMS FOR MAINTAINING RESGISTERS AND RECORDS
C o m p i l e d b y P o w e r H R F o r u m P a g e W 5
7. The Delhi Shops and Establishment Rules, 1954 FORM B Register of Establishments
FORM G Register of Employment & Remuneration
FORM H Register of Employment and Remuneration of Employees
FORM I Register of Leave
8. The Employees’ State Insurance (General) Regulations, 1950
FORM 6 Register of employees
FORM 11 Accident book
9. The Workmen’s Compensation Rules, 1924
FORM C Statement of disbursements
FORM R Register of agreements
10. The Minimum Wages (Central) Rules, 1950
FORM I Register of fines
FORM II Register of deductions for damage or loss caused to the employer, by the neglect or default of the employed persons
FORM IV Overtime register for workers
FORM V Muster roll
FORM X Register of wages
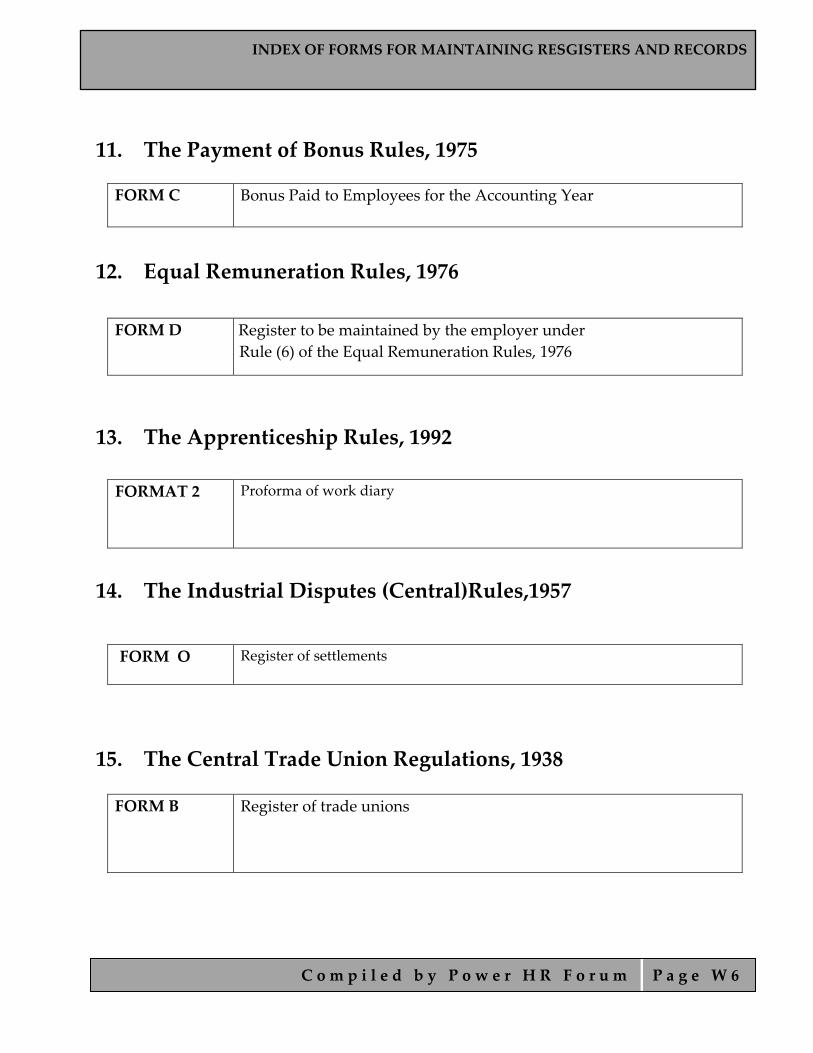
INDEX OF FORMS FOR MAINTAINING RESGISTERS AND RECORDS
C o m p i l e d b y P o w e r H R F o r u m P a g e W 6
11. The Payment of Bonus Rules, 1975
FORM C Bonus Paid to Employees for the Accounting Year
12. Equal Remuneration Rules, 1976
FORM D Register to be maintained by the employer under Rule (6) of the Equal Remuneration Rules, 1976
13. The Apprenticeship Rules, 1992
FORMAT 2
Proforma of work diary
14. The Industrial Disputes (Central)Rules,1957
FORM O Register of settlements
15. The Central Trade Union Regulations, 1938 FORM B Register of trade unions
INDEX OF FORMS FOR FILLING RETURNS
C o m p i l e d b y P o w e r H R F o r u m P a g e X 1
INDEX OF FORMS FOR FILLING RETURNS
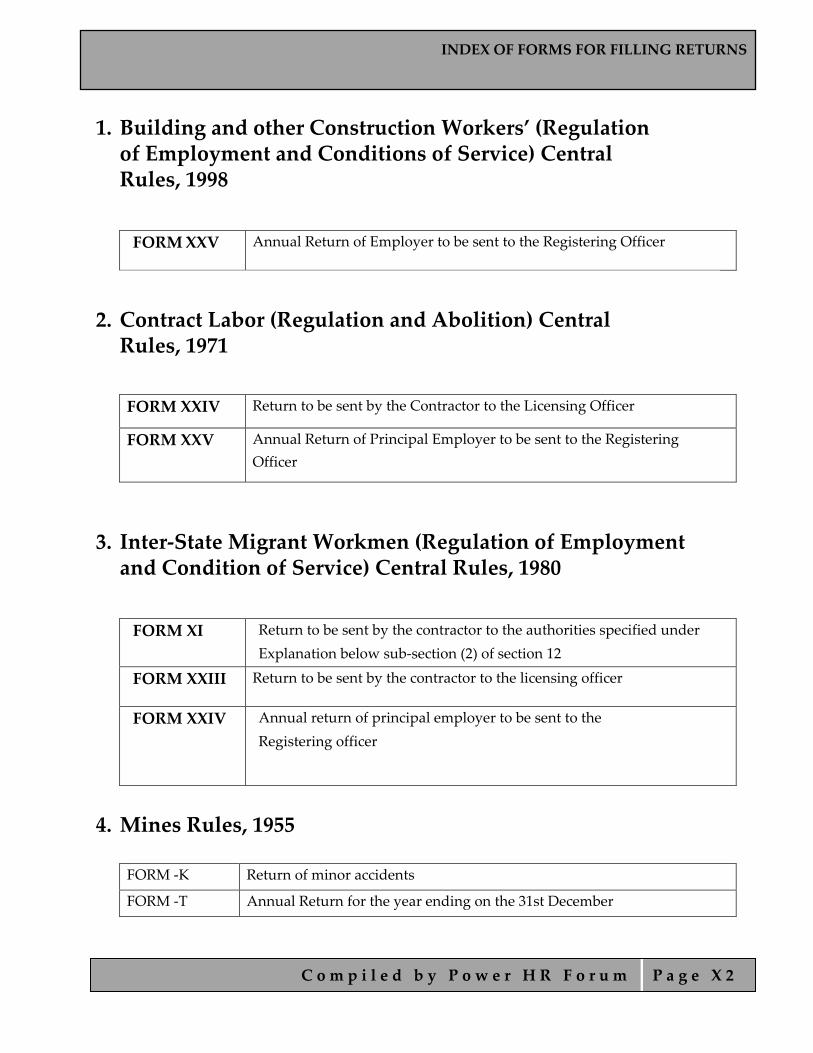
INDEX OF FORMS FOR FILLING RETURNS
C o m p i l e d b y P o w e r H R F o r u m P a g e X 2
1. Building and other Construction Workers’ (Regulation of Employment and Conditions of Service) Central Rules, 1998
FORM XXV Annual Return of Employer to be sent to the Registering Officer
2. Contract Labor (Regulation and Abolition) Central Rules, 1971
FORM XXIV Return to be sent by the Contractor to the Licensing Officer
FORM XXV Annual Return of Principal Employer to be sent to the Registering Officer
3. Inter‐State Migrant Workmen (Regulation of Employment and Condition of Service) Central Rules, 1980
FORM XI Return to be sent by the contractor to the authorities specified under Explanation below sub‐section (2) of section 12
FORM XXIII Return to be sent by the contractor to the licensing officer
FORM XXIV
Annual return of principal employer to be sent to the Registering officer
4. Mines Rules, 1955 FORM ‐K Return of minor accidents
FORM ‐T Annual Return for the year ending on the 31st December
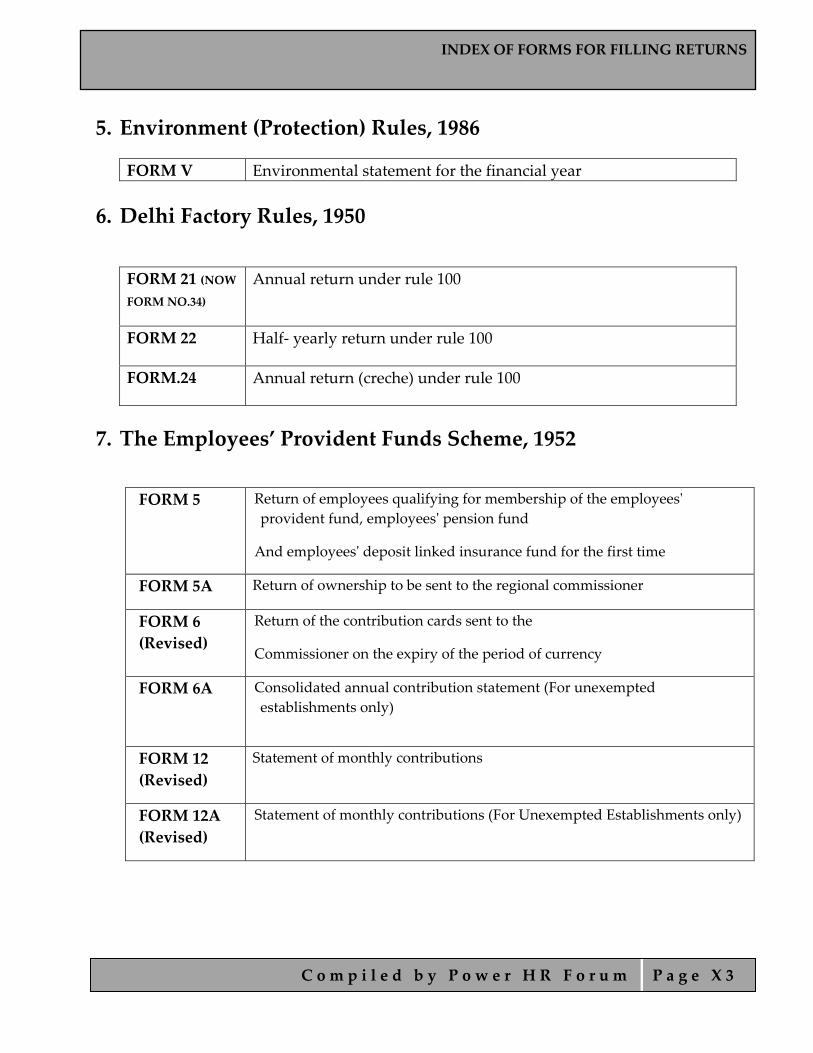
INDEX OF FORMS FOR FILLING RETURNS
C o m p i l e d b y P o w e r H R F o r u m P a g e X 3
5. Environment (Protection) Rules, 1986
FORM V Environmental statement for the financial year 6. Delhi Factory Rules, 1950
FORM 21 (NOW FORM NO.34)
Annual return under rule 100
FORM 22 Half‐ yearly return under rule 100
FORM.24 Annual return (creche) under rule 100
7. The Employees’ Provident Funds Scheme, 1952
FORM 5
Return of employees qualifying for membership of the employeesʹ provident fund, employeesʹ pension fund
And employeesʹ deposit linked insurance fund for the first time
FORM 5A Return of ownership to be sent to the regional commissioner
FORM 6 (Revised)
Return of the contribution cards sent to the
Commissioner on the expiry of the period of currency
FORM 6A
Consolidated annual contribution statement (For unexempted establishments only)
FORM 12 (Revised)
Statement of monthly contributions
FORM 12A (Revised)
Statement of monthly contributions (For Unexempted Establishments only)

INDEX OF FORMS FOR FILLING RETURNS
C o m p i l e d b y P o w e r H R F o r u m P a g e X 4
8. The Employees’ State Insurance (General) Regulations, 1950
FORM 01(A) Form of Annual Information of Factory/Establishment covered under ESI
Act
FORM 5 Return of contributions
FORM 5A Statement of advance contributions made for the contribution period
9. The Workmen’s Compensation Rules, 1924
FORM EE Report of fatal accidents
10. The Minimum Wages (Central) Rules, 1950
FORM III Annual returns
11. Payment of Bonus Rules,1975
FORM D
Annual Return—Bonus Paid to Employees for The Accounting Year
12. Employment Exchange (Compulsory Notification Of Vacancies) Rules, 1960
FORM ER‐I Quarterly return to be submitted to the local Employment Exchange
FORM ER‐II
Occupational return to be submitted to the Local Employment Exchanges once in two years

INDEX OF FORMS FOR FILLING RETURNS
C o m p i l e d b y P o w e r H R F o r u m P a g e X 5
13. The Apprenticeship Rules, 1992
FORMAT 1A Intimation regarding engagement of apprentices and forwarding their contracts for registration
FORM APPRENTICESHIP 1 Submission of Half Yearly Returns
APPRENTICESHIP TRAINING SCHEME 1
Submission of Half‐Yearly Returns
APPRENTICESHIP TRAINING SCHEME 2 (FOR RDAT)
Submission of Half‐Yearly Returns:
APPRENTICESHIP TRAINING SCHEME 3 (STATE/UNION TERRITORY)
submission of Half‐Yearly Returns
FORM APPRENTICESHIP 2
To be submitted within ten days from the date of engagement of apprentices applicable only to graduate or technician or technician (vocational) apprentices
FORM APPENTICESHIP 3
Record of progress of apprentice to be submitted once in a quarter in respect of graduate or technician or technician (vocational) apprentices
14. The Industrial Disputes (Central)Rules,1957
FORM G Progress report on constitution and functioning of works committee for the half‐year ending the 30th June/31st December
FORM N Form of report of strike or lock‐out in a public utility service





























