Embed Size (px)
Citation preview

MESOMELIC DYSPLASIA WITH SPECIFIC AUTOPODALSYNOSTOSES: A THIRD OBSERVATION AND FURTHERDELINEATION OF THE MULTIPLE CONGENITAL ANOMALYSYNDROME
Jules G. Leroy MD, PhD, and Lieve Claus MD u Department of Pediatrics,
Ghent University Hospital, Ghent, Belgium
Brendan Lee MD, PhD u Department ofMolecular and Human Genetics,
Baylor College ofMedicine, Houston,Texas, USA
Geert R. Mortier MD, PhD u Department ofMedical Genetics, Ghent University
Hospital, Ghent, Belgium
u We report on a 4-year-old boy with a multiple congenital anomaly syndrome comprising symmetric
carpometacarpal and tarsometatarsal synostoses and moderate acromesomelia. Because both the anatomy and
function in elbows, knees, and ankles were adversely a¡ected, mobility in the upper limbs and gait were ser-
iously impaired. Other important components of the syndrome included eyelid ptosis, hypoplastic soft palate
and uvula, atrial septal defect, ventricular septal defect, coarctation of the aorta, and bilateral hydronephrosis
due to congenital vesicoureteral junction stenosis.The stature was in the low normal range and the mental
development normal. Only two observations of a similar set of malformations previously have been reported.
This pleiotropic syndrome, most probably an autosomal dominant trait, is apparently the phenotypic result of
a single gene mutation disturbing antenatal pattern formation, more speci¢cally distal limb segmentation and
joint di¡erentiation.
Keywords Syndromic mesomelic dysplasia, autopodal synostoses, joint anomalies
In addition to his other congenital anomalies, the proband’s phenotype includes theclinical features of an acromesomelic dysplasia andapeculiar type of symmetric sy-nostoses in the hands and feet.This constellation of ¢ndings hasbeen described pre-viously in only one of the heterogeneous group of acromesomelic dysplasias listedin the International Nomenclature and Classi¢cation of the Osteochondrodys-plasias [1].This syndrome has been reported only twice previously [2, 3].This arti-cle describes in detail the clinical and roentgenographic ¢ndings of all the casesfurther delineating the speci¢c disorder. The synostoses and joint abnormalities
The support for this project to Dr. Leroy during a sabbatical leave at the Greenwood Genetic Center,Greenwood, South Carolina, and at the Baylor College of Medicine, Department of Molecular and HumanGenetics, Houston,Texas, is gratefully acknowledged.
Address corresponding toJules G. Leroy,MD, PhD, Departments of Pediatrics &Medical Genetics, GhentUniversity Hospital,185 De Pintelaan, B-9000 Ghent, Belgium. E-mail: [email protected]
Pediatric Pathology andMolecular Medicine 22: 23^35, 2003Copyright# 2003 Taylor & Francis1522-7952/03 $12.00 + .00DOI: 10.1080/15227950390168156
23
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

have not onlymajor implications for the patient’s posture andgait, but they promptheuristic hypotheses on‘‘candidate genes’’ that play a role in patterning the embryo-nic development of limbs and joints.
PATIENT REPORT AND RADIOGRAPHIC FINDINGS
ProbandTDwas the third child and second son of nonconsanguineous parentsandwas born at 39 weeks of gestation by normal vertex delivery. Because the preg-nancy was complicated by third trimester polyhydramnios and a fetal intra-abdominal mass detected by ultrasound examination, cytogenetic analysis inamniocytes was performed and showed a normal 46,XY karyotype. The father’sage was 45 and the mother’s 42 years. Birth weight was 3790 g, length 52 cm, andOFC 36 cm. There were multiple congenital anomalies including bilateral eyelidptosis, blepharophimosis, mild telecanthus, downslanting palpebral fissures, smallnose, large pinnae, prominent philtrum and mouth, hypoplastic soft palate anduvula, bilateral clubfoot and clubhand with ulnar deviation, and short campto-dactylic fingers. A complex heart defect was found including atrial septum defect(ASD), ventricular septum defect (VSD) with significant left-to-right shunt, andcoarctation of the aorta. A prominent abdomen related to bilateral hydronephrosisalso was observed.In the first year of life the patient had many hospital admissions for corrective
surgery.The hydronephrosis was treated successfully by bilateral percutaneous ure-terostomies leading to restoration of renal function. Coarctectomy was performedon day 12 but impending cardiac failure required open heart surgery at 2 months.Prompt casting of the clubfeet yieldedunsatisfactory results in the left ankle in parti-cular. The left Achilles tendon was lengthened at 3 and again at 11months of age,when the tibiotalar joint capsule also was released posteriorly. Partial dislocation ofthehips required splinting inthe first yearof life.The eyelidptosiswas corrected sur-gically at 8 months with only partial cosmetic effect, but significant improvementof gaze. Psychometric testing at 9months revealed adequatemental development.When referred to theUniversityHospital as an outpatient at11.5months of age,
clinical evaluation showed weight 8150 g (10th centile: 8700 g), length 71cm(10th centile: 72.5 cm), and OFC 46 cm (10th^25th centile). Mental developmentappeared normal, but due to the joint and limb anomalies, neuromotor develop-ment was delayed. The dysmorphic features noted previously were confirmed(Figure1left).The trunk, abdomen, and external genitaliawere normal. Extensionin elbows and knees was limited to 120�, but motion in both ankles was even moredeficient. The neurological examination revealed no abnormalities. The boy wasquite alert and could already pull himself up to stand unaided.Duringanadmissiontothe localhospitalatage18months for surgicaltransferof
theM. hallucis longus about the left ankle, a radiographic surveyof the entire skele-ton was performed showing the following symmetrical findings: shortening andmilddiaphysealbowingofallmesomelicbones, elbowdislocation, symmetric fusion
24 J. G. Leroy et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

of metacarpals III and IV with proximal carpal bone nuclei, and fusion of theproximal ends of metacarpals IVand V. Metatarsal IV was most shortened andfusedto the cuboidbone.The thirdcuneiformbone inthe tarsushadanarrow, linearshape.Themildly dysplastic talus and calcaneus hadan abnormal orientation.When reexamined at the age of 3 3=4 years at the UniversityMedical Genetics
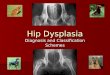
clinic, the patient’s normalmental development was readily confirmed. He had en-joyed adequate health and attended kindergarten schooling. Although languagedevelopment had progressed normally, pronunciation of several consonants re-maineddefective in spite of speech therapy,most probably related to the hypoplasticanddysfunctional soft palate anduvula. Gait was difficult and laborious andanup-right posture could only be briefly maintained. Stature, hardly measurable becauseof the lower limb joint restrictions, was recorded at 97.5 cm (25th^50th centile);weight13.1kg (3rd^10th centile), and OFC 49 cm (25th centile).The patient’s over-all habitus was thin and slender.The headwasmildly scaphocephalic with tall, ver-tical forehead and hypoplastic supraorbital ridges.The nose had more a beak-likeshape and a deep but broad nasal bridge.Telecanthus and mild downslanting pal-pebral fissures persisted.There was residual ptosis of the upper eyelids in additionto blepharophimosis. The face was flat and rather expressionless (Figure 1 right).Bothmaxillary andmandibular ridgeswere abnormally wide, the soft palate short,
FIGURE 1. Proband’s facial appearance at 11.5 months (left) and at 3 3=4 years of age (right). Note theresidual eyelid ptosis, blepharophimosis, mild downslanting palpebral ¢ssures, a small pointed nose, and aninfraoral crease.
Mesomelic Dysplasia with Synostoses 25
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

and the uvula hypoplastic. Mild retrognathia also was noticed.The neck was nor-mal (Figures1and 2).The heart ratewas normal, but soft systolic anddiastolicmur-murs were readily heard. Except for postoperative scars over thorax andabdomen, the ureterostomies having been removed at 21=2 years, the thorax, back,abdomen, and genitaliawere normal.Theboy hadacquired some compensatorymovements in dealing with the func-
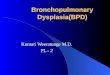
tional limitations inhisarmsandhands.Mobilityintheshoulderswasnormal,butsig-nificantly restricted in the elbowswith extension limited to two-thirds of the normalrange. Flexion, pro- and supinationwere somewhat less reduced.The forearmswereslightlybowed.Volar flexion inthewristswasseriouslyrestrictedbutextensionandro-tation less impaired.The hands were abnormally short and held in ulnar deviation
FIGURE 2. Posture of the proband at 3 3=4 years. Note the asymmetric stance and di⁄culty walking, short-ening and mild bowing of the mesomelic limb segments, limited extension in the elbows, broad genu valgumdeformities with extension asymmetrically restricted, right ankle impairment, left ankle nearly ¢xed in plantar£exion, andweight-bearing mainly on the right foot.
26 J. G. Leroy et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

(Figure 3). The fingers, the postaxial ones in particular, were brachydactylous. Ineitherhandthesecondfingerwasthelongestwiththefifthshowingradialclinodactyly.Of major concern was the difficult and crippled gait due to the known anoma-
lies in the lower limbs. In the hips, a 30� abduction deficiency was detected butother motions were near normal. Passive and active motionwere seriously deficientin knees and ankles, most evident during walking, when the genua valga deforma-tions worsened and knee instability with hyperlaxity of the joint capsular andperiarticular ligaments became more apparent. The difficult walking was com-pounded by the deformed and malfunctioning ankle joints.The left one was nearlyfixed in plantar flexion. Also in the right ankle dorsiflexion was considerablyimpaired.The feet were narrow and short at the base, the left one bearing several
FIGURE 3. Frontal view of the hands and feet at 33=4 years. Note the short hands in slight ulnar deviation,brachydactyly that is more pronounced in the postaxial ¢ngers, the indices are the longest digits, and there is 5th¢nger clinodactyly.The feet (not weight-bearing) have a short, narrowbase and are in an equinovalgus position.There are surgical scars on the left foot that is nearly ¢xed in plantar £exion.There is adduction of the forefeetand large toes and mainly postaxial brachydactyly most prominent in IV.
Mesomelic Dysplasia with Synostoses 27
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

postoperative scars. Brachydactyly was most prominent at the fibular side, thefourth toes being particularly short (Figure 3).Radiographs taken at 33=4 years confirmed and extended the earlier findings
(Figures 4^7).The skull, thoracic cage, and vertebral column were normal. Spinabifida occulta was noticed in L5 and S1. All abnormalities in the limbs were re-markably symmetrical. Ossification was appropriate for age. The distal humeralmetaphyses were unusually wide and round.There was bilateral dislocation of theulna and the radius at the elbows. Both bones had shortened and slightly boweddiaphyses and rounded distal metaphyseal ends. The distal part of the ulna washypoplastic (Figure 4). There was intracarpal extension of metacarpal III andespecially of IV. In addition the IVth andVthmetacarpals were fused at their prox-imal ends. All epiphyses of themetacarpals were narrow, small, conical, and fittinginto the corresponding cupped metaphyses.The second instead of the middle digitwas the longest in each hand (Figure 5).The pelvis had wide and squat iliac bones and quite horizontal acetabula.
There were symmetric coxa valga deformities, large proximal femoral epiphyses,and short femoral necks. Ossification of both distal femoral epiphyses and evenmore so in the proximal tibial epiphyses were deficient. The tibial and fibular dia-physes showed mildly abnormal bowing (Figure 6). The tali and calcanei wereabnormally orientedand the navicular bone abnormally positioned.The firstmeta-tarsal had an extra epiphysis distally and the normal proximal one was excessivelyflat. All metatarsals were significantly shorter than normal and had slightly cupped
FIGURE 4. Radiograph of the upper limbs at age 33=4 years. The mesomelic diaphyses are shortened andslightly bowed; there are dislocations of the radius and the ulna at the elbow; the distal ulna is particularlyhypoplastic.
28 J. G. Leroy et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

metaphyses and correspondingly conical epiphyses.There was a synostosis betweenthe cuboid bone and the IVth metatarsal and an apparent pseudometaphysealjunction between metatarsal III and the third cuneiform.The phalanges in the feetalso had conical epiphyses and cupped metaphyses. As in the hands, phalangealshortening decreased in the proximodistal direction (Figure 7).
DISCUSSION
The syndromal form of acromesomelic dysplasia in the proband differs signifi-cantly from all entities, except one, listed among themesomelic and acromesomelicdysplasias in the most recent International Classification of Osteochondrodyspla-
FIGURE 5. Hand radiographs at 2.5 months (upper panel) and 33=4 years (lower panel). Note the symmetricanomalies consisting of general shortening and mild ulnar deviation, short postaxial metacarpals and proximalphalanges, intracarpal extension of metacarpals III and probably IV, proximal synostosis of metacarpals IVandV, narrowmetacarpal epiphyses that are conical with matching cuppedmetaphyses, the 2nd digit is longest,and the middle and distal phalanges are nearly normal.
Mesomelic Dysplasia with Synostoses 29
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

sias [1]. It most probably represents only the third observation of the malformationsyndrome termed ‘‘mesomelic dysplasiaVerloos type’’ listed therein and otherwisenamed the ‘‘mesomelia^synostosis syndrome’’ (MIM 600383) [4].In differentiating the condition at hand, its syndromal extraskeletal features, in
addition to the apparent carpometacarpal and tarsometatarsal synostoses, are keycomponents.They are not observed in the multiple synostosis syndrome with prox-imal symphalangism as a cardinal feature.The latter syndrome deserves attentionas it also includes the extraskeletal components of a tubular-shaped nose with lackof alar flare, conductive hearing loss, and multiple progressive joint fusions com-mencing in the hands but continuing throughout life with ankylosis in the cervicalspine, hips, and humeroradial joints in adulthood.The causal gene of this autoso-mal dominant condition has recently beenmapped to17q21^q22 [5] and heterozy-gous mutations have been identified in the Noggin gene [6].The Noggin protein inhumans as well as in other vertebrates is of major importance in joint morphogen-esis [7] and apparently, at least indirectly, in subsequent anatomical and functionaljoint maintenance. The entities termed ‘‘proximal symphalangism’’ and multiplesynostosis syndrome are allelic [4^8].In a large three-generation family fromThailand, Kantaputra et al. [9] have
reported on an autosomal dominant mesomelic dysplasiawith severe shortening inthe forearms and milder effect in the shanks.The forearms were extremely bowed.
FIGURE 6. Lower limb radiographs at 33=4 years. Note the short femoral necks, coxa valga, mild diaphysealbowingof tibiae and¢bulae, distal shorteningof the ¢bulae, andde¢cient lateral ossi¢cation in the distal femoral,particularly the proximal tibial epiphyses.
30 J. G. Leroy et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

The ankle joints were practically absent with severe axial deviation of the feet as aconsequence. However, in these patients there are neither dysmorphic facialfeatures nor other extraskeletal anomalies. Differentiation of the Kantaputra-type mesomelic dysplasia is readily achieved radiologically as there are nocarpometacarpal or metatarsotarsal fusions and even carpal synostosis was an in-consistent finding. The gene involved in this condition remains unknown but hasbeen mapped to 2q24^q32 [10].The phenomenon of progressive coalescence of the joints with advancing age,
specifically of the carpal and tarsal bones in the acromesomelic dysplasia type
FIGURE 7. Radiographs of the feet at11=2 (upper) and 33=4 years (lower radiograph).The tali and calcanei areabnormally oriented; the narrow navicular is abnormally positioned; there is an extralarge third cuneiform anda distal extra epiphysis in metatarsal I and a £at normal one.The metacarpals, in particular the postaxial ones,are shortened with narrow, cupped metaphyses and conical epiphyses; there is synostosis of an elongated cuboidandmetatarsal IV; metatarsal III and an oblong third cuneiform are in close, almost synostotic, approximation;the large toe is in adduction.There are more conical epiphyses and matching metaphyseal cupping in the pha-langes with the more distal ones the least shortened.
Mesomelic Dysplasia with Synostoses 31
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

Osebold-Remondini [11], is reminiscent of our patient. However, this type of mildmesomelic short stature with pronouncedbrachymesophalangy andmisshapen fin-gers lacks associatedextraskeletal anomalies and, therefore, itmay readilybe differ-entiated fromthe disorder in our proband.Our patient ismost likely a newexample of themesomelia-synostosis syndrome
[4] reported only twice before, once occurring sporadically in a male adolescent[2] and in a father and his two children, a living 4-year-old girl and his elective ter-minated 18-week conceptus [3]. From the latter observation, an autosomal domi-nant mode of inheritance has been proposed. Although the rather advanced age ofthe father in our case may have favored the occurrence of a de novo germinal muta-tion with clinical effect in his son, our observation cannot formally confirm thismode of inheritance.The contention that our sporadic patient has the same condition as described in
the two previous reports is based on careful comparison of the clinical photographsand radiographs published and of the phenotypic features described [2, 3]. Thelatter are summarized inTable 1 and compared with the findings in our proband.The similarity of features is readily apparent, but some of the data require addi-tional comment. High-grade myopia and hearing deficit were observed only inthe adult [3].Whether or not these sensory handicaps are genuine components ofthe syndromewith adult onset or rather randomly associated phenomena is hither-to unknown. Otosclerotic deafness was observed as a late onset symptom also inthe multiple synostosis syndrome [5, 8] and in several other osteochondrodyspla-sias.The oral abnormality of hypoplastic uvula and significantly shortened soft pa-late, apparently without palatal cleft, known to be a more aspecific malformation,is remarkably consistent in the patients of this phenotype.Vesicoureteral stenosiswas observed in only twopatients including the proband
and the complex congenital heart defect only in the latter.The cardiac defect maybe a random occurrence or an inconsistent component. If the latter is the case, thedefect involves abnormal embryonic patterning notonly in limband joint structuresbut also in extraskeletal mesenchymal tissues.To term this syndrome amesomelic dysostosis or mesomelic dysplasia is of more
of than semantic interestbut implies apathogeneticmechanism.The termdysostosisimplies a fixed abnormality that occurred early in development, whereas dysplasiaindicates ongoing abnormalities into postnatal life.We continue to term this syn-drome a dysplasia tobe consistent with the current International Nomenclature [1].The proband described has had too short a follow-up to confirm the impression byVerloes andDavid [3] that themesomelicbowing, at least intheupper limbs, oftheirpatientswasprogressive.Theyobserved straightmesomelicbones inthe fetus,mildlybowed forearm diaphyses in the affected sister at 2 years of age, and severely bowedand shortenedulnaeand radii inthe father.Althoughthismight suggest the disorderis a dysplasia, the specific synostoses in the hands and feet arewell defined and sym-metrical since fetal life. As they seem to be stable malformations, changes in shapewith age may simply be the consequence of starting with an abnormal substrate
32 J. G. Leroy et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

TABLE 1. Clinical and Radiographic Features in this SyndromicMesomelic Dysplasia
Feature
Reference [2] [3]Patient1 Patient 2 Proband
Age at last observation (yrs) 15 43 4 3.5Craniofacial
Eyelid ptosis þ þ þ þPalpebral ¢ssures: downslanting þ þ þ þTelecanthus þ þ þ þNose: ¢ne,‘‘beaked’’ þ þ þ þFace: expressionless þ þ þ þPinnae: large ( ) � � þPalate, uvula: abnormal, hypoplastic þ þ þ þMicrognathia: mild þ þ þ �
Mental and Sensory Function
Intelligence: normal þ þ þ þMyopia (high grade) ( ) þ � �Hearing de¢cit ( ) þ � �Speech: impaired, nasal quality þ þ þ þ
General Physical
Stature: low normal þ � � þshort � þ þ �
Heart defect (complex) � � � þUmbilical cord: short, excess skin ( ) ( ) þ ( )Vesicoureteral stenosis: hydronephrosis þ � � þClubhand: brachydactyly, 2nd ¢nger longest þ þ þ þClubfoot: complex type, brachydactyly þ þ þ þAcromesomelic limb shortening þ þ þ þJoints: limited range of motion, malformed þ þ þ þDiaphyseal bowing long bones* ( ) þ ? þUmbilical hernia ( ) þ ( ) �
Radiology Upper Limbs
Mesomelic diaphyses: bowed; shortened þ þ þ � �Dislocation radial head þ þ þ þHypoplasia distal ulna þ þ þ þWidened mesomelic metaphyses þ þ þ þAbnormal elbow joints þ þ þ þUlnar deviation of hands þ þ þ þ þCarpal bones:dysplastic þ þ þ þintracarpal fusion þ þ ? ?
Metacarpals:postaxialSshortened þ þ þ þII and III fused with carpal bones þ þ þ þproximal fusion of IVandV þ þ þ þ
Proximal phalanges: short, hypoplastic þ � þ �
(More)
Mesomelic Dysplasia with Synostoses 33
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

for growth.Whether transient embryonic or prolonged postnatal expression of theresponsible gene equates to a clinical dysostosis or dysplasia, respectively, remainstobe seen.Apriori, a dysostosis gene couldcontinue tobe expressedpostnatallywith-out a demonstrable ongoing effect on either bone growth or shape.Regardless of the unresolved issue of the progressive nature of the entity under
discussion, it is safe to hypothesize that the causal gene encodes a signaling or pat-terning factor expressed at least during embryogenesis and contributes to organo-genesis and limb formation. In our proband, the basic anatomy of all four limbsand their triaxial polarity are present. Furthermore, nobasic asymmetry in his ske-letal involvement is observed. The major signaling and transcription factors re-quired for establishing limb patterning along the dorsoventral, anterior-posterior,or proximodistal axes could be causally involved in this syndrome. However, thesymmetric synostoses that are quite specifically located in themedian andpostaxialregion of the autopodal segments, in addition to themore generalized joint abnorm-ality involving anatomically minor structures, instead point to factors with a morespecific effect on joint differentiation and=or maintenance.SinceNoggin,aknownantagonistofbonemorphogeneticprotein [7], ismutated
in the multiple synostosis syndrome [6] and proximal symphalangism [8], we pro-pose that other factors such as GDF6 and 7, which act to pattern joint formation [12,13], aremore relevant candidate genes for themesomelic disorder in this proband.
REFERENCES
1. International nosology and classi¢cation of constitutional disorders of bone 2001.AmJMed Genet 2002;113:65^77.
2. Pfeifer RA,HirschfelderH,RottH-D. Speci¢c acromesomeliawith facial and renalanomalies: A new syndrome. Clin Dysmorph1995;4:38^43.
TABLE 1. (Continued)
Radiology Lower Limbs
Mesomelic diaphyses: mildly bowed,shortened þ þ ? �
Flaring of metaphyses (knees, ankles) þ þ � þAbnormal ankle joints þ þ � þFusion proximal tarsal bones þ þ þ ?Dysplastic tarsal bones þ þ þ þMetatarsals (axial, postaxial): dysplastic þ þ þ þproximal fusions III^V þ þ þ þIII fused with cuneiform III þ þ ? þIV fused with cuboid þ þ ? þ
þ ¼ present;� ¼ absent; ( )¼ not mentioned, not examined, information unavailable; ?¼patient too young, follow-up period too brief, ossi¢cation incomplete.*Progressive character still needs con¢rmation.
34 J. G. Leroy et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

3. Verloes A, David A. Dominantmesomelic shortness of staturewith acral synostoses,umbilical anomalies and soft palate agenesis. Am JMed Genet 1995;55:205^212.
4. McKusickVA.Mendelian Inheritance inman. Catalogue of Autosomal Dominant,Autosomal Recessive and X-Linked Phenotypes, 12th ed. Baltimore: Johns Hop-kins University Press,1998.
5. Krakow D, Reinker K, Powell B, Cantor R, Priore MA, Garber A, Lachman RS,Rimoin DL, Cohn DH. Localization of a multiple synostosis syndrome disease tochromosome17q21^22. Am JHumGenet1998;63:120^124.
6. GongY, Krakow D, MarcelinoJ,W|lkin D, Chitayat D, Babul-Hirji R, Hudgins L,Cremers CW, Cremers FPM, Brunner HG, Reinker K, Rimoin DL, Cohn DH,Goodman FR, Reardon W, Patton M, Francomano CA, Warman ML. Hetero-zygous mutations in the gene encoding noggin a¡ect human joint morphogenesis.Nat Genet 1999;21:302^304.
7. Brunet LJ, McMahon JA, McMahon AP, Harland RM. Noggin, cartilagemorphogenesis and joint formation in the mammalian skeleton. Science1998;280:1455^1457.
8. Polymeropoulos MH, Poush J, Rubenstein JR, Francomano CA. Localization ofthe gene (SYM1) for proximal symphalangism to human chromosome17q21^q22.Genomics1995;27:225^229.
9. Kantaputra PN, Gorlin RJ, Langer LO. Dominant mesomelic dysplasia, ankle,carpal and tarsal synostosis type: A new autosomal dominant bone disorder. AmJMed Genet 1992;44:730^737.
10. FujimotoM, Kantaputra PN, Ikegawa S, FukushimaY, Sonta S, MatsuoM, IshidaT,MatsumotoT,Kondo S,TomitaH, DengH-X,D’ursoM,RinaldiMM,VentrutoV,TakagiT,NakamuraY,NiikawaN.The gene formesomelic dysplasiaKantaputratype is mapped to chromosome 2q24^q32. J HumGenet1998;43:32^36.
11. OseboldWR, Remondini DL, Lester EL, Spranger JW, Opitz JM. An autosomaldominant syndrome of short stature with mesomelic shortness of limbs, abnormalcarpal and tarsal bones, hypoplasticmiddle phalanges andbipartite calcanei. Am JMed Genet1985;22:791^809.
12. Wolfman NM, Hattersley G, Cox K, Celeste AJ, Nelson R, Yamaji N, Dube JL,DiBlasio-Smith E, NoveJ, Song JJ,WozneyJM, RosenV. Ectopic induction of ten-don and ligament in rats by growth and di¡erentiation factor 6, and 7, members oftheTGF-beta gene family. JClin Invest 1997;100:321^330.
13. Davidson AJ, Postlethwaith JH, Yan YL, Beier DR, van Doren C, Foernzler D,Celeste AJ, Crozier KE, Crozier PS. Isolation of zebra¢sh gdf7 and comparativegenetic mapping of genes belonging to growth=di¡erentiation factor 5, 6, 7 sub-group of theTGB-beta superfamily. Genome Res1999;9:121^129.
Mesomelic Dysplasia with Synostoses 35
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/2
9/14
For
pers
onal
use
onl
y.

![Geochemical Studies for Gold in Alut Anomaly District · et al. [11] and Li et al. [12]. In this study, anomaly delineation and geochemical behavior of gold has been studied in Alut](https://img.dokumen.tips/doc/110x75/5fa24b6ca5687d3a5e22022a/geochemical-studies-for-gold-in-alut-anomaly-district-et-al-11-and-li-et-al.jpg)