Embed Size (px)
Citation preview
1
An Analysis of Preferred Maternal Education Topics among Prenatal and Postpartum
Women Employed in an Urban Corporate Setting in North Carolina
By Rebecca Merrick
May 2010
APPROVED BY:
PRIMARY PROFESSOR
Stephanie Jilcott, PhD Date
PROFESSIONAL PAPER CONTENT ADVISOR
April 1, 2010
Betsy LaForge, MPH Date
CHAIR, DEPARTMENT OF PUBLIC HEALTH
Lloyd Novick, MD, MPH Date

2
An Analysis of Preferred Maternal Education Topics among Prenatal and Postpartum
Women Employed in an Urban Corporate Setting in North Carolina
Rebecca Merrick, MPH Candidate
East Carolina University Brody School of Medicine, Department of Public Health
Hardy Building, 1709 W. Sixth Street
Greenville, NC 27834
MPH 6992 – Professional Paper II
Primary Professor:
Stephanie Jilcott, PhD Brody School of Medicine
Department of Public Health
Content Advisor:
Betsy LaForge Director, Member Health Partnerships
Blue Cross Blue Shield of North Carolina
Spring 2010

3
An Analysis of Preferred Maternal Education Topics among Prenatal and Postpartum
Women Employed in an Urban Corporate Setting in North Carolina
Rebecca Merrick, MPH1, Stephanie Jilcott, PhD1, Betsy LaForge, MPH2
1 Department of Public Health, Brody School of Medicine, East Carolina University, Greenville, NC 27834
2 Blue Cross Blue Shield of North Carolina
Corresponding Author:
Rebecca Merrick, MPH, Department of Public Health, Brody School of Medicine, East Carolina University, Greenville, NC 27834
Telephone: 252-555-1234
Fax: 252-744-4008
Email: [email protected]
Word Count: 8,559
Key Words: Maternal Education, Prenatal Care, Focus Groups, Social Cognitive Theory
Abstract Word Count: 229
Charts: 2
Tables: 6

4
An Analysis of Preferred Maternal Education Topics among Prenatal and Postpartum
Women Employed in an Urban Corporate Setting in North Carolina
Abstract
Although preterm birth and infant mortality remain prominent public health issues in the
United States, little is known about the causes of these problems. To minimize preterm birth
risks for both mother and child, it is important for pregnant and postpartum mothers to receive
the appropriate prenatal care and education on healthy behaviors. The purpose of this study is to
examine knowledge gaps of prenatal and postpartum women employed in an urban corporate
setting in North Carolina and subsequently refine maternal education materials by
recommending appropriate topics for prenatal and postpartum education programs sponsored by
health insurance companies. Two focus groups of pregnant or postpartum (<6 months) women
were conducted at a major insurance company. Six educational booklets currently being
considered by the insurance company for its member pregnancy program were used to assess the
women’s’ perceptions, experiences, and knowledge base of common prenatal and postpartum
concerns. Focus group responses were organized using NVivo. Results indicate a number of
topics that should be considered when developing educational materials for pregnant and
postpartum women, particularly visual content, interactivity, father involvement, breast and
bottle feeding, booklet length, and mental health/post partum depression. Since a major
limitation for this study is its small unit of analysis (n=2) and number of participants (n=4, n=4),
these results should be used as preliminary research used to frame more in-depth focus groups
and shape future studies.
5
Goal, Objectives, and Purpose of Research
The goal of this study is to increase adherence to prenatal care standards by improving
the information environment among women employed in an urban corporate setting in North
Carolina. In order to attain this goal, this study employs three outcome objectives as
investigatory tools: (1) Conduct focus groups with pregnant or recently delivered women in an
urban corporate setting in North Carolina, (2) Analyze responses from the focus groups to
determine differences and similarities in knowledge of pregnant or recently delivered women
from corporate urban settings, and (3) Recommend topics to include or exclude in education
materials and identify most economically feasible learning materials. These objectives will be
measured though attendance and participation during each focus group, using NVivo to analyze
participant responses, and the NVivo analysis results, respectively. Finally, the purpose of this
study is to examine knowledge gaps of prenatal and postpartum women employed in an urban
corporate setting in North Carolina and subsequently refine maternal education materials by
recommending appropriate topics for prenatal and postpartum education programs sponsored by
health insurance companies.
Introduction
The United States ranks 29th among industrialized nations in infant mortality rate.1 In
North Carolina, in 2005, the infant mortality rate was higher than the US average, reporting 8.53
deaths per live births in NC compared to 6.83 deaths per 100,000 live births nationwide, making
NC the 7th highest infant mortality rate among all the states.2
Short gestation and low birth weight are among the leading causes of premature infant
deaths. North Carolina exceeds the US preterm birth rate averages, with rates of 13.6 per
100,000 and 12.8 per 100,000, respectively.3 Among those premature babies who do survive,
low birth weight is associated with long-term disability such as cerebral palsy, mental
6
retardation, vision and hearing impairments.4 Hence, the Centers for Disease Control (CDC) and
the Health Resources and Services Administration (HRSA) have set national public health goals
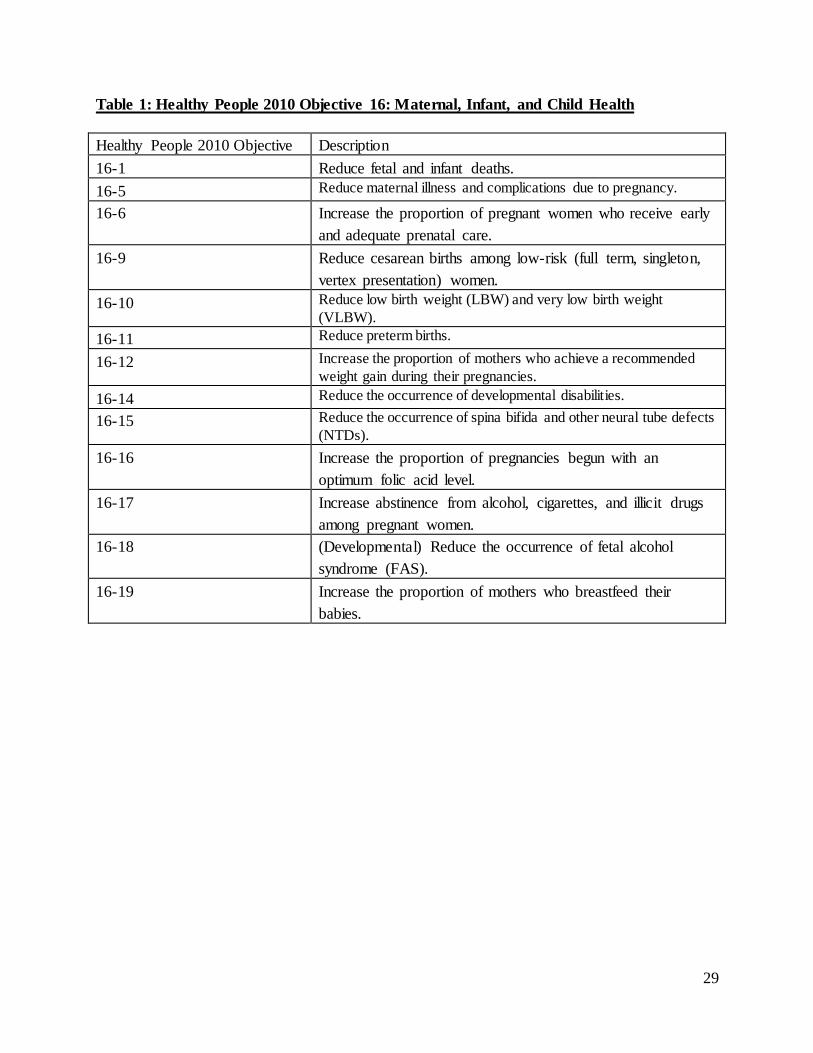
to improve maternal and child health care. For the public health community, Healthy People
2010 provides the most comprehensive national goals and objectives. Healthy People Objective
16 describes a number of areas to target in order to improve the health and well-being of women
and infants (Table 1). 5
Major cost drivers associated with pregnancy, in addition to premature deaths, are low
birth weight, premature birth, multiple gestations and elective Cesarean sections.6 Health plans
and employers struggle to manage these costs as the risk factors are either difficult to impact or
difficult to identify in a timely fashion. With today’s stagnant economy, most companies are
attempting to control costs and reduce expenses across the board. Even large private insurers and
managed care organizations need to reevaluate many of their programs and implement methods
to create efficiencies. A common approach to reaching members of such insurance companies is
mass mailings to members identified as having a certain condition, such as pregnancy. However,
large mailings can be expensive; reducing the volume and frequency of mailings is an effective
cost-reducing strategy. With economic restraints on pregnancy programs, health insurance
companies and physicians’ offices are looking to provide lower-cost yet high quality materials to
their members and patients.
Background and Literature Review
The prenatal and postpartum periods are critical times to influence the health of both
mother and child. Prenatal care potentially reduces rates of infant and maternal morbidity and
mortality.7 It is important that this population receives timely and accurate information
encouraging healthy behaviors to ensure a healthy pregnancy.

7
Not receiving appropriate prenatal care can lead to a myriad of problems, which create
high costs during pregnancy, delivery, and the immediate postpartum period. A 2003 study by E.
Kathleen Adams8 attempted to quantify the cost discrepancy between normal and preterm births.
This study calculated a mean cost for a normal, full term infant to be $1,139, while the mean cost
for an infant with problems to be $15,772. In addition, Adams9 showed that while the majority of
births were normal (76%), they only accounted for 18% of the total delivery costs. These total
costs reflected only inpatient costs for room and board, physician, ancillary, and inpatients drugs.
The infants born prematurely or with problems accounted for 82% of the total delivery costs.
Adams10 also showed that the use of cesarean delivery was a major cause of inflated costs for
premature delivery. Among normal infants, the cost of a vaginal delivery averaged $5,913.
Cesarean deliveries were markedly more expensive: uncomplicated cesarean deliveries averaged
$12,500 and complicated cesarean deliveries created costs averaging approximately $16,000.
These findings reflect the skewed nature of health care cost and the impact of preterm
complications.
Past studies have shown that prenatal care potentially improves birth outcomes11 and
disparities in outcomes due to socioeconomic factors.12 Parents need prenatal education,13 but no
studies (to our knowledge) have attempted to refine the topics presented to pregnant women in
materials originating from private insurance organizations. Privately insured pregnant women
typically receive education from physicians, laypersons, and their insurance plans. In contrast,
women without private insurance may not receive such education materials from physicians or
insurance programs due to access barriers associated with low socioeconomic status. A 2009
study by Jesse14 found that low-income African American women from a rural clinic in eastern
NC had a higher rate of preterm birth than African American women in the state of NC and the

8
United States. The women in the Jesse15 study did not have private insurance and represented a
population characterized by high poverty, morbidity, and infant mortality.
The goal of this study is to increase adherence to prenatal care standards by improving
the information environment among women employed in an urban corporate setting in North
Carolina. Furthermore, this study examines the differences and similarities in knowledge women
from an urban corporate setting during prenatal and postpartum periods using focus groups. By
analyzing responses obtained during the focus groups, this study will recommend topics to
include or exclude in education materials and identify the most economically feasible learning
materials for private insurance companies to provide for pregnant or recently delivered women.
Specifically, this study uses materials potentially distributed by a major private insurance agency
in North Carolina.
Although low-socioeconomic populations are particularly in need of prenatal education,
this study focuses on women employed by large corporations in urban environments who receive
private insurance through their employer health plans. A high-income population was used for
this study because it provided a sample of pregnant and recently postpartum women receiving
prenatal education and to obtain a representative sample of urban women of childbearing age.
Since increased insurance coverage and receipt of early prenatal care are directly related,16 an
urban corporate population can be studied to determine which risk factors are not being
addressed in prenatal care education initiatives currently being applied to pregnant and
postpartum women. The findings of this pilot study can further offer preliminary research used to
frame more in-depth studies and create tools to help better target other populations in need of
preterm birth interventions. Since the high-income population in this study is characterized at a
lower risk for preterm birth than lower socioeconomic women in NC, 17 the results of this study

9
may help identify other factors which may be contributing to the disparity in preterm birth rates.
Additionally, this study may identify characteristics of high-income populations that contribute
to healthier pregnancy outcomes and can potentially be used as points of intervention for the
lower income populations.
Applying the Social Cognitive Theory to Behaviors which Affect Prenatal Outcomes
The Social Cognitive Theory (SCT)18 is appropriate when describing factors and
behaviors that may affect prenatal outcomes, positing that self-efficacy, goals, and outcome
expectations determine the likelihood of a person changing a health behavior. This theory
operates at an interpersonal level, creating behavioral influences both within an individual and
from the external social environment (such as family, friends, and health professionals).
The six SCT constructs can be applied to programs that aim to improve prenatal
outcomes (Table 2). These constructs can help describe the relationship among factors that can
influence decision processes which lead to behaviors that ultimately affect prenatal outcomes.
The focus group data collected as a part of this study address all six of the constructs of the SCT.
In addition, a conceptual model can be used to depict the relationship between each of these
constructs and behaviors that impact prenatal outcomes. As an example, we will use the case of
maternal smoking during pregnancy since smoking is an established risk factor for abnormal
fetal development.19
Reciprocal determinism occurs as environmental and personal determinants interact with
a behavior such as smoking during the course of the expectant mother’s life. A woman may live
in a home where smoking during pregnancy is the norm or where she is exposed to secondhand
smoke from others (environmental determinants). Individual determinants, such as age and
education level, also contribute to a woman’s likelihood of smoking while pregnant. These
factors then influence the expectant mother’s decision to initiate, continue, or cease smoking.

10
This relationship impacts the self-efficacy for tobacco-use cessation and behavioral
capability the mother has to cease tobacco use, to improve the birth outcome. Behavioral
Capability is the actual knowledge a person has to carry out a behavior. Pregnant women have
very specific needs that may not be common knowledge. In the case of maternal smoking, some
women have been taught the hazards of tobacco use on fetal development. Others, however, may
not have gained this knowledge and therefore unknowingly continue to expose the developing
child to the hazards of smoking. Self-efficacy is a person’s confidence to take action to
overcome barriers and perform the desired behavior change. Sometimes pregnant women must
drastically change their lifestyle choices if the baby’s health is to be maintained. Women who
smoke prior to pregnancy must make the decision to either continue smoking or cease the habit
once a pregnancy is confirmed. Some women may have high confidence in their ability to cease
smoking, but others may not be able to overcome the barriers (e.g., nicotine cravings) and create
a safer environment for pregnancy.
If the levels of self-efficacy and behavioral capability are enough to overcome barriers to
smoking cessation, the expectant mother can further the process though observational learning
and formulating goals and expectations. These expectations are often learned though modeling,
or observing other women’s behaviors and associated outcomes. For instance, one mother may
smoke during pregnancy and consequently give birth to a child with low birth weight.20 Another
woman may then extrapolate the cause-and-effect relationship between smoking and the low
birth weight infant, causing her to avoid smoking during her pregnancy with the expectation that
this avoidance will lead to a healthier child.
The mother’s decision to smoke or not smoke may be reinforced in a number of ways.
Examples of a positive reinforcement for not smoking may include praise from a health

11
professional, feeling the baby’s activity as it moves within the womb, or support from family and
friends. Negative reinforcement can occur as the mother is observed smoking and criticized by a
health professional, family, friends, or others. Additionally, the mother may have feelings of
guilt as the smoking habit continues throughout the pregnancy.
These six constructs interact to influence the decision process to smoke or not during
pregnancy. By not smoking, the mother is adhering to prenatal care standards such as those
outlined by the American College of Obstetricians and Gynecologists (ACOG).21 Adherence to
these standards, particularly by not exposing the developing child to tobacco products, will
decrease her risk of preterm birth, and at the population level, lower the overall preterm birth
rate.
A Conceptual Model: The Social Cognitive Theory Influences Behaviors Affecting Prenatal
Outcomes

12
Methods
The target population for this study was urban women in North Carolina who were
currently pregnant or have delivered a child within the previous six months. Data were collected
during focus group discussions and examined using qualitative content analysis. For the purposes
of this study, the focus group was the unit of analysis. This study was approved by the East
Carolina University and Medical Center Institutional Review Board (ECU UMC IRB).
At the beginning of each session, the moderators explained the purpose of this study.
Both verbal and written consent were obtained from each participant. Participants also signed a
statement describing the study, showing their consent for responses to be audio-recorded and
used for this research project.
Methods of Data Collection in an Urban Corporate Environment
This study was conducted in a corporate environment at a major insurance company
located in Durham, NC. Two focus groups were conducted at different locations on the
company’s campus. These two locations were chosen a priori since they were the largest
employee centers for the company, and to minimize travel time for volunteers between their
offices and the focus group locations. The first focus group was conducted at the company
headquarters building. The second was conducted two days later at the customer service
building.
In order to recruit employees from the company to participate, a short article was posted
on the company’s intranet homepage. The article was posted five days before the first session
and seven days prior to the second session. Eligibility criteria included currently pregnant or had
delivered within the past six months and a current employee of the company. As an incentive,

13
lunch was provided at no cost to those who participated. All volunteers met eligibility criteria
and were included in the focus group discussions.
Both groups were composed of three pregnant women and one participant who had
recently delivered her child. All participants had at least some college-level education, and all
but one participant was married and living with her husband at the time (Table 3). These women
participating in both focus groups were assumed to have employer-based health insurance, as
their employer granted this reward.
When a volunteer signed up for a focus group, the materials and instructions were
immediately intra-office mailed to her, which helped ensure the participant had adequate time to
review the materials before the focus group session As part of the registration, volunteers chose
which focus group location they planned to attend (either the headquarters building or customer
service building). Six different booklets from patient education companies were included in the
packets (Table 4). Attached to each booklet was short questionnaire to aid participants in their
reviews. Additionally, a seven-question survey was included to attain a general overview of the
participants’ demographic background (Table 5). These surveys were collected at the end of each
focus group.
Each focus group took one hour. Two moderators assisted with prompting discussion
using prepared questions for the participants (Table 6). Each group included four women. In each
session, participants were assigned a number (1-4) to ensure confidentiality. Notes were taken
during the session to help assign each response to the correct participant. The sessions were
audio-recorded and later transcribed verbatim by one of the session moderators. This moderator
was able to minimize transcription error since she was familiar with the participants’ voices and
14
could correctly assign responses to each respective participant as opposed to a third-party
transcriptionist.
Data Analysis
Once both focus group sessions were transcribed, one of the moderators created a
codebook using both deductive and inductive codes. The deductive codes were established from
the Focus Group Discussion Guide based on questions asked during the focus groups.
Additionally, inductive codes were selected from the major themes and topics discussed during
the focus group sessions which were not originally anticipated. Each code and subcode were
defined and assigned criteria as to when a code would be used for a particular segment of text.
The transcripts and codes were then uploaded into Qualitative Solutions and Research
International NVivo software program (NVivo 8).22
This study used a double coding method to analyze data, with one of the moderators and
a second individual familiar with the study design independently coding both of the focus group
transcripts. The moderator and second coder met initially to review the codebook to ensure each
code was clearly defined and understood by each coder. Each coder then independently coded
the first transcript according to the codebook criteria. The coders reconvened to compare coding
assignments and discussed discrepancies between each coded transcript. After reaching an
agreement with respect to coding discrepancies, the codebook was refined with more exact codes
to better reflect the data and applied to the first transcript. Using the refined codebook, both
coders independently coded the second transcript then met to resolve coding discrepancies. The
final codes are listed in Appendix A: Codebook.

15
Results
This study utilized two focus groups of pregnant or recently postpartum (<6 months)
women. Each focus group had four participants. Three women in each focus group were
currently pregnant and one participant in each group had recently delivered a child. Additionally,
three women in each focus group had one previous child. Only one participant was not married
at the time of this study; the other married participants were currently living with their husbands.
Participants’ ages ranged from 25-40 with a median age of 33 years. Four women were African
American, three were Caucasian, and one was Asian. Three participants had some college
education, three had completed a college degree, and two had completed a graduate degree.
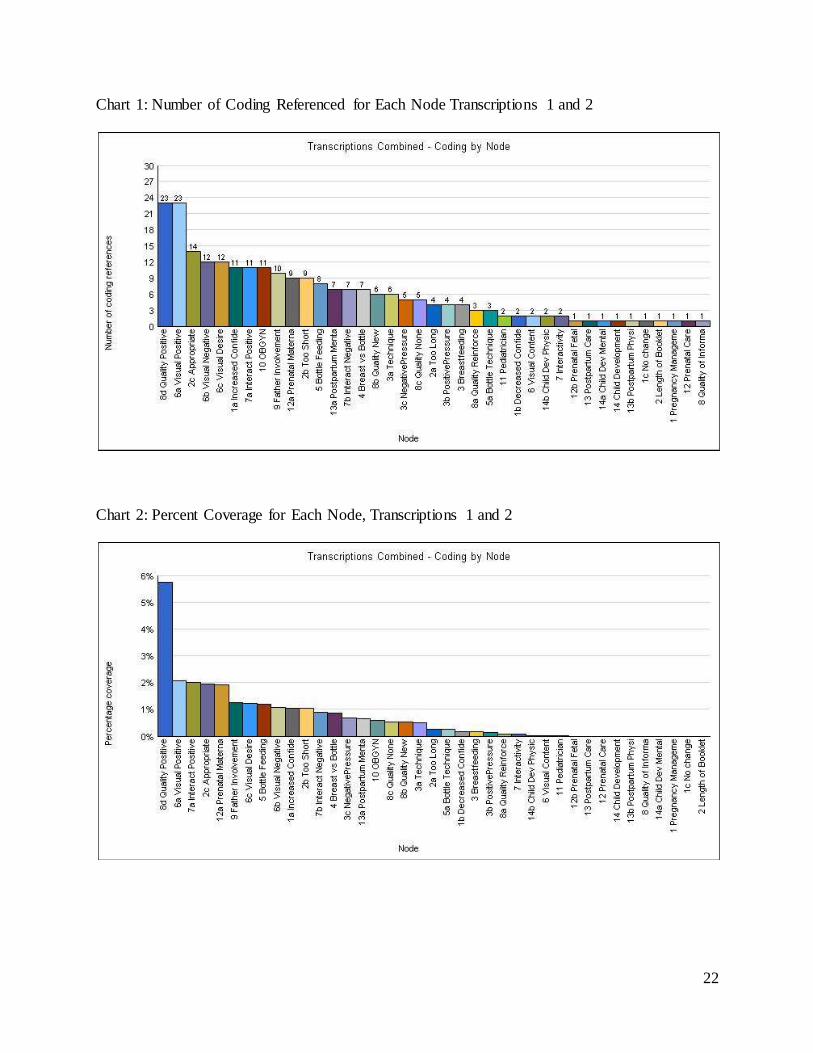
Using NVivo to organize the data, the most common codes were identified and used as a
guide to identifying themes. The researcher used the NVivo coding frequencies as a guide to
select major themes present in the focus group data. The NVivo figures informed the researcher
of patterns in the data and the most prevalent codes; the researcher then determined which codes
represented major themes and topics that can be applied to future educational materials.
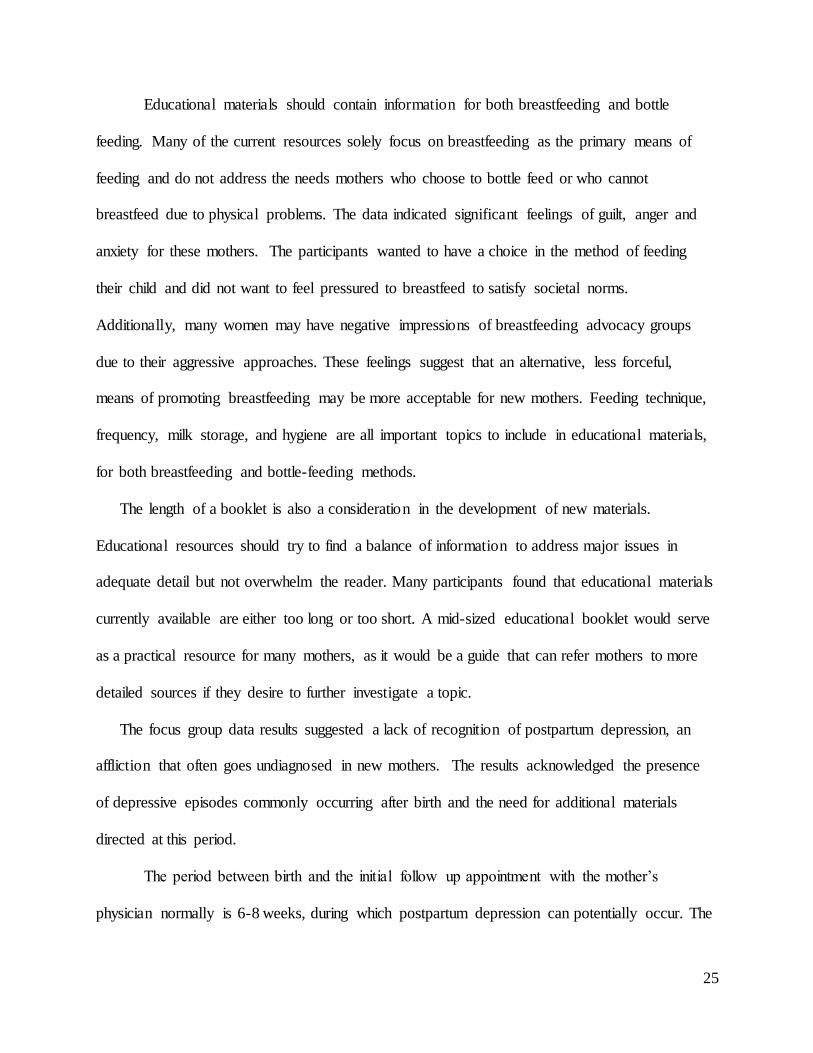
Chart 1 depicts the number of coding references for each node for both focus groups.
Chart 2 represents the percent of the total coding area each of the summed nodes covers. The
codes most often referenced were Quality Positive and Visual Positive, each with 23 references.
In other words, the participants most frequently mentioned what they liked about the educational
materials, specifically the visual aspects and quality of information, through constructive
criticism.
Visual Content
The visual layout and content of the booklets was a major discussion point in both focus
group sessions. A number of themes emerged using the codes relating to visual content, such as

16
the use of real people, color, and number of pictures in educational materials. The participants
noted positive and negative attributes of the colors, pictures, layout, and the usefulness of these
features. The codes Visual Negative (a negative statement about the visual content) and Visual
Specific Desire (any statement concerning a desire for some specific visual component),
although both only coded 12 times, were still ranked 3rd in the overall number coding references.
“I don’t like the layout, I don’t like the color, I don’t like the texture, and I
think the pictures aren’t as nice as the other one… color always beats black and
white”. (32-year old Caucasian woman, currently pregnant, one previous child)
Often, the specific desire for a visual component was related to the inclusion of pictures to
help participants understand the material presented.
“I mean you can read the descriptions and everything, but I think if you
had like a small picture I know it’s not a whole lot of space but if you had a little
you know example of what it might look like you know that would be a lot of
help”. (33-year old African American woman, currently pregnant, with one
previous child)
In addition to the inclusion of pictures, some participants asserted that a written description
was still necessary to convey the material clearly.
“I wish they had more pictures of the exercises. Here they tell you what to
do but when you’re pregnant you’re afraid that well I, think here, ok, I might be
doing this, this exercise and doing something, doing it in an adverse way not like
the pictures. You’re gonna suggest exercises, and give some descriptions or a
picture”. (33-year old African American woman currently pregnant with her first
child)
The participants felt that who was featured in pictures also impacted their views on a topic.
One participant felt that the use of female models or drawings generated a negative impression of
a booklet. Instead, she preferred “normal” looking women to which she could relate.

17
“It does help that it has real people. And not all of them look like
supermodels. That’s pretty”. (33-year old African American woman currently
pregnant with her first child)
Interactivity
The focus group data showed that some participants favored interactive materials, such as
interactive sections of workbooks, CDs, and worksheets. There were also negative responses for
interactive materials. There was considerable debate about the helpfulness of interactive
materials during each focus group. While some participants felt interactivity was a great way to
promote learning, others felt that these sections were not practical given the time constraints
involved with preparing for the birth of a child.
“I like the work- the workbook format. It really I guess in all the books but
it’s nice because I think it makes things a little more interactive and it soon
becomes a reference guide down the road where you can always pick it up and go
back to it”. (33-year old Asian woman, currently pregnant, one previous child)
“I do have to say, these little things about filling stuff out, I don’t even
have time to fill out my baby book so I found these to be like useless”. (32-year
old Caucasian woman, currently pregnant, one previous child)
Father Involvement
The focus group participants felt that the father’s role in prenatal education, the
pregnancy period, and newborn care warranted more attention. The participants asserted they
wanted the information directed towards the father included in pregnancy and postpartum
educational materials.
“They really did place an importance on the dad’s role and I thought it
was really pleasant and nice” (33-year old African American woman currently
pregnant with her first child)

18
Overall, the participants felt that the father’s role was often minimized, despite their
critical role in the child’s life.
“Pregnancy myth number one, father’s role does not begin until the birth
of the baby”. (A 33-year old Asian woman, currently pregnant with one previous
child)
Only one participant in the focus groups was not married. However, even she noted the
appeal of education materials for other family members:
“This book I think anybody can read, the dad, the mom, the grandma…
they can read it and see, you know they might know something the mom doesn’t
and you know vice versa”. (33-year old African American woman with one
previous child)
As part of their desire for more father involvement, the focus group participants said it
was their responsibility to inform the fathers of what information they needed to know. One way
mothers included the fathers in pregnancy education was to discuss what the mother had learned
after reading educational materials. Some participants felt that their husbands would not take
time to read comprehensive educational materials. Instead, the expectant mother can relay the
main points of the materials she has read to her husband.
“It’s not like my husband would look at the book. He always would just
goes ‘what did you read?’ and ‘just tell me that you did not see something’”. (32-
year old Caucasian women, currently pregnant, one previous child)
Breast and Bottle Feeding
A very prominent topic centered on the difficulties of feeding an infant. Using the NVivo
word frequency application, there were 53 references to breastfeeding (combining the words
“breastfeed”, “breast”, and “breastfeeding”), 23 references to bottle feeding, and 16 references to
feeding without specifying breast or bottle (“feed” or “feeding”).

19
Many participants had concerns with the proper feeding techniques for both breastfeeding
and bottle feeding, such as appropriate feeding schedules, when to wean a child off a bottle, how
to store milk properly and potential benefits to mother and child. These issues generate anxiety
with new mothers.
“Because I mean I didn’t know how. Once I stopped breastfeeding it was
a month in and I’m like, I didn’t know how to sterilize nipples. I didn’t know how
to do all that stuff”. (32-year old Caucasian women, currently pregnant, one
previous child)
Another participant was fearful of breastfeeding because of her friends’ experiences and
anecdotal stories:
“I didn’t want to breastfeed. I was the campaign like no, no, don’t come
over here…because I’m so nervous about it because everyone has those horror
stories about how it hurts and you just want to knock them off and you know you
bleed”. (32 year old African American woman, currently pregnant with her first
child)
The participants noted overwhelming societal pressures surrounding feeding an infant. These
pressures can lead to feelings of guilt and inadequacy if a mother could not breastfeed her child.
They pointed out that some mothers may consciously choose to bottle feed instead of breastfeed,
but many women who desire to breastfeed are not physically able to do so. To add to their
frustrations, most educational materials focus on the benefits of breastfeeding and minimize
information presented about bottle feeding, if any is included at all. One participant was
particularly upset about not being able to breastfeed, saying,
“It talks about breastfeeding and it’s really positive and then there’s this
little on bottle feeding. But it’s like it’s your choice. But the thing is you feel so
bad when you can’t… it would be nice if they had that in there because I was
really traumatized I cried and cried and cried”. (32-year old Caucasian woman,
currently pregnant, one previous child)

20
Notably, breastfeeding advocacy groups, particularly La Leche League, were generally
disliked due to their confrontational approaches. The participants felt that such advocacy groups
forced them to breastfeed without allowing them to make decisions for their own infants. One
participant who had recently delivered described her experience as she learned how to feed her
newborn:
“My baby just didn’t take to it. But, and it’s been the biggest struggle. And
so it’s very troubling to see ‘your baby was born to be breastfed. It wants to be
breastfed’. And LaLeche? No no no. Don’t. Don’t”. (40-year old Caucasian
woman, recently delivered)
Booklet Length
The length of each booklet was an issue for the women before even reading the content of the
materials. When combined, the code for Length and its associated subcodes accounted for 28
total nodes. Participants in both groups found a balance of information very important. While
some educational materials do not provide enough information to satisfy an expectant mother,
others present too much detail which overwhelms the reader.
“But honestly the choices are a really big thick book like this thing you’re
dispensing or this little thing from a doctor’s office that says nothing”. (40-year
old Caucasian woman, recently delivered her first child)
The popular book, “What to Expect When You’re Expecting” was cited in both focus groups
as being intimidating and scary due to its sheer size, exceeding 600 pages.
“I think though I would read What to Expect When Your Expecting, well
that’s the most depressing book you’ll ever read in your life… because you’ll
think that everything in the world is wrong with you if you read it. Because it’s
just hits everything”. (40-year old Caucasian woman, recently delivered her first
child)
Mental Health / Postpartum Depression

21
A recurring subject of both focus group discussions revolved around the mental health of
new mothers, particularly in regards to postpartum depression. Seven codes specifically
highlighted the mental health of the mother after delivery as a point of concern for the
participants. Although both groups agreed on the general need for additional materials directed
at identifying and coping with emotional stress during this time, they did not directly identify
postpartum depression as a major issue. Participants referred to postpartum depression as “baby
blues” and did not recognize it as an illness, but instead simply as a period of sadness.
“For baby blues, they say ok well you know you’re going to be moody
and whatever and it-it will pass in a week or two…And well I mean it does and
then it goes away… Well you don’t realize. I was like crying for a month you
know” (32-year old Caucasian woman with one previous child)
Interestingly, the participants revealed that their child’s pediatrician, not their OBGYN or
primary care doctors, are asking about the mother’s emotional well-being.
“I just took my daughter in for uh her checkup and the doctor was like,
‘how are you feeling? Are you having a good day?’ I was like, ‘Oh my gosh’”.
(33-year old Asian woman currently pregnant, one previous child)
22
Chart 1: Number of Coding Referenced for Each Node Transcriptions 1 and 2
Chart 2: Percent Coverage for Each Node, Transcriptions 1 and 2

23
Discussion
The three objectives of this study were achieved: The project conducted focus groups
consisting of pregnant or recently delivered women in an urban corporate setting in North
Carolina, the focus group responses were analyzed to assess knowledge gaps of pregnant and
postpartum women, and a number of topics were identified to refine education materials and
therefore create more cost-effective options. The results of this study can be used to promote the
overall goal of increasing adherence to prenatal standards by improving the information
environment, particularly when designing future studies to further investigate knowledge gaps
for pregnant and postpartum women.
It is important to recognize the third objective, identifying cost-effective materials, was
more in the interest of BlueCross BlueShield than the focus of this paper. BlueCross BlueShield
did utilize the recommendations of the focus group participants, eventually using one of the
favored booklets for their state-wide pregnancy program. At the same time, the data provided
valuable insight into potential knowledge gaps of pregnant and recently delivered women,
providing research to support potential points of intervention for educational programs.
Recommendations for Developing New Educational Materials
Results of this study reveal a number of issues and topics that should be considered when
developing educational materials for pregnant and postpartum women.
The use of pictures can also help the reader better understand the educational material,
but should not replace written information. This is an important consideration, since different
people have different learning styles. Some women may want a detailed description, but others
may depend more on illustrations to understand the materials. Prenatal exercises and infant

24
feeding positions were two instances that the participants felt that pictures were particularly
helpful.
Furthermore, prenatal and postpartum education materials should be culturally competent
with the pictures presented for their respective audiences. These images should depict people to
which the audience can relate instead of models or illustrations; those directed towards the
majority population should have different pictures than one directed towards a minority
population.
Prenatal and postpartum educational materials directed to a general audience should
include but limit the amount of space dedicated to interactive sections, such as places for the
mothers to create lists, take notes, and record reminders. While some of the focus group
participants felt interactivity was a great way to promote learning, other felt that these sections
were impractical due to time constraints. An expecting mother has many items to attend to before
the baby’s arrival; creating a day-by-day scrapbook, for example, may not be a priority. Instead,
these mothers looked for more content-oriented materials.
Pregnant mothers have a significant number of educational materials available to them,
but the information environment for expectant fathers is severely lacking. The participants
agreed that the father plays a critical role during and after pregnancy. This discrepancy reveals a
possible point of intervention to bolster the knowledge of expectant fathers. One method to
encourage fathers to participate in the educational process is to provide the fathers with a
compact, to-the-point booklet directed at their role. New educational materials need to
acknowledge the father’s role and allow them to take part in the educational process of
pregnancy and childbirth.
25
Educational materials should contain information for both breastfeeding and bottle
feeding. Many of the current resources solely focus on breastfeeding as the primary means of
feeding and do not address the needs mothers who choose to bottle feed or who cannot
breastfeed due to physical problems. The data indicated significant feelings of guilt, anger and
anxiety for these mothers. The participants wanted to have a choice in the method of feeding
their child and did not want to feel pressured to breastfeed to satisfy societal norms.
Additionally, many women may have negative impressions of breastfeeding advocacy groups
due to their aggressive approaches. These feelings suggest that an alternative, less forceful,
means of promoting breastfeeding may be more acceptable for new mothers. Feeding technique,
frequency, milk storage, and hygiene are all important topics to include in educational materials,
for both breastfeeding and bottle-feeding methods.
The length of a booklet is also a consideration in the development of new materials.
Educational resources should try to find a balance of information to address major issues in
adequate detail but not overwhelm the reader. Many participants found that educational materials
currently available are either too long or too short. A mid-sized educational booklet would serve
as a practical resource for many mothers, as it would be a guide that can refer mothers to more
detailed sources if they desire to further investigate a topic.
The focus group data results suggested a lack of recognition of postpartum depression, an
affliction that often goes undiagnosed in new mothers. The results acknowledged the presence
of depressive episodes commonly occurring after birth and the need for additional materials
directed at this period.
The period between birth and the initial follow up appointment with the mother’s
physician normally is 6-8 weeks, during which postpartum depression can potentially occur. The

26
focus group results indicate that the mothers were being asked about their emotional state by
their child’s pediatrician, not the mother’s physician. This interaction can provide a point of
early identification for postpartum depression symptoms, since the pediatric visits occur before
the mother’s follow-up appointments.
Mental health issues are still poorly understood compared to physical disease; it is important
to evaluate emotional well-being to ensure a healthy mental status of a new mother, which
inevitably impacts the child. New materials should dedicate resources to directly addressing
postpartum depression, as this illness can have devastating effects on both mother and child if
undiagnosed.
Strengths and Limitations
Using focus groups as a qualitative research strategy has both strengths and weaknesses.
This method allows for participants to discuss their attitudes, feelings, and opinions about a topic
with a group of peers who may share similar experiences. It also provides a setting for group
interaction which can facilitate the discovery of unexpected data and provide more insight than
individual interviews. Focus groups are a reasonable method to explore a topic in a low-cost,
flexible setting, and generate data with high face validity.
A limitation for this study was the small unit of analysis (n=2). Focus groups are usually
conducted until the responses to questions have been saturated, or similar responses are
continuously reported from different focus groups. In addition, the number of participants in
each focus group was small (n=4, n=4). Having 8-10 participants in each focus group may have
provided for better conversation and varied perspectives. The participants in this study were a
convenience sample of volunteers from the urban corporation. The views expressed by these
women cannot be generalized to other women in North Carolina, particularly those located in

27
rural environments or who are unemployed. The results of this study are only truly able to be
generalized to pregnant or recently delivered women working at BlueCross BlueShield of North
Carolina. While additional focus groups would have been beneficial to this study, we were
unable to conduct additional sessions due to time constraints for the research study.
Another limitation is that some of the participants did not have adequate time to review
the materials before the focus group session. Although the recruitment advertisement was posted
five to seven days before the sessions, some participants did not immediately enroll. Materials
were intra-office mailed to participants only after enrolling, giving several participants only one
or two days to review the six booklets.
Future Studies
The results of this pilot study can be used to frame future studies on identifying
knowledge gaps, educational preferences, and preferred topics for pregnancy programs. Future
studies can utilize the participants’ responses to create more specialized focus groups discussions
in order to encompass other populations. This can help assess knowledge gaps specific to
particular groups of women, characterized by race, geographic location, or cultural values. These
studies can help create educational materials unique to the needs and preferences of these women
and can identify which methods of outreach may work best for these populations.
Future studies can also assess how the self-efficacy for behaviors (such as adhering to the
ACOG recommendations) of pregnant women changes before and after education. Another study
can investigate how self-efficacy varies in response to different educational materials focusing
on the topics identified in this study. Additionally, future studies can assess how the timing of
educational intervention, related to the stage of pregnancy, affects the desired topics for mothers.
These findings can help build educational materials in a way to increase overall confidence and

28
decrease anxiety during pregnancy and the postpartum period related to inadequate educational
resources.
Conclusion
Overall, the results suggest that pregnant and recently postpartum women need mid-sized
educational materials that depict normal women, address the father’s role, present both breast
and bottle feeding recommendations, and include references for more in-depth information. The
findings of this qualitative study suggest the Social Cognitive Theory is a relevant framework for
understanding individual behaviors that contribute to pregnancy risks.
As a pilot study, the results can help form the basis of more in-depth, specific,
investigations into the knowledge gaps of pregnant and recently postpartum women. Particularly,
the results from this study can be used as a framework for investigations which address
disparities in birth outcomes for certain populations and how the information environment
impact’s a mother’s self-efficacy during pregnancy and the postpartum period. It is important to
ensure that educational materials for different populations address knowledge gaps unique to
each group that may lead to increased pregnancy risk. By having information presented in a way
that is culturally competent, easy to understand, and appealing, expectant mothers can better take
personal steps towards having a healthy pregnancy.
29
Table 1: Healthy People 2010 Objective 16: Maternal, Infant, and Child Health
Healthy People 2010 Objective Description
16-1 Reduce fetal and infant deaths.
16-5 Reduce maternal illness and complications due to pregnancy.
16-6 Increase the proportion of pregnant women who receive early
and adequate prenatal care.
16-9 Reduce cesarean births among low-risk (full term, singleton,
vertex presentation) women.
16-10 Reduce low birth weight (LBW) and very low birth weight
(VLBW).
16-11 Reduce preterm births.
16-12 Increase the proportion of mothers who achieve a recommended
weight gain during their pregnancies.
16-14 Reduce the occurrence of developmental disabilities.
16-15 Reduce the occurrence of spina bifida and other neural tube defects
(NTDs).
16-16 Increase the proportion of pregnancies begun with an
optimum folic acid level.
16-17 Increase abstinence from alcohol, cigarettes, and illicit drugs
among pregnant women.
16-18 (Developmental) Reduce the occurrence of fetal alcohol
syndrome (FAS).
16-19 Increase the proportion of mothers who breastfeed their
babies.

30
Table 2: The Six Constructs of the Social Cognitive Model
Construct How it applies to prenatal care and
preterm birth
Focus group question which
addresses construct
Reciprocal Determinism
This construct includes environmental, personal, and behavioral factors, such as
education level, socioeconomic status, and established habits. These
determinants can affect prenatal outcomes if they contribute to unhealthy behaviors.
Was the educational material easy to understand?
Where in your home would you keep this booklet?
How did you feel about this booklet overall?
Behavioral
Capability
A mother possesses a level of knowledge
about the prenatal period. If she is aware of certain healthy or unhealthy behaviors
prior to pregnancy, she can prevent poor birth outcomes by practicing the appropriate behavior.
Which sections of this book
would be most useful to a new parent?
Which sections of this booklet were not useful or difficult to
understand?
How helpful did you find the
content of the booklet?
Expectations By observing others and learning from educational resources, a mother can associate behaviors with birth outcomes.
This association can help her set goals to increase the likelihood of a healthy
infant.
What topics should be addressed in a pregnancy program?
What other topics should be included in this booklet?
Self-efficacy This construct encompasses a mother’s motivation and confidence to learn
healthy behaviors and comply with her provider’s recommendations, therefore decreasing the risk of preterm birth.
Would you use this booklet throughout your pregnancy?
How has reading this booklet changed your confidence to
manage your pregnancy or care for your infant
Observational learning
(Modeling)
Many behaviors unique to pregnancy are learned from family, friends, and other
resources during the pregnancy. By adopting these behaviors, a mother can
have a healthier pregnancy.
Are the pictures in this booklet
helpful to understanding the material?
Did you learn anything new or
useful from this booklet?
Reinforcements A behavior can generate positive or negative consequences which can
encourage or deter the mother from continuing that behavior. By learning
what consequences are associated with her own behaviors, a mother can build confidence to remain healthy during her
pregnancy.
Would you participate in a
pregnancy management program in order to receive this booklet?

31
Table 3: Characteristics of Urban Focus Group Participants
Headquarters Building
Assigned Number 1 2 3 4
Age 32 34 32 25
Race Caucasian African American African American Caucasian
Pregnant or Recently
Delivered
Pregnant Pregnant Pregnant Recently Delivered
Highest Level of
Education
College Graduate Graduate Degree Some College Some College
Relationship Status Married Married Married Married
Living Situation Husband Husband Husband Husband
Number of Children 1 1 0 1
Customer Service Building
Assigned Number 1 2 3 4
Age 40 33 33 33
Race Caucasian African American Asian African American
Pregnant or Recently
Delivered
Recently Delivered Pregnant Pregnant Pregnant
Highest Level of
Education
Masters Degree College Graduate Some College College Graduate
Relationship Status Married Single Married Married
Living Situation Husband Single Husband Husband
Number of Children 1 1 1 0

32
Table 4: Characteristics of Educational Booklets
Title Number
of Pages
Prenatal or
Postpartum
Period
Topics Covered
Nutrition and
Exercise
Common
Discomforts
Doctors Appointments
and Testing
Baby’s
Development
Complications and Preterm
Labor Risks
Labor and
Delivery
Breastfeeding Postpartum Depression
and Care
Immunizations Interactive
Sections
Great Expectations
64 Prenatal
Planning A Healthy
Pregnancy
31 Prenatal
Great
Beginnings
Start Before
Birth
23 Prenatal
The Joy of
Parenthood 104 Postpartum
A New
Beginning 45 Postpartum
Caring for
Your Baby 31 Postpartum

33
Table 5: Survey Questions, Urban Focus Group Sessions
In order for us to ensure the diversity of this focus group, we have included questions about your personal background. Your responses to these questions are CONFIDENTIAL and will be used
for comparison purposes only. Age:
Pregnant or Delivered within last 6 months:
Highest level of Education:
Race:
Relationship Status:
Living Situation (who lives in your household):
Number of Children:
Table 6: Interview Guide for Corporate Focus Group Sessions
1. What topics should be addressed in a pregnancy program?
2. What was your initial reaction to this booklet? 3. What did you think of the length of the booklet? 4. Approximately how long did you spend reviewing this booklet?
5. Where in your home would you keep this booklet? 6. Was the educational material easy to understand?
7. Are the pictures in this booklet helpful to understanding the material? 8. How helpful did you find the content of the booklet? 9. Which sections of this book would be most useful to a new parent?
10. Which sections of this booklet were not useful or difficult to understand? 11. Would you participate in a pregnancy management program in order to receive this
booklet? 12. Would you use this booklet throughout your pregnancy? 13. What did you like the most about this booklet?
14. What other topics should be included in this booklet? 15. Did you learn anything new or useful from this booklet?
16. How do you feel about this booklet overall? 17. How has reading this booklet changed your confidence to manage your pregnancy or care
for your infant?

34
References
1 NCHS Data Brief. No. 9. Oct 2008. Recent Trends in Infant Mortality in the United States National Center for
Health Statistics. Accessed 9/1/09. <http://www.cdc.gov/nchs/data/databriefs/db09.htm>. 2 National Center for Health Statistics. State Profile: North Carolina. Accessed 9/1/09.
<http://www.cdc.gov/nchs/pressroom/data/state_profile_NC.htm>. 3 National Center for Health Statistics. State Profile: North Carolina. Accessed 9/1/09.
<http://www.cdc.gov/nchs/pressroom/data/state_profile_NC.htm>. 4 The Mayo Clinic. Complications. Accessed 9/1/09. < http://www.mayoclinic.com/health/premature-
birth/DS00137/DSECTION=complications>. 5 Healthy People 2010. Objective 16:Maternal, Infant, and Child Health. Accessed 9/1/09.
<http://www.healthypeople.gov/document/HTML/Volume2/16MICH.htm>.
6 Washington, AE. Ectopic pregnancy in the United States: Economic Consequences and Payment Source Trends.
Obstetrics and Gynecology. 1993 Feb;81(2):287-92. 7 Centers for Disease Control and Prevention. Safe Motherhood: Promoting health for women before, during, and
after pregnancy. Accessed 9/3/09. <http://www.cdc.gov/nccdphp/publications/aag/pdf/drh.pdf>. 8 Adams, E. K., et al. "Costs of Poor Birth Outcomes among Privately Insured." Journal of Health Care Finance
29.3 (2003): 11-27. 9 Adams, E. K., et al. "Costs of Poor Birth Outcomes among Privately Insured." Journal of Health Care Finance
29.3 (2003): 11-27. 10 Adams, E. K., et al. "Costs of Poor Birth Outcomes among Privately Insured." Journal of Health Care Finance
29.3 (2003): 11-27. 11 Williams, K.J. Williams, K. J., A. Zolotor, and L. Kaufmann. "Clinical Inquiries: Does Group Prenatal Care
Improve Pregnancy Outcomes?" The Journal of Family Practice 58.7 (2009): 384a-c. 12 Beard, J. R., et al. "Socioeconomic and Maternal Determinants of Small-for-Gestational Age Births: Patterns of
Increasing Disparity." Acta Obstetricia et Gynecologica Scandinavica 88.5 (2009): 575-83. 13 Dumas, L. "Focus Groups to Reveal Parents' Needs for Prenatal Education." The Journal of Perinatal Education:
An ASPO/Lamaze Publication 11.3 (2002): 1-9. 14 Jesse, D. E., et al. "Racial Disparities in Biopsychosocial Factors and Spontaneous Preterm Birth among Rural
Low-Income Women." Journal of Midwifery & Women's Health 54.1 (2009): 35-42. 15 Jesse, D. E., et al. "Racial Disparities in Biopsychosocial Factors and Spontaneous Preterm Birth among Rural
Low-Income Women." Journal of Midwifery & Women's Health 54.1 (2009): 35-42. 16 Long SH, Marquis MS. 1998. “The Effects of Florida’s Medicaid Eligibility Expansion for Pregnant Women.”
American Journal of Public Health 88(3):371-376. 17 Jesse, D. E., et al. "Racial Disparities in Biopsychosocial Factors and Spontaneous Preterm Birth among Rural
Low-Income Women." Journal of Midwifery & Women's Health 54.1 (2009): 35-42. 18 National Cancer Institute. Theory at a Glance: A Guide for Health Promotion Practice . US Department of
Health and Human Services. Pages 12-15. Sept. 2005 19 March of Dimes. Quick Reference Facts Sheets: Smoking During Pregnancy. Accessed 9/8/09.
<http://www.marchofdimes.com/professionals/14332_1171.asp> 20 March of Dimes. Quick Reference Facts Sheets: Smoking During Pregnancy. Accessed 9/8/09.
<http://www.marchofdimes.com/professionals/14332_1171.asp> 21 American Academy of Pediatrics and American College of Obstetricians and Gynecologists. Guidelines for
Perinatal Care. 6th Ed. Chapter 4: Antepartum Care. 22 NVivo 8. Qualitative Solutions and Research International. January 2010.

35
Appendix A: Codebook
Code Subcode Description Inclusion Criteria Exclusion Criteria
Pregnanc
yManage
ment
A statement about the content
of a booklet which impacts the
mother’s ability to manage her
pregnancy or care for her infant
Any statement which regards
the content of the booklet with
respect to the mother’s ability
to manage her pregnancy or
care for her infant
Any statement which does not
describe the mother’s ability to
manage her pregnancy or care
for her infant
PM/Incre
ase
A statement about the content
of a booklet which can
increase confidence in
managing pregnancy or caring for a child
Any statement which reveals an
increase in confidence for
managing pregnancy or caring
for an infant resulting from the information presented in a
booklet
Any statement which reveals a
decrease or no change in
confidence for managing
pregnancy or caring for an infant resulting from the
information presented in a
booklet
PM/Decr
ease
A statement about the content
of a booklet which can
decrease confidence in
managing pregnancy or caring
for an infant
Any statement which reveals a
decrease in confidence for
managing pregnancy or caring
for an infant resulting from the
information presented in a booklet
Any statement which reveals an
increase or no change in
confidence for managing
pregnancy or caring for an
infant resulting from the information presented in a
booklet
NoChange
A statement revealing no change in confidence to
manage pregnancy or care for
an infant
Any statement which reveals the content of the booklet did
not impact the mother’s
confidence in managing her
pregnancy or caring for her
infant
Any statement which reveals increase or decrease in
confidence for managing
pregnancy or caring for an
infant resulting from the
information presented in a booklet
Length A statement which describes
the length of the booklet
Any statement which describes
the length, size, or time taken to review a booklet
Any statement which does not
describe the length, size, or time taken to review a booklet
Length/L
ong
A statement that the booklet is
too long or too large
Any statement which reveals
that the book is too large or
long to read
Any statement that the booklet
is too short, small, or of
appropriate size
Length/S
hort
A statement that the booklet is
too short or too small
Any statement which reveals
the booklet is too small or too
short
Any statement that the booklet
is too long, large, or of
appropriate size
Length/A
ppropriat
e
A statement that the booklet is
of appropriate length size
Any statement which reveals
the booklet is an appropriate
length for the reader and topic
Any statement that the booklet
is too long, large, short, or
small
Breastfee
ding
A reference to breastfeeding Any statement about
breastfeeding
Statement being described with
other types of feeding
techniques or does not
reference breastfeeding
Breastfee
ding
/Technique
A question or statement about
how to breastfeed correctly
Statement references proper
technique or frequency of
feedings
Statement does not reference
technique or frequency of
feedings
Breastfee
ding /PositiveP
ressure
A reference to the benefits of
breastfeeding instead of bottlefeeding
Statement encourages
individual to breastfeed
Statement discourages
individual from breastfeeding
Breastfee
ding /Negative
Pressure
A reference to societal or
personal pressure to breastfeed instead of bottlefeed and any
personal feelings of guilt for
not being able to breastfeed
Statement discourages
individual from breastfeeding
Statement encourages
individual to breastfeed

36
Breastvsb
ottle
A statement about deciding to
breastfeed or bottlefeed and the
benefits and drawbacks of each one
Any statement which references
both breast and bottlefeeding
Statements about each
breastfeeding or bottle feeding
without reference the other
Bottlefee
ding
A reference to bottlefeeding Any statement about
bottlefeeding
Statement being described with
other types of feeding
techniques
Bottlefee
ding
/Technique
A question or statement about
how to bottlefeed correctly
Any statement which references
proper technique or frequency
of feedings
Any statement which does not
reference technique or
frequency of feedings
Visual
Content
A statement about the visual
content or appearance of a booklet
Any statement about the color,
layout, pictures, or appearance of a booklet
Any statement which does not
refer to color, layout, pictures, or appearance
Visual/Po
sitive
A positive statement about the
visual content
Any positive statement about
the visual content
Any negative statement about
the visual content
Visual/Ne
gative
A negative statement about the
visual content
Any negative statement about
the visual content
Any positive statement about
the visual content
Visual/Sp
ecific
Desires
Any statement concerning a
desire for some specific visual
component
Any statement concerning a
desire for some specific visual
component
Any statement that does not
refer to a desire for specific
visual components
Interactivity
Any statement about the usefulness of interactive
sections of a booklet
Any statement about the usefulness of interactive
sections of a booklet
Statement does not refer to interactive sections of a booklet
Interact/Positive
A positive statement about an interactive section
Any positive statement about an interactive section
Any negative statement about an interactive section
Interact/N
egative
A negative statement about an
interactive section
Any negative statement about
an interactive section
Any positive statement about
an interactive section
Quality
of
Information
A statement regarding the
quality or comprehensiveness
or the information presented in a booklet
Any statement regarding the
quality or comprehensiveness
or the information presented in a booklet
Any statement which does not
refer to the quality or
comprehensiveness presented in a booklet
Quality/R
einforcer
A statement which reveals
information presented in a
booklet that reinforces something previously known
Any statement which infers
information presented is known
but reinforces knowledge
Any statement which infers
information presented in
booklet is new or not useful
Quality/N
ew
A statement which references
new information learned from a booklet
Any statement which infers
information presented is novel
Any statement which infers
information presented is known or not useful
Quality/N
one
A statement which references t
information presented in a booklet which is regarded as
not useful
Any statement which infers
information presented is not useful
Any statement which infers
information presented is novel or reinforces knowledge
Quality/P
ositive
A statement which reveals
information presented in a booklet is useful
Any statement which infers
information presented is generally useful
Any statement which infers
information presented is not useful; Any statement that
infers information is useful and
either new or reinforcement
Father
Involvem
ent
A statement about the
father/husband/significant
other’s role in prenatal,
postpartum, and child care
Any statement which references
father/husband/significant other
Any statement which does not
reference
father/husband/significant other
OBGYN A statement about OBGYNs,
issues pertaining to prenatal
visits or responsibilities of the
OBGYN
Any statement which pertains
to OBYGNs, prenatal visits or
responsibilities of the OBGYN
Any statement which does not
pertain to OBGYN, prenatal
visits, or OBYGN
responsibilities
Pediatrici
an
A statement pertaining to
pediatric visits or a
pediatrician’s responsibilities
Any statement which pertains
to pediatric visits or a
pediatrician’s responsibilities
Any statement which does not
pertain to pediatric visits or a
pediatrician’s responsibilities

37
PrenatalC
are
A statement pertaining to the
prenatal period and prenatal
care issues
Any statement pertaining to the
prenatal period and prenatal
care issues
Any statement which does not
pertain to the prenatal period
and prenatal care issues
Prenatal/
Maternal
A statement pertaining to
maternal health issues during
the prenatal period
Any statement pertaining to
maternal health issues during
the prenatal period
Any statement which does not
pertain to maternal health
issues during the prenatal
period
Paternal/f
etal
A statement pertaining to fetal
health and development issues
during the prenatal period
Any statement which pertains
to fetal health and development
issues during the prenatal period
Any statement which does not
pertain to fetal health and
development issues during the prenatal period
Postpartu
mCare
A statement pertaining to the
mother’s health during the postpartum period
Any statement which pertains
to the mother’s health during the postpartum period
Any statement which does not
pertain to the mother’s health during the postpartum period
Postpartu
m/Mental
A statement pertaining to the
mother ’s mental health in the
postpartum period
Any statement which pertains
to the mother’s mental health
during the postpartum period
Any statement which does not
pertain to the mother’s mental
health during the postpartum period
Postpartu
m/Physical
A statement pertaining to the
mother’s physical care and healing process during the
postpartum period
Any statement which pertains
to the mother’s physical health during the postpartum period
Any statement which does not
pertain to the mother’s physical health during the postpartum
period
ChildDevelopment
A statement about the child’s development after birth
Any statement which pertains to the child’s development after
birth
Any statement which does not pertain to the child’s
development after birth
ChildDev
/Mental
A statement pertaining to the
child’s mental health and development after birth
Any statement pertaining to the
child’s mental health and development after birth
Any statement which does not
pertain to the child’s mental health and development after
birth
ChildDev/Physical
A statement pertaining to the child’s physical health and
development after birth
Any statement pertaining to the child’s physical health and
development after birth
Any statement which does not pertain to the child’s physical
health and development after
birth
Topics A statement which refers to
topics of interest
Any statement referring to
specific topics that respondents
would like information to
address
Any statement which does not
refer to specific topics of
interest









