Embed Size (px)
Citation preview

MERIT STUDY
Jack Chen MBBS PhDAnnual Health Service Research Meeting, 26-28 June 2005 Boston

Background
• Hospitals are unsafe places
• Most patients who suffer adverse outcomes have documented deterioration
• Medical Emergency Team system educates and empowers staff to call a skilled team in response to specific criteria or if “worried”
• Team is called by group pager and responds immediately

MEDICAL EMERGENCY TEAM (MET) CONCEPT
• Criteria identifying seriously ill early
• Rapid response to those patients (similar to a cardiac arrest team)
• Resuscitation and triage

MET Calling Criteria

M.E.R.I.T Study
Medical Early Response Intervention AND
Therapy

Terminology• CAT - Cardiac arrest team
• NFR - Not for resuscitation (DNR, DNAR)
• Events - – Deaths without NFR– Cardiac arrests without NFR– Unplanned ICU admissions – MET and CAT calls independent of above

PRIMARY AIM
• The primary aim of this study was to test the hypothesis that the implementation of the hospital-wide MET system will reduce the aggregate incidence of:
– Unplanned ICU admissions (mainly general wards)
– Cardiac Arrests (-NFR) – Unexpected deaths (-NFR)

STUDY SAMPLE & SAMPLE SIZE:
(at design stage)
• 23 hospitals with at least 20,000 estimated admissions per year
• This will provide us with a 90% chance to detect a 30% reduction in the incidence at the significant level of 5%
Kerry & Bland (1998)
CLUSTER RANDOMISED TRIAL
• More complex to design• More participants to obtain equivalent statistical
power• Key determinants are number of individual units;
the intracluster correlation; and cluster size• More complex analysis than ordinary randomised
trial• Randomised at one time, rather than one at a
time
FRAMEWORK FOR DESIGN, ANALYSIS & REPORTING
CONSORT STATEMENT: extension to cluster randomised
trials
BMJ 2004;328:702
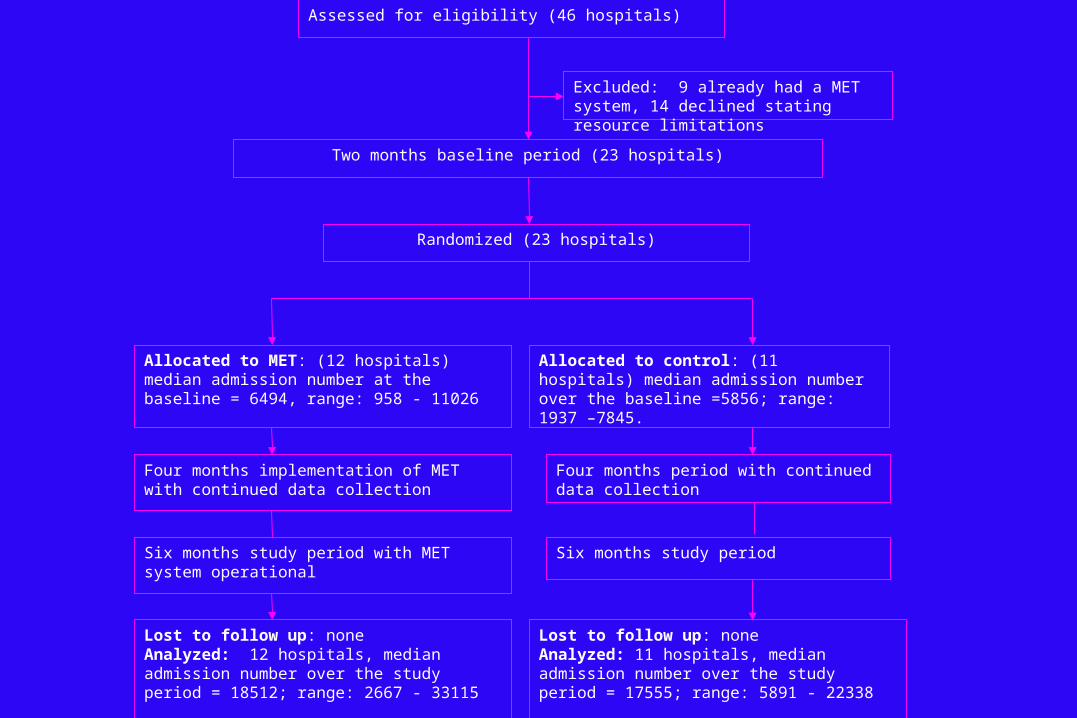
Assessed for eligibility (46 hospitals)
Excluded: 9 already had a MET system, 14 declined stating resource limitations
Randomized (23 hospitals)
Two months baseline period (23 hospitals)
Allocated to MET: (12 hospitals) median admission number at the baseline = 6494, range: 958 - 11026
Allocated to control: (11 hospitals) median admission number over the baseline =5856; range: 1937 –7845.
Lost to follow up: noneAnalyzed: 12 hospitals, median admission number over the study period = 18512; range: 2667 - 33115
Lost to follow up: noneAnalyzed: 11 hospitals, median admission number over the study period = 17555; range: 5891 - 22338
Four months implementation of MET with continued data collection
Four months period with continued data collection
Six months study period with MET system operational Six months study period

RANDOMISATION
• Stratified – blocked randomisation (4) based on teaching hospital status
• Independent statistician

DATA COLLECTION
• 18178 EVENT forms
• 2418 corrections (13.3%)
• Final EVENTS - 13142 after third round data consistency and logic checking
• In-patients – 750,000

DATA COLLECTION • Log books• Scannable technology • Photocopy forms kept by hospital• Filing of forms and storage in Simpson
Centre• Web-based tracking data• 4 databases• Separate neutral data repository
DATA CORRECTION LOOP
• 10 step standardised data entry and correction procedure
• Weekly data entry meeting between statistician, data manager, IT manager and research assistants
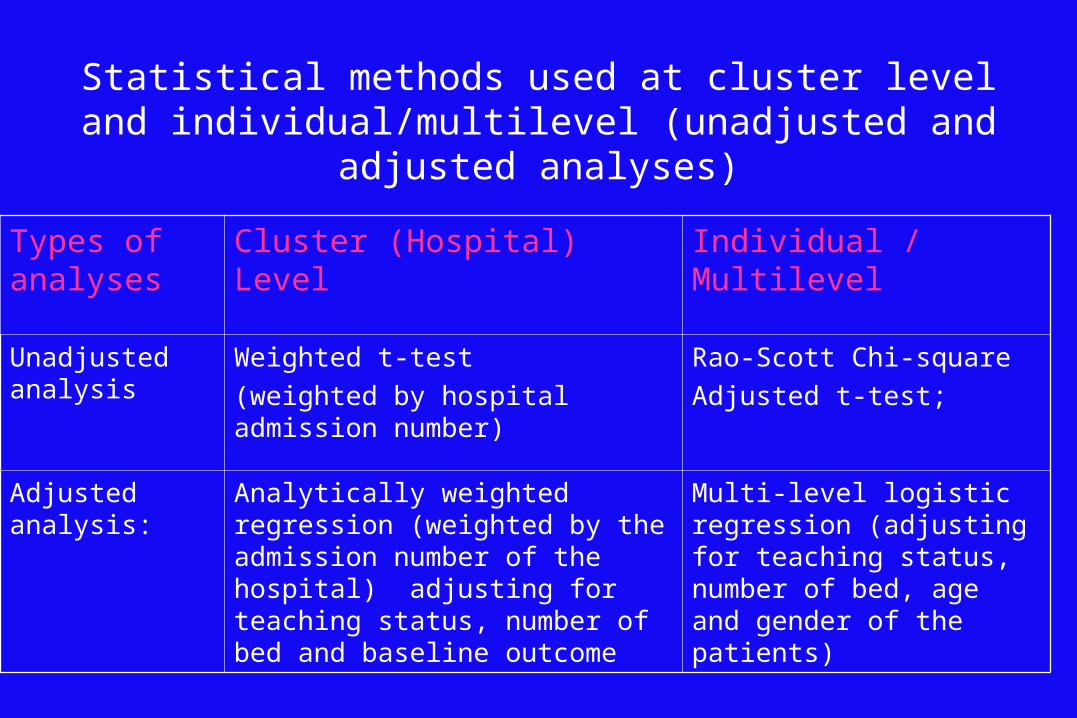
Types of analyses
Cluster (Hospital) Level Individual / Multilevel
Unadjusted analysis
Weighted t-test
(weighted by hospital admission number)
Rao-Scott Chi-square
Adjusted t-test;
Adjusted analysis: Analytically weighted regression (weighted by the admission number of the hospital) adjusting for teaching status, number of bed and baseline outcome
Multi-level logistic regression (adjusting for teaching status, number of bed, age and gender of the patients)
Statistical methods used at cluster level and individual/multilevel (unadjusted and adjusted analyses)

WEIGHTING AND ADJUSTMENT
• Weighting: by the number of admissions during the study period
• Cluster Adjustment for: teaching hospital status, bed size and baseline outcome variables, with hospitals weighted by the number of admissions during the study period
• Multilevel model adjustment for: teaching hospital status, bed size, age and gender of the patients
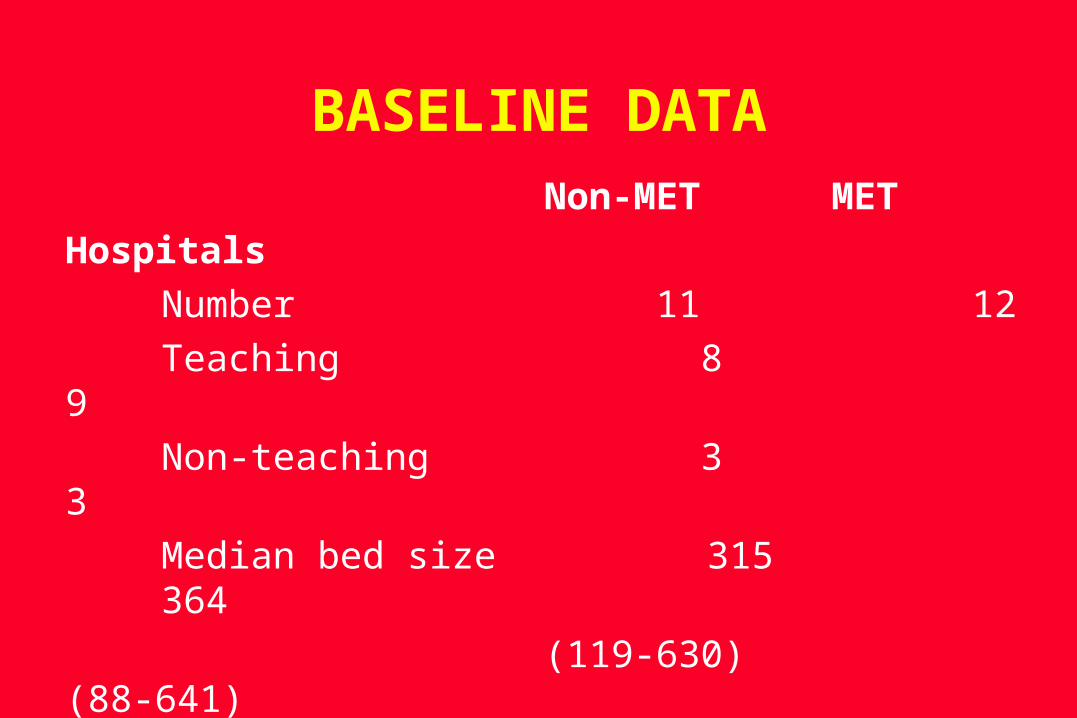
BASELINE DATANon-MET MET
Hospitals
Number 11 12
Teaching 8 9
Non-teaching 3 3
Median bed size 315 364
(119-630) (88-641)

BASELINE DATA
Outcomes (incidence rate/ Non-MET MET
1000 admissions)
Primary Outcome 6.775 6.291
Cardiac arrests (- NFR) 2.606 1.597Unplanned ICU admissions 4.132 4.267
Unexpected deaths (- NFR) 1.605 1.648
No significant differences

RESULTS - DIFFERENCE BETWEEN MET & NON-MET HOSPITALS
Incidence Rate/1000 admissions
OUTCOMES NON-MET
MET % AGE CHANGE
P
Primary outcome 5.860 5.306 10% 0.804
Cardiac arrest – NFR 1.640 1.31 25.1% 0.306
Unplanned ICU admission
4.683 4.185 12% 0.899
Unexpected deaths (– NFR)
1.175 1.063 10% 0.564
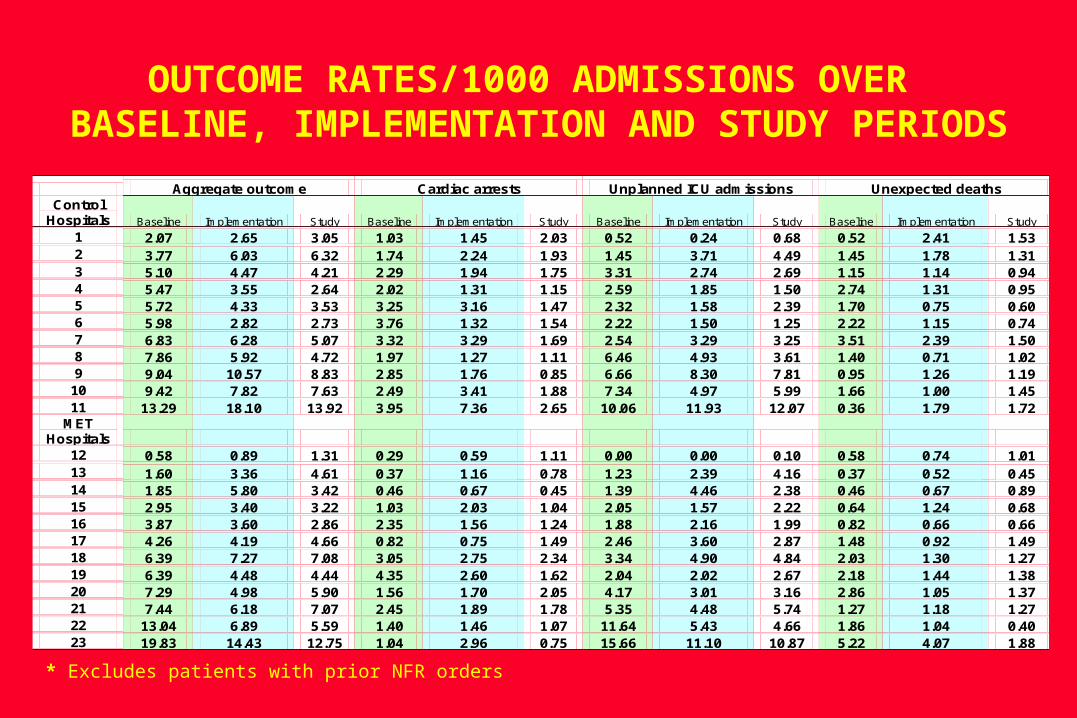
OUTCOME RATES/1000 ADMISSIONS OVER BASELINE, IMPLEMENTATION AND STUDY PERIODS
Aggregate outcome Cardiac arrests Unplanned ICU admissions Unexpected deaths Control
Hospitals Baseline Implementation Study Baseline Implementation Study Baseline Implementation Study Baseline Implementation Study
1 2.07 2.65 3.05 1.03 1.45 2.03 0.52 0.24 0.68 0.52 2.41 1.53 2 3.77 6.03 6.32 1.74 2.24 1.93 1.45 3.71 4.49 1.45 1.78 1.31 3 5.10 4.47 4.21 2.29 1.94 1.75 3.31 2.74 2.69 1.15 1.14 0.94 4 5.47 3.55 2.64 2.02 1.31 1.15 2.59 1.85 1.50 2.74 1.31 0.95 5 5.72 4.33 3.53 3.25 3.16 1.47 2.32 1.58 2.39 1.70 0.75 0.60 6 5.98 2.82 2.73 3.76 1.32 1.54 2.22 1.50 1.25 2.22 1.15 0.74 7 6.83 6.28 5.07 3.32 3.29 1.69 2.54 3.29 3.25 3.51 2.39 1.50 8 7.86 5.92 4.72 1.97 1.27 1.11 6.46 4.93 3.61 1.40 0.71 1.02 9 9.04 10.57 8.83 2.85 1.76 0.85 6.66 8.30 7.81 0.95 1.26 1.19
10 9.42 7.82 7.63 2.49 3.41 1.88 7.34 4.97 5.99 1.66 1.00 1.45 11 13.29 18.10 13.92 3.95 7.36 2.65 10.06 11.93 12.07 0.36 1.79 1.72
MET Hospitals
12 0.58 0.89 1.31 0.29 0.59 1.11 0.00 0.00 0.10 0.58 0.74 1.01 13 1.60 3.36 4.61 0.37 1.16 0.78 1.23 2.39 4.16 0.37 0.52 0.45 14 1.85 5.80 3.42 0.46 0.67 0.45 1.39 4.46 2.38 0.46 0.67 0.89 15 2.95 3.40 3.22 1.03 2.03 1.04 2.05 1.57 2.22 0.64 1.24 0.68 16 3.87 3.60 2.86 2.35 1.56 1.24 1.88 2.16 1.99 0.82 0.66 0.66 17 4.26 4.19 4.66 0.82 0.75 1.49 2.46 3.60 2.87 1.48 0.92 1.49 18 6.39 7.27 7.08 3.05 2.75 2.34 3.34 4.90 4.84 2.03 1.30 1.27 19 6.39 4.48 4.44 4.35 2.60 1.62 2.04 2.02 2.67 2.18 1.44 1.38 20 7.29 4.98 5.90 1.56 1.70 2.05 4.17 3.01 3.16 2.86 1.05 1.37 21 7.44 6.18 7.07 2.45 1.89 1.78 5.35 4.48 5.74 1.27 1.18 1.27 22 13.04 6.89 5.59 1.40 1.46 1.07 11.64 5.43 4.66 1.86 1.04 0.40 23 19.83 14.43 12.75 1.04 2.96 0.75 15.66 11.10 10.87 5.22 4.07 1.88
* Excludes patients with prior NFR orders

CALLING RATE/HOSPITAL/1,000 ADMISSIONS
CONTROL HOSPITALS MET HOSPITALS p
3.1 (1.5-5.8) 8.7 (3.5-16.5) <0.001

CALLS NOT ASSOCIATED WITH AN EVENT/1,000 ADMISSIONS
CONTROL MET HOSPITALS HOSPITALS p
1.2 (0-3.3) 6.3 (2.5-11.2) <0.001
194/528 (36.7%) 1329/1886 (70.5%) <0.001
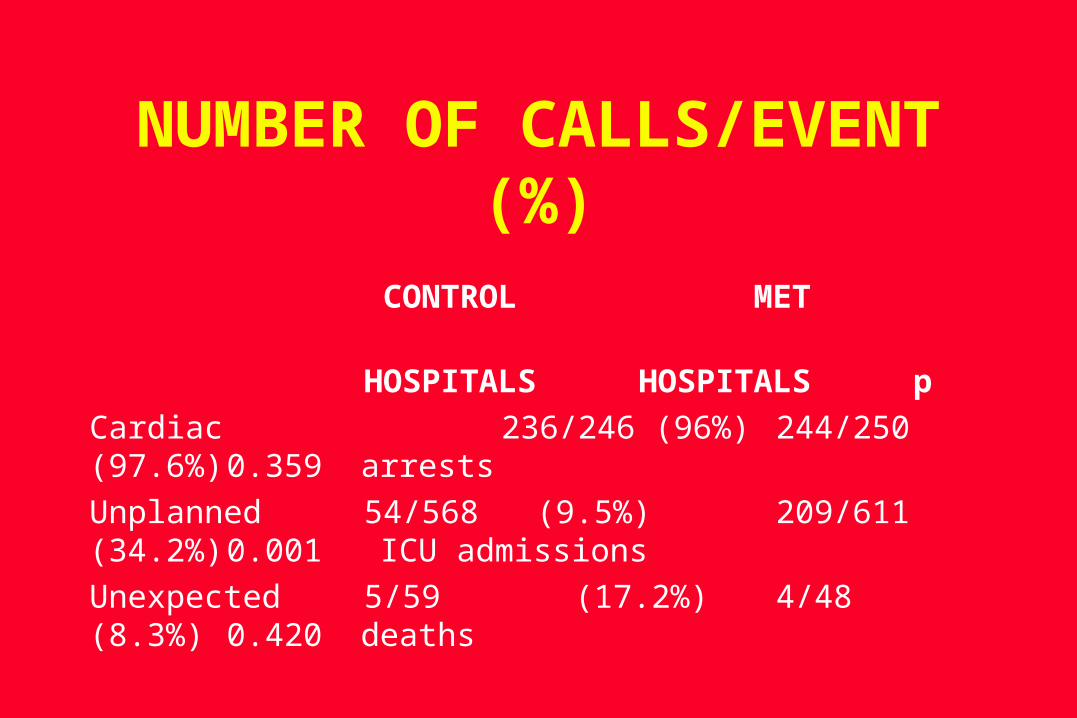
NUMBER OF CALLS/EVENT (%)
CONTROL MET
HOSPITALS HOSPITALS p
Cardiac 236/246 (96%) 244/250 (97.6%) 0.359 arrests
Unplanned 54/568 (9.5%) 209/611 (34.2%) 0.001 ICU admissions
Unexpected 5/59 (17.2%) 4/48 (8.3%) 0.420 deaths

EVENTS WHICH HAD MET CRITERIA BEFOREHAND (<15 min)
CONTROL MET
HOSPITALS HOSPITALS p
Cardiac 130/246 (53%) 115/250 (46%) 0.664 arrests
Unplanned ICU 121/568 (21%) 219/611 (36%) 0.090 admissions
Unexpected 10/29 (35%) 12/48 (25%) 0.473 deaths

EVENTS WHICH HAD MET CRITERIA BEFOREHAND (>15 min)
CONTROL MET
HOSPITALS HOSPITALS p
Cardiac 109/246 (44%) 76/250 (30%) 0.031 arrests
Unplanned ICU 314/568 (55%) 313/611 (51%) 0.596 admissions
Unexpected 16/29 (55%) 24/58 (50%) 0.660 deaths

CALLS WHEN MET CRITERIA WERE PRESENT (<15 min before event)
CONTROL MET
HOSPITALS HOSPITALS p
Cardiac 124/130 (95%) 112/115 (97%) 0.545 arrests
Unplanned ICU 28/121 (23%) 112/219 (51%) 0.049 admissions
Unexpected 4/16 (25%) 2/12 (17%) 0.298 deaths

CALLS WHEN MET CRITERIA WERE PRESENT (>15 min before event)
CONTROL MET
HOSPITALS HOSPITALS p
Cardiac 104/109 (95%) 72/76 (95%) 0.874 arrests
Unplanned ICU 27/314 (9%) 95/313 (30%) 0.009 admissions
Unexpected 4/16 (25%) 2/24 (8%) 0.231 deaths

NFR DESIGNATIONNon-MET MET
Prior NFR/1000 admissions 9.404 9.434
Prior NFR/Deaths 1.01 1.05
NFR made at time of event/
1000 admissions 0.274 0.799
NFR made at time of event/
1000 events 17.189 38.424

NFR ORDERS IN CALLS NOT ASSOCIATED WITH AN EVENT
CONTROL MET
HOSPITALS HOSPITALS p
6/197 (3%) 106/1332 (8%) 0.048

DIFFERENCES BETWEEN BASELINE AND STUDY PERIOD/1,000
ADMISSIONS (%)
p
Primary outcome -0.85 (13%) 0.089
Cardiac arrests -0.68 (33%) 0.003
Unplanned ICU -0.23 (5%) 0.577
admission
Unexpected deaths -0.48 (30%) 0.010
IN SUMMARY• Randomisation was successful and
appeared balanced
• Call rate was much higher in MET hospitals mostly due to calls not associated with events
• More of these event-free calls led to NFR orders in MET hospitals, but overall NFR rate was unaffected

IN SUMMARY• There was no STATISTICALLY SIGNIFICANT
decrease in the incidence of the primary outcome in MET hospitals
• There was no STATISTICALLY SIGNIFICANT decrease in the incidence of the secondary outcomes in MET hospitals
• WHEN ALL HOSPITALS CONSIDERED TOGETHER, The incidence of cardiac arrests and unexpected deaths decreased from baseline to study period
IN SUMMARYIf MET criteria were
documented and followed by an event, only a minority of
patients overall had an actual MET call made

IN SUMMARYThere was an increase in calls before ICU admission in MET
hospitals but not before cardiac arrests or unexpected
deaths
IN SUMMARY
Less than half of all events had MET
criteria documented beforehand

IN SUMMARY36.7% of all cardiac
arrest calls were not in response to an event

IN SUMMARY
Extreme variability in event rates amongst
hospitals

IN SUMMARY23 hospitals – needed >100 to
show a difference• Estimated primary outcome incidence
3% - actual rate 0.57%
• Between hospital variability high
• Intra-class correlation co-efficient high

Why no significant improvement ?•The MET may be ineffective;
•The implementation is less optimal;
•The participating hospitals are unrepresentative;
•We studied wrong outcome;
•The documentation of the vital signs is poor;
•The calling rate is low given the existing calling criteria;
•The contamination;
•The low statistical power

CONCLUSIONS• First large hospital system change trial ever
conducted according to rigorous principles of design and statistical analysis
• It encompassed close to 750,000 admissions• Although we did not demonstrate a significant
difference in the primary outcome, the study produced a large body of useful data on patient care, documentation and outcomes, which will hopefully illuminate future studies

MERIT STUDY
CONDUCTED BY:Simpson Centre for Health Services Research
ANZICS Clinical Trials Group
FUNDED BY:NHMRC
Australian COUNCIL FOR Quality and Safety in Health Care (AQSHC)

MERIT STUDY
MANAGEMENT COMMITTEEProf. Ken Hillman (Chair) Prof. Rinaldo Bellomo Mr. Daniel BrownDr. Jack ChenDr. Michelle CretikosDr. Gordon DoigDr. Simon FinferDr. Arthas Flabouris
PARTICIPATING HOSPITALS, INVESTIGATORS & RESEARCH NURSES
• Bendigo – John Edington, Kath Payne• Box Hill – David Ernest, Angela Hamilton• Broken Hill – Coral Bennet, Linda Peel,
Mathew Oliver, Russell Schedlich, Sittampalam Ragavan, Linda Lynott
• Calvery – Marielle Ruigrok, Margaret Willshire,
• Canberra – Imogen Mitchell, John Gowardman, David Elliot, Gillian Turner, Carolyn Pain
• Flinders – Gerard O’Callaghan, Tamara Hunt• Geelong – David Green, Jill Mann, Gary
Prisco• Gosford – Sean Kelly, John Albury• John Hunter – Ken Havill, Jane O’Brien• Mackay – Kathryn Crane, Judy Struik• Monash – Ramesh Nagappan, Laura Lister
• Prince of Wales – Yahya Shahabi, Harriet Adamsion
• Queen Elizabeth – Sandy Peake, Jonathan Foote
• Redcliffe – Neil Widdicombe, Matthys Campher, Sharon Ragou, Raymond Johnson
• Redland – David Miller, Susan Carney• Repatriation General – Gerard O’Callaghan,
Vicki Robb• Royal Adelaide – Marianne Chapman, Peter
Sharley, Deb Herewane, Sandy Jansen• Royal North Shore - Simon Finfer, Simeon Dale• St. Vincent’s – John Santamaria, Jenny Holmes• Townsville – Michael Corkeron, Michelle
Barrett, Sue Walters• Wangaratta – Chris Giles, Deb Hobijn • Wollongong - Sunny Rachakonda, Kathy
Rhodes• Wyong – Sean Kelly, John Albury




![ÁÁÁX µ Ç]v l] vX]v(} - Study in Pakistan Merit List of Candidates for admission in MBBS at KIMS against OPEN MERIT seats in session 2016-2017](https://img.dokumen.tips/doc/110x75/5ae77a117f8b9a6d4f8e2324/x-v-l-vxv-study-in-merit-list-of-candidates-for-admission-in-mbbs-at-kims.jpg)























![ÁÁÁX µ Ç]v l] vX]v(} · Provisional Merit List of Candidates for admission in MBBS at KIMS against OPEN MERIT seats in session 2016-2017](https://img.dokumen.tips/doc/110x75/5f0a69327e708231d42b8033/x-v-l-vxv-provisional-merit-list-of-candidates-for-admission-in.jpg)