Embed Size (px)
Citation preview

Men & Cancer Scotland
Professor Alan WhiteCentre for Men’s Health
Leeds Metropolitan [email protected]
www.leedsmet.ac.uk/health/menshealth


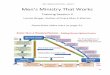
Comparison of the ratio of total deaths of men and women across the major disease classification groups, age brackets 1 to 24, 25 to 74 and 75+ years
0.00.51.01.52.02.53.03.54.04.5
Men
tal
diso
rder
s
Ext
erna
l cau
ses
Gen
itour
inar
ysy
stem
Dig
estiv
esy
stem
Circ
ulat
ory
syst
em
Res
pira
tory
syst
em
Neo
plas
ms
End
ocrin
e an
dm
etab
olic
Mus
culo
skel
etal
Rat
io
1_24
25_74
75+
White, AK & Cash, K (2003) The state of men’s health across 17 European Countries. Brussels, The European Men’s Health Forum

Median rate ratio between men and women across 44 countries for mortality from all causes, by age
White AK & Holmes M (2006) Patterns of morbidity across 44 Countries among
men and women aged 15-44. Journal of Men’s Health & Gender 3(2): 139-151
Age
75+65-74
55-64
45-54
35-44
25-34
15-24
5-141-4
5
4
3
2
1
0
Highest
Low est
Median

Death rates for Malignant Neoplasms, for men & women
Male
0
20
40
60
80
100
120
15 to 24 25 to 34 35 to 44
Ra
te p
er
10
0,0
00
Hungary 02
Thailand (00)
Romania 02
Armenia (02)
Portugal (02)
Latvia 02
Slovakia 00
Estonia 02
Lithuania 02
France 00
Hong Kong 00
Poland 02
Slovenia 02
Spain 01
Czech Rep
Denmark 99
Belgium 97
Argentina (01)
Greece 01
USA 00
Israel 99
Italy 01
New Zealand (00)
Brazil (00)
Chile
Australia (01)
Germany 01
UK 02
Netherlands 03
Austria 02
Canada 00
Norw ay (01)
Japan 02
Finland 02
Egypt 00
Sw eden 01
Female
0
20
40
60
80
100
120
15 to 24 25 to 34 35 to 44
Ra
te p
er
10
0,0
00
Hungary 02
Armenia (02)
Romania 02
Thailand (00)
Lithuania 02
Argentina (01)
Latvia 02
Slovakia 00
Denmark 99
New Zealand (00)
Poland 02
Portugal 02
Israel 99
Chile (01)
Belgium 97
Netherlands 03
Czech Rep 02
France 00
Brazil (00)
Estonia 02
UK 02
USA 00
Canada 00
Slovenia 02
Spain 01
Norw ay (01)
Italy 01
Australia (01)
Germany 01
Hong Kong 00
Austria
Greece 01
Japan 02
Finland 02
Sw eden 01
Egypt 00
Adapted from White & Holmes (2006)

Patterns of mortality in men and women, 15-44 years, UK, 2002
Males
0
5
10
15
20
25
30
35
40
45
15 to 24 25 to 34 35 to 44
Rat
e pe
r 10
0,00
0
Accidents and adverseeffects
Diseases of thecirculatory system
Malignant neoplasms
Suicide and self- inflictedinjury
Chronic liver disease andcirrhosis
Homicide and injurypurposely inflicted byother persons
Calculated from White, AK, Holmes, M, (2006) Patterns of mortality across 44 Countries among men and women aged 15-44. Journal of Men’s Health & Gender 3(2): 139-151
Females
0
5
10
15
20
25
30
35
40
45
15 to 24 25 to 34 35 to 44R
ate
per 1
00,0
00
Malignant neoplasms
Diseases of thecirculatory system
Accidents and adverseeffects
Suicide and self-inflicted injury
Chronic liver diseaseand cirrhosis
Homicide and injurypurposely inflicted byother persons

Patterns of mortality in men and women, 45-64years, UK, 2002
0
50
100
150
200
250
300
350
400
450
45 to 54 55 to 64
Rat
e pe
r 10
0,00
0
Malignant neoplasms
Diseases of the circulatorysystem
Chronic liver disease andcirrhosis
Accidents and adverseeffects
Suicide and self- inf lictedinjury
Homicide and injurypurposely inf licted by otherpersons
Calculated from WHOSIS Mortality Database
Males Females
0
50
100
150
200
250
300
350
400
450
45 to 54 55 to 64R
ate
per
100,
000
Malignant neoplasms
Diseases of the circulatorysystem
Chronic liver disease andcirrhosis
Accidents and adverseeffects
Suicide and self- inf lictedinjury
Homicide and injurypurposely inf licted by otherpersons

Proportion of cardiovascular disease, cancer and violence (injury and poisoning) within total causes of death; 3 years average (2001-
2003), EU 27 for Men
0%
20%
40%
60%
80%
100%
1-4
5-9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
485
+
Age Group
Pro
po
rtio
n
Other diseases
Injury and poisoning
Cancers
Other forms of cardiovascular diseases
Cerebrovascular diseases
Ischaemic heart disease
Vitozzi, L (2009) The status of health in the European Union: towards a healthier Europe.

Arriaga decomposition of changes in life expectancies,
EU15 average, 1990-2000 0
1-4
5-9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
5'-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
4
85+
0
5
10
15
20
25
30
35
%
Men
Women
Vitozzi, L (2009) The status of health in the European Union: towards a healthier Europe.

Contribution of change in mortality by circulatory diseases to changes in life expectancy at birth 1980-
2000, selected countries, for men
Change in life expectancy
As a % of change in life expectancy
Greece 0.5 19.1
Spain 2.4 67
France 1.1 34.7
Italy 2.6 43.2
Hungary 1 54.5
Netherlands 1.9 63.3
Austria 2.4 39
Poland 1.6 133.1
Portugal 1.6 36.1
Romania 0.1 -9.8
Sweden 2.8 61.2
United Kingdom 2.5 60.2
Norway 2.5 68.3
Vitozzi, L (2009) The status of health in the European Union: towards a healthier Europe.

Deaths due to selected cancers, for men and women,age 15 - 64 years, Scotland, 2008
Malignant neoplasm of liver and intrahepatic bile ducts
0
20
40
60
80
100
120
140
160
180
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
Oesophagus
-
10
20
30
40
50
60
70
80
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
Stomach
-
5
10
15
20
25
30
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
Colon & Rectrosigmoid junction
-
10
20
30
40
50
60
70
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
ISD Scotland (2009) http://www.isdscotland.org/isd/1508.html

Pancreas
-
5
10
15
20
25
30
35
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
Bronchus & lung
-
50
100
150
200
250
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
Brain
-
5
10
15
20
25
30
35
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
Bladder
-
5
10
15
20
25
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
ISD Scotland (2009) http://www.isdscotland.org/isd/1508.html

Calculated from Mortality statistics: cause. Review of the Registrar General ondeaths by cause, sex and age, in England and Wales, 2003 Series DH2 no.30
Malignant melanoma
-
1
2
3
4
5
6
7
8
9
10
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female Kidney, except renal pelvis
-
5
10
15
20
25
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
Non-Hodgkins lymphoma
-
5
10
15
20
25
30
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64
Male
Female
ISD Scotland (2009) http://www.isdscotland.org/isd/1508.html

Rate ratio of male to female cancer mortality, UK 2007
White, A, Thomson, C, Forman, D,(2009) The Excess burden of cancer in men, NCIN, London

Rate ratio of male to female cancer incidence, UK 2007
White, A, Thomson, C, Forman, D,(2009) The Excess burden of cancer in men, NCIN, London

ONS (2009) Cancer incidence and mortality in the United Kingdom and constituent countries, 2004–06

ONS (2009) Cancer incidence and mortality in the United Kingdom and constituent countries, 2004–06

ONS (2009) Cancer incidence and mortality in the United Kingdom and constituent countries, 2004–06

ONS (2009) Cancer incidence and mortality in the United Kingdom and constituent countries, 2004–06

Scotland had the highest overall mortality rates for both males and females, at 17 per cent
ONS (2009) Cancer incidence and mortality in the United Kingdom and constituent countries, 2004–06

In Scotland, the overall cancer mortality rates for both sexes were around 16 per cent higher than those for the UK as a whole, and the overall cancer incidence rates were 8 per cent higher.
ONS (2009) Cancer incidence and mortality in the United Kingdom and constituent countries, 2004–06

• The incidence of lung cancer was 34 per cent higher for males and 49 per cent higher for females than in the UK as a whole.
• The incidence of, and mortality from, other smoking-related cancers – oesophagus, lip, mouth and pharynx, and larynx – were also higher in Scotland than in the other countries of the UK.
• The incidence of prostate cancer was 14 per cent lower in Scotland than in the UK as a whole.

• The mortality rate for lung cancer in Scotland was 34 per cent higher for males and 48 per cent higher for females than in the UK as a whole.
• In males it was nearly three times the mortality rate for prostate cancer and in females it was 56 per cent higher than the mortality rate for breast cancer.
• Male mortality from colorectal cancer was 38 per cent higher in Scotland than in the UK and female
• Mortality from cancer of the kidney and stomach was 29 and 35 per cent higher, respectively.

Factors involved in the development of cancer in men
• Lifestyle (Martin-Moreno et al. 2008, White 2009)• Genetics (White 2009)• Knowledge of genetic links within families (Moynihan
& Huddart 2009) • Reduced uptake of available screening (Brenner, H et
al. 2007).• Humoral and cellular immunity (Bouman et al. 2004)• Help seeking behaviour (Smith et al 2005, Branney
2008)• Knowledge of cancer (Macdonald et al. 2004)
White, A, Thomson, C, Forman, D,(2009) The Excess burden of cancer in men, NCIN, London

Incidence and mortality rates by deprivation in Scotland
Considering all cancers combined, the most deprived areas have incidence rates almost 40% higher than the least deprived areas; mortality rates for all cancers combined are approximately 75% higher in the most deprived than the least deprived areas.

Cancer age standardised incidence by deprivation quintile and sex; Northern &
Yorkshire
Forman, White & Farley (2006)
ASR by Deprivation Quintile - All Cancers, 2002-2004
0
50
100
150
200
250
300
350
400
450
500
Male Female
imd2004
AS
R
Q1
Q2
Q3
Q4
Q5
Forman, White & Farley (2006)

Cancer age standardised incidence by deprivation quintile and sex after excluding
prostate and breast cancers; Northern & Yorkshire
Forman, White & Farley (2006)
ASR by Deprivation Quintile - All excl. prostate / breast, 2002-2004
0
50
100
150
200
250
300
350
400
450
500
Male Female
imd2004
AS
R
Q1
Q2
Q3
Q4
Q5
Forman, White & Farley (2006)

Cancer age standardised incidence by deprivation quintile and sex after excluding sex-specific, breast
and lung cancers; Northern & Yorkshire
Forman, White & Farley (2006)
ASR by Deprivation Quintile - All excl. sex specific & lung, 2002-2004
0
50
100
150
200
250
300
350
400
450
500
Male Female
imd2004
AS
R
Q1
Q2
Q3
Q4
Q5

The advantage of women in cancer survival: An analysis of EUROCARE-4 data
• Significant female advantages for head and neck, oesophagus, stomach, and pancreas, salivary glands, colon and rectum, lung, pleura, bone, melanoma of skin, kidney, brain, thyroid, Hodgkin’s disease and non-Hodgkin’s lymphoma.
• A significant female disadvantage for biliary tract, leukaemia and Bladder
Michelia et al (2009) The advantage of women in cancer survival: An analysis of EUROCARE-4 data. European Journal of Cancer 45 ( 2009) 1017 –102

“Women had significantly higher survival than men for all cancers combined in each age class; however, this advantage reduced progressively with age: from +12.0% points at 15–44 years to +1.3% points at 75–99 years.” (p1022)
Michelia et al (2009) The advantage of women in cancer survival: An analysis of EUROCARE-4 data. European Journal of Cancer 45 ( 2009) 1017 –102

Difference (%) between men and women in cancer survival across Europe
02468
1012141618
Slove
nia
Mal
ta
Czech
Rep
ublic
The
Net
herla
nds
Italy
Polan
d
Spain
EUROCARE-4
mea
n
North
ern
Irelan
d
Ger
man
y
Belgiu
m
Englan
d
Scotla
nd
Switzer
land
Wales
Finlan
d
Norway
Icela
nd
Irelan
d
Austri
a
Sweden
%
Verdecchia et al (2007) Eurocare 4

Cancer World

Registrations of newly diagnosed cases of malignant neoplasm of colon &
rectosigmoid junction & rectum, Scotland, by age and sex, 2008.
Colon, Rectosigmoid junction, Rectum
-
50
100
150
200
250
300
350
400
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+
Male
Female
ISD Scotland (2009) http://www.isdscotland.org/isd/1508.html

Deaths registered as a result of malignant neoplasm of colon & rectosigmoid junction,& rectum by age and sex, 2008 for Scotland
ISD Scotland (2009) http://www.isdscotland.org/isd/1508.html
Colon, Rectrosigmoid junction, Rectum
0
20
40
60
80
100
120
140
160
180
200
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+
Male
Female

The case of Colo-rectal cancer
• 35% genetic factor– Hereditary non-polyposis colorectal cancer (3-5%
of cancers, with many of these male)– 1st degree affected relative increases risk 2-4 fold– May include recessive genes, pathogenic
mutations of low penetrance and complex gene-gene and gene-environment interactions
Mitchell et al 2002
– Aggravated by mutations in APC, p53, k Ras and MSH2 genes
(Fearon & Volgestein 1990)

• Colo-rectal cancer risk increased by:– Diet low in fruit and vegetables– High intake of red and processed meat– Low physical activity– Alcohol– Smoking – Diabetes – Obesity


6.37 In 2006, a symposium organised by the Men’s Health Forum and chaired by the National Cancer Director discussed the issues around cancer and gender. The event highlighted that there are still many cancer types for which the reason for higher incidence and mortality in men is not known and that this higher incidence may be the result of unidentified risk factors or general biological predisposition. It is clear that more research is needed if we are to fully understand how gender impacts on cancer.6.38 The Symposium also highlighted that the range of settings in which men are offered advice, information and routine health checks should be expanded from traditional primary and secondary care settings, for example into the workplace.
CANCER REFORM STRATEGY 2007


The causes of these inequalities are not fully understood. Differences in lifestyle (e.g. smoking) and occupational exposure to risk factors are likely to be major factors.
Report of the All Party Parliamentary Group on Cancer’s Inquiry into Inequalities in Cancer, 2009 (p10)

National Cancer Equalities Initiative
• A response to the Cancer Reform Strategy
• Gender visioning event in Leeds this year
• Report to be published in January 2010
• Research and policy directives will emerge from this group

Conclusion
• Men are more at risk of developing and dying of those cancers that should affect men and women equally
• The reasons for men’s increased risk are many and are not just associated with higher smoking levels
• We need to be more proactive in reaching out to men to inform them of the risk and also what can be done about it.
• There is now recognition of this at Government and we will see progress…