Embed Size (px)
Citation preview

AJCP / Case Report
670 Am J Clin Pathol 2014;142:670-674 DOI: 10.1309/AJCPSUQVIGA8S1AH
© American Society for Clinical Pathology
Medullary-Like Hepatocellular Carcinoma
An Unusual Histologic Variant
Erin Quist, MD,1 Geoffrey Talmon, MD,1 Cleve Hartman, MD,2 and James Wisecarver, MD, PhD1
From the 1Department of Pathology and Microbiology, University of Nebraska Medical Center, Omaha, and 2Dr Hartman Family Practice Clinic, North Platte, NE
Key Words: Hepatocellular carcinoma; Medullary-like hepatocellular carcinoma; Hepatopathology
Am J Clin Pathol November 2014;142:670-674
DOI: 10.1309/AJCPSUQVIGA8S1AH
ABSTRACT
Objectives: Due to differences in prognosis and management, it is important to subclassify hepatocellular carcinoma (HCC). We encountered an unusual case of HCC with features not typical of the previously described subtypes that was composed of a markedly cellular background consisting of plasma cells and lymphocytes.
Methods: Review of the literature revealed a single prior case report describing a lesion with similar histology.
Results: In contrast to the previous case report suggesting a less aggressive course and a lesion with increased apoptotic activity, our patient died as a result of his disease within 30 days of diagnosis. In this report, we compare the features of our case with the previously described lesion and use immunohistochemistry for cleaved caspase 3 to evaluate apoptosis and mismatch repair proteins to evaluate microsatellite instability.
Conclusions: This report is presented to increase awareness of this unusual lesion and because it raises questions regarding the previous claim suggesting a less aggressive clinical course.
Hepatocellular carcinoma (HCC) is the most common primary hepatic malignancy of adults, with 20,000 new cases diagnosed in the United States and approximately half a million cases diagnosed worldwide each year.1,2 The overall prognosis is poor, with a 5-year survival rate below 12%.1
While most cases of HCC have a poor 5-year survival, some variants may behave differently. Fibrolamellar HCC, which typically arises in adolescents and young adults, appears to have a more favorable prognosis. Similarly, the very rare medullary-like HCC may also have a more indolent course. This tumor was first described by Zimmermann et al3 in 2002 in a 56-year-old man with a 6 × 6 × 4-cm solitary tumor, arising in the background of cirrhosis. The lesion demonstrated extensive lymphocytic (B- and T-cell) infiltration and a polyclonal plasma cell infiltrate. In addition, signs of tumor regression, evidenced by numerous apoptotic bodies and breakdown of the main tumor mass, were identified in varying stages of evolution. The patient underwent resection and showed no evidence of disease 25 months after resection.
Herein, we present a second case of this rare medullary-like HCC. However, unlike the previous report, this patient’s tumor arose in the absence of cirrhosis and was clinically aggressive, with radiographic evidence of metastatic spread, and the patient died 30 days after diagnosis. To further characterize this lesion and confirm the tumor regression identified in the initial case, we used immunohistochemical staining for cleaved caspase 3 to evaluate the level of tumor cell apoptosis. Staining for mismatch repair proteins, including mutL homolog 1 (MLH1), mutS homolog 2 (MSH2), mutS homolog 6 (MSH6), and postmeiotic segregation increased 2 (PMS2), was used to investigate the potential relationship of this unique lesion with microsatellite instability (MSI).
AJCP / Case Report
Am J Clin Pathol 2014;142:670-674 671 DOI: 10.1309/AJCPSUQVIGA8S1AH
© American Society for Clinical Pathology
BA
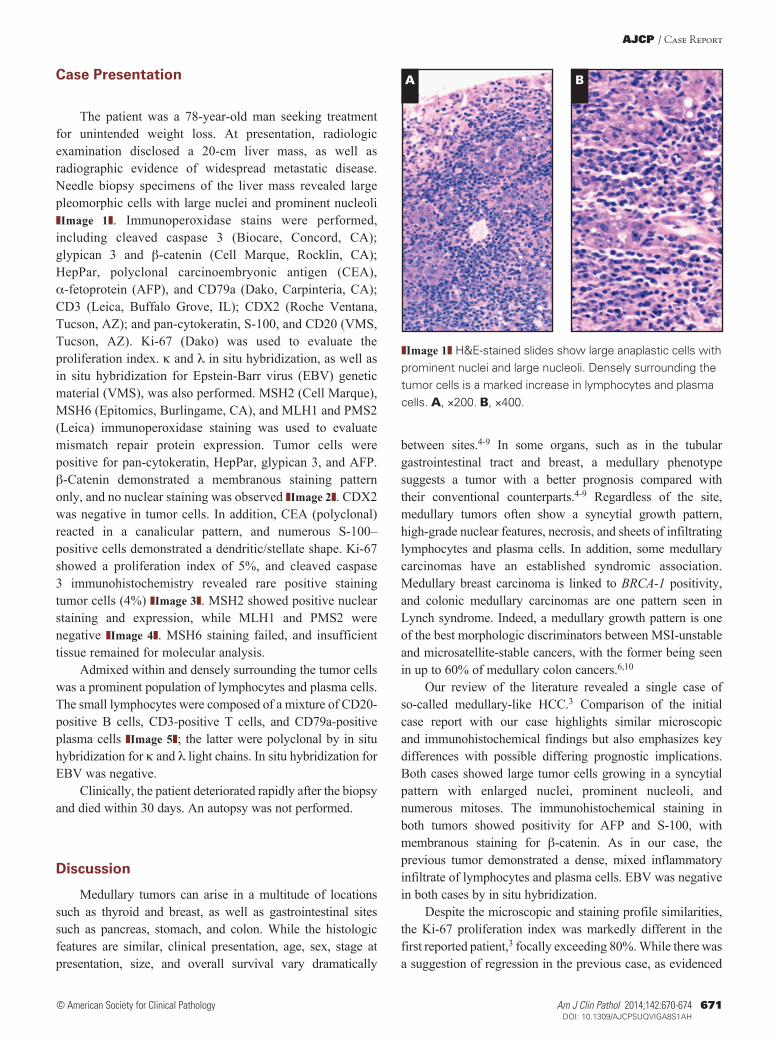
❚Image 1❚ H&E-stained slides show large anaplastic cells with prominent nuclei and large nucleoli. Densely surrounding the tumor cells is a marked increase in lymphocytes and plasma cells. A, ×200. B, ×400.
Case Presentation
The patient was a 78-year-old man seeking treatment for unintended weight loss. At presentation, radiologic examination disclosed a 20-cm liver mass, as well as radiographic evidence of widespread metastatic disease. Needle biopsy specimens of the liver mass revealed large pleomorphic cells with large nuclei and prominent nucleoli ❚Image 1❚. Immunoperoxidase stains were performed, including cleaved caspase 3 (Biocare, Concord, CA); glypican 3 and b-catenin (Cell Marque, Rocklin, CA); HepPar, polyclonal carcinoembryonic antigen (CEA), a-fetoprotein (AFP), and CD79a (Dako, Carpinteria, CA); CD3 (Leica, Buffalo Grove, IL); CDX2 (Roche Ventana, Tucson, AZ); and pan-cytokeratin, S-100, and CD20 (VMS, Tucson, AZ). Ki-67 (Dako) was used to evaluate the proliferation index. k and l in situ hybridization, as well as in situ hybridization for Epstein-Barr virus (EBV) genetic material (VMS), was also performed. MSH2 (Cell Marque), MSH6 (Epitomics, Burlingame, CA), and MLH1 and PMS2 (Leica) immunoperoxidase staining was used to evaluate mismatch repair protein expression. Tumor cells were positive for pan-cytokeratin, HepPar, glypican 3, and AFP. b-Catenin demonstrated a membranous staining pattern only, and no nuclear staining was observed ❚Image 2❚. CDX2 was negative in tumor cells. In addition, CEA (polyclonal) reacted in a canalicular pattern, and numerous S-100–positive cells demonstrated a dendritic/stellate shape. Ki-67 showed a proliferation index of 5%, and cleaved caspase 3 immunohistochemistry revealed rare positive staining tumor cells (4%) ❚Image 3❚. MSH2 showed positive nuclear staining and expression, while MLH1 and PMS2 were negative ❚Image 4❚. MSH6 staining failed, and insufficient tissue remained for molecular analysis.
Admixed within and densely surrounding the tumor cells was a prominent population of lymphocytes and plasma cells. The small lymphocytes were composed of a mixture of CD20-positive B cells, CD3-positive T cells, and CD79a-positive plasma cells ❚Image 5❚; the latter were polyclonal by in situ hybridization for k and l light chains. In situ hybridization for EBV was negative.
Clinically, the patient deteriorated rapidly after the biopsy and died within 30 days. An autopsy was not performed.
Discussion
Medullary tumors can arise in a multitude of locations such as thyroid and breast, as well as gastrointestinal sites such as pancreas, stomach, and colon. While the histologic features are similar, clinical presentation, age, sex, stage at presentation, size, and overall survival vary dramatically
between sites.4-9 In some organs, such as in the tubular gastrointestinal tract and breast, a medullary phenotype suggests a tumor with a better prognosis compared with their conventional counterparts.4-9 Regardless of the site, medullary tumors often show a syncytial growth pattern, high-grade nuclear features, necrosis, and sheets of infiltrating lymphocytes and plasma cells. In addition, some medullary carcinomas have an established syndromic association. Medullary breast carcinoma is linked to BRCA-1 positivity, and colonic medullary carcinomas are one pattern seen in Lynch syndrome. Indeed, a medullary growth pattern is one of the best morphologic discriminators between MSI-unstable and microsatellite-stable cancers, with the former being seen in up to 60% of medullary colon cancers.6,10
Our review of the literature revealed a single case of so-called medullary-like HCC.3 Comparison of the initial case report with our case highlights similar microscopic and immunohistochemical findings but also emphasizes key differences with possible differing prognostic implications. Both cases showed large tumor cells growing in a syncytial pattern with enlarged nuclei, prominent nucleoli, and numerous mitoses. The immunohistochemical staining in both tumors showed positivity for AFP and S-100, with membranous staining for b-catenin. As in our case, the previous tumor demonstrated a dense, mixed inflammatory infiltrate of lymphocytes and plasma cells. EBV was negative in both cases by in situ hybridization.
Despite the microscopic and staining profile similarities, the Ki-67 proliferation index was markedly different in the first reported patient,3 focally exceeding 80%. While there was a suggestion of regression in the previous case, as evidenced

Quist et al / Medullary-Like Hepatocellular Carcinoma
672 Am J Clin Pathol 2014;142:670-674 DOI: 10.1309/AJCPSUQVIGA8S1AH
© American Society for Clinical Pathology
BA
E
DC
❚Image 2❚ Immunoperoxidase staining of the tumor cells showed positivity for HepPar (Dako, Carpinteria, CA) (A), glypican 3 (Cell Marque, Rocklin, CA) (B), carcinoembryonic antigen (Dako) (D), and S-100 (VMS, Tucson, AZ) (E) (×200). b-Catenin (Cell Marque) (C) demonstrated a membranous staining pattern only (×200).
by abundant tumor cell apoptosis, it was not identified in our tumor, which was confirmed by, at most, only focal cleaved caspase 3 staining in tumor cells.
Review of the literature shows a limited amount of information on the relationship between HCCs and MSI, but it is thought that it is infrequent. In one study, 36 HCCs were tested for MLH1 and MSH2, and all retained immunohistochemical staining. The authors concluded that defective mismatch repair does not contribute significantly to hepatocellular carcinogenesis.11 In contrast, this tumor lost MLH1 and PMS2, which suggests that DNA mismatch repair may be associated with HCCs demonstrating this appearance. The pattern of staining is that most commonly seen in sporadic MSI, although germline mutations in mismatch repair enzymes cannot be ruled out. Unfortunately, insufficient tissue remained for molecular characterization, and the prior study did not evaluate these additional markers, so direct comparison is difficult.
The clinical behavior was also significantly different. In the earlier report,3 the patient was younger and the lesion arose in the background of cirrhosis. Our patient was significantly older and had no significant underlying liver disease evident in the adjacent hepatic parenchyma or by clinical history. The prior tumor was smaller than in our case and without metastasis, while our case demonstrated an aggressive phenotype.
Despite the similar histology, the rapidly fatal course in the present case raises the question as to whether the so-called medullary-like HCC predicts a more favorable clinical course as was originally suggested. In our tumor, the paucity of apoptotic activity and lack of widespread cleaved caspase 3 staining lend support that the “medullary” phenotype does not necessarily uniformly imply tumor
BA
❚Image 3❚ Immunohistochemistry for Ki-67 (Dako, Carpinteria, CA) (A) showed a proliferation index of 5%, and cleaved caspase 3 (Biocare, Concord, CA) (B) revealed rare positive staining tumor cells (4%) (×200).

AJCP / Case Report
Am J Clin Pathol 2014;142:670-674 673 DOI: 10.1309/AJCPSUQVIGA8S1AH
© American Society for Clinical Pathology
“regression,” and the lack of these findings may herald a worse prognosis. Correlating both the clinical and histologic evidence presented in this case, consideration should be given that these medullary-like HCCs do not universally have a favorable outcome and may actually portend a poorer prognosis than was initially suspected.
We have presented another case of the rare medullary-like variant HCC that may be associated with MSI and had an aggressive behavior. Because of the limited number of such cases, it is important for clinicians and surgical pathologists to be mindful of this pattern of HCC in their differential diagnosis of hepatocellular lesions.
Address reprint requests to Dr Quist: 983135 Nebraska Medical Center, Omaha, NE 68198-3135; [email protected].
References 1. Hashem EB. Hepatocellular carcinoma. N Engl J Med.
2011;365:1118-1127.
2. Burt AD, Portman BC, Ferrell LD. MacSween’s Pathology of the Liver. 5th ed. Philadelphia, PA: Churchill Livingstone Elsevier; 2007.
3. Zimmermann A, Kappeler A, Friess H, et al. Hepatocellular carcinoma with an unusual medullary-like histology and signs of regression (“medullary-like hepatocellular carcinoma”). Dig Liver Dis. 2002;34:748-753.
4. Ganeshan D, Paulson E, Duran C, et al. Current update on medullary thyroid carcinoma. AJR Am J Roentgenol. 2013;201:W867-W876.
5. Park I, Kim J, Kim M, et al. Comparison of the characteristics of medullary breast carcinoma and invasive ductal carcinoma. J Breast Cancer. 2013;16:417-425.
C
BA
❚Image 5❚ Immunoperoxidase staining of the surrounding inflammatory cells showed a lymphocytic and plasma cell infiltrate composed of CD20 B cells (VMS, Tucson, AZ) (A), CD3 T cells (Leica, Buffalo Grove, IL) (B), and CD79a plasma cells (Dako, Carpinteria, CA) (C) (×200).
DC
BA
❚Image 4❚ Staining for mutL homolog 1 (A) and postmeiotic segregation increased 2 (B) showed no nuclear staining in the tumor cells, while mutS homolog 2 (C) demonstrated positive nuclear staining (×400). Staining for mutS homolog 6 (D) failed (×400).

Quist et al / Medullary-Like Hepatocellular Carcinoma
674 Am J Clin Pathol 2014;142:670-674 DOI: 10.1309/AJCPSUQVIGA8S1AH
© American Society for Clinical Pathology
6. Thirunavukarasu P, Sathaiah M, Singla S, et al. Medullary carcinoma of the large intestine: a population based analysis. Int J Oncol. 2010;37:901-907.
7. Wilentz RE, Goggins M, Redston M, et al. Genetics, immunohistochemical, and clinical features of medullary carcinoma of the pancreas. Am J Pathol. 2000;156:1641-1651.
8. Otsuji E, Kuriu Y, Ichikawa D, et al. Clinicopathologic and prognostic characterization of poorly differentiated medullary-type gastric adenocarcinoma. World J Surg. 2004;28:862-865.
9. Lu BJ, Lai M, Cheng L, et al. Gastric medullary carcinoma, a distinct entity associated with microsatellite instability-H, prominent intraepithelial lymphocytes and improved prognosis. Histopathology. 2004;45:485-492.
10. Alexander J, Watanabe T, Wu TT, et al. Histopathological identification of colon cancer with microsatellite instability. Am J Pathol. 2001;158:527-535.
11. Wang L, Bani-Hani A, Montoya DP, et al. hMLH1 and hMSH2 expression in human hepatocellular carcinoma. Int J Oncol. 2001;19:567-570.





























