Embed Size (px)
Citation preview

The Evolving Environment for Outpatient Hospital Services: Medicare’s Site-Neutral Reimbursement for
New Off-Campus Locations
Jim Price, Rick Buchsbaum, and Kyle Price Progressive Healthcare Inc.
March 31, 2016

P a g e 2 | 16
1. What changed in Fall 2015 regarding outpatient hospital services?
On November 2, 2015, the Bipartisan Budget Act of 2015 was enacted. Section 603 provides
that “effective January 1, 2017, Medicare payments for most items and services furnished at
an off-campus department of a hospital that was not billing as a hospital service prior to the
date of enactment will be made under the applicable non-hospital payment system.”1. In other
words, new off-campus Hospital Outpatient Departments (HOPDs) will be reimbursed at the
lowest possible rate. The new provision attempts to address concerns raised by policymakers
that Medicare should not be paying varying amounts for the same services based on the
location or provider, and that incentives to acquire practices as outpatient departments may
have been improper due to the availability of higher service rates in outpatient settings.
2. Are there exceptions for off-campus HOPDs?
The only exceptions are the services provided by a dedicated off-campus emergency
department. As defined in Title 42 C.F.R. Section 489.24(b), a dedicated emergency
department must meet at least one of the following requirements:
1. “It is licensed by the State in which it is located under applicable State law as an
emergency room or emergency department;
2. “It is held out to the public (by name, posted signs, advertising, or other means) as a
place that provides care for emergency medical conditions on an urgent basis without
requiring a previously scheduled appointment; or
3. “During the calendar year immediately preceding the calendar year in which a
determination under this section is being made, based on a representative sample of
patient visits that occurred during that calendar year, it provides at least one-third of all
of its outpatient visits for the treatment of emergency medical conditions on an urgent
basis without requiring a previously scheduled appointment.” 2
Freestanding EDs face certificate-of-need (CON) limits in most states.
1 McDermott Will & Emery LLP, Congress Takes Step Toward Site-Neutral Medicare Payments in Bipartisan Budget Act of 2015, October 29, 2015, retrieved from www.mwe.com/publications on February 12, 2016. 2 Federal Register, Title 42 of the Code of Federal Regulations, Chapter IV, Subcategory G, § 489.24(b), Special responsibilities of Medicare Hospitals in emergency cases, (1994).

P a g e 3 | 16
3. Why is this change so threatening to hospitals?
Hospitals have enjoyed a Medicare reimbursement premium for many outpatient services,
when compared to other entities. As shown below, this premium could exceed 100%:
As noted by the Government Accountability Office, this reimbursement difference has
encouraged the acquisition of physician practices by hospitals, since hospitals could earn a
“reimbursement arbitrage” on acquired ancillary services.3
For example, by acquiring a cardiology practice with in-office diagnostics, the purchasing
health system would be paid $1,189, rather than $495 (for an increase of $694, 140%), per
Nuclear Stress Test / TMST procedure using the same facility and staff after designating the
diagnostics rooms as an HOPD. See the Technical Appendix for details.
3 Government Accountability Office, Increasing Hospital - Physician Consolidation Highlights Need for Payment Reform, December, 2015, retrieved from www.gao.gov on February 24, 2016.
Asof: 1/1/16 Atlanta
Specialty Service CPTPhysicianOffice
ASC/Other
OutpatientHospital Comments
All Officevisit,establishedpatient,Level4 99214 $108 n/a $181 $73 67%
Imaging MRIJointLowerExtw/ocontrast 73721 $239 $222 $343 $121 54%MRILunbarspinew/ocontrast 72148 $225 $224 $349 $126 55%
PTevaluation 97001 $76 n/a $76 $0 0%Manualtherapy(per15minutes) 97140 $30 n/a $30 $0 0%Therapeuticexercises 97110 $33 n/a $33 $0 0%E-Stim1/>notWndCarePart G0283 $14 n/a $14 $0 0%
Cardiology CardiacRehab 93798 $25 n/a $118 $93 365%Echo 93306 $231 n/a $481 $250 108%NuclearStressTest/TMST 78452 $495 n/a $1,189 $694 140%Pulmonarystresstest/simple 94620 $57 n/a $122 $65 115%StressECHO 93351 $275 n/a $503 $228 83%
GI DiagnosticColonoscopy 45378 $386 $620 $952 $332 54% GIswilltypicallyownanASC
Orthopedics Kneearthroscopy/surgery 29881 n/a $1,896 $2,952 $1,056 56%Wristendoscopy/surgery 29848 n/a $1,337 $1,979 $642 48%
Injforamenepidurall/s 64483 $225 $443 $701 $258 58%Injforamenepiduraladd-on 64484 $90 $54 $54Injectspinec/t 62310 $246 $439 $697 $258 59%Injectspinel/s(cd) 62311 $227 $419 $677 $258 61%Injecttriggerpoints=/>3 20553 $65 $79 $268 $189 238%
Pulmonary SleepLab 95810 $633 n/a $980 $347 55%
MedicareReimbursementforCommonOutpatientProceduresSite-of-ServiceDifferential
HealthSystemPremiumoverlower-
costsetting
PainManagement
MDswillusuallytrytoperformtheseproceduresinan(owned)ASC
TotalMedicareReimbursement(MD&Facility)bySetting
PhysicalTherapy

P a g e 4 | 16
The hospital outpatient services that are affected by Section 603 are those that are rendered in
a new off-campus location and for which Medicare paid via the Outpatient Prospective
Payment System (OPPS). Below are some common outpatient services that are/were not paid
under OPPS and hence are not affected by Section 603:
• Ambulance services
• Clinical diagnostic laboratory
• Physical, Occupational, and Speech Therapy
• Routine dialysis service for ESRD patients
• Diagnostics and screening mammography
4. When does the new policy apply?
This new payment policy is effective on January 1, 2017. It applies to off-campus outpatient
departments of a hospital that were NOT billing as a hospital department prior to November 2,
2015. This policy does not apply to dedicated emergency departments (“freestanding EDs”).
5. What impact will it have on hospitals?
From a reimbursement perspective:
a. There is no change to off-campus locations that were operating prior to November 2,
2015.
b. For new off-campus locations, which includes newly-developed sites and acquisitions
of physician practices, Medicare reimbursement will be reduced to the lowest
applicable amount (i.e., physician practice (known as “non-provider”) or ASC). This
does not apply to free-standing EDs.
From a business perspective, the magnitude of these Medicare reimbursement reductions may
be sufficient to make many prospective outpatient initiatives financially non-viable,
particularly if the patient mix is heavily-weighted toward Medicare and the “reimbursement
arbitrage” would have been significant.

P a g e 5 | 16
6. Can hospitals open new outpatient facilities and bill Medicare?
There is no restriction on the ability for hospitals to open new outpatient facilities and bill
Medicare.
7. For such new facilities, what is the impact from the new Medicare reimbursement rules?
Setting aside the free-standing ED exclusion, the impact from the new Medicare
reimbursement rules varies substantially by service, as the above table illustrates. In general,
Medicare rates will drop for many common services, except for Physician Therapy: At new HOPDs, reduction
Service in total Medicare reimbursement
Cardiac diagnostics ~ 50+ %
Office visits ~ 30-50 %
Pain management ~ 40 %
Surgery ~ 35 %
Imaging ~ 30 %
Physical Therapy 0 %
The above percentages include physician reimbursement. The percentage reductions in the
“hospital” (or “facility”) portion is often much larger, as illustrated in the Technical
Appendix.
For services whose patients are primarily Medicare (e.g. cardiac diagnostics), off-campus
growth (either via practice acquisition or new construction) is likely non-viable.
8. Why was this change enacted?
Numerous entities recommended this reimbursement change for a number of reasons:
1. The Medicare Payment Advisory Commission (MedPAC) has recommended since
2012 that Medicare pay hospitals at the same rates as other entities, for certain
outpatient services. MedPAC initially focused on evaluation and management
services (“office visits”), and the recommendation was expanded in 2013 to other
outpatient services. MedPAC estimated in 2015 that these policy changes would save

P a g e 6 | 16
$1.4 billion per year, although it is unlikely that this estimate accounted for the
“grandfathering” of existing HOPDs.4
2. The Congressional Budget Office (CBO) estimated that Section 603 will save $9.3
billion over 10 years.
3. The Government Accountability Office reported in December 2015 that hospital
acquisition of physician practices was correlated with the higher reimbursement for
hospitals, and that due to trends in increased hospital-physician consolidation, CMS
should “equalize payment rates between settings.”
4. Trade associations represent competitors to hospitals, including the American Medical
Association5, likely because physicians wanted to have their ancillary services paid at
the same rate as hospitals.
9. What changes to Section 603 is the American Hospital Association recommending?
The AHA is not trying to change the reimbursement impact that will be effective on January
1, 2017. Rather, its focus with Congress is merely on a “technical correction” with two
objectives:
1. “Hospitals that have made substantial investments in new facilities that were under
development when the Bipartisan Budget Act was signed into law should be protected
consistent with past precedent.”
2. Clarifying that “changes in ownership of a facility do not impact the grandfathered
status of a provider-based HOPD and that grandfathered HOPDs may relocate.” 6
4 Medicare Payment Advisory Commission (MedPAC), Payment Basics: Outpatient Hospital Services Payment System, October 2015, retrieved from www.medpac.gov on February 24, 2016. 5 American Medical Association, H-330.925 Appropriate Payment Level Differences by Place and Type of Service, (no date), retrieved from www.ama-assn.org on February 24, 2016. 6 American Hospital Association, AHA Factsheet: Site-neutral HOPD Technical Corrections, November 16, 2015, retrieved from www.aha.org on February 11, 2016.

P a g e 7 | 16
10. What new rules apply to outpatient services regarding modifiers, codes, et cetera?
In 2014, as part of the CY 2015 Outpatient Prospective Payment System Final Rule, CMS
required a new billing modifier on a facility (“provider”) claim and a new place of service
code on professional claims for services furnished in any off-campus provider-based
outpatient departments (e.g., HOPDs). This rule only applies to Medicare patients, and was
mandatory as of January 1, 2016. Use of the modifier (by the hospital) and place of service
code (by the physician) was voluntary during 2015. Hence, this billing change should not
have been a surprise to providers during late 2015. However, the billing rule and Section 603
are complementary, as CMS could not implement some form of “grandfathered” site-neutral
reimbursement without being able to differentiate off-campus from on-campus HOPDs or
identify those off-campus HOPDs that are already (as of January 1, 2016) billing Medicare.
The billing modifier itself is not directly tied to reimbursement. Rather, it was (and is) CMS’
method for segmenting off-campus from on-campus HOPD activity for future policy-setting.
It was seen by many (including Progressive), prior to the 2015 Budget Agreement, as a sign
that within a few years CMS would eliminate or greatly reduce the site-of-service premium
that HOPDs enjoy. This has been the recommendation of MedPAC. Thus, many expect that
CMS will study the volume data in 2017 and recommend reimbursement reductions to some
or all “grandfathered” HOPDs in 2018 or 2019. Since such a change would affect “existing”
hospital margins (and not just planned or potential HOPDs), the change would in turn be very
political.
11. What is the “35 mile rule”, and does it still apply?
In general, acute care hospitals (other than critical access hospitals) can operate outpatient
departments within 35 miles “as the bird flies” from the inpatient campus and structure them
as “provider-based” hospital outpatient departments. Section 603 does not affect this rule.
12. What is the outlook with other payors?
This likely varies by segment:
• Medicare Advantage. Typically, MA plans pay providers a slight (3-5%) premium on
Medicare reimbursement. Thus, MA plans will likely be able to leverage Medicare’s
effective rate reduction on new sites in 2017. However, since the vast majority of

P a g e 8 | 16
services will be provided by either campus-based or grandfathered off-campus locations,
there will likely be little change in actual total payments made by MA plans. Note: the
means by which CMS’ Fiscal Intermediaries will identify grandfathered off-campus
sites has not been promulgated by CMS, since the payment system must reimburse
“new” sites at the site-neutral rates beginning January 1, 2017.
• Commercial. What commercial payors actually do is dependent upon negotiations
between hospitals and payors, and cannot be mandated. However, hospital outpatient
departments already face pricing competition from lower-reimbursed providers, and this
shift in Medicare policy will heighten awareness of the rate premium. We have already
seen in many clients that commercial payors do not recognize the site-of-service
differential for the evaluation and management code (e.g. “facility fee” for “office-
visits”).
• Medicaid – Historically, Medicaid has followed Medicare policy in many
reimbursement areas. However, this will be state-specific.
• The biggest risk for hospitals may be increased patient knowledge regarding
reimbursement rate differentials across locations. Those differences are present today
across type of entity (HOPD/ASC/physician office), but beginning on January 1, 2017,
HOPD rates for Medicare will differ between new sites and those on campus or in
grandfathered locations. “Transparency” is the mortal enemy of large rate differences
for apparently-identical services.
In summary, it is difficult to develop a logical scenario whereby Section 603, by itself, leads
to lower negotiated rates with health plans (for all segments).

P a g e 9 | 16
13. What are the strategic implications on hospitals and health systems of this legislation?
A. Practice acquisitions or new outpatient locations by hospitals that depend upon
Medicare “reimbursement arbitrage” to make the investment financially-viable will be
hard to justify.
B. Outpatient growth for services that need relatively-high Medicare reimbursement will
be focused in existing HOPD locations and on campus.
C. New HOPD site growth will be limited to services that:
a. Are still profitable across all payers (such as Physical Therapy, for which
reimbursement rates have not changed)
b. Drive downstream volume. Examples include:
i. Primary care, including urgent care
ii. Low-end imaging
iii. Specialist care (for their non-diagnostic office visits)
iv. Physical Therapy
v. Medical specialists offices and chronic condition clinics (for 340B
margins on scripts written)
c. Meet “system” care management needs even if the HOPD itself is not profitable.
Such needs include:
i. Geographic coverage
ii. Low-cost facilities across the entire continuum of care
iii. Care management intervention services (rendered while performing a fee-
for-service task), such as:
1. Medication dispensing (and medication therapy management) to
patients with chronic conditions; or
2. Physical Therapy re-evaluations at milestones during an orthopedic
bundled payment episode (e.g., pre-surgery; 30 days post-surgery;
270 days post-surgery (for Medicare mandatory bundled payments
for hips/knees at 800 hospitals)), which could assist with managing
and improving reported outcomes, which drives the bonus payment.
d. Complement free-standing EDs.

P a g e 10 | 16
14. What happens next?
Many tactical issues are unresolved and will require clarification from CMS, such as7:
• What changes can a “grandfathered” off-campus department make?
i. Can an off-campus department add different services (e.g., add cardiac
diagnostics to a site that currently only offers physical therapy)?
ii. Could an off-campus department change locations and keep its status?
iii. Will the facility be able to expand its footprint? If so, by how much?
• How (if at all) will CMS change its billing, cost reporting, and/or enrollment
procedures?
i. How will CMS identify new/grandfathered departments?
ii. Is split-billing still required? If not, how do hospitals get paid?
• What kind of leniencies will be afforded to free-standing EDs?
i. How will CMS handle reimbursements for scheduled non-emergency services
furnished in a dedicated ED facility?
7 Russo, Greg; Hettich, Daniel J.; Kenny, Christopher; Dressel, Peter; Polston, Mark D., How Does Medicare Reduce Payments? Let Us Count the Ways, King & Spalding, 2016 Health Law & Policy Forum, Section 603.

P a g e 11 | 16
Bibliography
American Hospital Association, AHA Factsheet: Additional Hospital Outpatient Services at Risk
for Site-Neutral Cuts, September 8, 2015, retrieved from www.aha.org on February 11, 2016.
American Hospital Association, AHA Factsheet: Site-neutral HOPD Technical Corrections,
November 16, 2015, retrieved from www.aha.org on February 11, 2016.
American Hospital Association, Congress Passes Two-Year Budget Agreement FAQ, October 30,
2015, retrieved from www.aha.org on February 11, 2016.
American Medical Association, H-330.925 Appropriate Payment Level Differences by Place and
Type of Service, (no date), retrieved from www.ama-assn.org on February 24, 2016.
Cassidy, A., et al, Health Policy Brief: Site-Neutral Payment, Health Affairs, July 14, 2014,
retrieved from www.healthaffairs.org on February 12, 2016.
Daly, R., Budget to Slash Medicare Rates for Acquired Practices, October 28, 2015, retrieved
from Healthcare Financial Management Association: www.hfma.org on February 24, 2016.
Daly, R., Hospital-Physician Practice Mergers Drive Some Price Increases: Study, October 22,
2015, retrieved from Healthcare Financial Management Association: www.hfma.org on
February 24, 2016.
Ellison, A., 25 things to know about site-neutral payments, Becker’s Hospital Review, June 29,
2015, retrieved from www.beckershospitalreview.com/finance on February 23, 2016.
Federal Register, Title 42 of the Code of Federal Regulations, Chapter IV, Subcategory G, §
489.24(b), Special responsibilities of Medicare Hospitals in emergency cases, (1994)
Foley & Lardner LLP, Treatment of Off-Campus Outpatient Departments of a Provider,
November 2015, retrieved from www.foley.com on February 11, 2016.
Foley & Lardner LLP, What Do "Site Neutral Payments" Mean to Your Facility?, November 13,
2015, retrieved from www.foley.com on February 11, 2016.
Government Accountability Office, Increasing Hospital - Physician Consolidation Highlights
Need for Payment Reform, December, 2015, retrieved from www.gao.gov on February 24,
2016.

P a g e 12 | 16
Hall Render LLP, Reminder: New Billing Requirements for Off-Campus Provider-Based
Departments Effective January 1, 2016, December 21, 2015, retrieved from
http://blogs.hallrender.com on February 12, 2016.
McDermott Will & Emery LLP, Congress Takes Step Toward Site-Neutral Medicare Payments in
Bipartisan Budget Act of 2015, October 29, 2015, retrieved from www.mwe.com/publications
on February 12, 2016.
McDermott Will & Emery LLP, The Final Provider-Based Status Rule, April 14, 2000, retrieved
from www.mwe.com/publications on February 12, 2016.
Medicare Payment Advisory Commission (MedPAC), Payment Basics: Outpatient Hospital
Services Payment System, October 2015, retrieved from www.medpac.gov on February 24,
2016.
MedPAC, Payment Basics: Outpatient Therapy Services Payment System, October 2015,
retreived from www.medpac.gov on February 24, 2016.
Passon, E., & Molden, M., Site-neutral payments: The billion-dollar Medicare revenue hit you
should plan for now, April 10, 2015, retrieved from The Advisory Board Company: Care
Transformation Center Blog: www.advisory.com/research on February 23, 2016.
Russo, Greg; Hettich, Daniel J.; Kenny, Christopher; Dressel, Peter; Polston, Mark D., How Does
Medicare Reduce Payments? Let Us Count the Ways, King & Spalding, 2016 Health Law &
Policy Forum, Section 603.
Sanger-Katz, M., When Hospitals Buy Doctors' Offices, and Patient Fees Soar, The New York
Times, February 6, 2015, retrieved from www.nytimes.com on February 24, 2016.
P a g e 13 | 16
The Evolving Environment for Outpatient Hospital Services: Medicare’s Site-Neutral Reimbursement for New Off-Campus Locations
Technical Appendix: Reimbursement Details
Jim Price, Rick Buchsbaum, and Kyle Price Progressive Healthcare Inc.
March 31, 2016
Medicare reimbursement can be complex when comparing sites of service. This appendix disentangles the details of Medicare reimbursement.
In the “physician office” setting, which CMS refers to as “Non-Facility”, Medicare’s reimbursements for professional and facility services are paid via a Global fee, as a Part B claim. In the ASC or HOPD (“provider”) setting, a Part A facility fee is paid to the facility and the Part B fee is reduced to the physician.
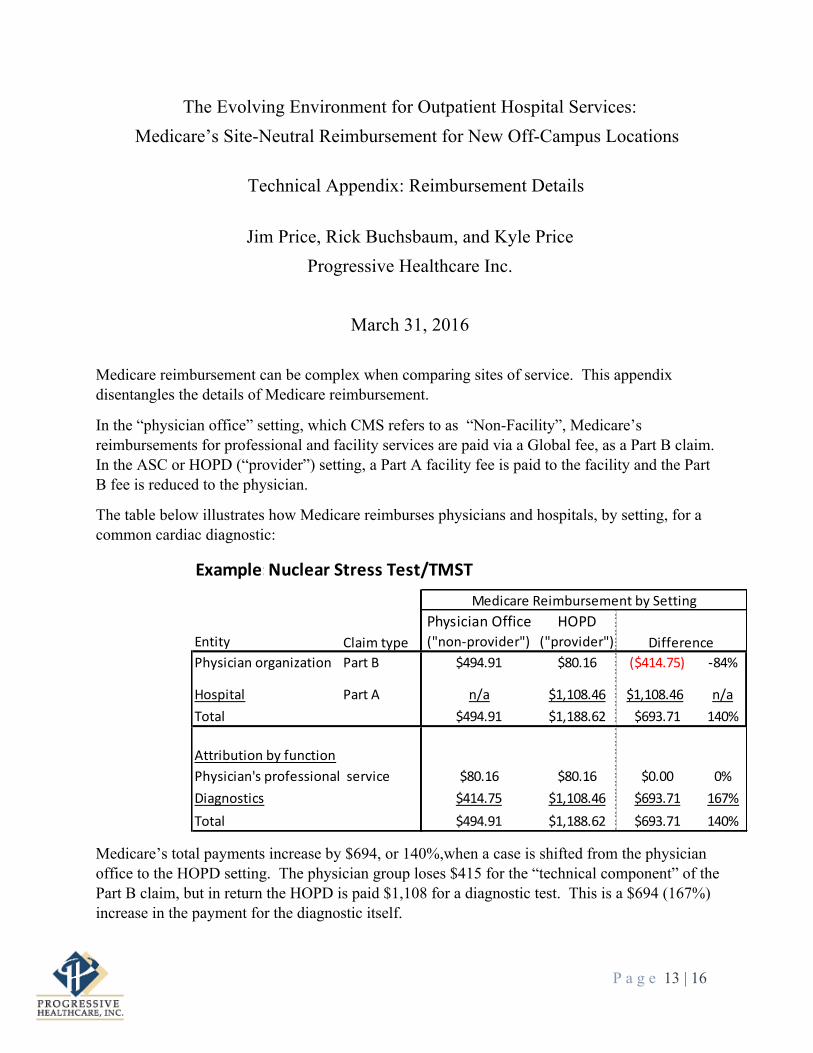
The table below illustrates how Medicare reimburses physicians and hospitals, by setting, for a common cardiac diagnostic:
Medicare’s total payments increase by $694, or 140%,when a case is shifted from the physician office to the HOPD setting. The physician group loses $415 for the “technical component” of the Part B claim, but in return the HOPD is paid $1,108 for a diagnostic test. This is a $694 (167%) increase in the payment for the diagnostic itself.
Example:NuclearStressTest/TMST
PhysicianOffice HOPDEntity ("non-provider") ("provider")
PartB $494.91 $80.16 ($414.75) -84%
Hospital PartA n/a $1,108.46 $1,108.46 n/aTotal $494.91 $1,188.62 $693.71 140%
AttributionbyfunctionPhysician'sprofessionalservice $80.16 $80.16 $0.00 0%Diagnostics $414.75 $1,108.46 $693.71 167%Total $494.91 $1,188.62 $693.71 140%
ClaimtypePhysicianorganization
Difference
MedicareReimbursementbySetting

P a g e 14 | 16
Below are the detailed reimbursements by CPT and related APC:
Asof: 1/1/16 Atlanta
All Officevisit,establishedpatient,Level4 99214 $108.18 $79.03 $0.00 $102.12 BHospitaloutptclinicvisit G0463 $79.03 $0.00 $102.12 5012 J2
Imaging MRIJointLowerExtw/ocontrast 73721 $238.83 $69.39 $152.96 $273.54 5581 Q3
MRILunbarspinew/ocontrast 72148 $225.13 $75.82 $147.94 $273.54 5581 Q3
PTevaluation 97001 $75.96 $0.00 $0.00 $75.96 A
Manualtherapy(per15minutes) 97140 $30.13 $0.00 $0.00 $30.13 A
Therapeuticexercises 97110 $32.62 $0.00 $0.00 $32.62 A
E-Stim1/>notWndCarePart G0283 $13.98 $0.00 $0.00 $13.98 A
Cardiology CardiacRehab 93798 $25.45 $14.30 $0.00 $103.92 5771 S
Echo 93306 $230.98 $64.43 $0.00 $416.80 5533 S
NuclearStressTest/TMST 78452 $494.91 $80.16 $619.83 $1,108.46 5593 S
Pulmonarystresstest/simple 94620 $57.01 $31.12 $0.00 $91.18 5734 Q1
StressECHO 93351 $274.76 $86.27 $0.00 $416.80 5533 S
GI DiagnosticColonoscopy 45378 $385.87 $199.12 $420.93 $752.76 5312 T
Orthopedics Kneearthroscopy/surgery 29881 $556.64 $556.64 $1,339.58 $2,395.59 5122 T
Wristendoscopy/surgery 29848 $523.69 $523.69 $813.76 $1,455.26 5121 T
Injforamenepidurall/s 64483 $224.56 $116.25 $327.22 $585.17 5442 T
Injforamenepiduraladd-on 64484 $89.60 $53.62 $0.00 $0.00 N
Injectspinec/t 62310 $245.79 $111.93 $327.22 $585.17 5442 T
Injectspinel/s(cd) 62311 $226.83 $92.25 $327.22 $585.17 5442 T
Injecttriggerpoints=/>3 20553 $64.82 $44.31 $35.10 $223.76 5441 T
Pulmonary SleepLab 95810 $633.49 $123.81 $0.00 $856.44 5724 S
APC SI
PhysicalTherapy
Specialty Service
Non-Facility
(Global)
Facility(Prof-
only)
MedicareReimbursementtoFacilitiesandPhysicians,bySettingandbyMedicareBenefit
Pain
Management
PhysicianFee FacilityFee
ASCOutpatient
HospitalCPT
PartB PartA

P a g e 15 | 16
Below are reimbursements by procedure for the Facility Fee (in an ASC or HOPD) or for the Technical Component of a global fee paid for services in a physician office:
At new HOPDs, reduction in Service facility-related Medicare reimbursement
Cardiac diagnostics ~ 60+ %
Office visits ~ 50-60 %
Pain management ~ 40-50 %
Surgery ~ 40-50 %
Imaging ~ 40-50 %
Physical Therapy 0 %
Asof: 1/1/2016 Atlanta
Specialty Service CPT (TConly) CommentsAll Officevisit,establishedpatient,Level4 99214 $29 n/a $102 $73 250%
Imaging MRIJointLowerExtw/ocontrast 73721 $169 $153 $274 $121 79%MRILunbarspinew/ocontrast 72148 $149 $148 $274 $126 83%
PTevaluation 97001 $76 n/a $76 $0 0%Manualtherapy(per15minutes) 97140 $30 n/a $30 $0 0%Therapeuticexercises 97110 $33 n/a $33 $0 0%E-Stim1/>notWndCarePart G0283 $14 n/a $14 $0 0%
Cardiology CardiacRehab 93798 $11 n/a $104 $93 832%Echo 93306 $167 n/a $417 $250 150%NuclearStressTest/TMST 78452 $415 n/a $1,108 $694 167%Pulmonarystresstest/simple 94620 $26 n/a $91 $65 252%StressECHO 93351 $188 n/a $417 $228 121%
GI DiagnosticColonoscopy 45378 $187 $421 $753 $332 79% GIswilltypicallyownanASC
Orthopedics Kneearthroscopy/surgery 29881 n/a $1,340 $2,396 $1,056 79%Wristendoscopy/surgery 29848 n/a $814 $1,455 $642 79%
Injforamenepidurall/s 64483 $108 $327 $585 $258 79%Injforamenepiduraladd-on 64484 $36 $0 $0Injectspinec/t 62310 $134 $327 $585 $258 79%Injectspinel/s(cd) 62311 $135 $327 $585 $258 79%Injecttriggerpoints=/>3 20553 $21 $35 $224 $189 537%
Pulmonary SleepLab 95810 $510 n/a $856 $347 68%
Site-of-ServiceDifferential
PainManagemen
MDswillusuallytrytoperformtheseproceduresinan(owned)ASC
PhysicalTherapy
ReimbursementbySetting HospitalPremiumoverlower-costsetting
ASC/Other
OutpatientHospital
MedicareReimbursementforCommonOutpatientProcedures:FacilityFeeor"TechnicalComponent(TC)"ofGlobalFee
PhysicianOffice
Facil ityFee

P a g e 16 | 16
Overview of Progressive Healthcare
Founded in 1997, Progressive Healthcare is a healthcare advisory services firm that provides:
• Consulting (strategic, financial, operational)
• Outsourced Services (ambulatory clinic set-up and management, Medicare CCM, ACO management).
We focus on Integration:
• Physician-hospital
• Clinical, financial, and programmatic
• Provider and payors / employers
Our offices are located in Nashville and Atlanta.
Contacts:
Rick Buchsbaum [email protected]
Bob Cameron [email protected]
Pete Dandalides, MD [email protected]
Jim Price [email protected]





























