Embed Size (px)
Citation preview

736 • AORN JOURNAL
MARCH 2006, VOL 83, NO 3 Health Policy Issues
single surgical procedure ina hospital may require par-ticipation from a number ofhealth care providers. Forexample, a surgeon, an an-
esthesiologist or nurse anesthetist, a cir-culating nurse, and a surgical assistantall may be present during the surgicalprocedure. Although they are all partic-ipating in the same procedure, themanner in which they receive Medicarereimbursement for their services variesgreatly.
MEDICARE OVERVIEWMedicare is the health insurance pro-
gram run and funded by the federalgovernment for eligible beneficiaries.The Centers for Medicare and MedicaidServices (CMS) is responsible for pro-gram oversight. Within Medicare thereare two ways practitioners in the surgi-cal suite may be reimbursed, throughMedicare Part A or Medicare Part B.These are two separate insurance pro-grams with different funding sources. Aglossary of common terms for MedicarePart A and B is listed in Table 1.
Medicare Part A is the hospital insur-ance plan funded by payroll taxes. Itpays for all inpatient hospital servicesused by Medicare beneficiaries. Phys-icians, nonphysician practitioners (NPPs)and hospital outpatient costs are reim-bursed through Medicare Part B.Beneficiary monthly premiums and gen-eral revenue dollars fund Medicare PartB. Hospital- or practice group-employedphysicians or NPPs do not bill inde-pendently for their services becausereimbursement from Medicare Part B isassigned to the hospital or practicegroup through a contractual arrange-ment between the provider and the hos-pital or practice group.1
These are two separate programswith different funding sources, so the
dollars in Medicare Part A are notaffected by those in Medicare Part Band vice versa. Although it may seemthat some services are paid for by bothMedicare Part A and Medicare Part B,the separation of the payment systemsallows the CMS to view reimburse-ment to hospitals as distinct from reim-bursement to physicians and NPPs.2
This is an important distinction whenadditional providers request separatereimbursement for their services to eli-gible Medicare beneficiaries.
Reimbursement tohospitals made throughMedicare Parts A and Bis composed of two sep-arate prospective pay-ment systems (PPSs).3,4
The PPS is a system ofpredetermined ratesthat Medicare uses toreimburse hospitals forinpatient and outpatientservices, as well as toreimburse skilled nurs-ing facilities, rehabilita-tion hospitals, andhome health services.5
The PPS is furtherdivided into two forms:the inpatient PPS,known as the IPPS, andthe outpatient PPS,known as the OPPS.The IPPS reimburses Medicare Part Ahospital expenditures; the OPPSreimburses Part B hospital expendi-tures. Physicians and NPPs are reim-bursed by Medicare Part B via thephysician fee schedule.6
According to the CMS there are sixcore elements to a PPS payment:• the standardized amounts, which
are the basic payment amounts;• a wage index to account for
differences in hospital labor costs;
Medicare reimbursementin the surgical suite
H E A L T H P O L I C Y I S S U E S
Melinda Johnson
A
Although manypeople are
working on thesame procedure,the manner in
which theyreceive Medicarereimbursementvaries greatly.
738 • AORN JOURNAL
MARCH 2006, VOL 83, NO 3 Health Policy Issues
• the diagnosis-related group(DRG) relative weights,which account for differ-ences in the mix of patientstreated across hospitals;
• an add-on payment forhospitals that serve a dis-proportionate share oflow-income patients;
• an add-on payment forhospitals that incur indi-rect costs of medical edu-cation; and
• an additional payment forcases that are unusuallyexpensive (ie, outliers).7
MEDICARE PART AREIMBURSEMENT
The IPPS is made up oftwo component payments (ie,capital and operating). Eachof these components is multi-plied by the DRG code. Thecapital component is intendedto compensate the hospital for
TABLE 1Medicare Glossary
its capital expenditures andthe physical building. Theoperating component paysfor the employees of the hos-pital and the actualmedical/surgical procedures,together with accompanyingservices (eg, magnetic reso-nance imaging, computedtomography scans).8-10
The DRG code calculationtakes into account primaryand secondary diagnoses,
Actual acquisition costThe net cost to the pharmacy of a medicationreimbursed by Medicare or Medicaid.
Actual chargeThe charge made by a hospital or other supplierof medical services; the data is used as a test of“reasonable charges.”
BeneficiaryThe enrollee in an insurance program and the onewho is entitled to receive its benefits; anyMedicare, Medicaid, or commercial insurancemember. Individuals entitled to Medicaid often arereferred to as “recipients” rather than beneficiaries.
The Centers for Medicare and MedicaidServices (CMS)The agency within the Department of Health andHuman Services, formerly known as the HealthCare Financing Administration (HCFA), thatadministers the Medicare and Medicaid programs.
CMS form 855RThe application form that allows individualhealth care practitioners to reassign Medicarebenefits to the organization with which the prac-titioner has an employment or independent-contractor relationship.
Current procedural terminology (CPT)Codes developed by the American MedicalAssociation (AMA) to describe physician proce-dures. The AMA develops and maintains theCPT codes and their meanings. These CPT codesare used to bill third-party payers.
Diagnosis-related group (DRG)A system using categories for classifying patients
according to diagnosis. Under the Medicareprospective payment system, the assumption isthat patients within these diagnostic categoriespresent with similar clinical symptoms andrequire similar hospital and medical resourcesduring treatment.
Fee scheduleA listing of the maximum fees that an insurerwill pay for services, procedures, tests, anddevices. Physician fee schedules typically arebased on CPT codes.
Hospital insuranceHospital insurance, also known as Medicare PartA, is an insurance program that provides basicprotection against the costs of hospital-relatedhealth services for people age 65 years or olderwithin the Social Security or Railroad Retirementsystems, as well as some disabled individuals.
Inpatient prospective payment system(IPPS)The Medicare system of payments to hospitalsbased on predetermined rates for the DRGassigned to each patient. In the aggregate, thehospital keeps the difference between its costs oftreating Medicare patients and the paymentsreceived from Medicare. Hospitals are at risk forcosts incurred above these prospectively deter-mined payments. In cases that are unusuallyexpensive (eg, outlier cases), the IPPS is increased.
Major diagnostic category (MDC)This classification of diagnoses, typicallygrouped by anatomic systems, is the basis forthe DRG prospective payment system. EachDRG falls into an MDC. Diagnosis-relatedgroups are assigned to report inpatient services
AORN JOURNAL • 739
Health Policy Issues MARCH 2006, VOL 83, NO 3
surgical procedures, age, gen-der, complications, and dis-charge status.11 Among otherelements, the DRG includesnursing costs for circulatingnurses, assistants, and staffnurses; costs of surgical andmedical supplies and pharma-ceuticals; and the costs forrecovery in a hospital.12 TheDRG is adjusted to take intoconsideration other factorssuch as hospital type (eg,
long-term care, rural, teach-ing, urban, psychiatric);patient outliers; wage rates inthe labor market; and numberof insured patients served.11
This final number is calledthe DRG weight. In deter-mining the payments foreach surgical procedure, theCMS has collaborated withthe American College of Sur-geons to establish what typeof services and equipment
are needed for each specificsurgical procedure and hascalculated those cost esti-mates into each DRG.13 Forexample, if a surgical proce-dure requires an assistant, ascrub person, a circulatingnurse, or a substantial num-ber of medical and surgicalsupplies, the DRG paymentfor that procedure is weight-ed higher to reflect thegreater costs to the hospital
TABLE 1Medicare Glossary (continued)
to Medicare, Medicaid, and private payers anddetermine payment.
MedicareMedicare provides health insurance benefits toolder adults (ie, age 65 or older), some disabledpeople, and people with end-stage renal disease. Itis funded by the federal government and adminis-tered by the CMS, although most enrollees pay amonthly premium for Part B coverage. Medicarehas 3 parts; Part A Hospital Insurance, Part BSupplementary Medical Insurance, and Part CMedicare + Choice. Part A covers institutionalservices such as hospitalization, nursing homecare, hospice, skilled nursing facility services, andthe services of a home health agency. Part B covershospital outpatient services, physician services,laboratory and radiology services, ambulance,durable medical equipment, orthotics, and pros-thetics. Part C governs plans that manageMedicare coverage for members; many of theseplans are health maintenance organizations orother types of managed care plans.
Outpatient prospective payment system(OPPS)This system is Medicare’s method of compensat-ing hospitals for outpatient services based onpredetermined rates.
Physician fee scheduleThe Medicare physician’s fee schedule delineatesdifferent payment fees (ie, facility and nonfacili-ty) based on the places where physicians provideservices. The nonfacility fee is higher than thefacility fee because nonfacility physicians typical-ly incur the costs of the resources associated withtheir service. Medicare payments to a facilitycover the clinical staff, supplies, and equipment
needed to care for the patient in the facility.
Prospective payment systemA system of predetermined rates that Medicareuses to reimburse for inpatient and outpatientservices.
ProviderA dispenser of health care products and servicesthat are reimbursable under the Medicare pro-gram. Providers are given a provider number,which allows them to bill Medicare and be reim-bursed according to regulations. Under Medicare,the term provider sometimes is used to refer onlyto institutional providers, such as hospitals, but atother times is used more broadly to includephysicians and other types of practitioners.
ReimbursementThe actual payments received by providers forservices rendered, based on benefits coveredunder an insurance plan.
Relative weightAn assigned weight for each DRG that is intend-ed to reflect the estimated relative cost of hospitalresources used with respect to charges associatedwith a specific DRG compared to discharges clas-sified to other DRGs. The higher the relativeweight, the greater the payment.
Supplementary medical insurance (SMI)Also known as Medicare Part B, SMI is a volun-tary insurance program that provides insurancebenefits for physician services and other profes-sional services in accordance with the provisionsof Title XVIII of the Social Security Act. The pro-gram is financed by premium payments fromenrollees together with federal funds.

AORN JOURNAL • 741
MARCH 2006, VOL 83, NO 3 Health Policy Issues
for such services. If a proce-dure is relatively uncompli-cated, the DRG weight isless, reflecting the lowercosts to the hospital.12 Thereare more than 500 DRGcodes. The CMS adjusts theDRG component valuesannually to account forchanges in hospital costs andtechnology. No specificgroups of employees in thehospital are identified forseparate or additional pay-ments under either the oper-ating component or theDRG.
Each patient is assignedone DRG code on admit-tance to the hospital, andone lump sum payment ismade per patient based onthe DRG assignment. TheDRG system was establishedto create an incentive for thehospital to operate more effi-ciently and more profitably.14
Before 1983, hospitals werereimbursed based on a per-centage of actual cost reflect-ed in line item billing.
MEDICARE PART BREIMBURSEMENT
Originally, Medicare Part Breimbursed only physiciansand hospitals for the servicesthey provided to eligible ben-eficiaries. Hospitals are reim-bursed for their outpatientservices under Medicare PartB through the OPPS, whichwas established by the CMSin 2000 and created more than700 ambulatory payment clas-sifications, or APCs. Similar toDRGs, APCs “are establishedfor groups of procedures orservices based on a set of rela-
tive weights, a conversion fac-tor, and an adjustment forgeographic differences.”14
In 1977, in response to ashortage of physicians in ruralareas, Congress enacted theRural Health Clinic ServicesAct (PL 95-210) to allow NPPs(ie, physician assistants and
nurse practitioners) to billMedicare for services theyprovide to eligible beneficiar-ies.15 Eventually, the CMSexpanded Medicare to allowNPPs to be reimbursedregardless of their location.
Physicians and NPPs arereimbursed based on a physi-cian fee schedule that isestablished by the CMS andupdated annually. Currently,the CMS recognizes four cat-egories of NPPs:• physician assistants who
are under the supervisionof a physician,
• nurse practitioners andclinical nurse specialists
who are working in collab-oration with a physician,
• certified nurse midwives,and
• certified RN anesthetists. The NPP’s services are onlyreimbursed when they“would be physicians’ servic-es if furnished by a physician”and are within the NPP’slegal scope of practice.16
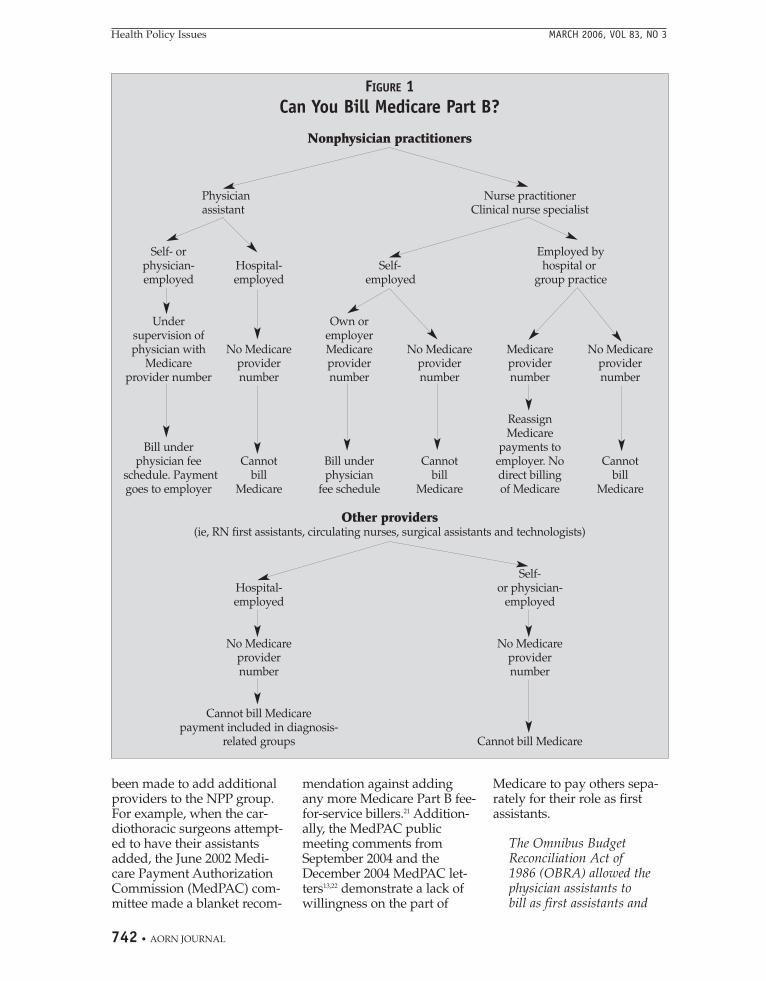
Nonphysician practition-ers receive reimbursementfrom Medicare in three ways.First, eligible NPPs may billMedicare Part B directly fortheir services under thephysician fee schedule usingtheir own provider numberor the provider number oftheir employer. In this case,NPPs or their employersreceive a percentage (ie, 80%to 85%) of the fee schedulepayment. Second, servicesmay be billed incident tophysician services, in whichcase the physician bills forthe services at 100% of the feeschedule payment, eventhough NPPs provided theservices. The major exceptionto this rule is that Medicarewill not cover or pay sepa-rately for “incident to” serv-ices that are furnished in ahospital setting, whether theyare furnished on an inpatientor outpatient basis.17-19 Finally,an NPP can be reimbursed byMedicare through the pay-ment bundle (ie, DRG) forservices provided in hospitalsand skilled nursing facili-ties.20 Figure 1 presents analgorithm for determiningwhether an NPP can billMedicare Part B.
Over the years, efforts have
The diagnosis-relatedgroup system was
established to createan incentive for
hospitals tooperate more
efficiently and moreprofitably.
742 • AORN JOURNAL
Health Policy Issues MARCH 2006, VOL 83, NO 3
been made to add additionalproviders to the NPP group.For example, when the car-diothoracic surgeons attempt-ed to have their assistantsadded, the June 2002 Medi-care Payment AuthorizationCommission (MedPAC) com-mittee made a blanket recom-
mendation against addingany more Medicare Part B fee-for-service billers.21 Addition-ally, the MedPAC publicmeeting comments fromSeptember 2004 and theDecember 2004 MedPAC let-ters13,22 demonstrate a lack ofwillingness on the part of
Medicare to pay others sepa-rately for their role as firstassistants.
The Omnibus BudgetReconciliation Act of1986 (OBRA) allowed thephysician assistants tobill as first assistants and
FIGURE 1Can You Bill Medicare Part B?
Nonphysician practitioners
Physician Nurse practitionerassistant Clinical nurse specialist
Self- or Employed byphysician- Hospital- Self- hospital oremployed employed employed group practice
Under Own orsupervision of employerphysician with No Medicare Medicare No Medicare Medicare No Medicare
Medicare provider provider provider provider providerprovider number number number number number number
ReassignMedicare
Bill under payments tophysician fee Cannot Bill under Cannot employer. No Cannot
schedule. Payment bill physician bill direct billing billgoes to employer Medicare fee schedule Medicare of Medicare Medicare
Other providers(ie, RN first assistants, circulating nurses, surgical assistants and technologists)
Self-Hospital- or physician-employed employed
No Medicare No Medicareprovider providernumber number
Cannot bill Medicarepayment included in diagnosis-
related groups Cannot bill Medicare
AORN JOURNAL • 743
Health Policy Issues MARCH 2006, VOL 83, NO 3
they were paid 65 percentof the physician firstassistant fee at the time.The expenditures were tobe subtracted from thehospital payments. Thisdid not happen. In fact inOBRA ‘90 they rescindedthat payment subtraction.It’s an important pointthough. From the begin-ning, the payment forphysician assistants andfirst assisting serviceswere recognized as dupli-cating hospital payments.PA first assistants, alongwith operating roomnurses and other operat-ing room personnel wereconsidered part of theservices the hospitals wereproviding, and thereforewere considered to beincluded in the hospitalpayment.22
FUTURE CHANGESHistorically, the CMS has
been reluctant to open Med-icare Part A to substantivechanges, which include mate-rially amending the DRGpayment by separately pay-ing any providers who areemployed by the hospital,because of the complexity ofthe PPS. The CMS addedproviders to Medicare Part B,but only after significant evi-dence demonstrated the needfor those providers andalways to help alleviate aphysician shortage.23
Although it appears that newproviders are entering the ORarena and being reimbursedfor their services, only thosegroups that the CMS has
specifically recognized are eli-gible for reimbursement byMedicare.❖
MELINDA JOHNSONSENIOR LEGISLATIVE ANALYST
GOVERNMENT AFFAIRS DEPARTMENT
NOTES1. “Application for individualhealth care practitioners to reas-sign Medicare benefits,” (Nov 1,2001) Centers for Medicare &Medicaid Services, http://new.cms.hhs.gov/CMSForms/CMSForms/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=1&sortOrder=ascending&itemID=CMS019478 (accessed 19 Jan 2006).2. T R Marmor, The Politics ofMedicare (New York: A deGruyter, 2000).3. “Report to the Congress: Medi-care Payment Policy,” (March2000) Medicare Payment AdvisoryCommission, http://www.medpac.gov/publications/congressional_reports/Mar00%20Entire%20report%20.pdf (accessed 19 Jan 2006).4. “GAO letter to CongressmanPete Stark,” (Sept 1, 2000),Government AccountabilityOffice, http://www.gao.gov/archive/2000/he00177r.pdf (accessed 19Jan 2006).5. “Medicare inpatient hospitalprospective payment system,”Stryker Reimbursement, http://www.stryker.com/reimbursement/pdfs/medicareipps0804.pdf(accessed 19 Jan 2006).6. “Physician fee schedule,”Centers for Medicare & MedicaidServices, http://www.cms.hhs.gov/PhysicianFeeSched/ (accessed 19Jan 2006).7. Z Huang, “Calculating hospital-specific DRG payments,” (January2003) Research Data AssistanceCenter, http://www.resdac.umn.edu/Tools/TBs/TN-004.asp (accessed 19Jan 2006).8. K Dalton, R T Slifkin, “PPSinpatient payment and the areawage index,” in North CarolinaRural Health Research and PolicyAnalysis Center Fact Sheet (Jan 22,2001), The Cecil G Sheps Center
for Health Services Research,http://www.shepscenter.unc.edu/research_programs/rural_program/fb67.pdf (accessed 19 Jan 2006).9. G M Carter, “Assessing the FY1989 change in Medicare PPS out-lier policy—Fiscal year; prospec-tive payment system,” Health CareFinancing Review 14 no 2 (1992) 69-82. 10. “Medicare prospective pay-ment system,” American Hos-pital Directory, http://www.ahd.com/pps.html (accessed 19 Jan2006).11. R E Roseblatt, S A Law, SRosenbaum, Law and theAmerican Health Care System,(Westbury, NY: Foundation Press,1997) 477.12. C Moora, personal communi-cation with the author, Littleton,Colo, 15 Oct 2005.13. Medicare Payment AdvisoryCommission communication withVice President Richard B. Cheney(Dec 30, 2004), Medicare PaymentAdvisory Commission, http://www.medpac.gov/publications/congressional_reports/Dec04_CRNFA.pdf (accessed 16 Jan 2006).14. “Medicare outpatient hospitalprospective payment system,”Stryker Reimbursement, http://www.stryker.com/reimbursement/pdfs/medicareopps0804.pdf(accessed 16 Jan 2006).15. “Starting a rural health clin-ic—A how-to manual,” USDepartment of Health andHuman Services, http://rural-health.hrsa.gov/RHC/RHCManual/RHCmanualintro.htm (accessed 19Jan 2006).16. “Title 42, Chapter 7, Section1395x (K)(i)(ii),” Cornell LawSchool US Code Collection,http://www4.law.cornell.edu/uscode/html/uscode42/usc_sec_42_00001395---x000-.html (accessed 19 Jan2006).17. “Medicare and ‘incident to’payment: Coverage of nursingservices in hospital outpatientclinics and emergency depart-ments,” American NursesAssociation, http:// www.nursing-world.org/readroom/inciden2.htm(accessed 19 Jan 2006).
744 • AORN JOURNAL
MARCH 2006, VOL 83, NO 3 Health Policy Issues
18. “Summary of P.L. 98-21,(H.R. 1900) Social SecurityAmendments of 1983,” SocialSecurity, http://www.ssa.gov /history/1983amend.html(accessed 19 Jan 2006).19. “P.L. 99-509, ApprovedOctober 21, 1986 (100 Stat 1874)Omnibus Budget ReconciliationAct of 1986,” Social Security, Officeof Disability and Income SecurityPolicy, http://www.socialsecurity.gov/OP_Home /comp2/F099-509.html(accessed 19 Jan 2006).20. Report to the Congress.
Medicare Payment to AdvancedPractice Nurses and PhysicianAssistants (Washington, DC:Medicare Payment AdvisoryCommission, June 2002). Alsoavailable at http://www.medpac.gov/publications/congressional_reports/jun02_NonPhysPay.pdf (accessed19 Jan 2006).21. Report to the Congress.Medicare Coverage of NonphysicianPractitioners (Washington, DC:Medicare Payment AdvisoryCommission, June 2002). Alsoavailable at http://ww.medpac.gov
/publications/congressional_reports/jun02_NonPhysCoverage.pdf(accessed 19 Jan 2006).22. “Medicare Payment AdvisoryCommission—Public meeting,”Medicare Payment AdvisoryCommission, http://www.medpac.gov/public_meetings/transcripts/090904_CRNS_DG _transc.pdf(accessed 19 Jan 2006).23. S Wysocki, “Rural health care:A challenge and opportunity fornurse practitioners,” NursePractitioner Forum 1 (September1990) 68-70.
Although the quality of health care for Americanshas improved modestly and health care inequali-
ties are narrowing overall for many minority Ameri-cans, disparities have widened in both quality ofcare and access to care for Hispanics, according to aJan 9, 2006, news release from the Agency forHealthcare Research and Quality (AHRQ). The AHRQ’s2005 reports on national health care quality and dis-parities focused on four key areas of health care—effectiveness, patient safety, timeliness, patient cen-teredness. The quality report employed measuresincluding health care outcomes (eg, incidence ofhealth care-acquired infections, reductions in deathsfrom certain diseases) and use of specific treatmentsthat are known to work most effectively. The dispari-ties report compared these measures by race, ethnic-ity, and income and also measured access to careusing indicators such as health insurance status andfrequency of visits to physicians.
The 2005 quality report found that overallquality of care for all Americans improved by 2.8%,although improvement has been much more rapidin some measures, especially where there have beenfocused efforts to improve care. Improvements weregreatest in quality measures for diabetes, heart dis-ease, respiratory conditions, nursing home care, andmaternal and child health care, with an overall rateof change of 5.4% for these measures.
The 2005 disparities report found that low-income people, regardless of race or ethnicity,experienced the largest disparities in measures ofhealth care quality and access. Overall, racial dis-parities in quality of care and access to care were
narrowing for blacks, Asians, and American Indians/Alaska Natives. For Hispanics, however, the majorityof disparities for both quality and access weregrowing wider. Findings from the disparities reportinclude the following.• Rates of late-stage breast cancer decreased
more rapidly from 1992 to 2002 among blackwomen (ie, 169 per 100,000 to 161 per100,000) than among white women (ie, 152 per100,000 to 151 per 100,000), resulting in anarrowing disparity.
• Although the quality of patient-provider commu-nication as reported by patients themselvesimproved from 2000 to 2002 among white adults(ie, 93% to 94%), it declined among Hispanicadults (ie, 87% to 84%).
• Treatment of heart failure improved more rap-idly from 2002 to 2003 among American Indi-an Medicare beneficiaries (ie, 69% to 74%)than among white Medicare beneficiaries (ie,73% to 74%), resulting in the elimination ofthis disparity.
• Access to a usual source of care increased slight-ly from 1999 to 2003 for Hispanics (ie 77% to78%) and whites (ie, 88% to 90%), but Hispan-ics were less likely to have access to a usualsource of care.
AHRQ Releases 2005 National Healthcare Quality andDisparities Reports (news release, Rockville, Md: Agencyfor Healthcare Research and Quality, Jan 9, 2006) http://www.ahrq.gov/news/press/pr2006/nhqrdrpr.htm(accessed 13 Jan 2006).
Health Care Quality and Disparities Show Improvement





























