Embed Size (px)
Citation preview

Medically important RNA Viruses

Retroviruses

Retroviruses
• Probably the most studied group of viruses in molecular biology!!!
• Enveloped, positive-strand RNA viruses
• Unique morphology and replication
• Replicate through a DNA intermediate by reverse transcriptase (RT)
Retroviruses
• Baltimore and Temin in 1970
• RNA-dependent DNA polymerase (reverse transcriptase ) encoded by retroviruses
• Retroviruses replicate through an DNA intermediate
• This DNA copy of viral genome integrates into host chromosome
• This discovery earned the Nobel prize: contradicted the central dogma of molecular biology-genetic information passed from DNA to RNA and then to protein
•Here: from RNA to DNA
History
• Rous sarcoma virus: solid tumors in chicken
• Other cancer causing retroviruses from other animal species (oncogenes)
• 1981: first human retrovirus: Human T-lymphotropic virus (HTLV-1)
• 1983: Human immunodeficiency virus (HIV)
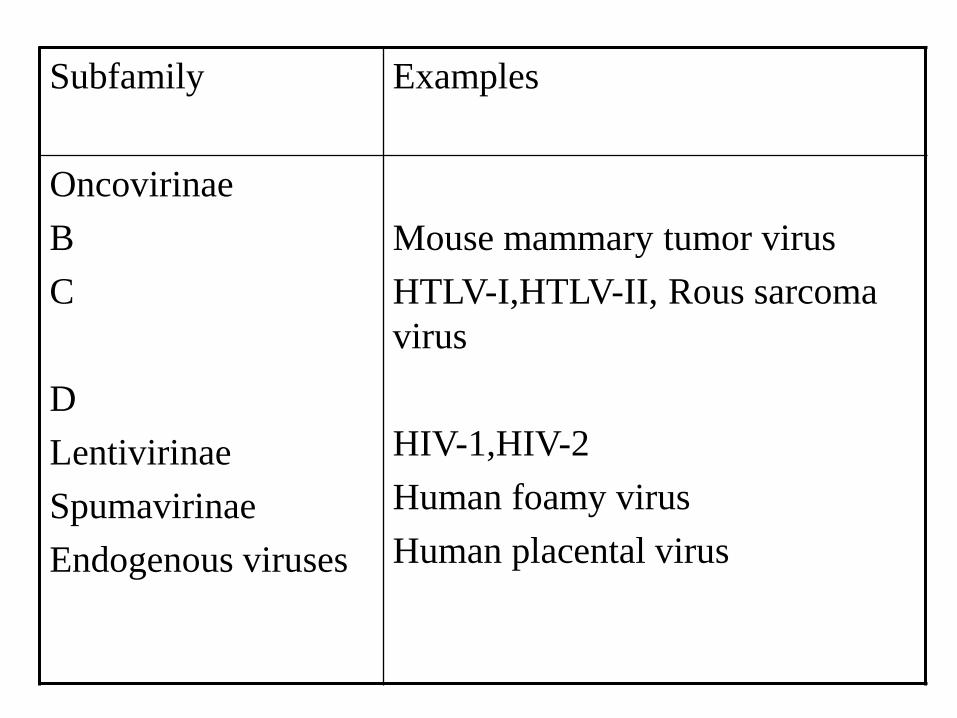
Subfamily
Examples
Oncovirinae
B
C
D
Lentivirinae
Spumavirinae
Endogenous viruses
Mouse mammary tumor virus
HTLV-I,HTLV-II, Rous sarcoma
virus
HIV-1,HIV-2
Human foamy virus
Human placental virus

• Oncoviruses:immortalize or transform target cells, A,B,C,D type according to their core and capsid
• Lentiviruses:slow viruses associated with neurologic and immunosuppresive disease
• Spumaviruses:no disease
• Endogenous viruses:transmitted vertically, 1% of human chromosome, in many animal species and humans, one detected in placental tissue which facilitates placental function

Retroviruses
•Enveloped sperical virion
•Two copies of positive-strand RNA genome
•RT
•Provirus integrates randomly into host chromosome

Retroviruses
•Simple retroviruses encode gag,pol and env genes
•Complex viruses also encode accessory –regulatory genes (tat,rev,nef, vif, vpu for HIV)
•Assembles and buds from the plasma membrane
•Final morphogenesis requires protease cleavage of gag and gag-pol polypeptides after envelopment.





Transmission
*Blood, semen,vaginal secretions
• Sexual contact
• Exposure to contaminated blood and blood products
• From infected mother to her baby perinatally
• No household contact!!!!
Seroconversion
• Usually 3 weeks
• 1.5,3,6 months

Viral Kinetics

Laboratory diagnosis
Serology: Adults and children older than 15 months:
• Initial screening: ELISA, latex agglutination
•Confirmation: Western-blot, rapid HIV-1/2 differential test
Molecular techniques:
-qualitative DNA detection: babies younger than 15 months
-quantitative RNA: follow up of HIV infected people who are on therapy
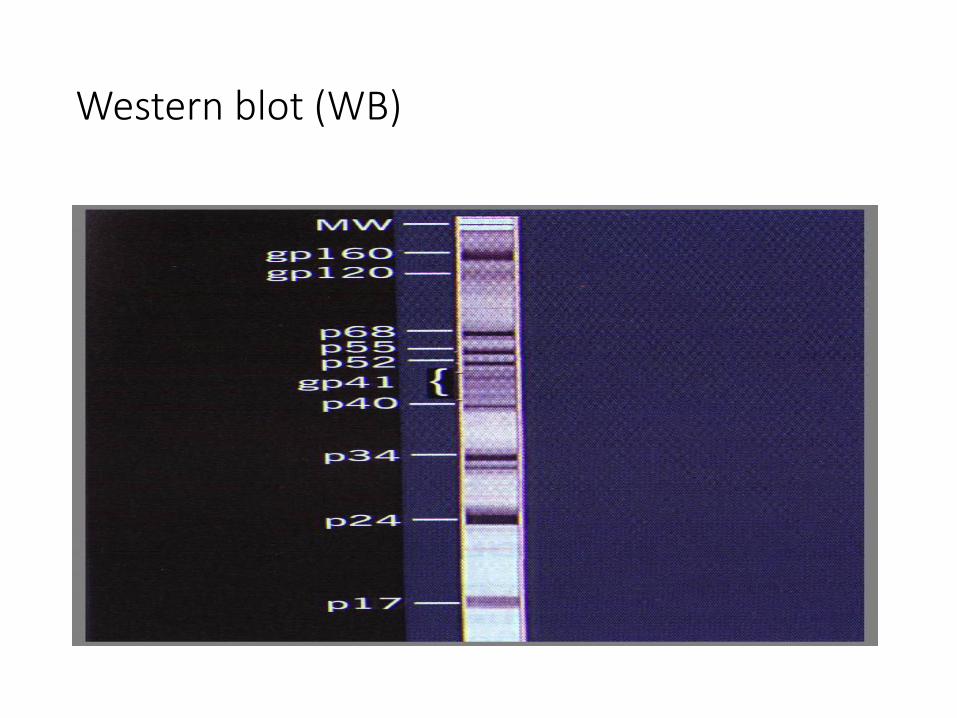
Western blot (WB)


Treatment
Highly Active Antiretroviral Treatment (HAART):
Combined therapy

Prevention and control
•Education
•Blood and blood product screening
• Infection control:
‘Universal Blood and body fluid precautions’:
All patients may be infectious for HIV and other blood-born infections:
-wear protective clothing(gloves, masks, gown) and other barriers to prevent exposure to blood products

Prevention and control
•10% household bleach(% 0.5 chlorine, 5g/litre 5000ppm •70% ethanol •2% glutaraldehyde •4% formaldehyde •6% Hydrogen peroxide •Washing laundry in hot water with detergent is
sufficient to inactivate HIV.

Modes of control
•Antiviral drugs limit progression of disease
•Vaccines for prevention and treatment are in trials
•Safe(Condom!) monogamous sex helps limit spread.
•Sterile injection neeedles should be used
• Large scale screening programs for blood transfusion, organs for transplants, clotting factors
Oncovirinae
• RNA tumor viruses
• Associated with leukemias, sarcomas and lymphomas in many animals
• Not cytolytic
• Distinquished by the mechanism of cell transformation and length of latency period between infection and the development of disease

Oncovirinae
Sarcoma and acute leukemia viruses:
•Protooncogenes(at least 35)
•Highly oncogenic, direct effect
•No human virus
Leukemia viruses: in Humans
•No oncogene
• Long latency period
•HTLV-I,HTLV-II,HTLV-5
Human T lymphotropic virus type 1( HTLV-I)
• Adult acute T-cell lymphocytic leukemia (ATLL)
• HTLV-associated myelopathy (tropical spastic paraparesis)
• Blood transfusion, sexual intercourse, breast feeding
• Long latency period: approximately 30 years

Orthomyxoviruses
• Negative-sense RNA virus
• Segmented genome
• Enveloped
• Hemagglutinin glycoprotein: viral attachment protein and fusion protein-It elicits neutralizing, protective antibody responses

Orthomyxoviruses
•Replicates in cell nucleus but assembles and buds from the plasma membrane
•Segmented genome promotes genetic diversity caused by mutation and reassortment of segments on infection with two different strains
• Influenza A, B and C
• Influenza A infects humans, mammals, and birds (zoonosis)

Orthomyxoviruses
•Only influenza A and B viruses cause significant human disease •Annual epidemics (mutation:drift) •Periodic pandemics(reassortment:shift) 1918-19:20 million death 1947 1957 1968
1977 2009

Influenza virus
• Virus likes cool,humidity (winter)
• Spread by inhalation of small aerosols
• Cell culture
• Antigen
• PCR

Influenza virus
• Rimantadine,Amandatine: inhibits uncoating of influenza A
• Zanamavir and oseltamivir: NA inhibitors
• Influenza vaccine: trivalent formalin inactivated, every year
Coronaviruses

Coronaviruses
• Named for solar corona-like appearance (surface projections) by electron microscope
• Second most prevalent cause of common cold( rhinovirus the first!)
• Gastroenteritis

Coronaviruses
• Positive RNA viruses
• Enveloped
• Infects epitelial cells
• Localizes to the upper respiratory tract (33-35° C)
• Spread by aerosol and large droplets

Coronaviruses
• Reinfection occurs in presence of serum antibodies
• Laboratory diagnosis: not routinely performed
• ELISA: acute and convalescent sera

New viruses
• Human metapneumovirus (2001)
• SARS-CoV (2002)
• Human rhinovirus C (2003)
• Human bocavirus (2005)
• HADV-14p1 (2006-ABD, Çin-yüzlerce olgu, mortalite düşük)
• A(H1N1)pdm09
• Influenza A virüsü H3N2 varyant (2011 end-2013 ABD- 340 cases)
• MERS-CoV: Middle East Respiratory Syndrome Corona Virus (2012)
• Influenza A virus H10N8 (2013-China)
• Influenza A virus H7N9 (2013-India 2014 China-448cases, %39 mortality)

Severe Acute Respiratory Syndrome (SARS)
•Came to global attention in February 2003
• In China about 305 cases of atypical pneumonia were reported
• In July 2003, more than 8,000 cases and 780 deaths had been reported from 29 countries worldwide.
•SARS-associated coronavirus (SARS-CoV)

• No one knows if, when, or where SARS-CoV will reappear.
• However, the rapidity of spread of infection and the high levels of morbidity and mortality associated with SARS-CoV call for careful monitoring for the reappearance of SARS-CoV


Noroviruses
• Calicivirus
• diarrhea, nausea, vomiting
• As few as 10 virions will initiate disease in humans:outbreaks

Paramyxoviruses

Paramyxoviruses
3 genera:
•Morbillivirus:
Measles
•Paramyxovirus
Parainfluenza, Mumps,
Nipah virus and Hendra virus: zoonosis
•Pneumovirus
Respiratory syncytial virus (RSV)
Metapneumovirus


Measles(Rubeola)
• Infects epithelial cells of respiratory tract
• Spreads systematically in lymphoctes and by viremia
• Replicates in cells of conjunctivae, respiratory tract, urinary tract, lymphatic system, blood vessels, nervous system
• Rash is caused by T-cell response to virus infected epitelial cells lining capillaries
• Sequelae in nervous system may result from immunopathogenesis (postinfectious measles encephalitis) or development of defective mutants (subacute sclerosing panencephalitis:SSPE)


Measles(Rubeola)
•Sybacute sclerosing panencephalitis (SSPE):late complication :central nervous system manifestations (high level of measles antibodies in the blood and cerebrospinal fluid)
•Specific IgG and IgM by ELISA
•Vaccine:a live attenuated vaccine
•Measles,Mumps Rubella :MMR vaccine
•Exposed susceptible people:immune globulin

Parainfluenza viruses
• 4 serotypes(1-4)
• Respiratory tract infections
• Coldlike symptoms,bronchitis,croup-laryngotracheobronchitis
• No viremia

Mumps
• Very communicable disease like measles by respiratory tract
• One serotype
• Respiratory droplets
• Acute benign parotitis
• Virus is present as long as 7 days before symptoms and 5 days in saliva and 2 weeks in urine after the symtoms
• Spreads by viremia
• Infection of testes and central nervous system occurs
• Vaccine:Live attenuated vaccine (Jeryl Lynn strain)
• Laboratory diagnosis: serology

Respiratory syncytial Virus (RSV)
•The most common fatal acute respiratory tract infection in infants and young children •Does not cuase viremia •Mild infection in reinfection •RSV antigen in nasopharyngeal aspirate by ELISA or
IFA •Treatment: Ribavirin •For premature infants: passive immunization with
anti-RSV immunoglobulin

Picornaviruses
Picornaviruses • Small (pico)
• RNA
• Naked capsid
• >230 members
• 5 genera

Picornaviruses • Enteroviruses
At least 72 serotypes • Polioviruses
• Coxsackieviruses
• Echoviruses

Picornaviridae •Enterovirus
• Poliovirus type 1, 2, and 3 • Coxsackie A virus types 1 to 22 and 24 • Coxsackie B virus types 1 to 6 • Echovirus (ECHO virus) types 1 to 9, 11 to 27, and 29 to 34 • Enterovirus 68 to 71
•Rhinovirus types 1 to 100+
•Cardiovirus
•Aphtovirus
•Heparnavirus • HAV

Picornaviruses • Enteroviruses
• Capsid very resistant facilitates transmission by the fecal-oral route
• Infection initiated in the gastrointestinal tract
• “Rarely cause enteric disease”
• Infections are usually asymptomatic

Enteroviruses/Epidemiology •“The enteroviruses are exclusively human pathogenes” • Spread by the fecal-oral route •Asymptomatic shedding can occur
•Poor sanitation and crowded living conditions foster transmission of the viruses
•Enterovirus epidemics sewage contamination of water supplies
•Outbreaks in schools & day care centers (summer)
•Spread via resp. tract coxsackie & echov.

Enteroviruses/Clinical syndromes
•Poliovirus infections •Asymptomatic illness (90%) •Abortive poliomyelitis (minor illness) •Nonspecific febrile illness (5%)
•Nonparalytic poliomyelitis or aseptic meningitis • 1 to 2%, symptomes of the minor illness + CNS sm
•Paralytic polio, the major illness • 0.1 to 2.0%

Enteroviruses/Clinical syndromes •Poliovirus infections •Paralytic poliomyelitis • Asymmetrical flaccid paralysis with no sensory loss • Poliovirus type 1 is responsible for 85% of cases • Vaccine-associated disease (reversion of type 2&3) • Recovery, within 6 months to 2 years
•Bulbar poliomyelitis •More severe, 75% death, iron lungs (1950’s) •Postpolio syndrome (30-40 years later) in 20-
80% of the original victims)

Enteroviruses/ Prevention & control “The prevention of paralytic polyomyelitis is one of the triumphs of
modern medicine”
Poliovirus vaccines:
1. IPV, developed by Jonas Salk
2. OPV, developed by Albert Sabin (live attenuated)
(refer to your book for details on polio vaccines and new vaccination schemes)

Rhinoviruses •Most important cause of the common cold and URTI •ICAM-1 •Unable to replicate in the GIT •Labile to “ pH” •Grow best @ 33oC •Infection can be initiated by as little as 1 (one) infectious viral particle •“Runny nose”
Rhinoviruses •Most important cause of URTI ~ 50%
•Common cold: •Enteroviruses •Coronaviruses •Adenoviruses •Parainfluenza viruses

Rhabdoviruses

Rhabdoviridae • Rhabdos (greek) rod
• Pathogens of mammals, birds, fish, plants

Rabies virus Unique features of Rhabdoviruses
• Bullet-shaped
• Enveloped
• Negative, single-stranded RNA
• Prototype for (-) RNA viruses
• Replication in the cytoplasm

Rabies virus/Disease Mechanisms
• Rabies is usually transmitted in saliva and is acquired from the bite of a rabid animal
• Virus is not very cytolytic and seems to remain cell-associated
• Virus replicates in the muscle at the site of the bite with minimal or no symptoms
• The length of the incubation phase is determined by the infectious dose and the proximity of the infection site to the CNS and brain

Rabies virus/Epidemiology • Transmission
•Zoonosis • Reservoir: wild animals • Vector: wild animals and unvaccinated dogs and cats • Source of virus:
• Major: saliva in bite of a rabid animal
• Minor: aerosols in bat caves containing rabid bats

Rabies virus/Epidemiology • At risk:
•Veterinarians and animal handlers •Person bitten by a rabid animal • Inhabitants of countries with no pet vaccination program

Rabies virus/Epidemiology • Geography/Season
•Worldwide •Except in some island nations •No seasonal incidence

Rabies virus/Epidemiology • Modes of control
•Vaccination • For pets • For at-risk personnel “Vaccination program have been implemented to
control rabies in forest mammals”

Rabies virus/Laboratory diagnosis
• Occurence of neurologic symptoms in a person who has been bitten by an animal
• ... too late...
• Laboratory tests are usually performed to confirm the diagnosis and to determine whether a suspected individual or animal is rabid post mortem

Rabies virus/Treatment & Prophylaxis • Clinical rabies is almost always fatal unless treated
• Only hope:
•Post exposure prophylaxis •For anyone exposed by bite or by contamination of an open wound or mucous membrane to the saliva or brain tissue of an animal suspected to be infected with the virus

Rabies virus/Treatment & Prophylaxis • First protective measure
•Local treatment •Washing •Rabies antiserum
• Then
•Vaccination •Ig (HRIG or EAS)
Rotaviruses
• Cause infantile diarrhea in winters

Togaviruses and Flaviviruses Arboviruses

Togaviruses and Flaviviruses
Virus group Human pathogens
Togaviruses
Alphavirus
Rubivirus
Pestivirus
Arterivirus
Flaviviruses
Hepaciviridae
Arboviruses
Rubella virus
None
None
Arboviruses
Hepatitis C virus
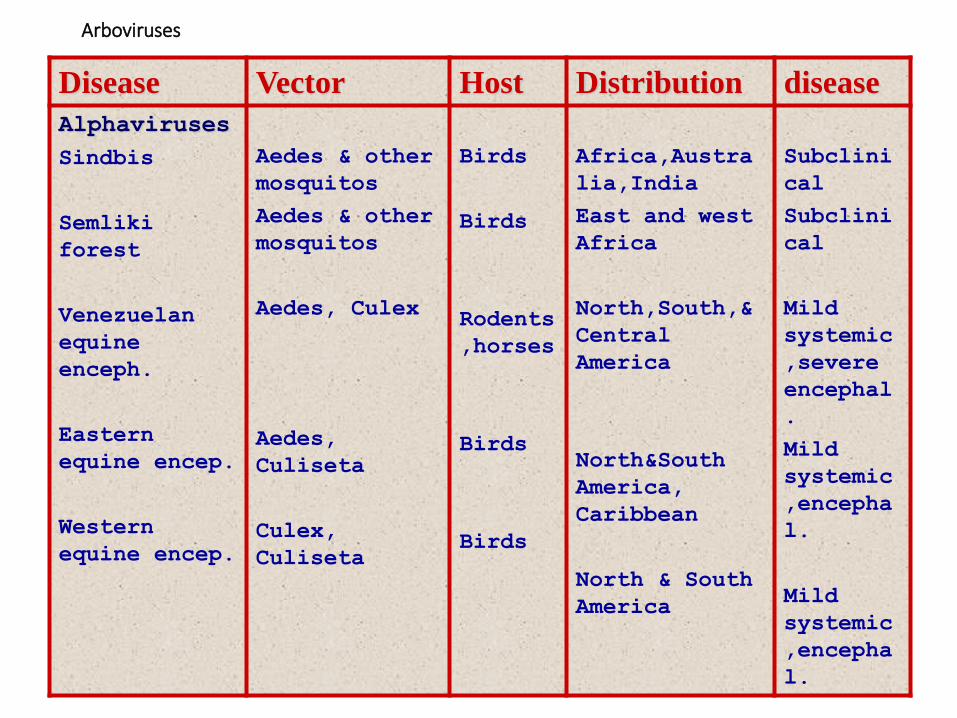
Arboviruses
Disease Vector Host Distribution disease
Alphaviruses
Sindbis
Semliki
forest
Venezuelan
equine
enceph.
Eastern
equine encep.
Western
equine encep.
Aedes & other
mosquitos
Aedes & other
mosquitos
Aedes, Culex
Aedes,
Culiseta
Culex,
Culiseta
Birds
Birds
Rodents
,horses
Birds
Birds
Africa,Austra
lia,India
East and west
Africa
North,South,&
Central
America
North&South
America,
Caribbean
North & South
America
Subclini
cal
Subclini
cal
Mild
systemic
,severe
encephal
.
Mild
systemic
,encepha
l.
Mild
systemic
,encepha
l.

Arboviruses Disease Vector Host Distribution disease
Alphaviruses
Chikungunya
Aedes
Humans,
Monkeys
Africa, Asia
Fever,
Arthralg
ia,
arthriti
s

Arboviruses Disease Vector Host Distribution disease
Flaviviruses
Dengue
Yellow fever
Aedes
Aedes
Humans,
Monkeys
Humans,
monkeys
Worldwide,esp.
Tropics
Africa, South
America
Mild
systemic;
break-bone
fever,
dengue
hemorrhagic
fever, and
dengue
shock
syndrome
Hepatitis,
hemorrhagic
fever

Arboviruses Disease Vector Host Distribution disease
Flaviviruses
Japanese
encephalitis
West Nile
encephalitis
St. Louis
encephallitis
Russian
spring-summer
encephalitis
Powassan
encephalitis
Culex
Culex
Culex
Ixodes
&
dermoce
ntor
ticks
Ixodes
ticks
Pigs,
birds
Birds
Birds
Birds
Small
mammals
Asia
Afr.,Eur.,Cent
ralAsia,N.Amer
N. America
Russia
N. America
Encephaliti
s
Fever,
encep.,
hepatitis
Encephaliti
s
Encephaliti
s
Encephaliti
s
Togaviruses & Flaviviruses/Clinical syndromes
• Alphavirus disease is usually characterized as low-grade disease • Can progress to encephalitis in humans
• Flavivirus infections are relatively benign • Serious aseptic meningitis, encephalitis, hemorrhagic disesase can occur
Togaviruses & Flaviviruses/Clinical syndromes
•Hemorrhagic disesases •Dengue •Yellow fever viruses
Togaviruses & Flaviviruses/Clinical syndromes
•Hemorrhagic disesases •Dengue virus •Major worldwide problem •100 million cases of dengue fever/year •250 000 cases of dengue hemorrhagic fever/y •Dengue shock syndrome

Togaviruses & Flaviviruses/Clinical syndromes
•Hemorrhagic disesases •Yellow fever viruses •Severe systemic disease •Degeneration of the liver, kidney, heart +
hemorrhages
• “JAUNDICE”
•Mortality rate: ~ 50% during epidemics

Togaviruses & Flaviviruses/Treatment, Prevention, and Control
• No treatment!
• “The easiest means of preventing the spread of any arbovirus is elimination of its vector and breeding grounds”
• Vaccines • Yellow fever live vaccine (17D strain)
• EEE, WEE, Japanese, Russian SSE killed vaccines

Zika virus
•a member of the Flaviridae
• spread by daytime-active aedes mosquitoes
• first isolated in 1947
•Since the 1950s, it has been known to occur within a narrow equatorial belt from Africa to Asia.
•From 2007 to 2016 the virus spread eastward, across the Pacific Ocean to the Americas, leading to the 2015–16 Zika virus epidemic.

Zika virus
•often causes no or only mild symptoms, similar to a very mild form ofdengue fever
• While there is no specific treatment, paracetamol (acetaminophen) and rest may help with the symptoms
•No vaccine
• Zika can spread from a pregnant woman to her baby. This can result in microcephaly, severe brain malformations, and other birth defects
•Zika infections in adults may result rarely in Guillain-Barre syndrome

Zika virus
• In January 2016, the United States Centers for Disease Control (CDC) issued travel guidance on affected countries, • including the use of enhanced precautions, and • guidelines for pregnant women including considering
postponing travel

Rubella virus • Rubella is a respiratory virus

Rubella
•One of the 5 classic childhood exantems •Measles •Roseola •Fifth disease •Chickenpox
Rubella
•Rubella: “little red” in Latin
•“German measles” •Infects URT local lymphe nodes viremia
•Shedding respiratory droplets
•Only one serotype
•Natural infection lifelong protective immunity
Rubella/Clinical syndromes
• Rubella disease • Normally benign • 3 day of maculopapular or macular rash
and swollen glands • More severe in adults

Rubella/Clinical syndromes
• Congenital disease • The fetus is at major risk until the 20th
week of pregnancy • Most common manifestations: • Cataracts • Mental retardation • deafness

Rubella/Treatment, Prevention, and Control
• No treatment
• Vaccination (live)

Bunyaviridae
• 4 genera
1. Bunyavirus
2. Phlebovirus
3. Nairovirus
4. Hantavirus

Bunyaviridae/Epidemiology • Transmission • Via arthropods through break in skin
• At risk: • People in habitat of arthropod vector • California encephalitis group: campers, forest
rangers, woodsmen
• Season • More common in summer
• Modes of control • Elimination of vector or vector’s habitat • Avoidence of vector’s habitat

Bunyaviridae/Clinical syndromes
• Non-specific febrile flu-like illness
• Encephalitis
• Hemorrhagic fever (CCHF-Kırım Kongo Hemorajik ateşi: tick-born)
• Hantavirus pulmonary syndrome

Filoviruses
•Ebola! Causes outbreaks in Africa
•Risk for health care personel.
•A bloodborn infection
•Body fluids
• Isolaton is important