Embed Size (px)
Citation preview

Medical Staff Orientation Manual
Welcome to The Jewish Hospital- Mercy Health Medical Staff A legacy of healing, in the heart of Cincinnati At The Jewish Hospital — Mercy Health, we’re proud of our legacy as the first Jewish hospital in the United States, founded in 1850 to serve the Jewish community of Cincinnati. Yet since the beginning, we’ve been privileged to welcome and care for people of all faiths. To this day, our doctors, residents, nurses and staff remain focused on delivering compassionate care and the best outcomes for patients and their families.
Located at 4777 E. Galbraith Road, Cincinnati, Ohio 45236, 513-686-3000.
The Jewish Hospital — Mercy Health was founded in 1850, when a cholera epidemic sickened thousands of Cincinnatians. The Jewish community saw a need to provide care for poor Jews, and founded the first Jewish hospital in the United States. Since its early days, The Jewish Hospital has always welcomed and cared for people of every faith. The Jewish Hospital’s legacy of teaching the next generation of physicians dates back more than 100 years, and today, residents in surgery, medicine, podiatry and pharmacy all train at The Jewish Hospital. The Jewish Hospital is located in Kenwood, a Cincinnati suburb that provides convenient access from around the Tristate.
Medical Staff Office (513-686-5447) An updated event and meeting calendar and any announcements are located in the physician lounge. Heather Davis is Manager of the Medical Staff at Jewish. Email address is [email protected] Dr. Imran Naqvi is the Vice President of Medical Affairs. His email is [email protected] Medical Staff Members Photo Identification Badge

Obtain a photo identification badge from the Medical Staff Office or Security Department during business hours. This must be worn at all times in the hospital. An extra tab identifies you as a physician. The badge contains an RFID chip that allows entrance to the physician lounge and the external door after hours. It is also used to authenticate medication orders in the electronic medical record. Physician Parking Physician parking is located in two areas. There are parking spaces in the garage and in the back of the hospital. The parking spaces are marked physician parking. Committees of the Medical Staff Monthly Meetings Medical Executive Committee Credentials Committee Advisory Committee Quality Improvement General Cancer Conference (CME offered) Breast Cancer Conference (CME offered) General Staff Meetings, and meetings of the Departments of Medicine and Surgery are scheduled as needed. The annual meeting of the General Staff is held in December during the annual social. 2020 Jewish Hospital Medical Staff Governance Chief of Staff – Robert Stevens, M.D. (chairs MEC) Chief of Staff Elect – Michael Willing, M.D. (chairs Quality committee) Past Chief of Staff – James Essell, M.D. Department Chairs Barry Brook, M.D. – Chief of Medicine Yasir Khan, M.D. – Chief of Surgery Michael Willing, M.D. – Chair of Emergency Medicine Samer Hasan, M.D. – Chair of Orthopaedics Robert Stevens, MD- Chair of Radiology Robert Brarens, DPM – Chair of Podiatry Barry Rubin, MD - Credentials Committee Chair

Patricia J. Davis-HagensPresident & Market Leader
MANAGEMENT ORGANIZATIONAL CHART
Vanessa Vonderhaar-PicardVice President / CNO Patient Services
Imran Naqvi VPMA,
Medical Director Internal Medicine Residency
June 2020
Craig SchmidtVice President / COO
Site Administrator
Mark Slye Director
Facilities and EOC
Ra-Keem JohnsonManager
Environmental Services, Patient TransportationAmbassadors
Ben Brooks Intrim
DirectorEmergency
Department
Ben BrooksManager
RookwoodMedical Center
Ben Brooks Intrim
DirectorEmergency
Department
Ben BrooksManager
RookwoodMedical Center
Robin BaldaufClinical Director
&Neuro Service
Line Leader
Sherry Varney Clinical Manager
ICU / 3 South Overflow
Kirk FisherManagerCath Lab,
Cardiovascular Services, Special procedures, PICC
Jeff BargainierDirector
Peri-operative Services
Emily Hayes Clinical Manager PACU, SDS, PAT,
Endoscopy
Melissa WaltersManager
Central Sterile Processing
Laura KoszoClinical Manager
OR
Jeff BargainierDirector
Peri-operative Services
Emily Hayes Clinical Manager PACU, SDS, PAT,
Endoscopy
Melissa WaltersManager
Central Sterile Processing
Laura KoszoClinical Manager
ORKristen
McSorleyClinical Manager
PCU
Sherry Varney ICU Clinical Manager &
InterimClinical Manager
6 South
VACANTClinical Manager
5 South Acute Rehab
Stephanie Eversole
Clinical Manager 5 Tower
Tammy Weber Clinical Director
Kristen McSorley
Clinical Manager PCU
Sherry Varney ICU Clinical Manager &
InterimClinical Manager
6 South
VACANTClinical Manager
5 South Acute Rehab
Stephanie Eversole
Clinical Manager 5 Tower
Tammy Weber Clinical Director
Tara Mink Director
Oncology & Regional Oncology
Service line leader
Melissa Campbell
Clinical Manager Oncology services
Kitty TierneyManager
Blood Cancer Programing
Tara Mink Director
Oncology & Regional Oncology
Service line leader
Melissa Campbell
Clinical Manager Oncology services
Kitty TierneyManager
Blood Cancer Programing
Amy HughesMedical Library
services
Scott Hobler, MD
Program Director Surgical
Residency Program
Robert Brarens, DPM
Podiatry
Scott Hobler, MD
Program Director Surgical
Residency Program
Robert Brarens, DPM
Podiatry
Amy HughesMedical Library
services
Scott Hobler, MD
Program Director Surgical
Residency Program
Robert Brarens, DPM
Podiatry
Farzan Irani DIO GME
Lee Lopez CFO
VACANTDirector
Case Management
Megan CaseManager
Patient Access
Kim CoyleManager
HIM
Scott DanielsManager Sports
MedicineBlue AshDeerfield
MontgomeryRookwood
Kim CoyleManager
HIM
Scott DanielsManager Sports
MedicineBlue AshDeerfield
MontgomeryRookwood
Andrew Thoman Manager
Supply Chain
Kim CoyleManager
HIM
Scott DanielsManager Sports
MedicineBlue AshDeerfield
MontgomeryRookwood
Andrew Thoman Manager
Supply Chain
Scott Brooks Food and Nutrition Services
Chris Bean Food Service Operations Manager
Scott Brooks Food and Nutrition Services
Chris Bean Food Service Operations Manager
Tiffany Best Regional DIO
AdminRuth Woosley
DirectorRadiology/
Imaging Services
Jennifer ScalesManager Women's Services
Robert Bennett, Manager
Imaging Services
Ruth Woosley Director
Radiology/ Imaging Services
Jennifer ScalesManager Women's Services
Robert Bennett, Manager
Imaging Services
Andrew Seitz Director of
Quality
Ronda SmithDirectorHuman
Resources
Toni KanterDirector Mission,
Volunteer Services, and Spiritual Care
Bobbi Beren Director
Risk Management
Heather DavisProgram manager
Medical Staff ServicesRegional
CME
GME
Tanya SchollManager
Respiratory Therapy,EEG
Ezra BradshawDirector
Pharmacy Services
Michelle TrikillisAcute Rehab
Program Director
Megan Brock Manager
Rehabilitation Services, Cardiac
& Pulmonary Rehab
Stacy ColemanManager
Laboratory Services
Ezra BradshawDirector
Pharmacy Services
Michelle TrikillisAcute Rehab
Program Director
Megan Brock Manager
Rehabilitation Services, Cardiac
& Pulmonary Rehab
Stacy ColemanManager
Laboratory Services
Tanya SchollManager
Respiratory Therapy,EEG
Ezra BradshawDirector
Pharmacy Services
Michelle TrikillisAcute Rehab
Program Director
Megan Brock Manager
Rehabilitation Services, Cardiac
& Pulmonary Rehab
Stacy ColemanManager
Laboratory Services
Mary RockeyOP Resident
Clinic
Renee Lyons Inerim
Supervisor ICU
Stephanie Schram
Supervisor Emergency
Department
Mashayle Colwell Dir
Outreach/Prog

Incident Reporting For Physicians Available Through SafeCare SafeCARE is an electronic reporting system available on all hospital computers. But if you need an alternative, the Medical Staff Office has established a voicemail SafeCARE Reporting Line at 624-4390. Report the facts in a brief narrative and risk management will enter the issue and follow up with you. Remember to specify the patient name and medical record number, location or department, and your contact information.
Bobbi Beren: Director of Risk Management Office: 686-5074 Modified Early Warning System (MEWS) -- Early Detection of Patient Deterioration A nurse may call and mention the MEWS score, which is a scoring system that identifies high risk patients. The score is calculated based on heart rate, blood pressure, respiratory rate, temperature, and neurologic status. The score is calculated in Epic to enable nurses to identify patients who are deteriorating and who need urgent intervention and may call for a Rapid Response Team. Rapid Response Team The Operator overhead pages “Rapid Response Team” and location three times. Respondents include the Hospitalist, ICU Charge RN, and Respiratory therapist. Others like radiology or EKG tech may be called as needed. This is intended for “pre-codes” or significant change in status requiring an immediate evaluation. Staff, patients, family members or visitors can activate the Rapid Response Team by calling the operator. Code Blue The operator overhead pages "Code Blue" and location three times. ICU Charge Nurse assumes leadership role and follow ACLS protocol until physician present. Primary responders to code blue are the Residents, Hospitalist, ICU Charge RN, Respiratory Therapist, and Transporter (chest compressions). Secondary responders to code blue are radiology and phlebotomist from laboratory. Code blue occurring in the Emergency Department are handled by ED staff; MD, RN, and Respiratory Therapist. Critical Care committee will review code blues quarterly. The Clinical Supervisor (CA) – Role Patient Throughput Coordinator Shifts: 7a-7p They cover the hospital 24/7 Location: office is located in the Patient Services Department Contact Information: 745-1710

Primary responsibilities: The CA is primarily responsible for throughput. They do all patient bed placement using EPIC and Awarix tracking board. They quick register direct admit patients in EPIC so physicians can perform order entry. They are the primary nursing responder to all RRT and Code Blue’s. They are all critical care trained and can manage patients anywhere in the hospital if needed. They are responsible for updating GCHC when the hospital is at or over capacity. They are responsible for initiating the chain of command when there is an issue that needs administrative assistance. They call in all OR teams and Cath lab teams for acute issues. Night shift CA’s do an in-house restraint log and are responsible for locating any equipment or supplies that might be needed through the house. EPIC Electronic Medical Records and Physician Order Entry also called Care Path The hospital provides a fully electronic environment for physicians including the Epic electronic medical records, physician-order entry, digital radiology and remote access. All physicians are required to attend EPIC physician training prior to caring for patients. You will receive you log-in at that time. Epic classes are scheduled for Thursdays 5-10 pm. Other times may be available. Schedule with Maria Phillips at 686-3238. Epic may be used for all documentation and is fast and easy with customization, dictation is still permitted. EPIC Access From Home or Office The website for OUTSIDE the hospital is https://chpEconnect.health-partners.org Best to use Windows Explorer or Firefox. Only works with Firefox on the Mac (not Safari). Does NOT work on an iPad. You will need to download Citrix the first time you use this site. Click Accept. This may take some time. Enter you Epic Username and password to enter the Citrix site. Very important – Scroll down to MSWO in the third box. Citrix will load. This takes a minute. Be patient. You will need to download Citrix the first time you do, call 981-5050 for guidance and help. Click on the EPIC Hyperspace PRD South Central icon. At the Epic Hyperspace log-in screen put in your username and password, just like in the hospital. Three Methods for Order Authentication The Ohio Board of Pharmacy requires a secondary authentication for any medication orders. That’s why we must use the RF-ID “tap” to sign orders or the challenge questions or RSA token outside the hospital. Away from the hospital, the RSA token is used as secondary authentication when ordering any medication. This must be activated and a PIN number specified before use. Call 981-5050 to set up an RSA token. Otherwise, challenge questions work in all three cases. EPIC Challenge Questions To meet Board of Pharmacy requirements, set a total of 15 “challenge questions” under the EPIC tab . Remember that no two answers can be the same, answers must be at least three characters, and case sensitive. The Ohio Board of Pharmacy requires a pool of 15 questions. You answer two questions with each order.

Dictation Instructions
Mercy Health - SWOH Region Cincinnati, Ohio
For assistance, contact the Health Information Management Department at (513) 981-6495
Dictation Instructions Data entry may be cleared by pressing * prior to the # key.
1. To dictate within the hospital, dial ext 76370; x63363 at The Jewish Hospital To dictate from outside the hospital, dial 513-981-6370 or 844-280-9950. 2. Enter your Facility Code followed by the # key.
71 - Anderson Hospital 74 - The Jewish Hospital 72 - Clermont Hospital 75 - West Hospital 73 - Fairfield Hospital
3. Enter your User ID followed by the # key. 4. Enter the Work Type Number followed by the # key. 5. Enter the Patient's Account Number followed by the # key. 6. To dictate, press 2. At the tone, please state your name, patient's name (please SPELL), any relevant dates and any providers to be cc'd on the report.

Work Types 1 – History & Physical 3 – Consultation 5 – Discharge Summary 2 – PreOperative H&P 4 – Operative Report 8 – Emergency Room Report 13 – Labor and Delivery Note 6 – Observation Report 9 – Procedure Note 15 – Colonoscopy 24 – Occupational Health Note 27 – Medical Oncology Report 28 – Radiation Oncology Report 14 – Letter 88 – Wound Care Clinic Report
21 – Cardiac Catheterization 62 – Cardiac Stress Test 57 – Echocardiogram / TEE 23 – Event Monitor 64 – Holter Monitor 50 – MUGA 60 – Non Stress Test 31 – Pulmonary Function 19 – Vascular Report 11 – Electroencephalogram 10 – Electromyogram 12 – Sleep Study Clermont Hospital Only 105 – Psychiatric Admission Note 106 – Psychiatric Evaluation
Keypad Options for Dictation 1 – Pause 2 – Record / Dictate (Overwrite) 3 – Short Rewind (5 sec) 4 – Fast Forward (5 sec) *4 – Go to End 5 – End dictation and disconnect
Press *0 or ## anytime during dictation for a confirmation number of your report
6 – Mark STAT 7 – Rewind to beginning and play 8 – Start new report (different work type and different patient) 9 – Play 0 – Suspend Dictation
*5 – Start new report (Same work type and different patient)
Mercy Health - SWOH Region Cincinnati, Ohio

To Listen: 1. To Listen to past dictations within the hospital, dial ext 76370; x63363 at The Jewish Hospital From outside the hospital, dial 513-981-6370 or 844-280-9950. 2. Enter your Facility Code followed by the # key.
71 - Anderson Hospital 74 - The Jewish Hospital 72 - Clermont Hospital 75 - West Hospital 73 - Fairfield Hospital
3. Enter your User ID followed by the # key. 4. Dial *9 to enter Listening mode 5. Dial 1 to listen by Job Number or 2 to listen by the Patient's Account Number followed by the # key. Then enter the requested information.
Keypad Options for Listening
1 – Pause / Play 2 – n/a 3 – Short Rewind (5 sec) 4 – Pause 5 – Get Next
6 – Go to End 7 – Fast Forward (5 sec) 8 – Rewind to beginning and play 9 – Return to the main menu 0 – Play Job Number
Rev 8-22-2016
Any problems with dictation or transcription, call regional transcription at 981-6495 or after hours call the IT Service Desk at 800-498-1408. Pick up a dictation card from transcription services located in the physician lounge or from the Medical Staff Office.

Translators Available, call the Operator In accordance with CLAS Standards and Title VI, patients who are identified as Limited English Proficient (LEP) will be provided access to qualified interpreters to aid in facilitating communication related to patient needs at all times. LEP patients are those do not speak English as their primary language and who have a limited ability to read, write, speak or understand English. To obtain a dual headset phone call the operator at “O”. This stays with the patient until discharge. Bilingual employees cannot be used as staff interpreters unless they have undergone the process to become a qualified interpreter. Services of a qualified foreign language interpreter must be offered, at no additional cost, to all patients and/or relatives identified as Limited English Proficient. To preserve patient confidentiality, family and friends should not be asked to interpret for a patient unless there is an emergency situation (until an interpreter can be arranged and arrives), or the patient expressly requests to use that person. Document this in the medical record. Over the phone Interpreters, dial “O” for the operator Pacific Interpreters is the preferred vendor. Language Line and Vocalink are used as a back up service for rare languages. Sign Language Interpreters The Jewish Hospital contracts with Affordable Language Services – who specialize in medical translation. They are used by Cincinnati Children's Medical Center. They are certified and trained on medical terminology with and required continuing education. When Patients Complain -- We Want to Know If you have any inpatients who complain or have issues with their hospital stay, please give them the Nursing Managers contact information post discharge please give them the number of our Patient Representative – Glenda Bernstein – at 686-5320. The call will be returned within 24 hours. We want to know when patients have a bad experience, we want to improve. Department of Pharmacy Pharmacy Director – Ezra Bradshaw Office: 686-4950 Employee Health On site 7am – 3pm Tuesday, Thursday and Friday. Located on second floor of the Hospital, near Administration.

Bloodborne Pathogen Exposure If you are exposed, page 343-5076. The hotline nurse will order labs on both the source patient and the physician involved free of charge. Labs include Rapid HIV, Hep C and Hep B antigen on source and HIV, Hep C and Hep B antibody on physician involved. This hotline is also used for any other communicable disease exposure that can be treated with prophylaxis, for example meningitis. Respirator Fit Testing -- Annual fit testing takes place in Employee Health every June, July and August and is available to any physician. Spiritual Care Services The Jewish Hospital provides chaplaincy services 24/7 and may be contacted by calling the operator. The Chaplains are board certified through professional chaplaincy associations and represent multi-faith backgrounds and approaches. Chaplains are available to all of our patients who need spiritual and/or emotional support; chaplains are members of the inter-disciplinary team; chaplains assess for spiritual needs without disrespecting anyone’s beliefs, values or faith background; chaplains support a holistic approach to patient care recognizing that attention to spiritual and emotional needs are important elements in healing; chaplains provide assistance with advance directives and end-of-life discussions with the patient and family members. Advance Directive Information and the Chaplaincy Role Health Care power of Attorney (HCPOA) and Living Will (LW) information is offered to all patients admitted to our facility. The HCPOA lets the patient name who they would want to make their health care decisions if they are unable to do so. The LW directs the physician on a patient’s wishes for end-of-life care. The HCPOA goes into effect if the patient is temporarily or permanently unable to speak for him/herself. The LW is activated only after two physicians determine and document the patient has a terminal condition (defined in the document) or is permanently unconscious with little hope of regaining consciousness. The LW is not a DNR order. A DNR order must be written by a physician. While chaplains are available to discuss issues related to a patients’ journey with illness, meaning and hope, they do not discuss DNR orders. Code status discussions are outside of the scope of practice of chaplains as they require the patient to understand how their medical condition affects their goals. Mercy belongs to the US Living Will Registry and offers registration free to any patient and their families. This is a national database that stores the ADs electronically so that caregivers have access to them wherever the patient is. Ethical concerns are handled with a multidisciplinary approach. Patients (or their decision makers) are given all the information and support they need to make decisions. The patient’s physician should be advised of patient concerns. The Ethics Committee is a consultative resource for patients, families, physicians and staff. This committee can be reached by calling the operator. Chaplains are available to support patients and their medical team in difficult discussions. Spiritual Care is represented on the hospital ethics committee.

Credentialed Medical Staff Required to Follow Ethical and Religious Directives (ERD) Catholic health care is premised on the human dignity of all persons and the sacredness of human life. Our ByLaws require that all medical staff abide by the Ethical and Religious Directives (ERDs) for Catholic Health Care Services. Compliance with these ERDs is a condition for medical staff privileges. When you accept hospital privileges, you are agreeing to practice in a manner consistent with the ERD when rounding and performing procedures at any Mercy facility. “Consistent” neither implies not suggests that the physician personally espouses the Directives or adheres to the Catholic faith. “Consistent” does imply that the physician will participate in the healing mission of the hospital and will not provide a limited set of prohibited services – direct abortion, direct sterilization, active euthanasia or some means of contraception. A full copy of the ERDs is available at http://www.usccb.org/bishops/directives.shtml. Fire Safety Plan Remember R A C E when responding to a fire. R = Rescue patients and visitors A = Sound the Alarm by dialing 66# and pull the fire alarm C = Confine or contain the fire E = Extinguish the fire Remember PASS when using Fire Extinguishers. P = Pull the pin A = Aim low S = Squeeze the lever below the handle S = Sweep from side to side Hazardous Materials Management Various hazardous materials are used throughout the hospital. These could pose a threat if a spill or release should occur. MSDS (Material Safety Data Sheets) are found on the intranet. The MSDS gives detailed information on a specific chemical product, including the chemical ingredients, potential hazards, and safety precautions. Call Safety/Security at 66# to report a spill. Do NOT attempt to clean up a spill unless you or the personnel involved are properly trained to do so.

Emergency (Disaster) Management This Emergency Preparedness Plan is designed to manage the hospital’s resources, such as, space, supplies, communications, and personnel, during such emergencies. Emergency Operations Center (Command Post) is located in the Internal Medicine Conference Room, 3rd Floor. Physicians/Medical Residents should report to the Emergency Operations Center (Command Post), for assignment. The Medical House Physician will take charge of the assignment of physicians until relieved by the Medical Staff Operations Chief on-call. Emergency Codes CODE RED = Fire CODE ADAM = Infant Abduction CODE BLACK = Bomb/Bomb Threat CODE GRAY = Severe Weather CODE ORANGE = Hazardous Material Spill/Release CODE BLUE = Medical Emergency CODE YELLOW = Disaster CODE VIOLET = Violent/Combative Person CODE SILVER = Person with Weapon/Hostage Situation CODE BROWN = Missing Patient CODE GREEN = All Clear is the ALL CLEAR signal representing the conclusion to the emergency. EPIC Downtime If Epic Production is unavailable, users will be able to access downtime reports via Epic’s BCA-Web website. All orders are available on the Business Continuity Access (BCA) PC in each department. BCA PCs are designated workstations with independent power sources that allow end users to print patient specific downtime reports from CarePATH. Once logged in, users will find a directory of folders that are receiving reports on each unit or area. Inside each folder or directory, the user can access each unit and department has paper forms to use interimly.
Disruptive & Inappropriate Behavior Indicators of potential for corrective action may include, but shall not be limited to, circumstances in which a Practitioner exhibits acts, demeanor, or conduct reasonably likely to be one or more of the following:
• detrimental to patient safety or to the delivery of quality patient care within the Hospital • contrary to the ethics of the medical profession • contrary to the Medical Staff Bylaws, Rules and Regulations, or the policies and procedures of the Hospital • below applicable professional standards • disruptive to Hospital operations or detrimental to the best interests of the Hospital

• interpreted by any individual working in the Hospital to create reasonable suspicion that a Practitioner is an impaired physician
Corrective action will only be imposed on a Practitioner when the in the Hospital’s reasonable belief that the action was in the furtherance of quality health care; after a reasonable effort to obtain the facts of the matter; after adequate notice and hearing procedures are afforded to the Practitioner involved or after such other procedures as are fair to the Practitioner under the circumstances; and in the reasonable belief that the action was warranted and, if applicable, after meeting the requirements of above.
Impairment* All people are vulnerable to illness -- illness that can result in impairment in one's personal, social or work life. Physicians, nurse practitioners, and allied health personnel are no exception -- and may even be at higher risk to certain types of illness and impairment than the general public. Studies have shown that, of all impaired health care personnel, at least one-half have problems with drug and/or alcohol abuse. As a physician, nurse practitioners, or allied health personnel, you may have been or may have known colleagues affected by the difficulties of impairment that interfered with family, social life and work performance. In such a situation, you may have felt very concerned but quite helpless. Much is at stake -- your or your colleague’s health, family, career, reputation within the community, and professional relationships or friendships. Perhaps you have weighed each of these considerations and decided that, in spite of your concerns, doing nothing seemed the only course. As background, estimates are that physicians, nurse practitioners, and allied health personnel have a 5-8% impairment rate for alcoholism, 1-2% for other substance abuse and 1% for psychiatric illness. In general, impairment occurs because of three major problems.
1. Substance abuse -- Alcohol abuse is the most common problem. Abuse of narcotics, sedatives and other depressants as well as stimulants, including cocaine, may also occur. According to current estimates, 5-8 percent of physicians abuse alcohol and 2 percent abuse narcotics.
2. Psychological problems -- Excessive stress, depression, anxiety and divorce are the most common issues. 3. Physical illness -- Physical ailments, either temporary or long-term, can lead to incapacity.
Of these three groups of illnesses, substance abuse is the problem for which physicians, nurse practitioners, and allied health personnel are least likely to seek help. If you or a colleague is in trouble, there are actions that you can and must take. These guidelines are intended to explain and encourage those actions, and to offer resources that can be of help regarding impairment caused by chemical dependency. Referrals can be made to the Practitioner’s Aid Committee.

The Practitioners’ Aid Committee is composed of Medical Staff members and other appropriate professionals, including a psychiatrist and a Medical Staff member who has expertise in chemical dependency matters. The Committee is responsible for serving as the identified point within the Hospital for self-referral by a Practitioner and confidential referral by other organization staff with respect to potential impairments. The Committee also refers affected Practitioners to the appropriate internal or external resources for diagnosis and treatment of the condition or concern and monitors compliance with such referrals. The Committee process does maintain the confidentiality of the Practitioner seeking referral or referred for assistance, except as limited by law, ethical obligation, or when the safety of a patient is threatened. *Brown Psychiatry Residency - Jane Eisen, M.D. and Robert Boland, MD
Safety Across the Chasm: Six Aims for Changing the Health Care System http://www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/ImprovementStories/Across+the+Chasm+Six+Aims+for+Changing+the+Health+Care+System.htm In 1999, the Institute of Medicine (IOM) in Washington, DC, USA, released To Err Is Human: Building a Safer Health System, an alarming report that brought tremendous public attention to the crisis of patient safety in the United States. In 2001, IOM followed up with Crossing the Quality Chasm: A New Health System for the 21st Century, a more detailed examination of the immense divide between what we know to be good health care and the health care that people actually receive. The report calls the divide not just a gap but a chasm, and the difference between those two metaphors is quantitative as well as qualitative. Not only is the current health care system lagging behind the ideal in large and numerous ways, but the system is fundamentally and incurably unable to reach the ideal. In order to begin achieving real improvement in health care, the whole system has to change. Let’s look at the other side of the chasm — at the ideal health care outlined by the report’s six "Aims for Improvement." To begin with, health care must be safe. This means much more than the ancient maxim "First, do no harm," which makes it the individual caregiver’s responsibility to somehow try extra hard to be more careful (a requirement modern human factors theory has shown to be unproductive). Instead, the aim means that safety must be a property of the system. No one should ever be harmed by health care again. Second, health care must be effective. It should match science, with neither underuse nor overuse of the best available techniques — every elderly heart patient who would benefit from beta-blockers should get them, and no child with a simple ear infection should get advanced antibiotics. Third, health care should be patient-centered. The individual patient’s culture, social context, and specific needs deserve respect, and the patient should play an active role in making decisions about her own care. That concept is especially vital today, as more people require chronic rather than acute care. Fourth, care should be timely. Unintended waiting that doesn’t provide information or time to heal is a system defect. Prompt attention benefits both the patient and the caregiver.

Fifth, the health care system should be efficient, constantly seeking to reduce the waste — and hence the cost — of supplies, equipment, space, capital, ideas, time, and opportunities. And sixth, health care should be equitable. Race, ethnicity, gender, and income should not prevent anyone in the world from receiving high-quality care. We need advances in health care delivery to match the advances in medical science so the benefits of that science may reach everyone equally. But we cannot hope to cross the chasm and achieve these aims until we make fundamental changes to the whole health care system. All levels require dramatic improvement, from the patient’s experience — probably the most important level of all — up to the vast environment of policy, payment, regulation, accreditation, litigation, and professional training that ultimately shapes the behavior, interests, and opportunities of health care. In between are the microsystems that bring the care to the patients, the small caregiving teams and their procedures and work environments, as well as all the hospitals, clinics, and other organizations that house those microsystems. "We’re trying to suggest actions for actors, whether you’re a congressman or the president or whether you’re a governor or a commissioner of public health, or whether you’re a hospital CEO or director of nursing in a clinic or chairman of medicine," says Donald M. Berwick, MD, MPP, Past President/CEO of the Institute for Healthcare Improvement, current Administrator for the Centers for Medicare and Medicaid Services and one of the Chasm report’s architects. "No matter where you are, you can look at this list of aims and say that at the level of the system you house, the level you’re responsible for, you can organize improvements around those directions." Infection Control There is substantial evidence that hand hygiene reduces the incidence of infections. Healthcare providers should practice hand hygiene at key points in time to disrupt the transmission of microorganisms to patients including: before patient contact; after contact with blood, body fluids, or contaminated surfaces (even if gloves are worn); before invasive procedures; and after removing gloves (wearing gloves is not enough to prevent the transmission of pathogens in healthcare settings). You can use alcohol-based hand gels when no visible soiling is present. Dispensers are located inside or outside every patient room. Two fundamental concepts for infection control in the hospital are Standard and Transmission-based precautions. Standard precautions include appropriate hand hygiene; respiratory etiquette; use of gloves gown mask, eye protection, or face shield, depending on the anticipated exposure; and safe injection practices.
Transmission-based precautions (commonly referred to as “isolation precautions” are practices in addition to Standard Precautions used for patients with known or suspected infectious diseases. Read the signs posted on patients’ room doors for requirements. Transmission-based precautions (isolation precautions) – Adherence required per hospital policy. Please contact Infection Prevention for discontinuation of isolation per policy.
• Contact [green sign] o Gown & Gloves required to enter room. o Hand Hygiene – use alcohol hand rub or soap and water

o This is the most common type – used for MDROs • Contact Plus [brown sign]
o Gown & gloves required to enter room. o Typically used only for suspected or confirmed C. difficile disease o Hand Hygiene with soap, water and friction for 15 seconds use a paper towel to turn off faucet. Use of alcohol hand
rub is discouraged when caring for patients with C. difficile o Disinfect with bleach- wipes are available on isolation cart for stethoscopes
• Droplet [blue sign] o Standard/surgical Mask o Common Indications: Meningococcal disease, Influenza, Pneumonia or rule outs o Hand Hygiene soap and water or alcohol
• Airborne [pink sign] o Fit-tested N95 mask or PAPR (may obtain by signing out from central service) o Negative air pressure room required o Common Indication: TB (including r/o TB), Disseminated Zoster
Influenza Transmission of Influenza:
• Influenza is transmitted by direct or indirect contact with respiratory droplets. The incubation period for influenza is 1-7 days
• Patients who are admitted with symptoms of influenza need to be placed in droplet precautions for the duration of illness. • The Infection Preventionist follows an algorithm for removal of isolation. Contact IC.
Influenza Vaccination Recommendations: – The Centers for Disease Control and Prevention recommend ALL persons over the age of 6 months get annual
influenza vaccine Impact of Influenza:
• The CDC reports as associated death rate worldwide of 250,000 to 500,000 each year due to influenza • Influenza hospitalizations ~ 110,000/year in the US • Experts estimate if 1 million persons were vaccinated, as many as 900 deaths and 1300 hospitalizations would be
prevented The national patient safety goals (NPSG) requires hospitals to educate staff and all licensed independent practitioners (MD, NP and PA) about healthcare associated infections, multi-drug resistant organisms (MDRO) and prevention strategies for Catheter related blood-stream (CL-BSI) and surgical site infections (SSI). Hand hygiene is required for all health care workers and

physicians as part of the overall strategy to reduce healthcare associated infections (HAI). Additionally, there is a requirement for patients and families to be instructed about health care associated infection strategies and hand hygiene. Prevention of central-line assoc. bloodstream infection (CLABSI) Adherence to hand hygiene practices before insertion of all invasive lines Wearing maximum sterile barriers during all insertions (mask, cap, surgeon gown, and sterile gloves) Using chlorhexidine (CHG) for skin asepsis of the insertion site Applying full body drape over patient Avoid femoral site for routine insertions Daily evaluation of continued need for central line
Prevention of surgical site infection (SSI) Maintaining OR room environments
o Positive air flow, increased number of room air exchanges Sterilization of surgical instruments Donning of surgical scrub attire by the OR team with pre-op surgical hand scrubbing Clipping of the hair around the surgical site (not shaving) Pre-operative skin antisepsis Pre-operative antibiotics as deemed appropriate
o Given on time before the incision is made o Proper selection of antibiotic and discontinuance within a timely manner
Pre-operative showering by patients Pre-operative Staph aureus nasal screening protocols
Prevention of catheter-assoc. UTI (CAUTI) Indications for urinary catheterization (CDC/HICPAC Guidelines, 2009)
o Urinary Retention or Obstruction o Surgical Procedure or procedure > 2 hours o Strict I&O in critically ill patients o Stage III or IV skin ulcers in incontinent patient o Comfort for terminal illness only o Foleys should not be in place for nursing convenience or patient request
• Placement
o First consider: Is foley really necessary? o Hand Hygiene and Aseptic technique o Maintain closed system o Secure catheter to leg – we use STATLOK o Daily assessment of need to continue catheter
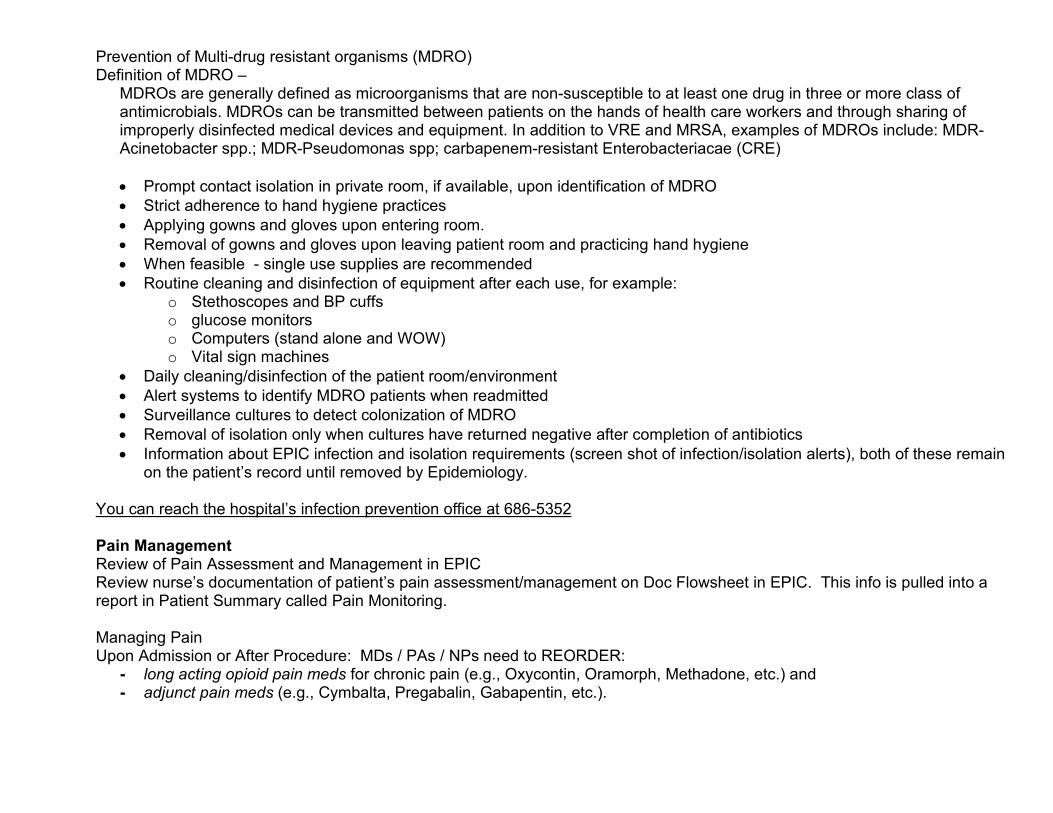
Prevention of Multi-drug resistant organisms (MDRO) Definition of MDRO –
MDROs are generally defined as microorganisms that are non-susceptible to at least one drug in three or more class of antimicrobials. MDROs can be transmitted between patients on the hands of health care workers and through sharing of improperly disinfected medical devices and equipment. In addition to VRE and MRSA, examples of MDROs include: MDR-Acinetobacter spp.; MDR-Pseudomonas spp; carbapenem-resistant Enterobacteriacae (CRE) • Prompt contact isolation in private room, if available, upon identification of MDRO • Strict adherence to hand hygiene practices • Applying gowns and gloves upon entering room. • Removal of gowns and gloves upon leaving patient room and practicing hand hygiene • When feasible - single use supplies are recommended • Routine cleaning and disinfection of equipment after each use, for example:
o Stethoscopes and BP cuffs o glucose monitors o Computers (stand alone and WOW) o Vital sign machines
• Daily cleaning/disinfection of the patient room/environment • Alert systems to identify MDRO patients when readmitted • Surveillance cultures to detect colonization of MDRO • Removal of isolation only when cultures have returned negative after completion of antibiotics • Information about EPIC infection and isolation requirements (screen shot of infection/isolation alerts), both of these remain
on the patient’s record until removed by Epidemiology.
You can reach the hospital’s infection prevention office at 686-5352 Pain Management Review of Pain Assessment and Management in EPIC Review nurse’s documentation of patient’s pain assessment/management on Doc Flowsheet in EPIC. This info is pulled into a report in Patient Summary called Pain Monitoring. Managing Pain Upon Admission or After Procedure: MDs / PAs / NPs need to REORDER:
- long acting opioid pain meds for chronic pain (e.g., Oxycontin, Oramorph, Methadone, etc.) and - adjunct pain meds (e.g., Cymbalta, Pregabalin, Gabapentin, etc.).

Patient Controlled Analgesia (PCA) & Chronic Pain Med Administration: - Patients appropriate for patient controlled analgesia (PCA) must be mentally alert and have the cognitive, emotional and
physicial abilities to understand the operation of the PCA and be able to safely manage his/her own pain. - Upon ordering PCA, following parameters must be specified:
o Loading bolus – initial analgesia dose o PCA dose (“bolus” dose) – the patient controlled dose delivered on patient demand o Continuous (“basal” rate) – low-dose, continuous infusion rate; only for opioid tolerant patients o One-hour limit – the maximum amount of analgesia the patient can receive in one hour o Lockout interval – the time period during which patient cannot activate the pump – i.e.., a 10-min lockout interval
would prevent the patient from receiving a bolus more frequently than every 10 minutes. - Other systemic narcotics should be limited while on PCA. - In order for the patient to receive their chronic pain narcotic with the PCA, the MD, who has ordered the PCA, needs to
approve (in verbal or written format) the chronic pain med to be given. When the Attending MD or the Resident MD is placing the order for the chronic pain narcotic, he/she needs to add in the Administration Instructions: “OK to give chronic pain opioid med with PCA per Dr. _____________ .”
ANALGESIC
EQUIANALGESIC DOSES DURATI
ON* (hours)
COMMENTS Parenteral (mg) (IV, IM,
SQ)
Oral (mg)
Morphine 10 30 3-4 hrs
Standard for comparison. Multiple routes of administration. Active metabolite M6G can accumulate with repeated dosing in renal failure.
Morphine Controlled Release Tablets
-- 30 8-12 hrs
Active metabolite M6G can accumulate with repeated dosing in renal failure. Do not crush or cut controlled release morphine.
Hydromorphone 1.5 7.5 2-3 hrs No evidence that metabolites are clinically
relevant. Shorter duration than morphine.
Fentanyl 100 mcg N/A 1-3 hr Short half-life, but at a steady state, slow elimination from tissues can lead to a prolonged half-life (up to 12 hrs).

Transdermal Fentanyl -- -- 72 hrs
Indicated for opioid-tolerant patients when around-the-clock analgesia is needed. Transdermal fentanyl is not recommended for acute pain. 180 mg oral morphine/24 hours = 50 mcg/hr transdermal fentanyl
Meperidine 75 300 NR* 3-4 hrs
Not recommended for the management of acute or chronic pain due to toxicity from accumulation of metabolite (normeperidine), which has 15-20 hr half-life and is not reversed by naloxone.
Methadone 10 20 4-6 hrs
Practitioners are advised to consult with a pharmacist or a pain/palliative care specialist if they are unfamiliar with methadone prescribing.
Oxycodone -- 20 3-5 hrs
Used for moderate pain. Available as single entity in immediate-release (with or without acetaminophen) and controlled-release formulations.
Oxycodone Controlled Release
-- 20 12 hrs Do not crush or cut controlled-release oxycodone.. Not indicated for PRN use due to long half-life and slow release.
Codeine 130 200 NR* 3-4 hrs
Used for mild to moderate pain. Known to be highly constipating. IM has unpredictable absorption and high side effect profile.
Hydrocodone -- 30 NR* 3-5 hrs
Used for mild to moderate pain. Available only in compounded formulation (ASA, APAP).
Oxymorphone 1 10 3-6 hrs
Used for moderate to severe pain. Non-formulary agent – patient must supply own medication or convert to alternative agent.
Tramadol -- 50-100 4-7 hrs Weak opioid receptor agonist with some anti-depressant activity. Used for mild to moderate pain. Recommended starting

dose is 50 mg PO q6h PRN. Max dose = 400mg/day or 300mg/day for elderly).
Nalbuphine 10 -- 3-6 hrs Agonist-Antagonist. May produce withdrawal in opioid dependent patients.
* Equianalgesic doses are drug and route conversions approximately equal to a single morphine 10mg IV or 30mg PO dose. This table is a guideline only. The equianalgesic dose is not the usual starting dose. Dosing must be individualized and titrated according to the patient’s age, condition, response, and clinical situation. * To account for incomplete cross-tolerance when converting to a new opioid, start with 50-75% of the equianalgesic dose and the new opioid and titrate to effectiveness. * Duration: the shorter time generally refers to parenteral administration of opioids; the longer time generally refers to oral administration of immediate-release opioids. * NR = not recommended at that dose
Anticoagulation Therapies Anticoagulation therapy can be used as therapeutic treatment for a number of conditions, the most common of which are atrial fibrillation, deep vein thrombosis, pulmonary embolism, and mechanical heart valve implant. However, it is important to note that anticoagulation medications are more likely than others to cause harm due to complex dosing, insufficient monitoring, and inconsistent patient compliance. In order to ensure the safe use of anticoagulation therapy at The Jewish Hospital, protocols, guidelines, and procedures for dosing and monitoring anticoagulation therapies have been developed. Heparin Pre-defined ordersets exist within the computerized order entry EPIC system for continuous infusion UFH. These ordersets include automatic orders for necessary lab work for review prior to initiation of UFH therapy. Therapeutic doses of UFH continuous infusions can only be initiated through the use of these ordersets. Use of UFH approved ordersets will ensure the following for patients:
• Baseline and ongoing laboratory tests are ordered and assessed as listed: o Baseline labs consisting of a Complete Blood Count (Hgb, Hct, Platelets, WBC), Protime/INR and aPTT are
ordered by default via the heparin orderset. o Subsequent anti-Xa levels are drawn according to protocol. o Subsequent CBC labs ordered in conjuction with the UFH orderset default to a frequency of q72h – but these can
be manually changed upon ordering. LMWH

Prior to initiation of LMWH, baseline labs (BMP, CBC, Protime/INR) should be obtained. As LMWH are renally eliminated, renal function should be monitored. LMWH is included in pharmacy renal dose adjustment policy – that is, a pharmacist can automatically adjust doses of enoxaparin (formulary LMWH) based on renal function. Appropriate documentation in patient chart (via a progress note) will be provided to inform providers that a dose adjustment has been made.
Therapeutic Anticoagulation Guidelines – Unfractionated Heparin & Low-Molecular Weight Heparin
INDICATION ENOXAPARIN (LOVENOX®)
Round doses to nearest 10 mg
UNFRACTIONATED HEPARIN
Round bolus doses to nearest 500 mg
Round infusion rates to nearest 10 units/hr
General Dosing (PE, DVT, Atrial Fibrillation) Patients weighing ≤ 100 kg
1 mg/kg subcut q12h OR
1.5 mg/kg subcut q24h
Bolus = 80 units/kg IV (maximum = 10,000 units)
Infusion = 18 units/kg/hr
(no maximum)
Obesity Patients weighing > 100kg 1 mg/kg subcut q12h
Renal Dysfunction (estimated CrCl < 30 mL/min) 1 mg/kg subcut q24h
Acute Coronary Syndrome 1 mg/kg subcut q12h
Acute Coronary Syndrome with concomitant
thrombolytic & GPIIbIIIa Inhibitors
Not indicated
Bolus = 60 units/kg IV (maximum = 4,000 units)
Infusion = 12 units/kg/hr
(maximum intial rate = 1,000 units/hr)
Note: when using enoxaparin in patients > 144 kg or patients with renal impairment, consider monitoring anti-Xa levels if concerned about efficacy/safety. Monitor peak anti-Xa level 4 hours after subcutaneous dose. Therapeutic range for enoxaparin: Q12H dosing: anti-Xa = 0.6-1 units/mL; Q24H dosing: anti-Xa = 1.0-1.8 units/mL
AGENT ADVANTAGES DISADVANTAGES

ENOXAPARIN
Subcutaneous injection vs. continuous infusion; routine lab monitoring not required; immediate therapeutic anticoagulation within 2 hours; can be used for outpatient therapy; safe & effective in patients up to 144 kg
Dose adjustment needed for impaired renal function; not typically recommended for ESRD; no proven reversal agent; longer duration of action (more difficult prior to procedures); expensive
UNFRACTIONATED HEPARIN
No dose adjusted needed in renal dysfunction; can be stopped within hours of a procedure; efficacy routinely monitored due to necessary anti-Xa monitoring; can be reversed by protamine; physician comfort due to many years of use
Requires hospitalization for IV infusion; lab draws required for monitoring; can take many hours to achieve therapeutic anticoagulation; unclear maximum dosing recommendations in obese patients
Prophylactic Anticoagulation Guidelines –Low-Molecular Weight Heparin
INDICATION ENOXAPARIN (LOVENOX®)*
Round doses to nearest 10 mg
RENAL DOSE RECOMMENDATION
FOR CrCl < 30 mL/min
General Dosing 40 mg q24h
30 mg q24h
Abdominal Surgery 40 mg q24h
Post-op hip replacement
30 mg q12h OR
40 mg q24h Post-op knee replacement 30 mg q12h
*All doses given as subcutaneous injection

Warfarin Prior to initiation of warfarin, a baseline INR (within 48 hours) should be obtained. Pharmacy policy requires baseline INR prior to dispensing by a pharmacist. INR required within 24 hours of any dose change. Subsequent monitoring of labs (CBC, Protime/INR) is recommended. Multiple drug/food interactions – consider pharmacy consult for warfarin dosing/monitoring. Oral Anticoagulants
• Baseline labs should be obtained – CBC, BMP prior to initiation. Routine monitoring of CBC, renal function recommended. Frequently monitor for signs/symptoms of bleeding.
• Most newer agents lack specific recommendations for reversal; can be an issue for procedures or cases of bleeding. Dabigatran –
- Mechanism: thrombin inhibitor - Advantages: oral medication, unlike warfarin, does not require routine INR monitoring - Disadvantages: like all anticoagulants, carries risk of bleeding; no recommended reversal agent; not recommended for
patients with bioprosthetic heart valves; case reports of bleeding in elderly patients; should be held for several days prior to invasive procedures; expensive
INDICATION DOSING RENAL DOSE ADJUSTMENT
Prevention of stroke/systemic
embolism in nonvalvular
atrial fibrillation
150 mg PO BID
Mild renal impairment (CrCl 50-80 mL/min): use with caution CrCl 30-50 mL/min: no adjustment needed unless on concomitant dronaderone or PO ketoconazole; use with caution CrCl 15-30 mL/min: 75 mg PO BID; if on dronaderone or PO ketoconazole, avoid use CrCl < 15 mL/min: use not recommended ESRD on HD: use not recommended
Rivaroxaban –
- Mechanism: factor Xa inhibitor - Advantages: oral medication, unlike warfarin, does not require routine INR monitoring
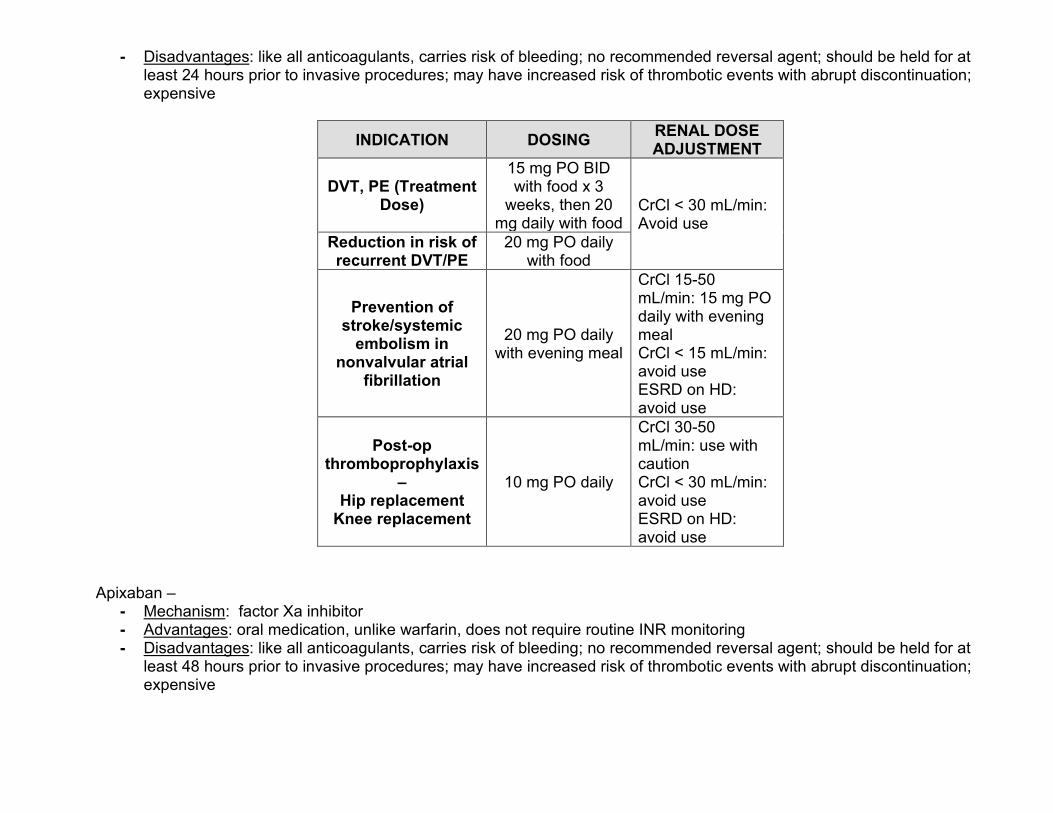
- Disadvantages: like all anticoagulants, carries risk of bleeding; no recommended reversal agent; should be held for at least 24 hours prior to invasive procedures; may have increased risk of thrombotic events with abrupt discontinuation; expensive
INDICATION DOSING RENAL DOSE ADJUSTMENT
DVT, PE (Treatment Dose)
15 mg PO BID with food x 3
weeks, then 20 mg daily with food
CrCl < 30 mL/min: Avoid use
Reduction in risk of recurrent DVT/PE
20 mg PO daily with food
Prevention of stroke/systemic
embolism in nonvalvular atrial
fibrillation
20 mg PO daily with evening meal
CrCl 15-50 mL/min: 15 mg PO daily with evening meal CrCl < 15 mL/min: avoid use ESRD on HD: avoid use
Post-op thromboprophylaxis
– Hip replacement
Knee replacement
10 mg PO daily
CrCl 30-50 mL/min: use with caution CrCl < 30 mL/min: avoid use ESRD on HD: avoid use
Apixaban –
- Mechanism: factor Xa inhibitor - Advantages: oral medication, unlike warfarin, does not require routine INR monitoring - Disadvantages: like all anticoagulants, carries risk of bleeding; no recommended reversal agent; should be held for at
least 48 hours prior to invasive procedures; may have increased risk of thrombotic events with abrupt discontinuation; expensive

INDICATION DOSING DOSE ADJUSTMENTS
Prevention of stroke/systemic
embolism in nonvalvular atrial
fibrillation
5 mg PO BID
If patient has 2+ of following, reduce dose to 2.5 mg PO BID: -age ≥ 80y, body weight ≤60kg, SCr ≥1.5mg/dL If on concomitant dual strong CYP3A4 and P-glycoprotein inhibitors (i.e., clarithryomycin, ketoconazole, itraconazole, ritonavir), reduce dose to 2.5 mg PO BID CrCl < 15 mL/min – not studied
Universal protocol policy As part of the Joint Commission National Patient Safety Goals, The Jewish Hospital adheres to the Universal Protocol for Preventing Wrong Site, Wrong Procedure and Wrong Person Surgery, while adding key elements from the World Health Organization (WHO). Policy Requirements:
• Physicians must complete site marking prior to procedure start and may perform site marking in the pre-procedure area (Same Day Surgery), at the bedside such as in radiology, or prior to the patient being transferred to the procedure table.
• Patients may be given analgesics (e.g. morphine) and anxiolytics (e.g. versed) prior to site marking (this should not preclude the patient from being involved).
• In limited circumstances, the licensed independent practitioner may delegate site marking to residents, licensed advance practice registered nurses (APRNs) and physician assistants (PAs). Surgeons should always be the primary person to perform site marking. There should be no standing orders for another person to perform site marking.
• Site Marking – The site should be marked with the licensed independent practitioner’s initials.
What procedures require site marking? • Mark the location of the intended procedure; examples include different limbs, fingers and toes, lesions, level of the
spine and organs. • For procedures that involve laterality of organs; (examples include right kidney biopsy, possible left ovary excision) but
the incision or approaches may be from the midline or from a natural orifice, the site is still marked. • For spinal procedures, there is a two step process: the general level of the procedure (cervical, thoracic or lumbar)
must be marked preoperatively. If the approach involves anterior versus posterior, or right versus left, then the mark must indicate this. Then, intraoperatively, the exact interspace(s) to be operated on should be precisely marked using the standard intraoperative radiographic marking technique.
Exclusions:

• Procedures in which there is an obvious wound, lesions or ulceration (e.g. fungating breast mass). • Procedures that do NOT involve laterality of organs, regardless of the approach (examples: C-section, CABG/PTCA,
stomach, gall bladder and spleen), as well as endoscopies without intended laterality. • Procedure sites that cannot be marked due to physical location (e.g., rectal or vaginal procedures). • Bilateral procedures • Emergency procedures may require variations to the policy to prevent further injury to the patient
In cases in which the intended site and actual procedure site may change during the course of the procedure, the intended site still needs to be marked prior to the procedure start. If, at any time, there is confusion or question among staff or physicians about whether a site should be marked or is appropriate for marking, then site marking must still occur. When in doubt, mark the site. Rapid Response Patient lives are saved when changes in their conditions are detected early, and addressed promptly with appropriate interventions. The challenge to all involved is to recognize signs of early change, communicate this change to the appropriate person(s), and act to prevent or correct unstable situations before critical changes require cardiopulmonary resuscitation. It is the intent of this policy to address the criteria, teamwork, and resources for activating the rapid response team. Criteria are established to consider team activation. They are: 1. Acute mental status change 2. Acute significant bleeding 3. Fall with injury 4. Heart rate more than 130/minute 5. Heart rate less than 40/minute 6. Systolic blood pressure less than 90 mm Hg 7. New seizures 8. New onset chest pain 9. Respiratory rate more than 30/minute 10. Respiratory rate less than 8/minute 11. SpO2 less than 90% despite increasing O2 delivery, or continuing increase in O2 support to maintain SpO2 12. Staff/family worried/concerned Call 66# to activate the rapid response team. Initial responders are a critical care nurse and respiratory therapist.
Restraint & Seclusion Organizationally, we strive toward a restraint-free environment by continuously improving our practice to provide for patients’ safety while respecting their dignity. Limited and justified use of restraints is supported with appropriate assessment planning,

education, family involvement and the use of safe and effective alternatives. Restraints are never used for discipline, convenience, retaliation or coercion. It is the expectation that less restrictive interventions have been determined to be ineffective to protect the patient, a staff member, or others from harm prior to employing the use of restraints. Examples of less restrictive interventions might be:
• More frequent visual checks or moving patient closer to a nurse station (closer observation) as possible; • Use of TV, radio, or other activity as diversion/distraction; • Diminish external stimulation by lowering lights, sound levels, etc.; • Offer of bedpan/assistance to the bathroom, food/fluids as appropriate; • Use of alert devices, etc. • Use of fall prevention plan • Encourage family member to stay close by and assist with reorientation/redirection.
Continuation of restraints requires an evaluation from the treating physician prior to renewal of the order.
Organ & Tissue Donation Contact LifeCenter at 513-558-5000 within one hour of the patient meeting one of the clinical triggers that indicate a potential organ or tissue donor:
1. the patient with a brain injury, on a ventilator and with a GCS of 5 or less; and/or unresponsive and missing two brain stem reflexes;
2. When families are considering the option of withdrawing ventilator or pressor support; 3. On all cardiac deaths.
LifeCenter shall coordinate all requests for organ and tissue donation with hospital staff. Conversations with the family about organ and tissue donation must be initiated by LifeCenter, who are specifically trained in the use of discretion and sensitivity to the circumstances, beliefs, and desires of the families of the potential organ, tissue, and/or eye donors. Incomplete Medical Records Practitioners are responsible for completing the medical record within thirty (30) days of discharge. Failure to complete medical records in a timely and accurate fashion may result in a reduction, suspension, restriction, denial, nonrenewal or termination of clinical privileges. A practitioner having medical record delinquencies that extend past 30 days from the date of patient discharge will receive a notification from Medical Records via their EPIC in basket on the first Tuesday after the initial 30 days have passed and will continue to receive an EPIC in basket notice each subsequent Tuesday until the record is completed. Their names will also be referred to the MEC if the records are not complete by the meeting date after the 30 day time frame has expired. While on the Probationary Hold list, you may not admit patients, schedule surgeries or procedures but can continue treatment of any current inpatients and perform any previously scheduled surgeries or procedures scheduled prior to the probationary hold. If the Practitioner’s medical records are not completed within 15 days of notice, the Practitioner may also be otherwise warned, placed on probation, have privileges reduced, suspended, restricted, denied, non-renewed, or terminated, on

a case-by-case basis. Should a suspension occur and last for more than 30 days, The Jewish Hospital is required to report this adverse action to the National Practitioner Data Bank. The staff in the Medical Records Department is available to assist you in completion of your records. Should you have any questions regarding this letter, please call Medical Records at (513) 686-3134.

MERCY HEALTH - JEWISH HOSPITAL
SURGERY
PACU SURGERY
AUDITORIUM
DININGVISITOR
PARKINGGARAGE
ENTRANCE A
ENTRANCE B
EMERGENCY DEPARTMENTPARKING ONLY
STERILEPROCESSING ADMINISTRATION
PRE/POST
E. GALBRAITH RD.
HAPPINESS WAY
KE
NW
OO
D R
D.
FR
OLI
C D
R.
ELEVATOR TO:
LOBBY
GIFTSHOP
ENDOSCOPY/CYSTOSCOPY
WOUNDCARE
KEY Elevators
Stairs
Patient Access Route
Entrances
EMERGENCYDEPARTMENTENTRANCE
Level 1: Emergency DepartmentLevel 2: Same Day SurgeryLevel 3: Blood Cancer Center; Blood Cancer Program; Outpatient Oncology InfusionLevel 4: ICULevel 5: 5 Tower Med-Surg
ELEVATOR TO:Level 1: Cath Lab; Gamma KnifeLevel 2: Surgery, PACULevel 4: 4 PCULevel 5: 5 South-Med-SurgLevel 6: 6 South-Med-Surg
ELEVATOR TO:Level 1: RadiologyLevel 2: OR & Endoscopy
ELEVATOR TO:Level 1: Simulation LabsLevel 2: Outpatient Cardiac Testing; Wound Care and AdministrationLevel 3: Acute Rehabilitation Unit
N
EMERGENCY DEPARTMENT ROOKWOOD
5.9mi
OUTPATIENT CLINICAL
.7mi








![MAG MODEL MEDICAL STAFF BYLAWS - Leadership in Web viewNCMS MODEL MEDICAL STAFF BYLAWS. Annotated ©2012 Legal Counsel for the Medical Staff PLLC. ... [Medical Staff Manager/Coordinator]](https://img.dokumen.tips/doc/110x75/5a78edb27f8b9a68148ca2ae/mag-model-medical-staff-bylaws-leadership-in-web-viewncms-model-medical.jpg)




















