Embed Size (px)
Citation preview

1 Medical Protocol - Diabetes | INESSS
MEDICAL PROTOCOL
Subject of this medical protocol:
Adjustment of hypoglycemic agents or insulin and laboratory tests for monitoring type 2 diabetes.
Validated by:
Original version (October 2013): The Comité d’experts ministériel sur les ordonnances collectives.
Revised version (October 2016): An expert committee of the Institut national d’excellence en santé et en services sociaux (INESSS).
Effective date:
October 2016
Reference:
Yes No
Adjustment of hypoglycemic agents or insulin and laboratory tests for monitoring type 2 diabetes (No.: ).
Approved by: INESSS Revision date:
April 2019
Expiry date:
October 2019
AUTHORIZED PROFESSIONALS
Nurses and pharmacists practicing their profession in Québec.
TARGETED CLINICAL CONDITIONS
Persons diagnosed with type 2 diabetes and referred by the treating physician for joint follow-up by an authorized professional.
OVERALL OBJECTIVES
To achieve the therapeutic target set by the treating physician.

2
INESSS | Medical Protocol - Diabetes
INSTRUCTIONS
1. GLYCEMIC TARGETS
GLYCEMIC CONTROL TARGETS: GLYCATED HEMOGLOBIN (HbA1C)
HbA1c (%) Details
≤ 7% For most persons with type 2 diabetes.
≤ 6.5% For certain individuals, to further lower their risk of retinopathy and nephropathy. Benefit should be weighed against the risk of hypoglycemia.
7.1 to 8.5%
For certain individuals for whom less aggressive treatment is desired (limited life expectancy, high level of functional dependence, severe coronary artery disease associated with high risk of an ischemic event, multiple comorbidities, unnoticed hypoglycemic episodes, severe recurrent hypoglycemic episodes, longstanding diabetes and difficulty achieving an HbA1c level ≤ 7% despite effective doses of several hypoglycemic agents and the use of basal insulin, and frail, elderly persons).
GLYCEMIC CONTROL TARGETS: CAPILLARY BLOOD GLUCOSE LEVELS
Capillary blood glucose level
Details
4.0 to 7.0 mmol/L Preprandial (AC) *
5.0 to 10.0 mmol/L 2 hours postprandial (PC)
5.0 to 8.0 mmol/L 2 hours postprandial (PC): if the target HbA1c is not achieved
* Preprandial (AC) capillary blood glucose levels for frail, elderly persons: 5.0 to 12.0 mmol/L.

3
Medical Protocol - Diabetes | INESSS
2. HYPOGLYCEMIC AGENTS
2.1 GENERAL PRINCIPLES
Therapeutic intent:
• HbA1C < 8.5%: if the targets are not achieved within 2 or 3 months with lifestyle management, metformin should be initiated.
• HbA1C ≥ 8.5% (with no metabolic decompensation): metformin should be initiated at the same time as lifestyle management. A combination of hypoglycemic agents may be considered.
• Symptomatic hyperglycemia (with metabolic decompensation): insulin should be initiated with or without metformin.
Combining hypoglycemic agents at submaximal doses helps achieve glycemic targets faster and with fewer adverse effects than monotherapy at the maximum dose.
When hypoglycemic agents are combined with or without insulin, classes with different mechanisms of action should be used.
All medication additions and adjustments, combined with lifestyle management, should make it possible to achieve glycemic targets within 3 to 6 months.
Adjustment principles:
Calculate the average capillary blood glucose level for each time of the day for the past 3 to 7 days.
Gradually increase the medication until:
• Preprandial capillary blood glucose levels < 7 mmol/L or < the targets set by the physician are obtained. • The occurrence of intolerance (e.g., gastrointestinal problems).
Modify the dose of only one hypoglycemic agent at a time.
Hypoglycemic and hyperglycemic episodes:
Correct hypoglycemic episodes first, starting with the first one of the day, before correcting hyperglycemic episodes.
Do not take into account a hypoglycemic or hyperglycemic episode associated with an exceptional or explainable one-time situation.
When adjusting hypoglycemic agents, return to the previous dose if intolerance or hypoglycemic episodes occur.

4
INESSS | Medical Protocol - Diabetes
2.2 GENERAL CONSIDERATIONS AND DOSAGE TITRATION REGIMENS
2.2.1 BIGUANIDES
GENERAL CONSIDERATIONS AND TITRATION REGIMENS FOR THE CLASS OF BIGUANIDES
Drug Starting dose * and
administration schedule
Titration regimen Details
METFORMIN Available strengths: 500 and 850 mg Scored tablets RAMQ: covered
250 to 500 mg PO BID at meals
Titration if BID administration: ↑ each dose by 250 mg every 1 to 2 weeks The daily dose can be split into 2 or 3 doses (BID or TID), depending on tolerance and compliance. Titration if TID administration: ↑ the dose by 250 mg (maximum: 2 doses/day) every 1 to 2 weeks. Maximum dose: 2550 mg/day If gastrointestinal intolerance: ↓ the dose to the lower adjustment step for 1 week or until symptom resolution. Resume with a slower dosage titration: ↑ the dose by 250 mg (maximum: 1 dose/day) or ↑ the adjustment interval.
Negligeable hypoglycemic episodes No weight gain Adverse effects: Gastrointestinal problems (e.g., nausea, diarrhea, abdominal cramps) Vitamin B12 deficiency Lactic acidosis: increased risk in the presence of conditions associated with hypoxemia and cardiovascular collapse Contraindications: Known drug allergy to biguanides History of lactic acidosis Severe renal failure: eGFR < 30 ml/min/1.73 m2 Severe liver failure Precautions: Radiological examination, surgery, severe dehydration: can exacerbate renal failure Pregnancy or breastfeeding Drug interactions: Drugs that can impair renal function (e.g., nonsteroidal anti-inflammatories (NSAIDs), antihypertensives, diuretics, iodine-containing contrast agents) Referral to physcian:
• Vitamin B12 deficiency • eGFR < 60 ml/min/1.73 m2
METFORMIN extended release Available strengths: 500 and 1000 mg Unscored tablets Not covered by the RAMQ
500 to 1000 mg PO daily at dinner
Titration: ↑ the dose by 500 mg every 1 to 2 weeks Maximum dose: 2000 mg/day If gastrointestinal intolerance: ↓ the dose to the lower adjustment level for 1 week or until symptom resolution before resuming the same dosage titration.
* Examples of usually prescribed starting doses.
LABORATORY TESTS
Tests Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
CBC √
Vitamin B12 √
Creatinine (eGFR) √ √
* Tests accepted if performed within the past 3 months. † When the capillary blood glucose targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.

5
Medical Protocol - Diabetes | INESSS
2.2.2 SECRETAGOGUES-SULFONYLUREAS
GENERAL CONSIDERATIONS AND DOSAGE TITRATION REGIMENS FOR THE CLASS OF SECRETAGOGUES-SULFONYLUREAS
Drug Starting dose * and
administration schedule
Titration regimen Details
GLICLAZIDE Extended release Available strengths: 30 and 60 mg 60 mg scored tablets 30 mg unscored tablets RAMQ codes
30 to 60 mg PO daily at breakfast or at the first main meal of the day
Titration: ↑ the dose by 30 mg every 2 weeks Maximum dose: 120 mg/day
Adverse effects: Weight gain Frequent hypoglycemic episodes (especially with glyburide). The risk is higher in the elderly and persons with renal failure. Contraindications: Known drug allergy to sulfonylureas Severe liver failure Renal failure:
Gliclazide, glimepiride: eGFR < 15 ml/min/1.73 m2 Glyburide: eGFR < 30 ml/min/1.73 m2
Precautions: Known drug allergy to sulfonamides Pregnancy or breastfeeding Drug interactions: Under the influence of sympatholytic drugs (e.g., β-blockers, clonidine), signs of adrenergic counter-regulation secondary to hypoglycemia may be ↓ or absent. GLP-1s and SGLT2s: risk of hypoglycemic episodes (a ↓ in the secretagogue dose is generally required, unless HbA1c > 8%) Referral to physician:
• Unexplainable hypoglycemic episodes: ↓ the dose to the lower adjustment step and advise the physician.
• Renal failure: Gliclazide and glimepiride: if eGFR < 30 ml/min/1.73 m2 Glyburide: if eGFR < 50 ml/min/1.73 m2
GLIMEPIRIDE Available strengths: 1, 2 and 4 mg RAMQ codes
1 mg PO daily at breakfast or at the first main meal of the day
Titration: ↑ the dose by 1 mg every 2 weeks Maximum dose: 8 mg/day
2 mg PO daily at breakfast or at the first main meal of the day
Titration: ↑ the dose by 1 to 2 mg every 2 weeks Maximum dose: 8 mg/day
GLYBURIDE Available strengths: 2.5 and 5 mg Scored tablets RAMQ: covered
1.25 mg PO daily or BIDat meals If daily administration, give at the first main meal of the day
Titration: ↑ each dose by 1.25 mg every 2 weeks OR every 3 weeks in individuals ≥ 60 years of age The daily dose can be split into 2 doses (BID) if the AC capillary blood glucose levels at breakfast remain > 7 mmol/L. Maximum dose: 20 mg/day (maximum: 10 mg/dose)
2.5 to 5 mg PO daily or BID at meals If daily administration, give at the first main meal of the day
Titration: ↑ each dose by 2.5 mg every 2 weeks OR every 3 weeks in individuals ≥ 60 years of age The daily dose can be split into 2 doses (BID) if the AC capillary blood glucose levels at breakfast remain > 7 mmol/L. Maximum dose: 20 mg/day (maximum: 10 mg/dose)
* Examples of usually prescribed starting doses.
LABORATORY TESTS
Tests Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
Creatinine (eGFR) √ √
* Tests accepted if performed within the past 3 months. † When the capillary blood glucose targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.

6
INESSS | Medical Protocol - Diabetes
2.2.3 SECRETAGOGUES-MEGLITINIDES
GENERAL CONSIDERATIONS AND TITRATION REGIMENS FOR THE CLASS OF SECRETAGOGUES-MEGLITINIDES
Drug Starting dose * and
administration schedule
Titration regimen Details
REPAGLINIDE Available strengths: 0.5, 1 and 2 mg RAMQ codes
0.5 to 2 mg PO daily , BID or TID Administer before the meal (0 to 15 min before)
Titration: If the average mealtime capillary blood glucose level is high (˃ 7 mmol/L or > target set by the physician), double the dose that was given at the previous meal (maximum: 3 doses/day). Adjustment interval: every week. The daily dose can be split into 3 doses (TID). Maximum dose: 12 mg/day
Effect more pronounced on postprandial blood glucose levels Safe in the presence of renal failure Adverse effects: Hypoglycemic episodes Weight gain Headaches Constipation Contraindications: Known drug allergy to meglitinides Pregnancy or breastfeeding Liver failure Precautions: Do not take repaglinide if the meal is skipped Drug interactions: Clopidogrel: ↑ in the plasma repaglinide concentration (↑ risk of hypoglycemic episodes) GLP-1s and SGLT2s: risk of hypoglycemic episodes (a ↓ in the secretagogue dose is generally required, unless HbA1c > 8%) Referral to physician:
• Unexplainable hypoglycemic episodes: ↓ the dose to the lower adjustment step and advise the physician.
* Examples of usually prescribed starting doses.
LABORATORY TESTS
Test Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
* Test accepted if performed within the past 3 months. † When the capillary blood glucose targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.

7
Medical Protocol - Diabetes | INESSS
2.2.4 ALPHA-GLUCOSIDASE INHIBITORS
GENERAL CONSIDERATIONS AND TITRATION REGIMENS FOR THE CLASS OF ALPHA-GLUCOSIDASE INHIBITORS
Drug Starting dose * and
administration schedule
Titration regimen Details
ACARBOSE Available strengths: 50 and 100 mg Scored tablets RAMQ: covered
25 mg PO daily, BID or TID at the start of the meal
Titration: the dose by 25 mg/day ( the dose for one meal at a time; maximum: 3 doses/day) every 2 weeks The daily dose can be split into 3 doses (TID). Maximum dose: 300 mg/day If gastrointestinal intolerance: ↓ the dose to the lower adjustment step for 1 week or until symptom resolution. Resume the titration, increasing the adjustment interval.
Negligible hypoglycemic episodes: if hypoglycemia occurs, do not give sucrose (p. ex., juice or white sugar), but rather honey or milk No weight gain Adverse effects: Gastrointestinal problems (e.g., diarrhea, flatulence, bloating) Contraindications: Known drug allergy to alpha-glucosidase inhibitors Pregnancy or breastfeeding Inflammatory bowel disease Intestinal obstruction Colonic ulcer Cirrhosis Renal failure: eGFR < 25 ml/min/1.73 m2 Referral to physician:
• eGFR < 25 ml/min/1.73 m2 • ↑ ALT (> 3 times the upper limit of normal
[ULN])
* Examples of usually prescribed starting doses.
LABORATORY TESTS
Tests Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
Creatinine (eGFR) √ √
ALT √ √
* Tests accepted if performed within the past 3 months. † When the capillary glycemic targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.
8
INESSS | Medical Protocol - Diabetes
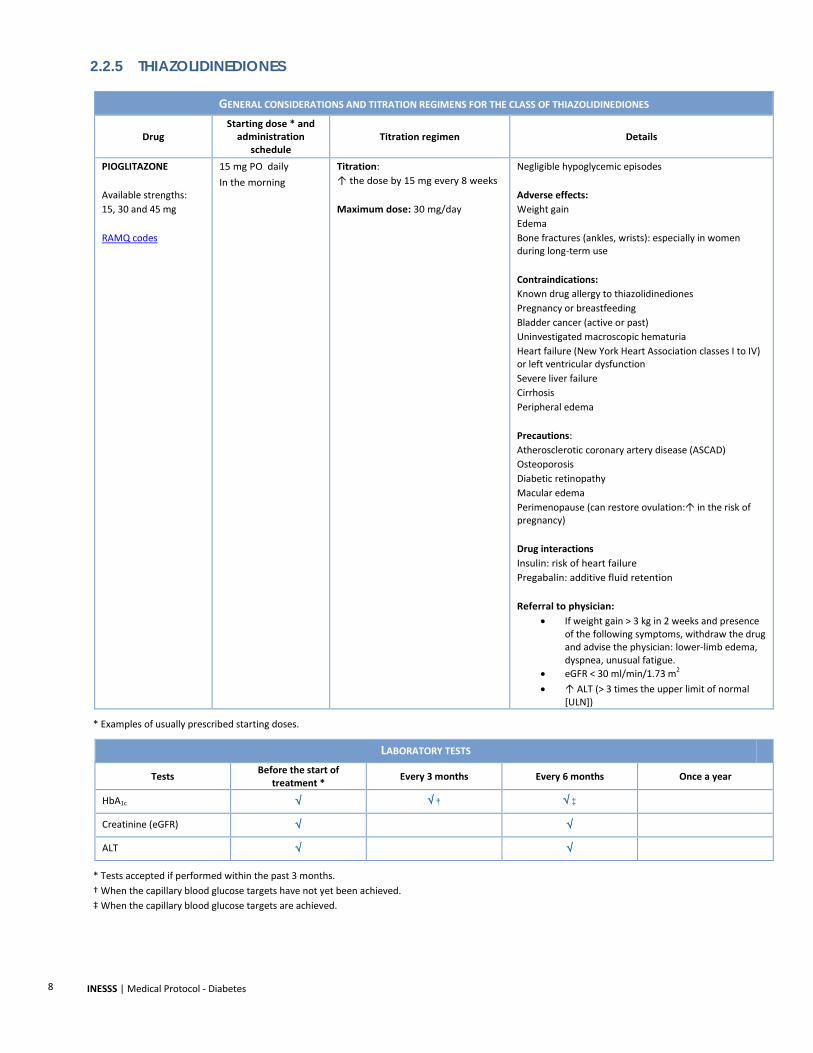
2.2.5 THIAZOLIDINEDIONES
GENERAL CONSIDERATIONS AND TITRATION REGIMENS FOR THE CLASS OF THIAZOLIDINEDIONES
Drug Starting dose * and
administration schedule
Titration regimen Details
PIOGLITAZONE Available strengths: 15, 30 and 45 mg RAMQ codes
15 mg PO daily In the morning
Titration: ↑ the dose by 15 mg every 8 weeks Maximum dose: 30 mg/day
Negligible hypoglycemic episodes
Adverse effects: Weight gain Edema Bone fractures (ankles, wrists): especially in women during long-term use Contraindications: Known drug allergy to thiazolidinediones Pregnancy or breastfeeding Bladder cancer (active or past) Uninvestigated macroscopic hematuria Heart failure (New York Heart Association classes I to IV) or left ventricular dysfunction Severe liver failure Cirrhosis Peripheral edema Precautions: Atherosclerotic coronary artery disease (ASCAD) Osteoporosis Diabetic retinopathy Macular edema Perimenopause (can restore ovulation: in the risk of pregnancy) Drug interactions Insulin: risk of heart failure Pregabalin: additive fluid retention
Referral to physician:
• If weight gain > 3 kg in 2 weeks and presence of the following symptoms, withdraw the drug and advise the physician: lower-limb edema, dyspnea, unusual fatigue.
• eGFR < 30 ml/min/1.73 m2 • ↑ ALT (> 3 times the upper limit of normal
[ULN])
* Examples of usually prescribed starting doses.
LABORATORY TESTS
Tests Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
Creatinine (eGFR) √ √
ALT √ √
* Tests accepted if performed within the past 3 months. † When the capillary blood glucose targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.

9
Medical Protocol - Diabetes | INESSS
2.2.6 GLUCAGON-LIKE PEPTIDE-1 (GLP-1) RECEPTOR AGONISTS
GENERAL CONSIDERATIONS AND TITRATION REGIMENS FOR THE CLASS OF GLP-1S
Drug Starting dose * and
administration schedule
Titration regimen Details
ALBIGLUTIDE Available formats: Injectable solutions of 30 mg/0.5 ml and 50 mg/0.5 ml Not covered by the RAMQ
30 mg SC every week The administration schedule can be modified: respect a minimum of 72 hrs between doses.
Titration: ↑ the dose to 50 mg after 4 weeks Maximum dose: 50 mg/week If gastrointestinal intolerance: ↓ the dose to the lower adjustment step for 1 week or until symptom resolution. Resume the titration, increasing the adjustment interval.
Negligible hypoglycemic episodes Significant weight loss Adverse effects: Gastrointestinal problems (e.g., nausea, vomiting): effects ↓ after a few weeks in heart rate Injection site reaction Contraindications: Known drug allergy to GLP-1s Pregnancy or breastfeeding Personal or family history of medullary thyroid carcinoma Multiple endocrine neoplasia syndrome type 2 Renal failure:
Liraglutide: if eGFR < 30 ml/min/1.73 m2
Precautions: History of pancreatitis Liver failure Heart disease that could be exacerbated by an in the heart rate (e.g., congestive heart failure, atrial fibrillation, ischemic heart disease) Inflammatory heart disease Drug interactions Insulin or secretagogues: risk of hypoglycemic episodes (a ↓ in the insulin or secretagogue dose is generally required, unless HbA1c > 8%) Referral to physician:
• eGFR < 30 ml/min/1.73 m2
DULAGLUTIDE Available formats: Injectable solutions of 0.75 mg/0.5 ml and 1.5 mg/0.5 ml Exceptional medication
0.75 mg SC every week The administration schedule can be modified: respect a minimum of 72 hrs between doses.
Titration: ↑ the dose by 0.75 mg after 4 weeks Maximum dose: 1.5 mg/week If gastrointestinal intolerance: ↓ the dose to the lower adjustment step for 1 week or until symptom resolution. Resume the titration, increasing the adjustment interval.
LIRAGLUTIDE Available format: Injectable solution of 6 mg/ml Exceptional medication
0.6 mg SC daily If severe nausea, the dose can be administered at bedtime (HS).
Titration: ↑ the dose by 0.6 mg every 2 weeks Maximum dose: 1.8 mg/day If gastrointestinal intolerance: ↓ the dose to the lower adjustment step for 1 week or until symptom resolution. Resume the titration, increasing the adjustment interval.
* Examples of usually prescribed starting doses.
LABORATORY TESTS
Tests Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
Creatinine (eGFR) √ √
* Tests accepted if performed within the past 3 months. † When the capillary blood glucose targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.
10
INESSS | Medical Protocol - Diabetes
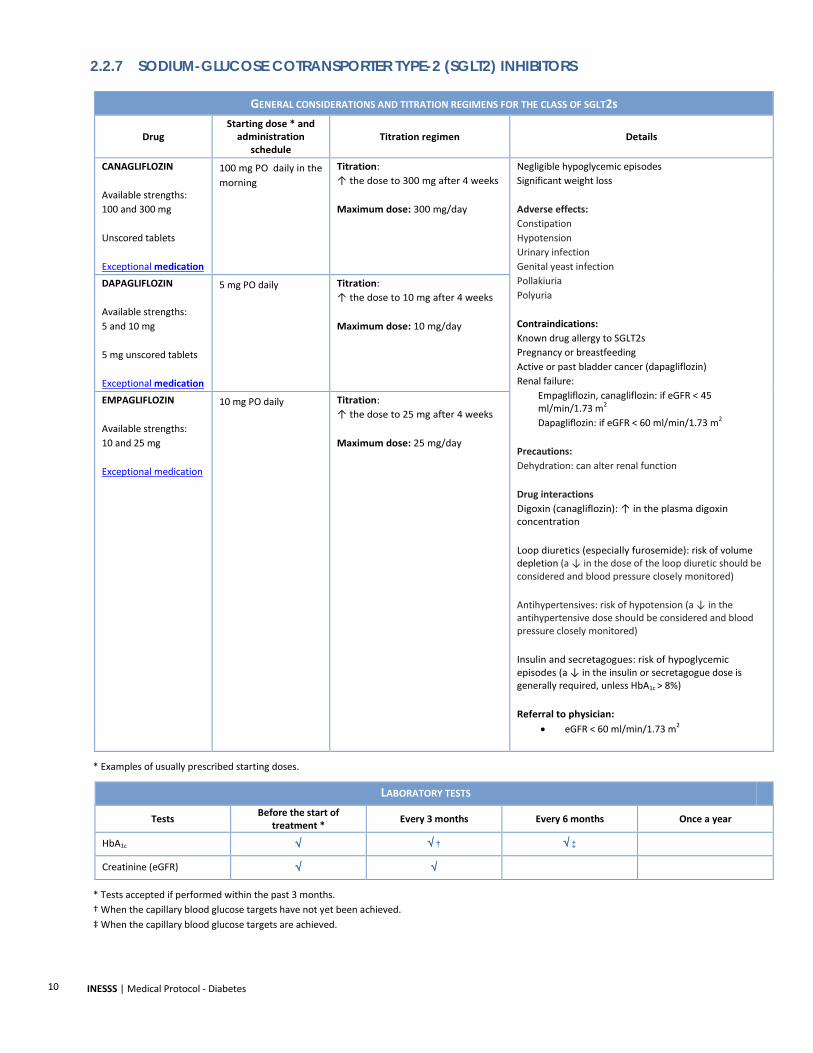
2.2.7 SODIUM-GLUCOSE COTRANSPORTER TYPE-2 (SGLT2) INHIBITORS
GENERAL CONSIDERATIONS AND TITRATION REGIMENS FOR THE CLASS OF SGLT2s
Drug Starting dose * and
administration schedule
Titration regimen Details
CANAGLIFLOZIN Available strengths: 100 and 300 mg Unscored tablets Exceptional medication
100 mg PO daily in the morning
Titration: ↑ the dose to 300 mg after 4 weeks Maximum dose: 300 mg/day
Negligible hypoglycemic episodes Significant weight loss Adverse effects: Constipation Hypotension Urinary infection Genital yeast infection Pollakiuria Polyuria Contraindications: Known drug allergy to SGLT2s Pregnancy or breastfeeding Active or past bladder cancer (dapagliflozin) Renal failure:
Empagliflozin, canagliflozin: if eGFR < 45 ml/min/1.73 m2 Dapagliflozin: if eGFR < 60 ml/min/1.73 m2
Precautions: Dehydration: can alter renal function Drug interactions Digoxin (canagliflozin): ↑ in the plasma digoxin concentration Loop diuretics (especially furosemide): risk of volume depletion (a ↓ in the dose of the loop diuretic should be considered and blood pressure closely monitored) Antihypertensives: risk of hypotension (a ↓ in the antihypertensive dose should be considered and blood pressure closely monitored) Insulin and secretagogues: risk of hypoglycemic episodes (a ↓ in the insulin or secretagogue dose is generally required, unless HbA1c > 8%) Referral to physician:
• eGFR < 60 ml/min/1.73 m2
DAPAGLIFLOZIN Available strengths: 5 and 10 mg 5 mg unscored tablets Exceptional medication
5 mg PO daily Titration: ↑ the dose to 10 mg after 4 weeks Maximum dose: 10 mg/day
EMPAGLIFLOZIN Available strengths: 10 and 25 mg Exceptional medication
10 mg PO daily Titration: ↑ the dose to 25 mg after 4 weeks Maximum dose: 25 mg/day
* Examples of usually prescribed starting doses.
LABORATORY TESTS
Tests Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
Creatinine (eGFR) √ √
* Tests accepted if performed within the past 3 months. † When the capillary blood glucose targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.

11
Medical Protocol - Diabetes | INESSS
3. INSULIN
3.1 GENERAL PRINCIPLES
Adjustment principles:
The adjustment should take into account the type of insulin, the administration schedule and the causes of hypoglycemic or hyperglycemic episodes.
Calculate, for each time of the day, the average capillary blood glucose level for the past 3 to 7 days.
It is best to adjust one type of insulin and correct one capillary blood glucose level at a time.
When insulin is used in combination, adjust the hypoglycemic agent first.
Opt for the maximum increase in the number of insulin units, unless there is a risk of hypoglycemic episodes.
Adjust insulin doses with considerable caution in elderly persons, given the increased risk of hypoglycemic episodes.
Hypoglycemic and hyperglycemic episodes:
Correct hypoglycemic episodes first, starting with the first one of the day, before correcting hyperglycemic episodes.
Do not take into account a hypoglycemic or hyperglycemic episode associated with an exceptional or explainable one-time situation. In the event of hypoglycemic episodes, adjust the insulin dose responsible (2 consecutive days at the same time of the day).
3.2 GENERAL CONSIDERATIONS
GENERAL CONSIDERATIONS REGARDING INSULIN
Drug Details
INSULIN Adverse effects: Frequent hypoglycemic episodes Significant weight gain Injection site reaction Contraindications: Known drug allergy to insulin Precautions: Pregnancy or breastfeeding: frequent dose adjustments required
Drug interactions: Thiazolidinediones: risk of heart failure Under the influence of sympatholytic drugs (e.g., β-blockers, clonidine), signs of adrenergic counter-regulation secondary to hypoglycemia may be ↓ or absent. GLP-1s and SGLT2s: risk of hypoglycemic episodes (a ↓ in the insulin dose is generally required, unless HbA1c > 8%)
LABORATORY TESTS
Test Before the start of treatment * Every 3 months Every 6 months Once a year
HbA1c √ √ † √ ‡
* Testaccepted if performed within the past 3 months. † When the capillary blood glucose targets have not yet been achieved. ‡ When the capillary blood glucose targets are achieved.

12
INESSS | Medical Protocol - Diabetes
3.3 TYPES OF INSULIN
INSULIN
Insulin Action Type of insulin Onset of
action Peak effect Duration of action
Administration schedule
Responsable for blood glucose level
BASA
L
Intermediate-acting
(RAMQ: covered)
Isophane (NPH)
1 to 3 hrs 5 to 8 hrs Up to
18 hrs
30 min before breakfast AC dinner blood glucose level
30 min before dinner
next-day AC breakfast blood glucose level
At bedtime next-day AC breakfast blood glucose level
Extended-action
analogues
(exceptional medications)
Detemir 90 min Not applicable 16 to 24 hrs At bedtime next-day AC breakfast blood
glucose level
Glargine 90 min Not applicable
Up to
24 hrs At bedtime next-day AC breakfast blood
glucose level
Glargine 300U Up to
6 hrs Not
applicable Up to
30 hrs At the same time
every day next-day AC breakfast blood
glucose level
PRAN
DIAL
Short-acting (RAMQ: covered)
Crystalline zinc (regular) 30 min 2 to 3 hrs 6.5 hrs 15 to 30 min
before a meal AC next-meal blood glucose level
Long-acting analogues
(RAMQ: covered)
Aspart 10 to 15 min 1 to 1.5 hrs 3 to 5 hrs 0 to 15 min
before breakfast
Pre-breakfast dose:
2-hr PC breakfast blood glucose level or AC lunch blood glucose
level *
Glulisine 10 to 15 min 1 to 1.5 hrs 3 to 5 hrs 0 to 15 min
before lunch
Pre-lunch dose:
2-hr PC lunch blood glucose level or AC dinner blood glucose level *
Lispro 10 to 15 min 1 to 2 hrs 3.5 to 4.75
hrs 0 to 15 min
before dinner
Pre- dinner dose:
2-hr PC dinner blood glucose level or HS blood glucose level *
PREM
IXED
(pra
ndia
l-bas
al)
Short/inter-mediate-
acting (RAMQ: covered)
Regular/NPH Depends on the prandial/basal ratio
15 to 30 min before breakfast
Pre-breakfast dose:
AC lunch blood glucose level and AC dinner blood glucose level
15 to 30 min before dinner
Pre-dinner dose:
HS blood glucose level and next-day AC breakfast blood glucose level
Rapid/inter-mediate-
acting analogues
(RAMQ codes)
Biphasic aspart Depends on the prandial/basal ratio 0 to 15 min before breakfast
Pre-breakfast dose:
2-hr PC breakfast blood glucose level or AC lunch blood glucose
level * and AC dinner blood glucose level
Lispro/lispro protamine Depends on the prandial/basal ratio 0 to 15 min
before dinner
Pre-dinner dose:
2-hr PC dinner blood glucose level or HS blood glucose level * and the
next-day AC breakfast blood glucose level
* If blood glucose level not determined 2 hours postprandially (PC).

13
Medical Protocol - Diabetes | INESSS
3.4 TITRATION REGIMENS
INSULIN TITRATION REGIMENS
ADJUSTMENT INTERVAL: EVERY 3 TO 7 DAYS
Time of day Capillary blood glucose level Adjustment * † Responsible insulin
NIGHT, BREAKFAST
Blood glucose level < 4 mmol/L or < glycemic targets
↓ the dose by 10% OR ↓ the dose by 2 to 4 units
Adjust the basal insulin administered at dinner or bedtime or the premixed insulin administered at dinner Blood glucose level > 7 mmol/L or > glycemic
targets and absence of nocturnal hypoglycemic episodes
↑ the dose by 10% OR ↑ the dose by 1 to 2 units (↑ the dose by 2 to 4 units if the blood glucose level ≥ 10 mmol/L)
LUNCHTIME
Blood glucose level < 4 mmol/L or < glycemic targets
↓ the dose by 10% OR ↓ the dose by 2 to 4 units
Adjust the prandial or premixed insulin administered at breakfast Blood glucose level > 7 mmol/L or > glycemic
targets ↑ the dose by 10% OR ↑ the dose by 1 to 2 units (↑ the dose by 2 to 4 units if the blood glucose level ≥ 10 mmol/L)
AFTERNOON (within 3 hrs after lunch)
Blood glucose level < 4 mmol/L or < glycemic targets
↓ the dose by 10% OR ↓ the dose by 2 to 4 units
Adjust the prandial insulin administered at lunchtime Blood glucose level > 7 mmol/L or > glycemic
targets ↑ the dose by 10% OR ↑ the dose by 1 to 2 units (↑ the dose by 2 to 4 units if the blood glucose level ≥ 10 mmol/L)
DINNER (more than 3 hrs after dinner)
Blood glucose level < 4 mmol/L or < glycemic targets
↓ the dose by 10% OR ↓ the dose by 2 to 4 units
Adjust the basal or premixed insulin administered at breakfast or the prandial insulin administered at lunchtime
Blood glucose level > 7 mmol/L or > glycemic targets
↑ the dose by 10% OR ↑ the dose by 1 to 2 units (↑ the dose by 2 to 4 units if the blood glucose level ≥ 10 mmol/L)
BEDTIME
Blood glucose level < 4 mmol/L or < glycemic targets
↓ the dose by 10% OR ↓ the dose by 2 to 4 units
Adjust the prandial or premixed insulin administered at dinner Blood glucose level > 7 mmol/L or > glycemic
targets ↑ the dose by 10% OR ↑ the dose by 1 to 2 units (↑ the dose by 2 to 4 units if the blood glucose level ≥ 10 mmol/L)
* Two insulin titration regimens: a) percentage of the insulin dose OR b) number of insulin units. † Round off the dose (minimum: 1 unit).

14
INESSS | Medical Protocol - Diabetes
DEVELOPMENT PROCESS
The development process is based on the triangulation of a number of data sources, including best clinical practice recommendations and both contextual and experiential data.
A systematic review of the clinical practice guideline literature, consensus reports and health technology assessment reports published between 2012 and 2016 was first conducted to identify recommendations concerning pharmacological treatment modalities for type 2 diabetes. Product monographs and Health Canada advisories were consulted as well. The methodology used to carry out this systematic literature review meets the production standards of the Institut national d’excellence en santé et en services sociaux (INESSS).
The analysis of the data from the systematic literature review was performed from a contextualization perspective regarding practice in Québec, using experiential data obtained from health professionals on an expert committee and the members of the INESSS project team.

15
Medical Protocol - Diabetes | INESSS
APPENDED A: HYPOGLYCEMIC AGENTS
HYPOGLYCEMIC AGENTS AVAILABLE IN CANADA
Biguanides Extended-release metformin Metformin
Secretagogues-sulfonylureas Chlorpropamide * Extended-release gliclazide Gliclazide * Glimepiride Glyburide Tolbutamide *
Secretagogues-meglitinides Repaglinide
Alpha-glucosidase inhibitors Acarbose
Thiazolidinediones Pioglitazone Rosiglitazone *
Dipeptidylpeptidase-4 (DPP-4) inhibitors Alogliptine † Linagliptine † Saxagliptine † Sitagliptine †
Glucagon-like peptide-1 (GLP-1) receptor agonists Albiglutide Dulaglutide Exenatide * Extented-release exenatide † Liraglutide
Sodium-glucose cotransportor type-2 (SGLT2) inhibitors Canagliflozine Dapagliflozine Empagliflozine
Combined formulations ‡ Alogliptin/metformin Alogliptin/pioglitazone Canagliflozin/metformin Dapagliflozin/metformin Empagliflozin/metformin
Linagliptine/metformine Rosiglitazone/glimepiride Rosiglitazone/metformin Saxagliptine/metformin Sitagliptine/metformin
* Used infrequently. † Fixed dose (no adjustment required) or adjustment made by the physician (based on the eGFR). ‡ The medical protocol targets individual formulations.

16
INESSS | Medical Protocol - Diabetes
ANNEXE B: ACRONYMS AND ABBREVIATIONS
AC preprandial
ALT alanine aminotransferase
ASCAD atherosclerotic coronary artery disease
BID twice daily
CBC complete blood count
DPP-4 dipeptidylpeptidase-4 inhibitor
e.g. for example
eGFR estimated glomerular filtration rate
GLP-1 glucagon-like peptide-1 receptor agonist
HbA1c glycated or glycosylated hemoglobin
HS at bedtime
NSAID nonsteroidal anti-inflammatory
PC postprandial
PO per os
RAMQ Régie de l’assurance maladie du Québec
SC subcutaneous
SGLT2 sodium-glucose cotransporter type 2 inhibitor
TID three times daily
ULN upper limit of normal

17
Medical Protocol - Diabetes | INESSS
REFERENCES
American Diabetes Association (ADA). Standards of medical care in diabetes—2016. Diabetes Care 2016;39(Suppl 1):S1-S112.
Canadian Diabetes Association (CDA). Traitement pharmacologique du diabète de type 2 : mise à jour intérimaire 2016. Toronto, ON:
ACD; 2016. Available at: http://guidelines.diabetes.ca/cdacpg_resources/Ch13_Traitement-pharmacologique-du-diabete-de-type-2-2016.pdf.
Canadian Diabetes Association (CDA). Chapitre 13. Figure 2. Antihyperglycémiants et fonction rénale. 2016 update. Toronto, ON:
CDA; 2016. Available at: http://guidelines.diabetes.ca/cdacpg_resources/Ch13_Fig2_Antihyperglycemiants-et-fonction-renale-2016.pdf.
Canadian Diabetes Association (CDA). Annexe 6. Considérations thérapeutiques en matière de traitements couramment utilisés chez
les patients diabétiques présentant une atteinte rénale à divers stades. 2015 update. Toronto, ON: CDA; 2015. Available at: http://guidelines.diabetes.ca/cdacpg_resources/appendices/Appendix_6_FR_2015.pdf.
Canadian Pharmacists Association (CPhA). Compendium des produits et spécialités pharmaceutiques (CPS). Ottawa, ON: CPhA.
Available at: https://www.e-therapeutics.ca/search?lang=fr. Canadian Agency for Drugs and Technologies in Health (CADTH). Optimal use recommendations for second and third-line therapy for
patients with type 2 diabetes. CADTH Optimal Use Report; Vol. 3, No. 1d. Ottawa, ON: CADTH; 2013. Available at: https://www.cadth.ca/sites/default/files/pdf/OP0512_Diabetes_RecsReport_2nd_3rd-line_e.pdf.
Canadian Diabetes Association (CDA) Clinical Practice Guidelines Expert Committee. Lignes directrices de pratique clinique 2013 de
l’Association canadienne du diabète pour la prévention et le traitement du diabète au Canada. Can J Diabetes 2013;37(Suppl 5):S361-S598.
Handelsman Y, Bloomgarden ZT, Grunberger G, Umpierrez G, Zimmerman RS, Bailey TS, et al. American Association of Clinical
Endocrinologists and American College of Endocrinology – Clinical practice guidelines for developing a diabetes mellitus comprehensive care plan - 2015. Endocr Pract 2015;21(Suppl 1):1-87.
Haute Autorité de Santé (HAS). Guide parcours de soins. Diabète de type 2 de l’adulte. Saint-Denis La Plaine: HAS; 2014. Available at:
http://www.has-sante.fr/portail/upload/docs/application/pdf/2014-04/guide_pds_diabete_t_3_web.pdf. Haute Autorité de Santé (HAS). Stratégie médicamenteuse du contrôle glycémique du diabète de type 2. Recommandation de bonne
pratique. Saint-Denis La Plaine: HAS; 2013. Available at: http://www.has-sante.fr/portail/jcms/c_1358579/recommandations-diabete-de-type-2.
National Institute for Health and Care Excellence (NICE). Type 2 diabetes in adults: Management. NICE guideline NG28. London,
England: 2015. Available at: https://www.nice.org.uk/guidance/ng28. Redmon B, Caccamo D, Flavin P, Michels R, O’Connor P, Roberts J, et al. Diagnosis and management of type 2 diabetes mellitus in
adults. Bloomington, MN: Institute for Clinical Systems Improvement (ICSI); 2014. Available at: https://www.icsi.org/_asset/3rrm36/Diabetes.pdf.
Health Canada. Inhibiteurs du SGLT2 [INVOKANA (canagliflozine), FORXIGA (dapagliflozine), XIGDUO (dapagliflozine/metformine),
JARDIANCE (empagliflozine)] - Risque d’acidocétose diabétique [website]. Ottawa, ON: Health Canada; 2016. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2016/58404a-fra.php.
Health Canada. FORXIGA et INVOKANA : Santé Canada commence l’examen de l’innocuité de médicaments antidiabétiques appelés
inhibiteurs du SGLT2 et du risque d’acidocétose [website]. Ottawa, ON: Health Canada; 2015. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2015/53892a-fra.php.

18
INESSS | Medical Protocol - Diabetes
Health Canada. ACTOS (chlorhydrate de pioglitazone) - Association potentielle avec le cancer de la vessie - Pour les professionnels de la santé [website]. Ottawa, ON: Health Canada; 2012. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2012/15854a-fra.php.
Health Canada. Santé Canada examine le lien possible entre le médicament antidiabétique pioglitazone (ACTOS) et le risque de
cancer de la vessie [website]. Ottawa, ON: Health Canada; 2011. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2011/13617a-fra.php.
Health Canada. État des médicaments contenant de la rosiglitazone au Canada (AVANDIA, AVANDAMET et AVANDARYL) [website].
Ottawa, ON: Health Canada; 2010. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2010/13407a-fra.php.
Health Canada. AVANDIA, AVANDAMET et AVANDARYL - Nouvelles restrictions importantes à l’emploi de produits contenant de la
rosiglitazone en raison de renseignements sur des problèmes cardiaques - Pour le public [website]. Ottawa, ON: Health Canada; 2010. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2010/16117a-fra.php.
Health Canada. Archivé – Mise à jour de Santé Canada sur l’innocuité de l’antidiabétique « LANTUS » (insuline glargine) [website].
Ottawa, ON: Health Canada; 2009. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2009/13315a-fra.php.
Health Canada. Archivé – Mise à jour de l’étiquetage du médicament antidiabétique ACTOS et risque d’insuffisance cardiaque
[website]. Ottawa, ON: Health Canada; 2008. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2008/13269a-fra.php.
Health Canada. Pour les professionnels de la santé - Renseignements importants en matière d’innocuité concernant les produits
contenant de la rosiglitazone : AVANDIA, AVANDAMET et AVANDARYL [website]. Ottawa, ON: Health Canada; 2007. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2007/14439a-fra.php.
Health Canada. Pour les professionnels de la santé - Association entre le traitement à long terme du diabète de type 2 par les
comprimés d’ACTOS (chlorhydrate de pioglitazone) et les fractures chez les femmes [website]. Ottawa, ON: Health Canada; 2007. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2007/14436a-fra.php.
Health Canada. Archivé – Innocuité cardiaque concernant AVANDIA (maléate de rosiglitazone) - Pour les professionnels de la santé
[website]. Ottawa, ON׃ Health Canada; 2007. Available at׃ http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2007/14440a-fra.php.
Health Canada. Archivé – Nouvelles restrictions concernant l’emploi des produits contenant de la rosiglitazone en raison de
préoccupations en matière d’innocuité cardiaque (AVANDIA, AVANDAMET et AVANDARYL) - Pour le public [website]. Ottawa, ON: Health Canada; 2007. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2007/13996a-fra.php.
Health Canada. Renseignements importants en matière d'innocuité approuvés par Santé Canada concernant AVANDAMET,
AVANDIA, COREG, PAXIL, PAXIL CR et RELAFEN – GlaxoSmithKline Inc. - Pour les professionnels de la santé [website]. Ottawa, ON: Health Canada; 2005. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2005/14331a-fra.php.
Health Canada. Association d'AVANDIA (rosiglitazone) et d'AVANDAMET (rosiglitazone/metformine) avec l’apparition ou
l’exacerbation d’un oedème maculaire - Pour les professionnels de la santé [website]. Ottawa, ON: Health Canada; 2005. Available at: http://www.canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2005/14308a-fra.php.
Health Canada. Archivé – Renseignements importants concernant l’innocuité de repaglinide (GlucoNorm®) [website]. Ottawa, ON:
Health Canada; 2003. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2003/14231a-fra.php. Health Canada. Archivé – Renseignements importants concernant l’innocuité en case d’utilisation concomitante de matériels
médicaux - Thrombose subaiguë sur endoprothèse coronaire (stent) CYPHERMC - Cordis Corporation [website]. Ottawa, ON: Health Canada; 2003. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2003/14230a-fra.php.

19
Medical Protocol - Diabetes | INESSS
Health Canada. Archivé – Mise en garde importante sur un médicament - ACTOS (pioglitazone hydrochloride) - Lilly [website].
Ottawa, ON: Health Canada; 2001. Available at׃ http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2001/14376a-fra.php.
Health Canada. Archivé – Information importante sur l'innocuité d'AVANDIA® (maléate de rosiglitazone) [website]. Ottawa, ON:
Health Canada; 2001. Available at: http://canadiensensante.gc.ca/recall-alert-rappel-avis/hc-sc/2001/14420a-fra.php. Scottish Intercollegiate Guidelines Network (SIGN). Management of diabetes. Edinburgh, Scotland: SIGN; 2013. Available at:
http://www.sign.ac.uk/pdf/sign116.pdf.