Embed Size (px)
Citation preview

1
Medical Microbiology Review
Rita Heuertz, PhD, MT(ASCP)
Saint Louis University
Objectives
1. Review clinical laboratory knowledge base relevant to Microbiology.
2. Link disease conditions with specific microbiologic agents.
3. Discuss specific strategies for identification of different microbiologic
agents.
Major Disease-Producing Microbes Encountered in
Major Organ Systems
Location, Location, Location:
As Important in Microbiology
as it is in Real Estate
2
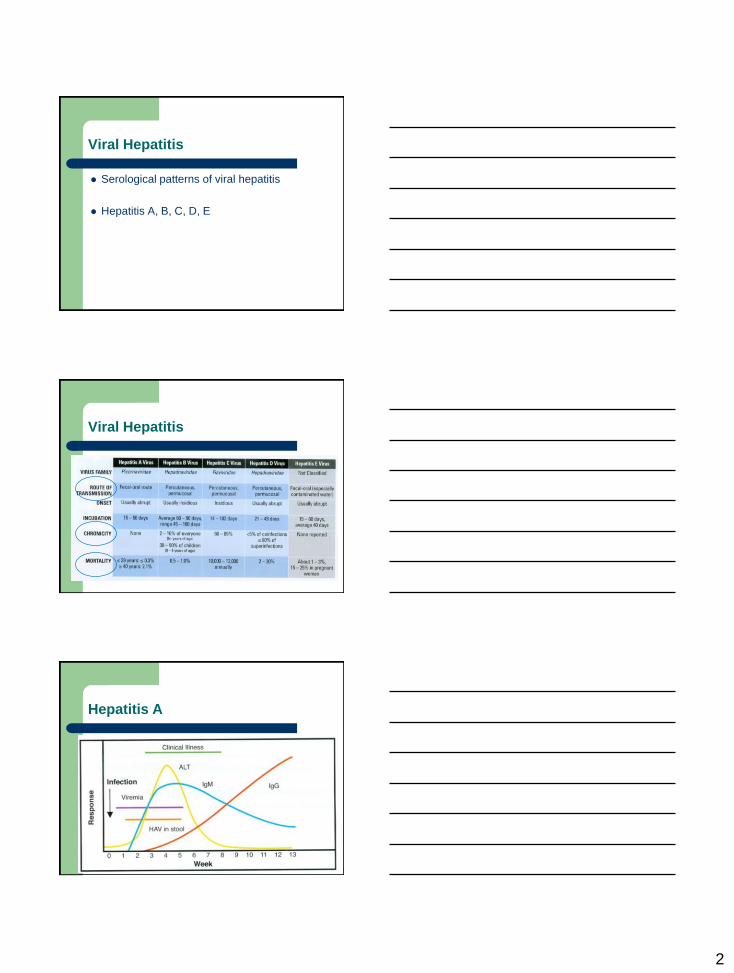
Viral Hepatitis
Serological patterns of viral hepatitis
Hepatitis A, B, C, D, E
Viral Hepatitis
Hepatitis A

3
Hepatitis B
CORE WINDOW
REMEMBER: Not everyone spends the same amount of time in each of these stages during disease progression.
Hepatitis B
Positive Diagnosis for Hepatitis B – HBsAg – Positive
– anti-HBc, IgM – Positive
CORE WINDOW: period of time patient may be HBV positive yet appear negative
Follow-Up Indicated: Monitoring Panel – HBsAg – persistence leads to chronic HBV infection
– HBeAg – determines relative infectivity
– Anti-HBe – seroconversion from HBeAg to anti-HBe usually indicates progression towards disease resolution
– Anti-HBs – seroconversion from HBsAg to anti-HBs positivity indicates resolution of disease and establishment of immunity
Progression to Chronic HBV
NOTE: ABSENCE OF ANTI-HBs

4
Hepatitis C with Progression to Chronic HCV
Acute HCV with Recovery
• anti-HCV plateau • no HCV RNA
• no ↑ ALT
Hepatitis D (requires HBsAg synthesis)
HDV superinfection of HBV
carrier
HDV coinfection with HBV
HBsAg pos: HDV also pos
HBsAg pos: HDV pos later
Hepatitis E

5
Respiratory – Pulmonary
Pharyngitis – Streptococcus pyogenes (GPC)
Otitis media – Streptococcus pneumoniae (GPC)
– Hemophilus influenzae (GNR)
Epiglottitis – Hemophilus influenzae
Pertussis (whooping cough)
– Bordetella pertussis (GNR)
Bronchitis, bronchiolitis – Mycoplasma pneumoniae
– Viruses
Diphtheria – Corynebacterium diphtheriae (GPR)
Thrush – Candida albicans (yeast)
Pneumonia – Hemophilus influenzae, type b (GNR)
– Streptococcus pneumoniae (GPC)
– Mycoplasma pneumoniae
– Klebsiella pneumoniae (GNR)
– Staphylococcus aureus/MRSA (GPC)
Tuberculosis – Mycobacterium tuberculosis
Emerging viral infections – Avian flu (H5N1)
– Novel flu (H1N1)
– SARS
Staphylococcus aureus (MRSA)
S. aureus colonizes anterior nares in 30% of population – pneumonia
Streptococcus pyogenes (Group A)
Beta hemolytic, bacitracin sensitive
Causes
– Pharyngitis
– Noninfectious sequelae (complications)
Post-streptococcal glomerulonephritis
Rheumatic fever

6
S. pyogenes (Group A) Sequelae
Pathologic processes of group A strep can extend
to the heart. Scarring and deformation change
capacity of valves to close and shunt blood
properly. A. Normal valves viewed from above. B.
Inset reveals scar tissue on damaged mitral valve.
Post-streptococcal glomerulonephritis Rheumatic fever
Streptococcus pneumoniae
Causes pneumonia (Gram positive cocci)
Optochin sensitive
Klebsiella pneumoniae
Causes pneumonia (Gram negative rod)
Colony morphology Biochemical Testing
IMViC - - + +. Lys -. Nonmotile.
Capsular morphology on BAP
GNR with capsule

7
Mycoplasma pneumoniae
Causes primary atypical
pneumonia: “walking
pneumonia” – Nonproductive cough, fever,
malaise, headache, lobar
pneumonia by chest X-ray
Gram negative pleomorphic
bacteria with no cell wall –
hard to stain
Fried egg appearance in
culture
Self-limiting but resolves
with tetracycline or
erythromycin
Hemophilus influenzae
Causes
epiglottitis
flap of cartilage at root of
tongue which is depressed
during swallowing to cover
opening of the windpipe
Hemophilus ID
Hemophilus Growth: X Growth: V Growth: XV Hemolysis
influenzae Neg Neg Pos Neg
parainfluenzae Neg Pos Pos Neg
hemolyticus Neg Neg Pos Pos
parahemolyticus Neg Pos Pos Pos
Growth around
XV only

8
Bordetella pertussis
Causes whooping cough
Bordet-Gengou agar
Erythromycin is drug of choice
DTP (diptheria, tetanus,
pertussis)
– Average duration of
protective antibody titers
following vaccination is 12
years.
Corynebacterium diptheriaeae
Elek in vitro toxigenicity test
2. Unknown (toxigenic)
4. Unknown (nontoxigenic)
Arch of
Identity
Positive Immunodiffusion Result
Causes diphtheria
Corynebacterium diptheriaeae
Gram stain Pseudomembrane

9
Mycobacterium tuberculosis
LABORATORY DIAGNOSIS staining as AFB
– serpentine cording – is indicator of virulence for M. tuberculosis
culture
– most common patient sample is sputum
– large amounts of bacterial flora, mucus need to be removed to prevent overgrowth, contamination of culture: digestion, decontamination done
digestion: uses liquefying, mucolytic agent (N-acetyl-L-cysteine: NALC)
decontamination: uses NaOH (2-4%)
concentration: specimen concentrated is by centrifugation
concentrate is stained, cultured
– aerobic – requires CO2, 35-37C – slow grower (2-6 weeks)
– media
Lowenstein Jensen (LJ), Middlebrook 7H10 or 7H11
Broth containing casein, albumin, 14C-palmitic acid for radiometric detection (e.g., Bactec machines)
Mycobacterium tuberculosis
AFB stain Colony morphology
Causes
tuberculosis
Mycobacterium tuberculosis
Biochemical ID Tubed Media
Niacin Pos
Nitrate Pos
Catalase Pos

10
Candida albicans
Gram stain Colony morphology
Causes thrush
germ tube test: positive
Add yeast colony to
serum (0.5 ml): incubate
2-3h at 37C.
Respiratory Viruses Clinical Signs Virus Lab Test
Common cold * Rhinovirus, coronavirus Virus culture
Pharyngitis * Adenovirus,
parainfluenzavirus 1-4
influenzavirus A & B
Virus culture
Gingivostomatitis,
pharyngitis, tonsillitis
Herpes Simplex Virus HSV IgM/IgG
Virus culture
Infectious mononucleosis Epstein Barr Virus
Cytomegalovirus
Human Herpesvirus 6
EBV serology
CMV IgM/IgG, culture
HHV6 IgM/IgG
Pharyngitis/Koplik’s spots Measles Measles IgM/IgG
Herpangina/hand foot and
mouth disease
Coxsackie A Virus culture
Primary HIV infection HIV HIV serology, culture, PCR
* = self-limiting, lab testing not routinely performed
Epstein Barr Virus – Infectious Mono
Epstein Barr Virus – infectious mononucleosis (in the USA), nasopharyngeal cancer, Burkitt’s
lymphoma, Hodgkin’s lymphoma
ACUTE and CONVALESCENT serum samples show Ab titer increase and decrease with
disease progression, such as for Epstein Barr Virus Viral Capsid Antigen (EBV VCA)
ACUTE CONVALESCENT

11
Skin, Tissue
Wounds, Lesions
Skin, Tissue, Wounds, Lesions
Dermatitis, dermaphyte infection – Superficial candidiasis (yeast), ringworm (Tinea corporis), athlete’s foot (Tinea pedis), jock itch
(Tinea cruris)
Rashes – Measles (virus), Scarlet fever (Group A Strep), Toxic shock syndrome (S. aureus), 2ndary syphilis
(treponeme bacteria), Lyme disease (spirochete)
Papules – Warts (virus), scabies (parasitic mite), cellulitis (S. aureus), fasciitis (Group A Strep), myonecrosis
(C. perfringens)
Vesicles – Herpes (virus), chickenpox (varicella virus), scalded skin syndrome (Group A Strep, S. aureus)
Pustules – Impetigo (S. aureus), acne (Propionibacterium), furuncles (S. aureus), carbuncles (S. aureus)
Skin, Tissue, Wounds, Lesions
Burns (P. aeruginosa)
Petechiae, purpura – Rocky Mountain Spotted Fever (rickettsia), meningococcemia (N. meningitidis), plague (Y. pestis),
dengue (virus) (p.826 picture)
Ulcers – Syphilis (treponeme bacteria), herpes (virus), chanchroid (H. ducreyi), impetigo (S. aureus),
histoplasmosis (fungus), anthrax (GPR bacteria), tularemia (GNR bacteria)
Bones – S. aureus osteomyelitis

12
Most Common Primary Pyodermas
Tinea infections (fungus)
Ringworm Athlete’s Foot Jock Itch
Tinea corporis Tinea cruris Tinea pedis
Staphylococcus aureus (superficial)
Scalded Skin Syndrome
Impetigo
Furuncle
On Hand
Carbuncle
On Neck

13
Staphylococcal Osteomyelitis (with ulna rupture)
Bone aspirate
has WBC and GPC (cl)
Bacteria spread through circulation from other site of infection, enter artery and lodge in small vessels of the bone.
Bacterial growth causes inflammation and damage that manifests as edema (swelling), necrosis (cell death).
Staph aureus and/or Strep pyogenes
Cellulitis
Impetigo
Streptococcus pyogenes
Scarlet fever Strep throat Erysipelas
Scarlet Fever Rash
14
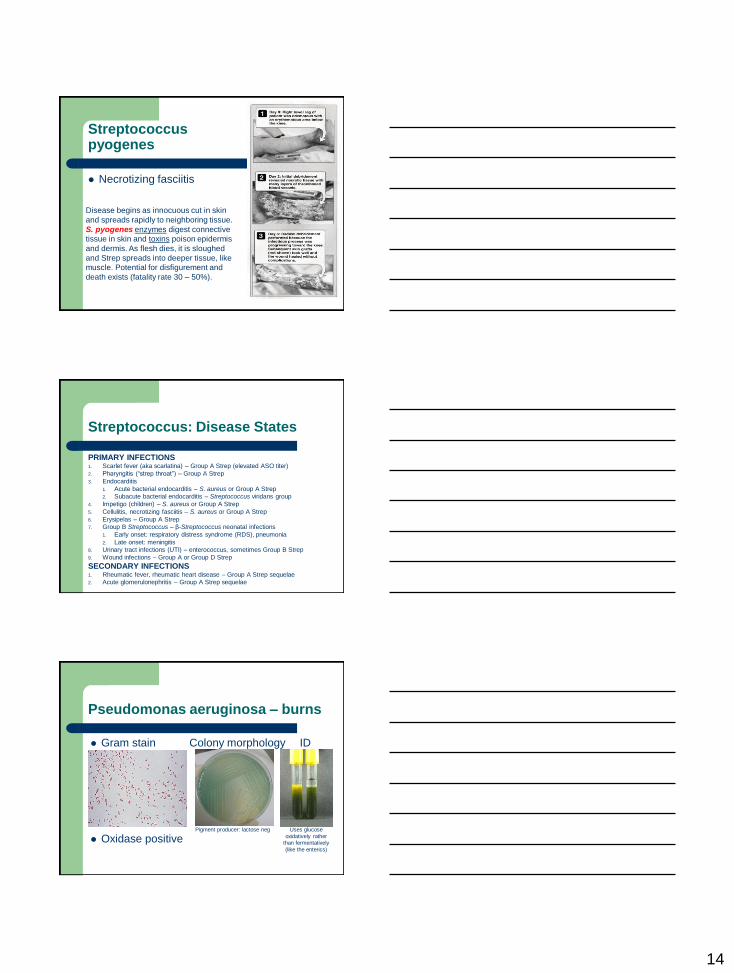
Streptococcus pyogenes
Necrotizing fasciitis
Disease begins as innocuous cut in skin
and spreads rapidly to neighboring tissue.
S. pyogenes enzymes digest connective
tissue in skin and toxins poison epidermis
and dermis. As flesh dies, it is sloughed
and Strep spreads into deeper tissue, like
muscle. Potential for disfigurement and
death exists (fatality rate 30 – 50%).
Streptococcus: Disease States
PRIMARY INFECTIONS 1. Scarlet fever (aka scarlatina) – Group A Strep (elevated ASO titer)
2. Pharyngitis (“strep throat”) – Group A Strep
3. Endocarditis
1. Acute bacterial endocarditis – S. aureus or Group A Strep
2. Subacute bacterial endocarditis – Streptococcus viridans group
4. Impetigo (children) – S. aureus or Group A Strep
5. Cellulitis, necrotizing fasciitis – S. aureus or Group A Strep
6. Erysipelas – Group A Strep
7. Group B Streptococcus – β-Streptococcus neonatal infections
1. Early onset: respiratory distress syndrome (RDS), pneumonia
2. Late onset: meningitis
8. Urinary tract infections (UTI) – enterococcus, sometimes Group B Strep
9. Wound infections – Group A or Group D Strep
SECONDARY INFECTIONS 1. Rheumatic fever, rheumatic heart disease – Group A Strep sequelae
2. Acute glomerulonephritis – Group A Strep sequelae
Pseudomonas aeruginosa – burns
Gram stain Colony morphology ID
Oxidase positive Uses glucose
oxidatively rather than fermentatively
(like the enterics)
Pigment producer: lactose neg

15
Bacillus anthracis (anthrax)
Gastrointestinal – spore ingestion
Inhalational – woolsorter’s disease
– respiratory distress
Cutaneous – black eschar
– Most commonly encountered
form of anthrax
Bacteroides fragilis (anaerobic wound infections)
Gram stain Colony morphology
Clostridium perfringens (anaerobic infection)
Gram stain Colony morphology
Gas Gangrene

16
Clostridium tetani (anaerobic infection)
Gram stain Uncontrollable Muscle Contraction
Tetanus
Gastrointestinal Tract
Gastrointestinal Tract
Stomach Ulcers – Helicobacter pylori
– Perform urease-CLOtest on gastric biopsy
Diarrhea – food/water borne
– Mediated by toxin
Enterotoxigenic E. coli, V. cholerae, C. perfringens, B. cereus, C. difficile,
S. aureus , C. botulinum
– Mediated by infection and mucosal surface invasion
Salmonella spp, Shigella, Campylobacter, Entamoeba histolytica,
Enterohemorrhagic E. coli (e.g., strain O157:H7)
– Mediated by infection and full bowel thickness invasion
Salmonella typhi, Yersinia enteocolitica
– Noninvasive
Giardia lamblia, rotavirus

17
Helicobacter pylori
Causes stomach ulcers
Ingestion of urea with labelled carbon labelled carbon in breath H. pylori urease
Food Poisoning: Food Infection
Food Poisoning: ingestion of microbe-produced preformed toxins
Food Infection: ingestion of microbes that grow/replicate, cause infection
Food Poisoning (Toxicity)
Staph aureus Salmonella E. coli O157:H7 Shigella
Infection/Toxin Toxin Infection Toxin Infection
Incubation Period
2-8 hours 18 hours 2-8 hours
2-3 days
Fever Absent Present Absent Present
Symptoms Vomiting, diarrhea, headache
Diarrhea, abdominal pain
Bloody diarrhea Bloody diarrhea
Abdominal cramps
Symptom Duration
24-48 hours 2-5 days 24-48 hours
2-7 days

18
Common Pathogens Causing Diarrhea
Clostridium botulinum (anaerobe)
Canned Food Neurological Disease of Toxin
BOTULISM
Clostridium botulinum Toxin Blockade of Neural Transmitter

19
Salmonella (GNR)
Typhoid Mary (S. typhi: typhoid fever)
– Identification of carrier status
(asymptomatic yet able to transmit
to others)
Preventatives
– Food handling
Refrigeration, proper cooking
No human vaccine is 100% effective
– Vivotif Berna
– Typhim Vi
Salmonella typhi: IMViC - + - + Lac - H2S + Motile
Shigella (GNR)
Gram stain Colony morphology
Causes
bacillary
dysentery
Shigella: IMViC -/+ + - - Lac - H2S - Nonmotile
Biochemical Rxns of Kligler Iron Agar (KIA) Slants: Primarily Useful for Enterobacteriaceae
NOTE: Triple Sugar Iron Agar (TSI) slants are read in similar manner.
# Slant
(lactose)
Base
(glucose)
Gas?
H2S?
Biochem
Result
1 Alkaline (K) Alkaline (K) Gas? no
H2S? no
All neg:
control
2 Alkaline (K) Alkaline (K) Gas? no
H2S? No
K/K
3 Alkaline (K) Acid (A) Gas? no
H2S? no
K/A
4 Alkaline (K) Acid (A) Gas? no
H2S? yes
K/A H2S
5 Acid (A) Acid (A) Gas? yes
H2S? no
A/A gas
6 Acid (A) Acid (A) Gas? no
H2S? no
A/A H2S
1 3 2 4 5 6

20
Carbohydrate Fermentation Tests
TSI agar reactions of
Enterobacteriaceae
(tube slant/base results after
18-24 hours incubation)
Tube 1: A/A gas (acid/acid with gas)
Tube 2: A/A H2S
Tube 3: K/A (alkaline/acid)
Tube 4: K/A, H2S, gas
Tube 5: K/K (alkaline/alkaline)
KIA agar reactions of Enterobacteriaceae (tube slant/base results after 18-24
hours incubation).
Left A: A/A gas (acid/acid with gas) Right A: K/A H2S
Left B: K/A (alkaline slant lactose/acid glucose) Right B: K/A, H2S
Left C: K/K (alkaline/alkaline) Right C: K/K (uninoculated)
Common KIA Results
5% are lac neg & pathogenic

21
MOTILITY: the motility test medium has agar concentrations of 0.4% which is
semi-solid thereby allowing free spread of the organism. A single stab into the
medium is made. After overnight incubation, movement away from the stab line
or hazy appearance throughout the medium indicates a motile organism.
Motility Results
IMViC Reactions for Enterobacteriaceae Family
Indole: Negative
Methyl Red: Negative
Voges Proskauer : Positive
Citrate: Positive
K. pneumoniae
Indole: Positive
Methyl Red: Positive
Voges Proskauer: Negative
Citrate: Negative
E. coli
Campylobacter (GNR)
Gram stain Colony morphology
Erythromycin: preferred treatment
Is a food-borne infection (has been associated with undercooked poultry)
Causes fever, cramps, bloody diarrhea (is a self-limiting disease)
22
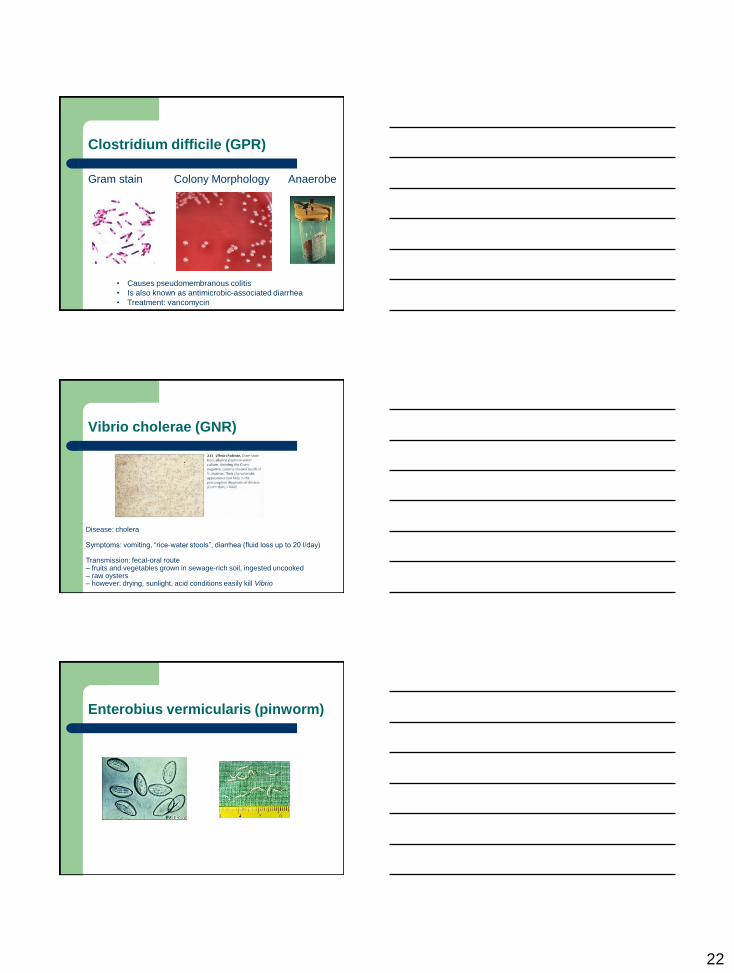
Clostridium difficile (GPR)
Gram stain Colony Morphology Anaerobe
• Causes pseudomembranous colitis
• Is also known as antimicrobic-associated diarrhea
• Treatment: vancomycin
Vibrio cholerae (GNR)
Disease: cholera Symptoms: vomiting, “rice-water stools”, diarrhea (fluid loss up to 20 l/day) Transmission: fecal-oral route – fruits and vegetables grown in sewage-rich soil, ingested uncooked – raw oysters – however: drying, sunlight, acid conditions easily kill Vibrio
Enterobius vermicularis (pinworm)

23
Giardia lamblia (parasite)
Microscopy
Cryptosporidium (parasite)
Single cell sporozoa parasite responsible for
contaminated water (e.g., Milwaukee water
outbreak of 1993)
Ascaris lumbricoides (roundworm)

24
Central Nervous System
Central Nervous System
Bacterial meningitis
– Group B Streptococcus, Hemophilus influenzae (type b), Streptococcus
pneumoniae, Listeria monocytogenes, Neisseria meningitidis, T. pallidum
(syphilis spirochete)
Mycobacterial meningitis
– M. tuberculosis (HIV is a risk factor)
Fungal meningitis
– Cryptococcus neoformans, Coccidioides immitis
Parasitic meningitis
– Naegleria fowleri
Viral meningitis
– Enteroviruses like poliovirus, coxsackieviruses (A and B), echoviruses
Bacteria that cause CNS infections are highly susceptible to cold
temperatures. Do not put CNS samples in the refrigerator or on ice.
Group B Streptococcus
Gram stain Colony morphology
Risk population for meningitis: newborn infants
birthed through a canal infected with Grp B Strep
Catalase negative

25
Listeria monocytogenes
LABORATORY DIAGNOSIS
At risk populations: pregnant women, newborn
infants (sepsis, meningitis), immunocompromised,
elderly
Gram positive rod that resembles lancet shape of
Streptococcus
Growth is with beta hemolysis (resembles Strep)
Catalase positive
Exhibits “umbrella” pattern of motility at room temp
(23-25oC) but not at human body temp (35-37oC)
Capable of growth at 4oC
Grows at high salt concentrations
23oC 37oC Listeriosis is leading
cause of fatal food-
borne infections in USA: heat ready-to-eat foods
to steaming hot before
ingestion
umbrella shape motility at RT
Neisseria meningitidis
Gram stain Culture & oxidase result
Petechial rash commonly develops with meningococcemia (invasion of bloodstream)
Waterhouse-Friderichsen Syndrome – adrenal gland hemorrhage
Risk population for meningitis: newborns-toddlers
ID of Neisseria Pathogens
Lab ID is by cystine trypticase agar (CTA)
sugar utilization method
Organism Glucose Maltose Sucrose Lactose
N. gonorrhoeae Pos Neg Neg Neg
N. meningitidis Pos Pos Neg Neg
N. lactamica Pos Pos Neg Pos
M. catarrhalis Neg Neg Neg Neg

26
Cryptococcus neoformans
ID of cryptococcal antigen in CSF
India Ink preparation of CSF for yeast
Bacteremia
Septicemia
Bacteremia, Septicemia
Bacteremia – usually transient periods of microbes in bloodstream (e.g., mouth flora after
vigorous dental flossing)
Septicemia – Common causes in 1960-1970: GNR like E. coli, P. aeruginosa
– Common causes in 1980-1990: GPC like S. aureus, coagulase negative
staphylococci, enterococcus
– 21st century Emerging Resistant Microbes:
Coagulase negative staphylococcus (31%)
S. aureus (20% with 40% of these being MRSA)
enterococcus (9%)
C. albicans (9%)
E. coli (6%)
Klebsiella (5%)
P. aeruginosa (4%) – recent hospital-based survey

27
Blood Parasite – Plasmodium
Plasmodium in RBC – Malaria
Urinary Tract
Causes of UTI E. coli is in this family

28
E. coli
Leading cause of all urinary track infection (UTI)
IMViC + + - -
E. coli tends to be susceptible to most antimicrobics
Leading Cause of Gram Negative UTI
Enterococcus
Gram stain Colony morphology
Leading Cause of Gram Positive UTI
Genital Tract
Sexually Transmitted Diseases (STD)

29
STD and Causative Agents
Neisseria gonorrhoeae (GC)
Gram stain Colony Morphology
JEMBEC system with
Thayer Martin agar for GC
Treponema pallidum (syphilis)
Tissue stain Dark-field microscopy
spirochetes
spirochetes
spirochetes

30
Trichomonas vaginalis (parasite)
Parasite – single cell flagellate
Gardernella vaginalis – Clue cells
Describe important
technical procedures
and their application

31
Gram Stain for Bacteria
IMViC (and other) Results
Escherichia coli + + - - lac - (usually) lys +
Edwardsiella tarda + + - - lac - H2S + lys +
Klebsiella pneumoniae - - + + lac + capsule lys - Nonmotile
(K. oxytoca is indole +)
Salmonella typhi - + - + lac - H2S + lys + Motile
Shigella -/+ + - - lac - H2S - lys - Nonmotile
Yersinia enterocolitica V + - - lac - H2S - lys –
Motile (25oC), Nonmotile(37oC)
Citrobacter freundii - + - + lac +/V H2S + lys -
Citrobacter diversus + + - + lac V HxS - lys -
Enterobacter aerogenes V - + + lac + orn + lys + Motile
Proteus vulgaris + + - - lac - H2S + lys - Motile
Proteus spp lac - phe + lys -
Antimicrobic Susceptibility by Disk Diffusion
E-test: MIC results with ease
of performance of KB test
Kirby-Bauer Susceptibility Test

32
AFB Stain for Mycobacterium
Culture for Mycobacterium
Culture for M. tuberculosis
Cannot culture for M. leprae
KOH Preparation for Fungus/Yeast
KOH destroys mammalian cells: yeast becomes evident

33
KOH Prep for Thrush
Candida albicans (direct
KOH prep of patient swab)
Culture for Fungus/Yeast
Candida albicans – pure culture
Saline Wet Prep for Trichomonas
parasite (Trichomonas vaginalis) from vaginal
secretions

34
Parasite Testing
Wet direct preparation
from fresh stool – for
trophozoites
Stool for parasite set-up
and concentration – for
cysts
Virus Testing
Cell Culture for Virus Infection and/or Growth
Amplification of Virus-Specific DNA:
Polymerase Chain Reaction (PCR) for Virus
Antibody Testing of Patient Serum for Disease
Presence, Progression, Resolution
Cell Culture for Viruses
Viruses, if present, infect the cells and cause
morphological changes to the cells (e.g., lysis)

35
Amplification of Virus DNA (PCR)
EXAMPLE:
HIV gene
PCR for Virus (e.g., H1N1 flu)
Ab Titer for Virus Infection (Acute, Convalescent)
Viremia and antibody kinetics of West Nile virus infection
Detects virus presence, progression, resolution
IgM increases followed by a decrease: IgG then increases and plateaus

36





























