Embed Size (px)
Citation preview

MedicalManagementofObesityinthe
OutpatientSetting:
WhatthePCPNeedstoKnow
JodyDushay,MDMMScAssistantProfessorofMedicine
HarvardMedicalSchool
DivisionofEndocrinology,BILH
COPYRIGHT

Outline/Objectives
• InitialMDconsultationforweightloss
• Guidelinesforthemedicaltreatmentofobesity
• Pharmacotherapyforweightloss– Indications,efficacy,sideeffects
• Beyondthescale:Additional importantlifestylechangesforimprovinghealthCO
PYRIGHT

Disclosures
• None
COPYRIGHT

Why(andhow)doweeat?
• Whatregulatesourappetite?
• Ourfoodchoices?
• Whenweeat?
• Howmuchweeat?
• Whenwestopeating?COPYRIGHT

Weeatforsurvivalandpleasure
• Homeostatic/survival
(metabolic)
• Hedonic/pleasure
(emotional)
COPYRIGHT

Homeostatic:eattosurvive
• Hunger(centraland
peripheralsignals)
• Seekfoodsource
• Hormonesignalsfromthe
GIsystemtothebrainthat
energystoresincreased
• Brainreleasessatietysignals
(neurotransmitters)
• Stopeating
Hedonic:eatforpleasure
• +/- hungersignal
• Desireapleasurableactivity
• Foodsource
– Sight,smell,thought
• Eatingisreinforcedby
neuropeptiderelease
– Differentcircuitryfrom
homeostaticdrive
• Ignoresatietysignals
COPYRIGHT

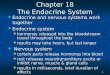
Hhypothalamic nuclei
involved infeeding
HOMEOSTATIC
COPYRIGHT

Itisdifficulttoloseweightand
maintainweightloss!
COPYRIGHT

Metabolicchangesdonotfavor
weightlossormaintenance
• Weightlossisusuallyassociatedwith
decreaseintotalenergyexpenditureoutof
proportiontochanges inleanbodymass
– Thispersistsaslongasreducedweightis
maintained
• Increasedhungeranddecreasedsatietyoccur
afterweightloss
– Increasesecretionofhungerhormonesand
perceptionofhunger
COPYRIGHT

Sumithran NEJM 2011
50 overweight adults, BMI 27-40
10 weeks of very low calorie diet
COPYRIGHT

Sumithran NEJM 2011
Hungerhormonesincreaseandsatiety
hormonesdecreaseafterweightloss
HUNGER
SATIETY
SATIETY
SATIETY
COPYRIGHT

Sumithran NEJM 2011
Hungeranddesiretoeatareincreased
afterweightloss
COPYRIGHT

Howcanwehelpourpatients
improvetheirhealth
andloseweight?
COPYRIGHT

Ourenvironmentisnotconducivewellnessorweightloss
COPYRIGHT

Obesity-FocusedHistory
WeightLossReadiness
• Motivation andsocialsupport
• Psychiatricstatus
• Presenceof stressful lifecircumstances
• Timeconstraints
• Goalsandexpectations
Kushner RF. Circulation. 2012;126:2870-2877.
ReviewofSystems
• Checklist ofobesity-related
complications
• smoking cessation
• medication initiation
• pregnancyormenopause
• lifestressors
• majorlifestyle change
(surgeryà sedentary)
• Extent ofdailyphysicalactivity
• Sleep habits anddifficulties
• Foodpreferences and
frequency/quantity ofmeals
• Psychological assessment
– Mood/anxietydisorders,ADD,PTSD
– Eatingdisorders
LifeEventsandWeightGain DietandActivity
COPYRIGHT

Whatistheroleof
pharmacotherapyinthe
treatmentofobesity?
COPYRIGHT

Whyusepharmacotherapytotreatobesity?
• Obesityisachronicmetabolicandneurobehavioral disease
• Weusemedicationstotreatchronicdiseases– Withoutnearlyasmuchhesitation
• Medicationcanhelp…– Improveadherencetolifestylechange
– Achieveclinicallysignificantweightloss
– Butto“jumpstartweightloss”?– Notsomuch
COPYRIGHT

EndocrineSocietyClinicalPracticeGuidelines
• Patientsunabletosuccessfullyloseandmaintainweightandwhomeetlabelindicationsarecandidatesforweightlossmedication(strongevidence)
• Appropriatetouseapprovedweightlossmedicationovernopharmacologictherapytoamelioratecomorbiditiesandamplifyadherencetobehavioralchange
• BMI≥30,or≥27withcomorbidities
• Lowqualityevidenceforthesecutoffs
• ONLYasadjunctivetreatmenttolifestylechange
Apovian et al, JCEM 2015
COPYRIGHT

Generalguidelinesforallobesitymedications
• Assessefficacyandsafetyeverymonthforfirst3mos,thenatleastevery3mos
• Currentlyavailablemedicationsdonotchangeunderlyingphysiologyofweightregulationinanypermanentway
• Nopermanenteffectonappetite/satiety
– Effectslastonlyaslongasmedicationiscontinued
COPYRIGHT

DrugsfortheTreatmentofObesity
• Phenterminemonotherapy (short term)
• Orlistat
• Lorcaserin
• Phentermine- Topiramate
• Bupropion– Naltrexone
• Liraglutide
COPYRIGHT

Phentermine
DEA = Drug Enforcement Agency; T2D = type 2 diabetes.
Adipex-P prescribing information. Sellersville, PA: Teva Pharmaceuticals.; 2013.
§ 15,30,or37.5mgoncedaily,in
themorning
MechanismofAction
§ Sympathomimeticamine
anorectic
Indications
§ Short-termadjuncttodietand
exerciseinpatientswith
§ Treatment duration≤12weeks
§ BMI≥30kg/m2
§ BMI≥27kg/m2 with≥1weight-
related comorbidity
§ Hypertension
§ T2D
§ Hyperlipidemia
§ DEAScheduleIVControlled
Substance
Dosing
COPYRIGHT

Orlistat
T2D = type 2 diabetes.
Xenical prescribing information. South San Francisco, CA: Genentech USA, Inc.; 2013.
MechanismofAction
§ Reversiblegastrointestinal
lipaseinhibitor
Indications
§ Weightlossandweight
maintenanceinconjunction
withareducedcaloriediet
§ BMI≥30kg/m2
§ BMI≥27kg/m2 with≥1
weight-relatedcomorbidity
§ Hypertension
§ T2D
§ Dyslipidemia
Dosing
§ 120mgTIDwitheachmain
mealcontainingfatCOPYRIGHT

Lorcaserin
DEA = Drug Enforcement Agency; T2D = type 2 diabetes.
Belviq prescribing information. Woodcliff Lake, NJ: Eisai Inc.; 2012.
MechanismofAction
§ Specific5-HT2C(serotonin)
receptoragonist
Indications
§ Adjuncttodietandexercisein
patientswith
§ BMI≥30kg/m2
§ BMI≥27kg/m2 with≥1weight-
related comorbidity
§ Hypertension
§ T2D
§ Dyslipidemia
§ ScheduleIVControlledSubstance
Dosing
§ 10mgtwicedaily
COPYRIGHT

LorcaserinWeightLoss
Bohula et al NEJM 2018
COPYRIGHT

Phentermine/TopiramateER
T2D = type 2 diabetes.
Qsymia prescribing information. Mountain View, CA: Vivus, Inc.; 2012.
MechanismofAction
§ Central noradrenergic effects
§ Phentermine: immediate-release
sympathomimetic
§ Topiramate ER: delayed-release gabanergic
Indications
Dosing
§ Once daily in morning§ Start: phentermine 3.75/topiramate ER
23 mg
§ Usual dose: 7.5/46 mg
§ Maximum dose: 15/92 mg
§ If <3% weight loss after 12
weeks, discontinue or advance to
next dose
§ If <5% weight loss after 12
weeks on maximum dose,
discontinue
§ Schedule IV Controlled Substance
§ Adjunct to diet and exercise in
patients with
§ BMI ≥30 kg/m2
§ BMI ≥27 kg/m2 with ≥1 weight-related comorbidity
§ Hypertension§ T2D§ Dyslipidemia
COPYRIGHT

CONQUER Trial
WeightLosswithPhentermine/Topiramate in
ObeseAdults
29
Data are shown with mean (95% CI).
Phen/TPM ER = phentermine/topiramate extended release.
Garvey WT, et al. Am J Clin Nutr. 2012;95(2):297-308.
SEQUEL Extension
SEQUEL Study
(CompleterAnalysis)
Placebo Phen/TPM ER 7.5/46 Phen/TPM ER 15/92
LS
mean
weig
ht
loss (
%)
-2
-4
-6
-8
-10
-12
-14
-160 12 20 92
0
Weeks
28 36 44 52 60 68 76 84 100 108 LOCF
Placebo n: 227 227 227 208 197 227
Phen/TPM 7.5/46 n: 153 152 153 137 129 153
Phen/TPM 15/92 n: 295 295 295 268 248 295
COPYRIGHT

Naltrexone/BupropionSR
32T2D = type 2 diabetes.
Contrave prescribing information. Deerfield, IL: Takeda Pharmaceuticals America, Inc.; 2014.
MechanismofAction
§ Naltrexone:opioidreceptor
antagonist
§ Bupropion:norepinephrine-
dopaminereuptakeinhibitor
Indications
§ Adjuncttodietandexercisein
patientswith
§ BMI≥30kg/m2
§ BMI≥27kg/m2 with≥1
weight-relatedcomorbidity
§ Hypertension
§ T2D
§ Dyslipidemia
§ Other
Dosing
§ Eachtabletis8mg
naltrexone/90mgbupropion
§ Titrateupto2tabletsbid
COPYRIGHT

Naltrexone-Bupropion:WeightLoss
Greenway FL et al. Lancet 2010; 376:696-605
COPYRIGHT

DIYislessexpensive
• Phentermineavailableas8mgtablet
• Topiramateavailable25,50,100mg
• Startwith4mgphentermine,25mg
topiramate
• Canalsoprescribebupropionandnaltrexone
independently
– Contrave:360mgbuproprion,32mgnaltrexone
(8mgnaltrexone/90mgbuproprionpertablet)
COPYRIGHT

Liraglutide
T2D = type 2 diabetes.
Saxenda prescribing information. Plainsboro, NJ: NovoNordisk Inc.
MechanismofAction
§ GLP-1receptoragonist
Indications
§ Adjuncttodietandexercisein
patientswith
§ BMI≥30kg/m2
§ BMI≥27kg/m2with≥1
weight-related
comorbidity
§ Hypertension
§ T2D
§ Dyslipidemia
Dosing
§ Titratefromto1.8to3mgonce
dailysubcutaneousinjectionCOPYRIGHT

LiraglutideandBodyWeightOver3Years
37
All arms included lifestyle intervention: −500 kcal/day hypocaloric diet + 150 min/week increased physical activity.
Full analysis set, fasting visit data only. Line graphs are observed means ( SE). Points (sqaure, triangle) are observed means
with last observation carried forward (LOCF).
Fujioka K, et al. ENDO 2016, April 1-4, 2016; Abstract 24365.
778
320
DW
eig
ht
(%)
-2.1
-5.2
1467 1295 1223 1161 1100 1030 971 885 849 830 780805911
734 635 576 544 508 465 436 375 365 354 327336399
n=
n=
747
322
-2.7
-7.1
Week
-3.5
-9.2
-3.4
-8.5
Off-drug follow-up
Liraglutide 3.0 mg Placebo
COPYRIGHT

Orlistat1,2 Lorcaserin3-5Phentermine/
topiramate6-8Naltrexone/
bupropion9,10Liraglutide
3mg11,12
Study(no.weeks),
no.ITTpatientsin
treatmentgroup
Davidson
etal(52),
n=657
XENDOS
(208),
n=1640
BLOSSOM
(52),
n=1602
BLOOM
(52),
n=1538
BLOOM-
DM(52),
n=256
EQUIP
(56),
n=512
CONQUER
(56),
n=995
SEQUEL
(108),
n=295
CORI
(56),
n=583
CORII
(56),
n=1001
SCALE-
Main(56),
n=212
SCALE
(56),
n=2487
Baselineweight(kg) 100.7 110.4 100.1 100.4 106.0 115.2 103.0 101.9 99.7 100.3 100.4 106.2
ComparisonofWeight-LossMedications
ApprovedforLong-TermUse
40
Placebo-SubtractedChangesfromBaseline,HighestApprovedDose
(NotHead-to-HeadTrials)
DW
eig
ht
(%)
ITT = intent to treat.
1. Davidson MH, et al. JAMA. 1999;281:235-242. 2. Torgerson JS, et al. Diabetes Care. 2004;27:155-161. 3. Fidler MC, et al. J Clin
Endocrinol Metab. 2011;96:3067-3077. 4. Smith SR, et al. N Engl J Med. 2010;363:245-256. 5. O’Neil PM, et al. Obesity.
2012;20:1426-1436. 6. Allison DB, et al. Obesity (Silver Spring). 2012;20:330-342. 7. Gadde KM, et al. Lancet. 2011;377:1341-1352.
8. Garvey WT, et al. Am J Clin Nutr. 2012;95(2):297-308. 9. Greenway FL, et al. Lancet. 2010;376:595-605. 10. Apovian CM, et al.
Obesity (Silver Spring). 2013;21:935–943. 11. Wadden TA, et al. Int J Obes (Lond). 2013;37:1443-1451. 12. Pi-Sunyer X, et al. N Engl
J Med. 2015;373:11-22.
COPYRIGHT

Week
DW
eig
ht
(%)
Week
DW
eig
ht
(%)
Yancy WS, et al. Arch Intern Med. 2010;170:136-145.
OrlistatPlusLow-FatDietLow-CarbohydrateKetogenicDiet
HeterogeneityofTreatmentEffect
forWeightLoss
41
COPYRIGHT

Heterogeneity isalsotruefor
pharmacotherapy
Earlyweightlosspredicts
longtermweightloss
COPYRIGHT

ClinicalCase
• 53yofemale,BMI36
– 50+lbweightgainwithlastpregnancy,lost10lbs
postpartum
– Steadyweightgainsincemenopause
• PMHnotableforIBS,chronicbloating,
depression,andelevatedcholesterol
– Hasbeenonbupropioninthepast,noweightloss
• BP118/60,HR70s
• Medications:MVI,SSRI
COPYRIGHT

ClinicalCase
• Startedpharmacotherapy forweightloss
193
167 Weight (lbs)
COPYRIGHT

ClinicalCase
• 44yomale,BMI33
• Medicalhistory:HTN,
OSA,HIV+,depression,
compulsiveeating,
voraciousappetite
• Medications:ART,SSRI
COPYRIGHT

ClinicalCase
• 51yomale,BMI46
• HistoryofGraves’ disease,nowinremission
• Impairedglucosetolerance(A1c5.8%),NAFLD
withNASscore5/8,moderatefibrosis,
elevatedcholesterol
• Nighttimeeatingisamajorproblem
• Travelsforwork,eatsoutoften
• Nomedications
COPYRIGHT

ClinicalCase
Weight, lbs
COPYRIGHT

ClinicalCase
• 41yo female
• T2DM,NAFLD,PCOS,ADD,anxiety
• Medications:metformin, spironolactone
– Prefersasfewmedicationsaspossible
COPYRIGHT

Weight, lbs
241 lbs
190 lbs
ClinicalCase
COPYRIGHT

Summary
• Manyfactorscontrolappetiteandfoodintake
– Redundantsystemsprotectourbodyweight/body
fatsetpoint
• Obesityisachronicdiseaseresultingfrom
dysregulationofenergyhomeostasis
• Attentiontolifestyle isthecornerstoneof
obesity treatment
• Thereisaroleforpharmacotherapy totreat
obesity
– Considerrisk/benefitandpatientpreference
COPYRIGHT

Myapproach
• Detailedhistoryincludingweight,diet,meds
• Secondarycausesforobesity
– Usuallyunrevealing,don’tgooverboard
• Riskstratify
• Patient’sconcern,goals,levelofmotivation
• Patient’sviewon
– meds/nomeds
– newmeds/oldmeds
– Pills/injections
COPYRIGHT

Myapproach
• Remember contraindications
• Orderlabsyouneedatbaseline
– Repeatdependingonmedication
• Planwhenwillyoufollowupandhow
– Thisisahightouchundertaking!
– 3moswon’tdothejob
• Remember taperoffphentermine/topiramate
• NOmedications approvedwithout lifestyle
change
COPYRIGHT

COPYRIGHT