Embed Size (px)
Citation preview

MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA
LUIS H. TELLO MV, MS, DVM, COS Portland Hospital “Classic”
International Medical Advisor Banfield Pet Hospital
ABDOMINAL TRAUMA
• 70-80% of multiple trauma patients
• 55% of motor vehicle accidents
• Undiagnosed in human trauma patients
• 40% of them are asymptomatic
• The most frequent are • BLUNT TRAUMA
• PENETRATING TRAUMA
MASSIVE ABDOMINAL BLUNT TRAUMA

ABDOMINAL TRAUMA • PHYSIOPATHOLOGY
– Combining forces :
• Compression
• Extension
• Separation
– Kinetic energy is transferred to abdominal organs
– The transmitted energy overcomes organ resistance
ABDOMINAL TRAUMA
• PHYSIOPATHOLOGY – The energy dissipated in the abdomen is:
KE= MV2 2
KE: Kinetic Energy M : Mass V : Velocity
ABDOMINAL TRAUMA • ASSOCIATED CLINICAL SIGNS:
– Abdomen Haematoma
– Perineal Haematoma (Retroperitoneal)
– Abdominal tenderness (Pain)
– Hemodynamic instability (Hemorrhage)
– Pelvic fractures - Caudal ribs
– Lumbar spine injuries
– Abdominal distention

ABDOMINAL TRAUMA
ABDOMINAL TRAUMA
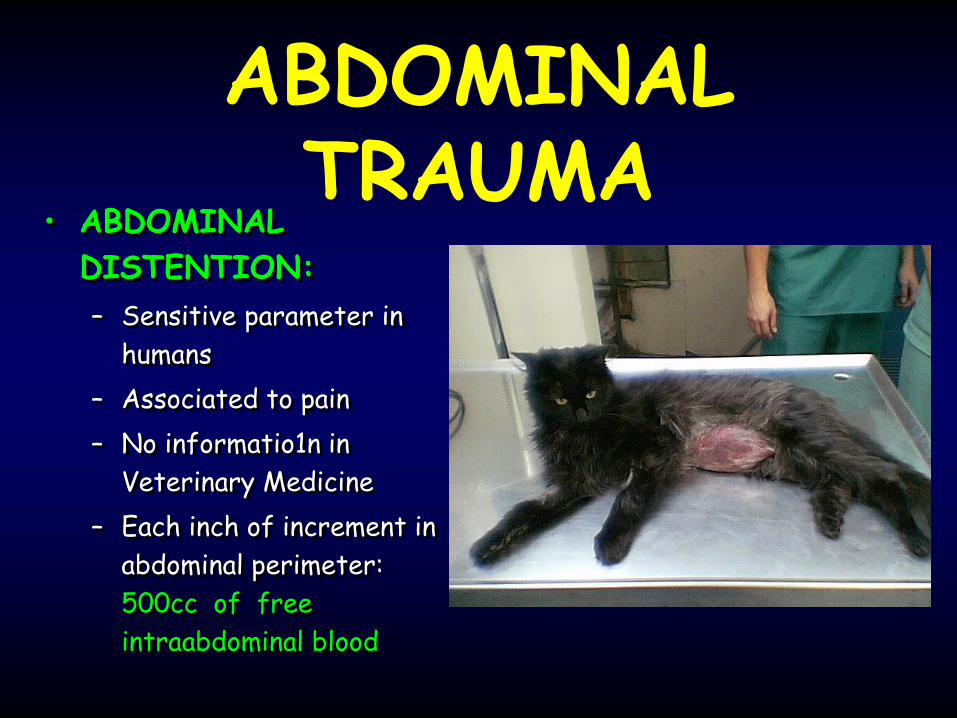
• ABDOMINAL
DISTENTION:
– Sensitive parameter in
humans
– Associated to pain
– No informatio1n in
Veterinary Medicine
– Each inch of increment in
abdominal perimeter:
500cc of free
intraabdominal blood
Massive Abdominal Trauma
First dogs used for hunting

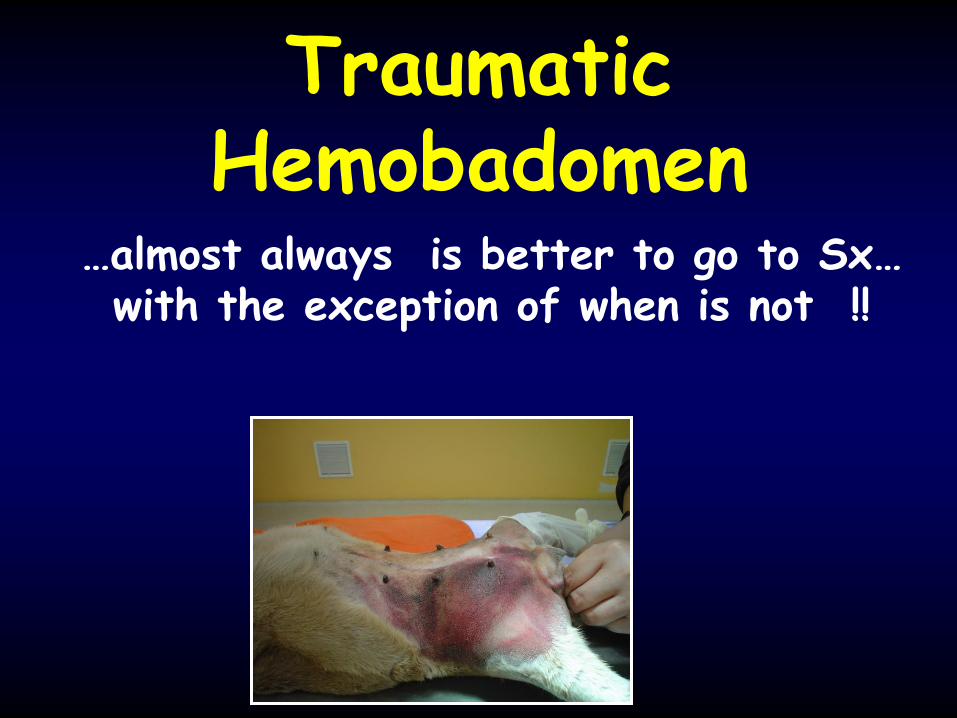
Traumatic Hemobadomen
…almost always is better to go to Sx… with the exception of when is not !!
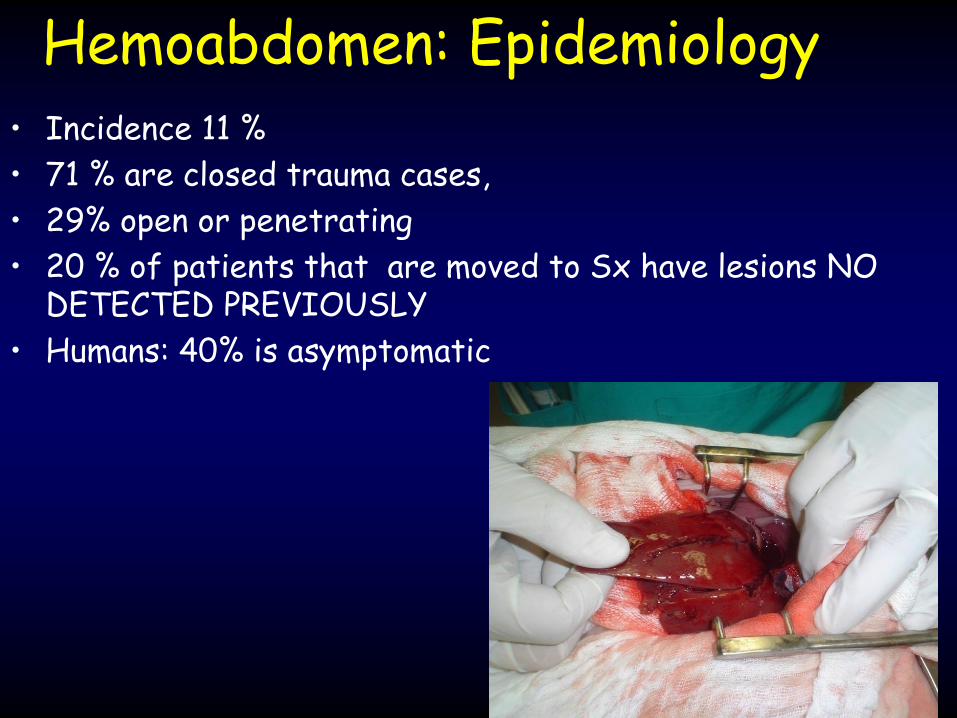
Hemoabdomen: Epidemiology • Incidence 11 %
• 71 % are closed trauma cases,
• 29% open or penetrating
• 20 % of patients that are moved to Sx have lesions NO DETECTED PREVIOUSLY
• Humans: 40% is asymptomatic
Cats may have spontaneous hemoabdomen!
• JVECCS 2010, Drobatz, et al • Sixteen cases of feline, non-traumatic hemoperitoneum were
evaluated retrospectively.
• The causes of hemoperitoneum were hepatic neoplasia (31%), hepatic necrosis (19%), hepatic amyloidosis (13%), non hepatic neoplasia (13%), hepatopathy (6%), hepatic rupture (6%), necrotic/hemorrhagic cystitis (6%), and ruptured bladder (6%).
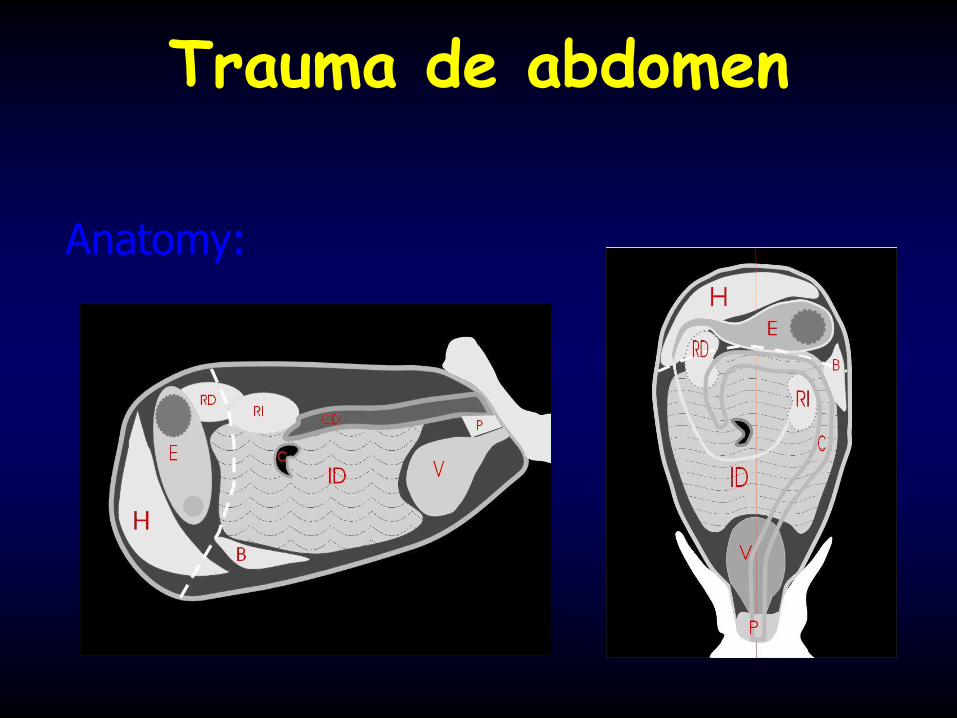
Trauma de abdomen
Anatomy:
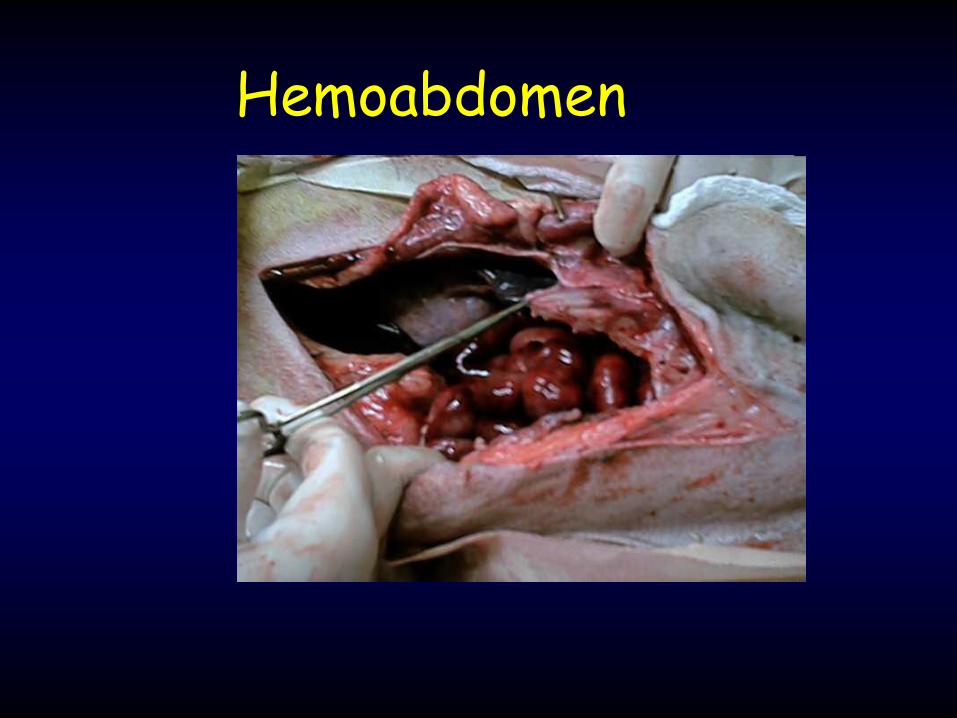
Hemoabdomen
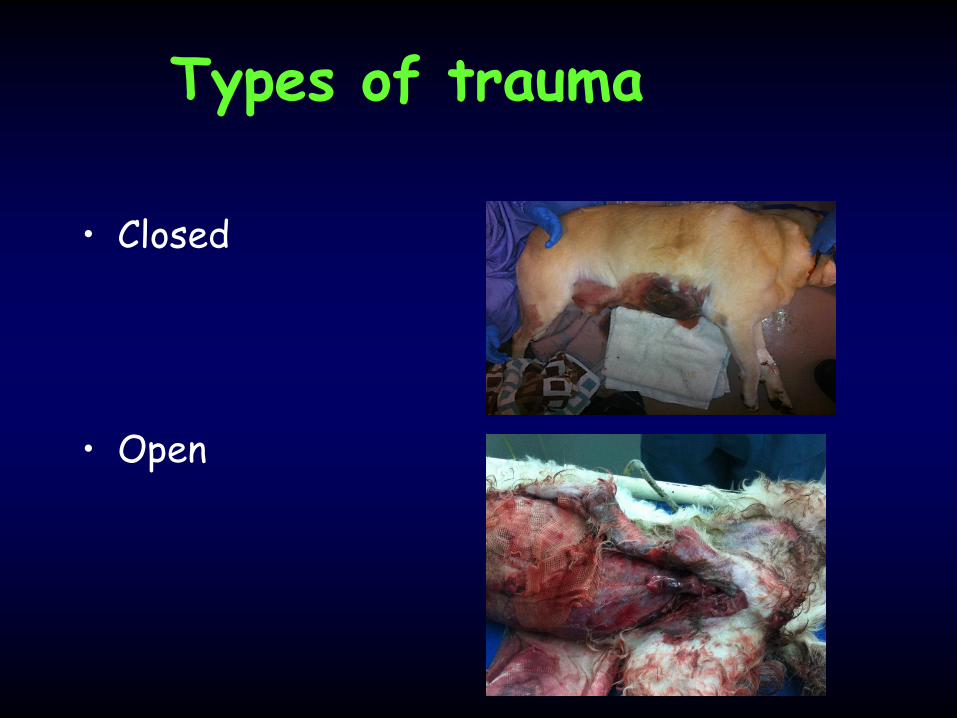
Types of trauma
• Closed
• Open

Penetranting Trauma
• Bullets, arrows, impalement, bites,
• Caudal lesions in the thorax may be abdominal
Closed abdominaltrauma: Approach
• PE is difficult and equivocal
• Key: 5 signs – Temperature
– Pulse
– Respiratory rate
– Blood Pressure
– Pain Score
Goals during initial assessment
Determine:
• There is an intraabdominal lesions
• Require medical or surgical Tx
• Find out signs of the TRIADE of DEATH – ACIDOSIS
– HYPOTHERMIA
– COAGULOPATHY

ABDOMINAL TRAUMA
• DIAGNOSTIC
PROCEDURES:
– ABDOMINOCENTESIS
– PERITONEAL LAVAGE
– ABDOMINAL
ECOTOMOGRAPHY
– ABDOMINAL
RADIOGRAPHY
– C.A.T. SCAN

ABDOMINAL TRAUMA
• ABDOMINOCENTESIS:
ABDOMINAL TRAUMA
• ABDOMINOCENTESIS:
– 20-22G Needle or Butterfly
catheter+syringe
– Medium line caudal to umbilical scar
– Get inside, infusing saline 0,9%
– Negative: 4 quadrants puncture
– Negative: peritoneal lavage


ABDOMINAL TRAUMA
• PERITONEAL LAVAGE:
– 20 - 22 G needle or butterfly catheter
– Central medium caudal to umbilical scar
– Infuse 20 ml/Kg warm saline NaCl 0,9%
– Rotate or walk the patient
– Obtain a few ml for evaluation
ABDOMINAL TRAUMA
• PERITONEAL LAVAGE : evaluation
– PCV
– PROTEINS
– CITOLOGY
– BUN - CREATININ
– BILIRRUBIN
– “BOYSCOUT” TEST

ABDOMINAL TRAUMA
• BOY SCOUT TEST:
– PUT A DROP OF PERITONEAL LAVAGE
FLUID ON A MICROSCOPE SLIDE
– HEAT TO DIRECT FLAME
– AMMONIA RELEASE? URINE !!
– SCOUTS PUT OUT FIRES WITH URINE

ABDOMINAL TRAUMA
• POSITIVE LAVAGE:
HEMOPERITONEUM
– PCV > than peripherical
– Spleen has a higher PCV
than blood
– The peritoneum absorbs
water and electrolytes
– More than 100.000
erythrocytes/ml
– More than 500 leukocytes/ml
– Can it be read through the
tube??
HEMOPERITONEUM
MANY
POINTS
OF VIEW!!!!
Lab Data Base
• Hct y Hb
• Glycemia
• Creatinine
• Ca - Mg
• CPL
• Proteines
• UA
• Coagulation profile
• Blood gases- electrolytes
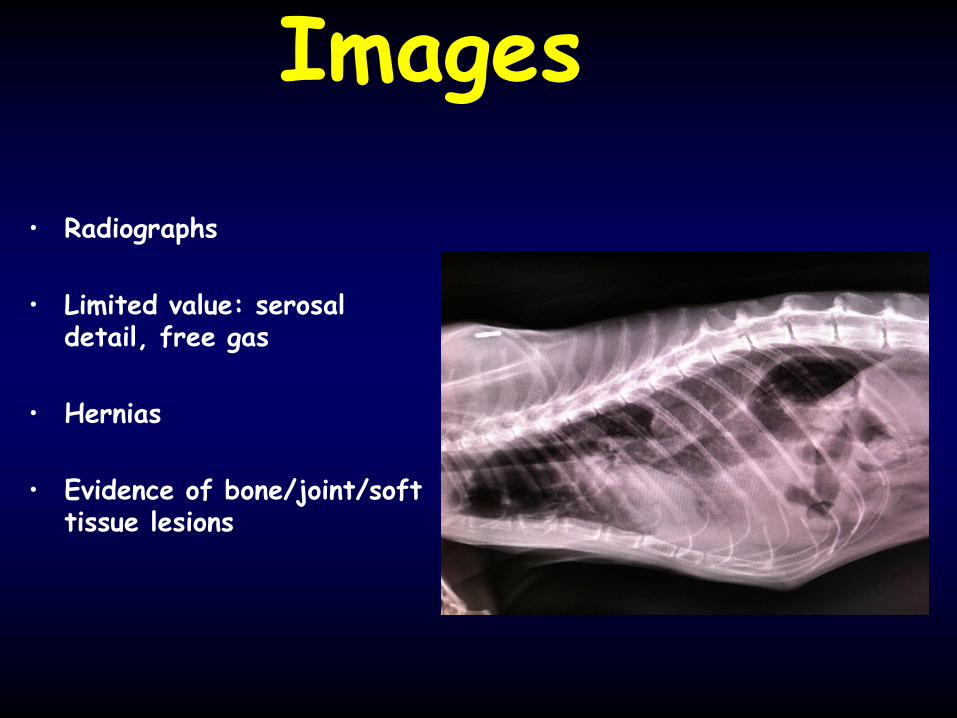
Images
• Radiographs
• Limited value: serosal detail, free gas
• Hernias
• Evidence of bone/joint/soft tissue lesions
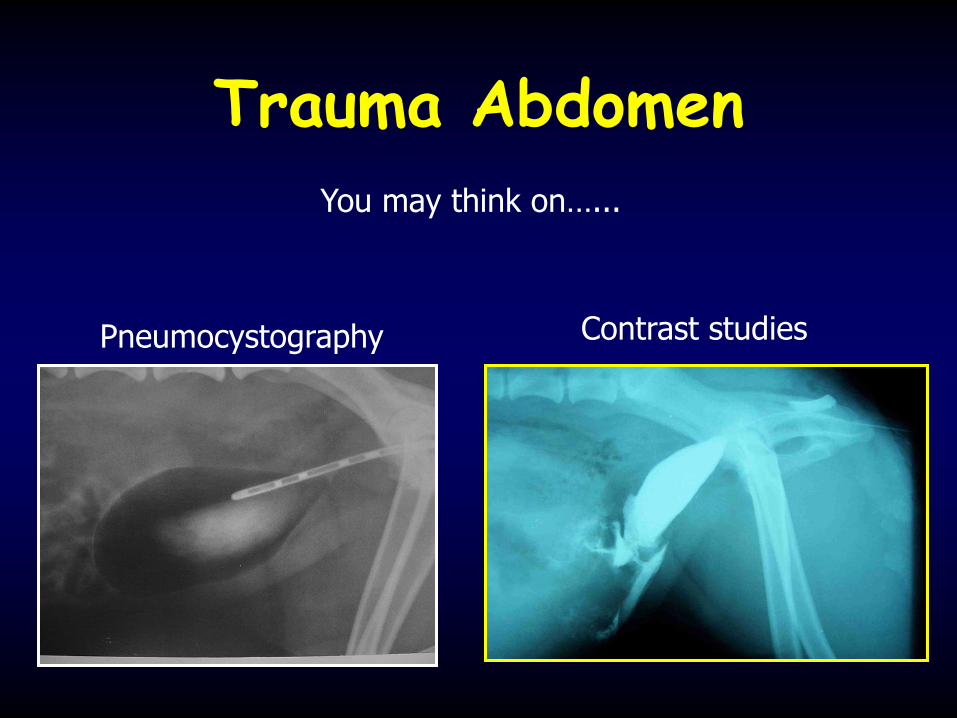
Trauma Abdomen
You may think on…...
Pneumocystography Contrast studies
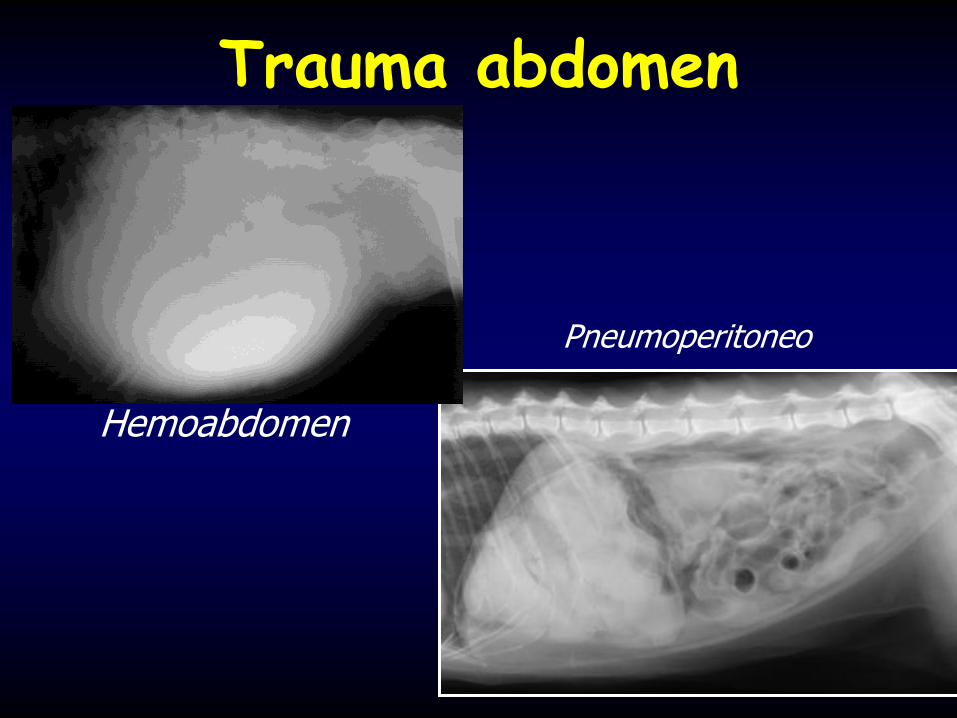
Trauma abdomen
Hemoabdomen
Pneumoperitoneo

Radiographs
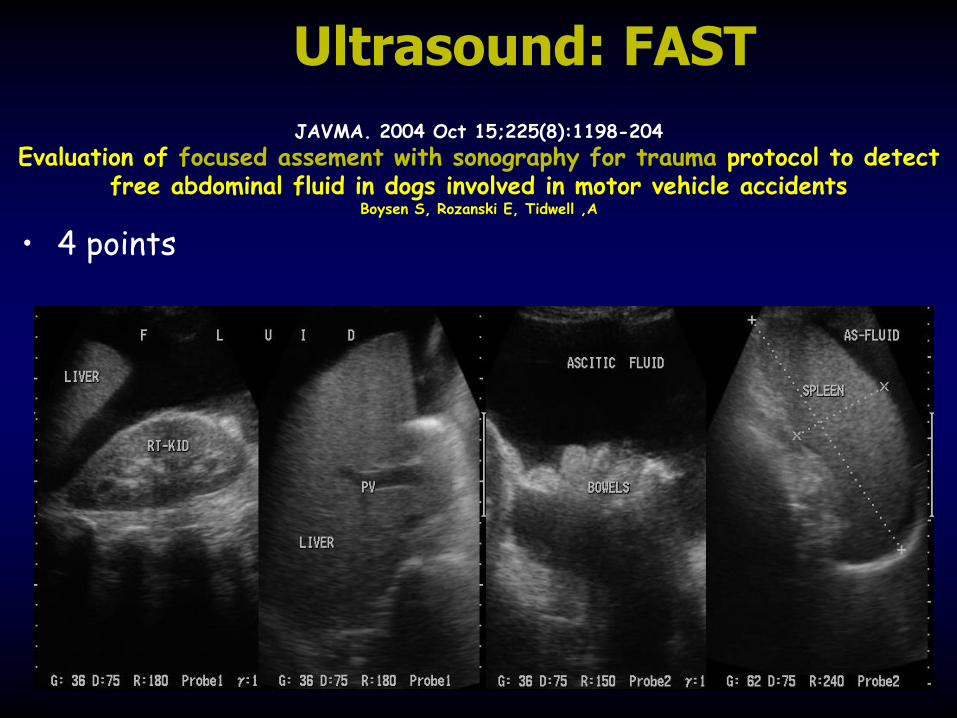
JAVMA. 2004 Oct 15;225(8):1198-204
Evaluation of focused assement with sonography for trauma protocol to detect free abdominal fluid in dogs involved in motor vehicle accidents
Boysen S, Rozanski E, Tidwell ,A
• 4 points
Ultrasound: FAST

Tap the abdomen
• Easy, fast, cheap
• High percentage of false negatives
• Should be more than 5 ml/Kg of free fluid

Abdomen Trauma
Abdominal centesis: 4 quadrants
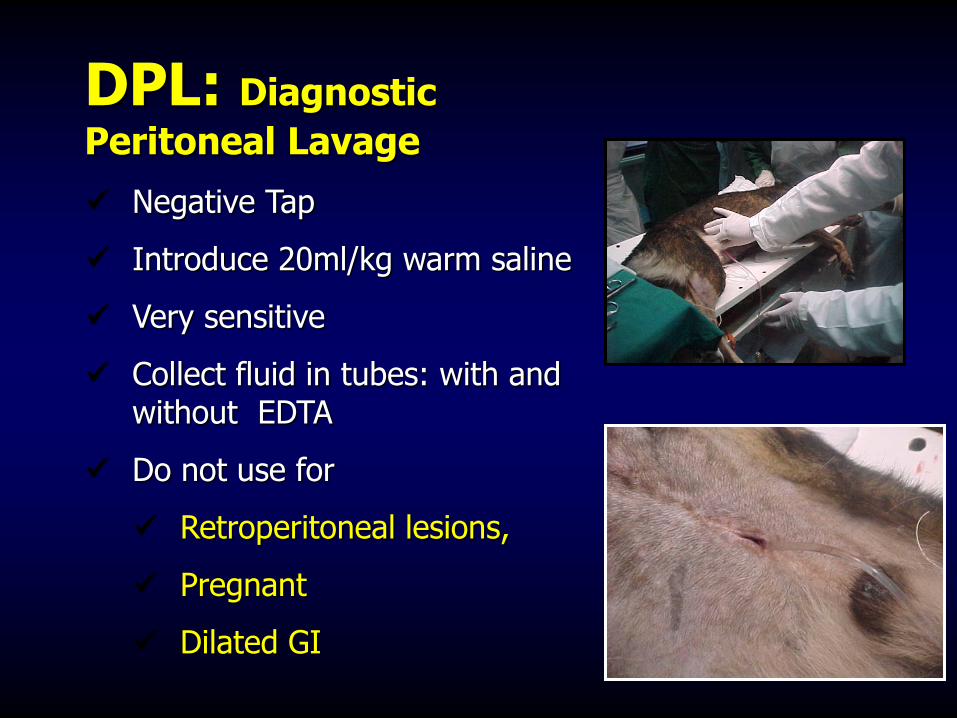
DPL: Diagnostic
Peritoneal Lavage
Negative Tap
Introduce 20ml/kg warm saline
Very sensitive
Collect fluid in tubes: with and without EDTA
Do not use for
Retroperitoneal lesions,
Pregnant
Dilated GI
Materials

Mini Laparotomy





Entonces….cortamos o no?

Gross examination
RED: Hemorrhage
GREEN:Gallbladder – Biliary tract
YELLOW: Urinary tract
BROWN” GI tract
So….cut or not? • The key seems to be on the patient
– No response to Tx
– Worsening hypotension
– Mentation worsening
– Drop on the Hct (20%)
– If you are not sure…..
No Sx Tx of HEMOBANDOMEN)
• FLUID Tx (NO EXCESSIVELY AGGRESSIVE)
• PLASMA – Coagulation factors
• Pain management
• Sedation
• Oxygen
• ICU MONITORING
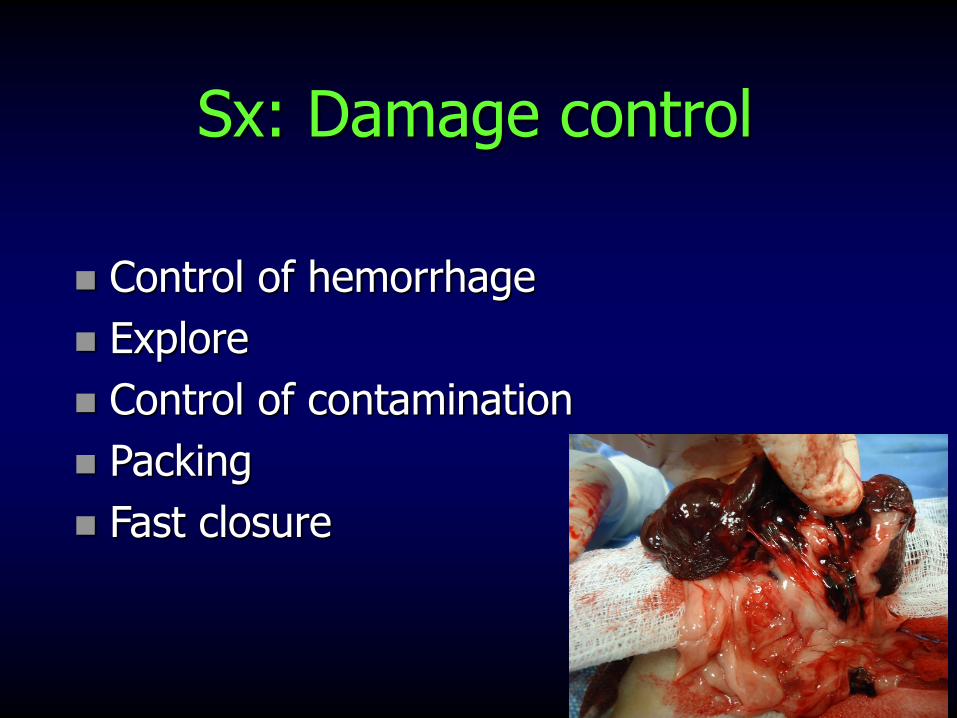
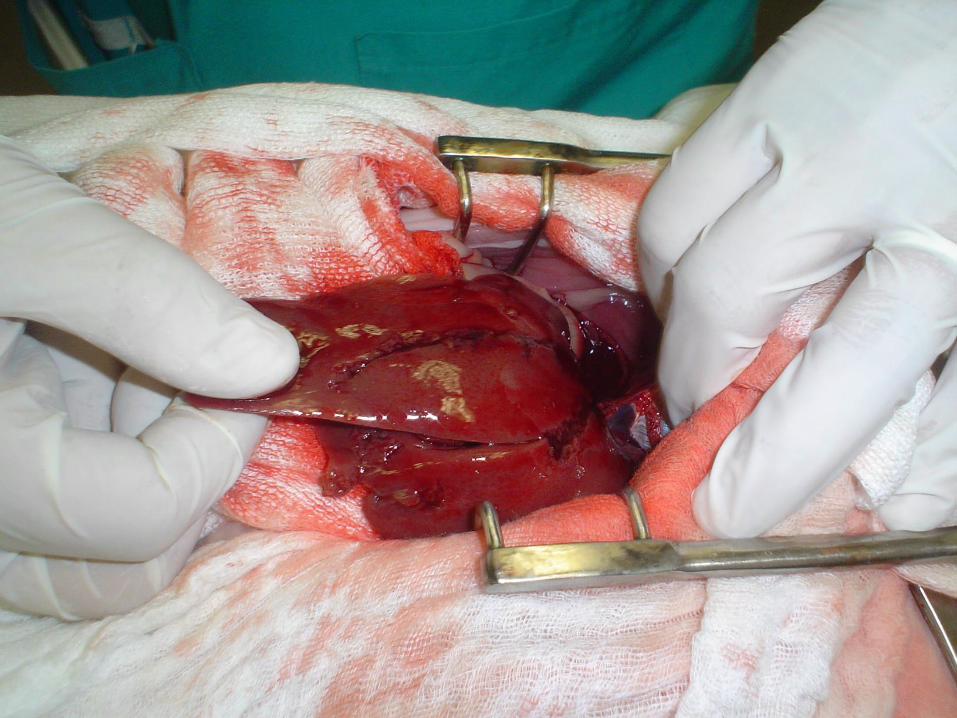
Sx: Damage control
Control of hemorrhage
Explore
Control of contamination
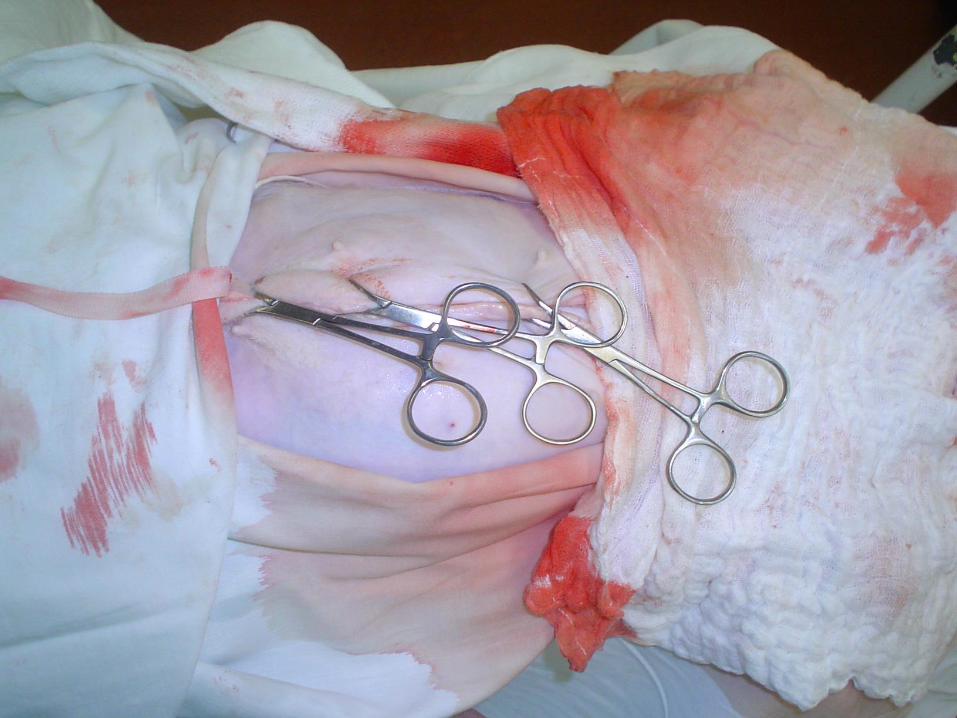
Packing
Fast closure
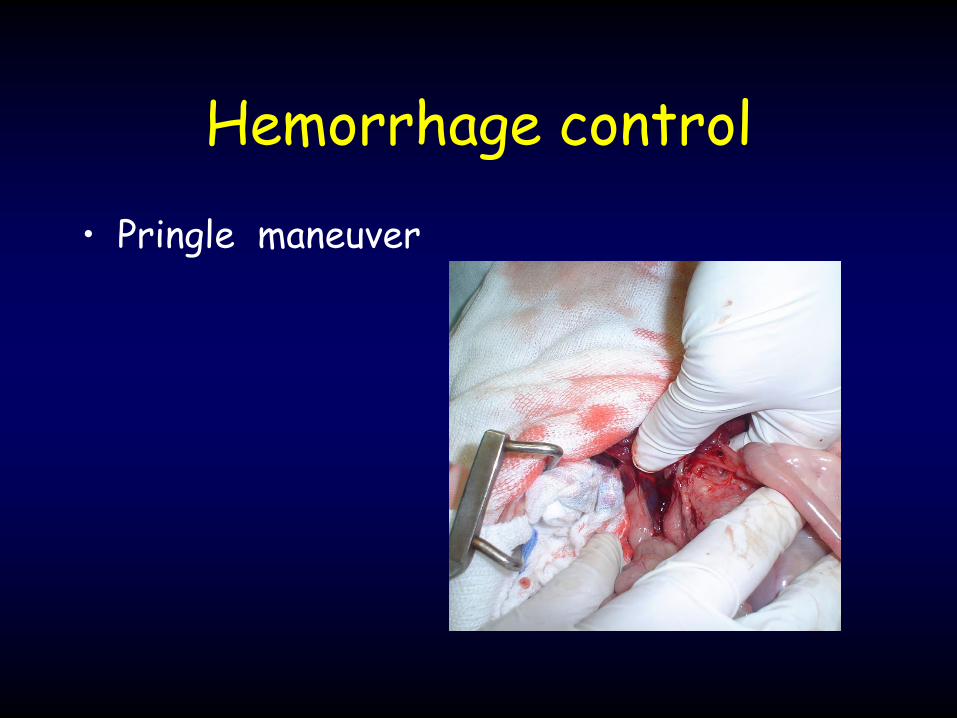
• Pringle maneuver
Hemorrhage control
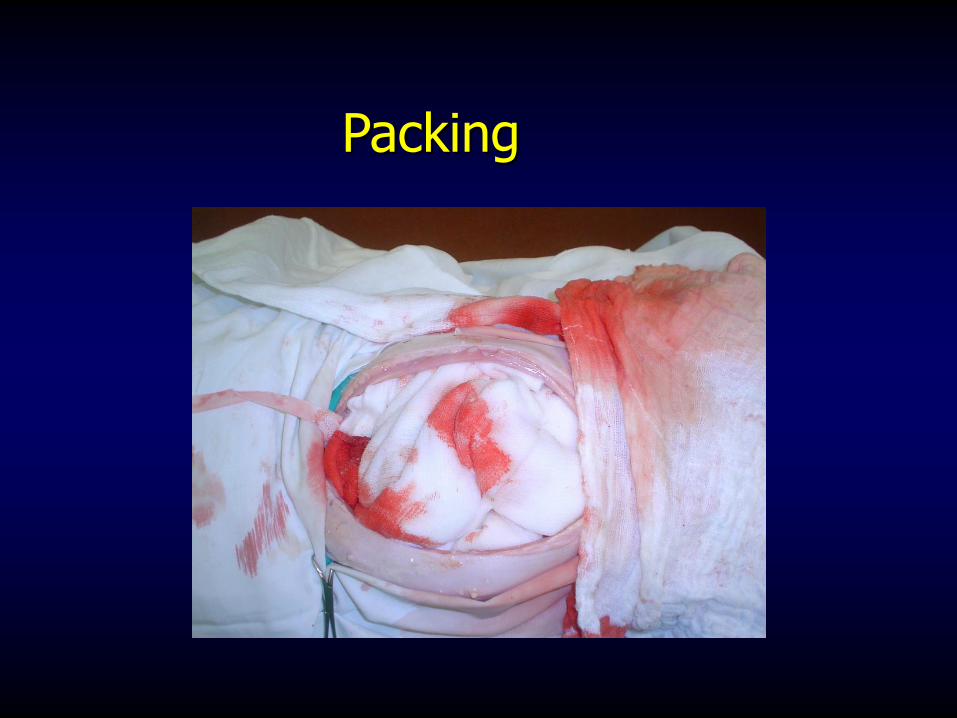
Packing
Post Sx
• Fluids, Atb, Nutrition
• Check Hct, Proteines, Albumine
• Monitor Blood Pressure
• Monitor ECG
• Monitor Urine production
• DO NOT FEEL SAFE BEFORE 72 HOURS POST SX

UROPERITONEUM
UROPERITONEUM • Massive rupture is frequent in blunt
trauma with full bladder
• It can be diagnosed with contrasted
X-rays :
• Excretion Nephrogram
• Contrasted Cystogram
• Pneumocystogram
UROPERITONEUM • Massive rupture is frequent in blunt
trauma with full bladder
• It can be diagnosed with contrasted
X-rays :
• Excretion Nephrogram
• Contrasted Cystogram
• Pneumocystogram

UROPERITONEUM • SURGICAL THERAPY

THANKS





