Embed Size (px)
Citation preview

Breast Cancer Vol. 2 No. 2 October 1995
Original Article
Medical Economics and Quality of Life: Analysis of Factors That Influence the Perception of Medical Cost by Post-surgical Breast Cancer Patients
K O J I R O S H I M O Z U M A .1, H I R O S H I S O N O 0 .1, A N D K I Y O S H I I C H I H A R A .2
Recently, the impor tance of achieving a balance in terms of length of life (LL), quali ty of life (QOL) and medical costs has been emphasized in the evaluation of cancer treatment, and it is also said that the cost should be seen from the viewpoints of both the society and the patient. Few studies, however , have been pe r fo rmed to investigate how the patients bear the cost and the inf luence of this factor. Therefore , in the present study we examined the percept ion of medical care cost (PMC) in 83 non - r ecu r r en t post surgical breast cancer patients. The factors that inf luence the PMC were analyzed by univariate and multivariate analyses using the variables represent ing QOL, sociodemographic and clinical characteristics, types of therapy, and various types of medical cost. First, the results of the relat ionship be tween the variables and the PMC revealed that the patients with better QOL, especially those with better social category QOL, t ended to have a lower PMC. However , no other variable had any significant associations with the PMC. Second, the results of mult iple regression analyses revealed that patients with better QOL, especially those with better social category QOL, in the elderly, a n d / o r those with higher level of educat ion t ended to show a lower PMC. In conclusion, the results of the present s tudy suggest that, when we consider evaluating the cost of cancer t reatment for post surgical breast cancer patients, we should take into account the patients ' QOL, age, and their level of educat ion.
Breast Cancer 2:143-153, 1995
Key words: Breast cancer, Medical cost, Quality of life (QOL), Cancer in the elderly, Adjuvant therapy
For many years, the main objective of cancer treatment was to prolong the length of life (LL) (disease-free survival or overall survival). Recently however, it has become a well recog- nized fact that the consideration of the quality of life (QOL) of the patients is necessary to fully
*1Division of Endocrine Surgery and *2Department of Clinical Pathology, Kawasaki Medical School. Reprint requests to Kojiro Shimozuma, Division of Endocrine Surgery, Kawasaki Medical School, 577 Matsushima, Kurashiki 701- 01, Japan.
Abbreviations: LL:Length of life; QOL:Quality of life; PMC:Perception of medical cost; DMC:Direct medical cost; BDMC:Burden of direct medical cost; DMCP:Direct medical cost that patients actually pay; QOL-ACD:The QOL Questionnaire for Cancer Patients Treated with Anticancer Drugs; SD:Standard deviation; rs:Spearman's rank correlation coefficient
Received April 14, 1995; accepted July 5, 1995
evaluate cancer treatment. Gelber and Goldhirsh et al ~) have performed pioneering work to develop an appropriate evaluation system inte- grating LL and QOL: ie, TWIST (time without symptom of disease and subjective toxic effects of treatment) and Q-TWiST (quality adjusted TWIST). Another factor that has become em- phasized as one of the societal endpoints is the cost of medical care that continues to rise in many countries. It is suggested that these three aspects (LL, QOL and cost) must be well balanced in cancer treatment. Lastly, some attempts 2-4) to combine these three features, ie, cost per QALY (quality adjusted life year) and cost in relation to QALE (quality adjusted life expectancy) have been reported.
Moreover, when integrating these features, it is said that the costs and outcomes should be judged
143

Shimozuma K, et al Medical Economics and Quality of Life
according to the viewpoint of society, the patient, the payer, or the provider 5). Few approaches, however, have been made to evaluate those end- points emphasizing the patients' point of view. In Japan, clinicians previously have not taken into consideration the QOL and cost seriously in evaluating cancer treatment. Therefore, to our knowledge, there have been no attempts whatso- ever by Japanese clinicians to integrate these three aspects, nor are there any reports to investi- gate the patients' perception of medical cost (PMC), although there are numerous studies set- ting LL as an endpoint of cancer treatment and a few studies ~-9) investigating QOL.
The health care system in Japan has some unique features. The direct medical cost exceed- ing u 000 per month in the same medical facil- ity is refunded several months later. Patients are simply classified into four groups according to their burden of direct medical cost: ie, almost free (patients more than 70 years of age, or physically handicapped persons 65-69 years of age), 10% (employees), 20% (retired persons, or their hospitalized dependents), and 30% (unemployed persons, their dependents, the dependents of retired persons on an outpatient basis, or persons without a regular occupation). There may be some differences in the PMC depending on the patients.
In this study, we applied multiple regression analyses to reveal the factors that influence the PMC by post-surgical breast cancer patients among the variables related to QOL, sociodemo- graphic and clinical characteristics, types of ther- apy, and various types of medical costs.
Patients and Methods
Recrui tment and Characteris t ics o f Pa t ien ts Patients were selected from the Division of
Endocrine Surgery of Kawasaki Medical School Hospital. The subjects were selected from the patients who participated in other studies to evaluate QOLS'91:83 non-recurrent post-surgical breast cancer patients, who had undergone sur- gery at our clinic within the last 5 years, were asked to participate in the QOL evaluation studies from February 1993 to June 1994. They were informed about the purpose of the studies. All the patients agreed to take part in the study. All the patients had already been notified of their cancer, and had been well informed of the treat-
ment they received and of their prognoses. The sociodemographic and clinical character-
istics of the 83 patients are listed in Table 1. The clinical stage of each case was determined by the UICC TNM classifications TM. All the subjects underwent resection of their primary lesion and all the patients who received breast conserving surgery had adjuvant radiotherapy to the resid- ual breast within two months after the surgery. Types of adjuvant therapy adopted in this study were those given within a month prior to the QOL questionnaire. Most patients received chemother- apy and/or endocrine therapy as an adjuvant therapy within around 1 to 3 years after the surgery. Twenty-six cases received only chemo- therapy, 11 received only endocrine therapy, and 22 received chemoendocrine therapy. Five cases received radiotherapy, including two chemother- apy cases and one endocrine therapy case. Nine- teen patients received no therapy during the study. As orally administered drugs, tamoxifen (TAM) and medroxyprogesterone acetate (MPA) (only in 1 case) were used for endocrine therapy, and cyclophosphamide (CPA), tegafur, tegafur. uracil (UFT), doxifluridine (DFUR) and car- mofur (HCFU) were used for chemotherapy. Three cases were exceptionally given intra- venous chemotherapy in the form of sequential CAF therapy (CPA+doxorubicin [ADM] {or farmorubicin [4'-epi ADM] } +5-fluorouracial [5-FU~) (2 cases of them in combination with TAM, all 3 cases were in stage liD.
Calculation o f Medical Costs Direct costs of medical services usually neces-
sary for breast cancer treatment, ie for surgery, adjuvant therapy, and hospitalization calculated based on the book "Interpretation of medical costs" edited by the Ministry of Health and Welfare of Japan in 1994 are illustrated in Table 2. Based on the costs illustrated in Table 2, we calculated the actual direct medical costs of each patient within 1 month prior to the questionnaire. The median of the direct medical costs (DMC) for the subjects was Y61 000, which did not include the direct medical costs for laboratory tests, rehabilitation and long-term care, and non- medical expenditures of services such as food, transportation, lodging, family care, home aids, and clothing. The distributions of the burden of direct medical costs (BDMC) are also indicated in Table 2 and the median of the direct medical
1 4 4

Breast Cancer Vol. 2 No. 2 October 1995
Table 1. Sociodemographic and Clinical Characteristics
Factor No. of cases Mean+ SD a> Median (Range)
Months after surgery 83 10.0_+ 11.0 6.0 (0-52) Age 83 52.6 + 10.9 52.0 (27-75) Body weight (kg) 79 b) 54.9 +8.8 55.0 (37-81)
Score set for the multiple Factor No. of cases
regression analysis
Stage T is / I /II/III 5/33/36/9 0/1/2/3
Performance status (PS) 0/1 80/3 1/0
Hospitalization No/Yes 67/16 0/1
Marital status Single/Divorced/Widowed 2/5/7 0 Married 69 1
Children No/Yes 8/75 0/1
Education (years) -9 9 0 10-12 53 1 13- 7 2 Missing 14
Religion No or Missing 68 0 Yes 15 1
Buddhist/Christian 13/2 Types of surgery
Breast conserving surgery 19 1 Lumpectomy 3 Quadrantectomy 16
Modified radical masteetomy 64 0 Auchincloss 19 Patey 45
Types of adjuvant therapy c> Chemotherapy alone
No/Yes 57/26 0/1 Endocrine therapy alone
No/Yes 72/11 0/1 Chemoendocrine therapy
No/Yes 61/22 0/1 Radiotherapy
with any other therapies d) No/Yes 78/5 0/1
No therapy No/Yes 64/19 0/1
a>Standard deviation; b>The body weight was not measured in the remaining 4 cases; C>Types of adjuvant therapy given within 1 month prior to the questionnaire; d>Two chemotherapy cases and 1 endocrine therapy case were included.
costs that patients actually pay (DMC • BDMC) (DMCP) was u 18 300.
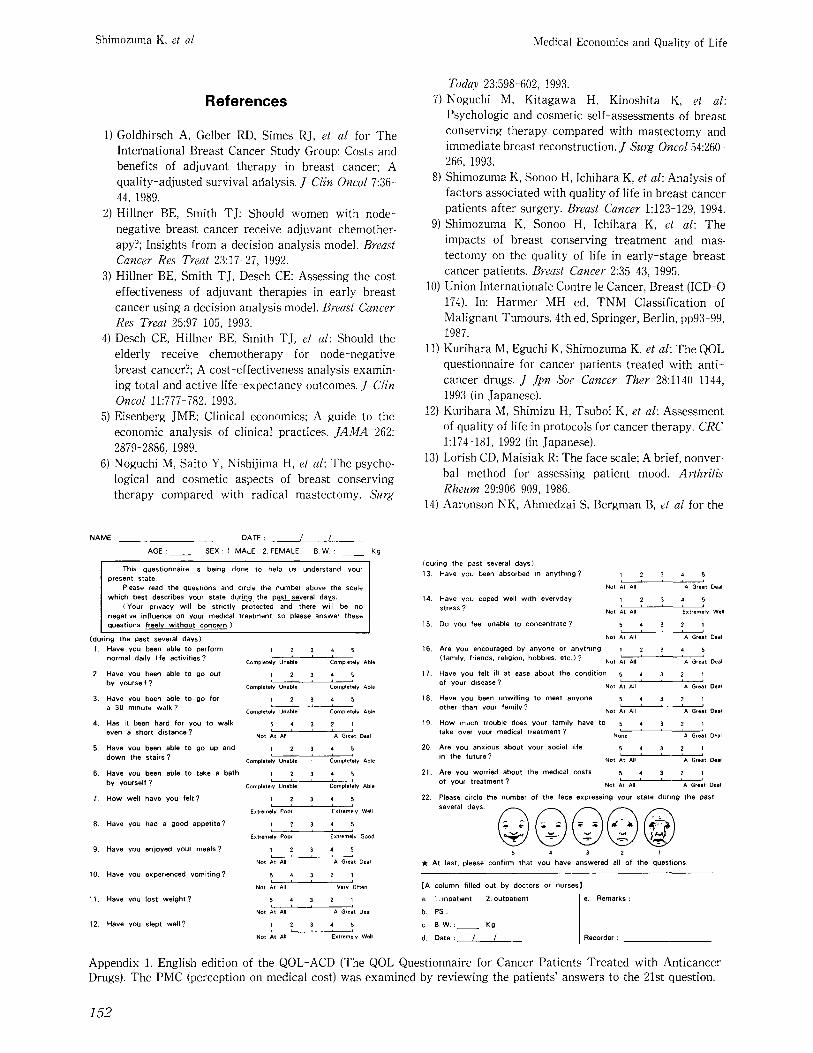
Assessment of PMC The PMC was examined by reviewing the
patients' answers to the 21st question of the QOL ACD (The QOL Questionnaire for Cancer
Patients Treated with Anticancer Drugs, as ab- breviated by permission of Kurihara TM) (see below). The question reads: 'Are you worried about the medical costs of your treatment?' This question belongs to the category of social rela- tionship in the five main categories of the QOL- ACD. The score of the question (PMC score)
145

Shimozuma K, et al Medical Economics and Quality of Life
Table 2. Medical Costs
Types of therapy or care Costs (u
Surgery Breast conserving surgery Modified radical mastectomy
Adjuvant therapy Radiotherapy to the residual breast
(50 Gy/5 weeks) Chemotherapy
Cyclophosphamide (CPA) (100 mg • 14 days/4 weeks/1 cycle)
Tegafur (800 rag/day) Tegafur.uracil (UFT)(400 rag/day) Doxifluridine (DFUR) (800 rag/day) Carmofur (HCFU) (300 rag/day) 5-fluorouracil (5-FU) (500 mg• weeks) Doxorubicin (ADM) (30rag • 2/4 weeks) Farmorubicin (4'-epi ADM)
(50 mg• 2/4 weeks/1 cycle) Endocrine therapy
Tamoxifen (TAM) (20 rag/day) Medroxyprogesterone acetate (MPA)
(800 mg/day) Hospitalization
112 000 160 000
262 500
1500/4 weeks
14 200/month 55 900/month 61 000/month 30 600/month
2400/4 weeks 21 100/4 weeks 95 200/4 weeks
19 700/month 59 000/month
366 400~)/month
Costs/month (N) Factor No. of cases Median (Range)
Direct medical cost (DMC) 83 61 000 (0-764 000)
Score set for the multiple Factor No. of cases
regression analysis
Burden of direct medical cost (BDMC) Free 7 0 10% 25 1 20% 3 2 30% 48 3
Costs/month (u Factor No. of cases Median (Range)
Direct medical cost that patients 83 18 300 (0-202 400) actually pay (DMC • BDMC)(DMCP)
a~not including costs for meals, extra room charge, etc. All the figures have been rounded out.
ranged from 1 to 5, with a higher score represent-
ing the patients' competency in bearing the medi- cal cost.
Assessment of QOL The QOL ACD is a pat ient- ra ted QOL evalua-
tion system developed for Japanese cancer patients by a scientific group called 'The Research Group For Scientific Assessment Mea- sures of Trea tments with Anticancer Drugs' established by the Japanese Ministry of Health and Welfare (April 1989 to March 1991, director:
M. Kurihara), and by 'The Research Group for Scientific Assessment of Drug Trea tment ' (April 1991 to March 1993, director: M. Kurihara). The exact formulation of the QOL-ACD (English edition) is given in Appendix 1. Its validity and reliability have been verified TM. The QOL-ACD was developed as a core questionnaire for evaluating the QOL of cancer patients, applicable to any organs involved or any types of therapy, although it was mainly designed to reflect changes in QOL following t reatment with anti- cancer drugs.
1 4 6

Breast Cancer Vol. 2 No. 2 October 1995
The following is a brief description of the QOL- ACD. It consists of 22 questions covering five categories: (1) activity (six items), (2) physical condition (five items), (3) psychological condition (five items), (4) social relationship (five items), and (5) overall aspects of QOL (one item) as represented by a face scale that consists of five different faces selected from the 20 original ones by Lorish and Maisiak TM. Patients are instructed to answer all questions by circling the number that best represents their state. The score for each question (1 to 5) is summed to give an overall QOL score, the minimum being 22 and the maximum being 110. A higher score represents a higher QOL.
During the data processing of this study, the questionnaires with 2 or less unanswered ques- tions among the 22 questions (just 1 case in this study) were judged valid. The unanswered ques- tions were substituted by the mean score for the rest of the questions. By this criterion, all the 83 questionnaires were valid (100%). The 21st ques- tion (PMC score) was excluded in the calculation of the QOL score.
Stat is t ical Procedures PMC scores were analyzed in two stages. First,
the relationships between the PMC score and the following variables were examined: ie, the over- all QOL score, the mean scores of 4 of 5 cate- gories of the QOL-ACD (except 1 category cover- ing the overall aspects of QOL by face scale), sociodemographic and clinical characteristics indicated in Table 1, and the various types of medical cost indicated in Table 2. For statistical analysis, Spearman's rank correlation coeffi- cient test for serial variables, the Mann-Whitney U test for two independent samples, and the Kruskal-Wallis one-way analysis of variance test was used for variables with more than two groups.
Second, to explore the relative importance of the factors, multiple regression analyses were carried out. In the first multivariate analysis, the PMC score was set as a dependent variable. The overall QOL score and the factors indicated in Tables 1 and 2 were set as independent variables. In the second multivariate analysis, instead of the overall QOL score, the mean scores of the four categories of the QOL-ACD were used as in- dependent variables. Tables 1 and 2 list the score assigned to each category of the qualitative vari-
ables for use in the multiple regression analysis. Lotus 1 2-3 (Lotus Development Co, Cambrid-
ge, USA) was used for accumulation of the data and calculation of the score. The statistical ana- lyses, including the multivariate analyses, were carried out by general purpose statistical soft- ware, Stat Flex (View Flex Co, Tokyo, Japan).
Results
PMC Score The mean_+SD (standard deviation) of the
5-
4-
3-
2,
1
�9 g o � 9 1 4 9 ~ OOOOO$$==== OgO
�9 � 9 1 4 9 g o � 9 1 4 9 �9 2 = 3 = $ = �9
O �9 �9 �9 �9 �9
122 326 7- '12 13124 25136 37260
M o n t h s af ter Surgery The bar represents the mean of the score.
100 o
_J 0 0
75
0
50
�9 �9
8 �9 �9 8
I '2 326 7- '12 13224 25236
M o n t h s after Surgery The bar represents the mean of the score.
37~6o
Fig 1. Top, The distribution of the PMC (perception of medical cost) scores in relation to the period after surgery. No significant relation was observed between the PMC score and the period aft& surgery (Kruskal Wallis test). Bottom, The overall QOL (quality of life) scores in rela- tion to the period after surgery. Significant incremental trend was observed in the mean scores from 0 to 3-6 months after surgery (P-0.016 by the Kruskal Wallis test). The mean score at 0 months after surgery was significantly lower than those at 3-6, 7-12, 13 24, and 25- 36 months (P<0.01, 0.01, 0.005, and 0.05, respectively, by the Mann Whitney test). The bar represents the mean of the score.
147

Shimozuma K, et al Medical Economics and Quality of Life
5
~ 4
~3
5.
o 4,
2~ 3 �84 13.
rs = 0.516
�9 . . . . - -_2 . -
~0 io ~o 8'o ~0 1;0 1~0 Overall QOL Score
rs = 0 . 3 6 9
The Mean Score of Activity
Fig 2. Top, Correlation between the overall QOL score and the PMC score. The overall QOL score had a signifi- cantly positive association with the PMC score. Spear- man's rank correlation coefficient (rs) of this analysis was 0.515 (P = 0.0000). Middle and bottom, Correlation between the mean scores of the four categories of the QOL and the PMC score. Only social relationship had signifi- cantly positive association with the PMC score (rs =0.616).
O (D Q.
rs = 0.282
5
4
3
2
1
The Mean Score of Physical Condition
== O o (13
rs =i"
The Mean Score of Psychological Condition
5 -
o #2 4-
3 O_
rs = 0.616 J I
The Mean Score of Social Relationship
The elipse represents the 95 % confidence area.
PMC scores was 3.6+1.3, and the median was 4.0 (ranging from 1 to 5). The distribution of the PMC scores in relation to the period after sur- gery is illustrated in Fig 1, top. No significant relation was observed between the PMC score and the period after surgery (Kruskal-Wallis test).
QOL Score The mean+SD of the overall QOL score was
90.7+ 13.5, and the median was 90.0 (ranging from 50 to 110). The m e a n + SD of the scores of the four categories of the QOL-ACD were 4.3___0.7 (activ- ity), 4.5+0.5 (physical condition), 4.0___0.8 (psy-
chological condition), and 3.7+0.9 (social rela- tionship). The overall QOL scores in relation to the period after surgery are illustrated in Fig 1, bottom. A significant incremental trend was observed in the mean scores from 0 to 3-6 months period after surgery (P = 0.016 by Kruskal-Wall is test). The mean score 0 months after surgery was significantly lower than those at 3-6, 7-12, 13-24, and 25-36 months (P<0.01, 0.01, 0.005, and 0.05, respectively, by Mann-Whitney test).
Relationships between the PMC Score and Other Variables
The overall QOL score had significantly posi-
148

Breast Cancer Vol. 2 No. 2 October 1995
tive association with the PMC score (Fig 2, top): ie, the patients with better QOL tended to indi- cate less PMC. Spearman's rank correlation co- efficient (rs) of this analysis was 0.516 ( P = 0.0000). Among the mean scores of the four cate- gories of the QOL-ACD, only social relationship had a significantly positive association with the PMC score (rs=0.616) (P=0.0000) (Fig 2, middle and bottom).
None of the sociodemographic and clinical factors had significant relations with the PMC scores: The r~ for the associations of the PMC scores with period after surgery, age, and body weight were 0.165, 0.275, and 0.030, respectively. The P values by the Kruskal-Wall is test for associations with clinical stage and level of edu- cation were 0.723 and 0.469, respectively. The P values by the Mann-Whitney test for associa- tions with performance status (PS), hospitaliza-
tion, marital status, children and religion were 0.633, 0.056, 0.433, 0.605, and 0.460, respectively. Therapeutic factors such as types of surgery or adjuvant therapy also showed no significant associations with the PMC score (P=0.951 by Mann-Whitney test and P=0.979 by Kruskal- Wallis test, respectively) (Fig 3).
None of the variables concerning cost, such as the DMC, the BDMC, or the DMCP had signifi- cant associations with the PMC score (Fig 4). That is, the rs between the PMC score and the DMC was -0.303, and that between the PMC score and the DMCP was -0.115. The P value by the Kruskal-Wall is test for the association of the PMC score with the BDMC was 0.105.
Multiple Regression Analysis of the Factors The result of the multiple regression analysis
by setting the overall QOL score as an indepen-
Fig 3. Top, Relationship between the types of surgery and the PMC (perception of medical cost) score. No significant association was observed between them (P =0.951 by the Mann-Whitney test). Bottom, Relationship between the types of adjuvant therapy and the PMC score. No signifi- cant association was observed between them (P = 0.9?9 by the Kruskal-Wallis test).
Fig 4. Top, Relationship between the BDMC (burden of direct medical cost) and the PMC (perception of medical cost) score. No significant association was observed between them (P=0.105 by the Kruskal-Wallis test). Bottom, Correlation between the DMCP (direct medical cost that patients actually pay) and the PMC score. No significant association was observed between them (r~= -0.115).
1 4 9

Shimozuma K, et a/ Medical Economics and Quality of Life
dent variable was as follows.: The overall QOL score showed a close association with the PMC score (P =0.0000). Second, age had a significant association with it (P = 0.0081). Third, the patients' level of education had a weak but signif- icant association with it (P =0.0320) (Table 3a). In contrast, the remaining factors concerning sociodemographic and clinical characteristics and the various types of medical cost had no significant associations with it. In other words, the patients with a better QOL, at a greater age, and/or with a higher level of education had a lower PMC. The final multiple correlation coeffi- cient (R) after stepwise selection of the variables was 0.5819 (P -- 0.0000).
On the other hand, the analysis done by setting the mean scores of the four categories of the QOL ACD as independent variables revealed that social relationship had a close association with the PMC score (P = 0.0000), while age had a slight association with it (P=0.0260) (Table 3b). The final multiple correlation coefficient (R) after
stepwise selection of the variables was 0.6623 (P = 0.0000).
Discussion
There were two main questions at the start of this study. The first was how to evaluate the influence of medical costs in patients with cancer. There was no known evaluation method. We thought the method should be reliable, easy to fill out, and easily dealt with by quantitative analy- sis. Fortunately, some of the QOL questionnaire measures include items focused on economic aspects, eg,QOL ACD, and 'The European Organ- ization for Research and Treatment of Cancer (EORTC) QLQ-C3014). ' In this study we decided to adopt the score of the 21st question of the QOL- ACD as a measure for representing the PMC. We are not sure whether a single question can be truly representative of the PMC. Actually, the question item belongs to one of the QOL cate- gories representing social relationship. There-
Table 3. Multiple Regression Analysis of the Factors Associated with the PMC (Perception of Medical Cost) Score
(a) The Overall QOL (Quality of Life) Score Is Set as an Independent Variable Representing QOL
Factor Regression Standard error t value P value coefficient
1. QOL 0.04843 9.656E-3 5 .015 0.0000"** 2. Age 0.03193 0.01174 2 .720 0.0081"* 3. Level of education 0.53796 0.24619 2.185 0.0320* 4. Performance - 1.1512 0.68087 1.691 0.0950
status (PS) 5. Types of surgery 0 . 5 0 8 5 8 0.30698 1.657 0.1017 6. No adjuvant 0.42593 0.29511 1.443 0.1530
therapy
R (multiple correlation coefficent)=0.5819 (P-0.0000).
(b) The Mean Scores of the Four Categories Are Set as Independent Variables Representing QOL
Factor Regression Standard error t value P value coefficient
1. Social relationship 0.97360 0.14295 6 .811 0.0000"** 2. Age 0.02424 0.01068 2.270 0.0260* 3. Level of education 0.41662 0.21830 1.909 0.0601 4. Radiotherapy 0.82747 0.48815 1.695 0.0941 5. Performance -0.8771 0.61452 1.427 0.1575
status (PS)
R (multiple correlation coefficent)-0.6623 (P =0.0000). *P<0.05; **P<0.01; ***P<0.001. The results of the multiple regression analyses were those after stepwise selection of the variables.
150
Breast Cancer Vol. 2 No. 2 October 1995
fore, the PMC may appear to reflect the QOL item in this context. The item, however, was excluded in the calculation of the QOL score in this study.
The second question was, what are the factors that potentially influence the PMC and should be included as independent variables in multiple regression analysis. We thought it essential to accumulate information on the actual property, income or annuity of the patients for analysis, but we were unable to obtain them for ethical and technical reasons. We thought that the patients' level of education often reflected the status and could be a substitute for it. Another important factor to be considered was cost. As Eisenberg ~) noted, there are mainly four types of costs: ie, direct medical costs, direct nonmedical costs, indirect morbidity and mortali ty costs, and indef- inite costs. He also pointed out that a substantial portion of the direct costs is for nonmedical services such as food, transportation, lodging, family care, home aides, and clothing, which appear as consequences of the illness but which do not involve purchasing medical services. Among these costs, only direct medical costs were available and used in this study.
The results of the present study revealed that the QOL, especially social aspects of QOL, seemed to be the most important factor influenc- ing the PMC of the subjects. However, such a relationship was not predictable, because the question asking about the PMC was excluded in the calculation of the QOL score. Furthermore, the total omission of the QOL score during the calculation of the multiple regression resulted in a too low multiple correlation coefficient (R) to predict the PMC (data not shown). These results may suggest that the medical cost, at least from the viewpoint of the patients, is not an indepen- dent attribute of their QOL.
The multiple regression analyses in the present study indicated that age was also a significant factor influencing the PMC, because elderly patients tended to have lower PMC. How do we interpret this result? We noticed that there was a positive relationship between age and the social aspect of QOL in another QOL study of patients with advanced or recurrent patients with breast cancer 15). Therefore, age can be related to the PMC, since the PMC was closely associated with the social aspects of QOL in this study. Another reason might be that the direct medical costs are
almost zero in the elderly patients (especially those more than 70 years of age). From a societal point of view, Desch et a114) reported in their cost effectiveness analysis of breast cancer treatment that the benefits of adjuvant chemotherapy decline steadily from age 60 to 80 and the average survival benefit never exceeds the average dura- tion of chemotherapy treatment, while some researchers 1~-19) stressed that elderly patients should be given more intensive therapy because most of them are able to tolerate chemotherapy without adverse physical or psychosocial conse- quences. These controversies can be resolved by considering the cost-effectiveness or cost-benefit of cancer treatments from the viewpoints of both the society and the patient.
The results of the present study also revealed that patients with a higher level of education, and therefore with a better financial situation, had a lower PMC. Kiebert el aF ~ reported, in their study investigating factors influencing patients' treatment preference, that for persons with a lower level of education, the presence of children, the disease related chances of survival, and the baseline levels of QOL were more important considerations than they were for persons with a higher level of education.
Unexpectedly, the DMC, the BDMC and the DMCP were not shown to have significant associ- ations with the PMC by the multiple regression analyses. This result can be interpreted to mean that the distribution of the actual burden of medical cost in each patient was complex: ie, the actual refunded rate of medical cost is subtly different among the companies in which patients those who support them are working. Another reason may be that some patients make contracts with the medical insurance organizations by themselves.
In conclusion, the results of the present study suggest that, when we consider evaluating the cost in cancer treatment for post-surgical breast cancer patients we should take into account the patients' QOL, age, and their level of education.
Acknowledgment
We are grateful to our colleagues at Kawasaki Medical School for their helpful suggestions.
151
Shimozuma K, et al Medical Economics and Quality of Life
References
1) Goldhirsch A, Gelber RD, Simes R J, et a/ for The International Breast Cancer Study Group: Costs and benefits of adjuvant therapy in breast cancer; A quality-adjusted survival afialysis. J Clin Oncol 7:36- 44, 1989.
2) Hillner BE, Smith T J: Should women with node-- negative breast cancer receive adjuvant chemother- apy?; Insights from a decision analysis model. Breast Cancer Res Treat 23:17-27, 1992.
3) Hillner BE, Smith T J, Desch CE: Assessing the cost effectiveness of adjuvant therapies in early breast cancer using a decision analysis model. Breast Cancer Res Treat 25:97-105, 1993.
4) Desch CE, Hillner BE, Smith T J, et al: Should the elderly receive chemotherapy for node-negative breast cancer?; A cost-effectiveness analysis examin- ing total and active life-expectancy outcomes. J Clin Oncol 11:777 782, 1993.
5) Eisenberg JME: Clinical economics; A guide to the economic analysis of clinical practices. JAMA 262: 2879-2886, 1989.
6) Noguchi M, Saito Y, Nishijima H, et al: The psycho- logical and cosmetic aspects of breast conserving therapy compared with radical mastectomy. Surg
Today 23:598-602, 1993. 7) Noguchi M, Kitagawa H, Kinoshita K, et al:
Psychologic and cosmetic self-assessments of breast conserving therapy compared with mastectomy and immediate breast reconstruction. J Surg Oneo/ 54:260- 266, 1993.
8) Shimozuma K, Sonoo H, Ichihara K, et al: Analysis of factors associated with quality of life in breast cancer patients after surgery. Breast Cancer 1:123-129, 1994.
9) Shimozuma K, Sonoo H, Ichihara K, e t a / : The impacts of breast conserving treatment and mas- tectomy on the quality of life in early-stage breast cancer patients. Breast Cancer 2:35-43, 1995.
10) Union Internationale Contre le Cancer, Breast (ICD-O 174). In: Harmer MH ed, TNM Classification of Malignant Tumours, 4th ed, Springer, Berlin, pp93-99, 1987.
11) Kurihara M, Eguchi K, Shimozuma K, et al: The QOL questionnaire for cancer patients treated with anti- cancer drugs. J Jpn Soc Cancer Ther 28:1140 1144, 1993 (in Japanese).
12) Kurihara M, Shimizu H, Tsuboi K, et al: Assessment of quality of life in protocols for cancer therapy. CRC 1:174-181, 1992 (in Japanese).
13) Lorish CD, Maisiak R: The face scale; A brief, nonver- bal method for assessing patient mood. Arthritis Rheum 29:906 909, 1986.
14) Aaronson NK, Ahmedzai S, Bergman B, et al for the
NAME: DATE : / /
AGE : - - SEX : 1. MALE 2, FEMALE B.W. : Kg
This quest ionnaire is being done to help us understand your present state.
Please read the quest ions and circle the number above the scale wh ich best describes your state dur ing the past several days.
(Your privacy wil l be str ict ly protected and there wi l l be no negative inf luence on your medical treatment, so please answer these quest ions freely w i thou t concern.)
(dur ing the past several days) 1. Have you been able to perform
normal daily life activit ies ?
2. Have you been able to go Out by yourself ?
3. Have you been able to go for a 30 minute wa lk ?
4. Has it been hard for you to wa lk even a short d is tance?
5. Have you been able to go up a n d
down the stairs ?
6. Have you been able to take a bath by yourself ?
7. How wel l have you felt ?
8. Have you had a good appet i te?
9. Have you enjoyed your meals?
10. Have you experienced vomi t ing?
1 I . Have you lost we ight ?
1 2 . Have you slept wel l ?
2
Completely Unable
2
Completely Unable
2
Completely Unable
4
Not At A"
2
Completely Unable
2 i
Completely Unable
I 2 i i
Extremely Poor
1 2
ExtremeW Poor
1 2
Not At All
5 4
Not At All
5 4 , =
Not At All
1 2
Not At All
3 4 5
Completely Able
3 4 5
Completely Able
3 4 5
Completely Able
3 2 1
A Great Deal
3 4 5
Complet ely Able
4 5 i i
Completely Able
4 5 i i Extremely Well
4 E
Extremely Good
4 5
A Great Deal
2 1
Very Often
2 ] i i i
A Great Deal
4 5
Extremely Well
(dur ing the past several days)
13. Have you been absorbed in any th ing ?
14.
15.
16.
1 7 .
1 8 .
19.
Have you coped wel l w i th everyday stress ?
Do yOU feel unable to concent ra te?
Are You encouraged by anyone or anyth ing (family. friends, religion, hobbies, e tc . )?
Have you felt ill at ease about the condit ion of your disease?
Have you been unwi l l ing to meet anyone other than your family ?
How much trouble does your family have to
1 2 3 4 5
Not At All A Great Deal
1 2 3 4 5
Not At All Extremely Well
5 4 3 2 1
Not At All A Great Deal
i 2 3 4 5
Not At All A Great Deal
5 4 3 2 1
Not At All A Great Deal
5 4 3 2 1 , i i i J
Not At All A G~eat Deal
5 4 3 2 1 take over your medical t reatment ? None A Great Deal
20. Are you anxious about your social life 5 4 3 2 1 in the fu tu re? Not At All A Great Deal
21. Are you worried about the medical costs E 4 3 2 1 of your t reatment ? Not i t = i = i ' All A Great Deal
2 2 . Please circle the number of the face expressing your state dur ing the past
5 4 3 2 t
* At last. please confirm that you have answered all of the questions.
[A co lumn fil led out by doctors or nurses ]
c.ba" B . w . : p s 1 . inpatient: Kg2" outpat ient e. Remarks :
d. Date : / / Recorder :
Appendix 1. English edition of the QOL-ACD (The QOL Questionnaire for Cancer Patients Treated with Anticancer Drugs). The PMC (perception on medical cost) was examined by reviewing the patients' answers to the 21st question.
152

Breast Cancer Vol. 2 No. 2 October 1995
European Organization for Research and Treatment of Cancer Study Group on Quality of Life: The Eur- opean organization for research and treatment of cancer QLQ-C30; A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365-376, 1993.
15) Shimozuma K, Sonoo H, Ichihara K: Analysis of the factors influencing the quality of life of patients with advanced or recurrent breast cancer. Surg Today. In press.
16) Nerenz DR, Love RR, Leventhal H, et al: Psychosocial consequences of cancer chemotherapy
for elderly patients. Health Services Res 20:961-976, 1986.
17) Ganz PA, Shagg CC, Heinrich RL: The psychosocial impact of cancer on the elderly; A comparison with younger patients. J A m Geriatr Soc 33:429-435, 1985.
18) Begg CB, Carbone PP: Clinical trials and drug tox- icity in the elderly. Cancer 52:1986-1992, 1983.
19) Balducci L, Ades T, Carbone PP, et al: Issues in treatment. Cancer 68:2527-2529, 1991.
20) Kiebert GM, Stiggelbout AM, Kievet J, et al: Choices in oncology; Factors that influence patients' prefer- ence. Quality Life Res 3:175-182, 1994.
153





























