Embed Size (px)
Citation preview

Case ReportMediastinal Hematoma and Tracheal Compression followingTransradial Percutaneous Coronary Intervention
Nathaniel R. Smilowitz , Muhamed Saric, Michael J. Attubato, and James N. Slater
Division of Cardiology, Department of Medicine, NYU School of Medicine, NYU Langone Health, New York, NY, USA
Correspondence should be addressed to Nathaniel R. Smilowitz; [email protected]
Received 11 December 2017; Accepted 5 February 2018; Published 22 February 2018
Academic Editor: Ramazan Akdemir
Copyright © 2018 Nathaniel R. Smilowitz et al. *is is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Vascular complications from transradial percutaneous coronary intervention (PCI) are rare. We report an unusual case of stridorafter PCI due to brachiocephalic artery perforation, pseudoaneurysm formation, and development of a large mediastinal he-matoma with tracheal compression. Endovascular repair of the brachiocephalic artery was achieved with covered stent placementat the neck of the pseudoaneurysm. *is case highlights the importance of careful guide catheter placement from the right radialapproach. Ultimately, rapid diagnosis of vascular perforation, appropriate airway management, and prompt endovascular repairof the injured vessel is critical to the successful management of this life-threatening condition.
1. Introduction
Percutaneous coronary intervention (PCI) via the radialartery is an effective approach to treat patientswith coronaryartery disease. In large randomized trials of transradialversus transfemoral arterial access, patients who underwenttransradial catheterization had fewer major adverse car-diovascular events, fewer access site bleeding events, andlower mortality than those who underwent transfemoralcoronary intervention [1–3]. *us, transradial access hasbeen hailed as the preferred approach to minimize vascularcomplications associated with cardiac catheterization.Major vascular complications of transradial arterial access,although rare, occur in approximately 0.2% of coronaryprocedures [4, 5]. Vascular perforation, one of the mostsevere complications of radial PCI, can occur followingaggressive manipulation of guidewires or catheters as theyare advanced through the radial, brachial, subclavian, andbrachiocephalic arteries. Complications typically occurwhen wires or catheters shear the arterial wall in looped,tortuous, or small caliber arterial segments. In this report,wepresent an unusual case of stridor after PCI due to bra-chiocephalic artery perforation, pseudoaneurysm forma-tion, anddevelopment of a largemediastinal hematomawithtracheal compression.
2. Case Report
A 69-year-old man with a history of hypertension, dysli-pidemia, and type 2 diabetes mellitus presented withlifestyle-limiting angina. He underwent diagnostic coronaryangiography that revealed stenoses of the left anteriordescending (LAD) coronary artery, ramus intermediuscoronary artery, and the distal right coronary artery (RCA).Coronary artery bypass grafting was recommended, but thepatient refused surgery and elected for percutaneous cor-onary intervention (PCI) instead. Initially, transradial PCI ofthe LAD and ramus coronary arteries was performed withplacement of drug-eluting stents in each vessel. *e patientwas discharged on aspirin and ticagrelor with a plan forstaged coronary intervention of the distal RCA at a later date.
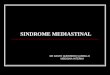
*ree months after the initial coronary intervention, thepatient returned for planned PCI of the distal RCA stenosis.Access was again obtained in the right radial artery witha short 6 French slender sheath. After routine diagnosticcoronary angiography confirmed a severe stenosis in thedistal RCA (Figure 1(a)), bivalirudin was administered. A 6French AL 0.75 guide catheter (Medtronic, Minneapolis,MN, USA) was advanced over an exchange length 0.035″J-wire, but could not be delivered to the ascending aorta dueto resistance in the brachiocephalic artery. *e guide was
HindawiCase Reports in CardiologyVolume 2018, Article ID 6790120, 4 pageshttps://doi.org/10.1155/2018/6790120

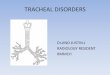
removed and exchanged for a 6 French JR 4 guide catheter(Medtronic, Minneapolis, MN, USA), which was easilyadvanced into the ascending aorta and used to engage theostium of the RCA without complication. Next, a standard0.014″ Run*rough coronary guidewire (Terumo, Tokyo,Japan) was placed in the distal RCA, and percutaneouscoronary intervention was performed. *e lesion was pre-dilated with a 2.0mmMaverick compliant balloon (BostonScientific,Marlborough,MA, USA) inflated to 10 ATM, anda Xience Alpine 2.75×12mm cobalt chromium everolimusdrug-eluting stent (Abbot Vascular, Abbott Park, IL, USA)was delivered to the lesion and deployed at 16 ATM. *erewas a good angiographic result of the distal RCA withno residual stenosis (Figure 1(b)). Immediately followingcompletion of the procedure, the patient reported an epi-sode of chest discomfort, a new cough, bilateral expiratorywheezes, and respiratory stridor. A transient episode ofhypotension was noted but resolved without intervention.*e patient was rapidly administered IV methylpredniso-lone, famotidine, diphenhydramine, and inhaled racemicepinephrine for presumed allergic reaction to iodinatedcontrast. Although his symptoms largely improved, stridorpersisted. Urgent otolaryngology consultation was obtainedfor the evaluation of possible laryngeal edema, but flexiblefiber-optic laryngoscopy was unremarkable. Next, chest ra-diography was promptly obtained, which revealed a markedlywidened superior mediastinum (Figure 2).
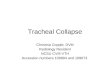
Based on the findings on chest radiography, trans-esophageal echocardiography (TEE) was urgently performed.Echocardiography revealed no evidence of aortic dissection,but vague echodensities were noted anterior to the right heartsuggestive of a hematoma.*us, computed tomography (CT)of the chest without intravenous contrast was performed toobtain cross-sectional imaging of the mediastinum. *e chestCTrevealed a large hyperdense region surrounding the tracheasuggestive of an anterior mediastinal hematoma, resulting insevere airway compression (Figure 3(a)). Due to the severity oftracheal compression, the decision was made to perform
endotracheal intubation and mechanical ventilation andtransfer to the intensive care unit.After intubation, a repeatCTof the chest with administration of intravenous contrast wasnotable for a small pseudoaneurysm arising from the inferioraspect of the brachiocephalic artery, as well as significantnarrowing of the distal trachea below the endotracheal tube(Figure 3(b)).
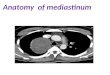
After consultation with cardiothoracic and vascularsurgery, the decisionwasmade to pursue endovascular repairof the brachiocephalic artery pseudoaneurysm and presumedsite of vascular perforation. Access was obtained in the leftcommon femoral artery, and angiography of the brachio-cephalic arterywas performed,which confirmed the presenceof a brachiocephalic artery pseudoaneurysm (Figure 4(a)).Next, a SupraCore wire (Abbot Vascular, Abbott Park, IL,USA) was placed in the right subclavian artery and a10× 40mm iCAST covered stent (Atrium Medical, Hudson,NH, USA) was deployed across the neck of the pseu-doaneurysm. *e covered stent was postdilated with a12× 20mm Armada balloon (Abbot Vascular, Abbott Park,
Distal RCA stenosis
Guide catheter
(a)
Guide catheter
Distal RCA stent
(b)
Figure 1: Coronary angiography of the right coronary artery in the left anterior oblique view before (a) and after (b) percutaneous coronaryintervention and drug-eluting stent placement.
Widenedmediastinum
Cardiacsilhouette
Figure 2: Chest radiography (AP orientation) demonstrating awidened superior mediastinum.
2 Case Reports in Cardiology

IL, USA). Following the intervention, there was an excellentangiographic result with preserved subclavian and carotidrunoff (Figure 4(b)).Aspirinwas continued; P2Y12 inhibitorswere temporarily withheld.
Due to persistent tracheal compression after endovas-cular repair of the brachiocephalic artery, a TracheobronxaneDumon silicone tracheal stent (Novatech, La Ciotat, France)was inserted by interventional pulmonology to maintainairway patency while the mediastinal hematoma resorbed.Over the ensuring days, serial imaging demonstrated nofurther enlargement of the mediastinal hematoma, and dualantiplatelet agents were resumed. *e tracheal stent wasretrieved and removed after 12 days. *e patient was ulti-mately discharged to inpatient rehabilitation on hospitalday 19.
3. Discussion
Vascular perforation associated with delivery of a 6 Frenchguide catheter in the subclavian and brachiocephalic arteriesis rare, with few cases reported in the literature [6–8]. In thiscase, brachiocephalic artery perforation resulted in pseu-doaneurysm formation and a large mediastinal hematomawith tracheal compression and stridor. *is highlights theimportance of careful guide catheter placement from theright radial approach. When guide catheters are advancedthrough tortuous subclavian and brachiocephalic arteries,
the application of forward pressure against resistance canlead to vascular complications, even when a guidewire isappropriately positioned in the ascending aorta. If resistanceis encountered, fluoroscopy should be used to confirm therelative positions of the distal guidewire and guide catheter,and care should be taken to ensure appropriate guidewireposition before advancing the guide further. Abduction ofthe arm and deep inspiration may also facilitate advance-ment of guide catheters to the ascending aorta. When theguide catheter cannot be easily advanced, balloon-assistedtracking (or similar techniques employing a low-profile0.035″ compatible support catheter protruding throughthe lumen of a standard 6 Fr guiding catheter) can smooththe transition at the distal tip of the guide catheter. *is canprevent vessel shearing from the “razor effect” at the distaltip of the guide catheter and minimize vascular trauma.Hydrophilic guiding catheters may also be used to passtortuous subclavian or brachiocephalic anatomy. Rigidguide catheters, larger French sizes, and those with a moretortuous or curved shape at the distal tip may be most likelyto cause traumaduring catheter delivery. In the present case,the Amplatz shape of the initial guiding catheter may haveplayed a role in the resulting perforation.
*is report also illustrates the importance of main-taining a broad differential diagnosis when respiratorydistress occurs after PCI. In this case, an allergic reaction toiodinated contrast was initially suspected when stridor andwheezing developed after completion of the procedure.Reactions to contrast media affect approximately 1 in every500 patients undergoing coronary angiography in the car-diac catheterization laboratory, and the clinical presentationcan range from urticaria to laryngeal edema and bron-chospasm to cardiovascular shock and respiratory arrest [9].*e likelihood of an anaphylactoid reaction to contrastmedia is not necessarily related to contrastmedia dose, nor isit always an immediate response to contrastmedia exposure.When angioedema is suspected, patients require promptairway evaluation and may require tracheal intubation tomaintain airway patency. In this case, flexible fiber-opticlaryngoscopy was urgently performed to exclude thisdangerous diagnosis. Once it was evident that laryngealedema was absent and anaphylactoid reaction to contrastmedia was unlikely, alternate diagnoses were considered.Ultimately, this rare vascular complication of PCI was onlyidentified after a series of diagnostic imaging studies, in-cluding chest radiography, transesophageal echocardiog-raphy, computed tomography, and finally, invasiveangiography. *erefore, all providers in the cardiac cathe-terization laboratory should be aware of procedural risksspecific to the transradial approach.
In conclusion, vascular perforations due to guidecatheter advancement from the right radial artery are rare. Inthis case, a 6 French AL 0.75 guide catheter led to bra-chiocephalic artery perforation, pseudoaneurysm formation,and a large mediastinal hematoma with tracheal compres-sion. Prompt recognition, appropriate airway management,and endovascular repair of the injured vessel is critical to thesuccessful management of this potentially life-threateningcondition.
Trachea
Descending aorta
AorticarchMediastinal
hematoma
(a)
Ascendingaorta
Le�ventricle
Brachiocephalic artery
pseudoaneurysm
(b)
Figure 3: Computed tomography (CT) of the chest without intra-venous contrast demonstrating a hyperdense region surrounding thetrachea suggestive of an anterior mediastinal hematoma (a). Computedtomography (CT) of the chest with intravenous contrast demonstratinga small pseudoaneurysm arising from the inferior aspect of the bra-chiocephalic artery (b).
Case Reports in Cardiology 3

Conflicts of Interest
Dr.Muhamed Saric serves on a speaker bureau for Philips andMedtronic and an advisory board for Siemens. Dr. MichaelJ. Attubato is a consultant to Boston Scientific.*e remainingauthors have no relevant conflicts of interest to disclose.
References
[1] M. Valgimigli, A. Gagnor, P. Calabro et al., “Radial versusfemoral access in patients with acute coronary syndromesundergoing invasive management: a randomised multicentretrial,” !e Lancet, vol. 385, no. 9986, pp. 2465–2476, 2015.
[2] G. Ferrante, S. V. Rao, P. Juni et al., “Radial versus femoralaccess for coronary interventions across the entire spectrumof patients with coronary artery disease: a meta-analysis ofrandomized trials,” JACC: Cardiovascular Interventions, vol. 9,no. 14, pp. 1419–1434, 2016.
[3] G. Ando and D. Capodanno, “Radial access reduces mortalityin patients with acute coronary syndromes: results from anupdated trial sequential analysis of randomized trials,” JACC:Cardiovascular Interventions, vol. 9, no. 7, pp. 660–670, 2016.
[4] E. Tatli, A. Buturak, A. Cakar et al., “Unusual vascular com-plications associated with transradial coronary proceduresamong 10,324 patients: case based experience and treatmentoptions,” Journal of Interventional Cardiology, vol. 28, no. 3,pp. 305–312, 2015.
[5] T. Patel, S. Shah, K. Sanghavi, and S. Pancholy, “Managementof radial and brachial artery perforations during transradialprocedures–a practical approach,” Journal of Invasive Cardi-ology, vol. 21, no. 10, pp. 544–547, 2009.
[6] N. Habib, A. Jerzewski, E. M. Koomen et al., “Subclavian arteryperforation complicating coronary angiography,” NetherlandsHeart Journal, vol. 20, no. 6, pp. 288–290, 2012.
[7] F. Farooqi, J. Alexander, and A. Sarma, “Rare vascular perforationcomplicating radial approach to percutaneous coronary angio-plasty,” BMJ Case Reports, vol. 2013, p. bcr2012007732, 2013.
[8] M. A. Abdool, S. Morrison, and H. Sullivan, “Iatrogenicperforation of subclavian artery as a complication of coronaryangiography from the radial route, endovascularly repairedwith a covered stent-graft,” BMJ Case Reports, vol. 2013,p. bcr2012007602, 2013.
[9] J. E. Goss, C. E. Chambers, and F. A. Heupler Jr., “Systemicanaphylactoid reactions to iodinated contrast media duringcardiac catheterization procedures: guidelines for prevention,diagnosis, and treatment. Laboratory Performance StandardsCommittee of the Society for Cardiac Angiography and In-terventions,” Catheterization and Cardiovascular Diagnosis,vol. 34, no. 2, pp. 99–104, 1995.
Brachiocephalic arterypseudoaneurysm
Aorticarch
Subclavian artery
Carotid artery
(a)
Carotid artery
Subclavian artery
Brachiocephalic arterystent
(b)
Figure 4: Angiography of the brachiocephalic artery demonstrating a small pseudoaneurysm (a).*ere was an excellent angiographic resultafter deployment of a covered stent (b).
4 Case Reports in Cardiology

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com