Embed Size (px)
Citation preview

REVIEWwww.nature.com/clinicalpractice/cardio
Mechanisms of Disease: β-adrenergic receptors—alterations in signal transduction and pharmacogenomics in heart failureDavid S Feldman*, Cynthia A Carnes, William T Abraham and Michael R Bristow
INTRODUCTIONHeart failure (HF) is the final common pathway for many cardiovascular patients, and for more than a decade it has been the most frequent hospital diagnosis in patients older than 65 years.1 Physiologic and molec-ular analyses indicate that the β- adrenergic signaling cascade is an important regulator of myo cardial function, and several lines of inves-tigation support alterations in β- adrenergic receptor (β-AR) signal- transduction mech-anisms as primary determinants of the natural history of HF. During progressive HF, a reproducible collection of biochemical defects arises in the β-AR signaling pathway.2 Cellular analysis of heart tissue has shown a down regulation of β1-ARs in myo cardial membranes and a decrease in the functional coupling of the remaining receptors to the Gαs-adenylyl cyclase system.3 In previous reports from clinical studies, an upregula-tion or activation of the adrenergic nervous system has been directly correlated with shortened survival.4 This finding has been further substantiated in large clinical trials, in which β-blocker therapy has been shown to decrease morbidity and mortality significantly for patients with left-ventricular dysfunction and HF.5,6
Although significant advances have been made in the pharmacologic and device-based treatment of HF, our understanding of the full range of the signaling and genomic mecha-nisms involved in HF progression is incom-plete and mortality remains high. Limited therapeutic options for severe HF, and an inability to substantially and consistently reverse pathologic remodeling and myocardial dysfunction in most HF patients, continue to challenge cardiovascular scientists and prac-titioners. Here, we discuss the current under-standing of β-adrenergic signal- transduction pathways, the best-described β-AR poly-morphisms and therapies that target the β-AR pathway in HF.
SUMMARYβ-adrenergic signaling is an important regulator of myocardial function. During the progression of heart failure (HF), a reproducible series of biochemical events occurs that affects β-adrenergic receptor (β-AR) signaling and cardiac function. Furthermore, there are pathophysiologic alterations in the expression and regulation of proteins that are regulated by β-ARs during HF. Analyses of these complex signaling pathways have led to a better understanding of HF mechanisms and the use of β-adrenergic antagonists, which have notably altered HF-related morbidity and mortality. Despite therapeutic advances that have affected β-AR signaling, HF remains a leading cause of hospitalization and a principal cause of death in industrialized nations. In this review, we summarize current insights into β-adrenergic signal-transduction pathways, the best-described β-AR polymorphisms, and therapies that target the β-AR pathway in HF.
KEYWORDS β-adrenergic receptor, gene polymorphism, heart failure, pharmacogenomics, signal transduction
DS Feldman is the Director of Heart Failure and Cardiac Transplantation, CA Carnes is an Associate Professor of Pharmacy and Biophysics and WT Abraham is the Director of Cardiovascular Medicine, at Ohio State University, Columbus, OH, USA. MR Bristow is a professor of Cardiovascular Medicine at the University of Colorado Health Science Center, Denver, CO, USA.
Correspondence*Davis Heart and Lung Research Institute, Suite 200, 473 West 12th Avenue, Division of Cardiology/Medicine, Ohio State University, Columbus, OH 43210, [email protected]
Received 14 February 2005 Accepted 23 June 2005
www.nature.com/clinicalpracticedoi:10.1038/ncpcardio0309
REVIEW CRITERIAMEDLINE searches were done for the terms “β-adrenergic”, “signal transduction”, “heart failure”, “genetic”, “therapy”, “therapeutic” and “heart”. All of the papers identified were full-text, English-language publications that were published between 1966 and May 2005. We also performed a manual search of references listed in the authors’ personal collections of resources.
SEPTEMBER 2005 VOL 2 NO 9 NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE 475
Nature Publishing Group© 2005

REVIEW
476 NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE FELDMAN ET AL. SEPTEMBER 2005 VOL 2 NO 9
www.nature.com/clinicalpractice/cardio
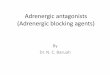
β-ADRENERGIC CELLULAR SIGNAL-TRANSDUCTION MECHANISMS IN HEART FAILUREThe human heart contains β1, β2 and β3 receptors.7 The ratio of β1 to β2 ARs in a normal heart is approximately 70:30.8 The β3 receptor is pre dominantly inactive during normal physiologic conditions and its role in HF remains unclear.9–11 Once a specific β-AR is activated, cellular changes are initiated by the activation of one or more heterotrimeric G proteins (Figure 1).
β1-ARs activate Gs proteins, thereby producing an increase in cyclic AMP (cAMP) via adenylyl cyclases; β2-ARs use both Gi and Gs protein signaling.12–14 Metaphorically, Gs signaling acts as the ‘accelerator’ for the receptor and the Gi signaling pathway acts as the ‘brake’. Gs signaling initiates the activation of the second-messenger protein kinase A (PKA) and cAMP, which modu-late the activity of several proteins essential for cardiac function, including L-type calcium channels, ryanodine receptors, phospholamban, troponin I, hyperpolarization-activated cyclic-nucleotide-gated channels, and myosin-binding
proteins.13,15,16 In addition, an increasing body of evidence indicates that cAMP-independent pathways also participate in numerous cellular processes, many of which are pathologic. These intracellular events subsequently lead to observable changes in the function of the whole organ or system (e.g. an increase in heart rate or myocardial contractility). Gi signaling decreases cAMP levels, activates mitogen- activated protein kinases (MAPKs), and helps to regulate receptor signaling and the activation of nuclear transcription. As mentioned above, in patients who develop HF, β1-ARs are down regulated in myocardial membranes and the functional coupling of the remaining receptors to the Gαs-adenylyl cyclase system is decreased.17 In addition, levels of both Gαi (particularly Gαi2) signaling proteins and the G-protein receptor kinases (GRKs) are increased.18
Taken together, these changes serve to desens-itize the β-adrenergic signal-transduction pathway and result in cardiac hypofunction when stimulated by the adrenergic neuro transmitter norepinephrine or other cate cholamines.19
L-type calcium channel
P
PP
AC
cAMP
cAMPand/orPKA
ATP
RyR
PLB SERCA
Sarcoplasmicreticulum
Sarcomere
Myofilament proteins
PKA
+ Gαs– Gαi
+
HCN channel
β-adrenergic receptor
βγ
Ca2+
Ca2+ Ca2+
Ca2+
Ca2+
Figure 1 Schematic of β-adrenergic and calcium intracellular trafficking in myocytes, showing ion channels, contractile pathways and β-adrenergic signal transduction. This representation focuses on many of the consensus signaling pathways that have been identified between adrenergic G-protein-coupled receptors, two specific membrane ion channels (hyperpolarization-activated cyclic-nucleotide-gated cation channels and L-type calcium channels), the sarcoplasmic reticulum and cardiac sarcomeres. AC, adenylyl cyclase; β and γ, G-protein subunits; Ca2+, calcium ions; cAMP, cyclic AMP; Gαi and Gαs, G protein α-subunit subtypes; HCN, hyperpolarization-activated cyclic-nucleotide-gated cation channel; P, phosphorylated; PKA, protein kinase A; PLB, phospholamban; PP, protein phosphatase; RyR, ryanodine receptor; SERCA, sarcoendoplasmic reticulum Ca2+-ATPase.
Nature Publishing Group© 2005

REVIEW
SEPTEMBER 2005 VOL 2 NO 9 FELDMAN ET AL. NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE 477
www.nature.com/clinicalpractice/cardio
Feedback inhibition is a basic principle of β-adrenergic signaling and is an ideal target for altering signal-transduction mechanisms. These receptors can be pharmacologically targeted by modification of the signaling activity via the unique internal inhibitors, the GRKs. In HF patients, it has been observed that GRKs are upregulated. Raf-kinase-inhibitor protein (RKIP) is one specific inhibitor of GRK2. After stimulation of the AR, RKIP dissociates from its known target, RAF1, and subsequently associates with GRK2 and blocks its activity. This switch is triggered by PKC-dependent phosphorylation of RKIP at Ser153. In addi-tion, GRK carboxy-terminus inhibitors have also been used successfully in animal models. The attenuation of GRK2 activity functions as a negative- feedback pathway affecting many portions of the adrenergic signaling cascade, as GRK2 interacts with receptors, free Gβ and Gγ subunits, activated Gαq subunits, phosphatidyl-inositol 4,5-bisphosphate (PIP2), PKC and calmodulin.20–22 These therapeutic strategies might provide new interventions to modulate adrenergic signaling in HF.
Receptor-generated signaling is often over-simplified under the assumption that one external stimulus produces a single chain of events, a single perceivable product or a lone event. In reality, the perceived global activity of any single cell is the summation of a multi-tude of serial events. The interactions of β-ARs and other signaling pathways can be regulated in two main ways—spatially or temporally. Several lines of evidence support discrete spatial interactions as regulators of cell signaling (e.g. docking proteins and protein proximity). The stimulation of β2-ARs by Gs leads to differences in levels of cAMP, heart rate and inotropy, which have been observed in experimental models. Furthermore, other studies in transgenic mice show that low-level overexpression of β1-ARs leads to HF, whereas similar levels of over-expression of β2-ARs produce hypertrophy but not HF.23–25 Time-dependent signaling also regulates signal transduction by altering receptor activity. These signaling alterations can be divided into receptor sequestration, downregulation and desensitization.13,26
Since increased sympathetic activity and desensitization of β-adrenergic signal trans-duction are fundamental abnormalities in the failing heart, one or both of these dysregulated mechanisms seem feasible targets for therapy.
Therefore, some investigators have sought to inhibit β-AR signaling and others have attempted to restore β-AR sensitivity. The classic model of β-AR signaling in HF suggests that chronic stimulation of β-ARs leads to chronic G-protein activation, and desensitization or downregulation is a physiologically adap-tive mechanism that attempts (but ultimately fails) to stop progressive HF. An alternative explanation, however, is that densensitization is adaptive only in the short term, but ultimately is chronically maladaptive and results in the dysregulation of calcium handling and other cellular effects, leading to the progression of myocardial failure or a cardiomyopathy pheno-type. These two hypotheses represent the main mechanisms of β-AR signaling currently under investigation in HF. Data supporting these concepts are presented below.
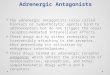
The waning of β-AR signaling during chronic HF is accomplished by a co-ordinated series of events (Figure 2). Desensitization can be classified as heterologous or homologous.26 Heterologous desensitization is mediated by second-messenger-dependent and PKA- dependent signaling. Stimulation of the receptor is not required for this desensitization to occur. Simultaneously, PKA desensitizes β-ARs by the phosphorylation of L-type calcium channels and intracellular calcium-regulatory proteins (Figure 2). Homologous, or ligand-mediated desensitization, involves the phosphorylation of β-AR by GRKs and the subsequent binding of β-arrestin-regulatory proteins.18,26,27
The principal function of the GRKs in adren-ergic signaling is now recognized as increasing receptor affinity for β-arrestin.28 The poten-tial relevance of GRK as a therapeutic target has been exemplified in Grk-transgenic mice models. Specifically, alterations in the β1-adrenergic receptor kinase (Adrbk1) and Gprk5 genes have been shown to significantly alter signal- transduction mechanisms in mice with cardiopulmonary disease.22,28 The binding of β-arrestin to the AR complex, rather than GRK phosphorylation, leads to homologous desensiti-zation. The arrestins accomplish these alterations in cell signaling by forming scaffolds of proteins, which start at the cell surface and end at the nucleus.29 Data indicate that β-arrestins regu-late MAPK activity, resulting in the formation of discrete MAPK pools in the cell. The MAPKs are involved in the trans duction of externally derived signals that regulate cell growth, division,
Nature Publishing Group© 2005

REVIEW
478 NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE FELDMAN ET AL. SEPTEMBER 2005 VOL 2 NO 9
www.nature.com/clinicalpractice/cardio
differentiation and apoptosis.25,30,31 Mammalian cells contain at least three main classes of MAPKs: externally regulated kinases, Jun kinases and p38.32 Once activated, MAPKs phosphory-late a range of membrane, cytoplasmic, nuclear and cyto skeletal substrate proteins. In some cases, the activated MAPKs can translocate to the nucleus, where they phosphorylate and activate nuclear transcription factors involved in DNA synthesis, hypertrophy and cell death. Whether desensitization of β-ARs and altera-tions in MAPK pathways are epiphenomena or are causal in HF remains unclear. The relation-ship between β-ARs, receptor signaling and MAPKs, and changes in cellular or genomic signaling during HF, continue to be topics of intense investigation.
DOWNSTREAM MECHANISMS IN HEART FAILUREAlterations in β-adrenergic signaling have been implicated in the development of apoptosis in several in vitro and in vivo experimental models, in which exposure to catecholamines has been shown to be toxic to cardiac myocytes and result in cell death.33,34 This toxic effect was initially reported in adult isolated feline myocytes. Use of a β-AR agonist resulted in spontaneous contractions followed by hypercontracture
and cell death.35 An α-AR antagonist had a slight blocking action on the toxic effects of nor epinephrine on cardiomyocytes, but a β-AR antagonist led to greater attenuation.34 Additional experiments to evaluate the phenom-enon of cell death following β-AR stimulation revealed DNA fragmentation and an increase in terminal-deoxynucleotidyl-transferase- mediated dUTP nick-end labeling (TUNEL assay) staining, consistent with apoptosis.34,35 In vivo experiments with isoproterenol, a β-AR agonist, also support a proapoptotic effect for excess β-AR stimulation. These findings have been attributed to direct cell-signaling mecha-nisms of β-ARs and seem to be independent of heart rate or myocardial ischemia.
The available experimental evidence indi-cates that β1-ARs, through Gs signaling, have proapoptotic effects. By contrast, β2-AR signaling, mediated by Gi, has antiapoptotic effects owing to the activation of Akt (PKB) and phosphatidylinositol 3-kinase (PI3) kinases,29,36 which can have protective or antiapoptotic effects.30,36 In reality, these signaling cascades are entwined. Views differ about which intracellular signaling pathways are prosurvival and which are proapoptotic. Furthermore, it is unclear whether apoptosis occurs as a result of the direct stimulation of one of these pathways, or owing
Desensitization
Heterologous Homologous
Internalization
Signalingscaffolding
Downstream effectorse.g. calcium signaling
Effectorse.g. PI3K, PDE
GRK
cAMPAC
H
PKA
+ Gαs+ Gαi
Ligand
β-arrestinP
PP
P
Figure 2 Schematic of the desensitization and intracellular trafficking of β-adrenergic receptors. Agonist occupancy of the adrenergic receptor is not required for protein-kinase-A-dependent desensitization. AC, adenylyl cyclase; cAMP, cyclic AMP; Gαi and Gαs, G protein α-subunit subtypes; GRK, G-protein-receptor kinase; H, conformational change due to ligand binding; P, phosphorylated; PDE, phosphodiesterase; PI3K, phosphatidylinositol 3-kinase; PKA, protein kinase A.
Nature Publishing Group© 2005

REVIEW
SEPTEMBER 2005 VOL 2 NO 9 FELDMAN ET AL. NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE 479
www.nature.com/clinicalpractice/cardio
to downregulation or an imbalance between competing signaling pathways. Although many investigators have focused on apoptosis, several other lines of investigation have shown that perturbations in β-ARs, specifically β1, are primary contributors to HF. Consequently, the signaling mechanisms mediated by cAMP or PKA and downstream phosphorylation have been intensely studied. In addition, gene-expression studies in the intact failing human heart indicate that β1-ARs are also coupled to the induction of a fetal pattern of gene expres-sion of the contractile proteins, consisting of upregulation of the fetal genes, β-myosin heavy chain and atrial natriuretic peptide (ANP), and downregulation of the adult genes, α-myosin heavy chain and sarcoendoplasmic reticulum Ca2+-ATPase 2a (SERCA2a).37,38 A reversal of this fetal pattern of gene expression could be one of the ways in which β-blocking agents improve the dilated cardiomyopathy phenotype in patients with HF.
PKA directly phosphorylates L-type calcium channels, phospholamban (an inhibitor of SERCA2a) and the ryanodine receptor, which collectively results in an increased calcium current and improved cardiac inotropy.39,40 When phospholamban is phosphorylated at Ser16, the SERCA2a protein is disinhibited, which allows maximum ATPase activity and sarcoplasmic calcium loading. This action leads to increased contractile function during systole.39 In chronic HF, phospho lamban is, surprisingly, underphosphorylated at Ser16, which, in turn, leads to hypofunction of SERCA2a. This underphosphorylation of phospholamban might be due to desensitiza-tion-related reduction in cAMP per unit adren-ergic stimulation in the sarcoplasmic reticulum compartment, an increase in protein phospha-tase 1 activity, or both.3 In addition, SERCA2a expression by the ATP2A2 gene is decreased in the failing human heart.37,41 Phosphorylation of phospholamban, gene therapy and recon-stituted SERCA2a have been proposed as therapeutic targets for HF, but there might be differences between mouse models and humans in this regard.39,40,42
Several other calcium-handling proteins have been postulated to contribute to the patho genesis of HF. PKA phosphorylation of the protein phosphatase inhibitor 1 further enhances cardiac contractile function by inter-fering with the dephosphorylation effected by
protein phosphatase 1 at Ser16 on phosphol-amban. Although the exact role of protein phos-phatase inhibitor 1 in HF is unknown, there is empirically a twofold to fivefold upregulation of this protein in HF.39,43 Phosphorylation of the ryanodine receptor, hyperpolarization- activated cyclic- nucleotide-gated cation channels, the sodium proton exchanger NHE1 and the L-type calcium channel have all also been impli-cated in the pathogenesis of HF.13 Finally, the PKA- dependent phosphorylation of contractile proteins (e.g. troponin I and myosin-binding protein) facilitates the relaxation of cycling myofilaments.40
In summary, chronically elevated adren-ergic signaling and the subsequent desensitiza-tion of signal-transduction mechanisms leads to altered calcium homeostasis in the failing hypertrophied cardiac myocyte. The net effect of these changes is an increase in the intra-cellular calcium concentration during diastole. Ultimately, long-term organ and physiologic changes might be predominately caused by changes in transcription and protein transla-tion that are mediated by calcium-activated gene expression, resulting in the induction of a ‘fetal’ gene expression profile for the contractile proteins that directly contributes to contractile dysfunction and pathologic hypertrophy.38,41
PHARMACOGENOMICS AND FEATURES OF ADRENERGIC SIGNALINGGenomic alterations in adrenergic drug metabolismAlthough some HF patients respond favorably to drug and device therapies, the nonresponder rate for NYHA class III and IV HF patients could be 25–30%, which is similar to the nonresponder rate for device therapy.43,44 These results might be partly explained by genomic idiosyncrasies in drug metabolism or cardiac genomics. The metabolic pathways of carvedilol and meto-prolol, but not bisoprolol, use cytochrome P450 2D6 oxidation. This cytochrome is expressed by the CYP2D6 gene and 7–10% of white patients lack the active enzyme, whereas studies have shown that up to 29% of Ethiopians and approx-imately 3% of patients from central Europe have a gene duplication.45–47 Unexpectedly high or low drug concentrations might occur, there-fore, as a result of metabolic polymorphisms, which could alter the clinical response to such therapies. One study reported, however, that the CYP2D6 genotype did not result in a difference
Nature Publishing Group© 2005

REVIEW
480 NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE FELDMAN ET AL. SEPTEMBER 2005 VOL 2 NO 9
www.nature.com/clinicalpractice/cardio
in HF events during the titration of meto-prolol.48 For carvedilol, the situation is further complicated by the stereoselective metabolism of the R and S enantiomers, which have different affinities for different ARs.5
Adrenergic polymorphisms and implications for heart-failure patients’ outcomesThe genes that encode β-ARs in the heart contain many single-nucleotide polymorphisms, few of which have been extensively studied.49 The two best-described β1-AR receptor variants are Arg389→Gly and Ser49→Gly.13,50 The poly-morphism that results in Arg389→Gly is known to alter signaling mechanisms in vitro. The Gly389 variant produces a presumed protective phenotype, with an attenuated adenylate cyclase response in both white (25%) and black (42%) patients, whereas the Arg389 variant, when combined with an α2c-AR carboxy-tail deletion, can be deleterious under some conditions or in certain patients.51–53 Another clinically relevant polymorphism in the gene that encodes the β1-AR results in Ser49→Gly. This Gly49 variant has been associated with improved survival in HF patients, especially those who have been treated with β-AR blockers.54
The three best-described variants for the β2-AR are the Arg16→Gly, Gln27→Glu and Thr164→Ile mutations. In genetically engi-neered mice, the Ile164 variant resulted in attenuated receptor binding and a more favor-able phenotype.55 Patients without HF who were heterozygous for the Ile164 allele had a lower chronotropic response to a β2-AR agonist, reduced exercise capacity and possibly poorer survival than patients without this variant.56 The Gly16 and Gln27 variants have been associated with altered down regulation following agonist exposure and decreased exercise tolerance.53 The relevance of these poly morphisms will have to be substantiated in large, prospective clinical trials.
Therapeutic strategies targeted at the adrenergic signalβ-AR antagonists have been shown in clin-ical HF trials to result in reverse remodeling (i.e. decreased ventricular dimensions and improved systolic function), improvement in the myo cardial molecular phenotype, and reduced morbidity and mortality.5,6,38 These beneficial effects do not, however, extend to all β-AR antagonists. Specifically, treatment
with the β1-AR selective antagonists meto-prolol succinate and bisoprolol, have proven efficacy in this population. The nonselective β1-AR and β2-AR antagonist, carvedilol, which also has α1-AR antagonist and antioxidant activities, decreases morbidity and mortality in HF. The Carvedilol or Metoprolol European Trial (COMET)57 reported that carvedilol treat-ment was superior to metoprolol treatment in reducing mortality. Interpretation of this result is confounded, however, by the particular formu-lation of metoprolol and the dosing regimens that were used in the trial, which resulted in a lower β1-AR blocking dose for metoprolol than for carvedilol.
Bucindolol is similar in many respects to carvedilol in its pharmacology; it is a non selective β-AR antagonist with vaso dilator properties, but with much weaker α1-AR antagonist activity. In addition, bucindolol is unique among the β-blockers that are used to treat HF in that it has sympatholytic properties and substantially lowers norepinephrine levels.58 The β-Blocker Evaluation of Survival Trial (BEST)6 of bucindolol, however, which was conducted in a mixed population of patients with advanced NYHA class III or IV HF, did not show a statistically significant survival benefit. The lower-than-expected reduction in mortality for bucindolol in the BEST trial has been attributed to its sympatholytic properties, which were more pronounced in class IV patients and black patients.58Alternatively, the partial agonist activity of bucindolol might have contributed to the lower than expected efficacy.59
Another issue that complicates β-AR antag-onist therapy in HF is the presence of poly-morphisms in the genes that encode the β-ARs. As discussed above, there is increasing evidence that a beneficial therapeutic response might depend on these polymorphisms.60 Therefore, identification of the genotype of a given patient has the potential to identify the optimum candidates for such therapies. β-AR antago-nists have been the most important pharma-cologic advance in the lowering of morbidity and mortality in HF. It therefore stands to reason that functionally important β-AR poly-morphisms would affect β-blocker clinical responses. Support for this hypothesis has been obtained from the BEST-DNA substudy61 of 1,040 patients, and through the work of Terra and colleagues.62 In BEST-DNA, a greater clinical response to bucindolol was seen in the
Nature Publishing Group© 2005

REVIEW
SEPTEMBER 2005 VOL 2 NO 9 FELDMAN ET AL. NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE 481
www.nature.com/clinicalpractice/cardio
47% of patients who were homozygous for the high-functioning Arg389 β1-AR than in those who were hetero zygous or homozygous for the Gly389 β1-AR. The reduction in mortality in Arg389 homozygotes was 38%, which is the largest effect on survival that has been measured, so far, in a mortality study in HF. The work of Terra and colleagues corroborated these results by showing a greater reduction of end-diastolic and end-systolic diameters in patients with Arg389 and Gly49 variants. In contrast to these findings, both the Metoprolol Controlled Release/Extended Release Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF) polymorphism substudy63 and a clinical investigation carried out by de Groote and colleagues64 showed no advantage with β-blocker therapy for any polymorphism studied. The differences between these four studies can be explained partly by variation in the observed endpoints, the investigational models and the pharmacology of the drugs that were used.
Another approach to the correction of adrenergic dysfunction in the failing heart is the combined use of a low dose of a phospho-diesterase type 3A inhibitor and a β-blocker.65 The hypothesis behind this treatment strategy is to inhibit the adverse effects of β1-AR stimu-lation while increasing cAMP and phospho-lamban phosphorylation in the sarcoplasmic reticulum (through β2-AR signaling).60 A large phase III clinical trial using this strategy has been completed and the results will be reported soon.
In addition to β-ARs, many other β- adrenergic signal-transduction therapeutic targets are under investigation. GRK antagonists (such as the peptide inhibitor of β-AR kinase, β-ARKct) and modulators of the calcium- regulatory proteins (e.g. SERCA2, phospholamban and protein phosphatase inhibitor 1) are now in the preclinical development stage.13 These approaches all attempt to reverse or prevent the adverse cellular effects of chronic adrenergic signaling, such as the uncoupling of β-ARs by GRK-mediated phosphorylation, the under-phosphorylation of phospholamban per unit of adrenergic stimulation and the hypofunction of SERCA2.
CONCLUSIONHF is an increasingly prevalent disease.1 The dysregulation of β-AR signaling and signal transduction are key determinants in the natural history of this disorder. Extensive
research into β-adrenergic-blocking agents has led to important therapeutic advances for HF. These findings could potentially be extended by the use of new information, such as identi-fied genetic poly morphisms, to prospectively identify nonresponders or hyper-responders to β-adrenergic-blocking drugs. Future therapeutic strategies could target discrete portions of the β-adrenergic signaling cascade to affect specific pathways, while leaving other signaling cascades unperturbed. These pathways could be modi-fied by alteration of protein expression with intra cellular antagonists, gene therapy or both. Further studies involving animal models and large clinical trials will be necessary to determine the role of these additional signal-transduction targets in the treatment of HF.
References1 American Heart Association Heart Disease and Stroke
Statistics 2005 Update [http://www.americanheart.org/presenter.jhtml?identifier=1928] (accessed 23 March 2005)
2 Lefkowitz RJ et al. (2000) Catecholamines, cardiac β-adrenergic receptors, and heart failure. Circulation 101: 1634–1637
3 Port JD and Bristow MR (2001) Altered β-adrenergic receptor gene regulation and signaling in chronic heart failure. J Mol Cell Cardiol 33: 887–905
4 Kaye DM et al. (2004) Interaction between cardiac sympathetic drive and heart rate in heart failure: modulation by adrenergic receptor genotype. J Am Coll Cardiol 44: 2008–2015
5 Bristow MR (2000) β-adrenergic receptor blockade in chronic heart failure. Circulation 101: 558–569
6 Domanski MJ et al. (2003) A comparative analysis of the results from 4 trials of β-blocker therapy for heart failure: BEST, CIBIS-II, MERIT-HF, and COPERNICUS. J Card Fail 9: 354–363
7 Skeberdis VA (2004) Structure and function of β3-adrenergic receptors. Medicina (Kaunas) 40: 407–413
8 Brodde OE and Michel MC (1999) Adrenergic and muscarinic receptors in the human heart. Pharmacol Rev 51: 651–690
9 Kohout TA et al. (2001) Augmentation of cardiac contractility mediated by the human β3-adrenergic receptor overexpressed in the hearts of transgenic mice. Circulation 104: 2485–2491
10 Konkar AA et al. (2000) β1-adrenergic receptors mediate β3-adrenergic-independent effects of CGP 12177 in brown adipose tissue. Mol Pharmacol 57: 252–258
11 Heubach JF et al. (2002) Physiological antagonism between ventricular β1-adrenoceptors and α1-adrenoceptors but no evidence for β2- and β3-adrenoceptor function in murine heart. Br J Pharmacol 136: 217–229
12 Feldman DS et al. (2002) Selective inhibition of heterotrimeric Gs signaling. Targeting the receptor-G protein interface using a peptide minigene encoding the Gαs carboxyl terminus. J Biol Chem 277: 28631–28640
13 Lohse MJ et al. (2003) What is the role of β-adrenergic signaling in heart failure? Circ Res 93: 896–906
14 Koch WJ et al. (1995) Cardiac function in mice overexpressing the β-adrenergic receptor kinase or a β ARK inhibitor. Science 268: 1350–1353
Nature Publishing Group© 2005

REVIEW
482 NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE FELDMAN ET AL. SEPTEMBER 2005 VOL 2 NO 9
www.nature.com/clinicalpractice/cardio
15 Marx SO et al. (2000) PKA phosphorylation dissociates FKBP12.6 from the calcium release channel (ryanodine receptor): defective regulation in failing hearts. Cell 101: 365–376
16 Biel M et al. (2002) Cardiac HCN channels: structure, function, and modulation. Trends Cardiovasc Med 12: 206–212
17 Colucci WS (1998) The effects of norepinephrine on myocardial biology: implications for the therapy of heart failure. Clin Cardiol 21 (Suppl 1): I20–I24
18 Ungerer M et al. (1994) Expression of β-arrestins and β-adrenergic receptor kinases in the failing human heart. Circ Res 74: 206–213
19 Brodde OE et al. (1992) Receptor systems affecting force of contraction in the human heart and their alterations in chronic heart failure. J Heart Lung Transplant 11 (Pt 2): S164–S174
20 Lorenz K et al. (2003) Protein kinase C switches the Raf kinase inhibitor from Raf-1 to GRK-2. Nature 426: 574–579
21 Theilade J et al. (2001) G protein-coupled receptor kinase 2—a feedback regulator of Gq pathway signalling. Curr Drug Targets Immune Endocr Metabol Disord 1: 139–151
22 Hata JA et al. (2004) Genetic manipulation of myocardial β-adrenergic receptor activation and desensitization. J Mol Cell Cardiol 37: 11–21
23 Engelhardt S et al. (1999) Progressive hypertrophy and heart failure in β1-adrenergic receptor transgenic mice. Proc Natl Acad Sci U S A 96: 7059–7064
24 Milano CA et al. (1994) Enhanced myocardial function in transgenic mice overexpressing the β 2-adrenergic receptor. Science 264: 582–586
25 Xiao RP et al. (1999) Recent advances in cardiac β2-adrenergic signal transduction. Circ Res 85: 1092–1100
26 Luttrell LM (2003) ‘Location, location, location’: activation and targeting of MAP kinases by G protein-coupled receptors. J Mol Endocrinol 30: 117–126
27 Lohse MJ et al. (1996) Mechanisms of β-adrenergic receptor desensitization: from molecular biology to heart failure. Basic Res Cardiol 91 (Suppl 2): 29–34
28 Walker JK et al. (2004) G protein-coupled receptor kinase 5 regulates airway responses induced by muscarinic receptor activation. Am J Physiol Lung Cell Mol Physiol 286: L312–L319
29 McDonald PH et al. (2000) β-arrestin 2: a receptor-regulated MAPK scaffold for the activation of JNK3. Science 290: 1574–1577
30 Singh K et al. (2001) Adrenergic regulation of cardiac myocyte apoptosis. J Cell Physiol 189: 257–265
31 Zhu WZ et al. (2003) Linkage of β1-adrenergic stimulation to apoptotic heart cell death through protein kinase A-independent activation of Ca2+/calmodulin kinase II. J Clin Invest 111: 617–625
32 Pearson G et al. (2001) Mitogen-activated protein (MAP) kinase pathways: regulation and physiological functions. Endocr Rev 22: 153–183
33 Mann DL et al. (1992) Adrenergic effects on the biology of the adult mammalian cardiocyte. Circulation 85: 790–804
34 Communal C et al. (1999) Opposing effects of β1- and β2-adrenergic receptors on cardiac myocyte apoptosis: role of a pertussis toxin-sensitive G protein. Circulation 100: 2210–2212
35 Communal C et al. (2003) β1 integrins expression in adult rat ventricular myocytes and its role in the regulation of β-adrenergic receptor-stimulated apoptosis. J Cell Biochem 89: 381–388
36 Adams JW and Brown JH (2001) G-proteins in growth and apoptosis: lessons from the heart. Oncogene 20: 1626–1634
37 Abraham WT et al. (2002) Coordinate changes in myosin heavy chain isoform gene expression are selectively associated with alterations in dilated cardiomyopathy phenotype. Mol Med 8: 750–760
38 Lowes BD et al. (2002) Myocardial gene expression in dilated cardiomyopathy treated with β-blocking agents. N Engl J Med 346: 1357–1365
39 Schmidt AG et al. (2001) Phospholamban: a promising therapeutic target in heart failure? Cardiovasc Drugs Ther 15: 387–396
40 Dorn GW and Molkentin JD (2004) Manipulating cardiac contractility in heart failure: data from mice and men. Circulation 109: 150–158
41 Frey N et al. (2000) Decoding calcium signals involved in cardiac growth and function. Nat Med 6: 1221–1227
42 El Armouche A et al. (2003) Evidence for protein phosphatase inhibitor-1 playing an amplifier role in β-adrenergic signaling in cardiac myocytes. FASEB J 17: 437–439
43 Diaz-Infante E et al. (2005) Predictors of lack of response to resynchronization therapy. Am J Cardiol 95: 1436–1440
44 Adamson PB and Abraham WT (2003) Cardiac resynchronization therapy for advanced heart failure. Curr Treat Options Cardiovasc Med 5: 301–309
45 Rau T et al. (2002) Effect of the CYP2D6 genotype on metoprolol metabolism persists during long-term treatment. Pharmacogenetics 12: 465–472
46 Wuttke H et al. (2002) Increased frequency of cytochrome P450 2D6 poor metabolizers among patients with metoprolol-associated adverse effects. Clin Pharmacol Ther 72: 429–437
47 Cascorbi I et al. (2004) Pharmacogenomics of heart failure—focus on drug disposition and action. Cardiovasc Res 64: 32–39
48 Terra SG et al. (2005) β-adrenergic receptor polymorphisms and responses during titration of metoprolol controlled release/extended release in heart failure. Clin Pharmacol Ther 77: 123–126
49 Drysdale CM et al. (2000) Complex promoter and coding region β2-adrenergic receptor haplotypes alter receptor expression and predict in vivo responsiveness. Proc Natl Acad Sci U S A 97: 10483–10488
50 Hein L (2001) Physiological significance of β-adrenergic receptor polymorphisms: in-vivo or in-vitro veritas? Pharmacogenetics 11: 187–189
51 Mason DA et al. (1999) A gain-of-function polymorphism in a G-protein coupling domain of the human β1-adrenergic receptor. J Biol Chem 274: 12670–12674
52 Small KM et al. (2002) Synergistic polymorphisms of β1- and α2c-adrenergic receptors and the risk of congestive heart failure. N Engl J Med 347: 1135–1142
53 Small KM et al. (2003) Pharmacology and physiology of human adrenergic receptor polymorphisms. Annu Rev Pharmacol Toxicol 43: 381–411
54 Borjesson M et al. (2000) A novel polymorphism in the gene coding for the β1-adrenergic receptor associated with survival in patients with heart failure. Eur Heart J 21: 1853–1858
55 Turki J et al. (1996) Myocardial signaling defects and impaired cardiac function of a human β2-adrenergic receptor polymorphism expressed in transgenic mice. Proc Natl Acad Sci U S A 93: 10483–10488
56 Liggett SB et al. (1998) The Ile164 β2-adrenergic receptor polymorphism adversely affects the outcome of congestive heart failure. J Clin Invest 102: 1534–1539
57 Bristow MR et al. (2003) Selective versus nonselective β-blockade for heart failure therapy: are there lessons to be learned from the COMET trial? J Card Fail 9: 444–453
Nature Publishing Group© 2005

REVIEW
SEPTEMBER 2005 VOL 2 NO 9 FELDMAN ET AL. NATURE CLINICAL PRACTICE CARDIOVASCULAR MEDICINE 483
www.nature.com/clinicalpractice/cardio
58 Bristow MR et al. (2004) Effect of baseline or changes in adrenergic activity on clinical outcomes in the β-blocker evaluation of survival trial. Circulation 110: 1437–1442
59 Maack C et al. (2000) Different intrinsic activities of bucindolol, carvedilol and metoprolol in human failing myocardium. Br J Pharmacol 130: 1131–1139
60 Liggett SB (2004) Polymorphisms of β-adrenergic receptors in heart failure. Am J Med 117: 525–527
61 Mialet Perez J et al. (2003) β1-adrenergic receptor polymorphisms confer differential function and predisposition to heart failure. Nat Med 9: 1300–1305
Competing interestsD Feldman and MR Bristow declared competing interests; go to the article online for details. The other authors declared they have no competing interests.
62 Terra SG et al. (2005) β1-adrenergic receptor polymorphisms and left ventricular remodeling changes in response to β-blocker therapy. Pharmacogenet Genomics 15: 227–234
63 de Groote PA et al. (2005) Association between β-1 and β-2 adrenergic receptor gene polymorphisms and the response to β-blockade in patients with stable congestive heart failure. Pharmacogenet Genomics 15: 137–142
64 White HL et al. (2003) An evaluation of the β-1 adrenergic receptor Arg389Gly polymorphism in individuals with heart failure: a MERIT-HF sub-study. Eur J Heart Failure 5: 463–468
65 Bristow MR et al. (2001) Inotropes and β-blockers: is there a need for new guidelines? J Card Fail 7 (2 Suppl 1): 8–12
Nature Publishing Group© 2005